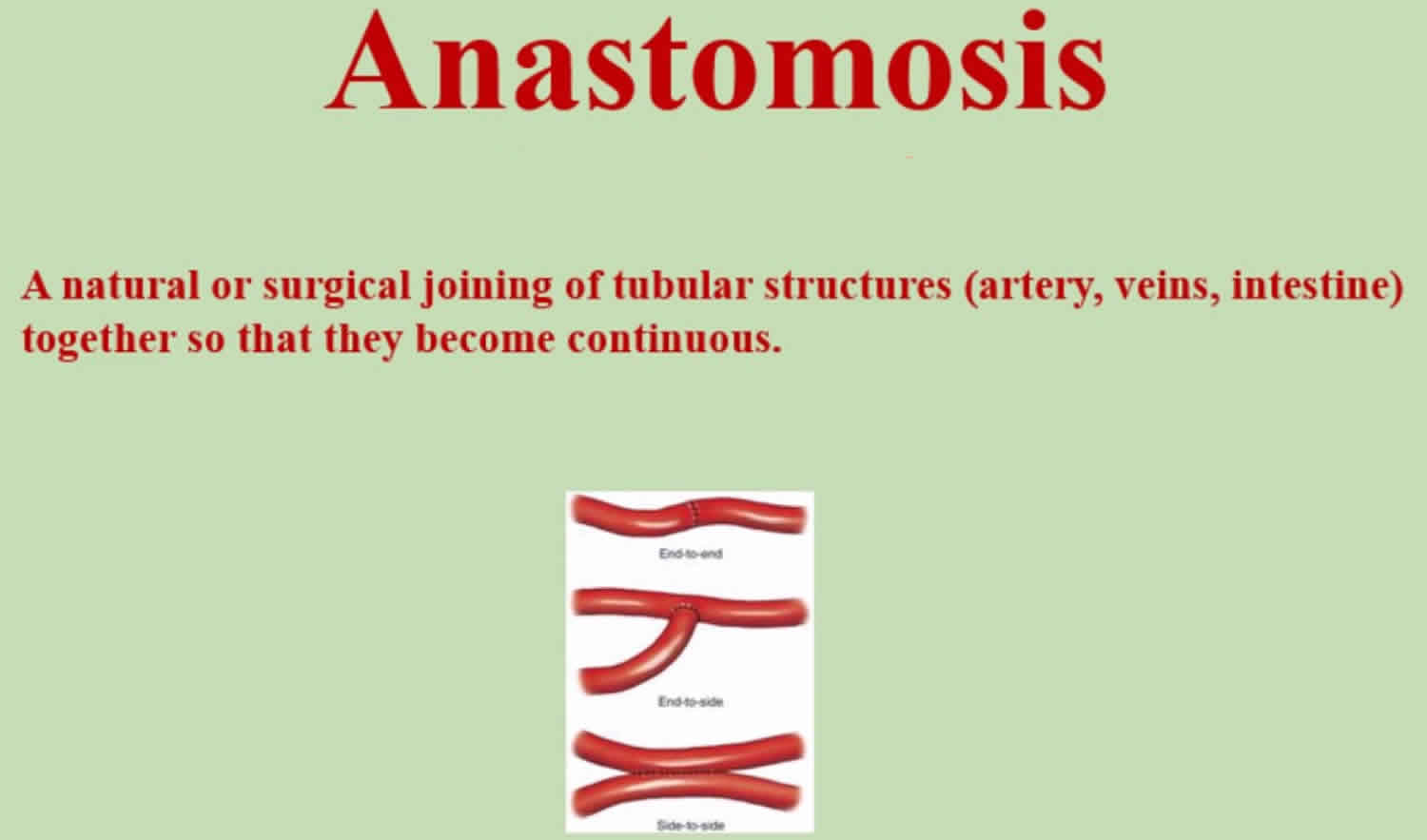
What is anastomosis
An anastomosis is a surgical connection between two structures or the surgical establishment of a communication, shunt, fistula, between two conduits or cavities which normally are separate, in order to short-circuit the intervening portion or to effect a repair after its removal. Anastomosis usually means a connection that is created between tubular structures, such as blood vessels or loops of intestine.
For example, when part of an intestine is surgically removed, the two remaining ends are sewn or stapled together (anastomosed). The procedure is known as an intestinal anastomosis.
