What is angle closure glaucoma
Angle closure glaucoma also called closed-angle glaucoma, results from appositional or synechial closure of the anterior chamber angle leading to reduction in aqueous outflow facility, intraocular pressure (IOP) elevation, and subsequent damage to the optic nerve with associated visual field loss. Angle closure glaucoma is a major cause of blindness worldwide, with a particularly high prevalence in some Inuit and Asian populations. Angle closure glaucoma has a familial tendency and is associated with increasing age and hyperopia.
There are primary and secondary forms of angle closure glaucoma. In primary angle closure glaucoma, the mechanism causing disease is primarily pupillary block (iridotrabecular contact is present in three or more quadrants of the drainage angle), being either functional or absolute, in the presence of documented optic nerve damage and visual field loss. Doctors don’t clearly understand why primary angle closure glaucoma happens. While in secondary angle closure glaucoma there are other underlying identifiable pathologic causes, such as neovascularization or uveitis, that either push the iris forward from behind or pull the iris forward to contact trabecular meshwork. If angle closure results in elevated intraocular pressure (IOP) that causes glaucomatous optic disc damage, it is referred to as secondary angle closure glaucoma.
Both primary and secondary angle closure glaucoma can result in dramatic acute angle closure attacks and chronic asymptomatic angle closure disease leading to glaucoma.
Acute angle closure glaucoma is an urgent but uncommon dramatic symptomatic event with blurring of vision, painful red eye, headache, nausea, and vomiting. Diagnosis is made by noting high intraocular pressure (IOP), corneal edema, shallow anterior chamber, and a closed angle on gonioscopy. Medical or surgical therapy is directed at widening the angle and preventing further angle closure. If glaucoma has developed, it is treated with therapies to lower intraocular pressure.
Chronic angle-closure glaucoma is diagnosed by noting peripheral anterior synechiae on gonioscopy, as well as progressive damage to the optic nerve and characteristic visual field loss. Chronic angle-closure glaucoma is treated with therapies to lower intraocular pressure.
