What is an aromatase inhibitor
Aromatase is the enzyme responsible for the conversion of testosterone to estrone (E1) and androstenedione to estradiol (E2) 1. The human aromatase enzyme is a member of the cytochrome P450 family and expressed by the CYP19A1 gene located on chromosome 15q21.2 2. Highest levels of aromatase are found in the ovary and placenta, which are the major sources of estrogen in premenopausal women. However, aromatase is also found in other tissues, such as liver, kidney, adrenals, brain, muscle and subcutaneous fat where it is also active in producing estrogens, although at low levels. These tissues are the major source of estrogen after menopause or oopherectomy. Aromatase inhibitors were developed to block the synthesis of estrogen in the peripheral tissues and, thus, as antiestrogen therapy of estrogen receptor positive breast cancer in postmenopausal women. The first aromatase inhibitor used in clinical medicine was aminoglutethimide, which was initially developed as an anticonvulsant, but later found to inhibit adrenocorticoid steroid synthesis.
Aromatase inhibitors block the aromatase cytochrome P450 enzyme. Aromatase inhibitors lower estrogen levels by stopping an enzyme in fat tissue (called aromatase) from changing other hormones into estrogen. These drugs don’t stop the ovaries from making estrogen. They only lower estrogen levels in women whose ovaries aren’t making estrogen (such as women who have already gone through menopause). Because of this, they are used mainly in women who are past menopause.
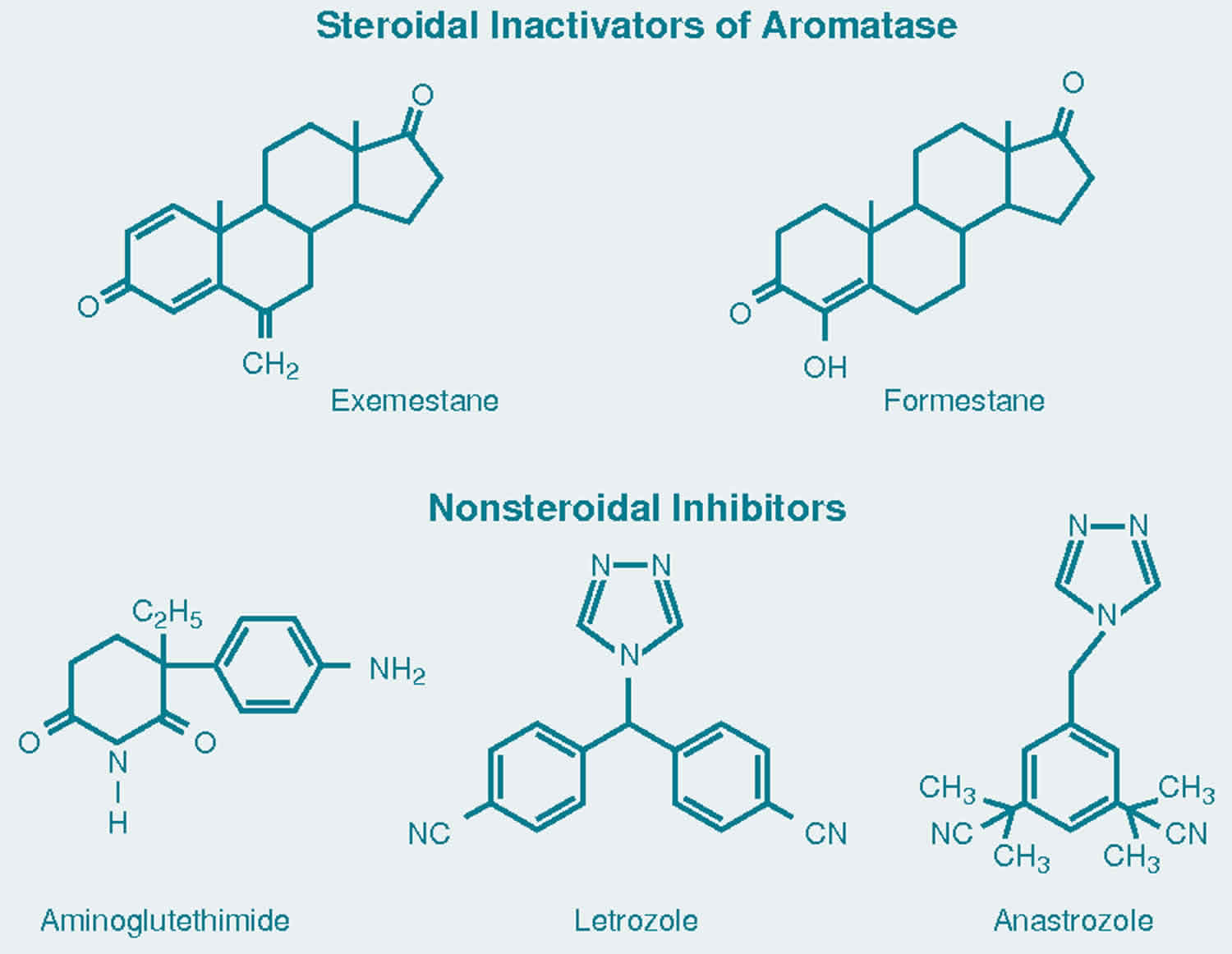
More specific aromatase inhibitors with antiestrogen effects only were subsequently developed, the current agents being considered third generation inhibitors. These inhibitors include anastrozole and letrozole which are nonsteroidal, and exemestane which is a steroidal aromatase inhibitor. These agents have little or no effect on adrenal glucocorticoid or mineralocorticoid synthesis. The commercial names and year of approval in the United States are: letrozole (Femara, 1995), anastrozole (Arimidex, 1997), and exemestane (Aromasin, 1999). All three