What is adrenal cancer
Adrenal cancer also called adrenocortical cancer or adrenal cortical carcinoma, is a very rare cancer with an incidence of 0.7–2.0 cases/million people per year 1, that begins in the adrenal cortex of the adrenal glands located on top of your kidneys. Adrenal glands produce hormones that give instructions to virtually every organ and tissue in your body. Adrenal cancer occurs at any age, with two peak incidence: the first one in the first decade in children and the second one between 40 and 50 years. Women are most frequently affected (55–60%) 2.
Adrenal cancer is often aggressive. When found early, there is a chance for cure. But if the cancer has spread to areas beyond the adrenal gland, cure becomes less likely. Treatment can be used to delay progression or recurrence.
Not all growths that form in the adrenal glands are cancer. Noncancerous (benign) adrenal tumors, such as adenoma or pheochromocytoma, also can develop in the adrenal glands.
Diagnosing adrenal cancer involves blood and urine tests to look for unusual levels of hormones produced by the adrenal glands. Imaging tests like CT scans and MRI are used to look for growths on your adrenal glands. Surgery to remove the adrenal gland allows doctors to examine the tissue for cancer cells.
Adrenal cancer treatment usually involves surgery to remove the adrenal gland. Other treatments include radiation using high-powered beams like X-rays, and chemotherapy with drugs that kill cancer cells,
Can adrenal cancer be found early?
It is hard to find adrenal cancers early, and they are often quite large by the time they are diagnosed.
Adrenal cancers are often found earlier in children than in adults because cancers in children are more likely to secrete hormones that lead to signs and symptoms. For example, children may develop signs of puberty at an early age due to sex hormones made by adrenal cancer cells.
These tumors are sometimes found early by accident in adults, such as when a CT (computed tomography) scan of the abdomen is done for some other health concern.
About the adrenal glands