A thorough history and eye examination are essential in differentiating between primary and secondary angle closure glaucoma. This distinction is crucial as the treatment of each form can vary greatly. The mainstays of therapy are medications that lower intraocular pressure and laser peripheral iridotomy for any component of pupillary block. Although angle closure glaucoma in all its forms is vision threatening, early diagnosis and appropriate management can stabilize the angle closure glaucoma and minimize vision loss.
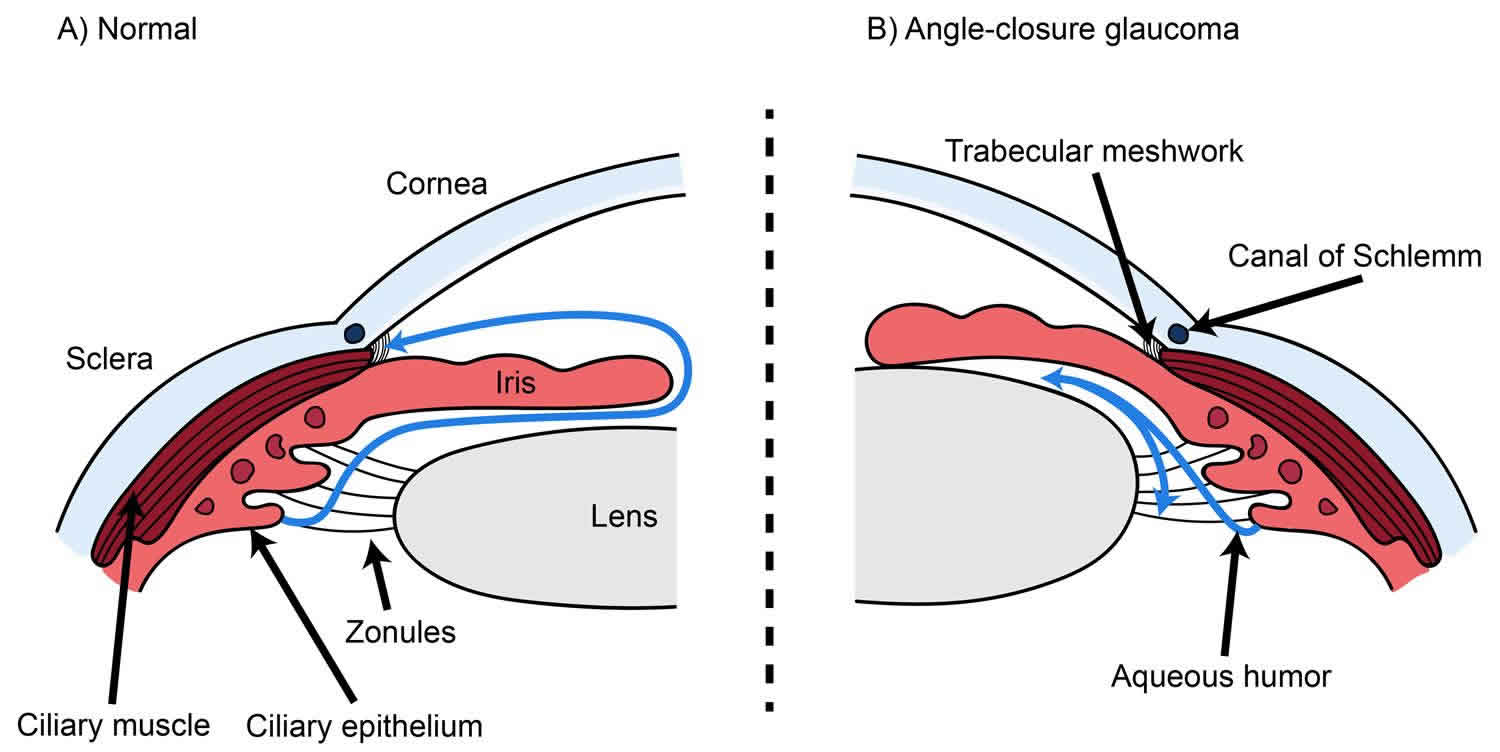
Figure 1. Angle closure glaucoma (blocked aqueous outflow increases intraocular pressure causing glaucoma)
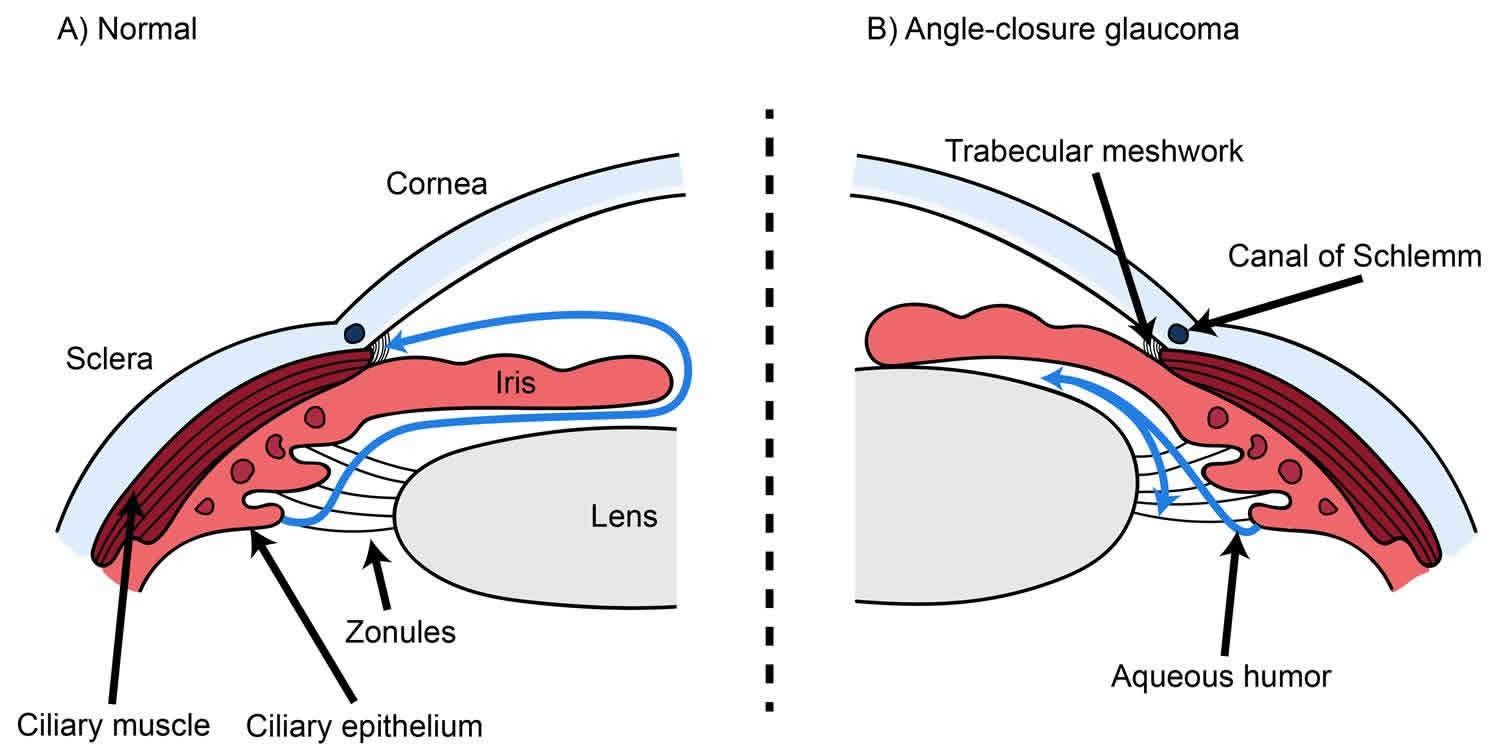
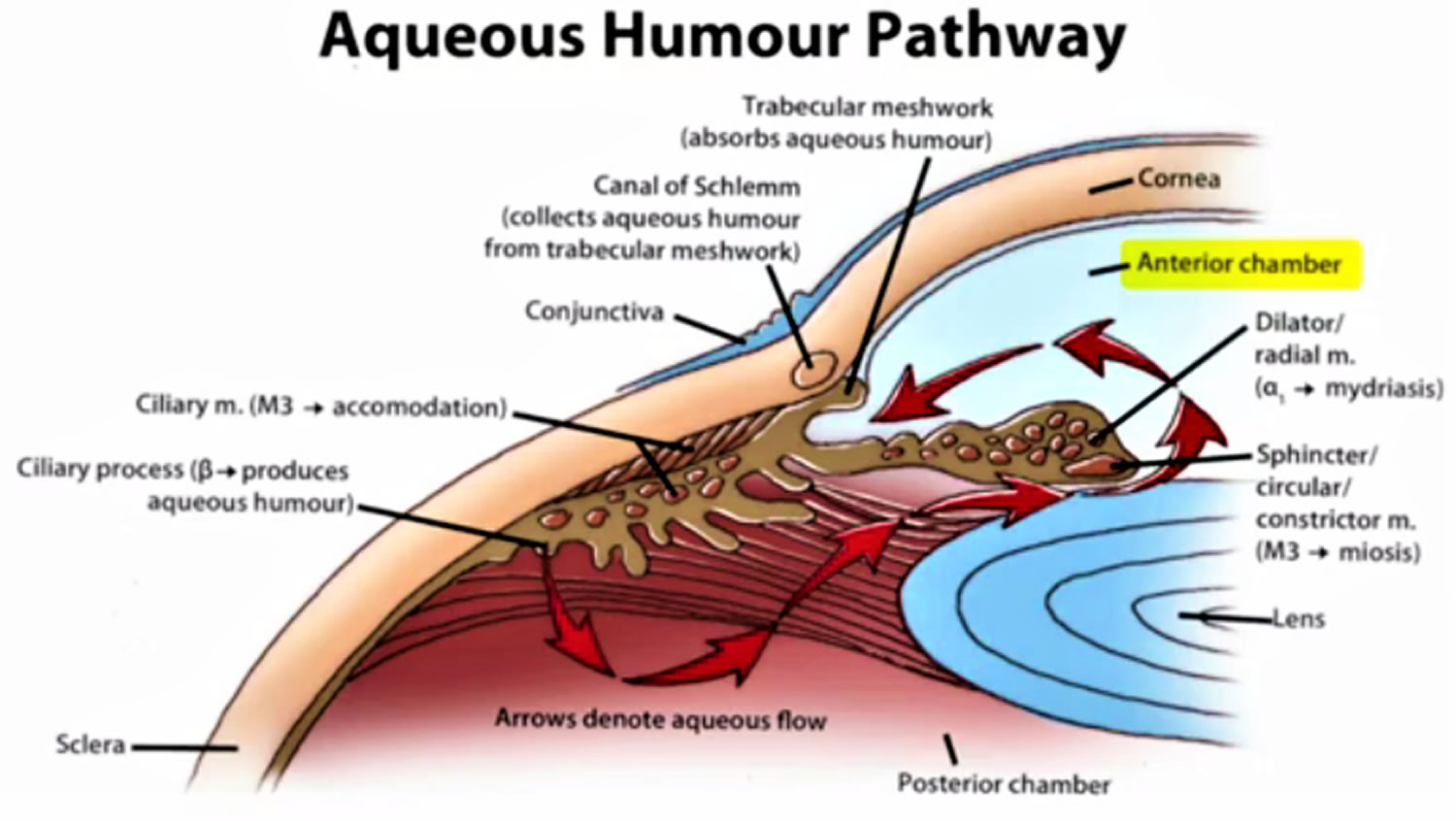
Figure 2. Normal aqueous outflow
Angle closure glaucoma causes
Primary angle closure glaucoma
Primary angle closure glaucoma is caused by relative pupillary block in the majority of cases. In pupillary block, aqueous humor encounters increased resistance as it flows from the posterior to anterior chamber through the iris-lens channel. Some degree of relative pupillary block is present in most phakic eyes. The risk of pupillary block is highest with a mid-dilated pupil where there appears to be maximum contact between the iris and the lens. In eyes with angle closure, other factors exacerbate the block, such as the front lens surface being anterior to the plane of iris insertion into the ciliary body base. The increased pressure gradient across the pupil causes the peripheral iris to bow forward and cover some or all of the filtering portion of the trabecular meshwork, resulting in appositional angle closure. Peripheral anterior synechiae form after prolonged or repeated contacts of the peripheral iris with trabecular meshwork. Another mechanism thought to be important in primary angle closure is iris angle crowding, which is caused by a thickened peripheral iris filling the space between the trabecular meshwork and angle recess under dark conditions 1.
Eyes that experience angle closure glaucoma are anatomically different than normal eyes — they have shorter axial lengths, shallower anterior chambers, thicker and relatively anteriorly positioned lenses, and flatter corneas 2 and they are also physiologically different. Thicker irides may increase the posterior to anterior pressure differential 3. Dynamic factors in angle closure eyes that can contribute to increased pupillary block are the tendency to retain more iris volume after dilation and choroidal expansion causing forward lens movement 4. As imaging modalities, such as ultrasound biomicroscopy and anterior segment optical coherence tomography improve, these dynamic factors will be better studied and understood.
