
Best brain supplements
According to the 2019 American Association of Retired Persons (AARP) Brain Health and Dietary Supplements Survey, the majority of adults surveyed view vitamins and dietary supplements positively, with 78% saying they are extremely or somewhat important to health, but supplements are more popular among older adults 1. More than a quarter of adults in the United States age 50 and older take at least one supplement for brain health reasons. However, according to an in-depth report titled “The Real Deal on Brain Health Supplements” released Global Council on Brain Health (GCBH) — an independent working group of top neurologists, nutritionists and researchers — finds that supplements to preserve or boost memory or cognition aren’t worth the plastic they’re bottled in 2. Consumers should not begin taking any supplements for brain health without first consulting with their health care provider. “The Real Deal on Brain Health Supplements” report focused on the vitamins, minerals, and other supplements that were commonly marketed for brain health, including B vitamins, vitamin D, vitamin E, apoaequorin, caffeine, coenzyme Q10, curcumin, cocoa, Ginkgo biloba, huperzine A, medium-chain triglycerides (MCT coconut oil), melatonin, nicotinamide riboside, omega-3 fatty acids, and phosphatidylserine 2. The Global Council on Brain Health consensus statements and recommendations on brain supplements are based on the Global Council on Brain Health experts’ knowledge of the field and their evaluation of the best available evidence from peer-reviewed, published observational studies and randomized controlled trials in humans, as well as studies conducted in animals designed to help determine the effects of dietary supplements on brain health 2. The Global Council on Brain Health Experts examined the evidence on whether dietary supplements can impact people’s cognitive functions and summarized their consensus along with their recommendations and tips. The Global Council on Brain Health concluded that for most people, the best way to get your nutrients for brain health is from a healthy diet and what is good for your heart is also good for your brain. Common conditions influenced by diet such as elevated blood pressure, high cholesterol, and diabetes harm both cardiovascular and cognitive health. Therefore, a heart healthy diet is a brain healthy diet.
The typical, contemporary Western diet (high in salt, sugar, excess calories, and saturated fats) is not good for the brain. Although this remains a broad area of research exploration, the strongest published data suggests that there are certain diets (like the Mediterranean diet, the DASH diet, the MIND diet), specific foods (such as olive oil), and particular nutritional supplements (including phenolic compounds like curcumin and quercetin) that may prove effective for Alzheimer’s disease prevention. A plant-based diet that is rich in a variety of fruits and vegetables, particularly green-leafy vegetables and berries, is associated with better brain health.
Mediterranean diet is low in saturated fat and high in fiber 3:
- Fruits, vegetables, grains, beans, nuts, and seeds are eaten daily and make up the majority of food consumed.
- Fat, much of it from olive oil, may account for up to 40% of daily calories.
- Small portions of cheese or yogurt are usually eaten each day, along with a serving of fish, poultry, or eggs.
- Red meat is consumed now and then.
- Small amounts of red wine are typically taken with meals.
- Main meals consumed daily should be a combination of three elements: cereals, vegetables and fruits, and a small quantity of legumes, beans or other (though not in every meal). Cereals in the form of bread, pasta, rice, couscous or bulgur (cracked wheat) should be consumed as one–two servings per meal, preferably using whole or partly refined grains. Vegetable consumption should amount to two or more servings per day, in raw form for at least one of the two main meals (lunch and dinner). Fruit should be considered as the primary form of dessert, with one–two servings per meal. Consuming a variety of colors of both vegetables and fruit is strongly recommended to help ensure intake of a broad range of micronutrients and phytochemicals. The less these foods are cooked, the higher the retention of vitamins and the lower use of fuel, thus minimizing environmental impact.
Dietary Approaches to Stop Hypertension (DASH) diet 4:
- Grains and grain products: 7–8 servings per day, more than half of which are whole-grain foods
- Fruits: 4–5 servings per day
- Vegetables: 4–5 servings per day
- Low-fat or non-fat dairy foods: 2–3 servings per day
- Lean meats, fish, poultry: 6 or less servings or fewer per day
- Nuts, seeds, and legumes: 4–5 servings per week
- Added fats and oils: 2–3 servings per day
- Sweets: 5 or less servings per week
- Salt (sodium): 1,500 milligrams (mg) sodium lowers blood pressure even further than 2,300 mg sodium daily.
MIND diet is short for Mediterranean-DASH Intervention for Neurodegenerative Delay diet 5. The MIND diet is similar to two other healthy meal plans: the DASH diet and the Mediterranean diet. Morris et al. 5 originally devised the MIND diet and found that the diet can slow cognitive decline over an average of 4.7 years in adults aged 58–98 years old. Interestingly, recent research found that the MIND diet and not the Mediterranean diet, protected against 12-year incidence of mild cognitive impairment and dementia in older adults 6. Also, a large observational study with older adults found that longer adherence to the MIND diet was associated with better verbal memory 7. The MIND diet promotes 10 healthy foods (Leafy greens, other veg, nuts, berries, fish, poultry, olive oil, beans, whole grains, red wine) and limits 5 other foods (red meat, butter, cheese, pastries and sweets, fried foods). While previous research shows that higher consumption of vegetables are associated with lower risk of cognitive decline 8, the strongest association was observed for higher intake of leafy greens 9. Previous research on cognitive function or dementia do not observe protective effects for overall fruit consumption 10. However, berries were shown to slow cognitive decline, particularly in global cognition and verbal memory in older adults 11.
- The MIND diet has 15 dietary components, including 10 “brain-healthy food groups” 12:
- Green leafy vegetables (like spinach and salad greens): At least six servings a week
- Other vegetables: At least one a day
- Nuts: Five servings a week
- Berries: Two or more servings a week
- Beans: At least three servings a week
- Whole grains: Three or more servings a day
- Fish: Once a week
- Poultry (like chicken or turkey): Two times a week
- Olive oil: Use it as your main cooking oil.
- Wine: One glass a day
- You AVOID:
- Red meat: Less than four servings a week
- Butter and margarine: Less than a tablespoon daily
- Cheese: Less than one serving a week
- Pastries and sweets: Less than five servings a week
- Fried or fast food: Less than one serving a week
- You AVOID:
The research found that high scores in all three diets were associated with a reduced risk of Alzheimer’s disease, but the MIND diet was the only diet in which even moderate adherence was beneficial. The MIND diet was also associated with a slower decline in global cognition, the equivalent of being 7.5 years younger in age cognitively. However, all of these studies are still observational, making it very difficult to confirm whether the benefits are caused by the diet or by other characteristics shared by the people who choose these foods. More research could help determine which of these diets has the most potential benefit for brain health. In the meantime, take note of the basic characteristics that they share: high levels of fruits, vegetables, fish, and legumes and low levels of processed foods, red meat, sweets, and sugars.
Many clinical and animal studies have demonstrated the importance of polyunsaturated fatty acids in neural development and neurodegeneration. Omega-3 fatty acid is a polyunsaturated fatty acid that must be obtained through dietary intake from fish as well as other types of seafood as it is not produced naturally in the human body 13. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are essential fatty acids present in omega-3 14. DHA (docosahexaenoic acid) makes up 97% of the brain’s total omega-3 fatty acid content 14, particularly in brain regions involved in attention and memory 15. Docosahexaenoic acid (DHA) is involved in multiple brain functions including cell membrane fluidity, receptor affinity, modulation of signal transduction molecules, and cognitive function 16. Omega-3 fatty acid is important for normal cognitive development in early life and may be associated with a reduced decline in cognitive function in older adults 17. Recently, omega-3 fatty acids are suggested to act as recovery aids, or possibly as a prophylactic nutritional measure for concussion or mild traumatic brain injury. Animal studies and (pre)clinical studies show that DHA (docosahexaenoic acid) might have a positive effect on the outcomes of mild traumatic brain injury. However, there is a need for well-controlled studies before polyunsaturated fatty acids supplementation can be advised as a therapeutic or preventative measure against sports-related concussion 16.
However, the Global Council on Brain Health does not endorse any ingredient, product, or supplement specifically for brain health, unless your healthcare provider has identified that you are deficient in a specific nutrient or are at risk of becoming so (i.e., for reasons of deficiencies caused by diet, lifestyle, certain surgeries or other health issues). You should not begin taking any supplements without first consulting with your healthcare provider. The next time you see your healthcare provider, take all supplements you currently take to your appointment so you can discuss them. For the few supplements that have been researched for their effect on brain health, studies have found no benefit in people with normal nutrient levels 2. The research is inconclusive on whether people with nutritional deficiencies can benefit their brains by taking a supplement. Therefore, beyond a few very specific nutrients taken to replace an identified deficiency, there is insufficient evidence to support the use of supplements to benefit the brain 2.
If you are experiencing significant memory loss, consult your health care provider, who may wish to check your Folate (vitamin B9) and vitamin B12 levels. Vitamin B12 deficiency and folate (vitamin B9) deficiency may negatively affect your brain health; healthcare providers may recommend supplementation in people with lower-than-recommended levels of these vitamins. Individuals should follow their health care provider’s advice to make sure the supplements taken are appropriate to address their specific deficiency or problem. Make sure you do not take too much of any of the B vitamins and check to see if the foods you eat are already fortified with them. If your health care provider advises that you take folic acid, ask whether you should take it with vitamin B12. Vitamin B “complex” supplements contain different mixtures of B-vitamins at different doses, not all of which are needed by a particular individual.
Eating fatty fish (salmon, mackerel, tuna, etc.) may benefit cognitive function, but there is insufficient evidence to recommend taking a fish oil-derived omega-3 supplement for brain health.
For people with vitamin D deficiency, healthcare providers may recommend vitamin D supplementation to correct the low levels for general health; however, there is insufficient evidence that vitamin D supplementation benefits brain health.
Mild Cognitive Impairment, Dementia and Other Brain Disorders
There is insufficient evidence to support the use of popular and often expensive medical foods or dietary supplements being marketed to older adults for brain health 2. For example, Souvenaid is a medical food sold in Europe and Asia for the purpose of improving symptoms in those with mild or early Alzheimer’s disease. In Hong Kong, it is available over-the-counter without a prescription. It is not approved for sale in the United States. Until there is evidence of effectiveness, these products are not recommended for brain health 2.
For people suffering from Mild Cognitive Impairment (MCI), Dementia and Other Brain Disorders, the Global Council on Brain Health recommends:
- Adopting healthy lifestyle habits. Work with your health care provider to ensure that you do not have any vitamin or mineral deficiencies that need correcting.
- Scientific evidence does not support the use of any supplement to prevent, slow, reverse, or stop mild cognitive impairment (MCI) or dementia or other related neurological disease.
- Melatonin is NOT recommended for older people with dementia due to risk of increased falls and other adverse events, according to 2015 guidelines from the American Academy of Sleep Medicine.
Brain supplements review
Polyphenols
Polyphenols are naturally occurring compounds found largely in the fruits, vegetables, cereals and beverages. Polyphenols are abundant micronutrients in plant-derived foods and are powerful antioxidants. Fruits like grapes, apple, pear, cherries and berries contains up to 200–300 mg polyphenols per 100 grams fresh weight 18 and beverages such as tea, red wine, cocoa, and coffee are major dietary sources of polyphenols. The products manufactured from these fruits, also contain polyphenols in significant amounts. Cereals, dry legumes, chocolate and beverages, such as tea, coffee, or wine also contribute to the polyphenolic intake 19, 20. Typically a glass of red wine or a cup of tea or coffee contains about 100 mg polyphenols.
Polyphenols are secondary metabolites of plants and are generally involved in defense against ultraviolet radiation or aggression by pathogens and may also contribute to the bitterness, astringency of the food. Researchers have explored that these molecules are very good antioxidants and may neutralize the destructive reactivity of undesired reactive oxygen/nitrogen species produced as byproduct during metabolic processes in the body. Epidemiological studies have revealed that polyphenols provide a significant protection against development of several chronic diseases such as cardiovascular diseases, cancer, diabetes, infections, aging, asthma, etc 18.
There has recently been growing interest, supported by a number of epidemiological and experimental studies, on the possible beneficial effects of polyphenols on brain health 21.The largest group of polyphenols is the flavonoids. There are six dietary groups of flavonoids: flavones (e.g., apigenin, luteolin), which are found in parsley and celery; flavanones/flavanonols (e.g., hesperetin, naringenin/astilbin, engeletin), which are mainly found in citrus fruit, herbs (oregano), and wine; isoflavones (e.g., daidzein, genistein), which are mainly found in soy and soy products; flavonols (e.g., kaempferol, quercetin), which are found in onions, leeks, and broccoli; flavanols (e.g., –catechin, [–]-epicatechin, epigallocatechin, and epigallocatechin gallate), which are abundant in green tea, red wine, and chocolate; and anthocyanidins (e.g., pelargonidin, cyanidin, and malvidin), whose sources include red wine and berry fruits. The nonflavonoid group of polyphenols may be separated into two different classes: the phenolic acids, including the hydroxybenzoic acids (C1–C3 skeleton) and hydroxycinnamic acids (C3–C6 skeleton), and the stilbenes (C6–C2–C6 skeleton). Caffeic acid is generally the most abundant phenolic acid, and is mainly found as the quinic ester, chlorogenic acid in blueberries, kiwis, plums, and apples. Resveratrol, the main stilbene, can be found in the cis or trans configurations, either glucosylated (piceid) or in lower concentrations as the parent molecule of a family of polymers such as viniferins, pallidol, or ampelopsin A. Resveratrol dietary sources include grapes, wine, and peanuts.
The consumption of tea, polyphenol-rich foods, fruit and vegetables, and total amounts of flavonoids have been shown to be associated with protection against, or slowed progression of, cerebrovascular diseases, such as stroke and neurologic disorders, including dementia, and cognitive impairment/decline in elderly populations. The literature on the effects of the above supplements and plant products on a healthy young population however is very scarce. Especially, literature on the effects of these products on brain functioning, cognition, motor performance, and so on, in an athlete population is almost inexistent.