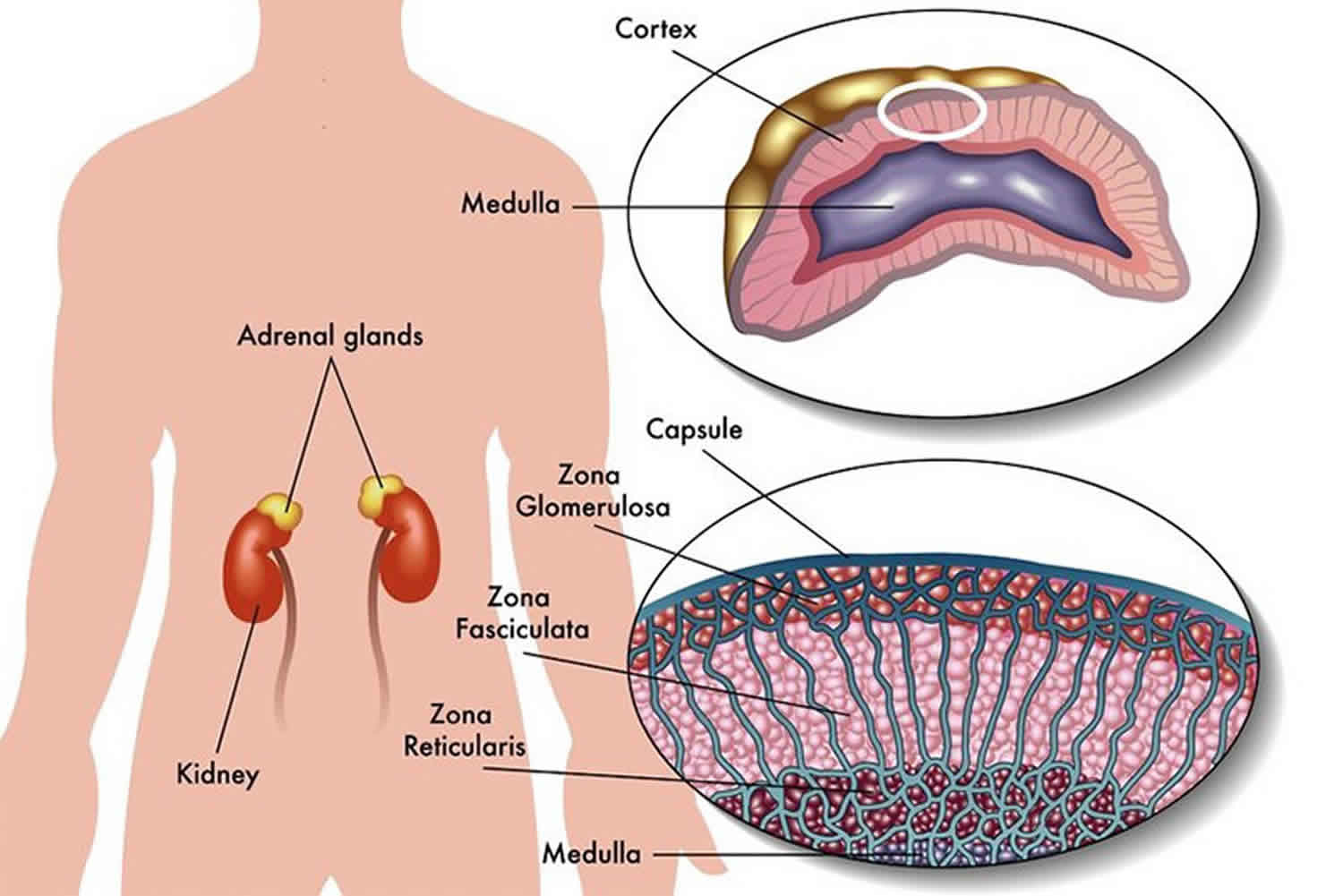
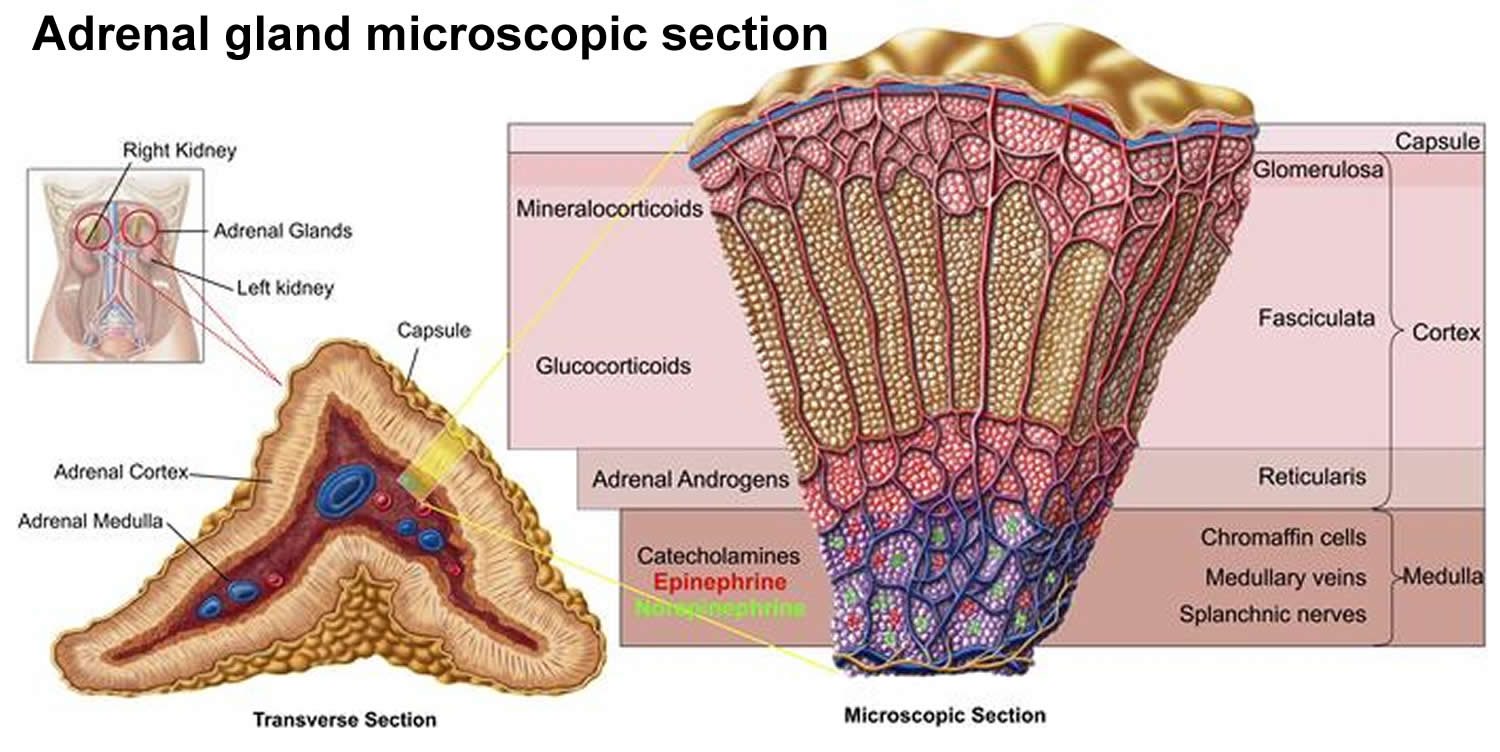
The adrenals are small glands that sit above each of the kidneys. The kidneys are located deep inside the upper part of the abdomen. Each adrenal gland has 2 parts. The outer part, the adrenal cortex, is where most tumors develop. The adrenal cortex makes certain hormones for the body. These hormones all have a similar chemical structure and are called steroids:
- Cortisol causes changes in metabolism to help the body to handle stress.
- Aldosterone helps the kidneys regulate the amount of salt in the blood and helps regulate blood pressure.
- Adrenal androgens can be converted to more common forms of the sex hormones estrogen and testosterone in other parts of the body. The amount of these hormones that result from conversion of adrenal androgens is small compared to what is made in other parts of the body. The testicles produce most of the androgens (male hormones) in men. The ovaries produce most of the estrogens (female hormones) in women.
Non cancerous (benign) or cancerous (malignant) adrenal cortical tumors can make too much of any of these hormones. The hormones may cause symptoms that affect your whole body.
The inner part of the adrenal gland, the adrenal medulla, is really an extension of the nervous system. Nervous system hormones such as norepinephrine and epinephrine (also called adrenaline) are made in the medulla. Tumors and cancers that start in the adrenal medulla include pheochromocytomas (which are most often benign) and neuroblastomas.
Figure 1. Adrenal gland anatomy
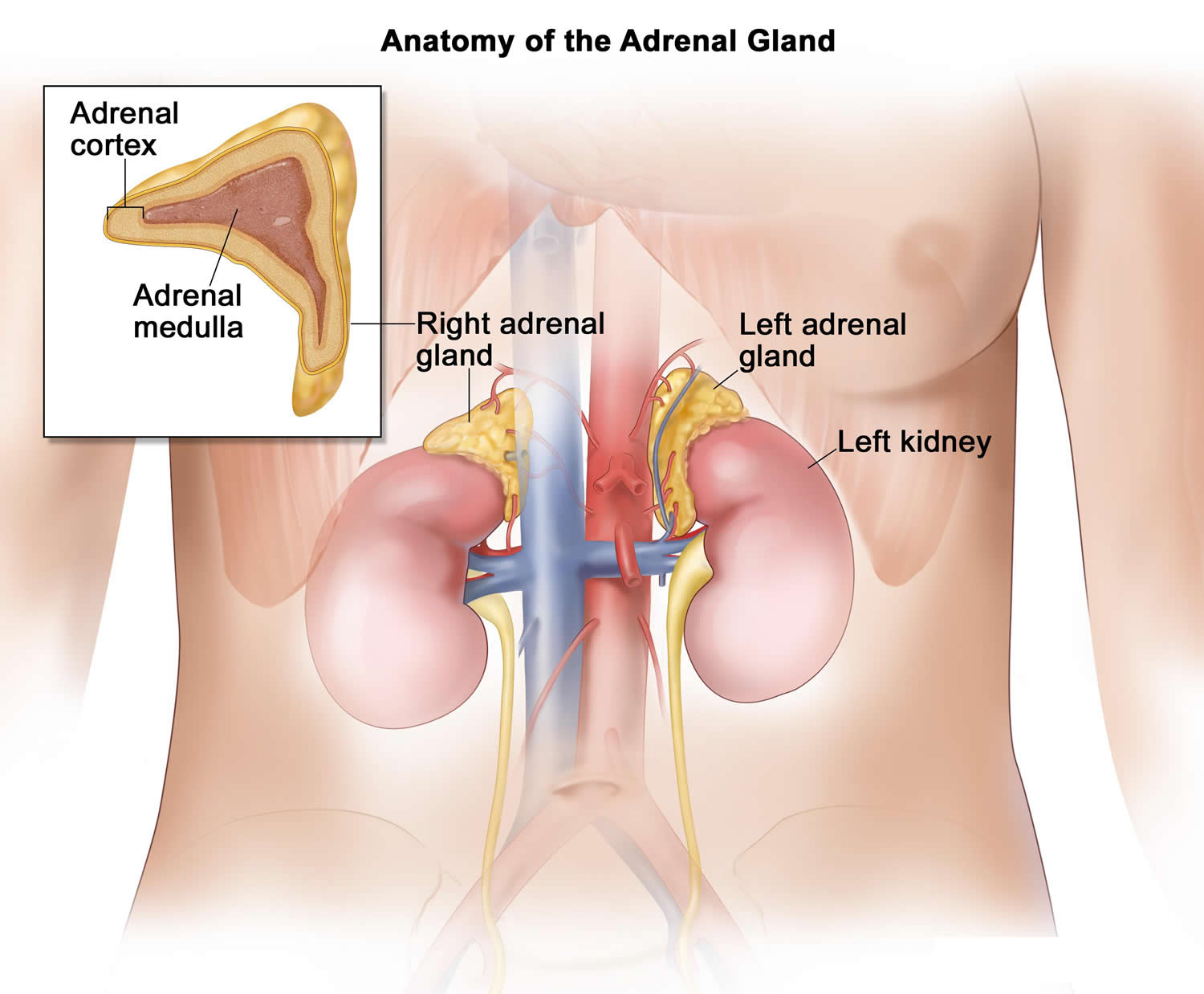
Figure 2. Adrenal gland microscopic section
Adrenal cortex tumors
The 2 main types of adrenal cortex tumors are:
- Adenomas (benign or non-cancerous tumors)
- Carcinomas (malignant or cancerous tumors)
These types of tumors can sometimes be hard to tell apart when the cells are looked at under the microscope. Sometimes the only way to know for sure that an adrenal tumor is a cancer is when it spreads to lymph nodes or other organs and tissues. Adenomas do not spread outside the adrenal gland.
