What is Bartonella
Bartonella is a bacteria that cause several diseases in humans. The three most common are cat scratch disease, caused by Bartonella henselae; trench fever, caused by Bartonella quintana; and Carrión’s disease, caused by Bartonella bacilliformis. Patients with cat scratch disease (Bartonella henselae) usually have suffered a scratch or bite from a cat or kitten that is infected with the bacteria Bartonella henselae, a common infection in young cats.
Bartonella Disease
Cat scratch disease (Bartonella henselae)
People can get cat scratch disease from the scratches of domestic or feral cats, particularly kittens. Cat scratch disease (Bartonella henselae also known as Rochalimaea henselae) occurs most frequently in children under 15. Cats can harbor infected fleas that carry Bartonella henselae bacteria. The bacteria is passed from cat to cat via fleas. In the absence of fleas, an infected cat cannot pass the infection to uninfected cats. The bacteria are present in saliva deposited in cat’s fur and claws. These Bartonella henselae bacteria can be transmitted from a cat to a person during a scratch. Some evidence suggests that cat scratch disease may be transmitted directly to humans by the bite of infected cat fleas, although this has not been proven.
Cat scratch disease (Bartonella henselae) occurs worldwide and may be present wherever cats are found. Stray cats may be more likely than pets to carry Bartonella. In the United States, most cases of cat scratch disease occur in the fall and winter.
Ticks may carry some species of Bartonella bacteria, but there is currently no convincing evidence that ticks can transmit Bartonella infection to humans.
People at risk of getting cat scratch fever include those:
- owning a cat younger than 12 months
- licked, bitten or scratched by an infected kitten
- petting an infected cat
- owning at least one kitten or cat with fleas.
Cat scratch fever can occur in people of all ages but is most common in children and adolescents. 80% of patients with cat scratch disease are less than 21 years old.
Figure 1. Cat scratch disease papulopustular lesions

Figure 2. Cat scratch disease neck abscess that developed over 3 weeks on a 2.5-year-old boy who acquired cat scratch disease 10 months before

Serious but rare complications of cat scratch disease (Bartonella henselae)
People
Although rare, cat scratch disease can cause people to have serious complications. cat scratch disease can affect the brain, eyes, heart, or other internal organs. These rare complications, which may require intensive treatment, are more likely to occur in children younger than 5 years and people with weakened immune systems.
Cats
Most cats with Bartonella henselae infection show NO signs of illness, but on rare occasions this disease can cause inflammation of the heart—making cats very sick with labored breathing. Bartonella henselae infection may also develop in the mouth, urinary system, or eyes. Your veterinarian may find that some of your cat’s other organs may be inflamed.
How cats and people become infected with bartonella henselae?
Cats can get infected with Bartonella henselae from flea bites and flea dirt (droppings) getting into their wounds. By scratching and biting at the fleas, cats pick up the infected flea dirt under their nails and between their teeth. Cats can also become infected by fighting with other cats that are infected. The germ spreads to people when infected cats bite or scratch a person hard enough to break their skin. The germ can also spread when infected cats lick at wounds or scabs that you may have.
Cat scratch disease is caused by a bacterium called Bartonella henselae. About 40% of cats carry Bartonella henselae at some time in their lives, although most cats with this infection show NO signs of illness. Kittens younger than 1 year are more likely to have Bartonella henselae infection and to spread the germ to people. Kittens are also more likely to scratch and bite while they play and learn how to attack prey.
My cat is completely healthy. How can it carry an infection?
Cats become infected with Bartonella henselae (the bacteria that cause cat scratch disease) through flea bites or, less commonly, fights with other infected cats or feline blood transfusions. While some cats become ill, most simply carry the bacteria in their blood without getting sick. Some studies have found the Bartonella henselae bacteria in the blood of up to 1/3 of healthy cats, particularly kittens.
Should I get my pet treated for Bartonella, just to be safe?
Treatment is not recommended unless your pet becomes sick. Treating Bartonella with antibiotics can take a long time and it’s considered safer and more practical to let the pet handle the infection naturally. For cats that do become sick, the illness usually consists of fever for 2-3 days, with the cat recovering on its own. Symptoms requiring veterinary care include fever, vomiting, lethargy, red eyes, swollen lymph nodes or decreased appetite.
My daughter got scratched by the neighbor’s kitten and now my husband is worried about “cat scratch disease.” How worried should we be?