Polyphenol intake can be increased by conscious dietary choices of foods with high content (juices, tea infusions, chocolate, etc.), but the concentration of active substances are much higher in supplements. Some of the experiments performed in animal studies typically used high doses, which represent sometimes large amounts of fresh fruits to have the same absolute amount of active substances in humans.
A recent first meta-analysis of polyphenols and their effect on human athletic performance suggest that polyphenol supplementation (and especially quercetin) is associated with a clear moderate improvement of performance with no reported adverse effects 22. Polyphenols have consistently been associated with a reduced risk of developing dementia, improved cognitive performance in normal aging, and improved cognitive evolution 21. The neuroprotective actions of dietary polyphenols involve a number of effects within the brain, including a potential to protect neurons against injury induced by neurotoxins, an ability to suppress neuroinflammation, and the potential to promote memory, learning, and cognitive function 23. While many of the mechanisms underpinning their beneficial effects remain to be elucidated, it has become clear that they partly involve decreases in oxidative/inflammatory stress signaling, increases in protective signaling, and may also involve hormetic effects to protect neurons against oxidative and inflammatory stressors. Also, polyphenols can improve regional cerebral perfusion 24.
Figure 1. Polyphenols Chemical Structure
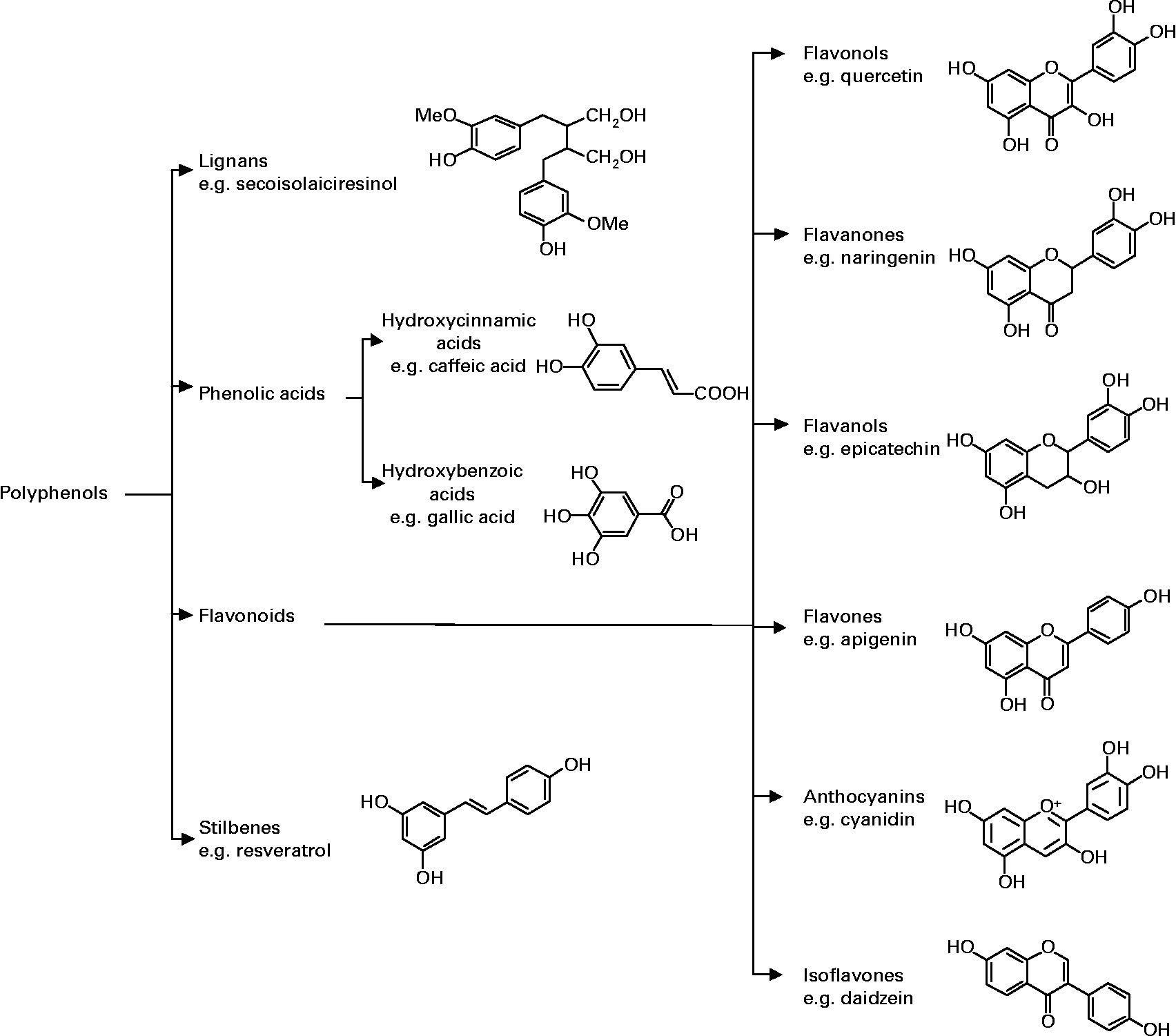
Table 1. Polyphenols Rich Foods
| Source (serving size) | Polyphenol content | ||
| By wt or vol | By serving | ||
| mg/kg fresh wt (or mg/L) | mg/serving | ||
| Hydroxybenzoic acids | Blackberry (100 g) | 80–270 | 8–27 |
| Protocatechuic acid | Raspberry (100 g) | 60–100 | 6–10 |
| Gallic acid | Black currant (100 g) | 40–130 | 4–13 |
| p-Hydroxybenzoic acid | Strawberry (200 g) | 20–90 | 4–18 |
| Hydroxycinnamic acids | Blueberry (100 g) | 2000–2200 | 200–220 |
| Caffeic acid | Kiwi (100 g) | 600–1000 | 60–100 |
| Chlorogenic acid | Cherry (200 g) | 180–1150 | 36–230 |
| Coumaric acid | Plum (200 g) | 140–1150 | 28–230 |
| Ferulic acid | Aubergine (200 g) | 600–660 | 120–132 |
| Sinapic acid | Apple (200 g) | 50–600 | 10–120 |
| Pear (200 g) | 15–600 | 3–120 | |
| Chicory (200 g) | 200–500 | 40–100 | |
| Artichoke (100 g) | 450 | 45 | |
| Potato (200 g) | 100–190 | 20–38 | |
| Corn flour (75 g) | 310 | 23 | |
| Flour: wheat, rice, oat (75 g) | 70–90 | 5–7 | |
| Cider (200 mL) | 10–500 | 2–100 | |
| Coffee (200 mL) | 350–1750 | 70–350 | |
| Anthocyanins | Aubergine (200 g) | 7500 | 1500 |
| Cyanidin | Blackberry (100 g) | 1000–4000 | 100–400 |
| Pelargonidin | Black currant (100 g) | 1300–4000 | 130–400 |
| Peonidin | Blueberry (100 g) | 250–5000 | 25–500 |
| Delphinidin | Black grape (200 g) | 300–7500 | 60–1500 |
| Malvidin | Cherry (200 g) | 350–4500 | 70–900 |
| Rhubarb (100 g) | 2000 | 200 | |
| Strawberry (200 g) | 150–750 | 30–150 | |
| Red wine (100 mL) | 200–350 | 20–35 | |
| Plum (200 g) | 20–250 | 4–50 | |
| Red cabbage (200 g) | 250 | 50 | |
| Flavonols | Yellow onion (100 g) | 350–1200 | 35–120 |
| Quercetin | Curly kale (200 g) | 300–600 | 60–120 |
| Kaempferol | Leek (200 g) | 30–225 | 6–45 |
| Myricetin | Cherry tomato (200 g) | 15–200 | 3–40 |
| Broccoli (200 g) | 40–100 | 8–20 | |
| Blueberry (100 g) | 30–160 | 3–16 | |
| Black currant (100 g) | 30–70 | 3–7 | |
| Apricot (200 g) | 25–50 | 5–10 | |
| Apple (200 g) | 20–40 | 4–8 | |
| Beans, green or white (200 g) | 10–50 | 2–10 | |
| Black grape (200 g) | 15–40 | 3–8 | |
| Tomato (200 g) | 2–15 | 0.4–3.0 | |
| Black tea infusion (200 mL) | 30–45 | 6–9 | |
| Green tea infusion (200 mL) | 20–35 | 4–7 | |
| Red wine (100 mL) | 2–30 | 0.2–3 | |
| Flavones | Parsley (5 g) | 240–1850 | 1.2–9.2 |
| Apigenin | Celery (200 g) | 20–140 | 4–28 |
| Luteolin | Capsicum pepper (100 g) | 5–10 | 0.5–1 |
| Flavanones | Orange juice (200 mL) | 215–685 | 40–140 |
| Hesperetin | Grapefruit juice (200 mL) | 100–650 | 20–130 |
| Naringenin | Lemon juice (200 mL) | 50–300 | 10–60 |
| Eriodictyol | |||
| Isoflavones | Soy flour (75 g) | 800–1800 | 60–135 |
| Daidzein | Soybeans, boiled (200 g) | 200–900 | 40–180 |
| Genistein | Miso (100 g) | 250–900 | 25–90 |
| Glycitein | Tofu (100 g) | 80–700 | 8–70 |
| Tempeh (100 g) | 430–530 | 43–53 | |
| Soy milk (200 mL) | 30–175 | 6–35 | |
| Monomeric flavanols | Chocolate (50 g) | 460–610 | 23–30 |
| Catechin | Beans (200 g) | 350–550 | 70–110 |
| Epicatechin | Apricot (200 g) | 100–250 | 20–50 |
| Cherry (200 g) | 50–220 | 10–44 | |
| Grape (200 g) | 30–175 | 6–35 | |
| Peach (200 g) | 50–140 | 10–28 | |
| Blackberry (100 g) | 130 | 13 | |
| Apple (200 g) | 20–120 | 4–24 | |
| Green tea (200 mL) | 100–800 | 20–160 | |
| Black tea (200 mL) | 60–500 | 12–100 | |
| Red wine (100 mL) | 80–300 | 8–30 | |
| Cider (200 mL) | 40 | 8 | |
Flavonoids
Flavonoids are natural polyphenol compounds found in fruits and other plants such as berries, apples, wine, tea, and cocoa 27. Sub-classes of flavonoids include isoflavones (in soybeans and peanuts), flavanols (in tea and cocoa), flavonols (in fruits and vegetables), flavones (in cereals and herbs), anthocyanidins (in berries), and flavanones (in citrus fruits) 28. The actions of dietary flavonoids on cognition appear to be related to various potential actions on the brain, including neuroprotection from neurotoxins and neuro-inflammation, synaptic signalling activation and improved cerebrovascular blood flow. These actions are driven by the apparent ability of flavonoids to interact with neuronal signalling cascades in the brain, resulting in the inhibition of cell death via exposure to neurotoxic species, the promotion of neuronal survival and differentiation, and an enhancement of peripheral and cerebral blood perfusion. Effects of flavonoids on cognition are likely the result of optimal maintenance of brain morphology due to the regulation of neuronal signalling and protection against neuronal losses 29.
Four included studies considered acute effects of flavonoids on cognitive performance in a total of 137 young healthy adults. All studies utilised crossover designs and were conducted in non-military populations. Although each study used participants from both genders, there was a greater proportion of female participants. The sub-classes of flavonoids investigated were flavanones, cocoa flavanols, anthocyanins, and epigallocatechin gallate (EGCG; a flavonoid typically found in green tea). The flavonoid dose and administration methods were as follows: 70.5 mg flavonones in a commercial citrus juice 30, 525 ± 5 mg of polyphenols per 60 kg of body weight in a blackcurrant extract and a blackcurrant fruit juice 31, 520 mg and 994 mg of cocoa flavanols in a dairy-based cocoa drink 27 and 135 mg and 270 mg of epigallocatechin gallate in capsules 32. All studies investigated the effects of single doses of flavonoids. Information processing speed, attention/vigilance, memory, and executive function were measured. Two studies used cognitive test batteries intended to increase the cognitive demand placed on participants 31.
Flavonone supplementation in citrus juice improved information processing speed (digit symbol substitution task) but not inhibitory control (Go/No-Go task) 31. Blackcurrant extract mitigated deteriorating accuracy in sustained attention (RVIP). In addition, Scholey et al. 27 found that the optimal dose of cocoa flavanols (520 mg) improved working memory, in terms of serial threes subtraction, but not serial sevens. Conversely, Wightman et al. 32 found no effect of EGCG on working memory (either serial threes or serial sevens subtraction). Across all studies, flavonoids had no impact on executive function 30. Despite the high quality of two of the included papers, there still remains insufficient quality empirical support to allow us to make any recommendations regarding flavonoid supplementation.
Cocoa flavanols
Cocoa flavanols, as found in dark chocolate, have been reported to have beneficial effects on cognition 33 but it is not known if this effect is also present in combination with exercise. Acute cocoa flavanols intake increased cerebral oxygenation during a cognitive task assessing executive function, but without any impact on cognitive performance. When combining cocoa flavanols and exercise, cocoa flavanols had no additive effect on the exercise-induced cognitive enhancement and the associated increased cerebral oxygenation and perfusion 24. The increased brain perfusion caused by acute cocoa flavanol intake is supported by a nitric oxide mediated vasodilatation 34. Also, due to the large variation in flavanol content in chocolate and cocoa products, it is critical to compare the dosages of flavanols rather than simply the amounts of chocolate or administered cocoa products in clinical trials 35.
