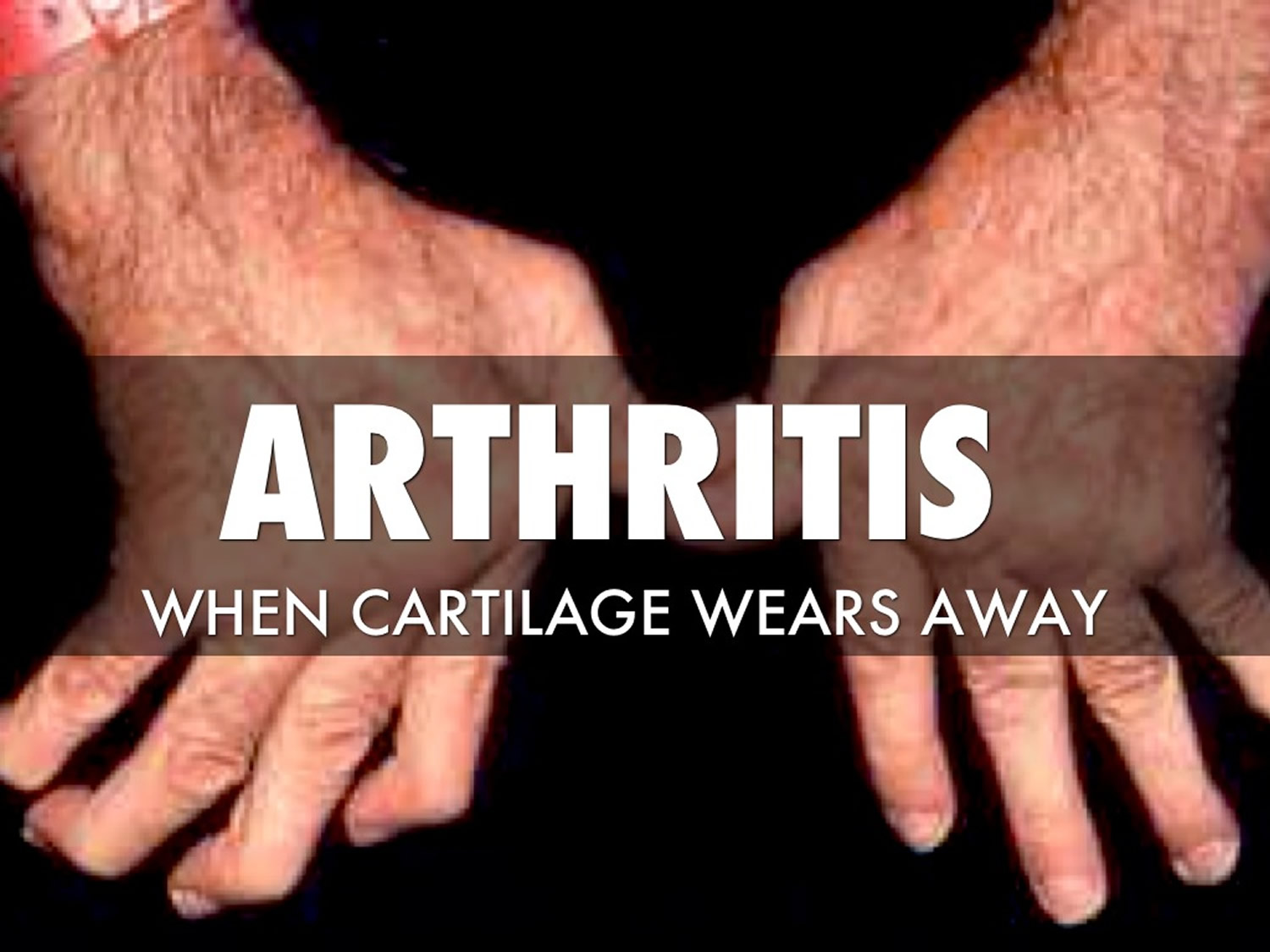
What is arthritis
Arthritis literally means joint inflammation 1. The term arthritis is derived from arthro meaning ‘joint’ and -itis meaning ‘inflammation’. However, arthritis is not one disease alone, but an umbrella term for more than 100 conditions that affect the joints of your body, because there are more than 100 different types of arthritis. Arthritis is a common condition that causes pain, swelling, and limited movement in your joints. Arthritis affects joints and connective tissues around the body. Joints are places where 2 or more bones meet, such as in the wrist, elbow, knuckles, hips, knees and ankles. If you have arthritis, the joints are inflamed, causing discomfort and pain. Arthritis can also cause permanent joint changes. These may be visible, such as knobby finger joints, but often the damage can be seen only on X-rays.
Common arthritis symptoms include swelling, pain, stiffness and diminished range of motion in joints. Symptoms vary from mild to severe and may come and go. Some may stay about the same for years, but symptoms can also progress and get worse over time. Severe arthritis can result in chronic pain, difficulty performing daily activities and make walking and climbing stairs painful and grueling.
An estimated 58.5 million U.S. adults have some form of arthritis 2. Experts believe that number will grow as the nation’s population gets older. Osteoarthritis affects more than 3.8% of people, while rheumatoid arthritis affects about 0.24% of people 3.
The 2 most common types of arthritis are:
- Osteoarthritis. This is the most common type of arthritis. It is a chronic disease of the joints, especially the weight-bearing joints of the knee, hip, and spine. Osteoarthritis destroys the coating on the ends of bones (cartilage) and narrows the joint space. Osteoarthritis can also cause bone overgrowth, bone spurs, and reduced function. Osteoarthritis occurs in most people as they age. It may also occur in young people because of an injury or overuse.
- Rheumatoid arthritis. This is an inflammatory disease of the joint linings. The inflammation may affect all of the joints. It can also affect organs such as the heart or lungs.
Other types of arthritis or related disorders include:
- Gout. This condition causes uric acid crystals to build up in small joints, such as the big toe. It causes pain and inflammation.
- Lupus. This is a chronic autoimmune disorder. It causes periods of inflammation and damage in joints, tendons, and organs.
- Scleroderma. This autoimmune disease causes thickening and hardening of the skin and other connective tissue in the body.
- Ankylosing spondylitis. This disease causes the bones of the spine to grow together. It can also cause inflammation in other parts of the body. It can affect the shoulders, hips, ribs, and the small joints of the hands and feet.
- Juvenile idiopathic arthritis (JIA) also known as juvenile rheumatoid arthritis (JRA). This is a form of arthritis in children that causes inflammation and joint stiffness. Children often outgrow juvenile idiopathic arthritis (JIA). But it can affect bone development in a growing child.
Arthritis is common among people with other chronic conditions including obesity, diabetes, and heart disease. Some types of arthritis affect other organs, such as your heart, eyes, lungs, kidneys and skin as well as the joints.
Talk to your doctor if you have arthritis symptoms such as pain, stiffness, or swelling in or around one or more of your joints.
Doctors usually diagnose arthritis using the patient’s medical history, physical examination, X-rays, and blood tests.
Treatments vary depending on the type of arthritis. The main goals of arthritis treatments are to reduce symptoms, minimize joint damage and improve or maintain physical function and quality of life. Fortunately, current treatments allow most people with arthritis to lead active and productive lives.
According to the American College of Rheumatology, arthritis treatment can include medications, nondrug therapies such as physical therapy or patient education, and sometimes surgery.
Figure 1. Arthritis
Joints get sore and swollen for many reasons. It could be due to an injury, overuse, or doing a new type of physical activity.
See your doctor if you have joint pain and stiffness that starts with no clear reason, lasts for more than a few days, and also causes swelling, redness and warmth. It is important to start treatment as soon as possible to prevent the condition from getting worse and causing long-term damage.
What should I do if I think I have arthritis?
See your doctor as soon as possible if you have symptoms of arthritis. Your doctor will ask you about your symptoms and examine your joints. They may do some tests or x-rays, but these can be normal in the early stages of arthritis. It may take several visits before your doctor can tell what type of arthritis you have. This is because some types of arthritis can be hard to diagnose in the early stages. Your doctor may also send you to a rheumatologist, a doctor who specialises in arthritis, for more tests.
Is there a cure for arthritis?
Currently there is no cure for most forms of arthritis. While there are treatments that can effectively control symptoms, you should be wary of any products or treatments that claim to cure arthritis.
Can arthritis be treated?
Many types of arthritis can be easily and effectively controlled by modern treatment. Early diagnosis and the right treatment can ease symptoms and may even prevent damage to your joints. Research has led to great improvements in this area. Because arthritis affects people in different ways, treatment has to be tailored to the needs of each person. It is important to work with your healthcare team to find treatments that suit you.
Can I exercise with arthritis?
Arthritis-friendly physical activity is good for people with arthritis. Participating in joint-friendly physical activity can improve your arthritis pain, function, mood, and quality of life. Joint-friendly physical activities are low-impact, which means they put less stress on the body, reducing the risk of injury. Examples of joint-friendly activities include walking, biking and swimming. Being physically active can also delay the onset of arthritis-related disability and help people with arthritis manage other chronic conditions such as diabetes, heart disease, and obesity. Learn how you can increase your physical activity safely.
Regular physical activity can:
- Help relieve arthritis pain and stiffness.
- Give you more energy.
- Lift your mood and make you feel more positive.
Stay as active as your health allows, and change your activity level depending on your arthritis symptoms. Some physical activity is better than none.
When starting or increasing physical activity, start slow and pay attention to how your body tolerates it.
How much exercise do I need?
Adults with arthritis should aim for at least 150 minutes a week of moderate-intensity activity such as brisk walking or 75 minutes a week of vigorous-intensity aerobic activity, like cycling at 10 mph or faster, or an equivalent combination. You should also aim for at least 2 days a week of activities that strengthen muscles and include activities to improve balance such as standing on one foot. If you cannot do 150 minutes a week, stay as active as your health allows. Change your activity level depending on your arthritis symptoms. Some physical activity is better than none.
What should I do if I have pain when I exercise?
It’s normal to have some pain, stiffness, and swelling after starting a new physical activity program. It may take 6 to 8 weeks for your joints to get used to your new activity level, but sticking with your activity program will result in long-term pain relief.
Here are some ways to manage your pain while your joints adjust to your new activity level.
Tips for managing your pain during and after exercise:
- Until your pain improves, modify your physical activity program by exercising less frequently (days per week), for shorter periods of time (amount of time each session), or with less intensity.
- Try a different type of exercise to reduce pressure on your joints—for example, switch from walking to water aerobics.
- Do proper warm-up and cool-down before and after exercise.
- Exercise at a comfortable pace—you should be able to carry on a conversation while exercising.
- Make sure you have good fitting, comfortable shoes.
See your doctor if you experience any of the following:
- Pain that is sharp, stabbing, and constant.
- Pain that causes you to limp.
- Pain that lasts more than 2 hours after exercise or gets worse at night.
- Pain or swelling that does not get better with rest, medication, or hot or cold packs.
- Large increases in swelling or if your joints feel “hot” or are red.
Does being overweight affect arthritis?
It is important for people with arthritis to maintain a healthy weight. For people who are overweight or obese, losing weight reduces pressure on joints, particularly weight bearing joints like the hips and knees. In fact, losing as little as 10 to 12 pounds can reduce pain and improve function for people with arthritis.
At any age, low-impact, arthritis-friendly physical activity and diet changes can help you lose weight.
Can children get arthritis?
Yes, children can get arthritis. The most common type of arthritis found in children is juvenile idiopathic arthritis (JIA), also known as childhood arthritis or juvenile rheumatoid arthritis (JRA).
Signs and symptoms of childhood arthritis may include:
- Joint pain
- Swelling
- Fever
- Stiffness
- Rash
- Fatigue (tiredness)
- Loss of appetite
- Inflammation of the eye
- Difficulty with daily living activities such as walking, dressing, and playing.
Childhood arthritis causes permanent damage to the affected joint or joints. Early diagnosis and proper treatment are important to prevent or minimize permanent damage. There is no cure for childhood arthritis, but some children with childhood arthritis achieve permanent remission, which means the disease is no longer active.
Types of arthritis
There are several types of arthritis. Common ones include:
- Ankylosing Spondylitis is arthritis that affects the spine. It often involves redness, heat, swelling, and pain in the spine or in the joint where the bottom of the spine joins the pelvic bone.
- Gout is caused by uric acid crystals that build up in the joints. It usually affects the big toe, but many other joints may be affected.
- Juvenile Arthritis is the term used to describe arthritis in children. Arthritis is caused by inflammation of the joints.
- Osteoarthritis usually comes with age and most often affects the fingers, knees, and hips. Sometimes osteoarthritis follows a joint injury. For example, you might have badly injured your knee when young and develop arthritis in your knee joint years later.
- Psoriatic Arthritis can occur in people who have psoriasis (scaly red and white skin patches). It affects the skin, joints, and areas where tissues attach to bone.
- Reactive Arthritis is pain or swelling in a joint that is caused by an infection in your body. You may also have red, swollen eyes and a swollen urinary tract. Reactive arthritis can cause inflammation of the joints, eyes and urethra (the tube that urine passes through). It develops shortly after an infection of the bowel, genital tract or, less frequently, after a throat infection.
- Rheumatoid arthritis happens when the body’s own defense system doesn’t work properly. It affects joints and bones (often of the hands and feet), and may also affect internal organs and systems. You may feel sick or tired, and you may have a fever.
- Enteropathic arthritis – a form of chronic, inflammatory arthritis associated with inflammatory bowel disease (IBD), the two best-known types being ulcerative colitis and Crohn’s disease. About one in five people with Crohn’s or ulcerative colitis will develop enteropathic arthritis. The most common areas affected by inflammation are the peripheral (limb) joints and the spine.
- Cervical spondylosis – also known as degenerative osteoarthritis, cervical spondylitis affects the joints and bones in the neck, which can lead to pain and stiffness.
- Secondary arthritis – a type of arthritis that can develop after a joint injury and sometimes occurs many years afterwards.
Arthritis is also seen with other conditions. These include:
- Systemic Lupus Erythematosus (Lupus). Lupus happens when the body’s defense system harms the joints, heart, skin, kidneys, and other organs.
- Infection (septic arthritis) that gets into a joint and destroys the cushion between the bones.
- Fibromyalgia – causes pain in the body’s muscles, ligaments and tendons.
- Polymyalgia rheumatica – a condition that almost always affects people over 50 years of age, where the immune system causes muscle pain and stiffness, usually across the shoulders and tops of the legs. It can also cause joint inflammation.
Ankylosing Spondylitis
Ankylosing spondylitis is a type of arthritis that affects the spine 4. Ankylosing spondylitis often involves redness, heat, swelling, and pain in the spine or in the joint where the bottom of the spine (sacrum) joins the pelvic bone (ilium).