Examples of surgical anastomoses are:
- Arteriovenous fistula (an opening created between an artery and vein) for dialysis
- Colostomy (an opening created between the bowel and the skin of the abdominal wall)
- Intestinal anastomosis, in which two ends of intestine are sewn together
- A connection between a graft and a blood vessel to create a bypass
Severe complications can occur if an anastomosis is poorly performed, including insufficiency or stenosis 1. In the case of an intestinal anastomosis, this will most likely require a re-operation for peritonitis due to drainage of intraluminal contents into the peritoneal cavity or for symptoms of obstruction. Similarly, poorly-performed vascular anastomoses will require additional suturing if bleeding occurs after the release of the clamps; otherwise, in a postoperative vascular stenosis of the anastomosis with a higher risk for early vascular occlusion on the anastomotic side can result.
Vascular anastomosis
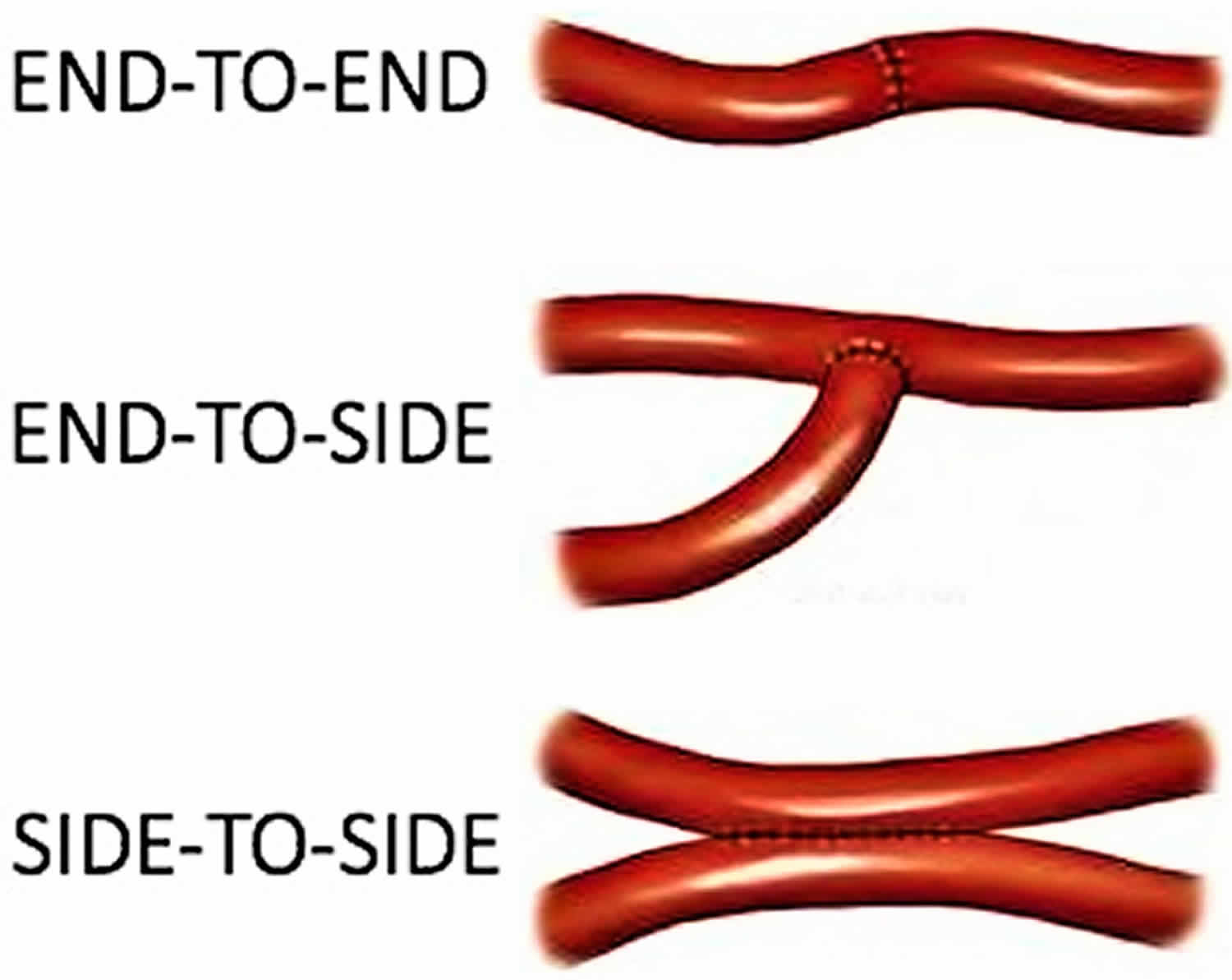
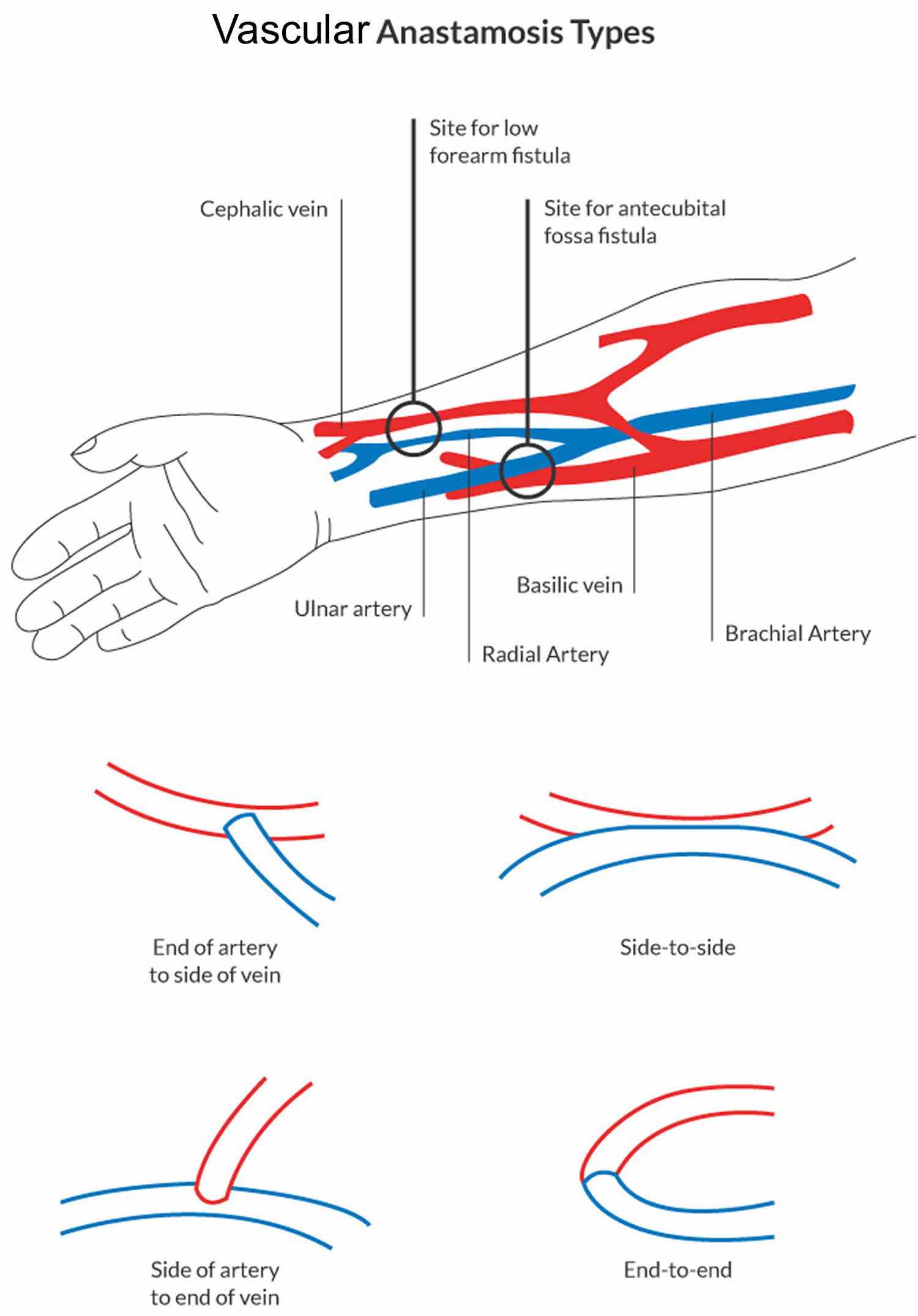
Vascular anastomosis is joining of two blood-carrying vessels. Some of the commonly practiced anastomoses are artery to artery, artery to vein, and artery to synthetic tube graft 2. Also, the two most common forms of an anastomosis are end to end; and end to side. In most cases vascular anastomoses are normally sutured conventionally. In the pathologic arteries and limited access surgery or through minimal surgical approaches, the hand suture sometimes is difficult. This procedure depends on surgeon dexterity and requires time and great technical effort 3. Therefore other efforts to sutureless vascular anastomosis of side-to-side, end-to-side, or end-to-end type, have been also tried with special devices, tools and equipment 4.