Nitrate
Nitrate is obtained in the diet through the consumption of nitrate (NO3−) rich vegetables, including beetroot, broccoli, lettuce, and spinach 36. Although there is limited research on the effects of nitrate supplementation on cognitive functions in humans, the beneficial effect of nitrate on cognition appears to be related to its conversion to nitric oxide (NO). Nitrate derived from vegetables is consumed as part of a normal diet and is reduced endogenously via nitrite to nitric oxide (NO). Nitric oxide (NO) is involved in the modulation of cerebral blood flow, which is important for optimal brain function. In older adults, dietary nitrate supplementation resulted in improved cerebral blood flow to areas of the brain related to executive functioning 37.
Two studies involving 56 participants have assessed the effect of a dietary nitrate supplementation on cognitive performance in healthy young adults 38, 36. A double-blind crossover design 38 and a double-blind, placebo-controlled, parallel groups design 36 were employed. Participants were non-military and were either recreationally active men 38 or a mixed male and female sample 36. Nitrate supplementation was assessed under different conditions: during a physically demanding task (cycling) 38 and in response to a cognitive demand battery 36 to measure cognition. Both studies assessed the effect of single doses of a similar nitrate-rich drink (beetroot juice with added apple and blackcurrant juice; containing 5 to 5.5 mmol of nitrate). Performance on measures of attention (rapid visual information processing test, RVIP), working memory (serial subtraction) 36, and executive function (Stroop) 38 were assessed.
The beetroot juice did not enhance attentional performance 36, nor did it mitigate the deterioration in attentional abilities as a result of increasing exercise intensity 38. Wightman et al. 36 observed greater accuracy on serial threes subtraction but not serial sevens subtraction. However, this effect should be interpreted with caution as the nitrate group underperformed at baseline. No positive effects of beetroot juice on executive functioning were observed 38. Although negligible improvements were found, the small number of papers investigating the impact of nitrates and cognitive performance indicate more research in this domain is warranted.
Caffeine
Caffeine is a plant alkaloid that is quickly absorbed and found in food and drinks such as coffee, tea, energy drinks, soft drinks, and chocolate 39; peak caffeine concentrations are reached between 15 and 120 minutes after ingestion 40. The energising and concentration boosting qualities of caffeine are well-known and are the reason caffeine is the most commonly used psychostimulant 41. A growing body of literature has investigated the effects of caffeine on cognitive performance, particularly during/after sleep deprivation. Caffeine works by blocking adenosine receptors within the brain and has demonstrated positive changes (at varying doses) on the alerting, orienting and executive control attention networks within the brain, specifically enhancing alertness, vigilance and reaction time. It has not demonstrated improvements in memory performance or other executive functions, such as decision-making 40. A recent systematic literature review found caffeine supplementation to be promising for maintaining or improving several aspects of cognitive performance in sleep-deprived people. These are tasks requiring attention, executive function and information processing speed 42.
There are no clinical trials that have studied the effects of caffeine on brain health or dementia prevention 43. Evidence suggests that caffeine has cognitive benefits, including alertness and attention 44. Human studies on whether long-term use of coffee or caffeine can reduce risk of cognitive decline or Alzheimer’s disease are inconclusive. Meta-analyses and systematic reviews of observational studies report that drinking coffee can either provide a long-term benefit to brain health or have no effect 45, 46. These observational studies have a number of issues that result in inconsistencies. For instance, it is unknown whether people who drink coffee share other aspects of health and lifestyle that might be responsible for better brain health. In addition, coffee and caffeine consumption are rarely measured in the same way between studies.
Few studies have examined whether coffee or caffeine is beneficial to patients with dementia. One study reported that caffeine consumption in elderly patients with dementia improved some physical symptoms and apathy, but it interrupted sleep when consumed after 6 pm 47. Another study reported that individuals with mild cognitive impairment (MCI) were much less likely to progress to dementia if they had higher caffeine levels in their blood 48. These studies, however, did not directly assess whether caffeine promotes brain health in individuals with MCI or dementia. In addition, people with dementia often suffer sleeping problems and are sometimes taken off caffeine for this reason. If caffeine impairs sleep, it could also impair cognitive function or even accelerate cognitive decline.
Even if long-term coffee intake does promote brain health, it is unclear whether elderly people might reduce their risk of Alzheimer’s disease if they start drinking coffee later in life. In one study, cognitively normal elderly people who increased their consumption of caffeine were at a greater risk of developing mild cognitive impairment (MCI) 49. The acute cognitive benefits from coffee may also decrease with age, eventually causing cognitive deficits 50. However, in another study, individuals with mild cognitive impairment (MCI) were less likely to progress to dementia if they had higher caffeine levels in their blood 48.
In sleep-deprived participants, caffeine enhanced the performance of military personnel on attentional tests 51. Furthermore, repeated doses of caffeine mitigated the decline in information processing speed, vigilance, and logical reasoning associated with sleep deprivation 51. Similar results have been found during a driving task undertaken by sleep-deprived 52 and sleep-restricted 53 university students. Driving a vehicle requires attentional control functions of alertness, orienting and executive attention, all of which can be impaired by sleep deprivation. Despite one of the driving studies measuring drowsiness objectively with the Johns Drowsiness Scale 52 and the other measuring subjective sleepiness 53, both studies found that drowsiness/sleepiness after sleep deprivation impaired driving ability. Caffeine mitigated this effect, and subsequently, driving ability did not deteriorate to the same extent after caffeine was consumed. Caffeine also mitigated the effect of sleepiness on driving ability after restricted sleep 53. Similar improvements in executive control performance were found in sleep-deprived and well-rested participants, with caffeine ameliorating the effect of sleep deprivation on logical reasoning 51.
In well-rested individuals, caffeine improved memory (recognition) and aspects of information speed, specifically, choice reaction time but not simple reaction time 54. In addition, 400 mg of caffeine enhanced executive function (conflict resolution) and alertness, but not selective attention (as measured by the Attention Network Task) 55. Furthermore, although one standard cup of caffeinated coffee improved executive function when measured by the ecologically valid Jansari Assessment of Executive Function, it failed to do so when assessed by the Stroop task 56. This suggests that one standard cup of coffee does not influence executive function, or that traditional tests of executive function such as the Stroop task may lack the sensitivity to detect the enhancing effects of caffeine. Caffeine was found to have no effect on other aspects of memory performance in well-rested participants 57.
Taken together, findings from the well-controlled studies suggest that the appropriate dose of caffeine might enhance attention, memory, problem solving and logical reasoning in sleep-deprived young adults 58. Furthermore, this supplement might also be used to mitigate the joint effect of sustained operations and sleep deprivation on attention and vigilance. Further quality research is necessary before definitive conclusions can be reached about other cognitive functions or contexts.
Ginseng
Panax ginseng also known as Korean ginseng or Asian ginseng, is a plant used in traditional Chinese medicine 59. Panax ginseng often comes in either white or red ginseng forms. White ginseng is fresh ginseng that has been air-dried without being heated and is often used for long periods. Red ginseng is first steamed, then dried, and has a reddish color; due to its stimulating effects, it is typically used short-term 60. Ginseng can also be consumed as soup (e.g., Samgye-tang, which is ginseng chicken soup), tea (Insam-cha, or ginseng tea), liquor (Insam-ju, or ginseng liquor), or in energy drinks. Ginseng roots contain compounds called ginsenosides (saponins), comprising of 30 identified types, which have antioxidative and anti-inflammatory effects 61. Panax ginseng is purported to enhance longevity, promote cognitive functions, and alleviate fatigue. Some clinical trials have reported that Panax ginseng treatment improves cognitive functions in healthy people and in dementia patients, but the evidence is mixed, and many others have shown a lack of benefit.
Currently, the mechanisms that explain the cognitive effects of ginseng are not known 62. Ginsenosides have been demonstrated to cause many forms of physiological effects, including modulation of the cardiovascular immune response systems, deceleration of platelet aggregation, modulation of neurotransmission, and nitric oxide synthesis 62.
There have been numerous clinical trials and observational studies on Panax ginseng supplementation. While some studies have reported benefit for cognitive functions 63, many others have shown a lack of benefit 64 and overall there is a lack of high-level evidence that the benefits of Panax ginseng outweigh the risks. A meta-analysis of five double-blind randomized controlled trials in healthy subjects reported that Panax ginseng treatment for 8-12 weeks showed improvement in some aspects of cognitive function, behavior, and quality of life, though the evidence was not convincing or consistent across studies 65.
One of the included trials showed that ginseng treatment (200 mg/day) significantly improved working memory and mental arithmetic, but not attention or concentration 66, while a different study reported that ginseng treatment (400 mg/day) significantly improved attention but not memory 67. In yet another study, ginseng treatment (400 mg/day) for 8-9 weeks improved selective reminding but not attention, concentration, or motor performance 68.
Several randomized controlled trials have tested Panax ginseng in Alzheimer’s disease patients. In one systematic review that included two randomized controlled trials for ginseng, both trials showed that ginseng supplementation resulted in significant improvements in cognitive outcomes; however, due to the limitations in the methodological quality of the trials, results have not been conclusive 69. In one study 70, patients with moderate-to-severe Alzheimer’s disease treated with 4.5 g/day of ginseng showed significant improvement in cognitive functions after 12 and 24 weeks of supplementation. Similar results were reported in another study with the use of 4.5 and 9.0 g/day of Korean white ginseng in patients with mild-to-moderate Alzheimer’s disease 71. However, improvements in cognitive functions disappeared 12 weeks after discontinuation of treatment.
The longest placebo-controlled clinical trial included 61 Alzheimer’s patients and lasted two years 72. In the low-dose Panax ginseng group (4.5 g/day), cognitive scores (as measured by the Mini-Mental State Examination) improved after 48 weeks, then slightly decreased at 96 weeks. In the high-dose group (9.0 g/day), cognitive scores showed slight improvement at 48 and 96 weeks. In this study, maximum cognitive improvement was observed around 24 weeks, then sustained for two years.
Although some positive findings have been reported, further studies with more optimal methodological quality are necessary to evaluate the safety and efficacy of ginseng supplementation in individuals with Alzheimer’s disease and other dementias.
Most recently, a double-blind randomized controlled trial of 52 healthy individuals reported that Panax ginseng treatment (1 g/day) for eight weeks significantly increased the volume of a brain region important for memory and improved scores on executive function, attention, and memory, effects that were not seen in the placebo group 63.
In an observational study of 6,422 elderly people in South Korea, those who had higher lifetime cumulative ginseng intake (over five years) showed higher cognitive scores compared to those who never consumed ginseng, after controlling for factors such as age, sex, education, socioeconomic status, smoking, alcohol intake, cardiovascular disease, and APOE genotype 73. But changes in cognitive function over four years of follow-up did not differ based on ginseng intake. As this study was an observational study, it was not designed to prove that ginseng intake is responsible for the higher cognitive functions.
Multiple meta-analyses that included data from numerous randomized controlled clinical trials have reported that Panax ginseng is generally safe when taken alone, is not associated with serious adverse events, and incidences of adverse events are comparable to those of placebo groups 74. However, high doses of ginseng or taking ginseng with caffeine or other products may lead to insomnia, rapid heartbeat, high blood pressure, headaches, nervousness, and gastrointestinal issues. Panax ginseng interacts with many medications, including warfarin, aspirin, medications for depression, immunosuppressants, alcohol, and others 75. Ginseng affects blood sugar levels, and therefore may interact with anti-diabetics.
Gingko biloba
Gingko biloba is an herbal supplement derived from extracts in the leaves of the gingko biloba tree 76 and is commonly used in a standardised form in clinical studies 77. Ginkgo biloba is believed to improve memory and other aspects of cognitive function. The results on the acute effects of Ginkgo biloba intake are conflicting 78. In clinical trials, ginkgo biloba failed to prevent cognitive decline or dementia. It might slightly improve memory in those with dementia, though the evidence is mixed. It is generally considered safe, though it does pose some health risks to specific groups. The active molecules of gingko biloba are believed to be linked to an array of potential physiological effects which can influence cognition. These physiological effects include: the scavenging and inhibition of free radicals, anti-platelet activating factor, reducing neuronal death, improved blood circulation, increased cerebral perfusion, and protection against hypoxia 79. Gingko biloba has been claimed to improve short-term memory, rate of learning, and reaction time 76. Multiple clinical trials involving thousands of patients have conclusively shown that treatment with ginkgo biloba for up to six years does not prevent cognitive decline or dementia, including Alzheimer’s disease 80. This is disappointing since preclinical studies indicated that gingko biloba contains several components that improve brain blood flow and mitochondrial function 81. Mitochondria are the “power plants” of human cells that often malfunction with age and in diseases such as Alzheimer’s disease.
Ginkgo biloba may slightly improve memory and cognitive function for people with memory problems or dementia. However, clinical guidelines are mixed. While the World Federation of Societies of Biological Psychiatry guidelines suggest that a certain ginkgo biloba extract may be used to treat dementia symptoms, the British Association for Psychopharmacology and the American Academy of Family Physician concluded that its benefits are inconsistent and unreliable.
Similarly, clinical trial results are mixed. A 2009 high-quality meta-analysis concluded that the effects of ginkgo biloba on cognitive impairment and dementia were inconsistent and unreliable 82. There are two other recent meta-analyses in dementia patients. In one analysis, seven studies showed that patients using ginkgo had improved scores on certain cognitive performance tests. Two studies in the same analysis using different assessments, however, did not show a statistically significant difference 83. Another meta-analysis of patients with mild cognitive impairment and Alzheimer’s disease showed that after 24 weeks of ginkgo, in combination with conventional medicine, they improved cognitive performance scores 84.