In some people, ankylosing spondylitis can also affect the shoulders, ribs, hips, knees, and feet. It can also affect areas where the tendons and ligaments attach to the bones. Sometimes it can affect the eyes, bowel, and very rarely, the heart and lungs.
Many people with ankylosing spondylitis have mild back pain that comes and goes. Others have severe pain that doesn’t go away. Sometimes the spine becomes stiff. In the worst cases, the swelling can cause two or more bones of the spine to fuse. This may stiffen the rib cage, making it hard to take a deep breath.
Who gets ankylosing spondylitis ?
A combination of genes may make it more likely you will get ankylosing spondylitis. The environment also probably plays a role. Men are about twice more likely than women to get ankylosing spondylitis.
Ankylosing spondylitis causes
- The cause of ankylosing spondylitis is unknown. It’s likely that genes (passed from parents to children) and the environment both play a role. The main gene associated with the risk for AS is called HLA-B27. Having the gene doesn’t mean you will get ankylosing spondylitis. Fewer than 1 of 20 people with HLA-B27 gets ankylosing spondylitis. Scientists recently discovered two more genes (IL23R and ERAP1) that, along with HLA-B27, make it more likely you will get ankylosing spondylitis.
Ankylosing spondylitis diagnosis
Your doctor will give you a physical exam and ask you about your medical history in order to diagnose you with ankylosing spondylitis. Bone/joint scans and lab tests may help confirm a diagnosis.
Medical history
Your doctor will probably ask you the following questions during a medical history:
- How long have you had pain?
- Where is the pain in your back or neck? Are other joints affected?
- Is back pain better with exercise and worse after inactivity, such as when you first get up in the morning?
- Do you have other problems, such as eye problems or fatigue?
- Does anyone in your family have back problems or arthritis?
- Have you recently suffered from a stomach upset or diarrhea?
- Do you have any skin rashes such as psoriasis?
Physical exam
During the physical exam, your doctor will look for symptoms of ankylosing spondylitis. These include pain in the spine, pelvis, joint between the pelvis and spine, heels, or chest. Your doctor may ask you to move and bend in different directions. This is to check the flexibility of your spine. You will also be asked to breathe deeply. This is to check for rib stiffness caused by continued swelling of the joints where the ribs attach to the spine.
Bone and joint scans
Your doctor may confirm you have ankylosing spondylitis by taking pictures of your spine and of the joint between your spine and pelvic bone. Pictures are taken using x-rays or magnetic resonance imaging (MRI), which uses magnets and radio waves (not radiation). However, you may have the disease for years before changes show on x-rays. MRI may allow for earlier diagnosis, because it can show damage to soft tissues and bone before it can be seen on an x-ray. Both tests may also be used to see if the disease worsens.
Lab tests
Your blood may be tested for the HLA-B27 gene, which is present in most people with ankylosing spondylitis. The test is less useful if you are African American or from some Mediterranean countries, since you are less likely to have the gene even if you do have ankylosing spondylitis. The gene is also found in many people who do not have ankylosing spondylitis, and will never get it. Still, having the gene is one more indicator you have ankylosing spondylitis, when you also have symptoms and x-ray evidence of the disease.
Ankylosing spondylitis treatment
There is no cure for ankylosing spondylitis, but some treatments relieve symptoms may possibly prevent the disease from getting worse. In most cases, treatment involves a combination of medication, exercise, and self-help measures. In some cases, surgery may be used to repair some of the joint damage caused by the disease.
You should work with your doctor to find the safest and most effective medications for you, which will likely include one or more of the following:
Nonsteroidal anti-inflammatory drugs (NSAIDs). NSAIDs relieve pain and inflammation, and are commonly used to treat ankylosing spondylitis. Examples include aspirin, ibuprofen, and naproxen.
Some NSAIDs are available over the counter, but others are available only with a prescription.
NSAIDs can have side effects, and some people seem to respond better to one NSAID than another. You should see your doctor on a regular basis if you take NSAIDs over a long period of time.
Corticosteroids. These strong inflammation-fighting drugs are similar to the cortisone made by your body. If NSAIDs alone do not control your joint swelling, your doctor may inject corticosteroids directly into the affected joints to bring quick but temporary relief. Injections may be given to the hip joint, knee joint, or joint between the spine and pelvic bone. Injections are not given in the spine.
Disease-modifying antirheumatic drugs (DMARDs). These drugs work in different ways. The most common DMARDs for ankylosing spondylitis are sulfasalazine and methotrexate.
Biologic agents. These medications block proteins involved in your body’s inflammatory response. Several biologics are approved by the Food and Drug Administration (FDA) for treating ankylosing spondylitis. These drugs are either injected or given intravenously (IV) and are often effective for ankylosing spondylitis when other treatments are not.
Surgery. Total joint replacement may be an option if ankylosing spondylitis causes severe joint damage that makes it difficult to do your daily activities. Your surgeon will remove the damaged joint and replace it with a man-made one made of metals, plastics, and/or ceramic materials. The most commonly replaced joints are the knee and hip.
There is also surgery to straighten the spine, if it has fused into a curved-forward position. This is generally considered a high-risk procedure, and it is only done in very rare cases. A surgeon who is highly experience in the procedure will cut through the spine so that it can be placed into a straighter up/down position. Hardware may be needed to hold the spine in its new position while it heals.
Home Remedies for ankylosing spondylitis
- Exercise: Besides seeing your doctor regularly and following your treatment plan, staying active is probably the best thing you can do for ankylosing spondylitis. Regular exercise can help relieve pain, improve posture, and maintain flexibility. Before beginning an exercise program, speak with your doctor or physical therapist about designing a program that’s right for you. Some helpful exercises include:
- Strengthening exercises, performed with weights or done by tightening muscles without moving the joints, build the muscles around your painful joints to better support them. Exercises that don’t require joint movement can be done even when your joints are painful and inflamed.
- You should gently straighten and bend your joints as far as they will comfortably go. This will improve movement flexibility and reduce stiffness in the painful joint. If the spine is painful and/or inflamed, exercises to stretch and extend the back can be helpful in preventing long-term disability.
- You may find it helpful to exercise in water.
- Diet: A healthy diet is good for everyone, and it may be very helpful if you have ankylosing spondylitis. There is no specific diet for people with ankylosing spondylitis, but keeping a healthy weight is important. It reduces stress on painful joints. Omega-3 fatty acids, found in coldwater fish (such as tuna and salmon), flax seeds, and walnuts, might reduce disease activity. This is still being studied.
- Posture: Another important thing you can do for yourself is to practice good posture. A good test for posture is to check yourself in a mirror. First, stand with a full-length mirror to your side and, if possible, turn your head to look at your profile. Next, imagine you have dropped a weighted string from the top of your head to the soles of your feet. Where does the string fall? If your posture is good, it should pass through your earlobe, the front of your shoulder, the center of your hip, behind your kneecap, and in front of your anklebone. If you are not standing that way already, practice holding your body that way in front of a mirror until you know well how it feels. Practicing good posture can help you avoid some of the complications that can occur with ankylosing spondylitis.
Arthritis pilates workout
A pilates exercise is suitable for people with arthritis.
This 32-minute class takes you through a series of gentle exercises to get your joints moving safely. You will need a cushion or a pillow for this class.
Regular pilates practice can help improve posture, muscle tone, balance and joint mobility, as well as relieve stress and tension.
Enteropathic arthritis
Enteropathic arthritis is a type of chronic, inflammatory arthritis associated with the occurrence of an inflammatory bowel disease (IBD), the two best-known types of which are ulcerative colitis and Crohn’s disease 5. About one in five people with Crohn’s or ulcerative colitis will develop enteropathic arthritis. However, the term enteropathic arthritis is also associated other gastrointestinal diseases, such as Whipple’s disease, celiac disease, and intestinal bypass surgery 6, 7.
The most common areas affected by enteropathic arthritis are the peripheral (limb) joints and, in some cases, the entire spine can become involved, as well. Abdominal pain and, possibly, bloody diarrhea associated with inflammatory bowel disease (IBD) are also components of the disease.
Interestingly, potential risk factors for arthritis in inflammatory bowel disease (IBD) patients are active bowel disease, family history of IBD, appendectomy, cigarette smoking, and the presence of others extraintestinal manifestations, such as erythema nodosum or pyoderma gangrenosum 8, 9, 10, 11.
Enteropathic arthritis causes
The precise causes of the enteropathic arthritis are unknown. Many people don’t realize that the gastrointestinal tract contains the largest immune system in the body. The immune system is the body’s natural defense against foreign invaders, and it is somehow altered in people who have enteropathic arthritis. Some researchers believe that the long-lasting inflammation found in the intestines of people with inflammatory bowel disease (IBD) damages the bowel, which in turn may allow bacteria to enter the damaged bowel wall and circulate through the blood stream. The body’s reaction to these bacteria may cause other problems, including inflammation in the joints and/or spine, skin sores, and inflammation of the eyes. Currently, this hypothesis is neither fully understood nor confirmed by rigorous scientific study.
Spondyloarthritis diseases tend to run in families, so there is a genetic factor involved, as well. Those who test positive for the HLA-B27 genetic marker are much more likely to have spinal involvement with enteropathic arthritis than those who test negative.
Enteropathic arthritis symptoms
The symptoms of enteropathic arthritis can be divided in two groups:
- Symptoms of inflammatory bowel disease (IBD)
- Arthritic symptoms in the joints and, possibly, elsewhere in the body.
Enteropathic arthritis diagnosis
A diagnosis of enteropathic arthritis is made through a complete medical examination including a history of symptoms and taking into account family history. Various tests may also be done to determine the presence of an inflammatory bowel disease and inflammatory arthritis.
Besides examining a full medical history of symptoms and taking a thorough family history, various tests may be performed:
- A stool culture may be taken if a diagnosis of an inflammatory bowel disease (IBD) such as ulcerative colitis and Crohn’s disease has not yet been established.
- A colonoscopy with or without bowel biopsies may also be done.
- Blood tests may be done including an erythrocyte sedimentation rate (ESR or SED Rate), which may help in detecting inflammation, a test to determine the presence of the HLA-B27 genetic marker, and/or a C-reactive protein (CRP), which is another test that may help detect the presence of inflammation in the body.
- Synovial fluid (fluid that lubricates the joints) may be taken from affected joints for study.
- X-rays of affected joints may be taken.
Enteropathic arthritis treatment
Currently, there is no known cure for enteropathic arthritis but there are medications and therapies available to manage the symptoms of both the arthritis and bowel components of the disease.
Treatment of inflammatory bowel disease (IBD), including surgery, should always be the initial strategy to induce remission of peripheral arthritis. Total colectomy or removal of affected colon induces remission of the peripheral arthritis in ulcerative colitis, but not in Crohn disease 12. Surgery provides no benefit for axial involvement in IBD.
Although nonsteroidal anti-inflammatory drugs (NSAIDs) are usually recommended as first-line therapy for spondyloarthropathies, in patients with IBD, these agents may exacerbate gastrointestinal symptoms 13. Selection of more cyclooxygenase-2 (COX-2)–selective NSAIDs may reduce the risk of bowel flares 14. Corticosteroids may be used systemically or by local injection.
Sulfasalazine (2-3g/day) has been shown to be effective for treatment of the peripheral arthropathy associated with IBD, but not axial disease 15. While methotrexate can be useful to treat bowel activity in Crohn disease, its effect on joint disease with IBD is less certain. Vedolizumab is approved for treatment of moderate to severe Crohn disease. A systematic review found evidence that it may be effective in preventing the onset of enteropathic anthropathy but there was no strong evidence for the efficacy of vedolizumab for treating existing arthritis 16.
Gout
Gout is a kind of arthritis that causes attacks of pain and stiffness in your joints, especially your big toe. Gout is caused by crystals of a substance called uric acid building up in your joints 17. Many people get their first attack of gout in one of their big toes, but it can also affect other joints in your feet, arms, and legs. In addition to pain, your joint may feel swollen, red, warm, and stiff.
Gout attacks often start suddenly at night. Intense pain and swelling may be bad enough to wake you up. Gout attacks are often triggered by stressful events, alcohol, drugs, or another illness.
Usually, a gout attack will get better in three to 10 days, even without treatment. After that, you may not have another attack for months or even years. Over time, however, your attacks may last longer and happen more often.
It can also cause lumps under the skin and kidney stones.
For some people, gout progresses through several stages:
- Hyperuricemia, when you have elevated levels of uric acid in your blood, but no symptoms.
- Acute gout, when you have an attack of intense pain and swelling in your joints. Acute attacks often come on at night and can be triggered by stress, drugs, alcohol, or another illness. An acute attack usually clears up within three to 10 days, even without treatment.
- Interval or intercritical gout, which is the time between gout attacks when you don’t have any symptoms.
- Chronic tophaceous gout, a late stage of gout when the condition may have permanently damaged your joints and kidneys. With proper treatment, most people do not reach this stage.
Who gets gout?
Millions of people get gout. It is especially common in men between the ages of 40 and 50. Women rarely develop gout before menopause.
You are more likely to get it if you:
- Have a family history of gout.
- Have had an organ transplant.
- Are a man.
- Are an adult.
- Are overweight.
- Drink alcohol.
- Eat foods that are rich in purines, a substance that breaks down into uric acid.
- Are exposed to lead in your environment.
Some health problems can also increase your risk of getting gout, including:
- Renal insufficiency, a condition in which your kidneys don’t eliminate enough waste.
- High blood pressure.
- Hypothyroidism, a condition in which your thyroid gland is underactive.
- A condition that cause your cells to turnover rapidly, such as psoriasis, hemolytic anemia, or some cancers.
- Kelley-Seegmiller syndrome or Lesch-Nyhan syndrome, two rare conditions in which your body either doesn’t have the enzyme that regulates uric acid levels or doesn’t have enough of that enzyme.
Some medications can increase your risk of getting gout, including:
- Diuretics, which help your body eliminate excess fluid.
- Salicylate-containing drugs, such as aspirin.
- Niacin, a vitamin.
- Cyclosporine, a medication used to treat some autoimmune diseases and people who have had organ transplants.
- Levodopa, a medication prescribed to treat Parkinson’s disease.
Gout causes
Gout is caused when a substance in your body called uric acid forms crystals in your joints. This causes pain, swelling, and other symptoms.
Uric acid comes from purines, which are found in your body’s tissues and many foods. When purines break down, they become uric acid. Uric acid normally dissolves in your blood and passes out of your body in urine. When too much of it builds up in your blood, however, it can form the crystals in your joints that cause gout.
Things that can cause uric acid to build up in the blood include:
- Your body increasing the amount of uric acid it makes.
- Your kidneys not getting rid of enough uric acid.
- Eating too many foods high in purines, such as liver, dried beans and peas, and anchovies.