agents are now available in generic forms as well. They are used largely as adjuvant therapy in postmenopausal women with estrogen sensitive breast cancer, generally given in daily oral doses for up to five years.
Figure 1. Aromatase mechanism of action
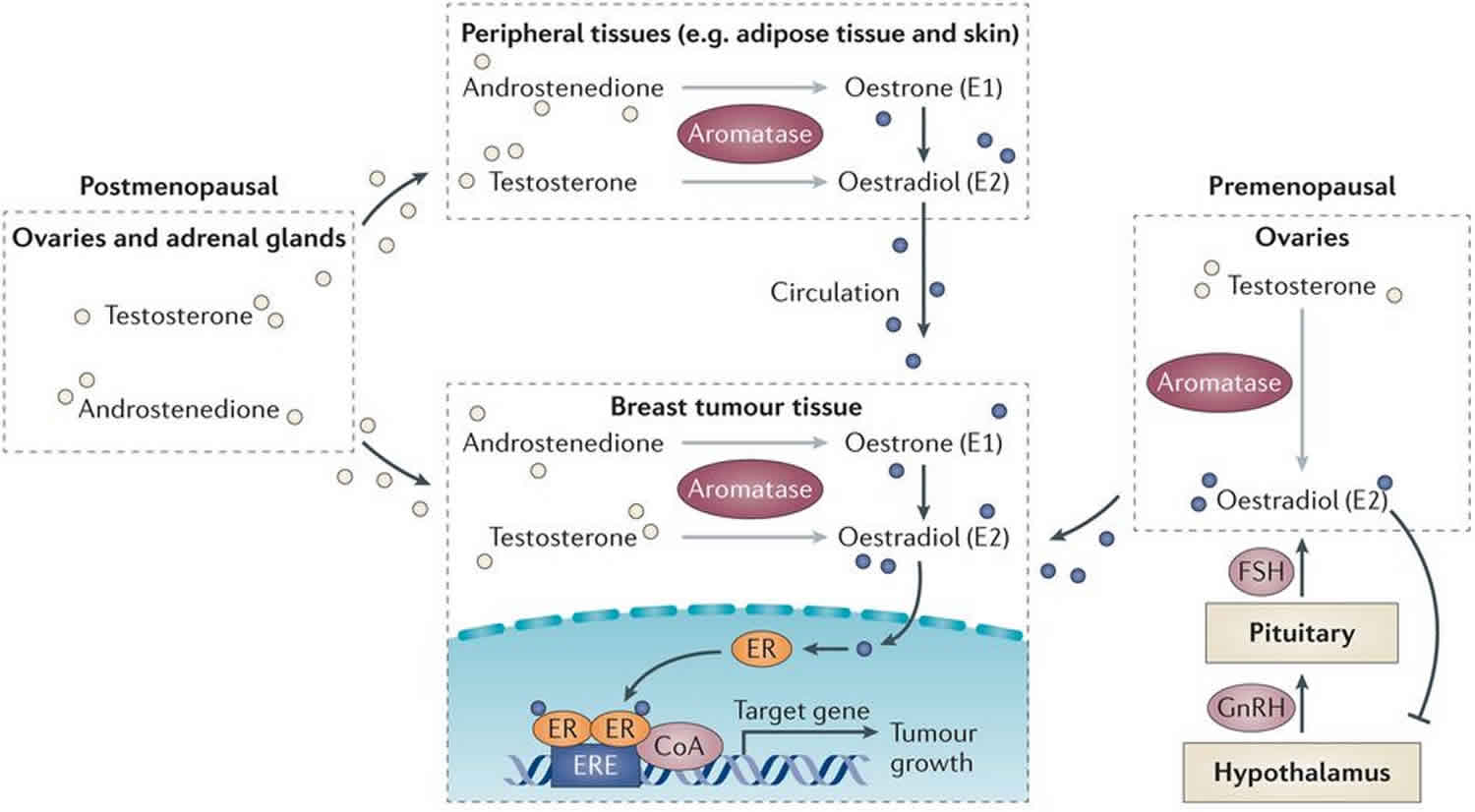
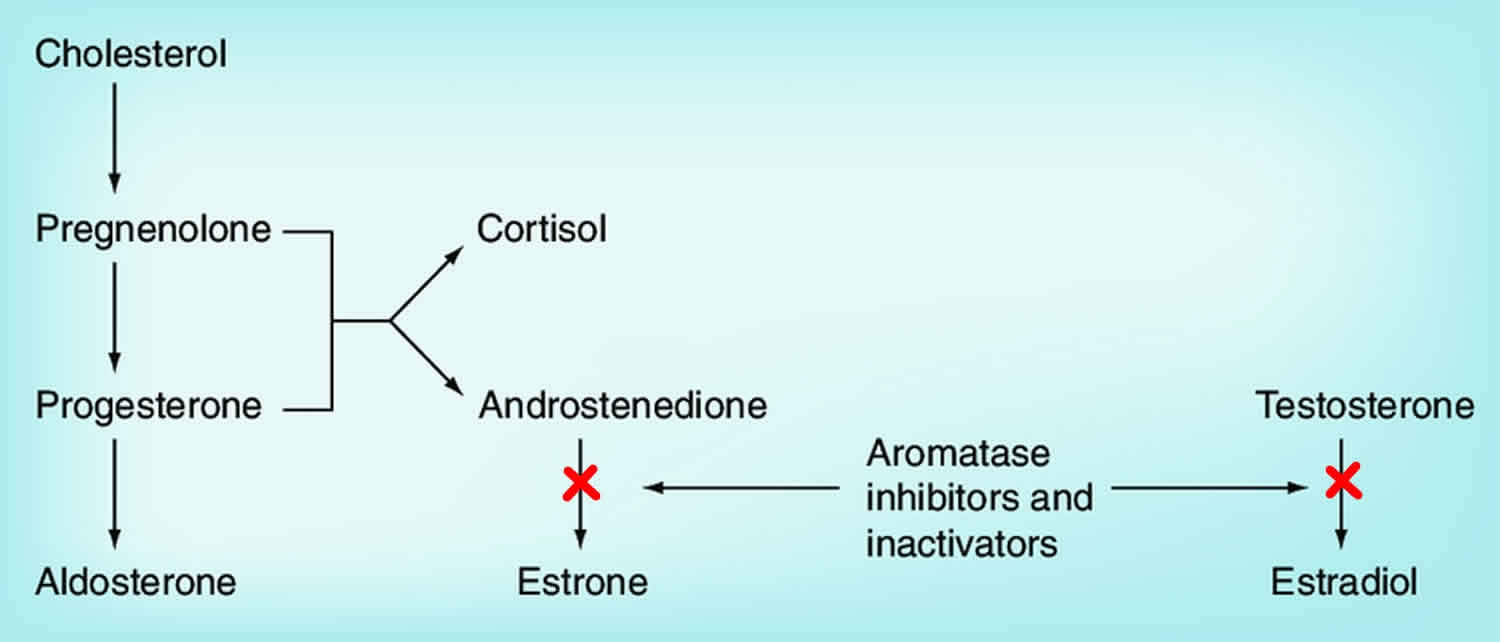
Figure 2. Aromatase inhibitors mechanism of action (aromatase inhibitors block the aromatase cytochrome P450 enzyme)
Aromatase inhibitors breast cancer
The aromatase inhibitors block estrogen synthesis and are used as therapy of estrogen receptor positive breast cancer, usually after resection and as a first line treatment or after failure of tamoxifen (another antiestrogen that acts by blocking the estrogen receptor).
Aromatase inhibitors may someday prove to be as good as or even better than tamoxifen or raloxifene in reducing breast cancer risk, but they haven’t been studied as much for this use. More research is needed to see how effective they are, who would most benefit from them, and how long treatment should be continued.