A less common cause of primary angle closure glaucoma is anterior non-pupillary block. This is observed in eyes in which angle closure progresses despite a patent iridotomy, for example, as seen in plateau iris. Plateau iris configuration is characterized by a normal central anterior chamber depth, flat iris profile, and crowding of the angle by the iris base. There is a forward displacement of the iris base by anteriorly located ciliary processes that can lead to subsequent angle closure. Plateau iris syndrome occurs when an eye with plateau iris configuration develops a closed angle 5. Prominent last iris roll is another mechanism of anterior nonpupillary block in which a very thick iris with prominent peripheral circumferential folds becomes more pronounced and contacts trabecular meshwork with dilation 6.
Secondary angle closure glaucoma
Secondary angle closure glaucoma is caused by a myriad of other eye diseases. There are several secondary causes of angle closure that involve relative and absolute pupillary block. In phacomorphic glaucoma, the mass effect of a thickened or intumescent cataract pushes the iris forward and causes pathological angle narrowing. Forward displacement of the lens in ectopia lentis or microspherophakia can also push the iris forward and shallow the angle. Absolute pupillary block occurs when there is no movement of aqueous through the pupil because of 360 degrees posterior synechiae between the iris and a crystalline lens, an intraocular lens, capsular remnants, or the vitreous face. In secondary angle closure glaucoma without pupillary block, angle closure is due to either a.) contraction of an inflammatory, hemorrhagic, or vascular membrane in the angle leading to peripheral anterior synechiae
, or b.) forward displacement of the lens-iris diaphragm, often associated with ciliary body swelling and anterior rotation.
Mechanisms that push the iris forward from behind:
- Relative pupillary block (primary angle closure)
- Plateau iris configuration (primary angle closure)
- Absolute pupillary block – 360o posterior synechiae secluding pupil
- Aqueous misdirection or malignant glaucoma
- Ciliary body swelling, inflammation or cysts
- Choroidal swelling, effusions, or detachments
- Posterior segment tumors or space-occupying substances (silicone oil or gas bubble)
- Contracting retrolental tissue as seen in retinopathy of prematurity
- Anteriorly displaced lens
- Encircling retinal bands/buckles
Mechanisms that pull the iris forward into contact with the trabecular meshwork:
- Contraction of inflammatory membrane or fibrovascular tissue
- Iridocorneal endothelial (ICE) syndrome with migration of corneal endothelium
- Fibrous ingrowth
- Epithelial downgrowth
- Iris incarceration in traumatic or surgical wound
Angle closure glaucoma risk factors
A large number of angle closure glaucoma risk factors have been identified:
- Hyperopia (farsightedness or hypermetropia) 7
- Family history of angle closure 8
- Advancing age 9
- Female gender 10
- Asian or Inuit descent 11
- Shallow anterior chamber depth 12
- Shorter axial length 13
- Thicker lens 14
Risk factors for secondary angle closure glaucoma are related to the underlying diseases that cause it.
Angle closure glaucoma prevention
Screening
Given the high prevalence and morbidity of angle closure glaucoma in many countries, there is a need for quick, inexpensive screening methods that do not require highly skilled operators.
Oblique flashlight test uses a penlight that is held next to the temporal side of an eye with the beam of light parallel to the iris and shining across the anterior chamber. If there is a shadow projected onto the nasal iris, the angle is narrow because the iris is bowed forward and blocking the path of light. If there is no shadow, the anterior chamber angle is considered open. Because of variability in flashlight illumination and subjectivity in assessment of the test result, however, this test has a relatively low specificity 15.
The Van Herick method uses a narrow slit beam at 60 degrees onto the cornea just anterior to the limbus to evaluate the anterior chamber depth. If the distance from the anterior iris surface to the posterior corneal surface is less than one-fourth the corneal thickness, the angle may be narrow and should undergo gonioscopy. Modification of this method by creating additional grades, called the limbal chamber depth test, outperformed central anterior chamber depth (as measured by optical pachymetry and ultrasound) and autorefraction as a screening tool for the detection of occludable drainage angles identified by gonioscopy 16.
Laser peripheral iridotomy for narrow angles
The goal of screening for narrow angles is to identify patients at risk of developing angle closure and to treat prophylactically with a laser peripheral iridotomy. Patients with narrow but open angles should be followed for intraocular pressure elevation, progressive angle narrowing, and development of PAS. There is no evidence that iridotomy is indicated for narrow but open angles with normal intraocular pressure; however, laser peripheral iridotomy is fairly safe and can prevent a potentially vision-threatening outcome so the risks and benefits must be carefully considered in each case and discussed with the patient in details.
Indications for laser peripheral ridotomy:
- Elevation of previously normal intraocular pressure
- Presence of potentially occludable angle
- Peripheral anterior synechiae attributable to episodes of angle closure
- Progressive narrowing of the angle
- Requirement for medication that may provoke pupillary block (i.e. — antidepressants, anticholinergics, etc.)
- Symptoms that suggest prior or intermittent subacute angle closure
- Situation limiting a patient’s ability to immediately receive ophthalmic care (e.g.,frequent travel to less developed countries where treatment may not be readily available, lack of insurance, and poor access to transportation)
- Having another eye disorder that requires frequent dilated eye exams (e.g. diabetic retinopathy)
- History of acute primary angle closure glaucoma in other eye
Angle closure glaucoma signs and symptoms
Angle closure glaucoma symptoms
Patients with anatomic narrow angles without acute angle closure are typically asymptomatic in both the primary and secondary angle closure glaucoma. Similarly, primary and secondary chronic angle closure glaucoma patients often experience no symptoms unless they develop end-stage glaucoma, in which case they may complain of decreased vision or reduced peripheral vision.
Acute angle closure glaucoma, on the other hand, usually presents with dramatic symptoms from the quick rise in intraocular pressure. Patients complain of blurred vision, rainbows, halos around lights, or even transient loss of vision. They often have intense pain that may be localized to the eye, may follow the trigeminal distribution, or may be described as diffuse discomfort. Nausea and vomiting are common.
Subacute or intermittent angle closure attacks are brief episodes of angle closure that resolve spontaneously. Patients experience the above symptoms of acute angle closure, but on a milder scale. They will typically experience some blurring of the vision or halos with mild to moderate eye pain, brow ache, or headache. These attacks are often resolved by entering a well lit room which may cause miosis or sleep as sleep-induced miosis ameliorates the lesser degree of pupillary block in these patients.
Angle closure glaucoma signs
Signs of a primary anatomic narrow angle on slit lamp exam can be subtle and include a shallow anterior chamber and an anteriorly bowed iris.
Both primary and secondary forms of angle closure can cause acute angle closure attacks. The intraocular pressure usually exceeds 40 mmHg and may rise to as high as 80 mmHg. The conjunctiva is significantly injected. The cornea develops stromal and microcystic edema in response to the acute rise in eye pressure and decompensation of the endothelial pump mechanism. Iris sphincter ischemia leads to a fixed, mid-dilated pupil. Sectoral iris atrophy may occur, releasing pigment into the anterior chamber that dusts the corneal endothelium and anterior lens capsule. The overall anterior chamber is shallow. The center is usually formed, but the mid-peripheral iris bows forward and may touch the peripheral cornea. Often there is anterior chamber inflammation. The fundus is typically difficult to examine because of corneal edema. If visualized, the optic nerve head may be hyperemic and edematous. The angle is often difficult to examine with gonioscopy because of corneal edema, but if visualized, reveals contact of the peripheral iris with cornea.