Gout symptoms
Gout causes pain in your joints, often in the big toe. Many people get their first attack of gout in one of their big toes, but it can also affect other joints in your feet, arms, and legs. In addition to pain, your joint may feel swollen, red, warm, and stiff.
Gout attacks often start suddenly at night. Intense pain and swelling may be bad enough to wake you up. Gout attacks are often triggered by stressful events, alcohol, drugs, or another illness.
Usually, a gout attack will get better in three to 10 days, even without treatment. After that, you may not have another attack for months or even years. Over time, however, your attacks may last longer and happen more often.
Gout diagnosis
Gout can be difficult to diagnose because its symptoms are similar to several different conditions. Your doctor may test your blood to see if you have high levels of uric acid. They may also draw a sample of fluid from one of your painful joints to look for crystals of uric acid.
Gout treatment
Proper treatment can reduce the pain from gout attacks, help prevent future attacks, and prevent damage to your joints.
Your doctor may recommend medications to treat your pain. These may include:
- Anti-inflammatory drugs (NSAIDs), which can reduce pain and swelling.
- Corticosteroids, such as prednisone, which are strong anti-inflammatory hormones.
- Colchicine, which works best when taken within the first 12 hours of a gout attack.
- Other medications to reduce symptoms or reduce the build-up of uric acid in your blood.
Your doctor may also recommend diet and lifestyle changes, such as losing weight, since being overweight puts you at a greater risk of gout attacks, and cutting back on alcohol and foods that are high in purines.
In addition to taking medications recommended by your doctor, you can make some changes to your diet to help you have fewer gout attacks. As always, talk with your doctor before making any changes to your diet or medications.
Your doctor may recommend that you lose weight, if you are overweight, or drink less alcohol. You can also avoid eating foods with lots of purines, since they can increase your uric acid levels.
Foods that are high in purines include:
- Anchovies.
- Asparagus.
- Beef kidneys.
- Brains.
- Dried beans and peas.
- Game meats.
- Gravy.
- Herring.
- Liver.
- Mackerel.
- Mushrooms.
- Sardines.
- Scallops.
- Sweetbreads.
Juvenile arthritis
Juvenile arthritis is a term that describes arthritis in children. There are more than 100 arthritic or rheumatic diseases that may affect the joints but can also cause pain, swelling, and stiffness in other supporting structures of the body such as muscles, tendons, ligaments, and bones. Some rheumatic diseases can also affect other parts of the body, including various internal organs.
In the Unites States, juvenile arthritis and other rheumatic conditions affect nearly 294,000 children age 0 to 17.
- Children can develop almost all types of arthritis that affect adults, but the most common type that affects children is juvenile idiopathic arthritis.
Juvenile idiopathic arthritis is an umbrella term, or classification system, for all of the more specific types of chronic, or long-lasting, arthritis in children. These conditions used to fall under the term, juvenile rheumatoid arthritis, which is no longer used.
Types of Juvenile idiopathic arthritis
There are seven separate subtypes of juvenile idiopathic arthritis, each with distinct symptoms. However, with every subtype, a child will have arthritis symptoms of joint pain, swelling, tenderness, warmth, or stiffness that last for more than 6 continuous weeks.
The subtypes are:
- Systemic juvenile idiopathic arthritis previously known as systemic juvenile rheumatoid arthritis. Systemic means the arthritis can affect the whole body, rather than just a specific organ or joint. A child has arthritis with, or that was preceded by, a fever that has lasted for at least 2 weeks. The fever has come and gone, but spiked, or hit its highest temperature, for at least 3 days. The fever occurs with at least one or more of the following:
- Generalized enlargement of the lymph nodes.
- Enlargement of the liver or spleen.
- Inflammation of the lining of the heart (pericarditis) or the lungs (pleuritis).
- The characteristic rheumatoid rash, which is flat, pale, pink, and generally not itchy. The individual spots of the rash are usually the size of a quarter or smaller. They are present for a few minutes to a few hours, and then disappear without any changes in the skin. The rash may move from one part of the body to another.
- Oligoarticular juvenile idiopathic arthritis previously known as pauciarticular juvenile rheumatoid arthritis. A child has arthritis affecting one to four joints during the first 6 months of disease. Two subcategories of this type are:
- Persistent oligoarthritis, which means the child never has more than four joints involved throughout the disease course.
- Extended oligoarthritis, which means that more than four joints are involved after the first 6 months of the disease.
- Polyarticular juvenile idiopathic arthritis – rheumatoid factor negative previously known as polyarticular juvenile rheumatoid arthritis – rheumatoid factor negative. A child has arthritis in five or more joints during the first 6 months of disease, and all tests for rheumatoid factor (proteins produced by the immune system that can attack healthy tissue, which are commonly found in rheumatoid arthritis and juvenile arthritis) are negative.
- Polyarticular juvenile idiopathic arthritis – rheumatoid factor positive previously known as polyarticular rheumatoid arthritis – rheumatoid factor positive. A child has arthritis in five or more joints during the first six months of the disease. Also, at least two tests for rheumatoid factor, at least three months apart, are positive.
- Psoriatic juvenile idiopathic arthritis. A child has both arthritis and psoriasis (a skin disease), or has arthritis and at least two of the following:
- Inflammation and swelling of an entire finger or toe (this is called dactylitis)
- Nail pitting or splitting
- A first-degree relative with psoriasis.
- Enthesitis-related juvenile idiopathic arthritis. The enthesis is the point at which a ligament, tendon, or joint capsule attaches to the bone. If this point becomes inflamed, it can be tender, swollen, and painful with use. The most common locations are around the knee and at the Achilles tendon on the back of the ankle. A child is diagnosed with this condition if he or she has both arthritis and inflammation of an enthesitis site, or has either arthritis or enthesitis with at least two of the following:
- Inflammation of the sacroiliac joints (at the bottom of the back) or pain and stiffness in the lumbosacral area (in the lower back).
- A positive blood test for the human leukocyte antigen (HLA) B27 gene.
- Onset of arthritis in males after age six years.
- A first-degree relative diagnosed with ankylosing spondylitis, enthesitis-related arthritis, or inflammation of the sacroiliac joint in association with inflammatory bowel disease or acute inflammation of the eye.
- Undifferentiated arthritis. A child is said to have this condition if the signs and symptoms of the arthritis do not fulfill the criteria for one of the other six categories or if they fulfill the criteria for more than one category.
Juvenile arthritis symptoms
The most common symptom of all types of juvenile arthritis is persistent joint swelling, pain, and stiffness that is typically worse in the morning or after a nap. The pain may limit movement of the affected joint, although many children, especially younger ones, will not complain of pain.
One of the earliest signs of juvenile arthritis may be limping in the morning because of an affected knee.
Besides joint symptoms, children with systemic juvenile arthritis may have:
- A high fever that may appear and disappear very quickly.
- A skin rash that may appear and disappear very quickly.
- Swollen lymph nodes located in the neck and other parts of the body.
- Inflammation of internal organs, including the heart (fewer than half of the cases) and the lungs (very rarely).
Juvenile arthritis causes
Most forms of juvenile arthritis are autoimmune disorders in which the body’s immune system – which normally helps to fight off bacteria or viruses – mistakenly attacks some of its own healthy cells and tissues. The result is inflammation, marked by redness, heat, pain, and swelling. Inflammation can cause joint damage.
Doctors do not know why the immune system attacks healthy tissues in children who develop juvenile arthritis. Scientists suspect that it is a two-step process. First, something in a child’s genetic makeup gives him or her a tendency to develop juvenile arthritis; then an environmental factor, such as a virus, triggers the development of the disease.
Not all cases of juvenile arthritis are autoimmune, however. Recent research has shown that some people, such as many with systemic arthritis, have what is called an autoinflammatory condition. Although the two terms sound similar, the disease processes behind autoimmune and autoinflammatory disorders are different.
- Autoimmune Disorders
When the immune system is working properly, foreign invaders such as bacteria and viruses provoke the body to produce proteins called antibodies. Antibodies attach to these invaders so the immune system can recognize and destroy them. In an autoimmune reaction, the antibodies attach to the body’s own healthy tissues by mistake, signaling the body to attack them. Because they target the self, these proteins are called autoantibodies.
- Autoinflammatory Disorders
Like autoimmune disorders, autoinflammatory conditions also cause inflammation. And like autoimmune disorders, they also involve an overactive immune system. However, autoinflammation is not caused by autoantibodies. Instead, autoinflammation involves a more primitive part of the immune system that, in healthy people, causes white blood cells to destroy harmful substances. When this system goes awry, it causes inflammation for unknown reasons. Besides inflammation, autoinflammatory diseases often cause fever and rashes.
Juvenile arthritis treatment
The main goals of treatment are to:
- Preserve a high level of physical and social functioning.
- Maintain a good quality of life.
To achieve these goals, doctors recommend treatments that:
- Reduce swelling.
- Maintain full movement in the affected joints.
- Relieve pain.
- Prevent, identify, and treat complications.
Most children with juvenile arthritis need a combination of medication and other treatments to reach these goals.
- Medications
Nonsteroidal anti-inflammatory drugs (NSAIDs). Aspirin, ibuprofen, naproxen, and naproxen sodium are examples of NSAIDs. They are often the first type of medication doctors prescribe for juvenile arthritis. All NSAIDs work similarly by blocking substances called prostaglandins that add to inflammation and pain. However, each NSAID is a different chemical, and each has a slightly different effect on the body. For unknown reasons, some children seem to respond better to one NSAID than another. NSAIDs should only be used at the lowest dose possible for the shortest time needed.
You can buy some NSAIDs over the counter, while several others, including a subclass called COX-2 inhibitors, need a prescription.
All NSAIDs can have significant side effects, so consult your child’s doctor before giving any of them. Your child’s doctor should monitor your child if he or she takes NSAIDs regularly to control juvenile arthritis.
Side effects of NSAIDs include stomach problems; skin rashes; high blood pressure; fluid retention; and liver, kidney, and heart problems. The longer a person uses NSAIDs, the more likely he or she is to have side effects, ranging from mild to serious. Many other medicines cannot be taken when a person is taking NSAIDs because NSAIDs alter the way the body uses or eliminates these other medicines.
Disease-modifying antirheumatic drugs (DMARDs). If NSAIDs do not relieve symptoms of your child’s juvenile arthritis, the doctor may prescribe this type of medication. DMARDs slow the progression of juvenile arthritis, but because they may take weeks or months to relieve symptoms, they often are taken with an NSAID. Although there are many different types of DMARDs, many doctors prescribe one called methotrexate.
Researchers have learned that methotrexate is safe and effective for some children with juvenile arthritis whose symptoms are not relieved by other medications. Because children only need small doses of methotrexate for relief of arthritis symptoms, potentially dangerous side effects rarely occur. The most serious complication can be liver damage, which a doctor can help prevent with regular blood tests and check-ups. Careful monitoring for side effects is important for people taking methotrexate. When side effects are noticed early, the doctor can reduce the dose and eliminate the side effects.
Corticosteroids. If your child has very severe juvenile arthritis, stronger medicines may be needed to stop serious symptoms, such as inflammation of the sac around the heart (pericarditis). Corticosteroids, such as prednisone, may be added to the treatment plan to control severe symptoms. This medication can be given by IV (intravenous), mouth, or injection directly into a joint. Corticosteroids are powerful anti-inflammatory medicines. Corticosteroids can interfere with your child’s normal growth and can cause other side effects, such as a round face, weakened bones, and an increased chance of having infections. Once the medication controls severe symptoms, the doctor will reduce the dose gradually and, in time, stop it completely. It can be dangerous to stop taking corticosteroids suddenly. Carefully follow the doctor’s instructions about how to take or reduce the dose. For inflammation in one or just a few joints, injecting a corticosteroid compound into the affected joint or joints can often bring quick relief without the systemic side effects of oral or IV medication.
Biologic agents. If your child has received little relief from other medications, he or she may be given one of a newer class of medications called biologic response modifiers, or biologic agents. These are based on compounds made by living cells. Tumor necrosis factor (TNF) inhibitors are biologic agents that work by blocking the actions of TNF, a naturally occurring protein in the body that helps cause inflammation. Other biologic agents block other inflammatory proteins, such as interleukin-1 or immune cells called T cells. Different biologics tend to work better for the different subtypes of the disease.
All medicines can have side effects. Some medicines and side effects are mentioned in this publication. Some side effects may be more severe than others. You should review the package insert that comes with your medicine and ask your child’s health care provider or pharmacist if you have any questions about the possible side effects.
- Other Treatments
Physical therapy. A regular, general exercise program is an important part of a child’s treatment plan. Exercise can help to maintain muscle tone and preserve and recover the range of motion of the joints. A physiatrist (rehabilitation specialist) or a physical therapist can design an appropriate exercise program for your child. The specialist also may recommend using splints and other devices to help maintain normal bone and joint growth.
Complementary and alternative therapies. Many adults seek alternative ways of treating arthritis, such as special diets, supplements, acupuncture, massage, or even magnetic jewelry or mattress pads. Research shows that increasing numbers of children are using alternative and complementary therapies as well.
Although there is little research to support many alternative treatments, some people seem to benefit from them. If your child’s doctor feels the approach has value and is not harmful, you can incorporate it into the treatment plan. However, do not neglect regular health care or treatment of serious symptoms.
Osteoarthritis
Osteoarthritis is the most common type of arthritis and is seen especially among older people. It is sometimes called degenerative joint disease.
Osteoarthritis initially affects the smooth cartilage lining of the joint. This makes movement more difficult than usual, leading to pain and stiffness.
Once the cartilage lining starts to roughen and thin out, the tendons and ligaments have to work harder. This can cause swelling and the formation of bony spurs, called osteophytes.
Severe loss of cartilage can lead to bone rubbing on bone, altering the shape of the joint and forcing the bones out of their normal position.
The most commonly affected joints are those in the:
- hands
- spine
- knees
- hips
People with osteoarthritis usually have joint pain and stiffness. The most commonly affected joints are in the hands (ends of the fingers and thumbs), neck, lower back, knees, and hips. Unlike some other forms of arthritis, osteoarthritis does not affect the skin, lungs, eyes, or blood vessels. It can also occur in only one joint or can affect a joint on one side of the body much more severely.
Osteoarthritis affects each person differently. For some people, osteoarthritis is relatively mild and interferes little with day-to-day life. For others, it causes significant pain and disability. Joint damage usually develops gradually over years, although it could worsen quickly in some people.
What happens in osteoarthritis?
Osteoarthritis damages cartilage, the tissue that covers the ends where two bones meet to form a joint. This allows the bones to rub together, causing pain, swelling, and loss of joint motion. Over time, the joint may lose its normal shape. Also, small bone growths, called osteophytes or bone spurs, may grow on the edges of the joint. Bits of bone or cartilage can also break off and float inside the joint space. This causes more pain and damage.