Adrenal cortex adenomas
Most tumors of the adrenal cortex are benign tumors known as adenomas. These tumors are usually less than 2 inches (5 centimeters) across. They usually occur in only one adrenal gland, but sometimes both.
Most people with adrenal adenomas have no symptoms and don’t know that they have an adrenal tumor. Some of these adenomas are discovered by accident (incidentally) when CT or MRI scans of the abdomen are done because of an unrelated health problem. About 5% of people who have a CT scan of the abdomen are found to have an adrenal tumor that was not suspected. Many of these are nonfunctional, meaning that they don’t make adrenal hormones. Sometimes these tumors are known by the nickname incidentalomas because they aren’t causing problems and were only found by accident.
Some adenomas make too many adrenal steroid hormones. Sometimes the excess hormones can cause the same symptoms as those from adrenal carcinomas (cancers). Adenomas are much more likely than carcinomas to make high levels of aldosterone, which can cause high blood pressure.
Treatment
Adenomas can be cured by removing the adrenal gland that contains the adenoma. Some adrenal adenomas that cause hormone-related symptoms can be treated effectively with drugs that block the production or actions of these hormones. This may be the best treatment choice for patients with other serious medical problems who might not be able to have a major operation.
The treatment of an adenoma depends on the chance that it may be a cancer and whether or not it is raising hormone levels. When an adrenal tumor is found accidentally, tests are often done to see if it is making hormones. If it is, surgery is often recommended. Otherwise, surgery may only be recommended if it is likely to be a cancer. Small tumors are less likely to be cancer, and are often watched but not treated right away. The CT (or MRI) scan can be repeated in 6 to 24 months to see if the tumor has grown. If it has, it may need to be removed. If it hasn’t grown, hormone levels will be watched over the next few years. If the tumor stays small and doesn’t make any hormones, it might not need to be treated at all.
Adrenal cortex cancer
The type of cancer that develops in the cortex of the adrenal gland is called adrenal cortical carcinoma or just adrenal cancer. This rare type of cancer is also known as adrenocortical cancer (or carcinoma).
Adrenal cancer most often is discovered when:
- It is found accidentally on an imaging test done to look for something else.
- It makes hormones that cause changes such as weight gain and fluid retention, early puberty in children, or excess facial or body hair growth in women.
- It starts causing symptoms because it has gotten very large. Large tumors can press on other organs in the abdomen, causing pain or a feeling of fullness. Generally, adrenal cancers are much larger than adrenal adenomas. An adrenal tumor larger than 5 or 6 centimeters (about 2 to 2 1/2 inches) is assumed to be a cancer. In one study, the average size of an adrenal cancer was about 13 cm (5 inches).
Most cancers found in the adrenal gland did not start there and are not adrenal cancers. Instead, they started in other organs or tissues and then spread (metastasize) through the bloodstream to the adrenal glands. For example, lung cancers, melanomas, and breast cancers often spread to the adrenals. When other cancers spread to the adrenals, they are not considered adrenal cancer. They are named and treated based on the place where they started.
Cancers that spread to the adrenal glands
Cancer can start to grow elsewhere in the body and spread to the adrenal glands. This is called secondary cancer. Secondary cancer in the adrenal glands is more common than cancer that starts in the adrenal glands.
For example, kidney cancer can spread to the adrenal glands. This is known as secondary cancer and would be treated as kidney cancer, not an adrenal gland cancer.
You should look for information about your primary cancer type if you cancer has spread to the adrenal glands.
Adrenal cancer causes
Experts do not know exactly what causes most adrenal cancers (adrenal cortical tumors). Over the past several years, experts have made great progress in understanding how certain changes in a person’s DNA can cause cells in the adrenal gland to become cancerous. DNA is the chemical in our cells that makes up our genes, which controls nearly everything the cells do. We usually look like our parents because they are the source of our DNA. But DNA affects more than just the way we look. It also determines our risk for developing certain diseases, including some types of cancer.
- Genes that help our cells grow and divide are called oncogenes.
- Genes that slow down cancer cell division or make them die at the right time are called tumor suppressor genes.
Cancers can be caused by DNA mutations (changes) that turn on oncogenes or turn off tumor suppressor genes. Some people with cancer have inherited DNA mutations from a parent, which increase their risk for developing the disease. But most DNA mutations that are seen in cancers happen during life rather than having been inherited. Some of these mutations may result from exposure to things like radiation or cancer-causing chemicals. But most of these mutations seem to happen for no apparent reason, without having an outside cause.
Some of the DNA mutations that cause adrenal tumors in people with genetic syndromes are discussed in adrenal cancer risk factors below. Overall though, these rarely cause adrenal cortical cancer. However, because adrenal cancer is so rare, if you have adrenal cancer, it may be worthwhile to consider genetic testing to find out if you have one of these syndromes. If you do, you (and your family members) might have an increased risk of developing other cancers also.
The Li-Fraumeni syndrome is caused by inherited mutations that inactivate the TP53 tumor suppressor gene. This syndrome causes a small portion of adrenal cancer in adults (about 1 of every 20), but it’s often the cause of adrenal cancer in children. In fact, about 8 of every 10 cases of adrenal cancer in children are caused by Li-Fraumeni syndrome. Many other adrenal cancers have also been found to have TP53 gene changes that were acquired after birth (not inherited).
Adrenal cancer risk factors
A risk factor is anything that changes your chance of getting a disease such as cancer. Different cancers have different risk factors. Some risk factors, like smoking, can be changed. Others, like a person’s age or family history, can’t be changed.
Scientists have found few risk factors that make a person more likely to develop adrenal cancer. Even if a patient does have one or more risk factors for adrenal cancer, it is impossible to know for sure how much that risk factor contributed to causing the cancer.