In the aftermath of an acute attack, pupillary distortion may result if there is permanent sphincter damage and/or iris atrophy. Anterior lens capsule opacities, known as glaukomflecken, may result from damage to the anterior lens epithelium from high intraocular pressure. The angle may have permanent synechiae formation. Intraocular pressure may be low if the ciliary body is so ischemic that aqueous humor production is compromised. As the ciliary body recovers, normal aqueous humor production resumes and the intraocular pressure rises.
Angle closure glaucoma exhibits signs of optic neuropathy in the typical glaucomatous pattern with increased cupping of the optic nerve and retinal nerve fiber layer dropout.
Angle closure glaucoma complications
Complications of acute angle attacks are the result of a rapid, extreme rise in IOP. Possible sequelae include corneal decompensation, cataractous lens changes, iris ischemia resulting in atrophy and distortion, ciliary body shutdown with resultant hypotony, central retinal vein occlusion, optic nerve ischemia, and acute permanent vision loss.
Complications of chronic disease include all the same ones that can be seen in acute disease. The difference in chronic disease is that these conditions develop in a more insidious fashion over a longer period of time. These patients typically have asymptomatic progression of glaucomatous optic neuropathy with corresponding visual field defects developing over time.
Angle closure glaucoma diagnosis
Diagnosis of both primary and secondary angle closure glaucoma is based on history and eye exam. Gonioscopy is the gold standard for evaluating the anterior chamber angle, but imaging modalities assist in quantifying and objectifying angle characteristics. To distinguish between primary and secondary causes, the clinician must actively look for signs and symptoms of possible secondary causes and rule each out before the patient can be diagnosed with primary angle closure glaucoma.
History
- History of present illness – typical signs and symptoms of acute or subacute angle closure attacks and if patient was upset or in the dark when symptoms started
- Past ocular history
- Trauma – can cause zonular weakness or dehiscence allowing lens to displace anteriorly
- Incisional or laser surgery – can cause anterior chamber inflammation or predispose to epithelial/fibrous ingrowth; may also lead to aqueous misdirection (e.g. after laser peripheral iridotomy) or ciliary body engorgement (e.g. after extensive panretinal photocoagulation).
- History of prior retinal vein occlusion – can cause angle neovascularization or ciliary body engorgement rotating lens forward
- Past medical history – history of diabetes or carotid stenosis disease that can cause angle neovascularization
- Medications – use of systemic medications, such as sulfonamide, topiramate, and phenothizaines, that may cause ciliary body engorgement or suprachoroidal effusion; use of medications to treat allergy, bladder dysfunction, or depression; use of anticholinergics or sympathomimetics that can dilate pupil
- Family history of acute angle glaucoma
Physical examination
- Refractive status – hyperopic eyes tend to have shallower anterior chamber angles which places them at risk for angle closure
- Pupil size and reactivity
- Slit lamp exam
- Conjunctiva – injection
- Cornea – clarity, presence of edema, evidence of surgical or traumatic wounds
- Anterior chamber – central and peripheral depth, inflammation
- Iris – areas of atrophy, mass, neovascularization, or posterior synechiae
- Lens – thickness, phacodonesis, subluxation, glaucomflecken (necrosis of anterior lens capsule; may indicate previous attacks)
- Intraocular pressure measurement, preferably with applanation prior to gonioscopy
- Gonioscopy of both eyes with indentation to evaluate for appositional versus synechial angle closure
- Evaluation of fundus and optic nerve – dilation is often not advisable in primary angle closure attack until an iridotomy has been performed and/or the acute attack has resolved as dilation can exacerbate the condition. In contrast, dilation may be permissible as the appropriate treatment in certain forms of secondary angle closure. The fundus should be examined for underlying causes leading to the angle closure.
Gonioscopy
The key to diagnosis of anatomic narrow angle or angle closure is gonioscopy, which is still the gold standard method of angle evaluation. The ideal way to perform gonioscopy is in a dark room using a small rectangle of light only as bright as necessary to view the angle structures, as light can open an appositionally closed angle in about one-third of cases 17. Dynamic or compression or indentation gonioscopy is essential to differentiate appositional closure from synechial closure. Gentle pressure on the cornea with the goniolens pushes back the iris and reveals whether the angle can be opened any further; if not, synechial closure is present. This maneuver can also help break acute attacks by forcing fluid into the periphery and opening areas of appositional closure.
Occludable angles are typically described as eyes in which the posterior, usually pigmented, trabecular meshwork is seen for less than 90° of the angle circumference or if the angle width is less than 20° 18.
Angle Grading and Classification Systems
A. Scheie system (R)
- 0 – entire angle visible with wide ciliary body band
- I – last roll of iris obscuring part of the ciliary body
- II – nothing posterior to trabecular meshwork visible
- III – posterior portion of trabecular meshwork not visible
- IV – no structures posterior to Schwalbe’s line visible
Pigmentation graded 0 (no pigmentation) to 4 (heavily pigmented)
B. Shaffer system (R)
- 0 – closed or slit
- 1 – extremely narrow, ≤10 degrees
- 2 – narrow, 20 degrees
- 3 – open, 20-35 degrees
- 4 – wide open, 35-45 degrees
C. Spaeth system (R)
Level of iris insertion:
- A – anterior to trabecular meshwork
- B – anterior to posterior limit of trabecular meshwork
- C – posterior to scleral spur
- D – into the mid-ciliary body face (anterior ciliary body band visible)
- E – posterior ciliary body (wide band of ciliary body band visible)
Angle width – estimated in degrees from line tangential to the trabecular meshwork to line tangential to the iris surface one third of the way from the periphery (ranges from 0 – 40 degrees)
Curvature of iris:
- r – regular configuration, no significant forward or backward arching of iris
- s – steep or forward bowing (convex) curve
- q – queer or posterior bowing (concave) curve
Pigmentation: 0 (no pigment) to 4 (heavy pigmentation)
Change in angle configuration after indentation performed described by putting the original insertion in parenthesis, followed by the insertion after indentation. For example, if indentation shows that the insertion is actually a D when it originally appeared to be a C, it is indicated as a (C)D.
Provocative tests
Various provocative tests have been developed in an attempt to separate out patients who may be at higher risk of angle closure. In these tests, different maneuvers are used in an attempt to induce pupillary block, and then the pressure is rechecked and the angle is examined for narrowing. A test is considered positive if the IOP increases by 8 or more mmHg. In the dark room test, patients are placed in a dark room for 1-2 hours to dilate the pupil and increase resistance at the lens-iris channel.
The prone test involves placing the patient in the prone position for 1-2 hours without sleeping to anteriorly displace the lens and increase pupillary block. These tests have not been found to be very predictive of angle closure 19. Combining anterior chamber imaging (e.g. ultrasound biomicroscopy) with provocative testing assists in detecting apposition and allows measurement of various parameters of the angle 20, but their ability to predict future angle closure is not well established.
Pharmacologic provocative tests using mydriatic eye drops to increase pupillary block via pupil dilation have fallen out of favor as they carry a significant risk of angle closure in and of themselves.
Imaging modalities
To supplement information obtained through gonioscopy, there are several anterior segment imaging devices available that provide detailed images of structures and quantitative measurements. They are useful in primary angle closure but can also help detect secondary cases of angle closure, such as ciliary body masses or anterior rotation. At this time, there are no widely agreed upon quantitative measurement cutoffs obtained from these devices that distinguish a narrow angle from an open one.
Ultrasound biomicroscopy
This high-frequency B scan ultrasound provides high-resolution cross-sectional images of the anterior segment of the eye to the anterior vitreous. Because it uses sound, it can pass through opaque structures to visualize structures hidden from direct clinical examination, such as the ciliary body 21. It is particularly helpful for evaluating plateau iris and other ciliary body pathology. The disadvantages of ultrasound biomicroscopy include: requirement of a water bath immersion, specialized equipment, and a skilled technician to operate; it is also relatively costly and time consuming.
