
What is asthma
Asthma also known as bronchial asthma, is a long-term (chronic) lung condition that causes the airways of the lungs to swell (inflammation) and narrow. Normally, when someone breathes in, air goes in through the nose or mouth, down the windpipe (trachea), and into the airways (bronchioles) of the lungs. When people breathe out, air exits the body in the opposite direction. With asthma, air has a harder time passing through the airways of the lungs. Airways swell and fill with mucus. The muscles around the airways tighten, making airways narrower. It leads to wheezing, shortness of breath, chest tightness, and coughing. Certain things can set off or worsen asthma symptoms, such as pollen, exercise, viral infections, or cold air. These are called asthma triggers. When symptoms get worse, it is called an asthma attack.
According to data from the National Health Interview Survey, the prevalence of asthma in the United States in 2014 was 7.7% in all ages, with 44.7% of persons with asthma reporting having had one or more asthma attacks. Nearly 9 million of them are children. Children have smaller airways than adults, which makes asthma especially serious for them. Children with asthma may experience wheezing, coughing, chest tightness, and trouble breathing, especially early in the morning or at night. In 2011, there were 1.8 million emergency department visits for asthma and in 2012 there were 10.5 million physician office visits with asthma as the primary diagnosis (Centers for Disease Control) 1.
In childhood, asthma is more common in boys with a male to female ratio of 2:1 until puberty when the ratio becomes 1:1 2. After puberty, the prevalence of asthma is greater in females, and adult-onset cases after the age of 40 years are mostly females. Asthma prevalence is greater in extreme of ages due to airway responsiveness and lower levels of lung function 3.
Of all the asthma cases, about 66% are diagnosed before the age of 18 years. almost 50% of children with asthma have a decrease in severity or disappearance of symptoms during early adulthood 4. There are limited data about the natural history of asthma after diagnosis, but one longitudinal study showed that approximately 16% of adults with recently diagnosed asthma may experience clinical remission (no symptoms or asthma medication for at least 1 year) within 5 years 5.
Given the prevalence of asthma, the impact on patients and caregivers, and the health care resources it demands, clinical guidelines are critical to standardizing and improving care throughout health care systems. The plan may include monitoring, avoiding triggers, and using medicines.
For some people, asthma signs and symptoms flare up in certain situations:
- Exercise-induced asthma, which is transient, reversible bronchoconstriction that happens during or after strenuous exercise
- Occupational asthma, triggered by workplace irritants such as chemical fumes, gases or dust
- Allergy-induced asthma, triggered by airborne substances, such as pollen, mold spores, cockroach waste, or particles of skin and dried saliva shed by pets (pet dander)
Asthma key facts
- Asthma is a long-term lung condition that is caused by narrowing of the airways when they become inflamed.
- People with asthma experience difficulty breathing, and the most common symptoms are wheezing, coughing, feeling ‘out of breath’ and tightness in the chest.
- Asthma symptoms are usually mild but can flare up and cause an ‘asthma attack’ that may require hospital care.
- There are effective medicines for asthma that, if taken correctly, will help you feel well and keep you out of hospital.
- Asthma can be managed with reliever inhalers to treat symptoms and attacks. Preventer or controller medications such as inhaled corticosteroid (ICS) can prevent symptoms.
- Low dose inhaled corticosteroid (ICS) markedly reduces asthma hospitalizations and death 6
- Low dose inhaled corticosteroid (ICS) is very effective in preventing severe asthma exacerbations, reducing symptoms, improving lung function, and preventing exercise-induced bronchoconstriction, even in patients with mild asthma
- Early treatment with low dose inhaled corticosteroid (ICS) is associated with better lung function than if symptoms have been present for more than 2–4 years
- Patients not taking inhaled corticosteroid (ICS) who experience a severe exacerbation have lower long-term lung function than those who have started inhaled corticosteroid (ICS)
- In occupational asthma, early removal from exposure and early treatment increase the probability of recovery.
Seek emergency treatment:
Severe asthma attacks can be life-threatening. Work with your doctor to determine what to do when your signs and symptoms worsen — and when you need emergency treatment. Signs of an asthma emergency include:
- Rapid worsening of shortness of breath or wheezing
- No improvement even after using a quick-relief inhaler
- Shortness of breath when you are doing minimal physical activity
See your doctor:
- If you think you have asthma. If you have frequent coughing or wheezing that lasts more than a few days or any other signs or symptoms of asthma, see your doctor. Treating asthma early may prevent long-term lung damage and help keep the condition from getting worse over time.
- To monitor your asthma after diagnosis. If you know you have asthma, work with your doctor to keep it under control. Good long-term control helps you feel better from day to day and can prevent a life-threatening asthma attack.
- If your asthma symptoms get worse. Contact your doctor right away if your medication doesn’t seem to ease your symptoms or if you need to use your quick-relief inhaler more often. Don’t take more medication than prescribed without consulting your doctor first. Overusing asthma medication can cause side effects and may make your asthma worse.
- To review your treatment. Asthma often changes over time. Meet with your doctor regularly to discuss your symptoms and make any needed treatment adjustments.
Types of asthma
Asthma is a heterogeneous disease, with different underlying disease processes. Recognizable clusters of demographic, clinical and/or pathophysiological characteristics are often called ‘asthma phenotypes’ 7. Many clinical phenotypes of asthma have been identified 8. Some of the most common are 9:
- Allergic asthma: this is the most easily recognized asthma phenotype, which often commences in childhood and is associated with a past and/or family history of allergic disease such as eczema, allergic rhinitis, or food or drug allergy. Examination of the induced sputum of these patients before treatment often reveals eosinophilic airway inflammation. Patients with allergic asthma phenotype usually respond well to inhaled corticosteroid (ICS) treatment.
- Non-allergic asthma: some patients have asthma that is not associated with allergy. The cellular profile of the sputum of these patients may be neutrophilic, eosinophilic or contain only a few inflammatory cells (paucigranulocytic). Patients with non-allergic asthma often demonstrate less short-term response to inhaled corticosteroid (ICS).
- Adult-onset (late-onset) asthma: some adults, particularly women, present with asthma for the first time in adult life. These patients tend to be non-allergic, and often require higher doses of inhaled corticosteroid (ICS) or are relatively refractory to corticosteroid treatment. Occupational asthma (i.e. asthma due to exposures at work) should be ruled out in patients
presenting with adult-onset asthma. - Asthma with persistent airflow limitation: some patients with long-standing asthma develop airflow limitation that is persistent or incompletely reversible. This is thought to be due to airway wall remodeling.
- Asthma with obesity: some obese patients with asthma have prominent respiratory symptoms and little eosinophilic airway inflammation.
Asthma severity classification
To classify your asthma severity, your doctor will consider how often you have signs and symptoms and how severe they are. Your doctor will also consider the results of your physical exam and diagnostic tests.
Determining your asthma severity helps your doctor choose the best treatment. Asthma severity often changes over time, requiring treatment adjustments.
Asthma is classified into four general categories:
- Mild intermittent asthma: Mild symptoms up to two days a week and up to two nights a month
- Mild persistent asthma: Symptoms more than twice a week, but no more than once in a single day
- Moderate persistent asthma: Symptoms once a day and more than one night a week
- Severe persistent asthma: Symptoms throughout the day on most days and frequently at night
Asthma Attack
Asthma attacks happen when the airways swell and narrow more than usual, making it harder to breathe. During an asthma attack, symptoms get much worse. Attacks can come on fast or gradually and may be life-threatening. People with severe asthma tend to get asthma attacks more often.
Asthma attacks can be very scary. For some people, an attack starts with coughing. During an attack, your chest may feel tight or like someone is sitting on it. Some people say it’s like having the air sucked out of them or trying to suck air in through a straw. You may start to wheeze or feel lightheaded.
During an asthma attack (flare-up), you might have:
- trouble breathing or shortness of breath (dyspnea)
- a tight chest
- a whistling sound while breathing (wheezing)
- a cough
- a fast heartbeat
Some flare-ups are serious, but others are mild. Flare-ups can happen suddenly or build up over time, especially if people don’t take their asthma medicines as directed.
Things that bring on a flare-up are called triggers. Triggers vary from person to person, but common ones include:
- allergies to things like pollen, mold, and pet dander
- irritants and pollutants in the air
- respiratory infections, like colds or flu
- weather conditions
- exercise (some kids only have asthma symptoms during or after exercise)
- gastroesophageal reflux
An important part of managing asthma is avoiding triggers. Your child’s doctor will work with you to create a care plan that helps prevent flare-ups as much as possible.
You should go to the emergency room if at-home treatments are not working or if you have a severe asthma attack. If you need emergency care, you may be treated with medicines given with a nebulizer (a machine that changes liquid medicine into mist that you can breathe in) or through an intravenous (IV) in your arm. You may also receive oxygen therapy or breathing support with a ventilator.
Signs of an asthma attack
If you do not know if you have asthma, these 4 symptoms could be signs that you do:
- Coughing that sometimes wakes you up at night.
- Wheezing, or a whistling sound when you breathe. You may hear it more when you breathe out. It can start as a low-sounding whistle and get higher.
- Breathing problems that include having shortness of breath (dyspnea), feeling like you are out of breath, gasping for air, having trouble breathing out, or breathing faster than normal. When breathing gets very difficult, the skin of your chest and neck may suck inward.
- Chest tightness
Other Warning Signs
Other early warning signs of an asthma attack are:
- An itchy neck
- Dark bags under your eyes
- Fatigue
- Being short-tempered or irritable
- Feeling nervous or edgy
Danger Signs
Call your local emergency number right away if you have any of the following symptoms. These are signs of a serious medical emergency.
- You are having trouble walking or talking because it is so hard to breathe.
- You are hunching over.
- Your lips or fingernails are blue or gray.
- You are confused or less responsive than usual.
If your child has asthma, the child’s caregivers must know to call 911 if your child has any of these symptoms. This includes teachers, babysitters, and others who take care of your child.
Exercise induced asthma
Sometimes exercise triggers asthma symptoms. This is called exercise-induced asthma 10. Exercise induced asthma is defined as transient, reversible bronchoconstriction that happens during or after strenuous exercise. The symptoms of exercise induced asthma are coughing, wheezing, a feeling of tightness in your chest, or shortness of breath; however, many athletes will present with nonspecific symptoms, such as fatigue and impaired performance. Most times, these symptoms start soon after you stop exercising. Some people may have symptoms after they start exercising. Reports of severe symptoms with respiratory failure and death occur rarely.
More than 10 percent of the general population and up to 90 percent of persons previously diagnosed with asthma and up to 20% of those without asthma have exercise-induced asthma 11, 12, 13. Risk factors for exercise-induced asthma include a personal or family history of asthma, a personal history of atopy or allergic rhinitis, exposure to cigarette smoke, participating in high-risk sports, living and practicing in areas with high levels of pollution, and female gender. Some small studies suggest sugar-sweetened beverages may increase risk by increasing inflammation and adiposity 14, 15.
Exercise has paradoxically been shown to improve exercise induced asthma severity, pulmonary function, and reduce airway inflammation in people with asthma and exercise induced asthma 16. Early detection, diagnosis confirmed by the change in lung function during exercise, and treatment can improve quality of life and, when managed appropriately, allows patients to participate freely in exercise without limiting competition at the elite level 17. Non-pharmacologic treatments addressing the root cause of exercise induced asthma, an acute steep increase in ventilation and demand on the respiratory system, including warm-up exercises, and protecting the airway from cold, dry air, pollutants, and allergens is recommended. Pharmacologic treatments aimed at the pathophysiologic processes involved in the symptomatic bronchoconstriction, including short-acting beta-agonists (SABA), inhaled corticosteroids, leukotriene receptor antagonists and mast cell stabilizing agents are effective and without significant side effects 18.
Be Careful Where and When you Exercise
Having asthma symptoms when you exercise does not mean you cannot or should not exercise. But be aware of your exercise induced asthma triggers.
Cold or dry air may trigger your asthma symptoms. If you do exercise in cold or dry air 19:
- Breathe through your nose.
- Wear a scarf or mask over your mouth.
- DO NOT exercise when the air is polluted.
- DO NOT exercise near fields or lawns that have just been mowed.
Warm up before you exercise, and cool down afterward:
- To warm up, walk or do your exercise activity slowly before you speed up.
- The longer you warm up, the better.
- To cool down, walk or do your exercise activity slowly for several minutes.
Some kinds of exercise may be less likely to trigger asthma symptoms than others.
- Swimming is a good sport for people with exercise induced asthma. The warm, moist air helps keep asthma symptoms away.
- Football, baseball, and other sports with periods when you do not move fast are less likely to trigger your asthma symptoms.
Activities that keep you moving fast all the time are more likely to trigger asthma symptoms, such as running, basketball, or soccer.
Use Your Asthma Medicine Before you Exercise
Always follow your doctor’s advice on which medicines to use and when.
Take your short-acting, or quick-relief, inhaled medicines before you exercise.
- Short-acting beta agonists (SABAs) inhalers for asthma include:
- Albuterol (ProAir HFA, Proventil HFA, Ventolin HFA)
- Levalbuterol (Xopenex, Xopenex HFA)
- Metaproterenol
- Terbutaline
- Take short-acting beta agonists (SABAs) 10 to 15 minutes before exercise.
- They can help for up to 4 hours.