But having a risk factor, or even several, does not mean that you will get the disease. Many people with risk factors never develop adrenal cancer, while others with this disease may have few or no known risk factors.
Genetic syndromes
The majority of adrenal cortex cancers are not inherited (sporadic occurrence), but some (up to 15%) are caused by a genetic defect. This is more common in adrenal cancers in children.
Li-Fraumeni syndrome
The Li-Fraumeni syndrome is a rare condition that is most often caused by a defect in the TP53 gene. People with this syndrome have a high risk of several types of cancer, including include breast cancer, bone cancer, brain cancer, and adrenal cortex cancer.
Beckwith-Wiedemann syndrome
People with this problem have large tongues, are large themselves, and have an increased risk for developing cancers of the kidney, liver and adrenal cortex.
Multiple endocrine neoplasia (MEN1)
People with multiple endocrine neoplasia (MEN1) have a very high risk of developing tumors of 3 glands: the pituitary, parathyroid, and pancreas. About one-third to one-half of people with this condition also develop adrenal adenomas (benign tumors) or enlarged adrenal glands. These usually do not cause any symptoms. This syndrome is caused by defects in a gene called multiple endocrine neoplasia (MEN1). People who have a family history of multiple endocrine neoplasia (MEN1) or pituitary, parathyroid, pancreas, or adrenal cancers should ask their doctor if they might benefit from genetic counseling.
Familial adenomatous polyposis
People with this syndrome develop hundreds of polyps in the large intestine. These polyps will lead to colon cancer if the colon is not removed. Familial adenomatous polyposis also increases the risk of other cancers, and may increase the risk for adrenal cancer. Still, most adrenal tumors in patients with familial adenomatous polyposis are benign adenomas. This syndrome is caused by defects in a gene called APC.
Lynch syndrome or hereditary nonpolyposis colorectal cancer
Lynch syndrome (formerly known as HNPCC) is an inherited genetic disorder that increases the risk of colorectal cancer, stomach cancer, and some other cancers, including adrenal cortex cancer. In most cases, this disorder is caused by a defect in either the MLH1 or MSH2 gene, but other genes can cause Lynch syndrome, including MLH3, MSH6, TGFBR2, PMS1, and PMS2.
Lifestyle and environmental factors
Risk factors such as being overweight, smoking, living a sedentary lifestyle, and being exposed to cancer-causing substances in the environment can affect a person’s risk of many types of cancer. Although none of these factors has been found to definitely influence a person’s risk of developing adrenal cancer, smoking has been suggested as a risk factor by some researchers.
Adrenal cancer signs and symptoms
In about half of people with adrenal cancer, symptoms are caused by the hormones made by the tumor. In the other half, symptoms occur because the tumor has grown so large that it presses on nearby organs. If you or your child has any of the signs or symptoms described here, discuss them with your doctor without delay. These symptoms may be caused by an adrenal tumor or by something else. Getting the proper medical tests is the only way to find out and to get the proper treatment, if needed.
Symptoms caused by androgen or estrogen production
In children, symptoms are most often caused by the androgens (male-type hormones) that the tumor secretes. The most common symptoms are excessive growth of facial and body hair (such as in the pubic and underarm areas). Male hormones may also enlarge the penis in boys or the clitoris in girls.
If the tumor secretes estrogens (female-type hormones), girls can start puberty early. This can cause breasts to develop and menstrual periods to start. Estrogen-producing tumors can also enlarge breasts in boys.
The symptoms from high levels of sex hormones are less noticeable in adults because they have already gone through puberty and have breasts and adult patterns of body hair. Women with estrogen-producing tumors and men with androgen-producing tumors usually do not have any symptoms from the hormones, so they might not have symptoms until the tumor is large enough to press on nearby organs.
Symptoms are easier to notice if the tumor is making the hormone usually found in the opposite sex. For example, men with tumors that make estrogen may notice their breasts becoming enlarged and tender. They may also have sexual problems such as erectile dysfunction (impotence) and loss of sex drive. Women with tumors that make androgens (male hormones) may notice excessive facial and body hair growth, a receding hairline, irregular menstrual periods, and deepening of their voice.
Symptoms caused by cortisol production
Excessive levels of cortisol causes a problem known as Cushing syndrome. Some people have all of these symptoms, but many people with high cortisol levels have only a few. Possible signs and symptoms include:
- Weight gain, usually greatest above the collar bone, in the cheek area (moon face), and around the abdomen
- Fat deposits behind the neck and shoulders (fatty hump or buffalo hump)
- Purple stretch marks on the abdomen
- Excessive hair growth on the face, chest, and back in women
- Menstrual irregularities
- Weakness and loss of muscle mass in the legs
- Easy bruising
- Depression and/or moodiness
- Weakened bones (osteoporosis), which can lead to fractures
- High blood sugar levels, often leading to diabetes
- High blood pressure
Cushing syndrome may be caused by an adrenal cancer or an adrenal adenoma that makes high levels of cortisol and/or related hormones, but it can also have other causes. For example, benign pituitary gland tumors can make high levels of another hormone called adrenocorticotropic hormone (ACTH). This is often called Cushing disease. The high levels of ACTH in turn cause normal adrenal gland tissue to make more cortisol. This results in the same symptoms as Cushing syndrome. Very rarely, other tumors can make ACTH and cause the same symptoms.
Some people with immune system problems or some cancers, such as lymphomas, are treated with drugs chemically related to cortisol.
Because there are so many causes of high cortisol levels that can lead to Cushing syndrome, doctors do a number of tests to find out whether the patient has an adrenal cortical tumor or some other cause of Cushing syndrome.
Symptoms caused by aldosterone production
The main signs and symptoms caused by aldosterone-producing adrenal tumors are:
- High blood pressure
- Weakness
- Muscle cramps
- Low blood potassium levels
Adrenal adenomas often make aldosterone, but adrenal cancers rarely do.
Symptoms caused by a large adrenal cancer pressing on nearby organs
As an adrenal cancer grows, it presses on nearby organs and tissues. This may cause pain near the tumor, a feeling of fullness in the abdomen, or trouble eating because of a feeling of filling up easily.
Adrenal cancer diagnosis
Medical history and physical exam
If you have signs or symptoms that suggest adrenal cancer, the first step is usually for the doctor to take your complete medical history to find out more about them.
- Your doctor will want to know if anyone in your family has had adrenal cancer or any other type of cancer.
- Your doctor might also ask about your menstrual or sexual function and about any other symptoms you may be having.
A physical exam will give other information about possible signs of adrenal cancer or other health problems.
- Your doctor will thoroughly examine your abdomen for evidence of a tumor (or mass).
- Your blood and urine will likely be tested to look for high levels of the hormones made by some adrenal tumors.
- If an adrenal tumor is suspected, imaging tests will be done to look for it. These tests can also help see if it has spread.
