Beck Anxiety Inventory
Beck Anxiety Inventory is a well accepted self-report screening measure of the severity of anxiety in adults and adolescents for use in both clinical and research settings 1 and is validated in a number of languages, including German, French, Chinese, Spanish, Persian, Nepal, Icelandic, and others 2. The Beck Anxiety Inventory is a 21-item multiple-choice self-report inventory that measures the severity of an anxiety in adults and adolescents rated on a scale from 0 to 3. Because the items in the Beck Anxiety Inventory describe the emotional, physiological, and cognitive symptoms of anxiety but not depression, it can discriminate anxiety from depression. Although the age range for the measure is from 17 to 80, it has been used in peer-reviewed studies with younger adolescents aged 12 and older. Each of the items on the Beck Anxiety Inventory is a simple description of a symptom of anxiety in one of its four expressed aspects: (1) subjective (e.g., “unable to relax”), (2) neurophysiologic (e.g., “numbness or tingling”), (3) autonomic (e.g., “feeling hot”) or (4) panic-related (e.g., “fear of losing control”). The Beck Anxiety Inventory requires only a basic reading level, can be used with individuals who have intellectual disabilities, and can be completed in 5 – 10 minutes using the pre-printed paper form and a pencil. Because of the relative simplicity of the inventory, it can also be administered orally for sight-impaired individuals. The Beck Anxiety Inventory may be administered and scored by paraprofessionals, but it should be used and interpreted only by professionals with appropriate clinical training and experience.
Among counselors in primary health care settings, Beck Anxiety Inventory is reported to be the ninth most commonly used tools in the United States 3, owing to the advantages in cost-effectiveness and brevity in the application procedure. According to the meta-analysis of Beck Anxiety Inventory (k = 117), Beck Anxiety Inventory was reported to manifest an excellent internal consistency in clinical (0.91) and non-clinical sample (0.91) and a good test-retest reliability in clinical (0.66) and non-clinical (0.65) 1.
This 21-item self-report questionnaire was originally developed to assess clinical anxiety (i.e., an excess of normal anxiety resulting in significant distress and impairment of functioning 4, differentiated from normal anxiety (i.e., an adaptive emotional responses to danger or threat) 5, as well as the unique aspects of anxiety disorders that are assumed to differ from those of depressive disorders 6. While depression is defined as the experience of being sad, gloomy, and empty which is typically associated with events experienced in the past and decreased autonomic activity, anxiety is defined as feelings of fear and tension, and apprehension which is usually related to anticipation of future events and activation of autonomic nervous system 7.
However, some issues remain regarding the Beck Anxiety Inventory’s discriminant validity against depressive disorders. Distinguishing anxiety and depressive disorders through self-report measures has been the subject of debate due to a high rate of comorbidity or the possibility of a single, shared underlying mechanism, such as negative affect 7. Although Beck’s original studies report significantly higher Beck Anxiety Inventory mean scores for patients with anxiety disorders compared to those with depressive disorders 8, other studies fail to replicate the results 9. In one study conducted in Korean sample, correlation coefficients of Beck Anxiety Inventory with other depression assessments such as BDI and PHQ-9 are found to be even higher than other anxiety assessment tools 10. The ambiguity found in the mean scores difference of Beck Anxiety Inventory and correlation sizes with other anxiety and depression measures questions the utility of Beck Anxiety Inventory as measuring the general anxiety that are distinguishable from depression as Beck et al. 6. Because various anxiety and depression tools aim to assess the same construct with heterogeneous factors, more diverse assessments must be incorporated into an analysis to provide a comprehensive outlook on the divergent and convergent validity of the Beck Anxiety Inventory.
Another issue concerns the Beck Anxiety Inventory’s clinical utility as an anxiety screening tool and a measurement of severity in primary care settings. Although the Beck Anxiety Inventory was not originally developed as a diagnostic tool, it is essential to examine the degree of its diagnostic reliability and its score distribution in a sample before it can be utilized as a tool in anxiety screening, to track symptom changes, or as an outcome measure based on severity measurements. To date, 11 studies explored the diagnostic validity of Beck Anxiety Inventory, optimal cutoff scores ranging from 7 to 26 depending on the diversity of studied samples 1. As the diagnostic cutoff score can be varying across the ethnicity and cultural background behind the research setting, undertaking the diagnostic validity study in a new ethnic sample can benefit the existing literature. Negative and positive predictive powers are critical sources for determining the clinical utility of a screening tool, especially for disorders in low prevalence rate 11. Providing such information would thus help researchers to decide optimal Beck Anxiety Inventory cutoff scores for their individual purposes.