All studies assessed the effect of gingko biloba on memory; whilst improvements were found, this was not consistent across all memory tasks; dose-dependent effects were observed for gingko biloba, and in some cases differential effects were found for gingko biloba and ginkgo biloba complexed with phospholipids. A 360 mg dose of gingko biloba enhanced speed of memory, whereas a 240 mg dose degraded performance 76. A 120 mg dose of ginkgo biloba or 120 mg gingko biloba complexed with phosphatidycholine generally had no impact on overall speed of memory 76, 59, 79. Conversely, gingko biloba complexed with phosphatidylserine enhanced overall speed of memory, as well as memory accuracy in picture recognition 79. Longer durations of gingko biloba supplementation six weeks 85 or five days 86 also failed to enhance memory ability. Working memory (serial sevens subtraction speed) was enhanced four to six hours post-dose 59; however, this is in contrast to Scholey and Kennedy 87, who observed improved accuracy. A single 120 mg dose of gingko biloba improved secondary memory, a composite score derived from performance accuracy on delayed word/picture recognition, and immediate/delayed word recall tasks, with this effect being maximal one hour post supplementation 79. Nil or minimal effects were observed for: reaction time 86, attention 85, working memory (including serial threes subtraction) 79, and executive function (mental flexibility or planning ability) 85.
In addition, extended supplementation of gingko biloba (>1 week) failed to elicit any cognitive improvement 85. It should be noted that Kennedy et al.’s studies 79 combined results from individual tests into the cognitive factors of speed of attention, accuracy of attention, speed of memory and quality of memory, all derived from a factor analysis of the Cognitive Drug Research computerised assessment battery. However, in some of their studies they evaluated performance on underlying tasks when there was no impact on the overall cognitive factor 79.
In summary, the studies investigating the impact of gingko biloba on cognitive performance yielded mixed results. This fact, together with the uncertainty about risk of bias and poor paper quality, prevents us from making any recommendations about the use of gingko biloba as a means of enhancing cognitive performance. Nonetheless, further quality research is warranted that examines in more detail the dose- and time-dependent effects.
Ginkgo biloba is usually safe when properly used by healthy adults 88. Although some clinical trials suggested ginkgo might raise the risk of stomach bleeding in older adults, a meta-analysis of numerous clinical trials found no such association 89. Because ginkgo biloba can dilate blood vessels, it may not be safe in patients taking medication for high blood pressure. It may also be unsafe for children, people with diabetes, or women trying to become pregnant.
Standardized ginkgo biloba extracts are generally safe for most people at oral doses of 120 to 240 mg per day. Although some ginkgo biloba extracts are sold over-the-counter, the EGb761® formulations tested in clinical trials are only available by prescription.
Guarana
Guarana seed comes from plants found in the Amazon, and it contains theophylline, theobromine, and caffeine. Guarana plant extract is used predominantly as a food additive and is generally consumed with other herbal supplements, such as ginseng 90. Guarana’s stimulant properties have been attributed to its caffeine content and high quantities of saponins and tannins 90. The cognitive benefit of guarana is proposed to be related to its ability to decrease the physiological response to physical or psychological stressors 91. It has been proposed that the impact of guarana on cognition is due to the synergistic effect of its constituents, such as caffeine 92 and theanine 93. Theobromine is a methylxanthine that is an adenosine receptor antagonist (as caffeine) and might improve cognitive function.
Four studies, involving a total of 224 participants, examined the effect of acute doses of guarana on cognition. Two utilized crossover designs and two used an independent groups design. Sample compositions varied across the studies: predominantly female (two studies), approximate even gender distribution (one study), and active males only (one study). A standardized guarana extract was used by Kennedy et al. (75 mg) 91 and Haskell et al. (37.5 mg, 75 mg, 150 mg, 300 mg) 94. The other two studies administered a multivitamin + guarana supplement (Berocca Boost®, hereby referred to as guarana and multivitamins) in the form of an effervescent tablet dissolved in water. The guarana and multivitamins contained 222.2 mg of guarana (including 40 mg caffeine), and equal to or above the recommended dietary allowance (RDA) of B vitamins. The two guarana and multivitamins studies induced fatigue using a traditional cognitive demand battery 90 or exercise in combination with a repeated battery of cognitive tests 95. Attention, memory, working memory, and executive function were measured.
Two studies 96, 97 have investigated the effects of guarana on cognitive performance and found that memory, mood, and speed during an attention task improved. The administration of a vitamin and mineral complex with guarana has been shown to attenuate mental fatigue and improve performance during cognitively-demanding tasks 96, 97. Veasey et al. 98 showed that consuming a vitamin and mineral complex containing guarana, prior to exercise, can positively impact subsequent memory performance and reduce perceived exertion during a moderate-intensity run in active males. Probably, the caffeine content and/or the combination with theobromine could be responsible for these effects. Pomportes et al. 99 recently investigated the influence of serial mouth rinsing with guarana complex on cognitive performance (i.e., cognitive control and time perception) during a 40-minutes submaximal exercise, and found a likely improvement on a cognitive task. However, when examined more carefully, this commercial product also contains caffeine. Although no recommendation can be given for the efficacy of guarana for cognitive enhancement, further research using well-controlled studies might shed more light on the dosage and time effects of this supplement on cognitive performance.
Rhodiola rosea
Other plant products such as Rhodiola rosea and sage might also improve cognitive performance and reaction time. Rhodiola rosea is reported to influence endurance performance 100, but in this study there was no specific influence on sustained attention or reaction time. Noreen et al. 101 examined the effect of an acute dose of Rhodiola rosea on endurance exercise performance, perceived exertion, mood, and cognitive function. They found that ingestion of 3 mg/kg Rhodiola rosea decreases heart rate response to submaximal exercise and appears to improve endurance exercise performance by decreasing the perception of effort. No effects on cognition were found. Sage improves alertness 102 and memory 103.
Phosphatidylserine
Phosphatidylserine is a class of phospholipids found in cell membranes. Its levels and location within the brain can affect important signaling pathways for cell survival and communication. Phosphatidylserine includes two fatty acids that can vary from saturated or monounsaturated to polyunsaturated omega-6 and omega-3 versions like docosahexaenoic acid (DHA). Some clinical trials of phosphatidylserine supplements have shown modestly improved cognitive function, but better designed trials reported no benefit. No clinical research—observational or randomized trials—has evaluated whether phosphatidylserine supplements can protect against cognitive decline or dementia.
The amount of phosphatidylserine in the brain remains mostly constant throughout life, although slight changes have been reported with Alzheimer’s disease and aging 104. It is not clear whether supplements can increase phosphatidylserine brain levels, especially if they do not include DHA 104. Small trials suggested that phosphatidylserine might slightly improve cognition for Alzheimer’s patients but effects were short-lived or detectable only in severely impaired patients 105, 106, 107. Benefits have not been confirmed in larger trials. Small clinical trials suggest that phosphatidylserine supplements can yield slight cognitive improvements for elderly people, but effects were not large enough to be clinically relevant 108, 109, 110. Long-term use has not been well-studied, but one trial reported that effects were short-lived, fading before six months 111. The strongest trial of phosphatidylserine, which used a soy-derived formulation, reported no benefit 112.
Phosphatidylserine doses typically range from 80 to 500 mg per day. While supplements derived from marine animals often contain high amounts of DHA, those derived from soy lecithin do not. The presence of DHA may be important for increasing synthesis of phosphatidylserine in the brain. However, in theory, any phosphatidylserine taken with a separate DHA supplement could have the same effect as DHA-enriched phosphatidylserine because phospholipids are broken down in the gut before being absorbed 104.
Small clinical trials suggest that phosphatidylserine supplements produce no serious adverse effects for elderly patients, although it may reduce blood pressure or increase body weight 113. Since some supplements are prepared from cow brains, it is theoretically possible for those supplements to transmit prion diseases such as mad cow 114, though no cases have been reported.
L-serine
L-serine is an amino acid essential for the synthesis of phosphatidylserine, which is a component of the membrane of brain cells (i.e., neurons) 115. L-serine is also essential for growth of neuronal processes. It can be produced in the body, including the brain, but an external supply from the diet is essential in maintaining necessary levels. Although preclinical studies suggest L-serine may inhibit inflammation in the brain, levels of L-serine in humans do not appear to be associated with dementia or cognitive decline. However, it is not clear whether L-serine supplements directly increase L-serine levels in the brain. In a study on traumatic brain injury in small mammals, L-serine treatment helped to protect brain tissue and improve recovery of neurological functions by inhibiting inflammation 116. Such protective effects have not been confirmed in humans yet.
L-serine is a naturally occurring dietary amino acid. It is abundant in soy products, sweet potatoes, eggs, meat, and some edible seaweed. L-serine is also sold as a dietary supplement in capsule and powder forms. The dose used in an ongoing Alzheimer’s trial is 15 grams, twice daily, in the form of gummies 117. Most supplements come in the form of 500 mg capsules. Because L-serine is a naturally occurring amino acid, supplementation is likely safe in moderation.
No clinical studies have tested whether L-serine can prevent age-related cognitive decline or dementia, though one trial is underway now 117. No clinical studies have tested whether L-serine can improve cognitive functions or prevent age-related cognitive decline. Studies examining levels of L-serine have not reported any correlations with cognitive function 118.
A phase 2 clinical trial testing the effects of L-serine in early-stage Alzheimer’s patients is currently underway 117. There have been several studies examining cerebral spinal fluid and blood serum levels of L-serine in people with Alzheimer’s, but no clear differences with healthy people have been found, nor any correlations between L-serine levels and cognitive functions 119. Postmortem studies also showed that L-serine levels in the brain were comparable between Alzheimer’s disease patients and healthy people 120.
Preclinical studies suggest L-serine may benefit those exposed to the neurotoxin beta-methylamino-L-alanine (BMAA) 121. Your cells can mistake BMAA for L-serine and misincorporate it into proteins, which can lead to cell death and may increase biological markers of Alzheimer’s disease 122. Laboratory studies indicate that L-serine may prevent misincorporation of BMAA and cell death 122. However, it is unclear whether L-serine affects biological markers of Alzheimer’s in the absence of such neurotoxins.
Beta-alanine
Beta-alanine is an amino acid produced naturally in the body that can also be acquired via the diet from meat and/or dietary supplements 123. Due to its presence in other tissues, such as the brain, it is postulated that the beta-alanine precursor, carnosine, may have potential cognitive effects. Early animal studies indicate there may be a link to focus, alertness and cognitive function during stress and fatigue 124.
Only one known study to date has investigated the effects of beta-alanine on cognitive performance in healthy young humans 125, where both physical and cognitive performance were assessed after four weeks of 6 grams beta-alanine supplementation in a sample of military personnel. Twenty male soldiers were assessed on a variety of military tasks and a working memory task (serial subtraction) after induced fatigue from military training. Beta-alanine supplementation did not enhance working memory performance, but significant improvements in marksmanship and reaction time were found within the military context of operational task performance. This single study employing beta-alanine was deemed low quality.
Tyrosine
Tyrosine is a non-essential amino acid that is used by cells to synthesise proteins. Briefly, tyrosine is found in high-protein food sources and is synthesized from phenylalanine 126. Most importantly, tyrosine is the precursor for catecholamine synthesis, which occurs mainly in the brain or adrenal medulla. The catecholamines dopamine and noradrenaline are recognized as modulators of executive function, and are also released in response to stress. An appropriate level of dopamine and noradrenaline facilitates effective cognitive performance whereas an over- or under-abundance of either of these neurotransmitters can have an adverse effect. “Central fatigue hypothesis” 127 is where prolonged exercise and/or exposure to extreme stress (extreme temperatures, etc.) alter the synthesis and level of catecholamines. Taken together, this provides good evidence to support that tyrosine, delivered appropriately and at the right dose, can evoke positive cognitive enhancement effects. A recent review 128 identified that tyrosine mitigated the impact of stressors such as sleep deprivation, noise, extreme climates and military combat training on a range of cognitive processes including memory, perceptual motor skills, and logical reasoning. However, the poor quality of papers and lack of physiological measures related to uptake of tyrosine meant they were unable to make firm recommendations about tyrosine supplementation; nonetheless they concluded that tyrosine may enhance cognitive performance and warranted further investigation.
A further eight studies involving 160 participants and investigating the effect of tyrosine on cognitive processing were found to fit the inclusion criteria. Apart from one study using a single-blind crossover design 129, all studies employed a double-blind placebo-controlled crossover design to examine the role of tyrosine in mitigating stress-induced cognitive declines. Mainly female participants were recruited across the eight studies: three recruited male participants, three used female participants, and two had a mix of both sexes. Tyrosine was administered using different methods: powders, capsules and bars; and at different doses from 2 g to a total dose of 150 mg/kg (approximately 12 g for 80 kg participant) as single or double doses. Tyrosine supplementation has been demonstrated to be most effective in situations of significant stress, physical, cognitive or otherwise. As such, the studies covered: cognitive demand 130, 131, 132, 133 and external stressors such as noise and thermal changes 134, 135, 129. One study evaluated whether tyrosine would modulate the effect of transcranial direct current stimulation on working memory performance 136.
Under cognitively stressed conditions tyrosine improved working memory 130 and various aspects of executive function, namely inhibitory control 131, cognitive flexibility (smaller switching costs) 133 and creative convergent thinking 132. Although tyrosine had no impact on cognitive performance in warm/hot environments 129, when heat stress was combined with physical exertion, tyrosine supplementation enhanced vigilance 134. Changes in the event-related potentials N100, P300 and Contingent Negative Variation, also reflected enhanced attention and executive function related to stimulus evaluation and decision-making 135. Tyrosine also improved working memory in unstressed individuals 136.