If a mass is seen on an imaging test and it is likely to be an adrenal cancer, doctors will recommend surgery to remove the cancer. Generally, doctors do not recommend a biopsy (removing a sample of the tumor to look at under the microscope to see if it is cancer) before surgery to remove the tumor. This is because doing a biopsy can increase the risk that an adrenal cancer will spread outside of the adrenal gland.
Imaging tests
Chest x-ray
A chest x-ray can show if the cancer has spread to the lungs. It may also be useful to determine if there are any serious lung or heart diseases.
Ultrasound
Ultrasound tests use sound waves to make pictures of parts of the body. A device called a transducer makes the sound waves, which are reflected off of tissues and organs in the body. The pattern of sound wave echoes is detected by the transducer and analyzed by a computer to create an image of these tissues and organs. This test can show if there is a tumor in the adrenal gland. It can also show tumors in the liver if the cancer has spread there. In general, ultrasound is not used to look for adrenal tumors unless a CT scan can’t be done for some reason.
Computed tomography (CT)
CT scans show the adrenal glands fairly clearly and often can confirm the location of the cancer. It can also help show if the cancer has spread into your liver or other nearby organs. CT scans can also show lymph nodes and distant organs where metastatic cancer might be present. The CT scan can help determine if surgery is a good treatment option.
Magnetic resonance imaging (MRI)
Like CT scans, MRI scans show detailed images of soft tissues in the body. But MRI scans use radio waves and strong magnets instead of x-rays. MRI may sometimes provide more information than CT scans because it can better distinguish adrenal cancers from benign tumors.
MRI scans are particularly helpful in examining the brain and spinal cord. In people with suspected adrenal tumors, an MRI of the brain may be done to examine the pituitary gland. Tumors of the pituitary gland, which lies underneath the front of the brain, can cause symptoms and signs similar to adrenal tumor.
Positron emission tomography (PET)
For a PET scan, you are injected with a slightly radioactive form of sugar, which collects mainly in cancer cells. A special camera then creates a picture of areas of radioactivity in the body. The picture is not detailed like a CT or MRI scan, but a PET scan can look for possible areas of cancer spread in all areas of the body at once.
Some machines do both a PET and CT scan at the same time (PET/CT scan). This lets the doctor see areas that “light up” on the PET scan in more detail.
PET scans can be helpful in deciding if an adrenal tumor is likely to be benign or malignant (cancer), and if it may have spread.
Other tests
Laparoscopy
A laparoscope, a thin, flexible tube with a tiny video camera on the end, is inserted through a small surgical opening in the patient’s side to allow the surgeon to see where the cancer is growing. It can be used to help spot distant spread as well as enlarged lymph nodes (which might contain cancer). Sometimes it is combined with ultrasound to give a better picture of the cancer. Laparoscopy may be done to help predict whether it will be possible to completely remove the cancer by surgery. In addition to viewing adrenal tumors through the laparoscope, surgeons can sometimes remove small benign adrenal tumors through this instrument.
Biopsy
Imaging tests may find tumors, but often the only way to know for sure that a tumor is cancer is to remove a sample of tumor tissue to look at under the microscope. This is called a biopsy.
Since adrenal adenomas (benign tumors) and cancers can look alike under the microscope, a biopsy may not be able to tell whether or not an adrenal tumor is cancerous. A needle biopsy of an adrenal cancer also can actually spread tumor cells. For these reasons, a biopsy is generally not done before surgery if an adrenal tumor’s size and certain features seen on imaging tests suggest it is most likely cancer. Blood tests of hormone levels and imaging tests are more useful than biopsies in diagnosing adrenal cancer.
If the cancer appears to have metastasized (spread) to another part of the body such as the liver, then a needle biopsy of the metastasis may be done. If a patient is known to have an adrenal tumor and a liver biopsy shows adrenal cells are present in the liver, then the tumor is cancer.
In general, a biopsy is only done in a patient with adrenal cancer when there are tumors outside the adrenals and the doctor needs to know if these tumors are from the adrenal cancer or are caused by some other cancer or disease. Tumors in the adrenal glands are sometimes biopsied when the patient is known to have a different type of cancer (like lung cancer), and knowing if it has spread to the adrenal glands would alter treatment.
Blood and urine tests for adrenal hormones
Blood and urine tests to measure levels of adrenal hormones are important in deciding whether a patient with signs and symptoms of adrenal cancer has the disease. For urine tests, you may be asked to collect all of your urine for 24 hours. Blood and urine tests are as important as imaging tests in diagnosing adrenal cancer. Doctors might choose which tests to do based on the patient’s symptoms. But often doctors will check hormone levels even when symptoms of high hormone levels are not present. This is because symptoms of abnormal hormone levels can be very subtle, and blood tests might be able to detect changes in hormone levels even before symptoms occur.
Tests for high cortisol levels
The levels of cortisol are measured in the blood and in the urine. If an adrenal tumor is making cortisol, these levels will be abnormally high. These tests may be done after giving the patient a dose of dexamethasone. Dexamethasone is a drug that acts like cortisol. If given to someone who does not have an adrenal tumor, it will lower levels of cortisol and similar hormones. In someone with an adrenal cortex tumor, these hormone levels will remain high after they receive dexamethasone. Blood levels of another hormone called ACTH will also be measured to help distinguish adrenal tumors from other diseases that can cause high cortisol levels.
Tests for high aldosterone levels
The level of aldosterone will be measured and will be high if the tumor is making aldosterone. High aldosterone can also lead to low blood levels of potassium and renin (a hormone made by the kidneys) .
Tests for high androgen or estrogen levels
Patients with androgen-producing tumors will have high levels of dehydroepiandrosterone sulfate (DHEAS) or testosterone. Patients with estrogen-producing tumors will have high levels of estrogen in their blood.
Adrenal cancer stages
After someone is diagnosed with adrenal cancer, doctors will try to figure out if it has spread, and if so, how far. This process is called staging. The stage of a cancer describes how far the cancer has spread in the body. It helps determine how serious the cancer is and how best to treat it. The stage is one of the most important factors in deciding how to treat the cancer and determining how successful treatment might be.
To determine the cancer’s stage after an adrenal cancer diagnosis, doctors try to answer these questions:
- How large is the cancer?
- Has the cancer grown into nearby structures or organs?
- Has the cancer spread to nearby lymph nodes or to distant organs?
The stage of adrenal cancer is based on the results of physical exams, biopsies, and imaging tests (CT or MRI scan, x-rays, PET scan, etc.), which are described in tests for adrenal cancer above, as well as the results of surgery.
The adrenal cancer stages range from stages I (1) through IV (4). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means a more advanced cancer. Cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
Understanding your adrenal cancer stage
A staging system is a standard way for the cancer care team to describe how far a cancer has spread. Two major staging systems used for adrenal cancer are the American Joint Committee on Cancer (AJCC) TNM staging system and the ENSAT (European Network for the Study of Adrenal Tumors) staging system. Both are based on the same TNM categories, which are based on 3 key pieces of information:
- T describes the size of the main (primary) tumor and whether it has grown into nearby areas.