Anterior segment optical coherence tomography
This modality uses a diode light source instead of sound to produce highly detailed images of the cornea, angle region, and anterior ciliary body similar to those seen with ultrasound biomicroscopy. Compared to ultrasound biomicroscopy, anterior segment optical coherence tomography (OCT) is unable to image structures posterior to the iris plane well because of posterior pigmented iris shadowing and scleral light scattering 21. The advantages of anterior segment optical coherence tomography are that it is a noncontact exam: the patient can be imaged in an upright position avoiding positional lens changes, and all four quadrants can be scanned at once.
Scheimpflug photography
Digital images of the anterior chamber angle can be obtained using a Scheimpflug camera. Rotating versions of the camera provide three-dimensional photos that can be analyzed by computer software to measure specific parameters of the angle. The camera has an easy-to-use slit lamp type configuration but is expensive and requires special equipment. It cannot image the ciliary processes or body behind the iris.
Optic nerve assessment and imaging, retinal nerve fiber layer analysis, and visual field testing should be preformed to assess for signs of glaucomatous optic neuropathy in any patient with angle narrowing or angle closure glaucoma.
Summary of clinical findings in various types of secondary angle closure glaucoma
- Neovascularization of the angle – blood vessels from iris that cross scleral spur to arborize along trabecular meshwork, peripheral anterior synechiae
- Anterior chamber inflammation – keratic precipitates, posterior synechiae, iris bombé, inferior PAS (as opposed to primary angle closure where PAS tend to develop superiorly)
- Iridocorneal endothelial (ICE) syndrome – beaten-bronze corneal endothelium, corneal edema, high PAS that can extend anterior to the Schwalbe line, iris atrophy, corectopia
- Drug induced (e.g. systemic topiramate) – acute bilateral disease, acute myopic shift, uniformly shallow chamber with anterior iris and lens displacement, ciliochoroidal effusion or detachment
- Aqueous misdirection (malignant glaucoma) – flattening of central and periperhal anterior chamber, anterior displacement of lens (cystralline or intraocular lens) or vitreous face, clear “aqueous” zones in vitreous
- Lens-induced angle closure – thick cataract, unstable or subluxed lens
- Nanophthalmos – small but normal eye with short axial length, microcornea, large lens, and thickened sclera; choroidal effusion
- Retinopathy of prematurity or persistent hyperplastic primary vitreous – contracting retrolental tissue
- Iris or ciliary body mass lesions or cysts – irregular contour of iris or neovascularization, hyphema or vitreous hemorrhage, episcleral sentinel vessel, ciliary body mass through dilated pupil or on ultrasound biomicroscopy
- Posterior segment mass or large serous retinal detachment – signs of each on funduscopic exam
- Epithelial and/or fibrous downgrowth – wound dehiscence or gape, epithelial cysts in anterior chamber adjacent to wound, gray sheetlike membrane covering anterior segment structures that whitens with argon laser
- Pseudophakic or aphakic pupillary block – pupilary obstruction or synechiae to anterior hyaloid surface, the intraocular lens, or posterior capsule
- Ciliary body engorgement associated with retinal vascular occlusion or panretinal photocoagulation – anterior rotation of iris and lens; retinal signs of each underlying etiology, e.g. retinal hemorrhages for vein occlusion and extensive retinal laser scars from photocoagulation.
- Retinal surgery
- Encircling scleral buckle – relatively deep central anterior chamber with peripheral iris flattening, choroidal effusion
- Pars plana vitrectomy – pupillary block from expansile gases pushing iris and lens forward, silicone oil in the anterior chamber, non-patent iridotomy
Angle closure glaucoma treatment
The overall goals for management are to reverse or prevent the angle closure process, control intraocular pressure elevation, and prevent damage to the optic nerve. Some primary and secondary forms of angle closure may be treated similarly, while others require very different treatment approaches based on their underlying pathophysiology. Intraocular pressure (IOP) is lowered with glaucoma medications. Iridotomy is an essential part of treatment in primary angle closure glaucoma, but may not be indicated in some forms of secondary angle closure glaucoma. Trabeculectomy and tube shunts may also not be indicated for certain secondary forms of angle closure glaucoma.
Medical therapy
Acute angle closure glaucoma
The role of medical therapy in acute angle closure attacks is to lower IOP, reduce pain, and clear corneal edema in preparation for iridotomy. The medications below can be used, provided the patient has no condition contraindicating them:
Topical
- Beta blockers
- Selective alpha agonists
- Carbonic anhydrase inhibitors
- Miotics (e.g., pilocarpine 2%) may help break an early angle-closure attack, but may be ineffective if the iris is already ischemic. High-concentration miotics (e.g., pilocarpine 4%) should be avoided because of the potential for forward displacement iris-lens diaphragm.
- Prostaglandin analogues – unreliable effect in acute attack because of slow onset of action
- Hyperosmolar agent (e.g. 5% sodium chloride) – assists in clearing corneal edema
- Prednisolone 1% – decreases inflammation
Systemic
- Carbonic anhydrase inhibitors – oral acetazolamide’s maximum intraocular pressure reduction is reached in 2-4 hours and lasts for 6-8 hours. Intravenous acetazolamide drops the intraocular pressure (IOP) within 2 minutes with a peak effect noted by 10-15 minutes. In acute situations, a single dose of 500 mg acetazolamide should be given orally if the patient is not vomiting. Regular acetazolamide is preferred over the sustained-release sequel form because of quicker onset of action. If the patient is vomiting, acetazolamide can be given intravenously.
- Osmotic agents
- Mannitol can decrease the intraocular pressure (IOP) 30 mm Hg or more within 30 minutes of administration. The recommended intravenous dose is 0.5-1.5 g/kg body weight as a 15% or 20% solution, delivered at 3 to 5 mL/minute. Frail patients with cardiac or conditions may develop circulatory overload, pulmonary edema, congestive heart failure, and electrolyte imbalance. A rapid reduction in cerebral volume may result in subdural hematomas from vein rupture between the sagittal sinus and cortical surface. Therefore, patients receiving IV mannitol should be monitored in a hospital setting.
- Oral osmotic agents:
- Glycerin: 1 to 1.5 g/kg body weight of a 50% solution. Onset of pressure reduction is typically 10 to 30 minutes. Avoid in diabetics because the increased caloric load can cause ketoacidosis.
- Isosorbide is commercially available as a 45% (45 g/100 mL) solution (Ismotic; Alcon Surgical). The recommended dose is 1 to 1.5 g/kg body weight. Its effect is similar to glycerin’s but is safe for use in diabetics because it is not metabolized.
- Although less common, oral agents can also cause subdural hematomas. Headache and gastrointestinal upset are common adverse reactions.
Paracentesis
Paracentesis can be perfomed in an acute setting. Technically, it can be difficult to perform on a phakic eye in pain with a shallow chamber, and there is a risk of permanent damage to the cornea, lens, and iris. Devastating complications such as endophthalmitis and choroidal hemorrhage from a rapid pressure drop may occur. Also the effects are typically short-term, because, as the ciliary body begins to form aqueous again, the intraocular pressure (IOP) will inevitably rise. This procedure can be used in cases of extreme intraocular pressure (IOP) elevation to “buy time” until medications take effect or iridotomy can be performed.
Laser Iridotomy
Laser Iridotomy should be performed as soon as possible in the affected eye and in the contralteral eye to avoid an attack of acute angle closure glaucoma in the future.