Can aromatase inhibitors lower the risk of breast cancer?
Aromatase inhibitors are used mainly to treat women with hormone receptor-positive breast cancer. But large studies of anastrozole and exemestane have also found that they can lower breast cancer risk in postmenopausal women who are at increased risk.
Aromatase inhibitors are not yet approved in the US to lower breast cancer risk. However, some medical organizations include them as options along with tamoxifen and raloxifene to reduce breast cancer risk in women who are past menopause. For example, they might be a reasonable option for women who have an increased risk of blood clots and therefore should not take tamoxifen or raloxifene. When used to lower the risk of breast cancer, these drugs are taken daily for 5 years.
Aromatase inhibitors drugs
Aromatase inhibitors drugs include:
- Anastrozole (Arimidex),
- Letrozole (Femara) and
- Exemestane (Aromasin).
Aromatase inhibitors are pills taken once a day.
Anastrozole
Anastrozole is an nonsteroidal aromatase inhibitor that works by decreasing the amount of estrogen the body makes in postmenopausal women, which may slow the growth of certain types of breast tumors that need estrogen to grow in the body. Anastrozole is used with other treatments, such as surgery or radiation, to treat breast cancer in postmenopausal women. Anastrozole is often given to women whose cancer has progressed even after taking tamoxifen (Nolvadex, Soltamox). Anastrozole is also used in postmenopausal women, as a first treatment of breast cancer that has spread within the breast or to other areas of the body. Anastrozole is available only with your doctor’s prescription.
Anastrozole is a nonsteroidal inhibitor of aromatase, the enzyme responsible for the conversion of testosterone to estrone (E1) and of androstenedione to estradiol (E2). Highest levels of aromatase are found in the ovary and placenta, which are the major sources of estrogen in premenopausal women. However, aromatase is also found in other tissues, such as liver, kidney, adrenals, brain, muscle and subcutaneous fat where it is also active in producing estrogens, although at low levels. These tissues are the major source of estrogen in postmenopausal women. Inhibitors of aromatase were developed to block the synthesis of estrogen in the peripheral tissues and thus, as antiestrogen therapy of estrogen receptor positive breast cancer in postmenopausal women. The aromatase inhibitors in current use include letrozole, exemestane and anastrozole. Anastrozole is a nonsteroidal, specific aromatase inhibitor which has little or no effect on adrenal glucocorticoid or mineralocorticoid synthesis. Anastrozole was approved for use in postmenopausal women with breast cancer in the United States in 1995. Anastrozole is available in 1 mg tablets in generic forms and under the brand name Arimidex. Its current indications are as adjuvant therapy in postmenopausal women with hormone responsive breast cancer, as first line therapy of locally invasive or metastatic estrogen receptor positive breast cancer in postmenopausal women, and as adjuvant therapy in postmenopausal women with advanced breast cancer not responsive to tamoxifen.
Anastrozole comes as a tablet to take by mouth. Anastrozole is typically given in single oral doses of 1 mg daily for up to five years. But you may need to take anastrozole for several years or longer. Anastrozole is usually taken once a day with or without food. Take anastrozole at around the same time every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take anastrozole exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor. Continue to take anastrozole even if you feel well. Do not stop taking anastrozole without talking to your doctor.
Anastrozole common side effects include hot flashes, night sweats, fatigue, dizziness, headache, somnolence, abdominal discomfort, nausea, arthralgias, weight gain and rash. Uncommon, but potentially severe side effects of anastrozole include decrease in bone mineral density, increase in serum cholesterol and increased rate of cardiovascular events.
Exemestane
Exemestane is a steroidal inhibitor of aromatase which effectively blocks estrogen synthesis in postmenopausal women and is used as therapy of estrogen receptor positive breast cancer, usually after resection and after failure of tamoxifen. Exemestane is also used to treat early breast cancer in postmenopausal women and who have already been treated with a medication called tamoxifen (Nolvadex) for 2 to 3 years. Exemestane is also used to treat breast cancer in women who have experienced menopause whose breast cancer has worsened while they were taking tamoxifen. Exemestane is in a class of medications called aromatase inhibitors. It works by decreasing the amount of estrogen produced by the body. This can slow or stop the growth of some breast tumors that need estrogen to grow.