Who gets osteoarthritis?
Osteoarthritis becomes more common with age. However, younger people can also develop it, usually as the result of a joint injury, an abnormal joint structure, or a genetic defect in joint cartilage.
Before age 45, more men than women have osteoarthritis. After age 45, it is more common in women. It is also more likely to occur in people who are overweight and in those with jobs that stress particular joints.
Osteoarthritis causes
Osteoarthritis usually happens gradually over time. Some things that might make it more likely include:
- Being overweight.
- Getting older.
- Joint injury.
- Joints that are not properly formed.
- A genetic defect in joint cartilage.
Osteoarthritis symptoms
Early in the disease, your joints may ache after physical work or exercise. Later on, joint pain may become more persistent. You may also experience joint stiffness, especially when you first wake up in the morning or have been in one position for a long time.
Joints often affected by osteoarthritis include:
- Hands: If your mother or grandmother has or had osteoarthritis in their hands, you’re at an increased risk of having it too. Women are more likely than men to have osteoarthritis in the hands. For most women, it develops after menopause.
- Knees: Stiffness, swelling, and pain in the knees can make it hard to walk, climb, and get in and out of chairs and bathtubs. Osteoarthritis in the knees can lead to disability.
- Hips: You might feel pain and stiffness in the hip joint or in the groin, inner thigh, buttocks, or even knees. Moving and bending may be limited, making daily activities such as dressing and putting on shoes a challenge.
- Spine: You may feel stiffness and pain in the neck or lower back. In some cases, arthritis-related changes in the spine can cause pressure on the nerves where they exit the spinal column, resulting in weakness, tingling, or numbness of the arms and legs. In severe cases, this can even affect bladder and bowel function.
Osteoarthritis treatment
Treatment for osteoarthritis can include medications or surgery to reduce pain and improve functioning.
Medications commonly used in treating osteoarthritis include:
- Over-the-counter pain relievers such as acetaminophen.
- Nonsteroidal anti-inflammatory drugs (NSAIDs) to treat pain and inflammation. Ibuprofen and naproxen sodium, are available over the counter, whereas other NSAIDS are available by prescription only.
- Creams, rubs or sprays that are applied to the skin over sore joints to relieve pain.
- Prescription opioid pain relievers are sometimes prescribed when over-the-counter medications don’t work or a person may not be able to take NSAIDs.
- Corticosteroids are strong inflammation-fighting drugs that can be injected into the joint to temporarily relive pain. This type of treatment is usually not recommended for more than two to four treatments per year. These types of drugs are not typically given by mouth to treat osteoarthritis, unless treating inflammatory flares.
- Hyaluronic acid substitutes (viscosupplements) are injected into the knee to replace a normal component of the joint involved in lubrication and nutrition.
Surgery may be a factor after considering a variety of factors, including your age, occupation, level of disability, pain intensity, and the degree to which arthritis interferes with your lifestyle. Surgeries can include one or more of the following:
- Arthroscopic debridement: Removal of loose pieces of bone and cartilage from the joint.
- Osteotomy: Repositioning of bones.
- Joint resurfacing: Smoothing out bones.
- Prostheses are artificial joints that replace affected joints. The artificial joints can be made from metals, high-density plastic, or ceramic material. Artificial joints can last 10 to 15 years or longer. In some cases, your surgeon may replace only the damaged part of the knee joint, leaving undamaged parts of the joint in place.
Transcutaneous electrical nerve stimulation (TENS) directs mild electric pulses to nerve endings that lie beneath the skin in the painful area. It seems to work by blocking pain messages to the brain and by changing pain perception.
Alternative therapies for osteoarthritis can include:
- Massage can increase blood flow and bring warmth to a stressed area. However, arthritis-stressed joints are sensitive, so the therapist must be familiar with the problems of the disease.
- Acupuncture uses thin needles to relieve pain and restore health. Scientists think the needles stimulate the release of natural, pain-relieving chemicals produced by the nervous system.
Psoriatic Arthritis
Psoriatic arthritis is a form of arthritis (joint inflammation) that can occur in people who have psoriasis (scaly red and white skin patches) 18.
What happens in psoriatic arthritis?
Psoriatic arthritis affects the joints, and areas where muscles and ligaments attach to bone. Typically, skin disease precedes the arthritis, sometimes by several years. In some cases, arthritis occurs first.
The joints most commonly affected are:
- The outermost joints of the fingers or toes.
- Wrists.
- Knees.
- Ankles.
- Lower back.
Who gets psoriatic arthritis?
Anyone can be affected by psoriatic arthritis, but certain risk factors are associated with a greater risk for the disease:
- Race: Psoriatic arthritis is more common in Caucasians than African Americans or Asian Americans.
- Age: The disease typically begins between the ages of 30 and 50, but can begin in childhood.
Psoriatic arthritis causes
No one knows what causes psoriatic arthritis. People with the condition often have a family member with psoriasis or arthritis, suggesting that genetics are involved. In people with the disease gene, an infection may activate the immune system to trigger the development of psoriatic arthritis. This indicates that environment is also involved.
Psoriatic arthritis symptoms
Symptoms of psoriatic arthritis include:
- Joint pain and swelling that may come and go and may be accompanied by redness and warmth.
- Tenderness where muscles or ligaments attach to the bones, particularly the heel and bottom of the foot.
- Inflammation of the spinal column, called spondylitis, which can cause pain and stiffness in the neck and lower back.
- Morning stiffness.
- Reduced range of motion of the joints.
- Painful, sausage-like swelling of the fingers and/or toes.
- Thickness and reddening of the skin with flaky, silver white patches called scales.
- Pitting of the nails or separation from the nail bed.
- Tiredness.
- Pink eye, inflammation, or infection of the membrane lining the eyelid and part of the eyeball.
Psoriatic arthritis treatment
Treatment for psoriatic arthritis depends on its severity. Milder forms of the disease may be treated by:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) are used to treat pain and inflammation. Ibuprofen and naproxen sodium, are available over the counter, whereas other NSAIDS are available by prescription only.
- Corticosteroids, strong inflammation-fighting drugs, may be injected directly into the affected joint(s).
Forms of the disease that are persistent or affect multiple joints may be treated by:
- Disease-modifying anti-rheumatic drugs (DMARDs) that slow or stop the immune system from attacking the joints and causing damage.
- Anti-tumor necrosis factor (TNF) agents.
Reactive Arthritis
Reactive arthritis is a type of spondyloarthritis, a group of disorders that can cause inflammation throughout the body (especially in the knees, feet, toes, hips and ankles). Reactive arthritis is associated with inflammation of the joints, eyes, and urinary tract and its associated genital structures. These symptoms may occur alone, together, or not at all. Any of these symptoms may be so mild that you may not notice them.
Reactive arthritis usually develops after you’ve had an infection, particularly a sexually transmitted infection or food poisoning.
The symptoms of reactive arthritis usually last several months, it clears up within a few months and causes no long-term problems. The symptoms can return or develop into a long-term disease in a small percentage of people.
Men and women of any age can get it, but it’s more common in men, and people aged between 20 and 40.
Reactive arthritis is not contagious; that is, a person with the disorder cannot pass the arthritis on to someone else. However, the bacteria that can trigger reactive arthritis can be passed from person to person.
Most people with reactive arthritis recover fully from the initial flare of symptoms. They may have mild arthritis symptoms that last up to a year, although symptoms don’t usually interfere with daily activities. Some people will have long-term, mild arthritis. A few patients will have long-term, severe arthritis that is difficult to control with treatment and may cause joint damage.
Some patients will re-develop symptoms, such as back pain and arthritis, after the initial flare has disappeared. These relapses may be caused by reinfection.
What happens in reactive arthritis?
In many patients, reactive arthritis is triggered by an infection in the bladder, urethra, or vagina that is often transmitted through sexual contact (sexually transmitted infection). Another form of reactive arthritis is caused by an intestinal infection from eating food or handling substances that are contaminated with bacteria.
Who gets Reactive arthritis?
Men are nine times more likely than women to develop reactive arthritis caused by sexually acquired infections. However, women and men are equally likely to develop reactive arthritis as a result of food-borne infections. Women with reactive arthritis often have milder symptoms than men.
Reactive arthritis symptoms
Symptoms of reactive arthritis may be so mild that you do not notice them. They can come and go over a period of weeks or months. In a few people, symptoms can turn into a long-term disease.
Symptoms of reactive arthritis can include:
- Joint swelling and pain.
- Inflammation of the urinary and genital tract – causing pain when peeing, or discharge from the penis or vagina
- Redness and swelling of the eyes – causing eye pain, sticky discharge, conjunctivitis and, rarely, inflammation of the eye (iritis)
- Mouth sores and skin rashes.
See an eye specialist or go to emergency room as soon as possible if one of your eyes becomes very painful and the vision becomes misty. This could be a symptom of iritis – and the sooner you get treatment, the more successful it is likely to be.
Most people will not get all the above symptoms. They can come on suddenly but usually start to develop a few days after you get an infection somewhere else in your body.
Reactive arthritis causes
In many patients, reactive arthritis is triggered by a bacterial infection in the bladder, urethra, or vagina that is often transmitted through sexual contact. Another form of reactive arthritis is caused by an intestinal infection from eating food or handling substances that are contaminated with bacteria. Reactive arthritis typically begins within two to four weeks after infection.
Doctors do not know exactly why some people exposed to these bacteria develop reactive arthritis and others do not. One gene, human leukocyte antigen (HLA) B27, increases a person’s chance of developing reactive arthritis. However, inheriting the HLA B27 gene does not necessarily mean you will get reactive arthritis.
A person with the disorder cannot pass the arthritis on to someone else. However, the bacteria that can trigger reactive arthritis can be passed from person to person.
Reactive arthritis diagnosis
Although there is no single test for reactive arthritis, your doctor may do the following to diagnosis you with the condition:
- Medical history to learn about your symptoms and any previous medical problems or infections.
- Blood tests to:
- Detect the genetic factor HLA B27. A positive result does not always mean that you the disorder.
- Confirm inflammation somewhere in the body.
- Rule out other conditions.
- Take samples from the throat, urethra, cervix, urine, stool, or joints to test for bacteria.
- X-rays to help diagnose reactive arthritis and to rule out other causes of arthritis.
Reactive arthritis treatment
Although there is no cure for reactive arthritis, certain medications can relieve symptoms of the disorder:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) are used to treat pain and inflammation. Ibuprofen and naproxen sodium are available over the counter, whereas other NSAIDS are available by prescription only.
- Corticosteroids, strong inflammation-fighting drugs, may be applied directly on skin ulcers, or injected into a joint to temporarily relieve pain. Because they are potent drugs, your doctor will seek the lowest dose required to achieve the desired benefit.
- Antibiotics eliminate the bacterial infection that triggered reactive arthritis.
- Immunosuppressive medicines or biologics to stop the immune system from attacking the tissues.
Rheumatoid Arthritis
Rheumatoid arthritis, is an inflammatory disease that causes pain, swelling, stiffness, and loss of function in the joints. It occurs when the immune system, which normally helps protect the body from infection and disease, attacks the membrane lining the joints.
Rheumatoid arthritis is different from other kinds of arthritis in several ways. For example:
- Rheumatoid arthritis generally occurs in a symmetrical pattern, meaning that if one knee or hand is involved, the other one also is.
- Rheumatoid arthritis often affects the wrist joints and the finger joints closest to the hand.
- Rheumatoid arthritis can also affect other parts of the body besides the joints, such as the heart, lungs, blood, nerves, eyes, and skin.
- People with rheumatoid arthritis may have fatigue, occasional fevers, and a loss of appetite.
Fortunately, current treatments allow most people with the disease to lead active and productive lives. In recent years, research has led to a new understanding of rheumatoid arthritis, which may result in even better ways to treat the disease.
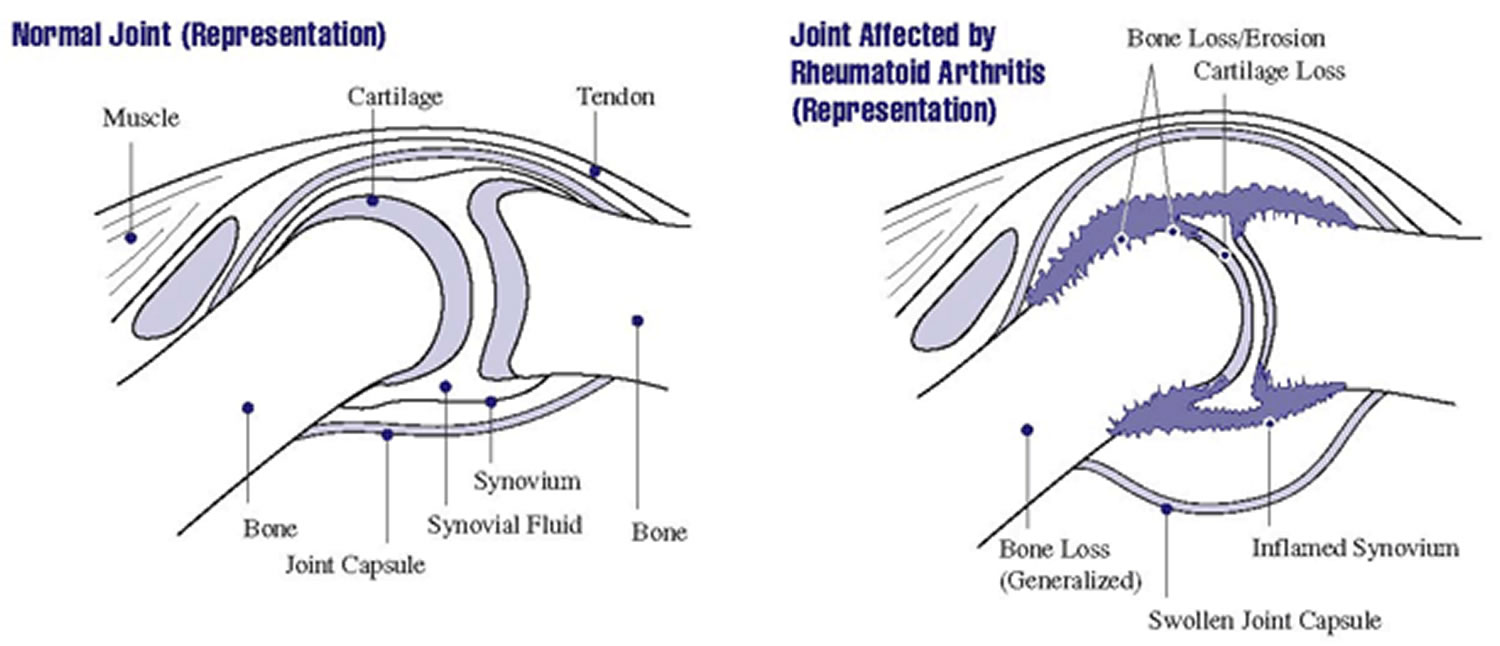
What happens in rheumatoid arthritis?