- American Thoracic Society guidelines from 2013 provide a strong recommendation with high-quality evidence for short-acting beta-2 agonists (SABAs) use 5 to 20 minutes (optimally 15) minutes before exercise 20. The bronchodilation is of rapid onset and can last 2 to 4 hours. Tolerance can develop with frequent short-acting beta-2 agonist use and is likely due to the downregulation of the beta 2 receptors. Short-acting beta-2 agonist’s are the preferred first-line treatment and have limited side effects 21. Mechanism of action is through relaxation of the airway smooth muscles and inhibition of mast cell degranulation 22.
Long-acting Beta Agonists (LABA)
- American Thoracic Society strongly recommends against, with high-quality evidence, the daily use of long-acting beta 2 agonists (LABA) because the potential side effects do not outweigh the benefits 20.
Inhaled Corticosteroids (ICS)
Inhaled corticosteroids prevent your airways from swelling in order to help keep your asthma symptoms away. Inhaled steroids are used with a metered dose asthma inhaler (MDI) and spacer. Or they may be used with a dry powder inhaler.
Inhaled corticosteroids include:
- fluticasone propionate (Flovent HFA, Flovent Diskus, Xhance),
- budesonide (Pulmicort Flexhaler, Pulmicort Respules, Rhinocort),
- ciclesonide (Alvesco),
- beclomethasone (Qvar Redihaler),
- mometasone (Asmanex HFA, Asmanex Twisthaler)
- fluticasone furoate (Arnuity Ellipta).
If symptoms are not well controlled with the short-acting beta-2 agonists (SABAs) or patient is using short-acting beta-2 agonist daily, additional medications can be added after medication adherence, and proper use has been confirmed. It is estimated that 15% to 20% of the patients will not respond to short-acting beta-2 agonist treatment. American Thoracic Society provides a strong recommendation with moderate-quality evidence for daily inhaled corticosteroids (ICS) 21. Inhaled corticosteroids may take 2 to 4 weeks for the maximal benefit. Inhaled corticosteroid appears to be more effective in patients with underlying asthma and are dose-dependent. Inhaled corticosteroids (ICS) are not effective when used intermittently before exercise 20. Inhaled corticosteroids (ICS) has multiple well-studied benefits in patients with asthma, including a reduction in mortality 21.
Leukotriene Receptor Antagonists (LTRA)
Leukotriene Receptor Antagonists (LTRA) or leukotriene modifiers are used to prevent asthma symptoms. Leukotriene Receptor Antagonists (LTRA) come in tablet or pill form and can be used together with a steroid inhaler.
Leukotriene Receptor Antagonists (LTRA) include:
- montelukast (Singulair): Montelukast has been linked to psychological reactions, such as agitation, aggression, hallucinations, depression and suicidal thinking. Seek medical advice right away if you experience any of these reactions.
- zafirlukast (Accolate)
- zileuton (Zyflo)
American Thoracic Society provides a strong recommendation with moderate-quality evidence for daily leukotriene receptor antagonist (LTRA) to address the inflammatory mediator release involved in exercise induced asthma 21. Leukotriene receptor antagonist (LTRA) may take 2-4 weeks for the maximal benefit 20. Leukotriene modifiers, including montelukast, zafirlukast, and zileuton, provide longer-lasting bronchodilation and are not associated with tolerance. The effect on FEV1 reduction is less than with inhaled corticosteroids (ICS) or short-acting beta agonist (SABA). The choice between adding inhaled corticosteroid or leukotriene modifier is patient-specific 20.
Mast Cell Stabilizing Agents (MCSA)
Mast Cell Stabilizing Agents (MCSA) prevent the release of mast cell mediators such as histamine through stabilization of the mast cell membrane. Mast Cell Stabilizing Agents (MCSA) are most effective when used prior to antigen exposure. Mast Cell Stabilizing Agents (MCSA) include sodium cromoglycate (cromolyn sodium) and nedocromil sodium. American Thoracic Society also makes strong recommendations with high-quality evidence for adding mast cell stabilizer (MCSA) before exercise. Mast cell degranulation plays a key role in exercise induced asthma pathology. There is no additional benefit when Mast Cell Stabilizing Agent (MCSA) is combined with short-acting beta-2 agonists (SABAs), and Mast Cell Stabilizing Agents are less effective than short-acting beta-2 agonist. Mast Cell Stabilizing Agents (MCSA) is not widely available in the U.S 20.
Antihistamine
An antihistamine may be beneficial in patients with underlying allergies 20.
Short-acting Muscarinic Antagonists (SAMA)
Inhaled anticholinergic agents are weakly recommended with low-quality evidence. Short-acting muscarinic antagonists (SAMA) such as ipratropium bromide are less effective than short-acting beta-2 agonist (SABA); however, they can be used in combination when short-acting beta-2 agonist tolerance develops 21.
When to see a medical professional
Call for an appointment with your doctor if asthma symptoms develop.
See your doctor or go to the emergency room if:
- An asthma attack requires more medicine than recommended
- Symptoms get worse or do not improve with treatment
- You have shortness of breath while talking
- Your peak flow measurement is 50% to 80% of your personal best
Go to the emergency room if these symptoms occur:
- Drowsiness or confusion
- Severe shortness of breath at rest
- A peak flow measurement of less than 50% of your personal best
- Severe chest pain
- Bluish color to the lips and face
- Extreme difficulty breathing
- Rapid pulse
- Severe anxiety due to shortness of breath.
Asthma symptoms
Asthma symptoms vary from person to person. You may have infrequent asthma attacks, have symptoms only at certain times — such as when exercising — or have symptoms all the time.
Asthma signs and symptoms may include:
- Chest tightness
- Coughing, especially at night or early morning (during cool weather) or after certain activities (such as exercise)
- Shortness of breath or difficulty breathing — feeling breathless, even while resting, or being unable to finish full sentences before needing to take another breath
- Wheezing, which is a whistling sound when breathing out (exhaling), which is a common sign of asthma in children
- Trouble sleeping caused by shortness of breath, coughing or wheezing
- A lack of energy
The following features are typical of asthma and, if present, increase the probability that the patient has asthma 23:
- Respiratory symptoms of wheeze, shortness of breath, cough and/or chest tightness:
- Patients (especially adults) experience more than one of these types of symptoms.
- Symptoms are often worse at night or in the early morning.
- Symptoms vary over time and in intensity.
- Symptoms are triggered by viral infections (colds), exercise, allergen exposure, changes in weather, laughter, or irritants such as car exhaust fumes, smoke or strong smells.
Other conditions can cause these symptoms. But in asthma, the symptoms often follow a pattern:
- They come and go over time or within the same day.
- They start or get worse with viral infections, such as a cold.
- They are triggered by exercise, allergies, cold air, or breathing too fast from laughing or crying.
- They are worse at night or in the morning.
During a severe asthma attack, you may notice more serious symptoms, such as:
- Asthma signs and symptoms that are more frequent and bothersome
- Increasing difficulty breathing, as measured with a device used to check how well your lungs are working (peak flow meter)
- The need to use a quick-relief inhaler more often
- Feeling very distressed, exhausted or even limp from trying to breathe
- Deep sucking motions at the throat or chest while trying to breathe.
The following features decrease the probability that respiratory symptoms are due to asthma 9:
- Isolated cough with no other respiratory symptoms
- Chronic production of sputum
- Shortness of breath associated with dizziness, light-headedness or peripheral tingling (paresthesia)
- Chest pain
- Exercise-induced shortness of breath (dyspnea) with noisy inspiration.
Emergency asthma symptoms that need prompt medical help include:
- Bluish color to the lips and face
- Decreased level of alertness, such as severe drowsiness or confusion, during an asthma attack
- Extreme difficulty breathing
- Rapid pulse
- Severe anxiety due to shortness of breath
- Sweating
Asthma complications
Asthma complications include:
- Signs and symptoms that interfere with sleep, work and other activities
- Sick days from work or school during asthma flare-ups
- A permanent narrowing of the tubes that carry air to and from your lungs (bronchial tubes), which affects how well you can breathe
- Emergency room visits and hospitalizations for severe asthma attacks
- Side effects from long-term use of some medications used to stabilize severe asthma
- Death
Proper treatment makes a big difference in preventing both short-term and long-term complications caused by asthma.
Causes of asthma
The cause of asthma is complex and it isn’t clear why some people get asthma and others don’t, but it’s probably due to a combination of environmental and inherited (genetic) factors. However, asthma often happens when the immune system strongly reacts to a substance in the lungs. Normally, the body’s immune system helps fight infections. But it may also respond to other things you breathe in, such as pollen or mold. In some people, the immune system reacts strongly by creating inflammation. When this happens, the airways swell, narrow, and may create more mucus. The muscles around the airways may also tighten. This can make it even harder to breathe. Over time, the airway walls can become thicker.
People with asthma may have a parent or other close relative with asthma. Those who are overweight may be more likely to have it.
In people who have sensitive airways, asthma symptoms can be triggered by breathing in substances called allergens or triggers.
Asthma triggers
Exposure to various irritants and substances that trigger allergies (allergens) can trigger signs and symptoms of asthma. Asthma triggers are different from person to person and can include:
- Airborne allergens, such as pollen, dust mites, mold spores, pet dander (pet hair) or particles of cockroach waste
- Respiratory infections, such as the common cold
- Physical activity or exercise
- Changes in weather (most often cold weather)
- Air pollutants and irritants, such as smoke
- Tobacco smoke
- Certain medications, including beta blockers, aspirin, and non-steroidal anti-inflammatory drugs (NSAIDS), such as ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve)
- Strong emotions and stress
- Sulfites and preservatives added to some types of foods and beverages, including shrimp, dried fruit, processed potatoes, beer and wine
- Gastroesophageal reflux disease (GERD), a condition in which stomach acids back up into your throat
Substances in some workplaces can also trigger asthma symptoms, leading to occupational asthma. The most common triggers are wood dust, grain dust, animal dander, fungi, or chemicals.
Many people with asthma have a personal or family history of allergies, such as hay fever (allergic rhinitis) or eczema. Others have no history of allergies.
Risk factors for developing asthma
A number of factors are thought to increase your chances of developing asthma. They include:
- Having a blood relative with asthma, such as a parent or sibling
- Having another allergic condition, such as atopic dermatitis — which causes red, itchy skin — or hay fever — which causes a runny nose, congestion and itchy eyes
- Being overweight
- Being a smoker
- Exposure to secondhand smoke
- Exposure to exhaust fumes or other types of pollution
- Exposure to occupational triggers, such as chemicals used in farming, hairdressing and manufacturing.
Asthma pathophysiology
Asthma is a condition of acute, fully reversible airway inflammation, often following exposure to an environmental trigger 2. The pathological process begins with the inhalation of an irritant (e.g., cold air) or an allergen (e.g., pollen), which then, due to bronchial hypersensitivity, leads to airway inflammation and an increase in mucus production. This leads to a significant increase in airway resistance, which is most pronounced on expiration.
Airway obstruction occurs due to the combination of:
- Inflammatory cell infiltration.
- Mucus hypersecretion with mucus plug formation.
- Smooth muscle contraction.
These reversible changes may become irreversible over time due to:
- Basement membrane thickening, collagen deposition, and epithelial desquamation.
- Airway remodeling occurs in chronic disease with smooth muscle hypertrophy and hyperplasia.
If not corrected rapidly, asthma may become more difficult to treat, as the mucus production prevents the inhaled medication from reaching the mucosa. The inflammation also becomes more edematous. This process is resolved (in theory complete resolution is required in asthma, but in practice, this is not checked or tested) with beta-2 agonists (e.g., salbutamol, salmeterol, albuterol) and can be aided by muscarinic receptor antagonists (e.g., ipratropium bromide), which act to reduce the inflammation and relax the bronchial musculature, as well as reducing mucus production 24.
Asthma Prevention
Because the exact cause of asthma is unknown, you may not be able to prevent asthma in yourself or your children. You or your child may develop asthma when the body’s immune system is still developing. Research suggests that you may be able to take some steps to help prevent asthma from developing. They include doing your best to keep your home free of dampness and mold, avoiding air pollution as much as possible, and making a healthy weight a priority for you and your children.
You can reduce asthma symptoms by avoiding triggers and substances that irritate the airways.
- Cover bedding with allergy-proof casings to reduce exposure to dust mites.
- Remove carpets from bedrooms and vacuum regularly.
- Use only unscented detergents and cleaning materials in the home.
- Keep humidity levels low and fix leaks to reduce the growth of organisms such as mold.
- Keep the house clean and keep food in containers and out of bedrooms. This helps reduce the possibility of cockroaches. Body parts and droppings from cockroaches can trigger asthma attacks in some people.
- If someone is allergic to an animal that cannot be removed from the home, the animal should be kept out of the bedroom. Place filtering material over the heating outlets to trap animal dander. Change the filter in furnaces and air conditioners often.
- Eliminate tobacco smoke from the home. This is the single most important thing a family can do to help someone with asthma. Smoking outside the house is not enough. Family members and visitors who smoke outside carry smoke residue inside on their clothes and hair. This can trigger asthma symptoms. If you smoke, now is a good time to quit.
- Avoid air pollution, industrial dust, and irritating fumes as much as possible.
- Take your medication as prescribed. Don’t change your medications without first talking to your doctor, even if your asthma seems to be improving. It’s a good idea to bring your medications with you to each doctor visit. Your doctor can make sure you’re using your medications correctly and taking the right dose.