Most cat scratches do not result in cat scratch disease, and short of cleaning the wound with soap and water, there is no particular action to take. If your child develops a fever; enlarged, tender lymph nodes that develop 1–3 weeks after being scratched; or a pustule at the scratch site, please take her to your health care provider. Treatment with antibiotics is usually not necessary but may help reduce lymph node swelling.
I have a medical condition that affects my immune system. Should I give my cat away?
If you’re HIV-positive, are being treated for cancer, or have any other condition that might disrupt your immune system, you can keep your cat. Just keep the following points in mind:
- Keep the cat indoors.
- Avoid rough play with cats and situations in which scratches are likely. Declawing is not recommended.
- Promptly wash any cat scratches or bites with soap and water.
- Avoid contact with fleas.
- Treat the cat with a flea control product recommended by your veterinarian.
- It’s not necessary to test or treat a healthy cat for Bartonella.
- If you are getting a cat, make sure it’s at least a year old, in good health, and free of fleas. Avoid stray cats and cats with flea infestations.
Trench fever (Bartonella quintana)
Trench fever is transmitted by the human body louse. Because of its association with body louse infestations, trench fever is most commonly associated with homeless populations or areas of high population density and poor sanitation. Trench fever received its name during World War I, when many soldiers fighting in the European trenches harbored infected body lice and became infected with the disease.
Trench fever has a worldwide distribution; cases have been reported from Europe, North America, Africa, and China.
Carrión’s disease (Bartonella bacilliformis)
Carrión’s disease, formerly known as bartonellosis, is transmitted by bites from sand flies (genus Lutzomyia) that are infected with the organism. Carrión’s disease has limited geographic distribution; transmission occurs in the Andes Mountains at 3,000 to 10,000 ft in elevation in western South America, including Peru, Colombia, and Ecuador. Most cases are reported in Peru.
A few cases of Oroya fever and verruga peruana (Peruvian warts) have been reported in travelers who returned from the Andean highlands in South America, but the risk is low. In 2007, a newly recognized species of Bartonella (Bartonella rochalimae) was identified in an ill traveler returning from Peru. Much is still unknown regarding the existence of other competent arthropod vectors and the identification of a natural, nonhuman, vertebrate reservoir.
The classical course of infections with Bartonella bacilliformis is known as Carrion’s disease and consists of Oroya fever as the acute phase with hemolytic anemia and a subsequent chronic phase hallmarked by multiple vasoproliferative lesions on the skin (verruga peruana for “Peruvian wart”) 1. The devastating hemolytic anemia during Oroya fever is a critical difference between the pathologies of Bartonella bacilliformis and the other bartonellae, since severe morbidity and hemolytic anemia are usually not observed during infections with the modern species. A recent compilation of various studies concluded that the mortality during Oroya fever ranges from close to zero in the case of hospitalized patients receiving antibiotic treatment to up to 88% in untreated cases 2. Approximately 70% of patients suffering from Oroya fever develop complications of the disease, of which approximately half are of an infectious and half of a noninfectious nature. Noninfectious complications such as fever, anorexia or an altered mental status have been suggested to be primarily a consequence of systemic infection 3. The impairment of immunity during Oroya fever favors secondary infections that contribute prominently to morbidity and mortality by provoking septicemia, most often with Salmonella 3. During Carrion’s disease, the abrogation of hemolytic anemia is characteristically followed by massive pathological angiogenesis as hallmark of the chronic tissue phase called verruga peruana. It is crucial to note that the nodules observed over the course of this phase are “clinically and histologically indistinguishable” from the tumors arising during bacillary angiomatosis with the modern Bartonella species 4. Like these, the pathological angiogenesis during the verruga peruana phase usually occurs in the skin, but atypical cases involving other organs such as the spleen 5 have been reported. In striking contrast to the acute phase of Carrion’s disease, verruga peruana is associated with only negligible mortality 2. Notably, the name of this biphasic infection and the discovery of the link between its two phases derive from Daniel Alcides Carrion, who died from Oroya fever after he inoculated himself with blood from a verruga peruana nodule 6. However, it is known today that this classical course of Carrion’s disease is not the only possible outcome of a B. bacilliformis infection, since natives in the areas of endemicity exhibit a significant baseline of asymptomatic bacteremia (see above) and suffer from Oroya fever relatively rarely 7 but frequently develop verruga peruana without prior hemolytic anemia 8.