Rheumatoid arthritis is an autoimmune disease (auto means self). The immune system attacks joint tissues for unknown reasons. Rheumatoid arthritis occurs when:
- White blood cells in the immune system travel to tissue that surrounds the joint, called synovium, and cause inflammation.
- The normally thin synovium becomes thick, making the joint swollen, red, painful, and sometimes warm to the touch.
- As rheumatoid arthritis progresses, the inflamed synovium invades and destroys the cartilage and bone within the joint.
- The surrounding muscles, ligaments, and tendons that support and stabilize the joint become weak and don’t work normally. This may cause the bone and cartilage to break down. This leads to pain and joint damage.
- People with rheumatoid arthritis can also develop problems with other tissues and organs in their body.
Researchers now believe that rheumatoid arthritis begins to damage the bones within the joint during the first year or two that a person has the disease. This is one reason why early diagnosis and treatment are so important.
Who gets Rheumatoid arthritis?
About 1.5 million people, or about 0.6 percent of the U.S. adult population, have rheumatoid arthritis. Rheumatoid arthritis is more common among certain groups:
- Age: The disease often begins in middle age and is more common in older adults, between 40 and 50 years old. However, older teenagers and young adults may also get the disease. Children and younger teenagers may be diagnosed with juvenile idiopathic arthritis, a condition related to rheumatoid arthritis.
- Sex: Like some other forms of arthritis, rheumatoid arthritis is more common among women than men. About two to three times as many women as men have the disease.
- Race/Ethnicity: Rheumatoid arthritis occurs in all races and ethnic groups.
Rheumatoid arthritis symptoms
Symptoms of rheumatoid arthritis, which can range from mild to severe, include:
- Tender, warm, swollen joints.
- Swollen joints on both sides of the body, such as in both your right and left wrist.
- Swollen joints often in the wrist and finger joints closest to the hand.
- Swollen joints sometimes in other joints, including the neck, shoulders, elbows, hips, knees, ankles, and feet.
- Feeling tired and having low energy.
- Fevers.
- Pain and stiffness lasting for more than 30 minutes in the morning or after a long rest.
- Symptoms that last for many years.
Rheumatoid arthritis causes
Scientists still do not know exactly what causes the immune system to turn against the body’s own tissues in rheumatoid arthritis. Research over the last few years has begun to piece together the factors involved. These include:
Genetic (inherited) factors: Scientists have discovered that certain genes known to play a role in the immune system are associated with rheumatoid arthritis. However, some people who have these particular genes never develop the disease. This suggests that genes are not the only factor in the development of rheumatoid arthritis. What is clear, however, is that more than one gene is involved in determining whether a person develops rheumatoid arthritis and how severe the disease will become.
Environmental factors: Many scientists think that something must occur to trigger the disease process in people whose genetic makeup puts them at risk for rheumatoid arthritis. Many factors have been suggested, but a specific one has not been confirmed.
Other factors: Some scientists also think that hormonal factors, such as shortages or changes in certain sex hormones, may play a role when genetic and environmental factors also are involved. Scientists believe this because:
- Women are more likely to develop rheumatoid arthritis than men.
- The disease may improve during pregnancy and flare after pregnancy.
- Breastfeeding may worsen the disease.
We do not know all the answers, but we do know that rheumatoid arthritis develops from an interaction of many factors. Researchers are trying to understand these factors and how they work together.
Rheumatoid arthritis diagnosis
Rheumatoid arthritis can be difficult to diagnose in its early stages for several reasons:
- There is no single test for the disease.
- Symptoms differ from person to person and can be more severe in some people than in others.
- Symptoms can be similar to those of other types of arthritis and joint conditions, and it may take some time for other conditions to be ruled out.
- The disease develops over time, and only a few symptoms may be present in the early stages.
As a result, doctors use a variety of the following tools to diagnose the disease and to rule out other conditions.
Medical History
The doctor will begin by asking you to describe your symptoms, when and how they started, and how they have changed over time. The doctor will also ask about any other medical problems you and close family members have and about any medications you’re taking. Answers to these questions can help the doctor make a diagnosis and understand the impact the disease has on your life.
Physical Examination
The doctor will:
- Check your reflexes and general health, including muscle strength.
- Examine bothersome joints and watch how you walk, bend, and carry out activities of daily living.
- Look at your skin for a rash.
- Listen to your chest for signs of inflammation in the lungs.
Laboratory Tests
A number of lab tests may be useful in confirming a diagnosis of rheumatoid arthritis. Some of the common tests include:
- Rheumatoid factor (RF): This blood test checks for RF, an antibody most people with rheumatoid arthritis eventually have in their blood. (An antibody is a special protein made by the immune system that normally helps fight invaders in the body.) Not all people with rheumatoid arthritis test positive for RF, and some people test positive for RF but never develop the disease. RF also can be positive in some other diseases. However, a positive RF in a person who has symptoms consistent with rheumatoid arthritis can be useful in confirming a diagnosis. Also, high levels of RF are associated with more severe rheumatoid arthritis.
- Anti-CCP antibodies: This blood test detects antibodies to cyclic citrullinated peptide (anti-CCP). This test is positive in most people with rheumatoid arthritis and can even be positive years before rheumatoid arthritis symptoms develop. When used with the RF, this test’s results are very useful in confirming a rheumatoid arthritis diagnosis.
- Others: Other common blood tests include:
- White blood cell count.
- Blood test for anemia, which is common in rheumatoid arthritis.
- Erythrocyte sedimentation rate (often called the sed rate), which measures inflammation in the body.
- C-reactive protein, another common test for inflammation that is useful both in making a diagnosis and monitoring disease activity and response to anti-inflammatory therapy.
Imaging Tests
Doctors use x-rays to see the degree of joint damage. They are not useful in the early stages of rheumatoid arthritis before damage is evident. Doctors may use them to rule out other causes of joint pain. X-rays may also be used later to monitor the progression of the disease. Magnetic resonance imaging (MRI) and ultrasound may be useful in identifying the early stages of rheumatoid arthritis and can help determine the severity of the disease.
Rheumatoid arthritis treatment
Doctors use a variety of approaches to treat rheumatoid arthritis. They may be used in combination and at different times during the course of the disease. Your doctor will choose treatments based on your situation.
No matter which treatment is chosen, the goals are the same:
- Relieve pain.
- Reduce inflammation.
- Slow down or stop joint damage.
- Improve well-being and ability to function.
To treat rheumatoid arthritis, doctors may suggest:
- Medications.
- Surgery.
- Routine monitoring and ongoing care.
- Complementary therapies.
Medications
Most people who have rheumatoid arthritis take medications. Studies show that early treatment with powerful drugs and drug combinations instead of one medication alone may be more effective in reducing or preventing joint damage than beginning with aspirin or other pain relievers. If you have persistent rheumatoid arthritis symptoms, see a doctor familiar with the disease and its treatment to reduce the risk of damage.
Many of the drugs used to treat rheumatoid arthritis reduce the inflammation that can cause pain and joint damage. However, inflammation is also one way the body fights infection and disease. But the level of risk is hard to judge because infections and cancer can occur in people with rheumatoid arthritis who are not on treatment. It is important to talk with your doctor about these risks.
Pain Relief and Anti-Inflammatory Drugs
Your doctor may prescribe some medications (analgesics) that only help with pain relief. Others, such as corticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs), can reduce inflammation.
Disease-Modifying Anti-Rheumatic Drugs (DMARDS)
DMARDs may to slow the course of the disease. Common DMARDs your doctor may prescribe include:
- Hydroxychloroquine.
- Leflunomide.
- Methotrexate.
- Sulfasalazine.
Other DMARDs, called biologic response modifiers, may be used if your disease is more severe. These are genetically engineered medications that help reduce inflammation and damage to the joints by interrupting the inflammatory process. Currently, several biologic response modifiers are approved for rheumatoid arthritis, including:
- Abatacept.
- Adalimumab.
- Anakinra.
- Certolizumab.
- Etanercept.
- Golimumab.
- Infliximab.
- Rituximab.
- Tocilizumab.
Another DMARD, tofacitinib, is from a new class of drugs called jak kinase (JAK) inhibitors. It fights inflammation from inside the cell.
Surgery
The primary purpose of surgery is to reduce pain, improve the affected joint’s function, and improve your ability to perform daily activities.
Surgery is not for everyone. Talk with your doctor and together decide what is the right choice for you. Discuss:
- Your overall health.
- The condition of the joint or tendon that will be operated on.
- The reason for, and the risks and benefits of the surgery.
Routine Monitoring and Ongoing Care
Regular medical care is important to monitor the course of the disease, determine the effectiveness and any negative effects of medications, and change therapies as needed.
Monitoring typically includes regular visits to the doctor. It also may include blood, urine, and other lab tests and x-rays.
Good communication between you and your doctor is necessary for effective treatment. Talking to the doctor regularly can help ensure that you receive:
- Necessary exercise and pain management programs.
- Necessary and appropriate medications.
- Information about surgical options if necessary.
Another factor to discuss with your doctor is the risk of osteoporosis, which is a condition in which bones become weakened and fragile. Having rheumatoid arthritis increases your risk of developing osteoporosis, particularly if you take corticosteroids. You may want to discuss with your doctor the potential benefits of calcium and vitamin D supplements or other osteoporosis treatments.
Complementary Therapies
Special diets, vitamins, and other complementary therapies are sometimes suggested to treat rheumatoid arthritis.
Research shows that some of these approaches, such as taking fish oil supplements, may help reduce inflammation. However, few, if any controlled scientific studies have been conducted on complementary approaches, and some studies have found no definite benefit to these therapies.
As with any therapy, you should discuss the benefits and risks with your doctor before beginning any complementary or new type of therapy. However, it is important not to neglect regular health care.
Systemic Lupus Erythematosus (Lupus)
Systemic lupus erythematosus (lupus) is a disease that can damage many parts of the body, such as the joints, skin, kidneys, heart, lungs, blood vessels, and brain. You can’t catch lupus from another person.
If you have lupus you will have periods of illness (flares) and periods of wellness (remission).
What happens in lupus?
Lupus occurs when the immune system, which normally helps protect the body from infection and disease, attacks different parts of the body.
Who gets systemic lupus erythematosus (lupus)?
We know that many more women than men have systemic lupus erythematosus (lupus). Lupus is more common in African American women than in Caucasian women and is also more common in women of Hispanic, Asian, and Native American descent. African American and Hispanic women are also more likely to have active disease and serious organ system involvement. In addition, lupus can run in families, but the risk that a child or a brother or sister of a patient will also have lupus is still quite low.
Although systemic lupus erythematosus (lupus) usually first affects people between the ages of 15 and 45 years, it can occur in childhood or later in life as well.
Systemic lupus erythematosus (lupus) causes
No one completely understands what causes systemic lupus erythematosus (lupus). Studies suggest that a number of different genes may determine your risk for developing the disease.
Some environmental factors also appear to play a role in lupus. In particular, scientists are studying the effects of sunlight, stress, hormones, cigarette smoke, certain drugs, and viruses.
Systemic lupus erythematosus (lupus) symptoms
Each person with systemic lupus erythematosus (lupus) has slightly different symptoms that can range from mild to severe. You may have symptoms in only one or in many parts of your body. Symptoms may also come and go over time.
Some of the most common symptoms of lupus include:
- Painful or swollen joints (arthritis).
- Unexplained fever.
- Extreme fatigue.
- Red rashes, most often on the face.
- Chest pain upon deep breathing.
- Hair loss.
- Sensitivity to the sun.
- Mouth sores.
- Pale or purple fingers and toes from cold and stress.
- Swollen glands.
- Swelling in the legs or around the eyes.
Other symptoms could include:
- Anemia (a decrease in red blood cells).
- Kidney inflammation, which typically requires drug treatment to prevent permanent damage.
- Headaches, dizziness, depression, confusion, or seizures if the disease affects the central nervous system.
- Inflammation of the blood vessels.
- Decreased number of white blood cells or platelets.
- Increased risk of blood clots.
- Inflammation of the heart or the lining that surrounds it.
- Heart valve damage.
Systemic lupus erythematosus (lupus) diagnosis
Diagnosing systemic lupus erythematosus (lupus) can be difficult and may take months or even years. Although there is no single test for lupus, your doctor may do the following to diagnosis you with the condition:
- Ask you about your medical history.
- Give you a physical exam.
- Take samples of blood, skin, kidney, or urine for laboratory tests. The most useful tests look for certain antibodies in the blood.
Systemic lupus erythematosus (lupus) treatment
Treatments for systemic lupus erythematosus (lupus) have improved dramatically in recent decades, giving doctors more choices in how to manage the disease. Because some treatments may cause harmful side effects, you should immediately report any new symptoms to your doctor. You should also talk to your doctor before stopping or changing treatments.
Treatments for lupus include:
- Medications:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) are used to treat joint or chest pain or fever. Ibuprofen and naproxen sodium are available over the counter, whereas other NSAIDS are available by prescription only.
- Antimalarials prevent and treat malaria, but doctors have found that they also are useful for treating fatigue, joint pain, skin rashes, and inflammation of the lungs caused by lupus. These drugs may also prevent flares from recurring.
- Corticosteroids, strong inflammation-fighting drugs, may be taken by mouth, in creams applied to the skin, by injection, or by intravenous (IV) infusion (dripping the drug into the vein through a small tube). Because they are potent drugs, your doctor will seek the lowest dose required to achieve the desired benefit.
- Immunosuppressives restrain an overactive immune system and may be prescribed if your kidneys or central nervous systems are affected by lupus. These drugs may be given by mouth or by IV infusion. The risk for side effects increases with the length of treatment.
- B-lymphocyte stimulator (BlyS)-specific inhibitors reduce the number of abnormal B cells thought to be a problem in lupus.
- Alternative and complementary therapies may improve symptoms, although research has not shown whether they help treat the disease. Examples include:
- Special diets.
- Nutritional supplements.
- Fish oils.
- Ointments and creams.
- Chiropractic treatment.
- Homeopathy.
In many cases you may need to take medications to treat problems related to lupus, such as high cholesterol, high blood pressure, or infection.
Septic arthritis (infectious arthritis)
Septic arthritis (also called infectious arthritis) is painful infection of a joint due to a bacterial, viral or fungal infection 19. The Septic arthritis infection can come from germs that travel through your bloodstream from another part of your body. Septic arthritis can also occur when a penetrating injury delivers germs directly into the joint.