Exemestane was approved for use in postmenopausal women with estrogen receptor positive breast cancer in the United States in 1999. Exemestane is available in 25 mg tablets in generic forms and under the brand name Aromasin. Current indications are as adjuvant therapy in postmenopausal women with estrogen sensitive breast cancer after failure, intolerance or as replacement of tamoxifen.
Exemestane is a steroidal inhibitor of aromatase which effectively blocks estrogen synthesis in postmenopausal women and is used as therapy of estrogen receptor positive breast cancer, usually after resection and after failure of tamoxifen. Aromatase is the enzyme responsible for the conversion of testosterone to estrone (E1) and of androstenedione to estradiol (E2). Highest levels of aromatase are found in the ovary and placenta, which are the major sources of estrogen in premenopausal women. However, aromatase is also found in other tissues, such as liver, kidney, adrenals, brain, muscle and subcutaneous fat where it is also active in producing estrogens, although at low levels. These tissues are the major source of estrogen in postmenopausal women. Inhibitors of aromatase were developed to block the synthesis of estrogen in the peripheral tissues and, thus, as antiestrogen therapy of estrogen receptor positive breast cancer in postmenopausal women. Exemestane is a steroidal, specific aromatase inhibitor which has little or no effect on adrenal glucocorticoid or mineralocorticoid synthesis.
Exemestane is given in doses of 25 mg once daily by mouth for up to five years.
Exemestane common side effects include hot flashes, night sweats, arthralgias, fatigue, dizziness, nervousness, insomnia, nausea, weight gain and headache. Uncommon, but potentially severe adverse reactions include reduction in body mineral density and embryo-fetal toxicity.
Letrozole
Letrozole is a nonsteroidal inhibitor of aromatase which effectively blocks estrogen synthesis in postmenopausal women and is used as therapy of estrogen receptor positive breast cancer, usually after resection and after failure of tamoxifen. Letrozole was approved for use in postmenopausal women with estrogen receptor positive breast cancer in the United States in 1997. Current indications are as adjuvant therapy in postmenopausal women with estrogen sensitive breast cancer, given in daily oral doses for up to five years. Letrozole is also indicated as a first line treatment of estrogen receptor positive (or unknown), locally advanced or metastatic breast cancer in postmenopausal women.
Letrozole is a nonsteroidal aromatase inhibitor that is widely used as therapy of breast cancer, usually after surgical resection. Aromatase is the enzyme responsible for the conversion of testosterone to estrone (E1) and of androstenedione to estradiol (E2). Highest levels of aromatase are found in the ovary and placenta, which are the major sources of estrogen in premenopausal women. However, aromatase is also found in other tissues, such as liver, kidney, adrenals, brain, muscle and subcutaneous fat where it is also active in producing estrogens, although at low levels. These tissues are the major source of estrogen in postmenopausal women. Inhibitors of aromatase were developed to block the synthesis of estrogen in the peripheral tissues and, thus, as antiestrogen therapy of breast cancer in postmenopausal women. Letrozole is a nonsteroidal, specific aromatase inhibitor which has little or no effect on adrenal glucocorticoid or mineralocorticoid synthesis.
Letrozole is available in 2.5 mg tablets in generic forms and under the brand name Femara. The recommended dose is one tablet daily.
Letrozole common side effects include hot flashes, night sweats, fatigue, dizziness, headache, somnolence, abdominal discomfort, nausea, arthralgias, weight gain and rash. Uncommon, but potentially severe side effects include decrease in bone mineral density, increases in serum cholesterol levels and embryo-fetal toxicity.
Aromatase inhibitors side effects
The most common side effects of aromatase inhibitors are symptoms of menopause, such as hot flashes, night sweats, and vaginal dryness.
These drugs can also cause muscle and joint pain. This side effect can be serious enough to cause some women to stop taking the drugs.
Unlike tamoxifen and raloxifene, aromatase inhibitors tend to speed up bone thinning, which can lead to osteoporosis. People with osteoporosis are more likely to have broken bones.
Aromatase inhibitors may raise cholesterol. Women with pre-existing coronary heart disease who take an aromatase inhibitor may be at risk of having a heart problem.
References- Production and actions of estrogens. Gruber CJ, Tschugguel W, Schneeberger C, Huber JC. N Engl J Med. 2002 Jan 31; 346(5):340-52.
- Human aromatase: cDNA cloning, Southern blot analysis, and assignment of the gene to chromosome 15. Chen SA, Besman MJ, Sparkes RS, Zollman S, Klisak I, Mohandas T, Hall PF, Shively JE. DNA. 1988 Jan-Feb; 7(1):27-38.





{kind=link}