Chronic angle closure glaucoma
Very few studies exist to address medical therapy in chronic angle closure glaucoma after laser iridotomy. In cases where elevated intraocular pressure becomes an issue, aqueous suppressants are helpful in reducing intraocular pressure (IOP) 22. Prostaglandin analogues have been shown to be effective in lowering intraocular pressure, even in angles that are partially closed 23. Evidence is not conclusive, however, regarding their effectiveness in cases of 360° degrees of synechial closure 24. The role of peripheral iridotomy and other surgical interventions are described below.
Peripheral iridotomy
See prevention section for information regarding prophylactic laser peripheral iridotomy for narrow angles.
Acute Angle Closure and Fellow Eyes
In angle closure secondary to pupillary block, an iridotomy is the definitive treatment. Laser peripheral iridotomy is considered an effective and safe treatment. It often breaks an attack of acute angle closure and can prevent future attacks. An incisional iridectomy may be necessary in cases of cloudy corneas, flat anterior chamber, poor patient cooperation at the laser, or inability to substantially lower the IOP with medications after a failed laser peripheral iridotomy attempt.
The fellow eyes of patients that have undergone primary acute angle-closure are generally at significant risk for an acute attack and should receive an iridotomy 25. An untreated fellow eye has a 40% to 50% chance of developing an acute primary angle-closure attack over the next 5 to 10 years 25. Chronic miotic therapy is not an acceptable alternative, as 50% of contralateral eyes of individuals suffering acute primary angle-closure developed acute attaks when treated with pilocarpine alone. This is in contrast to the 1.8% of patients treated with prophylactic incisional iridectomy who developed an attack during this same time period 26.
Chronic Angle Closure and Angle Closure Glaucoma
Laser peripheral iridotomy relieves the pupillary block component in chronic disease and may halt the progression of synechial closure and progressive IOP elevation 27. Its ability to control IOP, however, may not be long-lasting, especially in eyes where glaucomatous optic neuropathy has already developed. Additional medications or surgical treatment is often necessary 28. In cases where laser peripheral iridotomy does successfully lower IOP, eyes still need to be monitored routinely as IOP can increase months or years after the procedure 29.
Persistent or progressive rise in IOP after laser peripheral iridotomy
- Damage to trabecular meshwork and/or formation of PAS has occurred when iridocorneal apposition present
- Pupillary block may recur if iridotomy becomes occluded
- Factors other than pupillary block causing angle closure may have gone unrecognized until after the LPI (e.g. plateau iris syndrome)
- Angle closure may have been superimposed on pre-exisitng open angle glaucoma or another eye condition causing IOP elevation, such as pseudoexfolation
- There may be co-existing chronic open angle glaucoma
Complications of laser peripheral iridotomy
The most common complications of laser peripheral iridotomy are transient bleeding at site of treatment, hyphema, postoperative pressure spike, and anterior chamber inflammation. Occasionally, patients may complain of a seeing a double image if the lid does not cover the iridotomy site. More severe but rare complications include aqueous misdirection and injury to the cornea, lens, or retina.
Iridoplasty
In laser iridoplasty, contraction burns of long duration, low power, and large spot size are placed on the peripheral iris to contract the iris stroma and physically pull the iris from the drainage angle in an attempt to open the angle. In acute angle closure, iridoplasty has been found effective and safe in short-term lowering of IOP 30. It can be used in cases that are medically unresponsive, in which systemic carbonic anhydrase inhibitors must be avoided, when immediate iridotomy is not possible, or rarely when the attack continues despite a successful laser peripheral iridotomy. It is the procedure of choice for plateau iris syndrome when the angle fails to open and IOP remains elevated despite a patent peripheral iridotomy. In chronic cases of angle closure, iridoplasty may slightly decrease the formation of peripheral anterior synechiae 31.
It is important to note that iridoplasty does not eliminate pupillary block, so iridotomy remains necessary if pupillary block is the mechanism of angle closure 32. Potential complications include IOP spike, iris atrophy from destruction of iris vessels, corneal burns, marked anterior chamber inflammation, and corneal endothelial damage 24.
Cataract extraction
In primary angle closure glaucoma, since the lens is a key player in development of relative pupillary block, it makes sense that cataract extraction can lower IOP in both acute and chronic angle closure. Removal of the lens from an eye with a crowded anterior chamber opens the angle and may prevent or reduce peripheral anterior synechiae formation. In one study, early phacoemulsification was found to be better than laser peripheral iridotomy at preventing IOP rise after an acute angle closure event was controlled medically 33. Cataract extraction in the setting of an acute angle-closure attack, however, is technically difficult. The eye is inflamed with significant corneal edema, a shallow anterior chamber, an atrophic and atonic iris that is difficult to dilate, and possible zonular weakness. It may be more prudent to control the acute attack with medications and laser peripheral iridotomy first and then wait to perform surgery when the eye has recovered and is less inflamed.
In the chronic phase when patent laser iridotomy and medical treatment have failed to adequately control IOP, lens extraction many months after the initial attack has been found to reduce IOP and reduce the need for IOP medications 34. Cataract extraction can be combined with goniosynechialysis to further improve IOP control in the short term 35. Methods of goniosynechialysis include breaking synechiae with a heavy viscoelastic (viscogonioplasty), forceps, or a cyclodialysis spatula.
In lens-induced angle closure glaucoma, which includes phacomorphic glaucoma and angle closure due to forward subluxation of the lens, the definitive treatment is lensectomy. Acute attacks can be first controlled with medical therapy and/or laser peripheral iridotomy with lens extraction performed when the eye is quiet.
Filtration surgery
Filtration surgery has been performed for both acute and chronic angle closure glaucoma 36. The indications to perform filtration surgery in primary angle closure glaucoma are similar to those for surgery in POAG. In chronic cases, surgery is considered if the optic neuropathy is progressing and IOP is at a level believed to be contributing to the progression. Reasons for performing filtration surgery in the setting of an acute closure attack include medical unresponsiveness, lack of laser availability, or signs of glaucomatous optic neuropathy already present 37. The same techniques of filtration surgery are used as in primary open angle glaucoma, although some surgeons advocate tighter suturing of the trabeculectomy flap to avoid low IOP in the immediate postoperative period. A low IOP may contribute to further anterior chamber shallowing, which may lead to a higher rate of malignant glaucoma postoperatively 38.
Whether to perform filtration surgery versus a tube shunt procedure for secondary angle closure glaucoma depends on the underlying etiology. In most cases, dealing with the underlying pathology (e.g. stopping topiramate in drug-induced glaucoma, removing the lens in lens-induced glaucoma) will slow or stop the progression of disease. If medical therapy is not sufficient to control IOP, even when the primary pathology has been addressed, glaucoma surgery may be necessary and filtration surgery may be appropriate. Conditions such as neovascular glaucoma and ICE, however, tend to do better with glaucoma drainage implants. (see below). It has been proposed that combined phacotrabeculectomy may be more effective at controlling IOP than cataract extraction alone. Recent study results have been mixed, with some showing phacoemulsification as being superior for deepening the chamber 39, the two procedures being equal in terms of IOP control 40 and combined procedures being superior for IOP control 41. Of note, one randomized control trial found that patients who undergo combined procedures have more postoperative complications and progression of their optic neuropathy compared to the phacoemulsification alone group 42, so the risks and benefits of each procedure need to be carefully considered in each case until more definitive evidence is available.