L-theanine
L-theanine is an amino acid structurally similar to glutamate and GABA, two neurotransmitters? important for brain function. L-theanine is contained in green, black, and oolong teas, which are all derived from Camellia sinensis, a perennial evergreen shrub. L-theanine is traditionally used to promote relaxation without sedative effects. Several clinical trials have examined the effects of L-theanine, alone or in combination with caffeine or green tea, on brain health. L-theanine supplements are available in both capsule and powder forms. A single cup (200 ml) of tea can contain 5 to 85 mg of L-theanine depending on the type, quality, and preparation of tea. Clinical trials examining the effects of L-theanine on cognitive function have used doses ranging from 12–250 mg/day, with the majority of studies using 200 mg/day 137, 138. Research suggests it is safe and has positive effects on cognitive function when combined with caffeine, but the effects of L-theanine alone appear to be modest and short-term. No studies have tested whether it can prevent dementia or cognitive decline.
It is currently unknown whether L-theanine can improve cognition or slow cognitive decline in people with dementia. While some benefits have been observed in preclinical studies of Alzheimer’s disease 139, L-theanine has not been clinically studied in dementia patients.
The long-term effects of L-theanine on cognitive health are unknown, but a few short-term human studies have shown small benefits. In a randomized controlled trial in patients with mild cognitive impairment, L-theanine taken with green tea extract for 16 weeks had no significant effect on memory and attention, though a trend for an improvement in memory was seen midway through the trial 140. The patients who had more severe impairment at the start of the trial appeared more likely to benefit from treatment, but these results have not yet been replicated.
Combinations of L-theanine and caffeine have been reported to acutely improve attention and alertness in small clinical trials, but the positive effects have been primarily attributed to caffeine 141. L-theanine may interact with caffeine, improving attention and ability to ignore distractions, and together, enhance performance on cognitively demanding tasks 142. In a small randomized controlled trial of healthy adults, L-theanine alone did not affect attentional focus 143. Other studies have reported mixed effects, with L-theanine decreasing the beneficial effects of caffeine on cognition and mood 144.
Preclinical studies have reported that L-theanine may reduce brain cell death 139 and oxidative damage 145 and increase levels of protective chemicals 146, but these effects have not been confirmed in humans.
Large meta-analyses of long-term tea consumption containing L-theanine have found that side effects are mild 147, but these results on tea may not apply to supplements. In a short randomized controlled trial, an L-theanine supplement (400 mg/day) was well-tolerated with no significant adverse events 148. Larger, long-term studies are needed.
The interactions between L-theanine and other drugs have not been well-studied. Clinical data suggest that L-theanine lessens the blood pressure increase caused by caffeine 149. Because of its possible effects on blood pressure 150, it may be dangerous to use in combination with blood pressure medications.
Vitamin A
Vitamin A is the name of a group of fat-soluble retinoids, including retinol, retinal, and retinyl esters 151. Vitamin A is involved in immune function, vision, reproduction, and cellular communication 152. Vitamin A is critical for vision as an essential component of rhodopsin, a protein that absorbs light in the retinal receptors, and because it supports the normal differentiation and functioning of the conjunctival membranes and cornea 153. Vitamin A also supports cell growth and differentiation, playing a critical role in the normal formation and maintenance of the heart, lungs, kidneys, and other organs 154.
A characteristic feature of inflammation of the nervous system is microglial activation 155. Inflammation occurs in chronic and acute neuropsychiatric diseases. Literature data indicates that microglia activation is known to be one of the causes of Alzheimer’s disease. Moreover, malfunctioning of the microglia may result in changes in local concentrations of retinoic acid 156. In addition, vitamin A and its derivatives play an important role in the differentiation of nerve cells, as well as in the expression of neurotransmitters in the brain and gene expression through interaction with retinoic acid and retinoid X receptors 157.
A literature review showed that vitamin A was the least studied of the antioxidant vitamins. Vitamin A intake or dietary intake may improve cognitive function in Alzheimer’s disease patients
Low dietary intake of vitamin A is associated with an increased risk of dementia, which was confirmed in the group of 333 participants 158. A study by Yuan et al. 159 showed that higher consumption of beta-carotene reduced the risk of cognitive impairment. There are also studies that do not confirm the beneficial effects of this ingredient.
In a prospective study conducted by Pèneau et al. 160, it was shown that the consumption of fruits, which are a source of beta-carotene, did not reduce the risk of cognitive dysfunction. Other studies on the effects of vitamin A on Alzheimer’s disease do not meet the inclusion criteria for this article.
Moreover, vitamin A is involved in neuronal differentiation and also influences the secretion of neurotransmitters in the brain 157.
In conclusion, it has been shown that Alzheimer’s disease patients are deficient in vitamin A, but in the case of increased consumption of beta-carotene, the assessment of its effect on cognitive abilities has failed to provide definitive evidence of benefit. For example, the Recommended Dietary Allowances (RDAs) for Vitamin A for adult Americans is 900 mcg retinol activity equivalents (RAE)/day for men, for women: 700 mcg retinol activity equivalents (RAE)/day 152. Vitamin A are given as retinol activity equivalents (RAE) to account for the different bioactivities of retinol and provitamin A carotenoids, all of which are converted by the body into retinol 161. One mcg RAE is equivalent to 1 mcg retinol, 2 mcg supplemental beta-carotene, 12 mcg dietary beta-carotene, or 24 mcg dietary alpha-carotene or beta-cryptoxanthin 152.
Vitamin B
The B vitamins are a group of water soluble vitamins comprising thiamine (B1), niacin (B3), pantothenic acid (B5), vitamin B6, biotin (B7), folate (B9), and vitamin B12. The B vitamins collectively play a critical role at all levels of brain function as co-enzymes and precursors of enzymatic processes. They are important for energy production, DNA/RNA synthesis/repair, genomic/non-genomic methylation, and the production of neurochemicals and signalling molecules 162. The mechanisms by which B vitamins affect cognition are still unknown. The B vitamins folate, B6, and B12 are known to be involved in the modulation of homocysteine levels; this is important as elevated plasma homocysteine has been associated with poor cognition. Although there is no firm evidence of this relationship, it is likely that the association of the B vitamins with homocysteine metabolism is a by-product of other unknown biological factors that impact on cognitive function 163.
There is a shortage of well-controlled studies assessing the impact of supplementation of B vitamins on healthy young adults. One study assessed the effect of folate, vitamin B6, and vitamin B12 supplementation on cognitive function in 56 healthy young females with no external stressors 164. High doses of B vitamins (750 µg folate, 15 µg vitamin B12, 75 mg vitamin B6) were administered using tablets or capsules, for five weeks 164. Information processing speed, attention, memory and executive function were measured. There was a trend towards supplementation with folate, vitamin B6 and vitamin B12 enhancing aspects of memory performance. There was no impact on other cognitive measures. This study is of low quality with a high level of bias risk. More research is required to determine the effect of the vitamin Bs on cognitive performance.
Vitamin C and E
Vitamins C (ascorbic acid) and vitamin E are essential nutrients for humans. Naturally occurring vitamin E exists in eight chemical forms (alpha-, beta-, gamma-, and delta-tocopherol and alpha-, beta-, gamma-, and delta-tocotrienol) that have varying levels of biological activity 165. Alpha- (or α-) tocopherol is the only vitamin E form that is recognized to meet human requirements 166. People who consume high levels of these vitamins through their diets have a lower risk of dementia, although it remains unclear whether the key factor is a healthy diet or the specific vitamins. Supplements do not appear to offer the same protection. While vitamin C is generally safe for healthy people, some trials have linked vitamin E supplements with a slightly shorter lifespan and an increased risk of cancer.
In patients with Alzheimer’s disease, there is a correlation between blood vitamin C and vitamin E levels and dementia 167, but these could be due to the changes in nutrition and absorption that are common for such patients 168. Several meta-analyses of clinical trials reported that vitamin E supplementation has very little to no protective effects on cognitive function for dementia patients 169. However, a 2014 clinical trial of vitamin E and memantine reported that patients with mild-to-moderate Alzheimer’s disease taking 2000 IU/day of vitamin E experienced slower decline in their ability to carry out daily tasks 170. These results warrant further investigation.
Vitamin C (ascorbic acid) has a neuroprotective effect because it has the ability to scavenge free radicals, reduces beta-amyloid activity, and is also involved in the chelation of iron, zinc, and copper. Vitamin C (ascorbic acid) is a key antioxidant of the central nervous system 171. In a rat study, a pro-oxidative diet has been shown to increase the level of amyloid precursor protein 172. Very little is known about the effects of vitamin C supplementation alone.
Multiple meta-analyses and systematic reviews have examined the effects of vitamins C and E on cognitive functions, but the results vary depending on how the study was designed. In meta-analyses of observational research, a diet rich in vitamins C and E was linked to a 20 to 25 percent lower risk of Alzheimer’s disease 173, 174. However, results from each study vary based on the age and health status of the participants and the methods used to measure vitamin intake and track cognitive function. Some experts argue that the specific vitamins cannot be reliably separated from broader patterns of health and diet (i.e., benefit may be from a healthy diet rather than vitamins alone).
Even if the vitamins are protective, supplements are not a promising preventive measure. In two randomized controlled trials, vitamin E or vitamin E and C supplements did not help patients with mild cognitive impairment (MCI) 175, 176. Supplementation with both vitamins C and E failed to slow cognitive decline for women over age 65 177, although another observational study reported more promising results 178. It is possible that supplements are helpful but only for people who do not consume enough vitamin E or C through their diets. Nevertheless, current evidence suggests that vitamin C or E supplementation, alone or in combination, is unlikely to promote cognition or prevent cognitive decline in most people.
In a 13-year study on a group of 2533 French people aged 45 to 60, the relationship between fruit and vegetable consumption (400 g) and cognitive ability was assessed using neuropsychological tests 160. It was proved that the consumption of fruit and other products rich in vitamin C and vitamin E positively correlated with the results of verbal memory test, in contrast to the consumption of vegetables and vegetables rich in beta-carotene 160.
Another prospective, longitudinal cohort study (n = 9250) also confirmed the beneficial effect of fruit consumption on reducing the risk of Alzheimer’s disease 179.
In conclusion, research results indicate that decreased vitamin E concentration may be associated with an increased risk of Alzheimer’s disease, supplementation at higher doses (2000 IU) than lower doses (400 IU) is more effective, and increased consumption of antioxidant vitamins (E and C) may help to improve cognitive abilities 155. However, while vitamins C and E are essential for good health, excessive supplementation carries some risks. Some studies have linked vitamin E supplementation of approximately 225 IU/day to a slightly increased risk of death 180, although there is conflicting evidence 181. In men with high selenium levels, vitamin E supplementation at 400 IU/day has been reported to nearly double the risk of prostate cancer 182.
Alpha-tocopherol is the most extensively studied type of vitamin E, but recent research suggests that other vitamin E types, such as gamma-tocopherol and beta-tocotrienol, may also be important for proper health 183.
A healthy diet naturally rich in vitamins C and E is likely to offer the most benefit. Citrus fruits, sweet peppers, and Brussels sprouts are rich in vitamin C. Vitamin E is plentiful in green leafy vegetables, sunflower seeds, and almonds. Vitamin C intake by adults should be 90 mg/day for men and 75 mg/day for women 184. Because vitamin C absorption is limited to about 400 mg/day 185, higher doses are unlikely to be more beneficial. The Recommended Dietary Allowances (RDAs) for vitamin E (Alpha-Tocopherol) is 15 mg/day for men, for women, 15 mg/day 184.
Vitamin D
Vitamin D also referred to as “calciferol”, is a fat-soluble vitamin that is naturally present in a few foods, added to others, and available as a dietary supplement. Vitamin D is also produced endogenously when ultraviolet (UV) rays from sunlight strike your skin and trigger vitamin D synthesis.
Vitamin D obtained from sun exposure, foods, and supplements is biologically inert and must undergo two hydroxylations in the body for activation. The first hydroxylation, which occurs in the liver, converts vitamin D to 25-hydroxyvitamin D [25(OH)D], also known as “calcidiol.” The second hydroxylation occurs primarily in the kidney and forms the physiologically active 1,25-dihydroxyvitamin D [1,25(OH)2D], also known as “calcitriol” 186. Vitamin D is involved in various brain processes, and vitamin D receptors are present on neurons and glia in areas of the brain thought to be involved in the pathophysiology of depression 187.
There are two forms of vitamin D: vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol), that differ chemically only in their side-chain structures. While vitamin D2 (ergocalciferol) can be obtained from some plants and mushrooms, a significant percentage of vitamin D is produced in your skin as vitamin D3 (cholecalciferol) when stimulated by the sun 188. However, the skin’s ability to produce vitamin D3 (cholecalciferol) declines with age and vitamin D deficiency is more common in older adults than previously thought 189. Dietary sources of vitamin D3 include salmon, sardines, and fortified milk. Vitamin D is also a part of many multivitamins and is available separately as a dietary supplement in both liquid and pill forms. Most vitamin D supplements contain 400 IU (10 µg), either as D2 or D3. Although both D2 and D3 from supplements or diet can treat rickets (a disease caused by vitamin D deficiency), some evidence suggests that supplements with D3 are more potent than D2 190 and have better evidence for long-term health benefits 191.
People with lower vitamin D levels or low dietary intake of vitamin D appear to have a higher risk of age-related diseases, including cognitive decline, mild cognitive impairment (MCI) and dementia 192, but no clinical research has yet tested whether treatment with vitamin D can protect from this risk. Vitamin D also plays an important role in neurodegenerative processes. Vitamin D deficiency is a genetic risk factor for Alzheimer’s disease, Parkinson’s disease, multiple sclerosis, and vascular dementia 193.
While a few small studies suggest that vitamin D supplementation may improve some aspects of cognitive functions, no studies have confirmed that it can protect against dementia. In a small non-randomized clinical trial, elderly people receiving vitamin D3 supplements had better cognitive function compared to untreated people, with particular improvement in executive function 194, but the study was not controlled or designed to look at the risk of cognitive decline.