Figure 1. Vascular anastomosis types
Types of vascular anastomosis
- Arterial-Arterial anastomosis
- End to end anastomosis
- End to side anastomosis
- Side to side anastomosis
- Interposition prosthetic graft
- Arterial- Venous anastomosis
- End vein to side artery
- End vein to end artery
- Venous- Venous anastomosis
Techniques of vascular anastomosis
- Interrupted sutures technique
- Continuous single suture techniques
- Open
- Closed
- Continuous double suture technique
Types of grafts used in vascular anastomosis
- Arterial conduits
- Left Internal Mammary Artery (LIMA) & Right Internal Mammary Artery (RIMA)
- Radial artery
- Gastro-epiploec artery
- Vein conduits
- Great saphenous vein
- Umbilical vein
- Prosthetic grafts
- PTFE (Gore Tex)
- Dacron (woven, netted, +/- velour)
Factors affecting graft patency
The most significant factor in patency of vascular anastomosis is flawless surgical technique – Small pieces of adventia caught in the anastomosis can cause platelet thrombus formation – large bites may decrease the diameter of the lumen& invites thrombus formation.
Arteriovenous anastomosis
The first step is to select a suitable “healthy” artery and vein. This can be done by clinical and ultrasonographic investigation. Most procedures creating a primary vascular access can be carried out under local anaesthesia.
There are three basic types of arteriovenous anastomosis:
- Side-to-side
- End-to-end
- End-to-side
Side-to-side anastomosis
Side-to-side anastomosis lets blood flow in both directions.
With vessels in good condition and functioning venous valves, it is less likely to develop complications; however, it has proved to have more disadvantages and complications than other techniques.
End-to-end anastomosis
End-to-end anastomosis also lets blood flow in both directions. It was fashionable in the past but has several disadvantages: (1) the diameters of the artery and the vein differ, and this has to be overcome by inserting a rhombus-like vein patch into the suture; (2) the suture itself is performed in three independent sections without any connection between the closing knots.
This procedure is dangerous in diabetic and elderly patients who constitute the majority of patients currently seen.
End-to-side anastomosis
End-to-side anastomosis is the preferred technique today. With this technique the vein is isolated and has to be approximated to the artery across a certain distance. The angle between artery and vein at the site of the anastomosis differs from case to case. Each angle requires an individual length of arteriotomy and venotomy and requires close attention. The correct angle allows for preserved patency rates and reduces future complications.
Bowel anastomosis
Bowel anastomoses are common procedures in both elective and emergency general surgery. The anastomotic technique selected depends upon site of anastomosis, bowel calibre and quality and underlying disease process. One important factor in the decision to perform a particular anastomosis, however, remains individual surgical experience and personal preference.
The theory behind creating a safe, healthy bowel anastomosis remains constant, irrespective of the technique chosen. Unfortunately, however, despite the “perfect patient”, healthy bowel and meticulous technique some anastomoses continue to leak resulting in significant morbidity and mortality (e.g., 22% mortality in patients with a leak vs 7.2% mortality in those without 5. Approximately 4% of all anastomoses performed after resection of a colonic tumour (and a higher percentage of colorectal anastomoses) leak – reducing this rate would improve mortality 6.