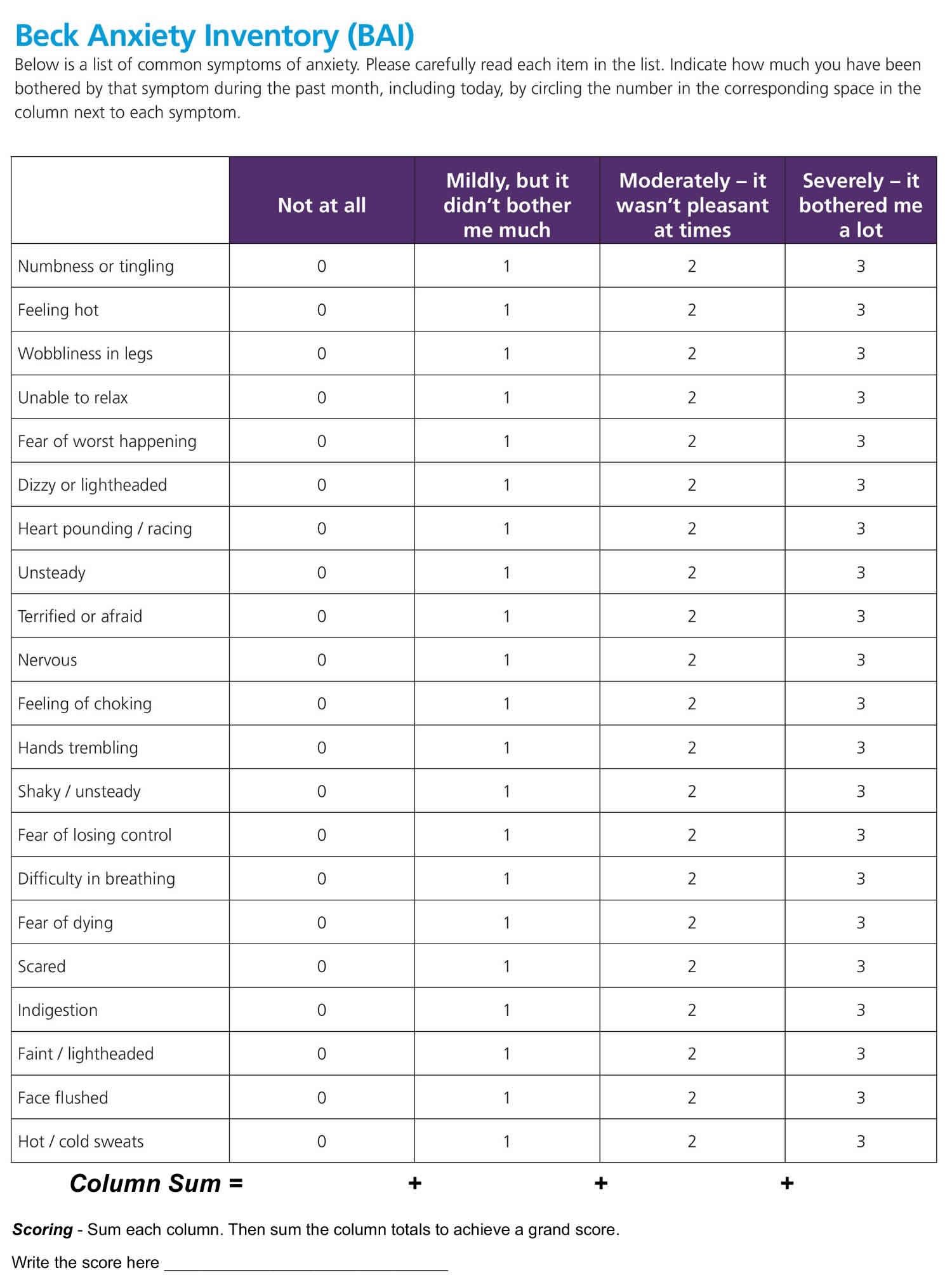
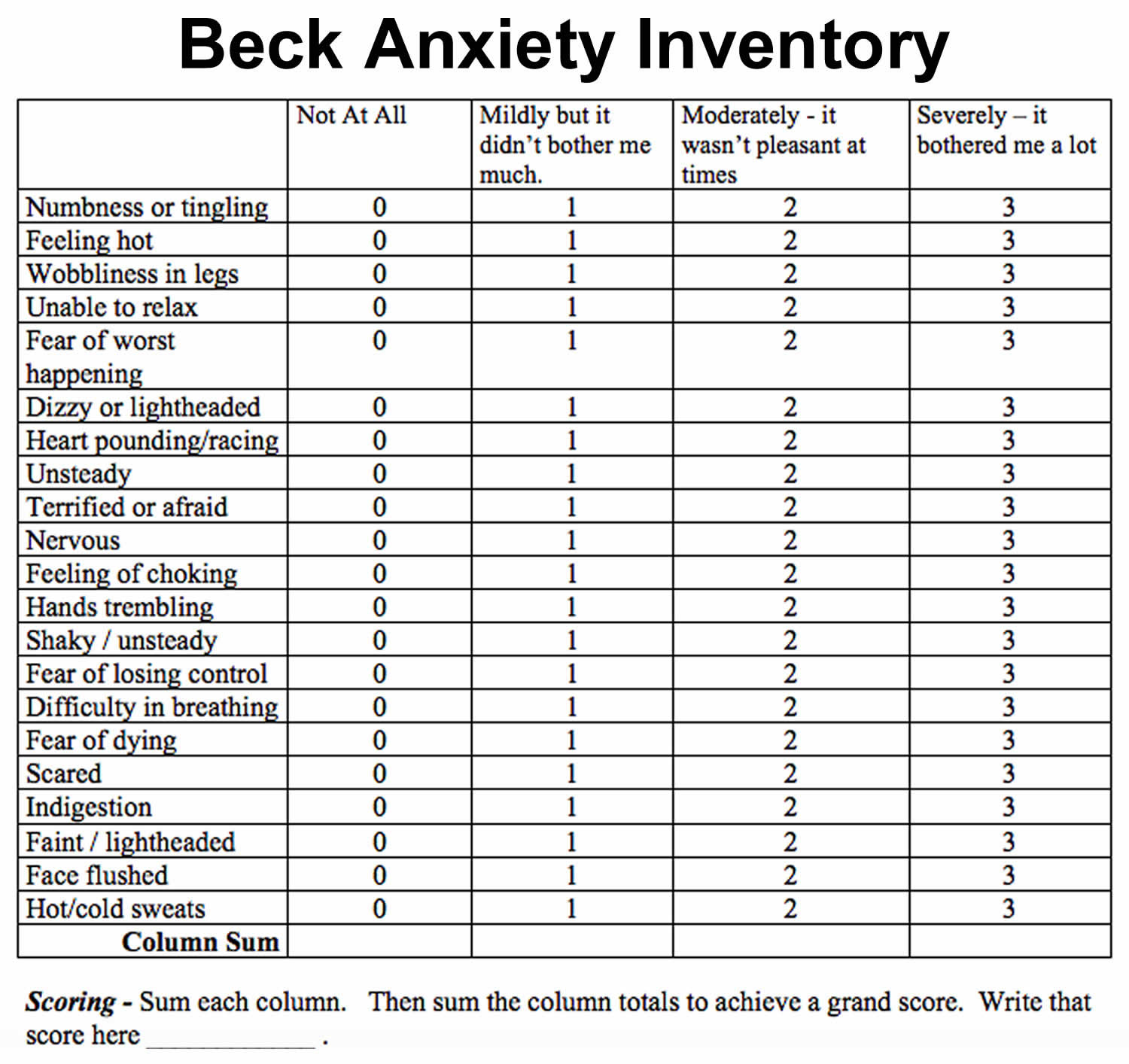
Footnote: Above is a list of common symptoms of anxiety. Please carefully read each item in the list. Indicate how much you have been bothered by that symptom during the past month, including today, by circling the number in the corresponding space in the column next to each symptom.