I have been suffering from fatigue and memory problems for the past year. Should I be tested for Bartonella infection?
There are many reasons why people might experience fatigue and memory problems. It’s unlikely that Bartonella is the cause of these issues. Work with your primary care physician to determine if a specialist is needed.
I heard that there are newer testing methods from laboratories that specialize in Bartonella testing. Are these new tests accurate?
Although Centers for Disease Control and Prevention (CDC) typically recommends FDA-cleared tests, there are not currently any Bartonella tests on the market that meet this standard. There are some things that you should keep in mind when evaluating the accuracy of a lab test.
- First, any laboratory that performs Bartonella serologic testing should provide you with information regarding the accuracy of the test.
- Second, be aware that while some labs may report that their tests find 100% of infected patients, this is unrealistic—the potential for false positives (and false negatives) almost always exists.
- Finally, it is important for all abnormal test results to be interpreted with your health care provider in the context of your medical history.
I got a tick bite. My friend said I should get tested for Lyme disease and Bartonella. Is that true?
The Centers for Disease Control and Prevention (CDC) don’t recommend it. To date, no study in the United States has shown that Bartonella can be transmitted to humans by ticks. Transmission studies with ticks have only used mice and artificial feeding systems. A single study showed that one species of tick in Europe could transmit a specific species of Bartonella to mice in a laboratory setting.
Other studies have identified Bartonella in ticks, probably from ticks feeding on animals that carry Bartonella. This doesn’t mean that the bacteria can be transmitted from the tick to a person or that the bacteria can survive in the tick for any length of time.
Unfortunately there is a great deal of misinformation regarding multiple tickborne infections (called coinfections) on the internet. The possibility of having several tickborne infections at once or having pathogens such as Bartonella that have not been shown to be tickborne, is extremely unlikely.
Bartonella infection prevention
Cat scratch disease (Bartonella henselae)
- Avoid rough play with cats, particularly strays and kittens, to prevent scratches. This is especially important for immunocompromised individuals. Wash hands promptly after handling cats.
- Treat cats for fleas using fipronil and other spot-on treatments. Check with your veterinarian. Permethrin should not be used on cats.
- Use a flea collar or similar topical preventive on dogs (fipronil, methoprene, imidocloprid, or permethrin), especially if you have both cats and dogs in your household.
- Keep cats indoors and away from stray cats.
- Immunocompromised individuals should avoid owning cats less than one year of age.
- Wash cat bites and scratches well with soap and running water. Do not allow cats to lick your wounds. Contact your doctor if you develop any symptoms of cat-scratch disease or infection.
Trench fever (Bartonella quintana)
- Avoid exposure to human body lice. Body lice are typically associated with conditions of crowding and limited access to proper personal hygiene.
- Do not share clothing, beds, bedding, and towels used by a person who might have body lice.
Body lice are spread most commonly by direct contact with an infested person or an infested person’s clothing or bedding. Body lice usually infest persons who do not launder and change their clothes regularly.
The following are steps that can be taken to help prevent and control the spread of body lice:
- Bathe regularly and change into properly laundered clothes at least once a week; launder infested clothing at least once a week.
- Machine wash and dry infested clothing and bedding using the hot water (at least 130°F) laundry cycle and the high heat drying cycle. Clothing and items that are not washable can be dry-cleaned OR sealed in a plastic bag and stored for 2 weeks.
- Do not share clothing, beds, bedding, and towels used by an infested person.
- Fumigation or dusting with chemical insecticides sometimes is necessary to control and prevent the spread of body lice for certain diseases.
Carrión’s disease (Bartonella bacilliformis)
Use repellents and protective clothing to avoid sand fly bites in areas where Carrión’s disease is common (South America). If possible, limit outdoor activities at dawn and dusk, when sand flies are most active.
Find the repellent that is Right for You here: https://www.epa.gov/insect-repellents/find-repellent-right-you
Bartonella Life Cycle and Infection Strategy
The infection cycle of Bartonella is initiated with the inoculation of a mammal reservoir host, characteristically following transmission via bloodsucking arthropods. Upon inoculation, the bartonellae are not capable of directly colonizing erythrocytes. Instead, a preceding period of residence in a primary niche is apparently necessary to make the bacteria and/or the host competent for this step. From the primary niche, the bartonellae are seeded into the bloodstream and infect erythrocytes in a sequence of steps ranging from adhesion to eventually invasion and intracellular persistence that enables continuous vector transmission (Figure 3).