- N indicates any cancer spread to lymph nodes near the adrenal gland (regional lymph nodes). Lymph nodes are small bean-sized collections of immune system cells, to which cancers often spread first.
- M indicates if the cancer has spread (metastasized) to distant sites, such as other organs or lymph nodes that are not near the adrenal gland (distant lymph nodes).
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, and M categories have been determined, usually after surgery, this information is combined in a process called stage grouping to assign an overall stage (numbered 1 through 4).
The staging system in the table below uses the pathologic stage. It is based on the results of physical exam, biopsy, imaging tests, and the results of surgery. This is likely to be more accurate than clinical staging, which only takes into account the tests done before surgery.
Adrenal cancer staging can be complex. If you have any questions about your stage, please ask your doctor to explain it to you in a way you understand.
Table 1. Adrenal cancer stages
| ENSAT stage | AJCC Stage | Stage grouping | Stage description |
| I | I | T1 N0 M0 | The tumor is 5 cm (about 2 inches) or less in size and it has not grown into tissues outside the adrenal gland (T1). It has not spread to nearby lymph nodes (N0) or distant sites (M0). |
| II | II | T2 N0 M0 | The tumor is greater than 5 cm (2 inches) in size and it has not grown into tissues outside the adrenal gland (T2). It has not spread to nearby lymph nodes (N0) or distant sites (M0). |
| III | III | T1 N1 M0 | The tumor is 5 cm (about 2 inches) or less in size and it has not grown into tissues outside the adrenal gland (T1). The cancer has spread to nearby lymph nodes (N1) but not to distant sites (M0). |
| OR | |||
| T2 N1 M0 | The tumor is greater than 5 cm (2 inches) in size and it has not grown into tissues outside the adrenal gland (T2). The cancer has spread to nearby lymph nodes (N1) but not to distant sites (M0). | ||
| OR | |||
| T3 Any N M0 | The tumor is growing in the fat that surrounds the adrenal gland. The tumor can be any size (T3). It might or might not have spread to nearby lymph nodes (Any N0). It has not spread to distant sites (M0). | ||
| OR | |||
| T4 Any N M0 | The tumor is growing into nearby organs, such as the kidney, pancreas, spleen, and liver or large blood vessels (renal vein or vena cava). The tumor can be any size (T4). It may or may not have spread to nearby lymph nodes (Any N). It has not spread to distant organs (M0). | ||
| IV | IV | Any T Any N M1 | The cancer has spread to distant sites like the liver or lungs (M1). It can be any size (Any T) and may or may not have spread to nearby tissues (Any T) or lymph nodes (Any N). |
The following additional categories are not listed on the table above:
- TX: Main tumor cannot be assessed due to lack of information
- T0: No evidence of a primary tumor
- NX: Regional lymph nodes cannot be assessed due to lack of information
Adrenal cancer prognosis
Three major criteria are mandatory in order to define the disease free survival for the localized adrenal cancer (stage 1, 2, and some 3) and the overall survival for stage 4 adrenal cancer 1:
- Staging;
- Resection status “R”;
- Grading (proliferation index, as Ki67% and mitotic count).
Staging
As mentioned above, staging is mandatory to assess prognosis. Five-year stage-dependent survival is 66–82% for stage 1, 58–64% for stage 2, 24–50% for stage 3, and 0–17% for stage 4, according to different series 4, 5, 6, 7.
Resection status “R”
In localized adrenal cancer, surgery is the single most important intervention and the complete resection (R0) correlates with a better prognosis 8. In fact, an incomplete microscopic resection (R1), an incomplete macroscopic resection (R2) or unknown resection (Rx) are associated with the worst overall survival of 20 and 15%, respectively 8.
Grading
Proliferation index, as Ki67 and mitotic count help to assess the adrenal cancer prognosis. Very recently, a large European study in localized adrenal cancer identified Ki67 as the single most important factor predicting recurrence in patients following R0 resection 9. Thus, evaluation of Ki67 indices should be introduced as standard grading in all pathology reports of adrenal cancer patients 9. More recently, in a large European study on stage 4 adrenal cancer, the tumor grading, as the association of the Ki67 and the Weiss score, has been considered as an important prognostic parameter of overall survival 10, confirming the data on the mitotic count showed in a previous French series 11.
Molecular markers
Molecular markers issued form genomic and epigenomic analyses are emerging and need to be confronted to the previous mentioned criteria. Hypermethylation status, miRNA profile or driver genes mutations, as TP53, ZNRF3, β-catenin constitute valuable candidates that could integrate a future clinico-molecular prognostic classification of adrenal cancer patients 12.
Adrenal cancer survival rate
Survival rates tell you what portion of people with the same type and stage of cancer are still alive a certain length of time (usually 5 years) after they were diagnosed. These numbers can’t tell you how long you will live, but they might help give you a better understanding about how likely it is that your treatment will be successful.
Statistics on the outlook for people with a certain type and stage of cancer are often given as 5-year survival rates, but many people live longer – often much longer – than 5 years. The 5-year survival rate is the percentage of people who live at least 5 years after being diagnosed with cancer. For example, a 5-year survival rate of 90% means that an estimated 90 out of 100 people who have that cancer are still alive 5 years after being diagnosed.
Relative survival rates are often a more accurate way to estimate the effect of cancer on survival. These rates compare people with adrenal cancer to people in the overall population. For example, if the 5-year relative survival rate for a specific type and stage of cancer is 90%, it means that people who have that cancer are, on average, about 90% as likely as people who don’t have that cancer to live for at least 5 years after being diagnosed.
But remember, the 5-year relative survival rates are estimates – your outlook can vary based on a number of factors specific to you.
Cancer survival rates don’t tell the whole story
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any particular person’s case. There are a number of limitations to remember:
- The numbers below are among the most current available. But to get 5-year survival rates, doctors have to look at people who were treated at least 5 years ago. As treatments are improving over time, people who are now being diagnosed with adrenal cancer may have a better outlook than these statistics show.
- These statistics are based on the stage of the cancer when it was first diagnosed. They do not apply to cancers that come back later or spread, for example.
- Besides the cancer stage, many other factors can affect a person’s outlook, such as age and overall health, and how well the cancer responds to treatment.
Your doctor can tell you how these numbers may apply to you, as he or she is familiar with your situation.
Survival rates for adrenal cancer
These survival rates come from the National Cancer Database. The database does not list survival statistics by American Joint Committee on Cancer (AJCC) or ENSAT (European Network for the Study of Adrenal Tumors) stages. Instead, it divides patients into 3 groups:
- Localized means that the cancer hasn’t grown outside of the adrenal gland at diagnosis (like stages 1 and 2).
- Regional means that the cancer has grown into nearby tissues or has spread to nearby lymph nodes (like stage 3).