- Pay attention to increasing quick-relief inhaler use. If you find yourself relying on your quick-relief inhaler, such as albuterol, your asthma isn’t under control. See your doctor about adjusting your treatment.
Stay away from asthma triggers
It is important to know what things make your asthma worse. These are called asthma “triggers.” Avoiding them is your first step toward feeling better.
Your homes can be filled with asthma triggers, found within:
- The air we breathe
- Furniture and carpets
- Your pets
Stay Away From Smoking
If you smoke, ask your health care provider for help quitting. No one should smoke in your house. This includes you and your visitors.
Smokers should smoke outside and wear a coat. The coat will keep smoke particles from sticking to their clothes. They should leave the coat outside or away from your child.
Ask people who work at your child’s day care, preschool, school, and anyone else who takes care of your child, if they smoke. If they do, make sure they do not smoke near your child.
Stay away from restaurants and bars that allow smoking. Or ask for a table as far away from smokers as possible.
Pollen
When pollen levels are high:
- Stay indoors and keep doors and windows closed. Use an air conditioner if you have one.
- Save outside activities for late afternoon or after a heavy rain.
- Wear a facemask while you are doing outdoor activities.
- DO NOT dry clothes outdoors. Pollen will stick to them. Have someone who does not have asthma cut the grass, or wear a facemask if you must do it.
Dust Mites
You can take several steps to limit exposure to dust mites.
- Wrap mattresses, box springs, and pillows in mite-proof covers.
- Wash bedding and pillows once a week in hot water (130°F to 140°F [54°C to 60°C]).
- If you can, get rid of upholstered furniture. Use wooden, leather, or vinyl furniture instead.
- Keep indoor air dry. Try to keep the humidity level lower than 50%.
- Wipe away dust with a damp cloth and vacuum once a week. Use a vacuum cleaner with a HEPA (high-efficiency particulate arrestor) filter.
- Replace wall-to-wall carpet with wood or other hard flooring.
- Keep stuffed toys off the beds, and wash them weekly.
- Replace slatted blinds and cloth draperies with pull-down shades. They will not collect as much dust.
- Keep closets clean and closet doors closed.
Mold Spores
Keeping indoor humidity at less than 50% will keep mold spores down. To do so:
- Keep sinks and tubs dry and clean.
- Fix leaky pipes.
- Empty and wash refrigerator trays that collect water from the freezer.
- Defrost your refrigerator often.
- Use an exhaust fan in the bathroom when you are showering.
- DO NOT let damp clothes sit in a basket or hamper.
- Clean or replace shower curtains when you see mold on them.
- Check your basement for moisture and mold.
- Use a dehumidifier to keep the air dry.
Pets can Make Asthma Worse
Keep pets with fur or feathers outside, if possible. If pets stay inside, keep them out of bedrooms and off upholstered furniture and carpets.
Wash pets once a week if possible.
If you have a central air conditioning system, use a HEPA filter to remove pet allergens from indoor air. Use a vacuum cleaner with HEPA filters.
Wash your hands and change your clothes after playing with your pet.
Roaches and Rodents
Keep kitchen counters clean and free of food crumbs. DO NOT leave dirty dishes in the sink. Keep food in closed containers.
DO NOT let trash pile up inside. This includes bags, newspapers, and cardboard boxes.
Use roach traps. Wear a dust mask and gloves if you touch or are near rodents.
Other Triggers to Watch Out for
DO NOT use wood-burning fireplaces. If you need to burn wood, use an airtight wood-burning stove.
DO NOT use perfumes or scented cleaning sprays. Use trigger sprays instead of aerosols.
Discuss any other possible triggers with your health care provider and how to avoid them.
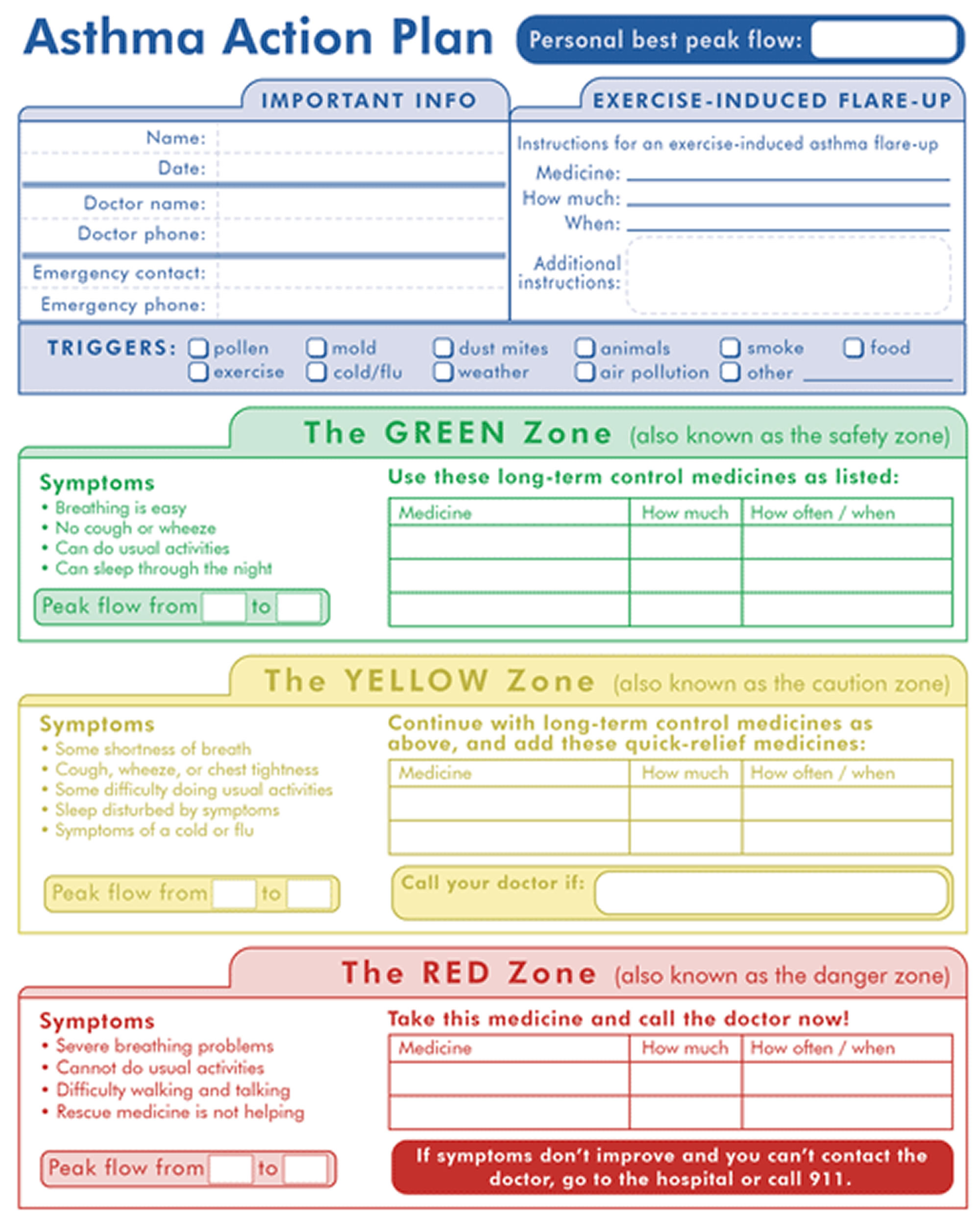
Asthma Action Plan
Early treatment is the most effective strategy for managing asthma exacerbations.
An asthma action plan is a care plan that you’ll develop with your doctor. The plan gives detailed instructions on how to manage asthma, including:
- what medicines you need and when
- what your asthma triggers are and how to avoid them
- how to manage a flare-up
- when to get emergency medical care
Following the plan can help you do normal everyday activities without having asthma symptoms.
Keeping an asthma diary is another way to help manage asthma. Tracking you symptoms and medicines will help you know when you are more likely to have a flare-up.
Your doctor may also recommend tracking your asthma symptoms or using a peak flow meter on a regular basis to monitor how well your treatment is controlling your asthma (see below how to use asthma peak flow meter). This handheld tool measures breathing ability. When peak flow readings drop, it’s a sign of narrowing airways.
By using these tools, taking medicines as prescribed and avoiding triggers, you’ll help keep yourself healthy and breathing well.
Figure 1. Asthma Action Plan
Management of Asthma Attacks (Flare-Ups)
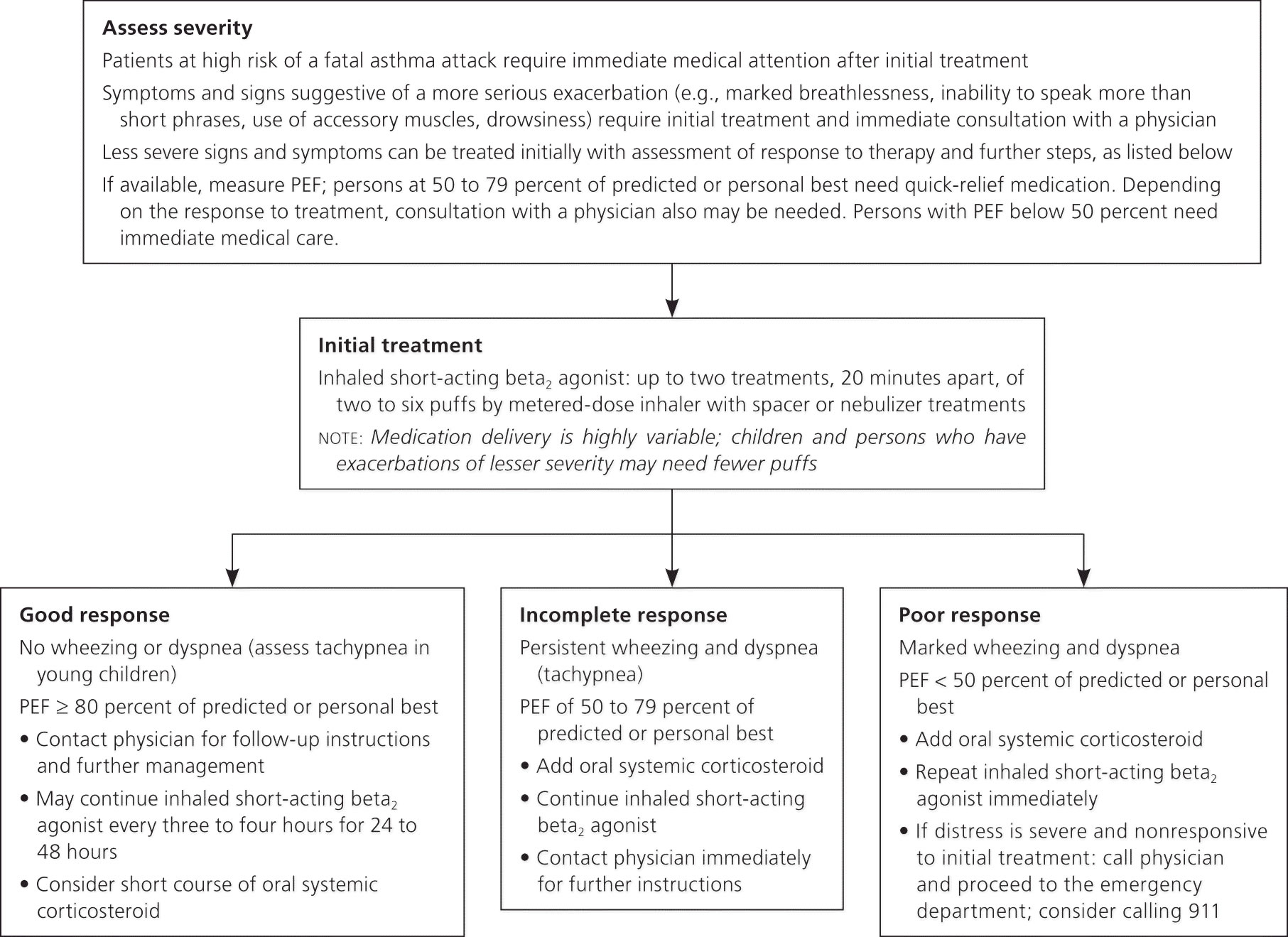
Footnote: Algorithm for home management of acute asthma exacerbations. (PEF = peak expiratory flow.)
[Source 26]Asthma Diagnosis
To diagnose asthma, doctors will ask questions about your health, problems with breathing, and family medical history. They’ll also ask about any allergies, illnesses, and exposure to things that may make your breathing worse.
You will have a physical exam and may have a lung function test. This usually involves testing breathing with a spirometer, a machine that analyzes airflow through the airways.
The diagnosis of asthma is based on the history of characteristic symptom patterns and evidence of variable expiratory airflow limitation. This should be documented from bronchodilator reversibility testing or other tests.
Exams and Tests for Asthma
The health care provider will use a stethoscope to listen to your lungs. Wheezing or other asthma-related sounds may be heard. Lung function tests often are done before and after taking a medication to open your airways called a bronchodilator, such as albuterol. If your lung function improves with use of a bronchodilator, it’s likely you have asthma.
Tests to measure lung function:
- Spirometry. This test estimates the narrowing of your bronchial tubes by checking how much air you can exhale after a deep breath and how fast you can breathe out. During the test, a technician will ask you to take a deep breath in. Then, you’ll blow as hard as you can into a tube connected to a small machine. The machine is called a spirometer. Your healthcare team may have you inhale, or breathe in, medicine that helps open your airways (bronchodilator) and then blow into the tube again. They can then compare your test results before and after taking the medicine. Some people feel lightheaded or tired from the required breathing effort.