During the whole course of infection, the lack of an effective host immune response and a globally moderated inflammatory profile are highly beneficial for Bartonella and are promoted by the pathogen via both passive immune evasion and active immunomodulation. The infection cycle of Bartonella has been extensively studied and reviewed elsewhere 9. Importantly, although it is obvious that certain differences from species to species do exist and probably arose due to specific paths of pathogen-host adaptation, it is generally believed that the overall concept of this infection cycle is conserved among members of the genus Bartonella.
Figure 3. Bartonella life cycle and infection strategy
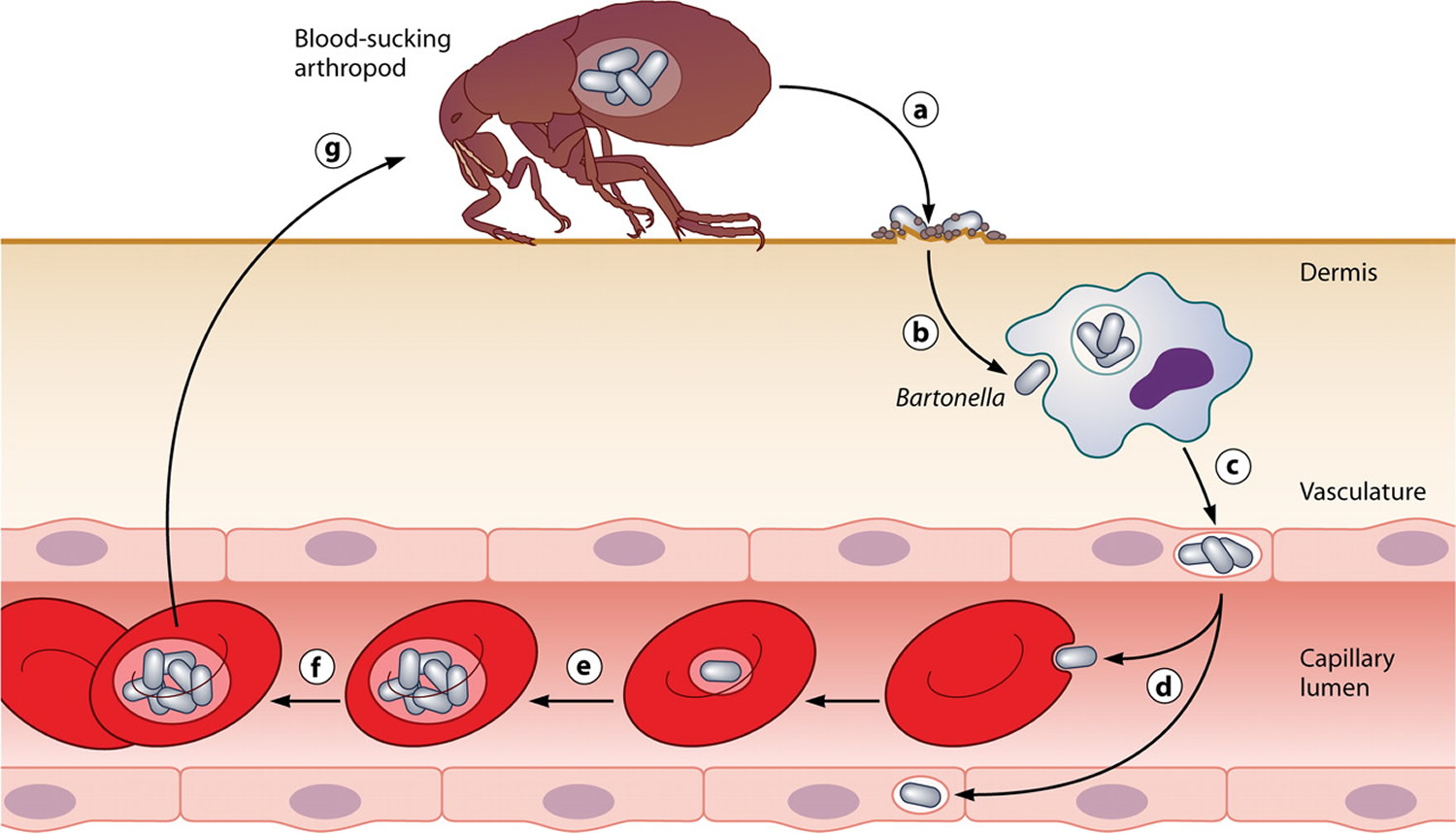
Common infection strategy of the bartonellae. The drawing illustrates the general concept of reservoir host infections with Bartonella. Following transmission by an arthropod vector (a), the bartonellae colonize the primary niche, which probably involves entry into migratory cells (b) and transport to the vascular endothelium (c), where the bacteria persist intracellularly. From the primary niche, the bacteria are seeded into the bloodstream (d), where they invade erythrocytes and reinfect the primary niche. After limited replication inside the red blood cell (e), they persist in the intraerythrocytic niche (f) competent for transmission by a bloodsucking arthropod (g). [Source 10]
Bartonella symptoms in humans
Cat scratch disease (Bartonella henselae)
- Low-grade fever may be present
- Enlarged, tender lymph nodes (lymphadenopathy) that develop 1–3 weeks after exposure
- A small red papule or pustule at the inoculation site
Rarely, unusual manifestations such as eye infections, severe muscle pain, or encephalitis may occur.