- Distant means that the cancer has spread further to distant sites (like stage 4).
The 5-year relative survival rates by stage for adrenal cancer are as follows:
Table 2. Survival rates for adrenal cancer
| Stage | 5-year Relative Survival |
| Localized | 65% |
| Regional | 44% |
| Distant | 7% |
Adrenal cancer treatment
The main treatments for adrenal cortical cancer are surgery, radiotherapy and chemotherapy.
Your treatment depends on:
- the size of the tumor
- whether it has spread
- your general health and fitness
Unfortunately, adrenal cancer can be quite a fast growing type of cancer. It is often diagnosed in the later stages when it is quite advanced. This means it can be difficult to cure.
Surgery for adrenal cancer
The main treatment for adrenal cancer is removal of the adrenal gland, an operation called an adrenalectomy. The surgeon will try to remove as much of the cancer as possible, including any areas of cancer spread. If nearby lymph nodes are enlarged, they also will need to be removed and checked for cancer spread.
One way to remove the adrenal gland is through an incision in the back, just below the ribs. This works well for small tumors, but it can be hard to see larger tumors well.
More often, the surgeon makes the incision through the front of the abdomen. This lets the surgeon see the tumor more clearly and makes it easier to see if it has spread. It also gives the surgeon room to remove a large cancer that has grown into tissues and organs near the adrenal gland. For example, if the cancer has grown into the kidney, all or part of the kidney must also be removed. If it has grown into the muscle and fat around the adrenal gland, these tissues will need to be removed as well.
Sometimes, the cancer can grow into the inferior vena cava, the large vein that carries blood from the lower body to the heart. If this is the case, it requires a very extensive operation to remove the tumor completely and preserve the vein. To remove the tumor from the vein, the surgeon may need to bypass the body’s circulation by putting the patient on a heart-lung bypass pump like that used in heart surgery. If the cancer has grown into the liver, the part of the liver containing the cancer might need to be removed, too.
It is also possible to remove some small adrenal tumors through a thin hollow, lighted tube (with a tiny video camera on the end) called a laparoscope. Instead of a large incision in the skin to remove the tumor, several small ones are made. The surgeon inserts the laparoscope through one of them. This lets him or her see inside the belly. Then, other instruments inserted through this tube or through other small incisions are used to remove the adrenal gland. The main advantage of this method is that because the incisions are smaller, patients recover from surgery more quickly.
Although laparoscopic surgery is used to treat adrenal adenomas (benign tumors), it often is not an option for treating larger adrenal cancers. This is because it’s important to remove the tumor in one piece whenever possible. To remove a large tumor with a laparoscope, the surgeon might have to break it up into small pieces first. Doing that raises the risk of the cancer spreading. Adrenal cancers that have grown into nearby tissues or lymph nodes can also be hard to remove completely using laparoscopy.
Hormones
Hormones produced by the cancer can make your blood pressure unstable so it can change suddenly during and immediately after the operation. To make sure it is as stable as possible, you might need to take blood pressure medicines from around 10 days before the operation. After surgery, your blood pressure should go back to normal.
Following an adrenalectomy, your other adrenal gland should carry on making all the hormones you need.
You will have to take hormone replacement tablets if you have both adrenal glands removed. You have these every day for the rest of your life.
Radiotherapy for adrenal cancer
Radiation therapy uses high-energy x-rays (or particles) to kill cancer cells. Radiation therapy is not used often as the main initial treatment for adrenal cancer because the cancer cells are not easy to kill with x-rays. Radiation may be used after surgery to help keep the tumor from coming back. This is called adjuvant therapy. Radiation can also be used to treat areas of cancer spread, such as in the bones or brain.
Types of radiation therapy
External beam radiation therapy
External beam radiation therapy focuses radiation on the cancer from a machine outside the body. Treatments are often given once or twice a day, 5 days a week for several weeks. Treatment is similar to getting an x-ray test, and is not painful. The actual treatment time lasts only a few minutes, although the setup time – getting you into place for treatment – usually takes longer so that the radiation is aimed accurately at the cancer. Before the treatment starts, the radiation team will take careful measurements to find the correct angles for aiming the radiation beams and the proper dose of radiation. This planning session, called simulation, usually includes getting imaging tests such as CT or MRI scans.
Brachytherapy (internal radiation therapy)
Brachytherapy (internal radiation therapy) uses small pellets of radioactive material placed next to or directly into the cancer, sometimes in thin plastic tubes. The tubes containing the pellets are left in place for a few days and then removed. The actual time is determined by the strength of the radioactive pellets and the size of the tumor. This type of radiation is not often used to treat adrenal cortical cancer.
Possible side effects
Common side effects of radiation therapy include:
- Nausea and vomiting
- Diarrhea (if an area of the abdomen is treated)
- Skin changes in the area being treated, which can range from redness to blistering and peeling
- Hair loss in the area being treated
- Fatigue
- Low blood counts
Chemotherapy for adrenal cancer
Chemotherapy (chemo) is the use of certain types of drugs to treat cancer. Typically, the drugs are given into a vein or by mouth (in pill form). These drugs enter the bloodstream and reach throughout the body, making this treatment useful for cancer that has spread (metastasized) to organs beyond the adrenal gland. Chemo does not work very well for adrenal cancer, so it is most often used for adrenal cancer that has become too widespread to be removed with surgery (although it is very unlikely to cure the cancer).
Mitotane
Mitotane is the drug most often used for people with adrenal cancer. It blocks hormone production by the adrenal gland and also destroys both adrenal cancer cells and healthy adrenal tissue. This drug can also suppress the usual adrenal steroid hormone production from your other, normal adrenal gland. This can lead to low levels of cortisol and other hormones, which can make you feel weak and sick. If this occurs, you’ll need to take steroid hormone pills to bring your hormone levels up to normal. Mitotane can also alter levels of other hormones, such as thyroid hormone or testosterone. If that occurs, you’d need drugs to replace these hormones as well.
Sometimes mitotane is given for a period of time after surgery has removed all the (visible) cancer. This is called adjuvant therapy and is meant to kill any cells that were left behind but were too small to see. Giving the drug this way may prevent or delay the cancer’s return. .
If the cancer has not been completely removed by surgery or has come back, mitotane will shrink the cancer in some patients. On average, the response lasts about a year, but it can be longer for some patients.
Mitotane is particularly helpful for people with adrenal cancers who have problems caused by excessive hormone production. Even when it doesn’t shrink the tumor, mitotane can reduce abnormal hormone production and relieve symptoms. Most patients with excess hormone production are helped by mitotane.
This drug can cause major side effects. The most common are nausea, vomiting, diarrhea, rashes, confusion, and sleepiness. Sometimes lower doses of the drug can still be effective and cause fewer side effects.
This drug is taken as a pill 3 to 4 times a day. Like other types of chemo, treatment with mitotane needs to be supervised closely by a doctor.