- At a time when FEV1 is reduced, confirm that FEV1/FVC is reduced (it is usually >0.75–0.80 in adults, >0.90 in children 27
- Positive bronchodilator reversibility test
- Adults: increase in FEV1 of >12% and >200 mL (greater confidence if increase is >15% and >400 mL).
- Children: increase in FEV1 of >12% predicted
- Change measured 10–15 minutes after 200–400 mcg salbutamol (albuterol) or equivalent, compared with pre-bronchodilator readings. Positive test more likely if bronchodilator withheld before test: short-acting beta-agonist (SABA) ≥4 hours, twice-daily long-acting beta-agonist (LABA) 24 hours, once-daily long-acting beta-agonist 36 hours
- Excessive variability in twice-daily peak expiratory flow (PEF) over 2 weeks
- Adults: average daily diurnal PEF variability >10%*
- Children: average daily diurnal PEF variability >13%*
- *Daily diurnal PEF variability is calculated from twice daily PEF as (day’s highest minus day’s lowest) divided by (mean of day’s highest and lowest), averaged over one week.
- Significant increase in lung function after 4 weeks of anti-inflammatory treatment
- Adults: increase in FEV1 by >12% and >200 mL (or PEF† by >20%) from baseline after 4 weeks of treatment, outside respiratory infections. †For PEF, use the same meter each time, as PEF may vary by up to 20% between different meters. Bronchodilator reversibility may be lost during severe exacerbations or viral infections and airflow limitation may become persistent over time 28. If reversibility is not present at initial presentation, the next step depends on the availability of other tests and the urgency of the need for treatment. In a situation of clinical urgency, asthma treatment may be commenced and diagnostic testing arranged within the next few weeks
- Positive bronchial challenge test (usually only for adults)
- Fall in FEV1 from baseline of ≥20% with standard doses of methacholine, or ≥15% with standardized hyperventilation, hypertonic saline or mannitol challenge
- Excessive variation in lung function between visits (good specificity but poor sensitivity)
- Adults: variation in FEV1 of >12% and >200 mL between visits, outside of respiratory infections
- Children: variation in FEV1 of >12% in FEV 1 or >15% in PEF† between visits (may include respiratory infections). †For PEF, use the same meter each time, as PEF may vary by up to 20% between different meters. Bronchodilator reversibility may be lost during severe exacerbations or viral infections and airflow limitation may become persistent over time 28. If reversibility is not present at initial presentation, the next step depends on the availability of other tests and the urgency of the need for treatment. In a situation of clinical urgency, asthma treatment may be commenced and diagnostic testing arranged within the next few weeks
- Positive exercise challenge test
- Adults: fall in FEV1 of >10% and >200 mL from baseline
- Children: fall in FEV 1 of >12% predicted, or PEF >15%
- Peak expiratory flow (PEF). A peak flow meter is a simple device that measures how hard you can breathe out. Lower than usual peak flow readings are a sign that your lungs may not be working as well and that your asthma may be getting worse. Your doctor will give you instructions on how to track and deal with low peak flow readings.
Other tests to diagnose asthma include:
- Allergy testing — skin or a blood test to see if a person with asthma is allergic to certain substances. Allergy testing tell you if you’re allergic to pets, dust, mold or pollen. If allergy triggers are identified, your doctor may recommend allergy shots.
- Arterial blood gas (usually only done with people who are having a severe asthma attack)
- Chest x-ray — a chest X-ray can help identify any structural abnormalities or diseases (such as infection) that can cause or aggravate breathing problems.
- Methacholine challenge. Methacholine is a known asthma trigger. When inhaled, it will cause your airways to narrow slightly. If you react to the methacholine, you likely have asthma. This test may be used even if your initial lung function test is normal.
- Nitric oxide test also called fractional exhaled nitric oxide (FeNO) test. This test measures the amount of the gas nitric oxide in your breath. When your airways are inflamed — a sign of asthma — you may have higher than normal nitric oxide levels. This test isn’t widely available.
- Sputum eosinophils. This test looks for certain white blood cells (eosinophils) in the mixture of saliva and mucus (sputum) you discharge during coughing. Eosinophils are present when symptoms develop and become visible when stained with a rose-colored dye.
- Provocative testing for exercise and cold-induced asthma. In these tests, your doctor measures your airway obstruction before and after you perform vigorous physical activity or take several breaths of cold air.
Asthma treatment
The goals of asthma treatment are 29:
- Control airway swelling
- Stay away from substances that trigger your symptoms
- Help you to be able to do normal activities without asthma symptoms
Asthma treatment usually depends on your age, how serious your asthma is, and how your body responds to the medicines. Prevention and long-term control are key to stopping asthma attacks before they start. Treatment usually involves learning to recognize your triggers, taking steps to avoid triggers and tracking your breathing to make sure your medications are keeping symptoms under control. In case of an asthma flare-up, you may need to use a quick-relief inhaler.
You and your doctor should work as a team to create a treatment plan, called an asthma action plan, to manage your asthma. Follow your doctor’s instructions on taking medicines, eliminating asthma triggers, and monitoring symptoms.
Many guidelines recommend that patients with mild asthma should be treated with as-needed (PRN) short-acting beta-2 agonists (SABA) reliever alone 30. This dates back more than 50 years, to when asthma was thought of primarily as a disease of bronchoconstriction 31. However, airway inflammation is found in most patients with asthma, even in those with intermittent or infrequent symptoms 6. Although short-acting beta-2 agonist (SABA) provides quick relief of symptoms, short-acting beta-2 agonist (SABA)-only treatment is associated with increased risk of exacerbations and lower lung function 32. Regular use of short-acting beta-2 agonist (SABA) increases allergic responses and airway inflammation, and reduces the bronchodilator response to SABA when it is needed. Over-use of short-acting beta-2 agonist (SABA) (e.g. ≥3 canisters dispensed in a year) is associated with an increased risk of severe exacerbations. Dispensing of ≥12 short-acting beta-2 agonist (SABA) canisters in a year (and possibly even less than this) is associated with increased risk of asthma-related death 6.
Since 2021, the Global Initiative For Asthma (GINA) no longer recommends treatment of asthma in adults and adolescents with short-acting beta-2 agonists (SABA) alone, without inhaled corticosteroids (ICS) 6. There is strong evidence that short-acting beta-2 agonist (SABA)-only treatment, although providing short-term relief of asthma symptoms, does not protect patients from severe exacerbations, and are ineffective in treating the underlying inflammatory process and that regular or frequent use of short-acting beta-2 agonist (SABA) increases the risk of exacerbations. Patients treated with short-acting beta-2 agonist (SABA) alone are at risk of asthma-related death 33 and urgent asthma-related healthcare utilisation 34, both are reduced with regular use of inhaled corticosteroids (ICS). In fact, Suissa et al 33 showed a clear inverse dose-dependent relationship between number of inhaled corticosteroids (ICS) canisters used in a year and the rate ratio for death from asthma. The benefit of using inhaled corticosteroids (ICS) at Step 1/mild asthma was further reinforced in 2006 when the results of a 10-year asthma programme in Finland was published 35. Through a comprehensive educational programme for primary care that focused mainly on the premise that asthma is an inflammatory disease and requires anti-inflammatory treatment from the outset, the use of inhaled corticosteroids (ICS) increased from 33% to 85% with a parallel decrease in asthma-related hospital admissions and days off work 35. The Global Initiative For Asthma (GINA) now recommends that all adults and adolescents with asthma should receive inhaled corticosteroids (ICS)-containing controller treatment to reduce their risk of serious exacerbations and to control symptoms.
For adults and adolescents, the treatment options for mild asthma are 6:
- As-needed low dose inhaled corticosteroids (ICS)-formoterol (preferred), or
- Regular low dose inhaled corticosteroids (ICS), plus as-needed short-acting beta-2 agonist (SABA)
In adults and adolescents with mild asthma, treatment with as-needed low dose inhaled corticosteroids (ICS)-formoterol reduces the risk of severe exacerbations by about two-thirds compared with short-acting beta-2 agonist (SABA)-only treatment 9. Treatment with regular daily low dose inhaled corticosteroids (ICS), with as-needed short-acting beta-2 agonist (SABA), is highly effective in reducing asthma symptoms and reducing the risk of asthma-related exacerbations, hospitalization and death 9.
There are five steps in the management of chronic asthma 36; treatment is started depending on the severity and then escalated or de-escalated depending on the response to treatment.
- Step 1: The preferred controller is as needed low dose inhaled corticosteroid formoterol.
- Step 2: The preferred controllers are daily low dose inhaled corticosteroid (ICS) plus as-needed short-acting beta 2 agonists (SABA).
- Step 3: The preferred controllers are low dose inhaled corticosteroid (ICS) and long-acting beta 2 agonists (LABA) plus as-needed short-acting beta 2 agonists (SABA).
- Step 4: The preferred controller is a medium-dose inhaled corticosteroid and long-acting beta 2 agonist plus as-needed short-acting beta 2 agonists.
- Step 5: High dose inhaled corticosteroid and long-acting beta 2 agonist plus long-acting muscarinic antagonist (LAMA) (tiotropium bromide, brand name RESPIMAT)/anti-IgE.
Table 1. Comparison of adult asthma chronic management guidelines
| Global Initiative for Asthma 2021 | National Asthma Education and Prevention Program Guidelines 2021 | British Thoracic Society Guidelines 2019 | |
|---|---|---|---|
| Non Applicable | Intermittent Asthma: PRN SABA | Suspected Asthma: Can Consider Monitored Initiation of Low Dose ICS | |
| “Step 1″ | As-needed low dose ICS/formoterol OR ICS used at the same time as SABA | Regular low dose ICS + PRN SABA OR ICS used at the same time as SABA | Regular low dose ICS + PRN SABA |
| “Step 2″ | As needed low dose ICS/formoterol OR Regular low dose ICS + PRN SABA | Regular and as required low dose ICS/formoterol | Regular low ICS/LABA + PRN SABA OR Low dose maintenance and reliever ICS/LABA |
| “Step 3″ | Low dose maintenance and reliever ICS/formoterol OR Low dose maintenance ICS/LABA + PRN SABA | Regular and as required medium dose ICS/formoterol | Medium dose ICS/LABA +PRN SABA OR Low dose ICS/LABA + LTRA +PRN SABA |
| “Step 4″ | Medium dose maintenance ICS/formoterol + as needed low dose ICS-formoterol OR Medium/high dose maintenance ICS/LABA + PRN SABA | Daily medium-high dose ICS/LABA + LTRA or LAMA + PRN SABA Consider adding asthma biologic | Refer patient to specialist care for consideration of specialist therapies (including asthma biologics) |
| ‘Step 5″ | Add LAMA Consider high dose ICS/formoterol OR Add on LAMA, consider high dose ICS/LABA Refer for consideration of asthma biologic | Daily high-dose ICS/LABA + PRN SABA + OCS Consider adding asthma biologic |
Abbreviations: ICS = inhaled corticosteroids; SABA = short-acting beta-agonist; LABA = long-acting beta-agonist; LTRA = leukotriene receptor antagonist; OCS = oral corticosteroid; PRN = as needed.
[Source 30 ]Indications for hospital admission
If a patient has received three doses of an inhaled bronchodilator and shows no response, the following factors should be used to determine admission 2:
- The severity of airflow obstruction
- Duration of asthma
- Response to medications
- Adequacy of home support
- Any mental illness
Patients with life-threatening asthma are managed with high flow oxygen inhalation, systemic steroids, back to back nebulizations with short-acting beta-2 agonists, and short-acting muscarinic antagonists and intravenous magnesium sulfate. Early involvement of the intensive care team consultation helps to reduce mortality. In the case of near-fatal asthma, early intubation and mechanical ventilation are needed.
Asthma medications
There are two kinds of medicines for treating asthma 1:
- Control medicines also known as preventer help prevent attacks: Preventive, long-term control medications contain inhaled corticosteroids (ICS) reduce the swelling (inflammation) in your airways that leads to symptoms 37.
- Quick-relief (rescue) medicines for use during attacks. Quick-relief inhalers (bronchodilators) quickly open swollen airways that are limiting breathing. In some cases, allergy medications are necessary.
- Allergy medications. Allergy medications may help if your asthma is triggered or worsened by allergies. These include:
- Allergen-specific immunotherapy (AIT) may be a treatment option when allergy is a prominent trigger for asthma symptoms and exacerbations 38. Allergen-specific immunotherapy (AIT) can be delivered through two approaches: subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT). The rationale behind and proposed mechanism for allergen-specific immunotherapy (AIT) is it modifies the underlying allergic pathways leading to allergen-specific tolerance and suppression of inflammation with clinical benefits seen in daily symptoms and exacerbations 38.
- Allergy shots (immunotherapy) also called subcutaneous immunotherapy (SCIT). Over time, allergy shots gradually reduce your immune system reaction to specific allergens. You generally receive shots once a week for a few months, then once a month for a period of three to five years.