About three to 14 days after the skin is broken, a mild infection can occur at the site of the scratch or bite. A small red raised spot develops at the site of contact with an infected cat’s saliva. This changes into a fluid-filled blister or pus that later forms a crusty sore. This usually heals without scarring in several days or months. It is often mistaken for an insect bite. Most are found on the hands, arms, face or neck as people often hold kittens close to their chest and face.
A person with cat scratch disease may also have a fever, headache, poor appetite, and exhaustion. Later, the person’s lymph nodes closest to the original scratch or bite can become swollen, tender, or painful.
The nearest lymph glands then become swollen and tender, most often those on the head, neck and armpit. This is known as regional lymphadenopathy. The lymph glands may swell to 10-12 cm in the first two weeks of the disease. On questioning, patients often recall being licked, bitten or scratched by a cat in the previous one to eight weeks.
About 50% of patients will experience additional signs and symptoms including:
- fever
- malaise/fatigue
- headache
- nausea and vomiting
- sore throat
- rash
- stomach pains
- conjunctivitis
Less common problems occur in about 10% of patients. These include:
- Parinaud’s oculoglandular syndrome, characterized by an inflamed lump in the eye and swollen lymph glands in front of the nearby ear
- Bacillary angiomatosis (infection of the blood vessels)
- Bacillary hepatitis and splenitis (infection of the liver and spleen)
- Erythema nodosum (red lumps on the shins)
- Sepsis (infection disseminated through the blood stream)
- Encephalopathy (brain infection)
- Bacterial endocarditis (heart valve infection)
Encephalopathy is an uncommon complication of cat scratch disease that occurs one to six weeks after the lymph glands swell up. The abrupt symptoms of fever, seizures and coma can be frightening. With hospitalization and high doses of antibiotics most patients recover completely.
Trench fever (Bartonella quintana)
- Fever (may present as a single bout of fever or bouts of recurrent fever)
- Headache
- Rash
- Bone pain, mainly in the shins, neck, and back
Carrión’s disease (Bartonella bacilliformis)
This disease has 2 distinct phases:
- Oroya fever: During this phase, patients may present with fever, headache, muscle aches, abdominal pain, and severe anemia.
- Verruga peruana: During this later phase, lesions appear under the skin as nodular growths, then emerge from the skin as red-to-purple vascular lesions that are prone to ulceration and bleeding.
Other complications
Bacillary angiomatosis
Bacillary angiomatosis (caused by Bartonella henselae or Bartonella quintana) and bacillary peliosis (caused by Bartonella henselae) occur primarily in immunocompromised people, such as those with advanced HIV infection. Bacillary angiomatosis may present as lesions in the skin, subcutaneous tissue, bone, or other organs. Bacillary peliosis causes vascular lesions in the liver and spleen.
Figure 4. Bacillary angiomatosis

Subacute endocarditis
Many Bartonella species can cause subacute endocarditis (infection of the heart valves), which is often culture negative.
Bartonella infection diagnosis
- Cat scratch disease (Bartonella henselae) may be diagnosed presumptively in patients with typical signs and symptoms and a compatible exposure history. Serology can confirm the diagnosis, although cross-reactivity may limit interpretation in some circumstances. In general, lymph node aspiration is not recommended except to relieve severe pain and swelling or in cases where the diagnosis is unclear.