The most common route of entry into the joint is hematogenous (bloodstream) spread during bacteremia (presence of bacteria in the blood) 20. Pathogens may also enter through direct inoculation (e.g., arthrocentesis, arthroscopy, trauma) or contiguous spread from local infections (e.g., osteomyelitis, septic bursitis, abscess) 21. Once in the joint, microorganisms are deposited in the synovial membrane, causing an acute inflammatory response 22. Inflammatory mediators and pressure from large effusions lead to the destruction of joint cartilage and bone loss 23.
Infants and older adults are most likely to develop septic arthritis. Knees are most commonly affected, but septic arthritis also can affect hips, shoulders and other joints. The infection can quickly and severely damage the cartilage and bone within the joint, so prompt treatment is crucial.
Septic arthritis causes
Septic arthritis develops when bacteria or other tiny disease-causing organisms (virus & fungi) spread through the blood to a joint. Septic arthritis can develop when an infection, such as a skin infection or urinary tract infection, spreads through your bloodstream to a joint. Less commonly, a puncture wound, drug injection, or surgery in or near a joint can give the microorganisms entry into the joint space. Joints that are commonly affected are the knee and hip.
The lining of your joints (synovium) has little ability to protect itself from infection. Your body’s reaction to the infection — including inflammation that can increase pressure and reduce blood flow within the joint — contributes to the damage.
Clinical presentations can be broadly grouped into three categories: nongonococcal, gonococcal, and other (e.g., Lyme disease, mycobacterial, fungal).
- Most cases of acute septic arthritis are caused by staphylococcus (40 percent) or streptococcus bacteria (28 percent) 24.
- Bacterial infection with Staphylococcus aureus (staph) is the most common cause. Staph commonly lives on even healthy skin.
Septic arthritis can also be due to the bacteria that cause gonorrhea [a common sexually transmitted infection 25], which is caused by the bacteria Neisseria gonorrhoeae. Gonococcal arthritis is a complication of gonorrhea. Gonococcal arthritis affects women more often than men. It is most common among sexually active teen girls. Any type of sex can spread gonorrhea. You can get it through contact with the mouth, vagina, penis, or anus. Gonorrhea is the second most commonly reported communicable disease. Approximately 330,000 cases occur in the US each year.
Septic arthritis symptoms
Symptoms usually come on quickly. Septic arthritis typically causes extreme joint pain and difficulty using the affected joint (usually in just one joint), which gets worse with movement. The joint could be swollen, red and warm, and you might have a fever.
Symptoms in newborns or infants:
- Crying when infected joint is moved (for example, during diaper changes)
- Fever
- Not able to move the limb with the infected joint (pseudoparalysis)
- Fussiness
Symptoms in children and adults:
- Not able to move the limb with the infected joint (pseudoparalysis)
- Severe joint pain
- Joint swelling
- Joint redness
- Fever
Chills may occur, but are uncommon.
Septic arthritis diagnosis
The health care provider will examine the joint and ask about the symptoms.
The following tests typically help diagnose septic arthritis:
- Joint fluid analysis. Infections can alter the color, consistency, volume and makeup of the fluid within your joints. A sample of this fluid can be withdrawn from your affected joint with a needle. Laboratory tests can determine what organism is causing your infection, so your doctor will know which medications to prescribe.
- Blood tests. These can determine if there are signs of infection in your blood. A sample of your blood is removed from a vein with a needle.
- Imaging tests. X-rays and other imaging tests of the affected joint can assess damage to the joint.
There are no data on imaging studies that are pathognomonic for acute septic arthritis. Plain films establish a baseline and may detect fractures, chondrocalcinosis, or inflammatory arthritis. Ultrasonography is more sensitive for detecting effusions, particularly in difficult-to-examine joints, such as the hip 26. Magnetic resonance imaging findings that suggest an acute intraarticular infection include the combination of bone erosions with marrow edema 27. Imaging may allow guided arthrocentesis, particularly in difficult-to-examine joints (e.g., hip, sacroiliac, costochondral).
Septic arthritis treatment
Antibiotics are used to treat the infection.
Removing the infected joint fluid is crucial. Drainage methods include:
- Needle. In some cases, your doctor can withdraw the infected fluid with a needle inserted into the joint space.
- Scope procedure. In arthroscopy, a flexible tube with a video camera at its tip is placed in your joint through a small incision. Suction and drainage tubes are then inserted through small incisions around your joint.
- Open surgery. Some joints, such as the hip, are more difficult to drain with a needle or arthroscopy, so an open surgical procedure might be necessary.
Resting, raising the joint above heart level, and using cool compresses may help relieve pain. After the joint starts to heal, exercising it can help speed recovery.
Antibiotics
To select the most effective medication, your doctor must identify the microbe causing your infection. Antibiotics are usually given through a vein in your arm at first. Later, you may be able to switch to oral antibiotics.
Typically, treatment lasts from two to six weeks. Antibiotics carry a risk of side effects, including nausea, vomiting and diarrhea. Allergic reactions also can occur. Ask your doctor about what side effects to expect from your medication.
Arthritis symptoms
The most common signs and symptoms of arthritis involve the joints and each person’s symptoms may vary . Depending on the type of arthritis you have, your signs and symptoms may include:
- Pain in 1 or more joints that doesn’t go away, or comes back
- Warmth and redness in 1 or more joints
- Swelling in 1 or more joints
- Stiffness in 1 or more joints
- Trouble moving 1 or more joints in a normal way
- Redness
- Decreased range of motion
Some people also get other problems outside their joints. Other common symptoms include:
- Tiredness
- Weight loss
- Feeling unwell
These symptoms can look like other health conditions. Always see your doctor for a diagnosis.
Arthritis causes
The cause of arthritis depends on the type of arthritis you have. The two main types of arthritis — osteoarthritis and rheumatoid arthritis — damage joints in different ways. Osteoarthritis is caused by the wear and tear of the joint over time or because of overuse. Rheumatoid arthritis, lupus, and scleroderma are caused by the body’s immune system attacking the body’s own tissues. Gout is caused by the buildup of uric acid crystals in the joints. Some forms of arthritis can be linked to genes. People with genetic marker HLA-B27 have a higher risk of ankylosing spondylitis. Arthritis caused by an infection is called ‘reactive arthritis’. It’s very difficult to diagnose and can develop at any age, but is more commonly seen in younger people. Reactive arthritis can last between a few weeks to 6 months. For some other forms of arthritis, the cause is not known.
Arthritis risk factors
A risk factor is anything that increases your chance of getting a disease such as arthritis. But having a risk factor, or even many, does not mean that you will get the disease. And some people who get the disease may not have any known risk factors.
Researchers have found several risk factors that might increase a person’s chance of developing arthritis.
Risk factors for arthritis include:
- Family history. Some types of arthritis run in families, so you may be more likely to develop arthritis if your parents or siblings have the disorder.
- Genetics and inherited traits. People born with specific genes are more likely to develop certain types of arthritis, such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and ankylosing spondylitis. These genes are called HLA (human leukocyte antigen) class 2 genotypes. These genes can also make your arthritis worse. Experts do not know why people with these genes are at higher risk for developing arthritis or why it can make their arthritis worse.
- Age. The risk of many types of arthritis — including osteoarthritis, rheumatoid arthritis and gout — increases with age.
- Your sex. Women are more likely than men to develop rheumatoid arthritis, while most of the people who have gout, another type of arthritis, are men. Experts don’t know exactly why women are at higher risk for developing most types of arthritis, or why men are at higher risk for developing gout.
- Previous joint injury. People who have injured a joint, perhaps while playing a sport, are more likely to eventually develop arthritis in that joint.
- Overweight and obesity. Carrying excess pounds puts stress on joints, particularly your knees, hips and spine. People with obesity have a higher risk of developing arthritis.
- Smoking. Cigarette smoking increases a person’s risk of developing rheumatoid arthritis (RA) and can make the disease worse. It can also cause other medical problems. Smoking can also make it more difficult to stay physically active, which is an important part of managing rheumatoid arthritis and other types of arthritis.
- Infection. Many microbial agents, like bacteria and viruses, can infect joints and potentially cause the development of some types of arthritis. Reactive arthritis can affect joints after an infection.
- Your job. Work that involves repeated bending or squatting can lead to osteoarthritis of the knee.
Arthritis prevention
You can reduce your risk of getting some types of arthritis by changing risk factors you can control. Risk factors you can control include overweight and obesity, joint injuries, and smoking. But there are some risk factors that can’t be prevented, such as your family history, age or sex.
You can reduce your risk of getting some types of arthritis by:
- Eating a healthy diet.
- Being physically active.
- Maintaining a healthy weight.
- Not drinking too much alcohol.
- Quiting smoking.
Arthritis complications
Arthritis can affect people’s quality of life due to pain and immobility. It can lead to problems with sleep, fatigue, depression and anxiety.
Severe arthritis, particularly if it affects your hands or arms, can make it difficult for you to do daily tasks.
Some types of arthritis also increase the risk of developing other chronic conditions such as lung disease, diabetes and cardiovascular disease. Lack of physical activity due the pain of arthritis can lead to frailty, loss of function, loss of independence and social isolation.
Arthritis of weight-bearing joints can keep you from walking comfortably or sitting up straight. In some cases, joints may gradually lose their alignment and shape.
Arthritis diagnosis
To determine if joint pain and other symptoms are caused by arthritis or a related condition, your doctor will gather information. During the medical history, your doctor will ask questions about your symptoms, general health, family history and habits to better evaluate your situation.
During the physical exam, your doctor will check your joints for swelling, redness and warmth. He or she will also want to see how well you can move your joints.
Depending on the type of arthritis suspected, your doctor may suggest some of the following tests.
- Laboratory tests: The analysis of different types of body fluids can help pinpoint the type of arthritis you may have. Fluids commonly analyzed include blood, urine and joint fluid. To obtain a sample of your joint fluid, your doctor will cleanse and numb the area before inserting a needle in your joint space to withdraw some fluid.
- Imaging. These types of tests can detect problems within your joint that may be causing your symptoms. Examples include:
- X-rays. Using low levels of radiation to visualize bone, X-rays can show cartilage loss, bone damage and bone spurs. X-rays may not reveal early arthritic damage, but they are often used to track progression of the disease.
- Computerized tomography (CT). CT scanners take X-rays from many different angles and combine the information to create cross-sectional views of internal structures. CTs can visualize both bone and the surrounding soft tissues.
- Magnetic resonance imaging (MRI). Combining radio waves with a strong magnetic field, MRI can produce more-detailed cross-sectional images of soft tissues such as cartilage, tendons and ligaments.
- Ultrasound. This technology uses high-frequency sound waves to image soft tissues, cartilage and fluid-containing structures near the joints (bursae). Ultrasound is also used to guide needle placement for joint aspirations and injections.
Laboratory tests
Blood and other lab tests play a critical role in diagnosing and monitoring arthritis. When your doctor needs to confirm an arthritis diagnosis, monitor disease progress, check medication effectiveness or determine if medications are causing potentially dangerous – but not evident – side effects, laboratory tests are ordered.
Most laboratory tests require drawing and testing the blood, but some may involve testing urine, joint fluid or even small pieces of skin or muscle.
Blood tests
If your doctor suspects you have inflammatory arthritis, these are the most common tests used to diagnose as well as monitor the disease:
- Antinuclear antibody (ANA) – Abnormal antibodies (blood proteins) can suggest the presence of lupus, polymyositis, scleroderma, Sjogren’s syndrome, mixed connective tissue disease or rheumatoid arthritis.
- Rheumatoid factor (RF) – Detects and measures the level of an antibody that acts against the blood component gamma globulin. This test is often positive in people with rheumatoid arthritis and negative in people with psoriatic arthritis
- Anti-cyclic citrullinated peptide (anti-CCP) – Looks for the presence of an autoantibody present in about 60-80 percent of people with RA.
- Uric acid – Measures the level of uric acid in the blood helping doctors diagnose gout
- HLA tissue typing – Detects the presence of certain genetic markers to confirm a diagnosis of ankylosing spondylitis or reactive arthritis
- Erythrocyte sedimentation rate (ESR) – Measures how fast red blood cells cling together, fall and settle to help determine the presence of inflammation.
- C-reactive protein (CRP) – Measures body-wide inflammation and may help to diagnose rheumatoid arthritis, psoriatic arthritis or lupus
- Lyme serology – Used to determine the presence of Lyme disease.
Other Lab Tests
- Skin biopsy – A small piece of skin is removed by a doctor. It’s usually done under local anesthetic. The sample is tested in a lab and the results help determine the presence of lupus, vasculitis and psoriatic arthritis.
- Muscle biopsy – A doctor takes the tissue sample from a muscle with a biopsy needle. The sample is reviewed for signs of damage to muscle fibers to help confirm a diagnosis of polymyositis or vasculitis.
- Joint fluid tests – A doctor removes a small amount of fluid from a joint to determine the presence of uric acid and diagnose gout.
Monitoring medication response and side effects
Prescription and over-the-counter medications are often used to treat arthritis, so your doctor will periodically order tests to check for effectiveness and adverse side effects. These include:
- Muscle enzyme (CPK, aldolase) – Muscles damaged by arthritis and inflammation can release enzymes into the blood. This test measures the amount of muscle damage and how well medications reduce the inflammation.
- Creatinine – Used to monitor kidney function in people with lupus or in those taking medications that could affect the kidneys.
- Multibiomarker disease activity (MBDA) – Checks 12 proteins, hormones and growth factors linked to rheumatoid arthritis to determine how aggressive a person’s disease is, how likely a flare may occur if medications are stopped and the drug combinations may work best
- Liver enzymes (aspartate aminotransferase [AST], alanine aminotransferase [ALT], bilirubin, alkaline phosphatase [ALP]) – Measures levels of liver enzymes in the blood and can help determine if there is liver damage.
- Hematocrit (HCT) and hemoglobin (Hgb) – Measures the number and quality of red blood cells. Low counts may suggest medications are causing gastrointestinal bleeding.
- White blood cell count – Measures the level of white blood cells. A low number may suggest that medication is decreasing the supply, hurting the body’s chances of fighting infection.
- Platelet count – Measures the number of platelets that help the blood to clot. A low number could suggest that medication has put you at risk of bleeding heavily.
Checking for comorbidities
People with arthritis are prone to developing other serious chronic diseases, or comorbidities, such as heart disease, diabetes, kidney disease and lung disease. Your doctor may regularly monitor you for these diseases and order blood and other lab tests as part of that monitoring.
Arthritis treatment
Arthritis treatment will depend on your symptoms, your age, and your general health. Arthritis treatment will also depend on what type of arthritis you have, and how severe your arthritis is.
Arthritis treatment focuses on relieving symptoms and improving joint function. It’s important to help keep your joints working by reducing pain and inflammation. You may need to try several different treatments, or combinations of treatments, before you determine what works best for you.
Work on a treatment plan with your healthcare provider that includes medicine and physical therapy.