- House dust mites sublingual immunotherapy (SLIT) has been shown to delay time to exacerbation during inhaled corticosteroids (ICS) reduction in adults with suboptimally controlled asthma and house dust mites allergic rhinitis 39. The European Academy of Allergy and Clinical Immunology recommends house dust mites-allergen-specific immunotherapy as add-on treatment for house dust mites-driven allergic asthma as there is evidence it can reduce exacerbations and improve asthma control 40. However, compared to pharmacological and avoidance options, the benefits of allergen-specific immunotherapy (AIT) need to be weighed against the cost to the patient and health system, potential side effects and inconvenience of the prolonged course of therapy.
- Biologics also called monoclonal antibodies. These medications (monoclonal antibodies) — which include omalizumab (Xolair), mepolizumab (Nucala), dupilumab (Dupixent), reslizumab (Cinqair) and benralizumab (Fasenra) — are specifically for people who have severe asthma or the presence of type 2 (T2) inflammatory processes (see Table 2). T2 inflammation may be orchestrated by either (CD4+) Type 2 helper (Th2) lymphocytes or innate lymphoid cells group 2 (ILC2) 41. Type 2 helper (Th2) lymphocytes elaborate cytokines that have critical “asthma-genic” actions including interleukin (IL)-4, IL-5 and IL-13. IL-4 promotes production of IgE from B lymphocytes, increases expression of low-affinity CD23 (FCεRII) IgE receptors on B lymphocytes and macrophages while directing class switching of naïve CD4 T-helper lymphocytes to the T2 type 42. IL-13 shares a common receptor (IL-4Rα) with IL-4 and shows similar effects including promoting IgE production and CD23 expression 43. IL-4 and IL-13 also induce goblet cell metaplasia and MUC5AC production, favouring mucus production in the asthmatic airway 44. IL-5 is a key driver of eosinophilic processes, responsible for eosinophil migration into the asthmatic airway where they are a predominant cell type in T2 disease 45. The Global Initiative for the management of Asthma (GINA) proposed a multidimensional algorithm to define T2 status – any of blood eosinophil count (BEC)≥ 150 cells/μL, sputum eosinophilia ≥2%, Fractional Exhaled Nitric Oxide (FeNO)≥ 20ppb, clinically allergy-driven asthma, or on maintenance oral corticosteroids for asthma 9. The Global Initiative for the management of Asthma (GINA) estimated that 50% of severe asthma is T2 in nature 9. In line with that estimate, recent data from UK-SAR (the United Kingdom Severe Asthma Registry) classified 45% of subjects as T2 when that was defined as both blood eosinophil count (BEC)≥150cells/μL and Fractional Exhaled Nitric Oxide (FeNO)≥ 25ppb 46. However, emerging real-world data using broader perspectives suggests a greater extent of T2 status among patients with severe asthma 30. Moreover, currently available biologics fail to prevent all exacerbations.
- Allergen-specific immunotherapy (AIT) may be a treatment option when allergy is a prominent trigger for asthma symptoms and exacerbations 38. Allergen-specific immunotherapy (AIT) can be delivered through two approaches: subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT). The rationale behind and proposed mechanism for allergen-specific immunotherapy (AIT) is it modifies the underlying allergic pathways leading to allergen-specific tolerance and suppression of inflammation with clinical benefits seen in daily symptoms and exacerbations 38.
The right medications for you depend on a number of things — your age, symptoms, asthma triggers and what works best to keep your asthma under control.
For the best outcomes, inhaled corticosteroids (ICS)-containing treatment should be initiated as soon as possible after the diagnosis of asthma is made, because 6:
- Patients with even mild asthma can have severe exacerbations
- Low dose inhaled corticosteroids (ICS) markedly reduces asthma hospitalizations and death
- Low dose inhaled corticosteroids (ICS) is very effective in preventing severe exacerbations, reducing symptoms, improving lung function, and preventing exercise-induced bronchoconstriction, even in patients with mild asthma
- Early treatment with low dose inhaled corticosteroids (ICS) is associated with better lung function than if symptoms have been present for more than 2–4 years
- Patients not taking inhaled corticosteroids (ICS) who experience a severe exacerbation have lower long-term lung function than those who have started inhaled corticosteroids (ICS)
- In occupational asthma, early removal from exposure and early treatment increase the probability of recovery
Your treatment should be flexible and based on changes in your symptoms. Your doctor should ask about your symptoms at each visit. Based on your signs and symptoms, your doctor can adjust your treatment accordingly. For example, if your asthma is well controlled, your doctor may prescribe less medication. If your asthma isn’t well controlled or is getting worse, your doctor may increase your medication and recommend more-frequent visits.
Table 2. Current Biologic agents in Severe Asthma. Targets, Eligibility, Dosing Regimen and Real World Impact
| Biologic Name | Molecular Target | Eligibility Criteria for Adults (Based on EMA) | Dosing Regimen | Real World Impacts |
|---|---|---|---|---|
| Omalizumab | Free IgE | As add-on therapy to improve asthma control in patients with severe persistent allergic asthma who have a positive skin test or in vitro reactivity to a perennial aeroallergen and who have reduced lung function (FEV1 <80%) as well as frequent daytime symptoms or night-time awakenings and who have had multiple documented severe asthma exacerbations despite daily high-dose inhaled corticosteroids, plus a long-acting inhaled beta2-agonist. | 2–4 weekly, subcutaneously based on Total IgE level and body weight | Improvement in FEV1, Asthma control, exacerbations, OCS requirements, healthcare utilisation |
| Mepolizumab | IL-5 | Severe refractory eosinophilic asthma | 100mg, 4 weekly, subcutaneously | Improvement in asthma control, exacerbations, OCS requirements, healthcare utilisation, AQLQ, FEV1 |
| Reslizumab | IL-5 | Severe eosinophilic asthma inadequately controlled despite high dose inhaled corticosteroids plus another medicinal product for maintenance treatment. | 3mg/kg 4 weekly, intravenously over 20–50 minutes | Improvement in exacerbations, OCS requirements, FEV1, healthcare utilisation |
| Benralizumab | Alpha subunit of IL-5 receptor | As an add on maintenance treatment in adult patients with severe eosinophilic asthma inadequately controlled despite high-dose inhaled corticosteroids plus long acting β agonists. | 30mg 4 weekly for the first three doses, then 8 weekly subcutaneously | Improvement in exacerbations, OCS requirements, healthcare utilisation, FEV1, AQLQ |
| Dupilumab | Alpha subunit of IL-4 receptor | Add-on maintenance treatment for severe asthma with type 2 inflammation characterised by raised blood eosinophils and/or raised fraction of exhaled nitric oxide, who are inadequately controlled with high dose ICS plus another medicinal product for maintenance treatment. | If on OCS + moderate-severe atopic eczema/CRSwNP: loading dose of 600mg followed by 300mg 2 weekly 400mg loading dose followed by 200mg 2 weekly, subcutaneously | Improvement in asthma control, exacerbations, FEV1, OCS requirements |
Abbreviations: IgE = immunoglobulin E; FEV1 = forced expiratory volume in 1 second; OCS = oral corticosteroid; AQLQ = asthma quality of life questionnaire; ICS = inhaled corticosteroids; IgE = Immunoglobulin E; IL-5 = Interleukin-5; IL-4 = Interleukin-4.
[Source 30 ]Asthma Quick-Relief Asthma Medications
Asthma quick-relief (rescue) medicines work fast to control asthma symptoms, for rapid, short-term symptom relief during an asthma attack. You take quick-relief (rescue) medications when you are coughing, wheezing, having trouble breathing, or having an asthma attack. They are also called rescue drugs.
These medicines are called “bronchodilators” because they open (dilate) and help relax the muscles of your airways (bronchi). They may also be used before exercise if your doctor recommends it.
You and your doctor can make a plan for the quick-relief drugs that work for you. This plan will include when you should take them and how much you should take.
Plan ahead. Make sure you do not run out. Take enough with you when you travel.
Asthma Quick-Relief Asthma Medications are taken:
- For coughing, wheezing, trouble breathing, or an asthma attack
- Just before exercising to help prevent asthma symptoms caused by exercise
Tell your doctor if you are using quick-relief medicines twice a week or more. If so, your asthma may not be under control and your doctor may need to change your dose of daily control drugs.
Asthma Quick-relief medicines include:
- Short-acting inhaled bronchodilators
- Oral corticosteroids for when you have an asthma attack that is not going away
A severe asthma attack requires a checkup by a doctor. You may also need a hospital stay. There, you will likely be given oxygen, breathing assistance, and medicines given through a vein (IV).
If you have an asthma flare-up, a quick-relief inhaler can ease your symptoms right away. But you shouldn’t need to use your quick-relief inhaler very often if your long-term control medications are working properly. Keep a record of how many puffs you use each week. If you need to use your quick-relief inhaler more often than your doctor recommends, see your doctor. You probably need to adjust your long-term control medication.
Short-acting Beta-agonists Asthma Inhalers
Short-acting beta-agonists (SABAs) are the most common quick-relief drugs for treating asthma attacks. They can be used just before exercising to help prevent asthma symptoms caused by exercise. They work by relaxing the muscles of your airways, and this lets you breathe better during an attack.
Short-acting beta agonists can be taken using a portable, hand-held inhaler or a nebulizer, a machine that converts asthma medications to a fine mist. They’re inhaled through a face mask or mouthpiece.
Tell your doctor if you are using quick-relief medicines twice a week or more to control your asthma symptoms. Your asthma may not be under control, and your doctor may need to change your dose of daily control drugs.
Some quick-relief asthma inhalers include:
- Albuterol (ProAir HFA, Proventil HFA, Ventolin HFA)
- Levalbuterol (Xopenex, Xopenex HFA)
- Metaproterenol
- Terbutaline
Quick-relief asthma inhalers may cause these side effects:
- Anxiety.
- Tremor (your hand or another part of your body may shake).
- Restlessness.
- Headache.
- Fast and irregular heartbeats. Call your doctor right away if you have this side effect.
Oral corticosteroids
Your doctor might prescribe oral corticosteroids when you have an asthma attack that is not going away. These are medicines that you take by mouth as pills, capsules, or liquids. Oral corticosteroids relieve airway inflammation caused by severe asthma. Oral steroids are not quick-relief medicines, but are often given for 7 to 14 days when your symptoms flare-up. They can cause serious side effects when used long term, so these drugs are used only on a short-term basis to treat severe asthma symptoms.
Oral steroids include:
- Prednisone (Prednisone Intensol, Rayos)
- Prednisolone
- Methylprednisolone (Medrol, Depo-Medrol, Solu-Medrol).
Anticholinergic agents
Like other bronchodilators, ipratropium (Atrovent HFA) and tiotropium (Spiriva, Spiriva Respimat) act quickly to immediately relax your airways, making it easier to breathe. Anticholinergic agents are mostly used for emphysema and chronic bronchitis, but can be used to treat asthma.
Long-term asthma control medications
Long-term asthma control medications are also called maintenance or control medicines. They are used to prevent symptoms in people with moderate to severe asthma. Long-term asthma control medications keep asthma under control on a day-to-day basis and make it less likely you’ll have an asthma attack. You must take them every day for them to work. Take them even when you feel OK.
Some long-term asthma control medications are breathed in (inhaled), such as steroids and long-acting beta-agonists. Others are taken by mouth (orally). Your doctor will prescribe the right medicine for you.
Asthma – control drugs
Control medicines for asthma are drugs you take to control your asthma symptoms. You must take them every day for them to work. You and your doctor can make a plan for the medicines that work for you. This plan will include when you should take them and how much you should take.
You may need to take these medicines for at least a month before you start to feel better.
Take the medicines even when you feel OK. Take enough with you when you travel. Plan ahead. Make sure you do not run out.
Inhaled Corticosteroids
Inhaled corticosteroids (ICS) prevent your airways from swelling in order to help keep your asthma symptoms away. Inhaled steroids are used with a metered dose asthma inhaler (MDI) and spacer. Or they may be used with a dry powder inhaler.
Inhaled corticosteroids include:
- fluticasone propionate (Flovent HFA, Flovent Diskus, Xhance),
- budesonide (Pulmicort Flexhaler, Pulmicort Respules, Rhinocort),
- ciclesonide (Alvesco),
- beclomethasone (Qvar Redihaler),
- mometasone (Asmanex HFA, Asmanex Twisthaler)
- fluticasone furoate (Arnuity Ellipta).
You should use an inhaled steroid every day, even if you do not have symptoms.
You may need to use these medications for several days to weeks before they reach their maximum benefit. Unlike oral corticosteroids, inhaled corticosteroids have a relatively low risk of serious side effects.
After you use it, rinse your mouth with water, gargle, and spit it out.
If your child cannot use an inhaler, your doctor will give you a drug to use with a nebulizer. This machine turns liquid medicine into a spray so your child can breathe the medicine in.
Long-Acting Beta-agonist Asthma Inhalers
Long-acting beta-2-agonists (LABAs) include salmeterol and formoterol, have 12-hour duration of action and are used with a twice-daily dosing regimen. Long-acting beta-2-agonists (LABAs) relax the muscles of your airways to help keep your asthma symptoms away.
Normally, you use these medicines only when you are using an inhaled steroid drug (ICS) and you still have symptoms. DO NOT take these long-acting medicines alone.
Use this medicine every day, even if you do not have symptoms.
Combination Therapy
Your doctor may ask you to take both a steroid drug and a long-acting beta-agonist drug. It may be easier to use an inhaler that has both drugs in them.