- Bartonella test
- Bartonella henselae DNA may be detected by polymerase chain reaction (PCR) or culture of lymph node aspirates or blood, though sensitivity of these methods is not optimal for blood samples.
- Since Bartonella henselae is a fastidious, slow-growing bacterium, cultures should be held for a minimum of 21 days.
- Trench fever can be diagnosed by isolation of Bartonella quintana from blood cultured on blood or chocolate agar under 5% CO2. Microcolonies can be seen after 21 days of incubation at 37°C.
- Trench fever can also be diagnosed by serology.
- Carrión’s disease is typically diagnosed via blood culture or direct observation of the bacilli in peripheral blood smears during the acute phase of infection (Oroya fever).
- Endocarditis due to Bartonella species can be diagnosed by serology and by polymerase chain reaction (PCR) or culture of excised heart valve tissue.
Bartonella treatment
Trench fever, Carrión’s disease, and endocarditis due to Bartonella spp. are serious infections that require antibiotic treatment. Health care providers should consult with an expert in infectious diseases regarding treatment options.
Bartonella henselae treatment
Treatment of uncomplicated cat scratch disease remains controversial. Because it is a benign and self-limiting condition, with most cases of regional lymphadenopathy resolving spontaneously in two to four months, no specific treatment is usually necessary. The use of antibiotics to shorten the course of disease is debated. Most cases of cat scratch disease resolve without treatment, although some patients may develop complications from disseminated disease. Azithromycin has been shown to decrease lymph node volume more rapidly compared to no treatment. The recommended dose of azithromycin for cat scratch disease is:
- For adults and children > 45.5 kg: 500 mg on day 1, followed by 250 mg for 4 days
- For children ≤ 45.5 kg: 10 mg/kg on day 1, followed by 5 mg/kg for 4 days
A number of other antibiotics are effective against Bartonella infections, including penicillins, tetracyclines, cephalosporins, and aminoglycosides. Since aminoglycosides are bactericidal, they are typically used as first-line treatment for Bartonella infections other than cat scratch disease. Often, with serious infections, more than one antibiotic is used.
Some studies suggest that certain antibiotics including doxycycline, erythromycin, gentamicin, rifampicin, trimethoprim + sulphamethoxazole and ciprofloxacin may significantly shorten the duration of lymphadenopathy. Antibiotics are warranted in patients with severe or persistent symptoms of cat scratch disease.
In rare cases, large pus-filled lymph nodes may persist for one to three years. The pus may need to be repeatedly drained through a needle. Pain and fever can be managed by increasing fluid intake and paracetamol. Warm moist compresses to affected lymph glands may decrease swelling and tenderness.
References- Maguina C, Guerra H, Ventosilla P. 2009. Bartonellosis. Clin. Dermatol. 27:271–280.
- Pachas P. 2000. Epidemiología de la Bartonelosis en el Peru. Oficina General de Epidemiología, Lima, Peru.
- Maguina C, Garcia PJ, Gotuzzo E, Cordero L, Spach DH. 2001. Bartonellosis (Carrion’s disease) in the modern era. Clin. Infect. Dis. 33:772–779.
- Caceres-Rios H, et al. 1995. Verruga peruana: an infectious endemic angiomatosis. Crit. Rev. Oncog. 6:47–56.
- Lydy SL, et al. 2008. Isolation and characterization of Bartonella bacilliformis from an expatriate Ecuadorian. J. Clin. Microbiol. 46:627–637.
- Schultz MG. 2010. Daniel Alcides Carrión [photo quiz]. Emerg. Infect. Dis. vol 16:1025–1027.
- Ricketts WE. 1948. Bartonella bacilliformis anemia (Oroya fever); a study of 30 cases. Blood 3:1025–1049.
- Garcia FU, Wojta J, Broadley KN, Davidson JM, Hoover RL. 1990. Bartonella bacilliformis stimulates endothelial cells in vitro and is angiogenic in vivo . Am. J. Pathol. 136:1125–1135.
- Chomel BB, et al. 2009. Ecological fitness and strategies of adaptation of Bartonella species to their hosts and vectors. Vet. Res. 40:29.
- Intruders below the Radar: Molecular Pathogenesis of Bartonella spp. Alexander Harms, Christoph Dehio. Clinical Microbiology Reviews Jan 2012, 25 (1) 42-78; DOI: 10.1128/CMR.05009-11 https://cmr.asm.org/content/25/1/42





{kind=link}