Beck Anxiety Inventory scoring
The Beck Anxiety Inventory (BAI) consists of 21 items with a Likert scale ranging from 0 to 3 and raw scores ranging from 0 to 63.
The total Beck Anxiety Inventory score is calculated by finding the sum of the 21 items.
The Beck Anxiety Inventory Scores Interpretation 12:
- A grand sum between 0 – 21 indicates very low anxiety. That is usually a good thing. However, it is possible that you might be unrealistic in either your assessment which would be denial or that you have learned to “mask” the symptoms commonly associated with anxiety. Too little “anxiety” could indicate that you are detached from yourself, others, or your environment.
- A grand sum between 22 – 35 indicates moderate anxiety. Your body is trying to tell you something. Look for patterns as to when and why you experience the symptoms described above. For example, if it occurs prior to public speaking and your job requires a lot of presentations you may want to find ways to calm yourself before speaking or let others do some of the presentations. You may have some conflict issues that need to be resolved. Clearly, it is not “panic” time but you want to find ways to manage the stress you feel.
- A grand sum that exceeds 36 is a potential cause for concern. Again, look for patterns or times when you tend to feel the symptoms you have circled. Persistent and high anxiety is not a sign of personal weakness or failure. It is, however, something that needs to be proactively treated or there could be significant impacts to you mentally and physically. You may want to consult a counselor if the feelings persist.
- Bardhoshi G, Duncan K, Erford BT. Psychometric meta-analysis of the english version of the beck anxiety inventory. J. Couns. Dev. (2016) 94:356–73. doi: 10.1002/jcad.12090
- Sæmundsson BR, Þ*órsdóttir F, Kristjánsdóttir H, Ólason DÞ*, Smári J, Sigurð*sson JF. Psychometric properties of the icelandic version of the beck anxiety inventory in a clinical and a student population. Eur J Psychol Assess. (2011) 27:133–41. doi: 10.1027/1015-5759/a000059
- Peterson CH, Lomas GI, Neukrug ES, Bonner MW. Assessment use by counselors in the United States: implications for policy and practice. J Couns Dev. (2014) 92:90–8. doi: 10.1002/j.1556-6676.2014.00134.x
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Washington, DC: American Psychiatric Pub (2013).
- Öhman A. Fear and Anxiety as Emotional Phenomena: Clinical Phenomenology, Evolutionary Perspectives, and Information-Processing Mechanisms, New York, NY: Guilford Press (1993).
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consul Clin Psychol. (1988) 56:893–7. doi: 10.1037/0022-006X.56.6.893
- Feldman LA. Distinguishing depression and anxiety in self-report: evidence from confirmatory factor analysis on nonclinical and clinical samples. J Consult Clin Psychol. (1993) 61:631–8. doi: 10.1037/0022-006X.61.4.631
- Steer RA, Ranieri WF, Beck AT, Clark DA. Further evidence for the validity of the beck anxiety inventory with psychiatric outpatients. J Anxiety Disord. (1993) 7:195–205. doi: 10.1016/0887-6185(93)90002-3
- Muntingh ADT, van der Feltz-Cornelis CM, van Marwijk HWJ, Spinhoven P, Penninx BWJH, van Balkom AJLM. Is the beck anxiety inventory a good tool to assess the severity of anxiety? A primary care study in The Netherlands study of depression and anxiety (NESDA). BMC Fam Pract. (2011) 12:66. doi: 10.1186/1471-2296-12-66
- Lee HK, Lee EH, Hwang ST, Hong SH, Kim JH. Psychometric properties of the beck anxiety inventory in the community-dwelling sample of Korean adults. Korean J Clin Psychol. (2016) 35:822–30. doi: 10.15842/kjcp.2016.35.4.010
- Leyfer OT, Ruberg JL, Woodruff-Borden J. Examination of the utility of the beck anxiety inventory and its factors as a screener for anxiety disorders. J Anxiety Disord. (2006) 20:444–58. doi: 10.1016/j.janxdis.2005.05.004
- Beck, A.T., Epstein, N., Brown, G., & Steer, R.A. (1988). An inventory for measuring clinical anxiety:Psychometric properties.Journal of Consulting and Clinical Psychology, 56, 893-897.





{kind=link}