Combination inhalers containing a long-acting beta agonist along with a corticosteroid include:
- fluticasone-salmeterol (Advair HFA, Airduo Digihaler, others),
- budesonide-formoterol (Symbicort),
- formoterol-mometasone (Dulera)
- fluticasone furoate-vilanterol (Breo Ellipta)
Leukotriene Modifiers
Leukotriene modifiers also called leukotriene receptor antagonist (LTRA), are used to prevent asthma symptoms. Leukotriene modifiers come in tablet or pill form and can be used together with a steroid inhaler.
Leukotriene modifiers include:
- montelukast (Singulair): Montelukast has been linked to psychological reactions, such as agitation, aggression, hallucinations, depression and suicidal thinking. Seek medical advice right away if you experience any of these reactions.
- zafirlukast (Accolate)
- zileuton (Zyflo)
Cromolyn
Cromolyn helps prevent swelling in your airways when you are around allergens or other asthma triggers. Cromolyn is a medicine that may prevent asthma symptoms. It can be used in a nebulizer, so it may be easy for young children to take.
Theophylline
Theophylline (Theo-24, Elixophyllin, Theochron) is a daily pill that helps keep the airways open by relaxing the muscles around the airways. Theophylline (Theo-24, Elixophyllin, Theochron) is not used as often as other asthma medications and requires regular blood tests.
Azithromycin
Azithromycin is macrolide antibiotic that has antibacterial and anti-inflammatory effects. Add-on azithromycin (three times a week) can be considered after specialist referral for adult patients with persistent symptomatic asthma despite high dose ICS-LABA. Before considering add-on azithromycin, sputum should be checked for atypical mycobacteria, ECG should be checked for long QTc (and re-checked after a month on treatment), and the risk of increasing antimicrobial resistance should be considered 47. Airway abundance of Haemophilus influenzae has been shown to predict a more favourable response to azithromycin 48 and in a personalized approach to asthma management prospective assessment for the presence of Haemophilus influenza should be used to facilitate the identification of patients for this treatment. Diarrhea is more common with azithromycin 500mg 3 times a week 49. Treatment for at least 6 months is suggested, as a clear benefit was not seen by 3 months in the clinical trials 49. The evidence for this recommendation includes a meta-analysis of two clinical trials 49, 50 in adults with persistent asthma symptoms that found reduced asthma exacerbations among those taking medium or high dose ICS-LABA who had either an eosinophilic or non-eosinophilic profile and in those taking high dose ICS-LABA 51. The option of add-on azithromycin for adults is recommended only after specialist consultation because of the potential for development of resistance at the patient or population level 49.
Bronchial thermoplasty
Bronchial thermoplasty is used for severe asthma that doesn’t improve with inhaled corticosteroids or other long-term asthma medications. It isn’t widely available nor right for everyone.
During bronchial thermoplasty, your doctor inserts a tube called a bronchoscope into your mouth. The bronchoscope has a camera at the end. Your doctor will guide the bronchoscope into your airways to see inside them. Your doctor will then apply heat to the muscles along the airways. This makes them thinner and helps prevent them from narrowing. This limits the ability of the airways to tighten, making breathing easier and possibly reducing asthma attacks. The therapy is generally done over three outpatient visits.
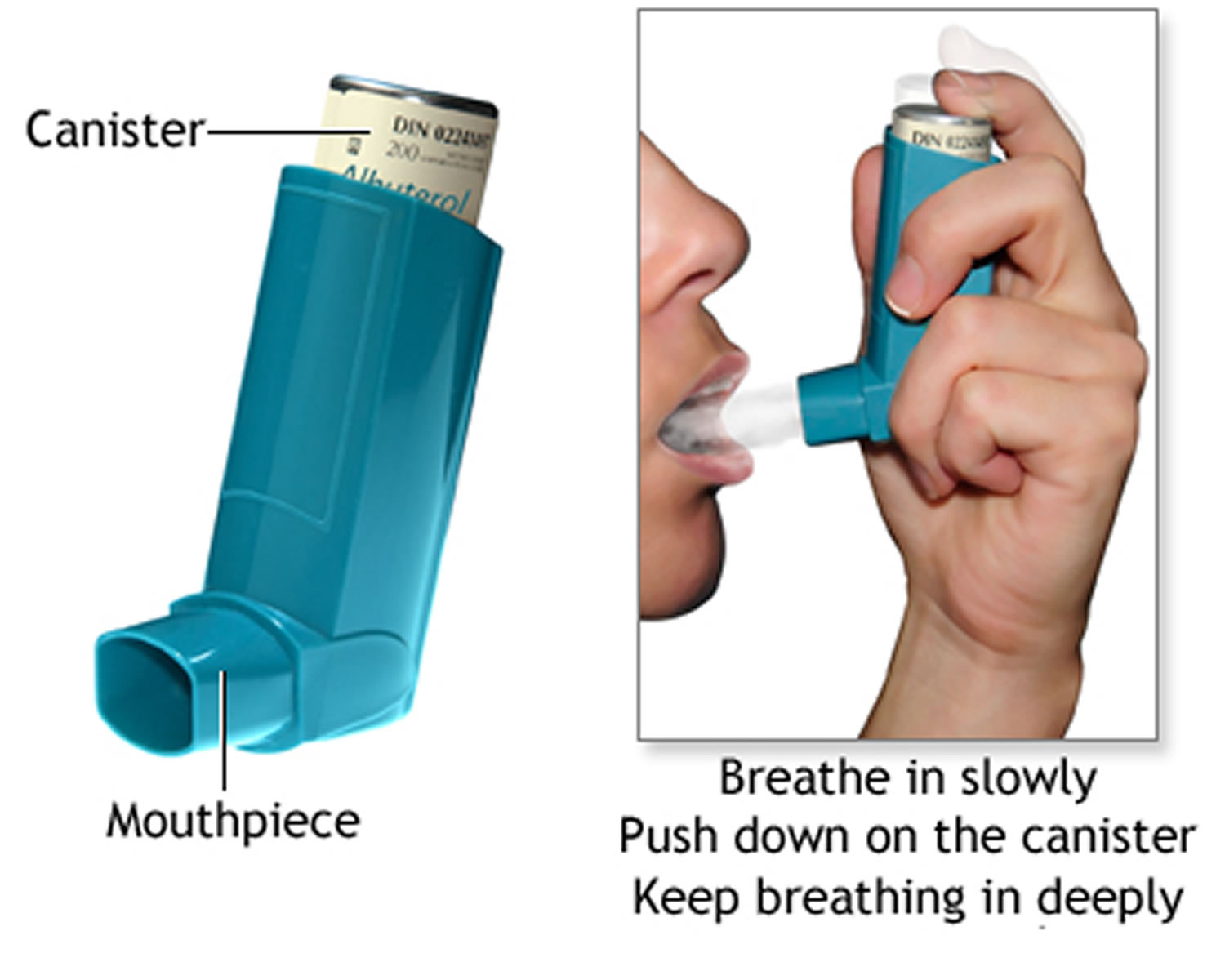
How to use asthma inhalers – without a spacer
Using a metered-dose asthma inhaler (MDI) seems simple. But many people do not use them the right way. If you use your metered-dose asthma inhaler (MDI) the wrong way, less medicine gets to your lungs and most remains in the back of your mouth 52. If you have a spacer, use it. It helps get more medicine into your airways.
- The instructions below are not for dry powder inhalers. They have different instructions (see below).
Getting Ready
- Take off the cap and shake the inhaler hard.
- If you have not used the inhaler in a while, you may need to prime it. See the instructions that came with your inhaler for how to do this.
- Breathe out all the way.
- Hold the inhaler 1 to 2 inches (2.5 to 5 centimeters) in front of your mouth (about the width of 2 fingers).
Breathe in Slowly
- Start breathing in slowly through your mouth, then press down on the inhaler 1 time.
- Keep breathing in slowly, as deeply as you can.
Hold Your Breath
- If you can, hold your breath as you slowly count to 10. This lets the medicine reach deep into your lungs.
- If you are using inhaled, quick-relief medicine (beta-agonists), wait about 1 minute before you take your next puff. You do not need to wait a minute between puffs for other medicines.
- After using your asthma inhaler, rinse your mouth with water, gargle, and spit. This helps reduce side effects from your medicine.
Figure 2. Using asthma inhalers without a spacer
Keep Your Asthma Inhaler Clean
Look at the hole where the medicine sprays out of your inhaler. If you see powder in or around the hole, clean your inhaler.
- Remove the metal canister from the L-shaped plastic mouthpiece.
- Rinse only the mouthpiece and cap in warm water.
- Let them air dry overnight.
- In the morning, put the canister back inside. Put the cap on.
- DO NOT rinse any other parts.
Replacing Your Asthma Inhaler
Most inhalers come with counters on the canister. Keep an eye on the counter and replace the inhaler before you run out of medicine.
DO NOT put your canister in water to see if it is empty. This does not work.
Bring your inhaler to your clinic appointments. Your doctor can make sure you are using it the right way.
Storing Your Inhaler
Store your inhaler at room temperature. It may not work well if it is too cold. The medicine in the canister is under pressure. So make sure you do not get it too hot or puncture it.
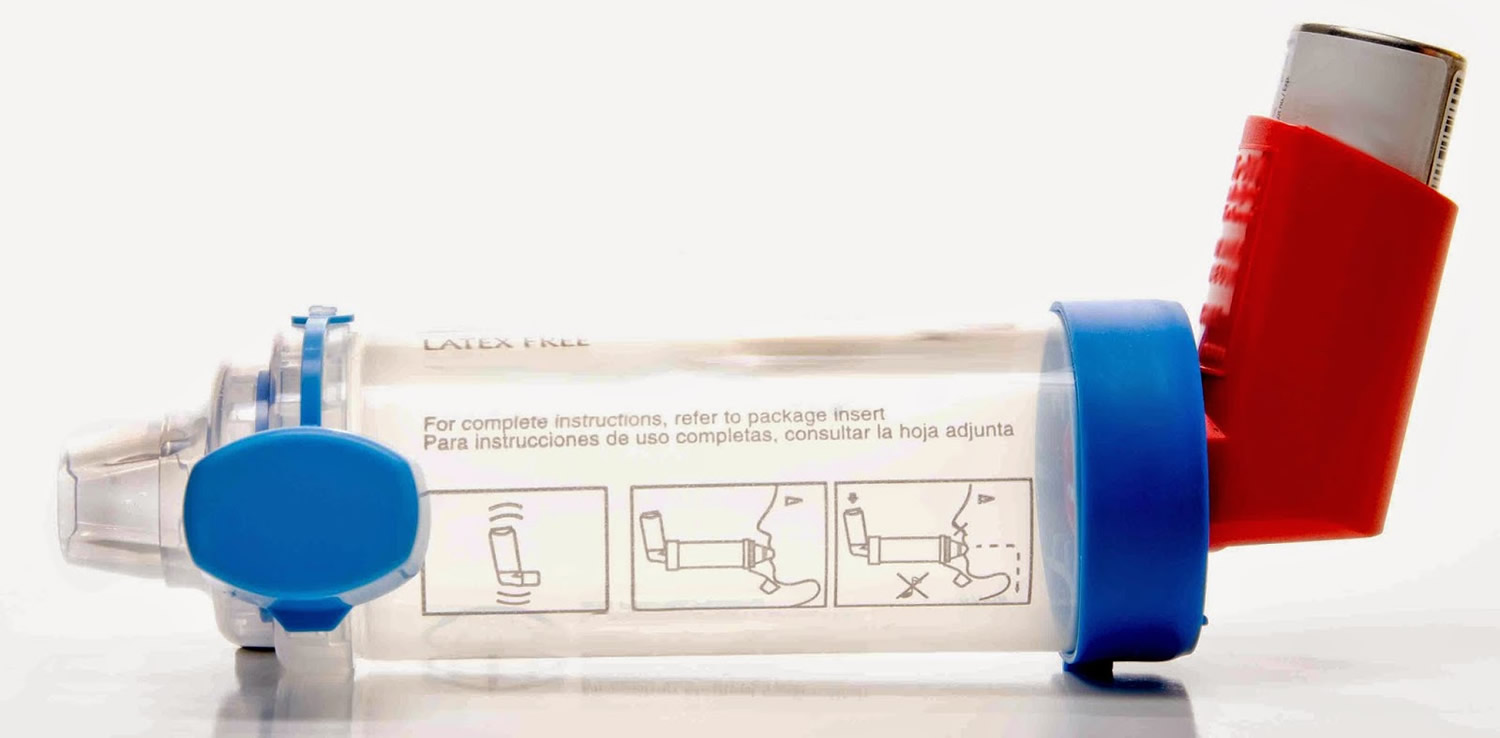
How to use asthma inhalers – with a spacer
Metered-dose asthma inhalers (MDIs) usually have 3 parts:
- A mouthpiece
- A cap that goes over the mouthpiece
- A canister full of medicine
If you use your asthma inhaler the wrong way, less medicine gets to your lungs. A spacer device will help. The spacer connects to the mouthpiece. The inhaled medicine goes into the spacer tube first. Then you take 2 deep breaths to get the medicine into your lungs. Using a spacer wastes a lot less medicine than spraying the medicine into your mouth.
Spacers come in different shapes and sizes. Ask your doctor which spacer is best for you or your child. Almost all children can use a spacer. You do not need a spacer for dry powder inhalers.
The steps below tell you how to take your medicine with a spacer 52.
Getting Ready
- Take the cap off the inhaler and spacer.
- Shake the inhaler hard.
- Attach the spacer to the inhaler.