Multiple meta-analyses and systematic reviews of observational research have examined the relationship between vitamin D levels and cognitive function. A few studies have tested the effects of vitamin D treatment on cognition, but randomized controlled trials on dementia risk or cognitive decline are lacking. In randomized, double-blinded placebo-controlled study on 2044 participants, supplementation of 1000 mg of calcium carbonate with 400 IU of vitamin D3 did not improve cognitive impairment 195. Clinical trials are underway to examine the effects of vitamin D on cognitive function in older adults who have low vitamin D levels 196, memory complaints 197, mild cognitive impairment 198 and type 2 diabetes 199, as well as those in good health 200. Another trial is testing whether vitamin D can reduce the risk of cancer, heart disease, and stroke in 20,000 men and women 201, with a subgroup undergoing testing for cognitive decline and dementia 202.
Research on the benefits of vitamin D for dementia patients is very limited and has produced mixed results. In a small, six-month pilot study, Alzheimer’s disease patients who were treated with memantine plus vitamin D improved their cognitive scores, whereas those taking memantine alone or vitamin D alone remained the same 203. A larger trial testing the effects of vitamin D in combination with memantine was scheduled to be completed in 2013 204, but the results have not been published. A small randomized trial of Parkinson’s disease patients suggested that vitamin D supplementation stabilized the disease, possibly by improving strength and balance 205.
In summary, a low level of vitamin D in the serum is associated with the risk of cognitive disorders, but supplementation with a dose of 400 IU does not bring any results (elderly people over age 70 the recommended dose is 800 IU).
Vitamin D supplementation is usually safe when used as directed but it can be harmful at artificially high levels 206. While it is impossible for the human skin to produce too much vitamin D, excessive unprotected sunlight exposure can increase risks of skin cancer. Recommended daily dietary intake of vitamin D is 600 IU (15 mcg) for adults and 800 IU (20 mcg) for people over age 70 206. Supplementation up to 4000 IU is likely to be safe 207. Taking too much vitamin D can elevate blood calcium levels and cause toxicity with symptoms such as nausea, vomiting, constipation, confusion, and heart rhythm abnormalities. Excess levels can also increase the risk of bone fractures, urinary tract infections, weight loss, digestive problems, and certain types of cancer 206. People with overactive parathyroids, kidney and liver disease, or certain immune disorders should take extra caution, as should people with diabetes and hypotensive disorders. Some common drugs can change the way that your body manages vitamin D 206.
Brain healthy diet
Recently published systematic reviews and meta-analyses show the beneficial effects of various diets, including the Mediterranean diet and the “healthy diet” 155. The Mediterranean diet is characterized by high consumption of vegetables and fruits, which are exceptionally rich in water-soluble vitamins. It has been shown that the Mediterranean diet protects against the development of cognitive impairment 208, whereas a ketogenic diet may have an impact on memory functions due to its influence on neurotransmission. In a systemic review by Grammatikopoulou et al. 209, the application of ketogenic therapy (Medium Chain Triglicerydes, MCT supplementation), both long-term and interventional, improved cognitive functions.
Ketogenic diet was initially developed in the 1920s as a potential therapy for children with difficult-to-treat epilepsy, the ketogenic diet is high in fats, very low in carbs, with moderate protein 210. Usually, carbohydrates are your brain’s primary energy source but ketone molecules generated from fats are also a potential source of fuel. The brains of patients with Alzheimer’s disease start to lose the ability to use carbohydrates but may still be able to use ketones. When Alzheimer’s disease mouse models are given a ketogenic diet, they may perform better on some cognitive tasks, even though their brains don’t have lower levels of amyloid beta or tau, the misfolded proteins common in Alzheimer’s disease patients. Although no study has tested the effect of the ketogenic diet in Alzheimer’s patients, one small study suggested that overweight elderly individuals with age-related memory decline performed better on memory tasks after six weeks on a low carbohydrate diet 211.
The ketogenic diet is not without its own concerns. The most common and relatively minor short-term side effects of ketogenic diet include a collection of symptoms like nausea, vomiting, headache, fatigue, dizziness, insomnia, difficulty in exercise tolerance, and constipation, sometimes referred to as ‘keto flu’ 210. These symptoms resolve in a few days to few weeks. Ensuring adequate fluid and electrolyte intake can help counter some of these symptoms. Long-term adverse effects include hepatic steatosis, hypoproteinemia, kidney stones, and vitamin and mineral deficiencies. Furtermore, if you eat few carbohydrates, you may miss out on important nutrients found in carbohydrate-rich foods such as fruits and vegetables 212. This is especially concerning in elderly individuals, particularly Alzheimer’s patients, who may be at greater risk for anorexia and frailty. In addition, low-carb diets may also increase your risk of high cholesterol, kidney problems, and osteoporosis 213.
The ketogenic diet is contraindicated in patients with pancreatitis, liver failure, disorders of fat metabolism, primary carnitine deficiency, carnitine palmitoyltransferase deficiency, carnitine translocase deficiency, porphyrias, or pyruvate kinase deficiency 210. People on a ketogenic diet rarely can have a false positive breath alcohol test. Due to ketonemia, acetone in the body can sometimes be reduced to isopropanol by hepatic alcohol dehydrogenase which can give a false positive alcohol breath test result.
The effect of “healthy diets” on cognition has also been studied. It has been reported that healthy eating patterns reduce the risk of dementia, while a high-fat diet and diets with a high glycemic index increase neuronal damage 214. Healthy diet is not about ‘dieting’. Healthy diet is about making smart choices and having a balance of different foods and nutrients in your diet for good health and wellbeing. Healthy diet is about enjoying your food, at the same time as being mindful about what you eat. A healthy diet can help reduce your risk of heart disease, stroke and lots of other things you’d rather avoid. The good news is, healthy eating right doesn’t have to be hard, boring or require you to give up all of the foods you love. Proinflammatory diet also may increase the progression of dementia 215.
It has also been proven that the use of nutritional formulas, fatty acids, ginseng, inositol, probiotics, and products rich in flavonoids may delay the progression of dementia 216. On the other hand, according to Heider et al.’s 217 systematic review and meta-analyses, supplementation of vitamin B, E, omega-3, and nutritional formulas does not improve cognitive function.
There are four main food groups in healthy eating. These are:
- Carbohydrates
- Fruit and Vegetables
- High Protein Foods
- Dairy (& alternatives)
The American Heart Association suggests these daily amounts:
- Vegetables – canned, dried, fresh and frozen vegetables; 5 servings
- Fruits – canned, dried, fresh and frozen fruits; 4 servings
- Whole grains – barley, brown rice, millet, oatmeal, popcorn and whole wheat bread, crackers and pasta; 3-6 servings
- Dairy – low fat (1%) and fat-free dairy products; 3 servings
- Proteins – eggs, fish, lean meat, legumes, nuts, poultry and seeds; 1-2 servings. Eat a variety of fish at least twice a week, especially fish containing omega-3 fatty acids (for example, salmon, trout and herring).
- Oils – polyunsaturated and monounsaturated canola, olive, peanut, safflower and sesame oil; 3 tablespoons
- Limit – sugary drinks, sweets, fatty meats, and salty or highly processed foods
- Choose foods with less salt (sodium) and prepare foods with little or no salt. To lower blood pressure, aim to eat no more than 2,300 milligrams of sodium per day. Reducing daily intake to 1,500 mg is desirable because it can lower blood pressure even further.
- Limit saturated fat and trans fat and replace them with the better fats, monounsaturated and polyunsaturated. If you need to lower your blood cholesterol, reduce saturated fat to no more than 5 to 6 percent of total calories. For someone eating 2,000 calories a day, that’s about 13 grams of saturated fat.
- Avoid – partially hydrogenated oils, tropical oils, and excessive calories
- Replace – highly processed foods with homemade or less-processed options
- If you drink alcohol, drink in moderation. That means no more than one drink per day if you’re a woman and no more than two drinks per day if you’re a man.
Carbohydrate
Carbohydrate (starch) is the body’s main energy (fuel) source. Starch is broken down to produce glucose which is used by your body for energy.
Starchy foods are an important part of the healthy diet. They should make up about a third of all the food that you eat. You don’t have to avoid or restrict them because they are ‘fattening’. Instead, be aware of the total amount of starch that you eat. Cutting out one food group, such as carbohydrate can cause dietary imbalance. Starchy foods include bread, potatoes, rice and pasta. Wholegrain options are healthier choices.
Fiber rich foods help your gut to function properly and have many other health benefits. Studies have shown that people who are overweight or obese tend to lose weight if they include plenty of high fiber, starchy carbohydrate in their diets.
Sugar
Sugar is a type of carbohydrate. Like starch, it breaks down into glucose, to provide energy for your body. ‘Free’ sugars are often added to foods during manufacture and include refined sugars such as sucrose (table sugar). This kind of sugar is also found naturally, in unsweetened fruit juices, and in syrups and honey.
Excess consumption of free sugars is linked to the risk of obesity, type 2 diabetes and tooth decay. Many of the free sugars that you consume, are in sugary drinks. A regular can of cola for instance, can contain the equivalent of seven teaspoons of sugar (35g). The guidance about free sugar consumption suggests a daily limit of 30g. This is equivalent to six teaspoons.
The natural sugars found in milk and in whole fruits and vegetables are not free sugars and do not need to be restricted in the same way.
Fruit and vegetables
Fruit and vegetables contain high levels of ‘micronutrients’. These include vitamins, minerals and antioxidants. Micronutrients are essential to the body’s many biochemical processes.
Fruit and vegetables are often high in fiber. They are generally low in calorie and they taste good. The current Dietary Guidelines for Americans recommends at least five portions of different fruit and vegetable per day 218. Like carbohydrate, fruit and vegetable should account for about one third of what you eat, per day. Dried, frozen, tinned, as well as fresh, fruit and veg are all included. One portion of pulses (baked beans, lentils, dried peas) can also count towards your five a day.
Dietary fiber
Fiber comes from plant-based foods, including fruits, vegetables and wholegrains. Dietary fiber is the part of plants that you eat but which doesn’t get digested in your small intestine. Instead, it is completely or partially broken down (fermented) by bacteria in your large intestine. Once broken down in your large intestine, it has been suggested that dietary fibers increase the beneficial bacteria in your gut. This improves your immune system. Fibre includes carbohydrates called polysaccharides and resistant oligosaccharides. Recent research suggests that fiber should be categorized by its physical characteristics; how well it dissolves (solubility), how thick it is (viscosity) and how well it breaks down (fermentability). Some commonly known terms are described below:
- Soluble fiber including pectins and beta glucans is found in foods like fruit and oats.
- Insoluble fiber including cellulose is found in wheat bran and nuts.
- Resistant starch is a soluble fiber that is highly fermentable in the gut. It gets broken down by good bacteria to produce short chain fatty acids (SCFAs). RS is naturally present in some foods such as bananas, potatoes, grains and pulses.
- Prebiotics are types of carbohydrate that only our gut bacteria can feed upon. Some examples are onions, garlic, asparagus and banana
Fibre is essential for your gut to work normally. It increases good bacteria which supports your immunity against inflammatory disorders and allergies. A high fiber diet seems to reduce the risk of chronic diseases such as heart disease, type 2 diabetes and bowel cancer.
Eating a range of dietary fiber can:
- Improve the diversity of your microbiota
- Improve constipation and lactose intolerance
- Enhance immunity
- Reduce inflammation in your gut
For example, high quality randomized controlled trials have shown that eating oat bran leads to lower blood pressure and lower total cholesterol.
Good sources of dietary fiber include:
- Pulses (like lentils and peas) and beans and legumes (think navy beans, small white beans, split peas, chickpeas, lentils, pinto beans)
- Fruits and vegetables, especially those with edible skin (like pears and apples) and those with edible seeds (like berries)
- Nuts—try different kinds (pumpkin seeds, almonds, sunflower seeds, pistachios and peanuts are a good source of fiber and healthy fats, but be mindful of portion sizes, because they also contain a lot of calories in a small amount!)
- Whole grains such as:
- Quinoa, barley, bulgur, oats, brown rice and farro
- Whole wheat pasta
- Whole grain cereals, including those made from whole wheat, wheat bran and oats
Choose fiber rich foods from a variety of sources including wholegrains, fruit and vegetable, nuts and seeds, beans and pulses. When you read food labels check for the grams of fiber per serving or per 100g. Foods that are naturally high in fiber and contain at least 3 grams per 100 gram are often labeled as a “good source,” and foods labeled as “excellent source” contain more than 5 grams of fiber per serving.
You may wish to see a dietitian if you:
- are unsure about how much and/or what types of fiber you currently have in your diet
- suffer with constipation or diarrhoea (e.g. irritable bowel syndrome (IBS))
- have a condition which can restrict your fiber intake (e.g. inflammatory bowel disease)
Keep in mind that if you haven’t been eating a lot of foods high in fiber on a daily basis, it’s important to increase your intake slowly to allow your body to adjust. A sudden increase in eating foods high in fiber (especially foods with added fiber or when using supplements) can cause gas, bloating or constipation. Be sure you are drinking enough water too, because fiber needs water to move through your body.
Protein
Protein is vital. It is your body’s main building block. Animal products such as meat, fish, eggs and dairy are good sources of dietary protein. Meat and fish also provide your body with a form of iron (heme), which is easy to absorb. Fish also contains essential fatty acids (e.g, Omega-3).
Protein also comes from foods of plant origin. Pulses, nuts, and seeds are all high in protein. Pulses are a very good meat alternative, whether or not you are vegetarian or vegan.
Cutting back on consumption of red meat (beef, lamb, goat, pork) especially, is better for your health and for the environment: current advice is to have no more than 300g of red meat per week. Try to avoid processed meats such as bacon, salami, hot dogs, ham. Consumption of these cured meat products has been linked to a much higher risk of certain gut cancers.