Home remedies
Work on lifestyle changes that can improve your quality of life. In many cases, arthritis symptoms can be reduced with the following lifestyle changes:
- Weight loss. Excess weight puts extra stress on weight-bearing joints, such as the hips and knees. Losing weight may increase your mobility and limit future joint injury.
- Exercise. Regular exercise may help reduce joint pain and stiffness and can help keep joints flexible. These exercises include swimming, walking, low-impact aerobic exercise, and range-of-motion exercises. Stretching exercises may also help keep the joints flexible. Swimming and water aerobics may be good choices because the buoyancy of the water reduces stress on weight-bearing joints.
- Heat and cold. Heating pads or ice packs may help relieve arthritis pain.
- Assistive devices. Using canes, crutches, shoe inserts, walkers, raised toilet seats, and other assistive devices can help protect joints and improve your ability to perform daily tasks.
- Using adaptive equipment. Reachers and grabbers let you extend your reach and reduce straining. Dressing aids help you get dressed more easily.
- Activity and rest. To reduce stress on your joints, switch between activity and rest. This can help protect your joints and lessen your symptoms.
Medications
The medications used to treat arthritis vary depending on the type of arthritis. Commonly used arthritis medications include:
- Painkillers. These medications help reduce pain, but have no effect on inflammation. An over-the-counter option includes acetaminophen (Tylenol, others). For more-severe pain, opioids might be prescribed, such as tramadol (Ultram, ConZip), oxycodone (OxyContin, Roxicodone, others) or hydrocodone (Hysingla, Zohydro ER). Opioids act on the central nervous system to relieve pain. When opioids are used for a long time, they may become habit-forming, causing mental or physical dependence.
- Nonsteroidal anti-inflammatory drugs (NSAIDs). NSAIDs reduce both pain and inflammation. Over-the-counter NSAIDs include ibuprofen (Advil, Motrin IB, others) and naproxen (Aleve). Some types of NSAIDs are available only by prescription. Oral NSAIDs can cause stomach irritation and may increase your risk of heart attack or stroke. Some NSAIDs are also available as creams or gels, which can be rubbed on joints.
- Counterirritants. Some varieties of creams and ointments contain menthol or capsaicin, the ingredient that makes hot peppers spicy. Rubbing these preparations on the skin over your aching joint may interfere with the transmission of pain signals from the joint itself.
- Disease-modifying antirheumatic drugs (DMARDs). Often used to treat rheumatoid arthritis, DMARDs slow or stop your immune system from attacking your joints. Examples include methotrexate (Trexall, Rasuvo, others) and hydroxychloroquine (Plaquenil). Side effects vary but most DMARDs increase your risk of infections.
- Biologic response modifiers. Typically used in conjunction with DMARDs, biologic response modifiers are genetically engineered drugs that target various protein molecules that are involved in the immune response. There are many types of biologic response modifiers. Tumor necrosis factor (TNF) inhibitors are commonly prescribed. Examples include etanercept (Enbrel, Erelzi, Eticovo) and infliximab (Remicade, Inflectra, others). Other medications target other substances that play a role in inflammation, such as interleukin-1 (IL-1), interleukin-6 (IL-6), Janus kinase enzymes, and certain types of white blood cells known as B cells and T cells.
- Corticosteroids. This class of drugs, which includes prednisone (Prednisone Intensol, Rayos) and cortisone (Cortef), reduces inflammation and suppresses the immune system. Corticosteroids can be taken orally or can be injected directly into the painful joint. Side effects may include thinning of bones, weight gain and diabetes.
Arthritis pain relief
Many professional organizations have guidelines for managing arthritis pain. A common theme across guidelines is that pain management strategies should be flexible, include options that do not involve medication, and be tailored to meet the needs of the patient. Such guidelines suggest the following for managing arthritis symptoms such as pain:
- Over-the-counter medications like acetaminophen (e.g., Tylenol®) or ibuprofen (e.g., Advil® or Motrin®) and other nonsteroidal anti-inflammatory drugs (NSAIDs). Emerging evidence suggests that these are safer and more effective treatments for managing long-term arthritis pain than opioids 28. A recent study of individuals with knee and hip osteoarthritis, the most common types of arthritis, found that after one year, people who took over-the-counter medications had greater reductions in pain severity than people who took opioids.
- Physical activity/exercise or community-based physical activity programs.
- Exercise therapy, including physical therapy.
- Self-management education workshops.
- Weight loss, if overweight or obese.
- Cognitive behavioral therapy (CBT) —a psychological, goal-directed approach in which patients learn how to modify physical, behavioral, and emotional triggers of pain and stress. In cognitive behavioral therapy (CBT), a psychotherapist helps you identify problematic behaviors (like becoming less active or doing fewer fun activities in response to pain), negative thoughts (about self, others and the future) and feelings (depression, guilt, anxiety). This can increase your awareness of how problematic patterns develop and help you understand the connection between thought patterns and feelings. You are then trained in pain coping skills, such as relaxation techniques, guided imagery and goal setting, encouraging you to have an active role in managing and controlling pain. CBT can increase your ability to control pain while acknowledging that there may be occasionally flares beyond your control.
Supplements
Several nutritional supplements have shown promise for relieving pain, stiffness and other arthritis symptoms. Glucosamine and chondroitin, omega-3 fatty acids, SAM-e (S-Adenosyl-L-methionine), MSM (methylsulfonylmethane), pycnogenol, Boswellia serrata (5-Loxin, Aflapin), curcumin (turmeric), Willow bark, avocado+soybean unsaponifiables (ASUs) and undenatured type II collagen (UC-II) are just some of the natural products researchers have studied for osteoarthritis (OA) and rheumatoid arthritis (RA).
Some of these natural remedies are better than others at easing pain and stiffness, especially when you use them in conjunction with traditional treatments. Check with your doctor before trying any of these products – many have some side effects and some may interfere with your medications. And only use them as part of a comprehensive arthritis management plan that includes exercising regularly, maintaining a healthy weight and protecting your joints.
Glucosamine and Chondroitin
Glucosamine and chondroitin are two of the most commonly used supplements for arthritis. They’re components of cartilage—the substance that cushions your joints.
Research has shown mixed results for using these popular supplements for osteoarthritis, in part because studies have used varying designs and supplement types. A large National Institutes of Health study called the GAIT trial compared glucosamine and chondroitin, alone or together, with an NSAID and inactive treatment (placebo) in people with knee osteoarthritis. Glucosamine improved symptoms like pain and function, but not much better than a placebo. Yet a 2016 international trial found the combination to be as effective as the NSAID celecoxib at reducing pain, stiffness and swelling in knee osteoarthritis.
Studies have also differed on which form of the supplements is most effective. Some evidence suggests glucosamine sulfate is best. Others find glucosamine hydrochloride to be more effective. One study that compared the two forms head to head showed they offered equivalent pain relief. Mayo Clinic researchers say evidence supports trying glucosamine sulfate – not hydrochloride – with or without chondroitin sulfate for knee osteoarthritis.
Glucosamine and chondroitin may interact with the blood thinning drug warfarin (Coumadin), and glucosamine can affect blood sugar control in people with diabetes.
Fish oil
Fish oil is loaded with the polyunsaturated omega-3 fatty acids DHA (docosahexaenoic acid) and EPA (eicosapentaenoic acid), which have potent anti-inflammatory properties, they help bring down inflammation in the body. Fish oil supplements have the potential to protect your heart and brain, which may be why they’re so widely used. Omega-3 fats seem to work better for rheumatoid arthritis than for osteoarthritis, most likely because rheumatoid arthritis is mainly driven by inflammation.
A 2017 systematic review of studies found that omega-3 supplements reduced joint pain, stiffness and swelling in rheumatoid arthritis. Taking these supplements might help some people cut down on their use of pain relievers and avoid their side effects. For mild cases of arthritis, it may be better to reach for the supplements before you go for the ibuprofen. Omega-3s have the added benefit of protecting against heart disease and dementia.
Plant-based sources such as flax and chia seeds also contain omega-3s, but in the form of short-chain alpha-linolenic acid (ALA). It’s the long-chain omega-3 fatty acids — eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) — that have the majority of the health benefits. When you buy fish oil, make sure the supplement lists the EPA and DHA content, and that you take at least one gram each of EPA and DHA. Vegans can get these omega-3s from an algae-based supplement.
S-adenosyl-methionine
SAM-e (S-adenosyl-methionine), is a substance your body naturally produces that has anti-inflammatory, cartilage-protecting and pain-relieving effects. In studies, SAM-e was about as good at relieving osteoarthritis pain as NSAIDs like ibuprofen and celecoxib, without their side effects.
SAM-e has a bonus benefit, too. The supplement is most useful when you also have depression, because it has a mild to moderate antidepressant effect.
Although SAM-e supplement is generally safe, it could be risky for people with bipolar disorder or who are immune-compromised, and it may interact with drugs, including antidepressants and the Parkinson’s treatment levodopa.
There’s theoretical reason to believe that taking SAM-e may promote Pneumocystis infection in people who are immunocompromised, such as those who are HIV-positive.
The typical SAM-e dose is 1,200 mg daily. If you plan to try this supplement, be patient. It’s going to take a few weeks to see the full effects.
Curcumin
Curcumin is the active compound that gives turmeric its distinctive yellow color, is a staple of Indian curries. In the body, curcumin acts as a powerful anti-inflammatory and anti-rheumatic agent, blocking the same inflammation-promoting enzyme as the COX-2 inhibitor drug, celecoxib.
In a study of 367 people with knee osteoarthritis, a 1,500 mg daily dose of curcumin extract was as effective as 1,200 mg a day of ibuprofen, without the gastrointestinal side effects. This supplement also appears to relieve rheumatoid arthritis swelling and tenderness.
One downside to curcumin is that it’s hard for the body to absorb. You want to take it with a source of fat. Some of the supplements will be in an oil base, which is really important. Black pepper also increases curcumin absorption. Some supplements add the black pepper extract, piperine. However, piperine could potentially cause liver damage, and it can increase the absorption of medications like carbamazepine (Tegretol) and phenytoin (Dilantin), making them more potent. Curcumin may also interact with blood thinners, such as warfarin.
One review of studies on knee osteoarthritis found that formulations of curcumin that are more easily absorbed by the body (such as Theracurmin or C3 Complex) reduced pain.
Methylsulfonylmethane (MSM)
Methylsulfonylmethane (MSM) is a compound found in green fruits and vegetables, that is used in the body to maintain and repair connective tissue, and it may have anti-inflammatory properties. Some studies found methylsulfonylmethane (MSM) may improve pain and function in knee osteoarthritis, and a recent review says that, despite poor quality of studies, limited evidence does support using it for osteoarthritis. Doses used in the studies ranged from 1.5 g to 6 g per day. MSM can cause side effects, including allergic reactions.
Pycnogenol
Pycnogenol, a bark extract of the maritime pine, is thought to have anti-inflammatory properties. A systematic review found that limited evidence supports trying Pycnogenol for osteoarthritis for a few months; studies show improvements in knee osteoarthritis pain and function when taken at 50 mg two or three times daily for three months. Side effects may include stomach upset and increased symptoms of autoimmune diseases so talk to your doctor before trying it.
Boswellia serrata
This plant extract has been used in Ayurvedic medicine for centuries to treat inflammatory diseases. In studies, proprietary extracts of Boswellia serrata (5-Loxin, Aflapin) temporarily reduced inflammation and pain and disability in knee osteoarthritis. A systematic review found noteworthy effects in easing osteoarthritis symptoms, although the quality of the evidence was weak. Minor side effects included nausea, headache, fever, diarrhea, abdominal pain and general weakness.
Avocado plus Soybean Unsaponifiables (ASUs)
Made of extracts from avocado and soybean oils, these hard-to-pronounce supplements block inflammatory substances that break down cartilage. Some studies found avocado plus soybean unsaponifiables (ASUs) improved pain, stiffness and joint function in knee and hip osteoarthritis, although a recent review of studies concluded that the quality of studies was weak and improvements were modest. In certain people, avocado plus soybean unsaponifiables (ASUs) can trigger an allergic reaction.
Willow bark
Willow bark comes from the same type of tree – Salix – that gives us salicylic acid, or aspirin. It’s been used for thousands of years to treat pain and inflammation. Whether willow bark works for osteoarthritis hard to say, because study results have been mixed or have not shown any improvement compared to placebo. And though its side effects are minimal, willow bark can cause allergic reactions in people who are sensitive to aspirin.
Undenatured type II collagen (UC-II)
Collagen is the structural protein in skin, tendons, and bones. Collagen type 2 is the form in the cartilage lining the joints. Undenatured type 2 collagen (UC-II) supplements come from the breastbone of chickens. One study showed that undenatured type 2 collagen (UC-II) improved pain, stiffness, and function in knee osteoarthritis better than a placebo, and slightly better than glucosamine and chondroitin supplements. Additional research is needed to confirm whether this supplement is effective for osteoarthritis.
Vitamins
Several vitamins have been studied for their effects on arthritis, including the antioxidant vitamins A, C, and E, and vitamins D and K. So far there’s no evidence that taking antioxidant vitamins improves arthritis symptoms, although eating a diet rich in these nutrients is healthy overall. Vitamins D and K are both important for bone strength, and vitamin K is involved in cartilage structure. Supplementing these two nutrients may be helpful if you’re deficient in them.
Supplement risks
When you take supplements as directed and under your doctor’s supervision, they’re generally safe. Yet even though they’re labeled “natural,” supplements can sometimes cause side effects or interact with the medicines you take. For example, high-dose fish oil supplements can thin the blood and may interact with anticoagulant medicines such as warfarin (Coumadin).
Sometimes you can overdo it and take too much, especially when it comes to vitamins. Some vitamins — like B and C — are water soluble. That means if you take too much of them, your body will flush out the extra. Yet fat-soluble vitamins such as A, D, E and K can build up in your body to the point where they become harmful, so check with your doctor about safe amounts.
Finally, supplements don’t go through the same rigorous approval process from the Food and Drug Administration (FDA) as medicines. The FDA has to review and approve every medication to make sure it works and that it’s safe. With supplements, the ingredients listed on the label may not be the same ones that are in the bottle.
How to take supplements safely
If you do want to try supplements, use them as an add-on to arthritis drugs, not as a replacement. They should never take the place of medications, which are the only proven way to slow joint damage.
Always check with your doctor before you try any new supplement to make sure that it’s right for you, and that you’re taking a safe dose. Also go through your entire supplement and medication list with your pharmacist to check for possible interactions.
Alternative medicine
Many people use alternative remedies for arthritis, but there is little reliable evidence to support the use of many of these products. The most promising alternative remedies for arthritis include:
- Acupuncture. This therapy uses fine needles inserted at specific points on the skin to reduce many types of pain, including that caused by some types of arthritis.