- If you have not used the inhaler in a while, you may need to prime it. See the instructions that came with your inhaler for how to do this.
- Breathe out gently to empty your lungs.
Breathe in Slowly
- Put the spacer between your teeth and close your lips tightly around it.
- Keep your chin up.
- Start breathing in slowly through your mouth.
- Spray 1 puff into the spacer by pressing down on the inhaler.
- Keep breathing in slowly. Breathe as deeply as you can.
Hold Your Breath
- Take the spacer out of your mouth.
- Hold your breath as you count to 10, if you can.
- Pucker your lips and slowly breathe out through your mouth.
- After using your inhaler, rinse your mouth with water, gargle, and spit. This helps reduce side effects from your medicine.
Figure 3. Using asthma inhaler with a spacer
Keep Your Asthma Inhaler Clean
Look at the hole where the medicine sprays out of your inhaler. If you see powder in or around the hole, clean your inhaler. First, remove the metal canister from the L-shaped plastic mouthpiece. Rinse only the mouthpiece and cap in warm water. Let them air dry overnight. In the morning, put the canister back inside. Put the cap on. DO NOT rinse any other parts.
Replacing Your Asthma Inhaler
Most inhalers come with counters on the canister. Keep an eye on the counter and replace the inhaler before you run out of medicine.
DO NOT put your canister in water to see if it is empty. This does not work.
Storing Your Asthma Inhaler
Store your inhaler at room temperature. It may not work well if it is too cold. The medicine in the canister is under pressure. So make sure not to get it too hot or puncture it.
How to use Dry Powder Asthma Inhalers
A dry powder asthma inhaler delivers pre-set doses of medicine in powder form. The medicine gets to your airways when you take a deep, fast breath in from the inhaler. To keep your asthma under control, it is important to take your medicine as prescribed by your doctor or other health care professional and to use the proper technique to deliver the medicine to your lungs. If you don’t use your asthma inhaler correctly, you won’t get the medicine you need.
Here are general steps for how to use and clean a dry powder inhaler. Be sure to read the instructions that come with your asthma inhaler. Ask your doctor, pharmacist, or other health care professional (such as nurse practitioner, physician assistant, nurse, respiratory therapist, or asthma educator) to show you how to use your inhaler. Review your technique at each follow-up visit.
- Remove cap and hold inhaler upright (like a rocket). If the inhaler is a Diskus®, hold it flat (like a flying saucer).
- Load a dose of medicine according to manufacturer’s instructions (each brand of inhaler is different; you may have to prime the inhaler the first time you use it). Do not shake the inhaler.
- Stand up or sit up straight.
- Take a deep breath in and blow out completely to empty your lungs. Do NOT blow into the inhaler.
- Place the mouthpiece of the inhaler in your mouth and close your lips around it to form a tight seal.
- Take a fast, deep, forceful breath in through your mouth.
- Hold your breath and count to 10.
- Take the inhaler out of your mouth. Breathe out slowly, facing away from the inhaler.
- If you are supposed to take more than 1 inhalation of medicine per dose, wait 1 minute and repeat steps 2 through 8.
- When you finish, put the cover back on the inhaler or slide the cover closed. Store the inhaler in a cool, dry place (not in the bathroom).
- If using an inhaled corticosteroid, rinse out your mouth with water and spit it out. Rinsing helps to prevent an infection in the mouth.
Keep Your Asthma Dry Powder Inhaler Clean
- Wipe the mouthpiece at least once a week with a dry cloth.
- Do NOT use water to clean the dry powder inhaler.
Figure 4. Asthma dry powder inhalers

How to use Asthma Nebulizer
A nebulizer is a machine that delivers medicine in a fine, steady mist. It is easy and pleasant to breathe the asthma medicine into your lungs this way. If you have asthma, you may not need to use a nebulizer. You may use an inhaler instead, which is usually just as effective. But a nebulizer can deliver medicine with less effort than an inhaler. You and your doctor can decide if a nebulizer is the best way to get the medicine you need. The choice of device may be based on whether you find a nebulizer easier to use and what type of medicine you take.
To keep your asthma under control, it is important to take your asthma medicine as prescribed by your doctor or other health care professional and to use the proper technique to deliver the medicine to your lungs. If you don’t use your asthma nebulizer correctly, you won’t get the medicine you need.
Most nebulizers are small, so they are easy to transport. Also, most nebulizers also work by using air compressors. A different kind, called an ultrasonic nebulizer, uses sound vibrations. This kind of nebulizer is quieter, but costs more.
Here are general steps for how to use and clean a asthma nebulizer. Be sure to read the instructions that come with your nebulizer. Ask your doctor, pharmacist, or other health care professional (such as nurse practitioner, physician assistant, nurse, respiratory therapist, or asthma educator) to show you how to use your nebulizer. Review your technique at each follow-up visit.
- Wash hands well.
- Put together the nebulizer machine, tubing, medicine cup, and mouthpiece or mask according to manufacturer’s instructions.
- Put the prescribed amount of asthma medicine into the medicine cup. If your medicine comes in a pre-measured capsule or vial, empty it into the cup.
- Place the mouthpiece in your mouth and close your lips around it to form a tight seal. If your child uses a mask, make sure it fits snugly over your child’s nose and mouth. Never hold the mouthpiece or mask away from the face.
- Turn on the nebulizer machine. You should see a light mist coming from the back of the tube opposite the mouthpiece or from the mask.
- Take normal breaths through the mouth while the machine is on. Continue treatment until the medicine cup is empty or the mist stops, about 10 minutes.
- Take the mouthpiece out of your mouth (or remove mask) and turn off the machine.
- If using an inhaled corticosteroid, rinse mouth with water and spit it out. If using a mask, also wash the face.
How To Clean and Store Asthma Nebulizer after each treatment:
- Wash hands well.
- Wash the medicine cup and mouthpiece or mask with warm water and mild soap. Do NOT wash the tubing.
- Rinse well and shake off excess water. Air dry parts on a paper towel.
Once a week:
Disinfect nebulizer parts to help kill any germs. Follow instructions for each nebulizer part listed in the package insert. Always remember:
- Do NOT wash or boil the tubing.
- Air dry parts on a paper towel.
Between uses:
- Store nebulizer parts in a dry, clean plastic storage bag. If the nebulizer is used by more than one person, keep each person’s medicine cup, mouthpiece or mask, and tubing in a separate, labeled bag to prevent the spread of germs.
- Wipe surface with a clean, damp cloth as needed. Cover nebulizer machine with a clean, dry cloth and store as manufacturer instructs.
- Replace medicine cup, mouthpiece, mask, tubing, filter, and other parts according to manufacturer’s instructions or when they appear worn or damaged.
Figure 5. Asthma nebulizer with a mask (for young children)

Figure 6. Asthma nebulizer with a mouthpiece (for teens and adults)

How to use your peak flow meter for Asthma
A peak flow meter is a small device that helps you check how well your asthma is controlled. Peak flow meters are most helpful if you have moderate to severe persistent asthma.
Figure 7. Peak Flow Meter for Asthma

How to Measure Peak Flow
Measuring your peak flow can tell you and your health care provider how well you blow air out of your lungs. If your airways are narrowed and blocked due to asthma, your peak flow values drop.
You can check your peak flow at home. Here are the basic steps:
- Move the marker to the bottom of the numbered scale.
- Stand up straight.
- Take a deep breath. Fill your lungs all the way.
- Hold your breath while you place the mouthpiece in your mouth, between your teeth. Close your lips around it. DO NOT put your tongue against or inside the hole.
- Blow out as hard and fast as you can in a single blow. Your first burst of air is the most important. So blowing for a longer time will not affect your result.
- Write down the number you get. But, if you coughed or did not do the steps right, do not write down the number. Instead, do the steps over again.
- Move the marker back to the bottom and repeat all these steps 2 more times. The highest of the 3 numbers is your peak flow number. Write it down in your log chart.
Many children under age 5 cannot use a peak flow meter very well. But some are able to. Start using peak flow meters before age 5 to get your child used to them.
Find Your Personal Best
To find your personal best peak flow number, take your peak flow each day for 2 to 3 weeks. Your asthma should be under control during this time. To finding your personal best, take your peak flow as close to the following times of day as you can:
- Between noon and 2 p.m. each day
- Each time after you take your quick-relief medicine to relieve symptoms
- Any other time your provider tells you to
These times for taking your peak flow are only for finding your personal best.
Write down the number you get for each peak flow reading. The highest peak flow number you had during the 2 to 3 weeks is your personal best.
Ask your provider to help you fill out an asthma action plan. This plan should tell you when to call the doctor for help and when to use medicines if your peak flow drops to a certain level.
Your personal best can change over time. Ask your doctor when you should check for a new personal best.
Use Your Peak Flow Meter Every Day
Once you know your personal best, make taking your peak flow a habit. Take your peak flow:
- Every morning when you wake up, before you take medicine. Make this part of your daily morning routine.
- When you are having asthma symptoms or an attack.
- After you take medicine for an attack. This can tell you how bad your asthma attack is and if your medicine is working.
- Any other time your doctor tells you to.
Check to see which zone your peak flow number is in. Do what your provider told you to do when you are in that zone. This information should be in your action plan. If you use more than one peak flow meter (such as one at home and another one at school or work), be sure that all of them are the same brand.
Home remedies for asthma
- Know the asthma symptoms to watch for.
- Know how to take your peak flow reading and what it means.
- Know which triggers make your asthma worse and what to do when this happens.
- Know how to care for your asthma when you exercise.
Asthma action plans are written documents for managing asthma.
An asthma action plan should include:
- Instructions for taking asthma medicines when your condition is stable
- A list of asthma triggers and how to avoid them
- How to recognize when your asthma is getting worse, and when to call your provider
A peak flow meter is a simple device to measure how quickly you can move air out of your lungs.
- It can help you see if an attack is coming, sometimes even before symptoms appear. Peak flow measurements help let you know when you need to take medicine or other action.
- Peak flow values of 50% to 80% of your best results are a sign of a moderate asthma attack. Numbers below 50% are a sign of a severe attack.
Outlook (Prognosis) for Asthma
Asthma accounts for 1 death per 100,000 people in some countries 2. The mortality is related to lung function and is exacerbated by smoking. Factors that affect mortality include age more than 40 years, cigarette smoking more than 20 pack-years, blood eosinophilia, FEV1 of 40-70% of predicted, and greater reversibility 53. Asthma leads to loss of time from work and school; it also leads to multiple hospital admissions increasing the cost of healthcare. Poorly controlled asthma can be disabling and leads to poor quality of life. With proper self-management and medical treatment, most people with asthma can lead a normal life.
Possible complications of asthma
The complications of asthma can be severe, and may include:
- Death
- Decreased ability to exercise and take part in other activities
- Lack of sleep due to nighttime symptoms
- Permanent changes in the function of the lungs
- Persistent cough
- Trouble breathing that requires breathing assistance (ventilator).
- Comorbidities (i.e., cardiovascular disease or other chronic lung disease)
- Difficulty perceiving airway obstruction or severity of exacerbation
- Illicit drug use
- Low socioeconomic status or inner-city residence
- Major psychosocial problems or psychiatric disorders
- Previous severe exacerbation (e.g., intubation or admission to intensive care unit for asthma)
- Two or more hospitalizations or three or more emergency department visits in the past year
- Two or more refills of short-acting beta2 agonists per month
Living with asthma
With the treatments available today, most people who have asthma are able to manage the disease. They may have few symptoms. They can live normal, active lives and sleep through the night without interruption from asthma.
Treating symptoms when you first notice them is important. This will help prevent a severe asthma attack. Severe asthma attacks may require emergency care. They can even be fatal.
Make healthy lifestyle changes
Your doctor may talk to you about healthy lifestyle changes to help keep asthma symptoms in check.
- Aim for a healthy weight. Being overweight and having obesity can make asthma harder to manage. Talk to your doctor about programs that can help. Even a 5% to 10% weight loss can help symptoms.
- Choose heart-healthy foods. Eating more fruits and vegetables can provide important health benefits.
- Get regular physical activity. Even though exercise is an asthma trigger for some people, you should not avoid it. Physical activity is an important part of a healthy lifestyle. Talk with your doctor about what level of physical activity is right for you. Ask about medicines that can help you stay active.
- Manage stress. Learn breathing and relaxation techniques, which can help symptoms. Meet with a mental health professional if you have anxiety, depression, or panic attacks.
- Quit smoking or avoid secondhand smoke. Smoking tobacco and inhaling smoke from secondhand smoke make asthma harder to treat. Heating tobacco and inhaling (vaping) electronic cigarettes (e-cigarettes) and being exposed to secondhand vapor may also be linked to asthma symptoms. NIH-funded research suggests that an ingredient in the tobacco plant that makes you addicted to smoking (nicotine), and flavorings found in vaping e-cigarettes can damage your lungs.
- Try to get good-quality sleep. Getting quality sleep can sometimes be hard with asthma. Develop healthy sleep habits by going to sleep and getting up at regular times, following a calming bedtime routine, and keeping your bedroom cool and dark.