The choice of anastomotic technique may be influenced by the diameter of the bowel ends, edema, accessibility and site of anastomosis, contamination, available time and equipment and underlying pathology.
Anastomoses can be described as follows:
- Sutured
- interrupted or continuous;
- single or 2-layer;
- end-to-end or side-to-side (or any combination);
- various suture materials;
- extramucosal or full-thickness sutures and
- size of and spacing between each suture;
- Stapled:
- side-to-side or end-to-end (or any combination);
- staple lines oversewn, buried or not and
- various stapling devices.
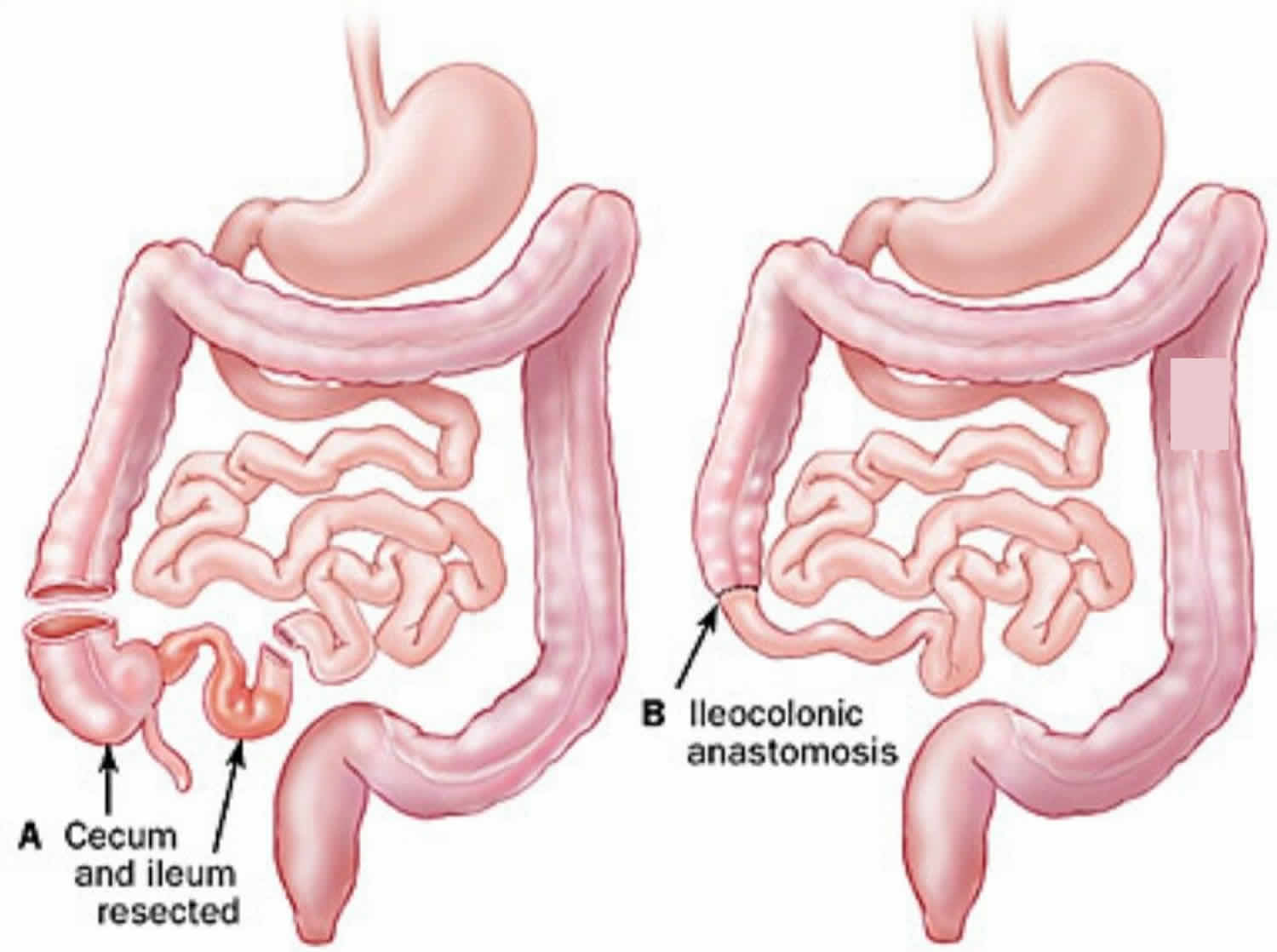
Ileocolic anastomosis
An ileocolic anastomosis is also called ileocolonic anastomosis, is the joining together of the end of the ileum, or small intestine, to the first part of the large intestine, called the colon. An ileocolic anastomosis is usually performed after the removal of the terminal ileum (the last part of the small intestine) and first part of the colon (bowel) in people with Crohn’s disease 7. This is because Crohn’s disease often affects the small intestine and first part of the large intestine.
An ileocolic anastomosis is usually done to rejoin the intestines after a bowel resection. A bowel resection is the removal of a damaged portion of the intestine.
People with the following conditions may need a bowel resection:
- Colorectal cancer
- Crohn’s disease
- Ulcerative colitis
- Diverticulitis
- Regional enteritis
- Intestinal abscess
- Meckel’s diverticulum, an abnormal sac of intestine present at birth
- Severe intestinal ulcers
- Blockage in the intestines
- Precancerous polyps
- Trauma, such as a gunshot wound
How is ileocolic anastomosis surgery done?
In most cases, anastomosis can be performed using laparoscopy. Laparoscopy means that the surgery is done through a small incision using a small instrument called a laparoscope. A laparoscope is a long, thin tube with a camera and light at the end of it. It helps doctors see inside your body while they perform surgery.
There are several techniques used by surgeons to perform an ileocolic anastomosis:
- End-to-end anastomosis. This technique connects the two open ends of the intestines together.
- Side-to-side anastomosis. This technique connects the sides of each part of the bowel together rather than the two ends. The ends are stapled or sewn closed. Side-to-side anastomoses are at less risk of having narrowing complications in the future.
- End-to-side anastomosis. This technique connects the end of the intestine that’s smaller with the side of the larger one.
The technique that a surgeon chooses may depend on the difference in diameter of each portion of the intestine that needs to be joined together. An end-to-side anastomosis is commonly used in a right hemicolectomy 8. This anastomosis proceeds in a manner very similar to that of the end-to-end anastomosis 9.
Staples vs. sutures
Surgeons can choose to join together the two parts of the intestine using either sewing (sutures) or staples. Sewing by hand has been used successfully for over 100 years. However, staples take less time to perform. Newer surgeons find it easier to learn as well.