Dairy
Dairy products and calcium-fortified alternatives are your body’s main source of calcium, which is necessary for the growth, development and maintenance of healthy bones and teeth. Dairy products and alternatives are also a source of protein. Milk, cheese, cream and milk-based sauces and yogurts can have a high saturated fat content. Fat reduced options are recommended, and small quantities.
Fats
Fats also known as lipids, is an essential nutrient (a primary storage form of energy, a kilojoule-dense nutrient) your body need for energy and to help your gut absorb vitamins A, D, E and K from foods. Fat has twice as many calories as proteins or carbohydrates. There are nine calories (37kJ) in every gram of fat, regardless of what type of fat it is. Fats are more energy-dense than carbohydrates and proteins, which provide four calories (17kJ) per gram. Dietary fat also plays a major role in your cholesterol levels. You need some fat in your diet but not too much. There are different types of fats, some are “good” and some are “bad”, however, you should try to avoid “bad” fats. When it comes to dietary fat, what matters most is the type of fat you eat. Contrary to past dietary advice promoting low-fat diets, newer research shows that healthy fats are necessary and beneficial for health.
Healthy fats are unsaturated. They keep cholesterol levels within a healthy range, reduce your risk of heart problems and may be good for the skin, eyes and brain. Unsaturated fats are the best choice for a healthy diet.
Unhealthy fats are saturated and trans fats, which can raise levels of ‘bad’ cholesterol and increase the risk of heart disease. Multiple studies have linked high levels of saturated fat with cognitive decline. A diet that is higher in unsaturated fats and lower in saturated fats is linked to better cognition.
- Saturated fats such as butter, solid shortening, and lard. Eating foods that contain saturated fats raises the level of cholesterol in your blood. High levels of LDL cholesterol (low-density lipoprotein or “bad” cholesterol) in your blood increase your risk of heart disease and stroke. The American Heart Association recommends aiming for a dietary pattern that achieves 5% to 6% of calories from saturated fat. For example, if you need about 2,000 calories a day, no more than 120 of them should come from saturated fat. That’s about 13 grams of saturated fat per day 219.
- Trans fats also known as trans fatty acids or “partially hydrogenated oils”. These are found in vegetable shortenings, some margarines, crackers, cookies, snack foods, and other foods made with or fried in partially hydrogenated oils. By 2018, most U.S. companies will not be allowed to add partially hydrogenated oils to food.
“Bad” fats, such as artificial trans fats and saturated fats, are guilty of the unhealthy things all fats have been blamed for—weight gain, clogged arteries, an increased risk of certain diseases, and so forth. Large studies have found that replacing saturated fats in your diet with unsaturated fats and omega-3 fatty acids can reduce your risk of heart disease by about the same amount as cholesterol-lowering drugs. Since fat is an important part of a healthy diet, rather than adopting a low-fat diet, it’s more important to focus on eating more beneficial “good” fats and limiting harmful “bad” fats. For good health, the majority of the fats that you eat should be monounsaturated or polyunsaturated. Eat foods containing monounsaturated fats and/or polyunsaturated fats such as canola oil, olive oil, safflower oil, sesame oil or sunflower oil instead of foods that contain saturated fats and/or trans fats.
For years you’ve been told that eating fat will add inches to your waistline, raise cholesterol, and cause a myriad of health problems. When food manufacturers reduce fat, they often replace it with carbohydrates from sugar, refined grains, or other starches. Your body digests these refined carbohydrates and starches very quickly, affecting your blood sugar and insulin levels and possibly resulting in weight gain and disease 220. But now scientists know that not all fat is the same. Research has shown that unsaturated fats are good for you. Healthy fats play a huge role in helping you manage your moods, stay on top of your mental game, fight fatigue, and even control your weight. These fats come mostly from plant sources. Cooking oils that are liquid at room temperature, such as canola, peanut, safflower, soybean, and olive oil, contain mostly unsaturated fat. Nuts, seeds, and avocados are also good sources. Fatty fish—such as salmon, sardines, and herring—are rich in unsaturated fats, too. You should actively make unsaturated fats a part of your diet. Of course, eating too much fat will put on the pounds too. Note also that by swapping animal fats for refined carbohydrates—such as replacing your breakfast bacon with a bagel or pastry—won’t have the same benefits. In fact eating refined carbohydrates or sugary foods can have a similar negative effect on your cholesterol levels, your risk for heart disease, and your weight. Limiting your intake of saturated fat can still help improve your health—as long as you take care to replace it with good fat rather than refined carbs. In other words, don’t go no fat, go good fat.
Healthy-eating tips:
- Use olive oil in cooking.
- Replace saturated fats with unsaturated fats; for example, use avocado, tahini, nut or seed butter instead of dairy butter.
- Eat fish, especially oily fish, twice a week.
- Consume legume- or bean-based meals twice a week.
- Snack on nuts or add them to your cooking.
- Throw avocado in salads.
- Choose lean meats and trim any fat you can see (including chicken skin).
- Use table spreads that have less than 0.1g of trans fats per 100g.
Saturated fats
Saturated fats are fat molecules that are “saturated” with hydrogen molecules (see Figure 1 above). Saturated fats are normally solid at room temperature. Saturated fats occur naturally in many foods — primarily meat and dairy foods (butter, cream, full-fat milk and cheese). Beef, lamb, pork on poultry (with the skin on) contain saturated fats, as do butter, cream and cheese made from whole or 2% milk. Plant-based foods that contain saturated fats include coconut, coconut oil, coconut milk and coconut cream, cooking margarine, and cocoa butter, as well as palm oil and palm kernel oil (often called tropical oils). Saturated fats are also found in snacks like chips, cakes, biscuits and pastries, and takeaway foods. Consuming more than the recommended amount of saturated fat is linked to heart disease and high cholesterol.
The American Dietary Guidelines recommend that:
- men should not eat more than 30g of saturated fat a day
- women should not eat more than 20g of saturated fat a day
- children should have less
For people who need to lower their cholesterol, the American Heart Association recommends reducing saturated fat to less than 6% of total daily calories. For someone eating 2,000 calories a day, that’s about 11 to 13 grams of saturated fat 219.
Examples of foods with saturated fat are:
- fatty beef,
- lamb,
- pork,
- poultry with skin,
- beef fat (tallow),
- meat products including sausages and pies,
- lard and cream,
- butter and ghee,
- cheese especially hard cheese like cheddar,
- other dairy products made from whole or reduced-fat (2 percent) milk,
- cream, soured cream and ice cream,
- some savory snacks, like cheese crackers and some popcorns,
- chocolate confectionery,
- biscuits, cakes, and pastries
In addition, many baked goods and fried foods can contain high levels of saturated fats. Some plant-based oils, such as palm oil, palm kernel oil, coconut oil and coconut cream, also contain primarily saturated fats, but do not contain cholesterol.
Unsaturated Fats
If you want to reduce your risk of heart disease, it’s best to reduce your overall fat intake and swap saturated fats for unsaturated fats. Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean, corn, safflower, canola, olive and sunflower, also contain unsaturated fats.
There are 2 types of unsaturated fats: monounsaturated and polyunsaturated. Unsaturated fats help reduce your risk of heart disease and lower your cholesterol levels.
- Polyunsaturated fats such as omega-3 and omega-6 fats are found in fish, nuts, and safflower and soybean oil.
- Monounsaturated fats are found in olive and canola oil, avocado, cashews and almonds.
Monounsaturated fats have one (“mono”) unsaturated carbon bond in the molecule. Polyunsaturated fats have more than one (“poly,” for many) unsaturated carbon bonds. Both of these unsaturated fats are typically liquid at room temperature.
Eaten in moderation, both kinds of unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats.
Polyunsaturated fats
Polyunsaturated fats are simply fat molecules that have more than one unsaturated carbon bond in the molecule, this is also called a double bond. Oils that contain polyunsaturated fats are typically liquid at room temperature but start to turn solid when chilled. Olive oil is an example of a type of oil that contains polyunsaturated fats.
There are 2 main types of polyunsaturated fats: omega-3 and omega-6. Oils rich in polyunsaturated fats also provide essential fats that your body needs but can’t produce itself – such as omega-6 and omega-3 fatty acids. You must get essential fats through food. Omega-6 and omega-3 fatty acids are important for many functions in the body. A deficiency of essential fatty acids—either omega-3s or omega-6s—can cause rough, scaly skin and dermatitis 221.
Polyunsaturated fats can help reduce bad cholesterol levels in your blood which can lower your risk of heart disease and stroke. Polyunsaturated fats also provide nutrients to help develop and maintain your body’s cells. Oils rich in polyunsaturated fats also contribute vitamin E to the diet, an antioxidant vitamin most Americans need more of.
Foods high in polyunsaturated fat include a number of plant-based oils, including:
- soybean oil
- corn oil
- sunflower oil
Other sources include some nuts and seeds such as walnuts and sunflower seeds, tofu and soybeans.
Omega-6 fats are found in vegetable oils, such as:
- rapeseed
- corn
- sunflower
- some nuts
Omega-3 fats are found in oily fish, such as:
- kippers
- herring
- trout
- sardines
- salmon
- mackerel
The American Heart Association also recommends eating tofu and other forms of soybeans, canola, walnut and flaxseed, and their oils. These foods contain alpha-linolenic acid (ALA), another omega-3 fatty acid.
Polyunsaturated fats (PUFAs) are frequently designated by their number of carbon atoms and double bonds. Alpha-linolenic acid (ALA), for example, is known as C18:3n-3 because it has 18 carbons and 3 double bonds and is an omega-3 fatty acid. Similarly, eicosapentaenoic acid (EPA) is known as C20:5n-3 and docosahexaenoic acid (DHA) as C22:6n-3. Omega-6 fatty acids (omega-6s) have a carbon–carbon double bond that is six carbons away from the methyl end of the fatty acid chain. Linoleic acid (LA) known as C18:2n-6 and arachidonic acid (AA) known as C20:4n-6 are two of the major omega-6s.
The human body can only form carbon–carbon double bonds after the 9th carbon from the methyl end of a fatty acid 222. Therefore, alpha-linolenic acid (ALA) and linoleic acid (LA) are considered essential fatty acids, meaning that they must be obtained from the diet 223. Alpha-linolenic acid (ALA) can be converted into eicosapentaenoic acid (EPA) and then to docosahexaenoic acid (DHA), but the conversion (which occurs primarily in the liver) is very limited, with reported rates of less than 15% 224. Therefore, consuming EPA and DHA directly from foods and/or dietary supplements is the only practical way to increase levels of these fatty acids in the body.
Alpha-linolenic acid (ALA) is present in plant oils, such as flaxseed, soybean, and canola oils 224. Docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) are present in fish, fish oils, and krill oils, but they are originally synthesized by microalgae, not by the fish. When fish consume phytoplankton that consumed microalgae, they accumulate the omega-3s in their tissues 224.
Some researchers propose that the relative intakes of omega-6s and omega-3s—the omega-6/omega-3 ratio—may have important implications for the pathogenesis of many chronic diseases, such as cardiovascular disease and cancer 225, but the optimal ratio—if any—has not been defined 226. Others have concluded that such ratios are too non-specific and are insensitive to individual fatty acid levels 227. Most agree that raising eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) blood levels is far more important than lowering linoleic acid (LA) or arachidonic acid levels.
Currently, most clinicians do not assess omega-3 status, but it can be done by measuring individual omega-3s in plasma or serum phospholipids and expressing them as the percentage of total phospholipid fatty acids by weight 228. Experts have not established normal ranges, but mean values for serum or plasma phospholipid eicosapentaenoic acid (EPA) plus docosahexaenoic acid (DHA) among U.S. adults not taking omega-3 supplements are about 3%–4% 228. Plasma and serum fatty acid values, however, can vary substantially based on an individual’s most recent meal, so they do not reflect long-term dietary consumption 229.
It is also possible to assess omega-3 status via analysis of erythrocyte fatty acids, a measurement that reflects longer-term intakes over approximately the previous 120 days 230. The “omega-3 index” proposed by Harris and von Schacky reflects the content of eicosapentaenoic acid (EPA) plus docosahexaenoic acid (DHA) in erythrocyte membranes expressed as a percentage of total erythrocyte fatty acids 231. This index can be used as a surrogate for assessing tissue levels of eicosapentaenoic acid (EPA) plus docosahexaenoic acid (DHA) 232. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) typically comprise about 3%–5% of erythrocyte fatty acids in Western populations with low fish intakes. In Japan, where fish consumption is high, erythrocyte eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) levels are about twice those of Western populations 224.