- Yoga and tai chi. The slow, stretching movements associated with yoga and tai chi may help improve joint flexibility and range of motion in people with some types of arthritis.
- Massage. Light stroking and kneading of muscles may increase blood flow and warm affected joints, temporarily relieving pain. Be sure to choose a massage therapist who understands arthritis and tell them which of your joints are affected.
- Biofeedback. You can learn to control your body’s responses to pain triggers. In biofeedback, through sensors connected to your body, a machine will show how thoughts and actions can affect your autonomic nervous system. This controls the heart, lungs, stomach and intestines, as well as the release of stress hormones. Learning how to control breathing and heart rate will allow you to control other physical reactions, such as pain.
- Hypnosis. This practice can help people manage pain or shift their attention away from it. In a hypnotic state, you give control to your subconscious mind. Your overworked conscious mind takes a break, allowing you to reach a state of deep relaxation.
Physical therapy
Physical therapy can be helpful for some types of arthritis. Exercises can improve range of motion and strengthen the muscles surrounding joints. In some cases, splints or braces may be warranted.
Lifestyle and home remedies
In many cases, arthritis symptoms can be reduced with the following measures:
- Weight loss. If you’re obese, losing weight will reduce the stress on your weight-bearing joints. This may increase your mobility and limit future joint injury.
- Exercise. Regular exercise can help keep your joints flexible. Swimming and water aerobics may be good choices because the buoyancy of the water reduces stress on weight-bearing joints.
- Heat and cold. Heating pads or ice packs may help relieve arthritis pain.
- Assistive devices. Using canes, shoe inserts, walkers, raised toilet seats and other assistive devices can help protect your joints and improve your ability to perform daily tasks.
Surgery
If conservative measures don’t help, your doctor may suggest surgery, such as:
- Joint repair. In some instances, joint surfaces can be smoothed or realigned to reduce pain and improve function. These types of procedures can often be performed arthroscopically — through small incisions over the joint.
- Joint replacement. This procedure removes your damaged joint and replaces it with an artificial one. Joints most commonly replaced are hips and knees.
- Joint fusion. This procedure is more often used for smaller joints, such as those in the wrist, ankle and fingers. It removes the ends of the two bones in the joint and then locks those ends together until they heal into one rigid unit.
Living with arthritis
There are many things you can do to help manage arthritis. Maintaining a healthy lifestyle can help control the symptoms.
Healthy Diet
Eating well is important for your overall health and wellbeing. A healthy diet can help you maintain a healthy weight, which reduces the pressure put on your joints. This might help reduce joint pain.
There is some evidence to suggest that eating healthy fats, such as monounsaturated and omega-3 fats, rather than unhealthy fats such as polysaturated fats, can help reduce the symptoms of arthritis. While these benefits are modest compared to medication, they have no side effects and have other benefits, such as reducing your risk of heart disease.
If you have arthritis, you should aim to eat:
- a healthy balanced diet
- a more Mediterranean-style diet, with plenty of fish, pulses, nuts, olive oil, fruit and vegetables
- more unsaturated fats, such as in vegetable oils, avocados and many nuts and seeds
- more omega-3 fatty acids, such as from oily fish
- less saturated fats, such as from red meat, poultry, and full-fat dairy
- less energy dense foods, such as in fatty and sugary foods to avoid gaining weight
- an adequate calcium dairy products do not cause arthritis. The calcium in dairy products is important for strong bones, which is especially important for people with arthritis, who may be at increased risk of osteoporosis (weak and brittle bones). Eat plenty of calcium-rich foods including dairy products (milk, cheese and yoghurt), nuts, seeds and fish, such as sardines or whitebait (particularly if you eat the bones).
If you have gout, avoid foods containing purines (meat, seafood, foods containing yeast)
Others believe acidic fruits, such as lemons, oranges and grapefruit, and nightshade vegetables, such as potatoes, eggplants and capsicum, can make symptoms worse. However, there is no proof of this, and avoiding these foods may do more harm than good.
If you need advice about your diet, ask your doctor to refer you to a dietitian.
Exercise regularly
Getting regular exercise is one of the most effective ways that you can treat arthritis. If you have arthritis, participating in joint-friendly physical activity can improve your arthritis pain, function, mood, and quality of life. Joint-friendly physical activities are low-impact, which means they put less stress on the body, reducing the risk of injury. Examples of joint-friendly activities include brisk walking, cycling, water aerobics, and swimming. Being physically active can also delay the onset of arthritis-related disability and help people with arthritis manage other chronic conditions such as diabetes, heart disease, and obesity. Learn how you can increase your physical activity safely.
Exercise can help in many ways, including:
- helping with balance
- keeping muscles strong to support the joints
- reducing joint stiffness
- reducing pain and tension in your joints
- decreasing fatigue and depression
- keeping you mobile
- boosting your energy and mood
- improving sleep
When starting or increasing physical activity, start slow and pay attention to how your body tolerates it.
The type of exercise that is best for you will depend on the type of arthritis. It is important to find the right type and level of exercise. Try to be realistic about the amount of exercise you are able to do and choose an activity you enjoy.
There are 5 types of exercise that combine to make up a good fitness program. They are:
- Range of movement exercise — this helps improve strength and flexibility and promotes good posture; try swimming, tai chi and golf
- Strengthening exercise — this will help build the muscles, which in turn provide better support for your joints; try weight training or working with resistance bands
- Low-impact aerobic exercise — low-impact aerobic activities do not put stress on the joints but raises your heartbeat, which helps to improve your level of fitness by strengthening your heart; some of the best forms of aerobic exercise are brisk walking, cycling, swimming and water aerobics
- For major health benefits, do at least:
- 150 minutes (2 hours and 30 minutes) of moderate-intensity aerobic activity, like cycling at less than 10 miles per hour, or
- 75 minutes (1 hour and 15 minutes) of vigorous-intensity aerobic activity, like cycling at 10 mph or faster, each week. Another option is to do a combination of both. A rule of thumb is that 1 minute of vigorous-intensity activity is about the same as 2 minutes of moderate-intensity activity.
- For major health benefits, do at least:
- Balance exercises like walking backwards, standing on one foot, and tai-chi are important for those who are at a risk of falling or have trouble walking. Balance exercises are included in many group exercise classes.
- Flexibility exercises like stretching and yoga are also important for people with arthritis. Many people with arthritis have joint stiffness that makes daily tasks difficult. Doing daily flexibility exercises helps maintain range of motion so you can keep doing everyday things like household tasks, hobbies, and visiting with friends and family.
You may experience some pain when you first start a new exercise program. This is often due to new muscles being used. However, if you feel pain for longer than 2 hours after exercising, or you have any pain in the joints, consult your doctor or physiotherapist before doing the exercise again.
If you have osteoarthritis, a moderate exercise program is far more beneficial than a strenuous program. Too much exercise can cause further pain and joint degeneration. Try to do small exercises every day to improve your range of movement. Never force a painful joint.
If you have rheumatoid arthritis, make sure you get the right balance between rest and activity. Exercise when you are least tired and try to do small exercises every day in every joint. Swimming and cycling are good low impact choices. You can still exercise during a flare-up, but you should reduce the intensity of your workout.
Manage your pain
Pain can be caused by inflammation, damage to the joints and muscle tension. It can be worse when you are tired or stressed.
Some things you can do to manage pain include:
- taking pain killers. Your doctor or pharmacist can advise you
- exercising regularly to keep the joints moving
- using hot (a warm bath, heat pack or hot water bottle) or cold (ice pack) treatments throughout the day
- looking after your joints by avoiding activities that make pain worse
- using therapies such as massage, acupuncture, transcutaneous electrical nerve stimulation (TENS) or mindfulness techniques
Modify your home
If you have arthritis, it’s important to protect your joints by finding the best techniques for doing daily tasks and making good use of equipment designed to make your life easier.
Products and equipment are available that can, for example, help you to:
- turn doorknobs and keys
- reach for and pick up objects
- get in and out of chairs
- get dressed
- prepare food
- do household cleaning
- manage in the bathroom
If your arthritis makes you unsteady, make sure you reduce your risk of falls.
References- Arthritis. https://www.niams.nih.gov/health-topics/arthritis
- Barbour KE, Helmick CG, Boring M, Brady TJ. Vital Signs: Prevalence of Doctor-Diagnosed Arthritis and Arthritis-Attributable Activity Limitation — United States, 2013–2015. MMWR Morb Mortal Wkly Rep 2017;66:246–253. DOI: http://dx.doi.org/10.15585/mmwr.mm6609e1
- March L, Smith EU, Hoy DG, Cross MJ, Sanchez-Riera L, Blyth F, Buchbinder R, Vos T, Woolf AD. Burden of disability due to musculoskeletal (MSK) disorders. Best Pract Res Clin Rheumatol. 2014 Jun;28(3):353-66. doi: 10.1016/j.berh.2014.08.002
- Ankylosing spondylitis. https://www.niams.nih.gov/health-topics/ankylosing-spondylitis
- de Vlam K, Mielants H, Cuvelier C, De Keyser F, Veys EM, De Vos M. Spondyloarthropathy is underestimated in inflammatory bowel disease: prevalence and HLA association. J Rheumatol. 2000 Dec;27(12):2860-5.
- Leirisalo-Repo M. Enteropathic arthritis, Whipple’s disease, juvenile spondyloarthropathy, and uveitis. Curr Opin Rheumatol. 1994 Jul;6(4):385-90. doi: 10.1097/00002281-199407000-00006
- Orlando A, Renna S, Perricone G, Cottone M. Gastrointestinal lesions associated with spondyloarthropathies. World J Gastroenterol. 2009 May 28;15(20):2443-8. doi: 10.3748/wjg.15.2443
- Manguso F, Staiano T, Astarita C, Scarpa R, Peluso R, Gargano D, Ayala F, D’Arienzo A. Consecutive occurrence of rhinoconjunctivitis, seronegative spondyloarthritis and pyoderma gangrenosum in a patient with ulcerative colitis. Int J Colorectal Dis. 2005 Jan;20(1):79-80. doi: 10.1007/s00384-004-0626-0
- Vavricka SR, Brun L, Ballabeni P, Pittet V, Prinz Vavricka BM, Zeitz J, Rogler G, Schoepfer AM. Frequency and risk factors for extraintestinal manifestations in the Swiss inflammatory bowel disease cohort. Am J Gastroenterol. 2011 Jan;106(1):110-9. doi: 10.1038/ajg.2010.343
- Veloso FT, Carvalho J, Magro F. Immune-related systemic manifestations of inflammatory bowel disease. A prospective study of 792 patients. J Clin Gastroenterol. 1996 Jul;23(1):29-34. doi: 10.1097/00004836-199607000-00009
- Manguso F, Sanges M, Staiano T, Gargiulo S, Nastro P, Gargano D, Somma P, Mansueto G, Peluso R, Scarpa R, D’Armiento FP, Astarita C, Ayala F, Renda A, Mazzacca G, D’Arienzo A. Cigarette smoking and appendectomy are risk factors for extraintestinal manifestations in ulcerative colitis. Am J Gastroenterol. 2004 Feb;99(2):327-34. doi: 10.1111/j.1572-0241.2004.04039.x
- Enteropathic Arthropathies Treatment & Management. https://emedicine.medscape.com/article/334746-treatment
- Takeuchi K, Smale S, Premchand P, Maiden L, Sherwood R, Thjodleifsson B, Bjornsson E, Bjarnason I. Prevalence and mechanism of nonsteroidal anti-inflammatory drug-induced clinical relapse in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol. 2006 Feb;4(2):196-202. doi: 10.1016/s1542-3565(05)00980-8
- Sandborn WJ, Stenson WF, Brynskov J, Lorenz RG, Steidle GM, Robbins JL, Kent JD, Bloom BJ. Safety of celecoxib in patients with ulcerative colitis in remission: a randomized, placebo-controlled, pilot study. Clin Gastroenterol Hepatol. 2006 Feb;4(2):203-11. doi: 10.1016/j.cgh.2005.12.002
- Clegg, D.O., Reda, D.J. and Abdellatif, M. (1999), Comparison of sulfasalazine and placebo for the treatment of axial and peripheral articular manifestations of the seronegative spondylarthropathies: A Department of Veterans Affairs cooperative study. Arthritis & Rheumatism, 42: 2325-2329. https://doi.org/10.1002/1529-0131(199911)42:11<2325::AID-ANR10>3.0.CO;2-C
- Thomas Chateau, Stefanos Bonovas, Catherine Le Berre, Nicolas Mathieu, Silvio Danese, Laurent Peyrin-Biroulet, Vedolizumab Treatment in Extra-Intestinal Manifestations in Inflammatory Bowel Disease: A Systematic Review, Journal of Crohn’s and Colitis, Volume 13, Issue 12, December 2019, Pages 1569–1577, https://doi.org/10.1093/ecco-jcc/jjz095
- Gout. https://www.niams.nih.gov/health-topics/gout/advanced
- Psoriatic arthritis. https://www.niams.nih.gov/health-topics/psoriatic-arthritis/advanced
- Septic arthritis. https://medlineplus.gov/ency/article/000430.htm
- Margaretten ME, Kohlwes J, Moore D, Bent S. Does this adult patient have septic arthritis? JAMA. 2007;297(13):1478–1488.
- Ross JJ, Saltzman CL, Carling P, Shapiro DS. Pneumococcal septic arthritis: review of 190 cases. Clin Infect Dis. 2003;36(3):319–327.
- Goldenberg DL. Septic arthritis. Lancet. 1998;351(9097):197–202.
- Smith JW, Piercy EA. Infectious arthritis. Clin Infect Dis. 1995;20(2):225–230.
- Ryan MJ, Kavanagh R, Wall PG, Hazleman BL. Bacterial joint infections in England and Wales: analysis of bacterial isolates over a four year period. Br J Rheumatol. 1997;36(3):370–373.
- Gonorrhea. https://medlineplus.gov/ency/article/007267.htm
- Zieger MM, Dörr U, Schulz RD. Ultrasonography of hip joint effusions. Skeletal Radiol. 1987;16(8):607–611.
- Graif M, Schweitzer ME, Deely D, Matteucci T. The septic versus non-septic inflamed joint: MRI characteristics. Skeletal Radiol. 1999;28(11):616–620.
- Skelly AC, Chou R, Dettori JR, Turner JA, Friedly JL, Rundell SD, Fu R, Brodt ED, Wasson N, Winter C, Ferguson AJR. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review. Comparative Effectiveness Review No. 209. (Prepared by the Pacific Northwest Evidence-based Practice Center under Contract No. 290-2015-00009-I.) AHRQ Publication No 18-EHC013-EF. Rockville, MD: Agency for Healthcare Research and Quality; June 2018. https://doi.org/10.23970/AHRQEPCCER209





{kind=link}