An end-to-end anastomosis can only be done with sutures. An side-to-side anastomosis is usually done with staples.
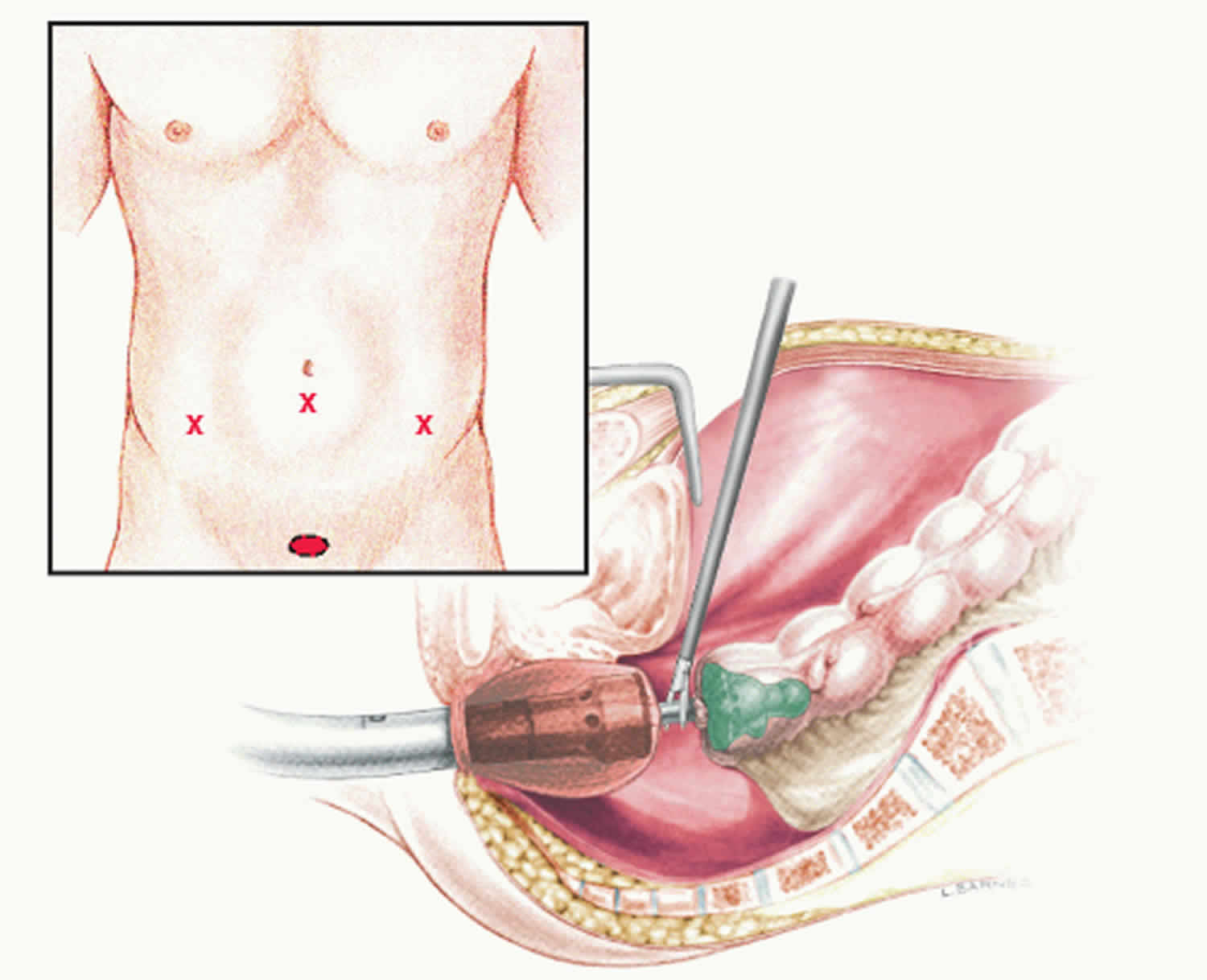
Figure 2. Ileocolic anastomosis
Risks of ileocolic anastomosis
There are risks associated with any abdominal operation. Pre-operative assessment of heart and lung conditions are made, as well as any coexisting medical conditions. During the hospital admission patients wear stockings and are given a regular tiny injections to prevent thrombosis (blood clots).
Bleeding if very rare in ileocolic anastomosis surgery, blood is always available if a transfusion is required.
Wound infections can occur in any form of intestinal surgery, open or laparoscopic. Wound infections rarely cause serious problems but may require treatment with antibiotics.