Glaucoma drainage implants
A limited number of studies look at the use of tube shunt devices in primary angle closure glaucoma. Primary angle closure glaucoma eyes are often placed into the category of refractory glaucoma along with other types of glaucoma and thus are not separately evaluated. Based on the limited data available in these studies, tube implants appear effective in controlling IOP in primary angle closure glaucoma 43. Drainage implants are considered more effective than filtering procedures in neovascular glaucoma and ICE syndrome because, in these diseases, a fibrovascular membrane often grows over the sclerostomy site causing bleb failure.
Other surgical procedures
- May be required depending on the etiology of the underlying disease.
- Aqueous misdirection: Nd:YAG laser can be used to disrupt the anterior vitreous in aphakic and pseudophakic eyes. If that is not successful, definitive surgical treatment in the form of vitrectromy with anterior hyaloid disruption combined with an anterior chamber deepening procedure may be indicated.
- Epithelial and/or fibrous downgrowth: radical surgery to remove the intraocular membrane and affected tissues may be necessary.
- Angle closure that develops after retina surgery may require removing or loosening encircling bands, opening up iridectomy sites, or removing silicone oil.
Surgical follow up
Patients typically need to be watched closely in the immediate postoperative period, sometimes weekly for several months. Once IOP control is achieved and the eye is stabilized, follow up can follow the schedule of routine primary angle closure glaucoma patients.
Angle closure glaucoma prognosis
Primary angle closure suspects
Primary angle-closure suspect or anatomic narrow angle – an eye in which the anterior chamber angle recess has an abnormally narrow angular width. The peripheral iris is located close to, but not touching, the posterior pigmented trabecular meshwork. No peripheral anterior synechiae are present. IOP, optic nerve, and visual field are normal.
The overall likelihood of an individual with a anatomic narrow angle developing acute angle closure glaucoma in the United States is less than 10% 44. A prospective multicenter study, however, found that patients judged to be at risk for developing angle closure glaucoma by experienced ophthalmologists through careful slit lamp exam and gonioscopy had a 30% risk of developing angle closure within 5 years when no prophylactic intervention was performed 19.
In contrast, fellow eyes in which the other eye has already suffered an acute angle closure attack have a much worse prognosis without prophylactic treatment. An untreated fellow eye has a 40% to 50% chance of developing an acute primary angle closure attack over the next 5 to 10 years 29. An iridectomy or iridotomy virtually eliminates the risk 25. The long-term fate (4–6 years) in terms of IOP and glaucomatous optic neuropathy is good for most fellow eyes after laser peripheral iridotomy with the majority not requiring any additional glaucoma treatment and retaining good vision 45.
Acute angle closure
In an eye suffering an acute angle-closure attack, the long-term outcomes vary depending on ethnicity (which may be a reflection of mechanism of angle closure), duration of attack, and severity of attack in terms of whether or not it can be aborted by medical treatment alone. If promptly treated, most (60%–75%) symptomatic episodes of angle closure recover without visual field or optic disc damage in the short term 46. Six months post-attack, one study reported 38% of eyes to have visual field loss secondary to nerve fiber bundle loss 46. In another study, 2 – 16 weeks after an attack, changes were noted in optic disk morphology, with preferential loss in the superotemporal and inferotemporal areas 47.
The longer the duration of an attack and the more difficult to manage, the worse the outcome for the eye, regardless of the initial IOP measurement 48. Patients with a 24 to 72 hour delay in presentation had a relative risk of 2.78 for developing chronic glaucoma, whereas those requiring laser iridotomy to control IOP or a trabeculectomy had relative risks of 3.63 and 4.83, respectively 48. In Singapore, risk of visual field loss was significant if the duration of symptoms was longer than 7 days 46.
Even despite successful termination of an acute attack by surgical iridectomy, late IOP increase is reported in 19% to 24% of cases 49. There may be ethnic differences in the rate of IOP control by laser peripheral iridotomy alone 9. A greater extent of peripheral anterior synechiae, a high presenting IOP, and a larger cup to disc ratio have been reported as predictors of poor pressure control following iridotomy in Asian and African eyes 50. A significant portion of patients go on to develop primary angle closure glaucoma and require further medical or surgical intervention in an attempt to control their disease. Unfortunately, up to 20% these patients deteriorate to lose significant vision and are classified as blind in that eye 51.
Chronic angle closure glaucoma
Asymptomatic angle-closure patients present with more severe visual field defects than symptomatic patients 52. In one study which examined visual field loss on presentation, 52.8% of asymptomatic primary angle-closure glaucoma had end stage visual field loss by Advanced Glaucoma Intervention Study criteria compared to only 17.5% of symptomatic primary angle-closure glaucoma cases. Although presenting IOP was considerably higher in the symptomatic group, the level of IOP was not found to be a significant predictor for visual field outcome 53. It is likely that the duration of elevated IOP has a major influence in causing optic nerve damage in primary angle-closure glaucoma, possibly more so than the level of IOP. Once glaucomatous optic neuropathy has developed, almost all cases will require further treatment to control IOP (94%–100%) 54. Closer monitoring of IOP is recommended in chronic angle closure glaucoma compared to primary open angle glaucoma, despite the efficacy of medical therapy. Chronic angle-closure glaucoma tends to progress more quickly and fail medical therapy sooner than primary open angle glaucoma 55. With aggressive management, however, chronic angle-closure glaucoma patients can maintain stable fields and long-term IOP control 13.
Secondary angle closure glaucoma
The prognosis for secondary angle closure patients depends on the underlying cause. Early recognition of the underlying pathology and timely directed treatment helps to improve outcomes.
References- Leung CK, Cheung CY, Li H, et al. Dyanamic analysis of light-dark changes of the anterior chamber angle with anterior segment OCT. IOVS. 2007;48:4116-22
- Alsbirk PH. Corneal diameter in Greenland Eskimos. Anthropometric and genetic studies with special reference to primary angle-closure glaucoma. Acta Ophthalmol (Copenh). 1975;53:635–646.
- Wyatt H, Ghosh J. Behaviour of an iris model and the pupil block hypothesis. Br J Ophthalmol. 1970;54:177–185.
- Quigley HA. Angle-closure glaucoma – simpler answers to complex mechanisms: LXVI Edward Jackson Memorial Lecture. Am J Ophthalmol. 2009;148(5):657-669.e1.
- Wand M, Grant WM, Simmons RJ, Hutchinson BT. Plateau iris syndrome. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1977;83:122–130.
- He M, Foster PJ, Johnson GJ, Khaw PT. Angle-closure glaucoma in East Asian and European people. Different diseases? Eye. 2006;20:3–12.
- Lowe RF. Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normal eyes and eyes with primary angle-closure glaucoma. Br J Ophthalmol 1970;54:161-9.
- Wang N, Wu H, Fan Z. Primary angle closure glaucoma in Chinese and Western populations. Chin Med J (Engl). 2002;115:1706–1715.
- Seah SK, Foster PJ, Chew PT, et al. Incidence of acute primary angle-closure glaucoma in Singapore. An island-wide survey. Arch Ophthalmol. 1997;115:1436-40.
- Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–267
- Lai JS, Liu DT, Tham CC, et al. Epidemiology of acute primary angle-closure glaucoma in the Hong Kong Chinese population: prospective study. Hong Kong Med J. 2001;7:118-23.
- Alsbirk PH. Anatomical risk factors in primary angle-closure glaucoma. A ten year follow up survey based on limbal and axial anterior chamber depths in a high risk population. Int Ophthalmol. 1992;16:265-72.
- Sihota R, Sood A, Gupta V et al: A prospective longterm study of primary chronic angle closure glaucoma. Acta Ophthalmol Scand 82:209–213, 2004
- Lowe RF. Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normal eyes and eyes with primary angle-closure glaucoma. Br J Ophthalmol. 1970;54:161–169.