- Sveum R, Bergstrom J, Brottman G, et al. Institute for Clinical Systems Improvement. Diagnosis and management of asthma. https://www.icsi.org/_asset/rsjvnd/Asthma-Interactive0712.pdf
- Hashmi MF, Tariq M, Cataletto ME. Asthma. [Updated 2022 Feb 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430901
- Burrows B, Barbee RA, Cline MG, Knudson RJ, Lebowitz MD. Characteristics of asthma among elderly adults in a sample of the general population. Chest. 1991 Oct;100(4):935-42. doi: 10.1378/chest.100.4.935
- Martin AJ, Landau LI, Phelan PD. Lung function in young adults who had asthma in childhood. Am Rev Respir Dis. 1980 Oct;122(4):609-16. doi: 10.1164/arrd.1980.122.4.609
- Westerhof GA, Coumou H, de Nijs SB, Weersink EJ, Bel EH. Clinical predictors of remission and persistence of
adult-onset asthma. J Allergy Clin Immunol 2018;141:104-9.e3. - A Pocket Guide for Health Professionals Updated 2021 (for Adults and Children Older than 5 Years). https://ginasthma.org/wp-content/uploads/2021/05/GINA-Pocket-Guide-2021-V2-WMS.pdf
- Moore WC, Meyers DA, Wenzel SE, et al. Identification of asthma phenotypes using cluster analysis in the Severe Asthma Research Program. Am J Respir Crit Care Med 2010;181:315-23.
- Wenzel SE. Asthma phenotypes: the evolution from clinical to molecular approaches. Nature Medicine 2012;18:716-25.
- Global Strategy For Asthma Management and Prevention. Updated 2021. https://ginasthma.org/wp-content/uploads/2021/05/GINA-Main-Report-2021-V2-WMS.pdf
- Weiler JM, Anderson SD, Randolph C, et al. Pathogenesis, prevalence, diagnosis, and management of exercise-induced bronchoconstriction: a practice parameter. Ann Allergy Asthma Immunol. 2010;105(6 Suppl):S1-S47. http://www.annallergy.org/article/S1081-1206(10)00891-4/fulltext
- Exercise-Induced Bronchoconstriction: Diagnosis and Management. Am Fam Physician. 2011 Aug 15;84(4):427-434. https://www.aafp.org/afp/2011/0815/p427.html
- Boulet, L. P., Turmel, J., Irwin, R. S., & CHEST Expert Cough Panel (2017). Cough in the Athlete: CHEST Guideline and Expert Panel Report. Chest, 151(2), 441–454. https://doi.org/10.1016/j.chest.2016.10.054
- Randolph C. An update on exercise-induced bronchoconstriction with and without asthma. Curr Allergy Asthma Rep. 2009;9(6):433–438.
- Rundell KW, Smoliga JM, Bougault V. Exercise-Induced Bronchoconstriction and the Air We Breathe. Immunol Allergy Clin North Am. 2018 May;38(2):183-204. doi: 10.1016/j.iac.2018.01.009
- Emerson SR, Rosenkranz SK, Rosenkranz RR, Kurti SP, Harms CA. The potential link between sugar-sweetened beverage consumption and post-exercise airway narrowing across puberty: a longitudinal cohort study. Public Health Nutr. 2016 Sep;19(13):2435-40. doi: 10.1017/S1368980015003109
- Bonini M, Silvers W. Exercise-Induced Bronchoconstriction: Background, Prevalence, and Sport Considerations. Immunol Allergy Clin North Am. 2018 May;38(2):205-214. doi: 10.1016/j.iac.2018.01.007
- Jayasinghe H, Kopsaftis Z, Carson K. Asthma Bronchiale and Exercise-Induced Bronchoconstriction. Respiration. 2015;89(6):505-12. doi: 10.1159/000433559
- Gerow M, Bruner PJ. Exercise Induced Asthma. [Updated 2021 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557554
- Lugogo N, Que LG, Gilstrap DL, Kraft M. Asthma. In: Broaddus VC, Mason RJ, Ernst JD, et al, eds. Murray and Nadel’s Textbook of Respiratory Medicine. 6th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 42.
- Parsons JP, Hallstrand TS, Mastronarde JG, Kaminsky DA, Rundell KW, Hull JH, Storms WW, Weiler JM, Cheek FM, Wilson KC, Anderson SD; American Thoracic Society Subcommittee on Exercise-induced Bronchoconstriction. An official American Thoracic Society clinical practice guideline: exercise-induced bronchoconstriction. Am J Respir Crit Care Med. 2013 May 1;187(9):1016-27. https://doi.org/10.1164/rccm.201303-0437ST
- Backer V, Mastronarde J. Pharmacologic Strategies for Exercise-Induced Bronchospasm with a Focus on Athletes. Immunol Allergy Clin North Am. 2018 May;38(2):231-243. doi: 10.1016/j.iac.2018.01.011
- Bonini M, Di Mambro C, Calderon MA, Compalati E, Schünemann H, Durham S, Canonica GW. Beta₂-agonists for exercise-induced asthma. Cochrane Database Syst Rev. 2013 Oct 2;(10):CD003564. doi: 10.1002/14651858.CD003564.pub3
- Levy ML, Fletcher M, Price DB, Hausen T, Halbert RJ, Yawn BP. International Primary Care Respiratory Group (IPCRG) Guidelines: diagnosis of respiratory diseases in primary care. Prim Care Respir J 2006;15:20-34.
- Southworth T, Kaur M, Hodgson L, Facchinetti F, Villetti G, Civelli M, Singh D. Anti-inflammatory effects of the phosphodiesterase type 4 inhibitor CHF6001 on bronchoalveolar lavage lymphocytes from asthma patients. Cytokine. 2019 Jan;113:68-73. doi: 10.1016/j.cyto.2018.06.007
- https://kidshealth.org/en/parents/action-plan-sheet.html
- National Heart Lung and Blood Institute. National Asthma Education and Prevention Program. Expert panel report 3: Guidelines for the diagnosis and management of asthma; 2007:382. https://www.nhlbi.nih.gov/health-pro/guidelines/current/asthma-guidelines/full-report
- Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J 2012;40:1324-43.
- Reddel H, Ware S, Marks G, Salome C, Jenkins C, Woolcock A. Differences between asthma exacerbations and poor asthma control [erratum in Lancet 1999;353:758]. Lancet 1999;353:364-9.
- Durrani SR, Busse WW. Management of asthma in adolescents and adults. In: Adkinson NF Jr, Bochner BS, Burks AW, et al, eds. Middleton’s Allergy Principles and Practice. 8th ed. Philadelphia, PA: Elsevier Saunders; 2014:chap 55.
- Rupani, H., Fong, W., Kyyaly, A., & Kurukulaaratchy, R. J. (2021). Recent Insights into the Management of Inflammation in Asthma. Journal of inflammation research, 14, 4371–4397. https://doi.org/10.2147/JIR.S295038
- Papi, A., Blasi, F., Canonica, G. W., Morandi, L., Richeldi, L., & Rossi, A. (2020). Treatment strategies for asthma: reshaping the concept of asthma management. Allergy, asthma, and clinical immunology : official journal of the Canadian Society of Allergy and Clinical Immunology, 16, 75. https://doi.org/10.1186/s13223-020-00472-8
- Miller MK, Lee JH, Miller DP, Wenzel SE; TENOR Study Group. Recent asthma exacerbations: a key predictor of future exacerbations. Respir Med. 2007 Mar;101(3):481-9. doi: 10.1016/j.rmed.2006.07.005
- Suissa S, Ernst P, Benayoun S, Baltzan M, Cai B. Low-dose inhaled corticosteroids and the prevention of death from asthma. N Engl J Med. 2000 Aug 3;343(5):332-6. doi: 10.1056/NEJM200008033430504
- Suissa, S., Ernst, P., & Kezouh, A. (2002). Regular use of inhaled corticosteroids and the long term prevention of hospitalisation for asthma. Thorax, 57(10), 880–884. https://doi.org/10.1136/thorax.57.10.880
- Haahtela, T., Tuomisto, L. E., Pietinalho, A., Klaukka, T., Erhola, M., Kaila, M., Nieminen, M. M., Kontula, E., & Laitinen, L. A. (2006). A 10 year asthma programme in Finland: major change for the better. Thorax, 61(8), 663–670. https://doi.org/10.1136/thx.2005.055699
- Rajan, S., Gogtay, N. J., Konwar, M., & Thatte, U. M. (2020). The global initiative for asthma guidelines (2019): change in the recommendation for the management of mild asthma based on the SYGMA-2 trial – A critical appraisal. Lung India : official organ of Indian Chest Society, 37(2), 169–173. https://doi.org/10.4103/lungindia.lungindia_308_19
- O’Byrne PM, Pedersen S, Lamm CJ, Tan WC, Busse WW. Severe exacerbations and decline in lung function in asthma. Am J Respir Crit Care Med 2009;179:19-24.
- Virchow JC. Allergen immunotherapy (AIT) in asthma. Semin Immunol. 2019 Dec;46:101334. doi: 10.1016/j.smim.2019.101334
- Virchow JC, Backer V, Kuna P, Prieto L, Nolte H, Villesen HH, Ljørring C, Riis B, de Blay F. Efficacy of a House Dust Mite Sublingual Allergen Immunotherapy Tablet in Adults With Allergic Asthma: A Randomized Clinical Trial. JAMA. 2016 Apr 26;315(16):1715-25. doi: 10.1001/jama.2016.3964
- Agache I, Lau S, Akdis CA, Smolinska S, Bonini M, Cavkaytar O, Flood B, Gajdanowicz P, Izuhara K, Kalayci O, Mosges R, Palomares O, Papadopoulos NG, Sokolowska M, Angier E, Fernandez-Rivas M, Pajno G, Pfaar O, Roberts GC, Ryan D, Sturm GJ, van Ree R, Varga EM, van Wijk RG, Yepes-Nuñez JJ, Jutel M. EAACI Guidelines on Allergen Immunotherapy: House dust mite-driven allergic asthma. Allergy. 2019 May;74(5):855-873. doi: 10.1111/all.13749
- Lambrecht BN, Hammad H. The immunology of asthma. Nat Immunol. 2015 Jan;16(1):45-56. doi: 10.1038/ni.3049
- Lambrecht BN, Hammad H, Fahy JV. The Cytokines of Asthma. Immunity. 2019 Apr 16;50(4):975-991. doi: 10.1016/j.immuni.2019.03.018
- Ingram JL, Kraft M. IL-13 in asthma and allergic disease: asthma phenotypes and targeted therapies. J Allergy Clin Immunol. 2012 Oct;130(4):829-42; quiz 843-4. doi: 10.1016/j.jaci.2012.06.034
- Zhu, Z., Homer, R. J., Wang, Z., Chen, Q., Geba, G. P., Wang, J., Zhang, Y., & Elias, J. A. (1999). Pulmonary expression of interleukin-13 causes inflammation, mucus hypersecretion, subepithelial fibrosis, physiologic abnormalities, and eotaxin production. The Journal of clinical investigation, 103(6), 779–788. https://doi.org/10.1172/JCI5909
- Pelaia, C., Paoletti, G., Puggioni, F., Racca, F., Pelaia, G., Canonica, G. W., & Heffler, E. (2019). Interleukin-5 in the Pathophysiology of Severe Asthma. Frontiers in physiology, 10, 1514. https://doi.org/10.3389/fphys.2019.01514
- Jackson, D. J., Busby, J., Pfeffer, P. E., Menzies-Gow, A., Brown, T., Gore, R., Doherty, M., Mansur, A. H., Message, S., Niven, R., Patel, M., Heaney, L. G., & UK Severe Asthma Registry (2021). Characterisation of patients with severe asthma in the UK Severe Asthma Registry in the biologic era. Thorax, 76(3), 220–227. https://doi.org/10.1136/thoraxjnl-2020-215168
- Taylor SL, Leong LEX, Mobegi FM, et al. Long-term azithromycin reduces Haemophilus influenzae and increases antibiotic resistance in severe asthma. Am J Respir Crit Care Med 2019;200:309-17.
- Taylor SL, Ivey KL, Gibson PG, Simpson JL, Rogers GB; AMAZES Study Research Group. Airway abundance of Haemophilus influenzae predicts response to azithromycin in adults with persistent uncontrolled asthma. Eur Respir J. 2020 Oct 1;56(4):2000194. doi: 10.1183/13993003.00194-2020
- Gibson PG, Yang IA, Upham JW, Reynolds PN, Hodge S, James AL, Jenkins C, Peters MJ, Marks GB, Baraket M, Powell H, Taylor SL, Leong LEX, Rogers GB, Simpson JL. Effect of azithromycin on asthma exacerbations and quality of life in adults with persistent uncontrolled asthma (AMAZES): a randomised, double-blind, placebo-controlled trial. Lancet. 2017 Aug 12;390(10095):659-668. doi: 10.1016/S0140-6736(17)31281-3
- Morales DR, Lipworth BJ, Guthrie B, Jackson C, Donnan PT, Santiago VH. Safety risks for patients with aspirin-exacerbated respiratory disease after acute exposure to selective nonsteroidal anti-inflammatory drugs and COX-2 inhibitors: Meta-analysis of controlled clinical trials. J Allergy Clin Immunol 2014;134:40-5.
- Hiles SA, McDonald VM, Guilhermino M, Brusselle GG, Gibson PG. Does maintenance azithromycin reduce asthma exacerbations? An individual participant data meta-analysis. Eur Respir J 2019;54.
- National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program. How to use a metered-dose inhaler. https://www.nhlbi.nih.gov/files/docs/public/lung/asthma_tipsheets.pdf
- Sly RM. Changing asthma mortality. Ann Allergy. 1994 Sep;73(3):259-68.





{kind=link}