Occasionally the join that the surgeon makes in the bowel can leak. This is known as an anastomotic leak. The risk of leakage is greater in patients who have Crohn’s disease and in patients who are on steroids. If a leak occurs sometimes this can be managed with antibiotics and/ or a drain placed through the abdominal wall, usually in the x-ray department. If the leak is larger and peritonitis develops another operation will be necessary and the surgeon will need to create a stoma (ileostomy).
Sometimes the bowel may take longer than normal to start working, this is known as ileus. Patients may develop abdominal distension and vomiting. If this happens the surgeon will normally recommend a period of bowel rest with continued intravenous fluids and sometimes a tube passed via the nose to the stomach (nasogastric tube).
When the bowel doesn’t start working properly, there may be a kink, twist or an adhesion causing a blockage. This is known as obstruction. Patients may develop colicky abdominal pains, abdominal distension and vomiting. If this happens the surgeon will normally recommend a period of bowel rest with continued intravenous fluids and sometimes a tube passed via the nose to the stomach (nasogastric tube). In most cases the obstruction settles spontaneously occasionally an operation is required to relieve the blockage.
Sometimes during the operation the surgeon discovers that it is not possible to carry out the procedure using a wholly keyhole approach. In this situation a cut is made and the operation is done as an open procedure. This is known as conversion.
Recovery after ileocolic anastomosis surgery
After the operation patients will have an intravenous drip, which is normally in place for 24 hours, or until, a normal fluid intake is resumed. A catheter (tube inserted to drain the bladder) is normally kept in place for 24 hours.
Occasionally an abdominal drain is used (small tube passing through the abdominal wall). This is normally removed after a few days.
An epidural is often used in keyhole and open surgery to provide pain relief after the operation and is usually continued at least until the next day. The anaesthetist will be able to discuss this with you before the operation.
Patients are allowed to eat and drink as soon as they feel able after the operation (usually the same day). Patients are encouraged to mobilize as soon as possible after the operation.
Hospital stay is usually 2-5 days for keyhole surgery and 5-7 days for open surgery although this may vary.
Following discharge from hospital, patients are encouraged to keep mobile. They should avoid heavy lifting or increased physical activities for about 6 weeks.
Patients can normally resume driving after about 2 weeks but this may vary particularly if the operation is done as an open procedure.
A follow up consultation is usually arranged after about two weeks. Patients can always be seen sooner if there are problems.
Colorectal anastomosis
A colorectal anastomosis is a surgery to join a section of the large intestine to the rectum. Colorectal anastomosis is done after the removal of the injured or diseased parts of the colon.
Colorectal anastomosis surgery is performed to treat a variety of conditions, including the following:
- Colorectal cancer
- Diverticular disease – small pouches form in the wall of the colon
- Inflammatory intestinal diseases colitis,Crohn’s disease
- Large bowel obstruction
- Trauma to the intestine
- Precancerous polyps, especially those seen in familial polyposis
- A hole in the bowel wall or dead piece of bowel
- Bleeding from the colon
For colon cancer, the goal is to remove all of the cancer. If you have a precancerous condition, then you may have prevented the development of cancer. If you had surgery due to other conditions, a successful operation will alleviate or improve your symptoms.
During a colorectal anastomosis surgery, the diseased part of the bowel is removed and the two healthy sections of the colon are reattached. If a colorectal anastomosis is not possible because of the extent of the disease or its location, the surgeon creates a colostomy. A temporary colostomy is made when the colon needs longer to heal after surgery and the colorectal anastomosis is performed later.
Figure 3. Colorectal anastomosis
How is colorectal anastomosis done?
Colorectal anastomosis is performed under general anesthesia.
There are two types of colorectal anastomosis: open surgery and laparoscopic surgery. The type of procedure performed depends on the diagnosis and the individual patient.
- Open colorectal anastomosis – where the surgeon makes a large midline incision in your abdomen in order to remove a section or the whole of the large intestine.
- Laparoscopic or ‘keyhole’ colorectal anastomosis – where the surgeon makes a number of smaller cuts in your abdomen, before using a special telescope and small surgical instruments to remove a section or the whole of the large intestine. A slightly larger incision is usually made to remove the diseased section of colon from the body.
Risks of colorectal anastomosis
Like any surgical procedure, a colorectal anastomosis carries risks of complications. These complications may include complication from anesthesia, pneumonia, urinary tract infection and heart attack.