Other chemo drugs used for adrenal cancer
Drugs are sometimes combined with mitotane to treat advanced adrenal cancer. The drugs used most often are:
- The combination of cisplatin, doxorubicin (Adriamycin), and etoposide (VP-16) plus mitotane
- Streptozocin plus mitotane
Chemo drugs used less often, include:
- Paclitaxel (Taxol)
- 5-fluorouracil (5-FU)
- Vincristine (Oncovin)
These drugs may be given in different combinations and are often given with mitotane.
Chemo drug side effects
Chemotherapy drugs kill cancer cells but also damage some normal cells, which can cause some side effects. Side effects from chemo depend on the type of drugs, their doses, and how long treatment lasts. Common side effects of chemo include:
- Nausea and vomiting
- Loss of appetite
- Loss of hair
- Hand and foot rashes
- Mouth sores
- Diarrhea
- Increased risk of infection (due to a shortage of white blood cells)
- Problems with bleeding or bruising after minor cuts or injuries (due to a shortage of blood platelets)
- Anemia, fatigue, or shortness or breath (due to low red blood cell counts)
Along with the risks above, some chemo drugs can cause other side effects.
Ask your health care team what side effects you can expect based on the specific drugs you will get. Be sure to tell your doctor or nurse if you do have side effects, as there are often ways to help with them. For example, drugs can be given to help prevent or reduce nausea and vomiting.
Other drugs used to treat adrenal cancer
Drugs other than mitotane may be used to block hormones made by the cancer or to lower the effects of the hormones. Treatment with some of these drugs may need to be supervised by an endocrinologist (hormone doctor) because they affect several hormone systems and might make it necessary to replace other hormones.
Ketoconazole and metyrapone can reduce adrenal steroid hormone production. This can help relieve symptoms caused by these hormones, but it doesn’t shrink the cancer.
Some drugs block the effects of the hormones made by the tumor. These include:
- Spironolactone (Aldactone), which decreases effects of aldosterone
- Mifepristone (Korlym), which decreases cortisol effects
- Tamoxifen, toremifene (Fareston), and fulvestrant (Faslodex), can block the effects of estrogen. These drugs are more often used to treat breast cancer, but can be useful in some patients (often men) who have adrenal tumors that make estrogen.
Coping and support
- Learn enough about adrenal cancer to feel comfortable making treatment decisions. Ask your doctor to write down as much information about your specific disease as possible. Then narrow your search for information accordingly.
- Write down questions for your doctor before each appointment, and look for information in your local library and on the internet. Good sources include the National Cancer Institute (https://www.cancer.gov), the American Cancer Society (https://www.cancer.org/).
- Lean on your whole health care team. At major medical centers and pediatric cancer centers, your health care team may include psychologists, psychiatrists, recreation therapists, child-life workers, teachers, dietitians, chaplains and social workers. These professionals can help with a whole host of issues, including explaining procedures to children, finding financial assistance and arranging for housing during treatment. Don’t hesitate to rely on their expertise.
- Explore programs for children with cancer. Major medical centers and nonprofit groups offer numerous activities and services specifically for children with cancer and their families. Examples include summer camps, support groups for siblings and wish-granting programs. Ask your health care team about programs in your area.
- Help family and friends understand your situation. Set up a free, personalized webpage at the nonprofit website CaringBridge (https://www.caringbridge.org/). This allows you to tell the whole family about appointments, treatments, setbacks and reasons to celebrate — without the stress of calling everyone every time there’s something new to report.
- Adrenocortical carcinoma (ACC): diagnosis, prognosis, and treatment. Front Cell Dev Biol. 2015;3:45. Published 2015 Jul 3. doi:10.3389/fcell.2015.00045 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4490795/
- Extent of disease at presentation and outcome for adrenocortical carcinoma: have we made progress? Kebebew E, Reiff E, Duh QY, Clark OH, McMillan A. World J Surg. 2006 May; 30(5):872-8.
- Adrenal Cancer Stages. https://www.cancer.org/cancer/adrenal-cancer/detection-diagnosis-staging/staging.html
- Fassnacht M., Johanssen S., Quinkler M., Bucsky P., Willenberg H. S., Beuschlein F., et al. (2009). Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma: proposal for a Revised TNM Classification. Cancer 115, 243–250. 10.1002/cncr.24030
- Icard P., Goudet P., Charpenay C., Andreassian B., Carnaille B., Chapuis Y., et al. . (2001). Adrenocortical carcinomas: surgical trends and results of a 253-patient series from the French Association of Endocrine Surgeons study group. World J. Surg. 25, 891–897. 10.1007/s00268-001-0047-y
- Lughezzani G., Sun M., Perrotte P., Jeldres C., Alasker A., Isbarn H., et al. . (2010). The European Network for the Study of Adrenal Tumors staging system is prognostically superior to the international union against cancer-staging system: a North American validation. Eur. J. Cancer 46, 713–719. 10.1016/j.ejca.2009.12.007
- Kerkhofs T. M., Verhoeven R. H., Van der Zwan J. M., Dieleman J., Kerstens M. N., Links T. P., et al. . (2013). Adrenocortical carcinoma: a population-based study on incidence and survival in the Netherlands since 1993. Eur. J. Cancer 49, 2579–2586. 10.1016/j.ejca.2013.02.034
- Bilimoria K. Y., Shen W. T., Elaraj D., Bentrem D. J., Winchester D. J., Kebebew E., et al. . (2008). Adrenocortical carcinoma in the United States: treatment utilization and prognostic factors. Cancer 113, 3130–3136. 10.1002/cncr.23886
- Beuschlein F., Weigel J., Saeger W., Kroiss M., Wild V., Daffara F., et al. . (2015). Major prognostic role of ki67 in localized adrenocortical carcinoma after complete resection. J. Clin. Endocrinol. Metab. 100, 841–849. 10.1210/jc.2014-3182
- Libé R., Borget I., Ronchi C. L., Zaggia B., Kroiss M., Kerkhofs T., et al. (2014). Prognostic factors in Stage III-IV adrenocortical carcinomas (ACC): an European Network for the Study of Adrenal Tumor (ENSAT) study. ASCO Annu. Meet. J. Clin. Oncol. 35:55.
- Assie G., Antoni G., Tissier F., Caillou B., Abiven G., Gicquel C., et al. . (2007). Prognostic parameters of metastatic adrenocortical carcinoma. J. Clin. Endocrinol. Metab. 92, 148–154. 10.1210/jc.2006-0706
- Assié G., Letouzé E., Fassnacht M., Jouinot A., Luscap W., Barreau O., et al. . (2014a). Integrated genomic characterization of adrenocortical carcinoma. Nat. Genet. 46, 607–612. 10.1038/ng.2953
- Survival Rates for Adrenal Cancer. https://www.cancer.org/cancer/adrenal-cancer/detection-diagnosis-staging/survival-by-stage.html





{kind=link}