- He M, Huang W, Friedman DS et al. Slit lamp simulated oblique flashlight test in the detection of narrow angles in chinese eyes: The Liwan eye study. Invest Ophthalmol Vis Sci. 2007;48:5459–5463.
- Nolan WP, Aung T, Machin D et al. Detection of narrow angles and established angle closure in Chinese residents of Singapore: Potential screening tests. Am J Ophthalmol. 2006;141:896–901.
- Palmberg P. Shedding light on gonioscopy. Arch Ophthalmol. 2007;125:1417–1418.
- Foster PJ, Aung T, et al. Defining “occludable” angles in population surverys: drainage anger width, peripheral anterior synechiae, and glaucomatous optic neuropathy in east Asian people. Br J Ophthalmol. 2004;88(4):486-90.
- Wilensky JT, Kaufman PL, Frohlichstein D et al. Follow-up of angle-closure glaucoma suspects. Am J Ophthalmol. 1993;115:338–346.
- Wang B, Congdon NG, et al. Dark room provocative test and extent of angle closure: an anterior segment OCT study. J Glaucoma. 2009 Jul 9 (Epub ahead of print).
- Garcia JP Jr, Rosen RB. Anterior segment imaging: optical coherence tomography versus ultrasound biomicroscopy. Ophthalmic Surg Lasers Imaging. 2008;39(6):476-84.
- Aung T, Wong HT, Yip CC et al. Comparison of the intraocular pressure-lowering effect of latanoprost and timolol in patients with chronic angle closure glaucoma: A preliminary study. Ophthalmology. 2000;107:1178–1183
- Hung PT, Hsieh JW, Chen YF, Wei T. Efficacy of latanoprost as an adjunct to medical therapy for residual angle-closure glaucoma after iridectomy. J Ocul Pharmacol Ther. 2000;16:43–47
- Aung T, Chew PT. Review of recent advancements in the understanding of primary angle-closure glaucoma. Curr Opin Ophthalmol. 2002;13:89–93.
- Edwards RS. Behaviour of the fellow eye in acute angle-closure glaucoma. Br J Ophthalmol. 1982;66:576–579.
- Lowe RF. Primary angle-closure glaucoma. Prevention and early treatment. Isr J Med Sci. 1972;8:1362–1365.
- Saw SM, Gazzard G, Friedman DS. Interventions for angle-closure glaucoma: an evidence-based update. Ophthalmology. 2003;11:1869-78.
- Alsagoff Z, Aung T, Ang LP, Chew PT. Long-term clinical course of primary angle-closure glaucoma in an Asian population. Ophthalmology. 2000;107:2300–2304.
- Ang LP, Aung T, Chew PT. Acute primary angle closure in an Asian population: long-term outcome of the fellow eye after prophylactic laser peripheral iridotomy. Ophthalmology. 2000;107:2092-6.
- Lim AS, Tan A, Chew P et al. Laser iridoplasty in the treatment of severe acute angle closure glaucoma. Int Ophthalmol. 1993;17:33–36.
- Sun X, Liang YB, et al. Laser Peripheral Iridotomy with and without Iridoplasty for Primary Angle-Closure Glaucoma: 1-Year Results of a Randomized Pilot Study. Am J Ophthalmol. 2010 May 14. Epub ahead of print.
- Ritch R, Tham CC, Lam DS. Argon laser peripheral iridoplasty (ALPI): An update. Surv Ophthalmol. 2007;52:279–288.
- Lam DS, Leung DY, et al. Randomized trial of early phacoemulsification versus peripheral iridotomy to prevent intraocular pressure rise after acute primary angle closure. Ophthalmology. 2008;115(7):1134-40.
- Imaizumi M, Takaki Y, Yamashita H. Phacoemulsification and intraocular lens implantation for acute angle closure not treated or previously treated by laser iridotomy. J Cataract Refract Surg. 2006;32:85–90.
- Teekhasaenee C, Ritch R. Combined phacoemulsification and goniosynechialysis for uncontrolled chronic angle-closure glaucoma after acute angle-closure glaucoma. Ophthalmology. 1999;106:669–674.
- Salmon JF. The role of trabeculectomy in the treatment of advanced chronic angle closure glaucoma. J Glaucoma. 1993;2:285–190.
- Lai JS, Tham CC, Lam DS. Incisional surgery for angle closure glaucoma. Semin Ophthalmol. 2002;17:92–99.
- Trope GE, Pavlin CJ, Bau A et al. Malignant glaucoma. Clinical and ultrasound biomicroscopic features. Ophthalmology. 1994;101:1030–1035.
- Tham CC, Leung DY, et al. Effects of phacoemulsification versus combined phaco-trabeculectomy on drainage angle status in primary angle closure glaucoma (PACG). J Glaucoma. 2010;19(2):119-23.
- Tsai HY, Liu CJ, Cheng CY. Combined trabeculectomy and cataract extraction versus trabeculectomy alone in pimary angle-closure glaucoma. Br J Ophthalmol. 2009;93(7):943-8.
- Tham CC, Kwong YY, et al. Phacoemulsification versus combined phacotrabeculectomy in medically uncontrolled chronic angle closure glaucoma with cataracts. Ophthalmology. 2009;116(4):725-31, 731.e1-3.
- Tham CC, Kwong YY, et al. Phacoemulsification vs phacotrabeculectomy in chronic angle-closure glaucoma with cataract complications. Arch Ophthalmol. 2010;128(3):303-11.
- Deokule SP, Molteno AC, Bevin TH, Herbison P. Long-term results of Molteno implant insertion in cases of chronic angle closure glaucoma. Clin Experiment Ophthalmol. 2007;35:514–519.
- Spaeth GL. Gonioscopy: Uses old and new. The inheritance of occludable angles. Ophthalmology. 1978;85:222–232.
- Friedman DS, Chew PT, Gazzard G et al. Long-term outcomes in fellow eyes after acute primary angle closure in the contralateral eye. Ophthalmology. 2006;113:1087–1091.
- Aung T, Looi AL, Chew PT. The visual field following acute primary angle closure. Acta Ophthalmol Scand. 2001;79:298–300.
- Shen SY, Baskaran M, Fong AC et al. Changes in the optic disc after acute primary angle closure. Ophthalmology. 2006;113:924–929.
- Wong JS, Chew PT, Alsagoff Z, Poh K. Clinical course and outcome of primary acute angle-closure glaucoma in Singapore. Singapore Med J. 1997;38:16–18.
- Saraux H, Offret H. Long-term study of patients with iridectomy for angle-closure glaucoma. Glaucoma. 1979;1:149–151.
- Nolan WP, Foster PJ, Devereux JG et al. YAG laser iridotomy treatment for primary angle closure in East Asian eyes. Br J Ophthalmol. 2000;84:1255–1259
- Aung T, Friedman DS, Chew PT et al. Long-term outcomes in Asians after acute primary angle closure. Ophthalmology. 2004;111:1464–1469.
- Dhillon B, Chew PT, Lim AS. Field loss in primary angle closure glaucoma. Asia Pac J Ophthalmol. 1990;2:85–87.
- Ang LP, Aung T, Chua WH et al. Visual field loss from primary angle-closure glaucoma: A comparative study of symptomatic and asymptomatic disease. Ophthalmology. 2004;111:1636–1540.
- Rosman M, Aung T, Ang LP et al. Chronic angle-closure with glaucomatous damage: Long-term clinical course in a North American population and comparison with an Asian population. Ophthalmology. 2002;109:2227–2231.
- See JL, Chew PT. Glaucoma in Singapore. J Glaucoma. 2004;3:417–420.





{kind=link}