Some possible surgical complications of colorectal anastomosis include:
- Damage to other organs or structures
- Bleeding
- Infection
- Leakage from the anastomosis
- Intra-abdominal abscess (a pus-filled swelling),
- Infection of the membrane that lines the abdominal cavity (peritonitis),
- Hernia forming at the incision site
- Anastomosis stenosis
- Intestinal obstruction due to development of scar tissue
Some complications will require further surgery. Colonic anastomotic leaks occur in the early or late postoperative phase, in which the bowel anastomosis fails. This may be a small leak that can be managed conservatively or less commonly complete dehiscence requiring repeat surgery. In one large surgical series, the incidence anastomotic leak after colorectal resection was 8.7% 10. Colorectal anastomotic leakage after colorectal resection is a dreaded complication and is reported to have a significant mortality (6%-22%) 11. Morbidity is dramatically increased opposed to patients without colorectal anastomotic leakage and leads to reoperations, radiological interventions and permanent stoma in 56% 12. Colorectal anastomotic leakage is the leading cause of postoperative death after colorectal surgery, increases the risk of a permanent stoma significantly. Many aspects of colorectal anastomotic leakage like the cause remains unclear 10.
Recovery after colorectal anastomosis surgery
After colorectal anastomosis surgery, the patient is taken to the recovery room and is closely monitored by the nursing staff until the anesthesia wears off. When vital signs are stable and the patient is awake and coherent, he or she is transferred to the surgical ward or sometimes to the intensive care unit (ICU) when needed.
On the day after surgery, most patients can get out of bed and move around. It is important to get up as soon as possible, because physical activity stimulates bowel function and helps blood circulation return to normal.
Until you are able to eat and drink normally, you will be fed intravenously (through a tube inserted directly into a vein). Most people are able to resume a light diet between 4-5 days after having a colorectal anastomosis surgery.
You will need to take painkillers for a few days. You should tell your treatment team if the painkillers that you are taking aren’t working because alternative painkillers are available. Antibiotics may also be given postoperatively. This depends on a number of factors, including the original diagnosis.
Following a colorectal anastomosis surgery, you will probably be able to return home within 1-2 weeks after having the operation.
Normal activity for all patients generally resumes within 1 to 3 weeks, but it takes much longer for the body to heal completely. So, patients must avoid strenuous exertion and heavy lifting for 4 to 6 weeks.
References- Khalil PN, Kleespies A, Rentsch M, Thasler WE, Jauch KW, Bruns CJ. Description and evaluation of a bench porcine model for teaching surgical residents vascular anastomosis skills. BMC Res Notes. 2010;3:189. Published 2010 Jul 13. doi:10.1186/1756-0500-3-189 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912942/
- Vokrri L, Krasniqi X, Qavdarbasha A, et al. The vascular connector, design of a new device for sutureless vascular anastomosis. Ann Surg Innov Res. 2014;8(1):8. Published 2014 Nov 22. doi:10.1186/s13022-014-0008-4 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4260208/
- A new mechanical connector for distal coronary artery anastomoses in coronary artery bypass grafting: a randomized, controlled study. Wiklund L, Bonilla LF, Berglin E. J Thorac Cardiovasc Surg. 2005 Jan; 129(1):146-50.
- Early clinical experience with a new sutureless anastomotic device for proximal anastomosis of the saphenous vein to the aorta. Calafiore AM, Bar-El Y, Vitolla G, Di Giammarco G, Teodori G, Iacò AL, D’Alessandro S, Di Mauro M. J Thorac Cardiovasc Surg. 2001 May; 121(5):854-8.
- Fielding LP, Stewart-Brown S, Blesovsky L, Kearney G. Anastomotic integrity after operations for large-bowel cancer: a multicentre study. Br Med J. 1980;281:411-414
- Phillips RKS, Steele RJC. A Companion to Specialist Surgical Practice: Colorectal Surgery. 4th ed. Philadelphia: Elsevier Saunders; 2009;58-59.
- http://www.birminghambowelclinic.co.uk/treatments-ileocolic-resection/
- Ileocolonic anastomosis after right hemicolectomy for colon cancer: functional end-to-end or end-to-side? World Journal of Surgical Oncology201412:306 https://wjso.biomedcentral.com/articles/10.1186/1477-7819-12-306
- Goulder F: Bowel anastomoses: the theory, the practice and the evidence base. World J Gastrointest Surg. 2012, 4 (9): 208-213. 10.4240/wjgs.v4.i9.208.
- Daams F, Luyer M, Lange JF. Colorectal anastomotic leakage: aspects of prevention, detection and treatment. World J Gastroenterol. 2013;19(15):2293-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3631979/
- Rullier E, Laurent C, Garrelon JL, Michel P, Saric J, Parneix M. Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg. 1998;85:355–358.
- Lindgren R, Hallböök O, Rutegård J, Sjödahl R, Matthiessen P. What is the risk for a permanent stoma after low anterior resection of the rectum for cancer? A six-year follow-up of a multicenter trial. Dis Colon Rectum. 2011;54:41–47.





{kind=link}