Table 2. Alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) content of selected foods
| Food | Grams per serving | ||
| ALA | DHA | EPA | |
| Flaxseed oil, 1 tbsp | 7.26 | ||
| Chia seeds, 1 ounce | 5.06 | ||
| English walnuts, 1 ounce | 2.57 | ||
| Flaxseed, whole, 1 tbsp | 2.35 | ||
| Salmon, Atlantic, farmed cooked, 3 ounces | 1.24 | 0.59 | |
| Salmon, Atlantic, wild, cooked, 3 ounces | 1.22 | 0.35 | |
| Herring, Atlantic, cooked, 3 ounces* | 0.94 | 0.77 | |
| Canola oil, 1 tbsp | 1.28 | ||
| Sardines, canned in tomato sauce, drained, 3 ounces* | 0.74 | 0.45 | |
| Mackerel, Atlantic, cooked, 3 ounces* | 0.59 | 0.43 | |
| Salmon, pink, canned, drained, 3 ounces* | 0.04 | 0.63 | 0.28 |
| Soybean oil, 1 tbsp | 0.92 | ||
| Trout, rainbow, wild, cooked, 3 ounces | 0.44 | 0.4 | |
| Black walnuts, 1 ounce | 0.76 | ||
| Mayonnaise, 1 tbsp | 0.74 | ||
| Oysters, eastern, wild, cooked, 3 ounces | 0.14 | 0.23 | 0.3 |
| Sea bass, cooked, 3 ounces* | 0.47 | 0.18 | |
| Edamame, frozen, prepared, ½ cup | 0.28 | ||
| Shrimp, cooked, 3 ounces* | 0.12 | 0.12 | |
| Refried beans, canned, vegetarian, ½ cup | 0.21 | ||
| Lobster, cooked, 3 ounces* | 0.04 | 0.07 | 0.1 |
| Tuna, light, canned in water, drained, 3 ounces* | 0.17 | 0.02 | |
| Tilapia, cooked, 3 ounces* | 0.04 | 0.11 | |
| Scallops, cooked, 3 ounces* | 0.09 | 0.06 | |
| Cod, Pacific, cooked, 3 ounces* | 0.1 | 0.04 | |
| Tuna, yellowfin, cooked 3 ounces* | 0.09 | 0.01 | |
| Kidney beans, canned ½ cup | 0.1 | ||
| Baked beans, canned, vegetarian, ½ cup | 0.07 | ||
| Ground beef, 85% lean, cooked, 3 ounces** | 0.04 | ||
| Bread, whole wheat, 1 slice | 0.04 | ||
| Egg, cooked, 1 egg | 0.03 | ||
| Chicken, breast, roasted, 3 ounces | 0.02 | 0.01 | |
| Milk, low-fat (1%), 1 cup | 0.01 | ||
Footnotes: *Except as noted, the U.S. Department of Agriculture (USDA) database does not specify whether fish are farmed or wild caught. **The USDA database does not specify whether beef is grass fed or grain fed.
Essential Fatty Acids
Essential Fatty Acids such as omega-3 oils are ‘essential’ because your body can’t make them and you have to obtain them from your food. Essential Fatty Acids are found in the skin of white fish but also in the flesh of oily fish such as fresh and tinned salmon, mackerel, sardines and fresh tuna. Advice for fish eaters is to have one portion of oily fish, and one portion of white fish per week.
Essential Fatty Acids can also be found in some plant oils such as flaxseed, rapeseed and soya but there is not as much in these oils as there is in fish and seafood.
Omega-3 fatty acids
Omega-3 fatty acids (omega-3s) are a type of polyunsaturated fat and have a carbon–carbon double bond located three carbons from the methyl end of the chain (see Figure 6). Omega-3 fatty acids, sometimes referred to as “n-3s,” are present in certain foods such as flaxseed and fish, as well as dietary supplements such as fish oil. Omega-3 fatty acids are especially beneficial to your health. Omega-3s play important roles in the body as components of the phospholipids that form the structures of cell membranes 221. There are different types of omega-3s: eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are found in fish and algae and have the most health benefits, while alpha-linolenic acid (ALA) comes from plants and is a less potent form of omega-3, although the body does convert ALA to EPA and DHA at low rates. Alpha-linolenic acid (ALA) contains 18 carbon atoms, whereas eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) are considered “long-chain” omega-3s because EPA contains 20 carbons and DHA contains 22 232.
Docosahexaenoic acid (DHA), in particular, is especially high in the retina, brain, and sperm 224. In addition to their structural role in cell membranes, omega-3s (along with omega-6s) provide energy for the body and are used to form eicosanoids. Eicosanoids are signaling molecules that have similar chemical structures to the fatty acids from which they are derived; they have wide-ranging functions in the body’s cardiovascular, pulmonary, immune, and endocrine systems 222. Higher concentrations of EPA and DHA than arachidonic acid tip the eicosanoid balance toward less inflammatory activity 233.
Research has shown that a diet rich in omega-3 fatty acids may help to:
- Prevent and reduce symptoms of depression, ADHD, and bipolar disorder.
- Protect against memory loss and dementia.
- Reduce the risk of heart disease, stroke, and cancer.
- Ease arthritis, joint pain, and inflammatory skin conditions.
- Support a healthy pregnancy.
- Battle fatigue, sharpen your memory, and balance your mood.
Fish the best source of omega-3 (high in EPA and DHA):
- Anchovies
- Herring
- Salmon
- Mackerel
- Sardines
- Trout
- Tuna
- Mussels
- Oysters
- Halibut
Vegetarian sources of omega-3s (high in ALA):
- Algae such as seaweed (high in EPA and DHA)
- Eggs (small amounts of DHA)
- Flaxseeds and flaxseed oil
- Chia seeds
- Canola and soybean oil
- Walnuts
- Mayonnaise
- Edamame
- Beans (refried, kidney, etc.)
- Brussels sprouts
- Kale
- Spinach
Fish is a good source of protein and omega-3 fatty acids, which are good for your heart. Research has shown that omega-3 fatty acids can reduce your risk of heart disease and stroke. A 2020 Cochrane review 234 of 86 randomized controlled trials published between 1968 and 2019 found that 0.5 g/day to more than 5 g/day omega-3 fatty acids for 12 to 88 months in a total of 162,796 participants reduced serum triglyceride levels by about 15% and slightly decreased rates of cardiovascular mortality and coronary heart disease events. However, the omega-3 fatty acids supplements did not affect all-cause mortality, cardiovascular events, stroke, or arrhythmia. The authors of several earlier meta-analyses and systematic reviews, as well as a 2016 report from the Agency for Healthcare Research and Quality, concluded that omega-3 fatty acids supplements do not appear to significantly reduce the risk of most cardiovascular events 235. Many of these analyses 236, however, but not all 237, did find that omega-3s reduce the risk of cardiac death.
The American Heart Association recommends eating 2 servings of fish (particularly fatty fish) per week. A serving is 3.5 ounce (100 g) cooked, or about ¾ cup of flaked fish. Fatty fish like salmon, mackerel, herring, lake trout, sardines and albacore tuna are high in omega-3 fatty acids. For people with existing coronary heart disease, such as a recent heart attack (myocardial infarction), the American Heart Association recommends approximately 1 gram/day EPA plus DHA, preferably from oily fish; however, supplements could also be considered under the direction of a physician 238. The American Heart Association does not recommend omega-3 supplements for people who do not have a high cardiovascular disease risk.
While omega-3s are best obtained through food, there are many omega-3 and fish oil supplements available. A typical fish oil supplement provides about 1,000 mg fish oil, containing 180 mg EPA and 120 mg DHA, but doses vary widely 239. If you need to substantially lower your triglycerides, your doctor may recommend prescription fish oil, which has been concentrated to contain about 900 mg of EPA plus DHA per capsule. Cod liver oil supplements provide vitamin A and vitamin D in addition to omega-3s. For strict vegetarians or vegans, as well as obtaining ALA from food sources, look for capsules containing DHA and EPA extracted from algae, the original source of omega-3s for fish. Although seafood contains varying levels of methyl mercury (a toxic heavy metal) 240, omega-3 supplements have not been found to contain this contaminant because it is removed during processing and purification 241.
Some types of fish may contain high levels of mercury, PCBs (polychlorinated biphenyls), dioxins and other environmental contaminants. Levels of these substances are generally highest in older, larger, predatory fish and marine mammals.
The benefits and risks of eating fish vary depending on a person’s stage of life.
Children and pregnant women are advised by the U.S. Food and Drug Administration (FDA) to:
- Avoid eating those fish with the potential for the highest level of mercury contamination (such as shark, swordfish, king mackerel or tilefish).
- Eat a variety of fish and shellfish that are lower in mercury (such as canned light tuna, salmon, pollock, catfish).
- Check local advisories about the safety of fish caught by family and friends in local lakes, rivers and coastal areas.
For middle-aged and older men and postmenopausal women, the benefits far outweigh the potential risks when the amount of fish eaten is within the recommendations established by the FDA and Environmental Protection Agency.
Eating a variety of fish will help minimize any potentially adverse effects due to environmental pollutants. Five of the most commonly eaten fish or shellfish that are low in mercury are shrimp, canned light tuna, salmon, pollock, and catfish. Avoid eating shark, swordfish, king Mackerel, or tilefish because they contain high levels of mercury.
Cholesterol
Dietary fat plays a major role in your cholesterol levels. Cholesterol is a type of fat, a wax-like substance that your body needs to function properly that comes from foods such as eggs and is also found in your blood mostly made by your body in your liver. In and of itself, cholesterol isn’t bad. But when you get too much of it, it can have a negative impact on your health. The 2 main types of cholesterol are:
- “Good” cholesterol or HDL (high-density lipoprotein) cholesterol. “Good” HDL cholesterol has a positive effect by taking cholesterol from parts of the body where there’s too much of it to the liver, where it’s disposed of.
- “Bad” cholesterol or LDL (low-density lipoprotein) cholesterol.
High levels of LDL cholesterol (low-density lipoprotein or “bad” cholesterol) can increase your risk of heart disease. The key is to keep your LDL levels low and HDL high, which may protect against heart disease and stroke. High levels of LDL cholesterol (low-density lipoprotein or “bad” cholesterol) can clog arteries and low HDL (high-density lipoprotein or “good” cholesterol) can be a marker for increased cardiovascular risk. However, eating foods that contain any type of cholesterol won’t actually raise your body’s cholesterol levels. Rather than the amount of cholesterol you eat, the biggest influence on your cholesterol levels is the type of fats you consume. Eating saturated or trans fats is far more likely to give you high cholesterol. So instead of counting cholesterol, it’s important to focus on replacing bad fats with good fats.
LDL (bad) cholesterol
LDL (low-density lipoprotein) cholesterol is considered the “bad” cholesterol, because it contributes to fatty buildups in arteries (atherosclerosis). This narrows the arteries and increases the risk for heart attack, stroke and peripheral artery disease. Your body naturally produces all the LDL cholesterol you need. Eating foods containing saturated fats and trans fats causes your body to produce even more LDL — raising the level of “bad” cholesterol in your blood.
HDL (good) cholesterol
HDL (high-density lipoprotein) cholesterol can be thought of as the “good” cholesterol because a healthy level may protect against heart attack and stroke. HDL carries LDL (bad) cholesterol away from the arteries and back to the liver, where the LDL is broken down and passed from the body. But HDL cholesterol doesn’t completely eliminate LDL cholesterol. Only one-third to one-fourth of blood cholesterol is carried by HDL.
Trans fats
Avoid trans fat. Trans fats also known as trans fatty acids or “partially hydrogenated oils”, are created in an industrial process that adds hydrogen to liquid vegetable oils to make them more solid, so they ‘behave’ like a saturated fat. There are two broad types of trans fats found in foods: naturally-occurring and artificial trans fats. Naturally-occurring trans fats are produced in the gut of some animals and foods made from these animals (e.g., milk and meat products) may contain small quantities of these fats. Artificial trans fats (or trans fatty acids) are created in an industrial process that adds hydrogen to liquid vegetable oils to make them more solid.
Trans fats increase the levels of ‘bad’ LDL cholesterol and decreases the levels of ‘good’ HDL cholesterol in your body, which increases your risk of developing heart disease and stroke. Trans fats is also associated with a higher risk of developing type 2 diabetes. Trans fats can be found in many foods such as in butter, margarine (in small amounts), deep-fried and processed foods like doughnuts, cakes and pastries. Baked goods, such as pastries, pizza dough, frozen pizza, pie crust, cookies, biscuits, and crackers also can contain trans fats.
Since 2006, the FDA has required trans fat content to be listed on the Nutrition Facts panel of packaged foods. In recent years, many major national fast-food chains and casual-dining restaurant chains have announced they will no longer use trans fats to fry or deep-fry foods.
The American Heart Association recommends that adults who would benefit from lowering LDL cholesterol eliminate trans fat from their diet.
To find the amount of trans fats in a particular packaged food, look at the Nutrition Facts panel. Companies must list any measurable amount of trans fat (0.5 grams or more per serving) in a separate line in the “Total Fat” section of the panel, directly beneath the line for “Saturated Fat.” This means if a food package states 0 grams of trans fats, it might still have some trans fats if the amount per serving is less than 0.5 g. You can also spot trans fats by reading ingredient lists and looking for the ingredients referred to as “partially hydrogenated oils.”
Salt
Salt or sodium is a mineral that’s essential for life. Table salt is a combination of two minerals — about 40% sodium and 60% chloride. Salt or sodium is regulated by your kidneys, and it helps control your body’s fluid balance. It also helps send nerve impulses and affects muscle function. High levels of salt in your diet can increase blood pressure. High blood pressure is known as the “silent killer” because its symptoms are not always obvious. It’s one of the major risk factors for heart disease, the No. 1 killer worldwide. Ninety percent of American adults are expected to develop high blood pressure over their lifetimes. Because high blood pressure is an important risk factor for stroke, and strokes are detrimental to cognitive health, excessive salt intake is harmful for your brain health. There is a well-established relationship between consuming high levels of sodium and risk of stroke. In Japan, a public health education intervention in the 1960s showed the effectiveness of dietary interventions to reduce sodium intake. A 50% reduction in salt in the diet was associated with an 85% reduction in mortality caused by stroke.
Most of the salt that you eat is added to processed foods. More than 70% of the sodium you consume comes from packaged, prepared and restaurant foods. The rest of the sodium in the diet occurs naturally in food (about 15 percent) or is added when we’re cooking food or sitting down to eat (about 11 percent). Current recommendations from the Dietary Guidelines for Americans are to limit sodium intake to 2,300 milligrams (mg) a day, which amounts to about one teaspoon of salt. The American Heart Association recommends an ideal limit of no more than 1,500 mg per day for most adults. On average, Americans eat more than 3,400 milligrams of sodium each day — much more than the American Heart Association and other health organizations recommend. Because the average American eats so much excess sodium, even cutting back by 1,000 milligrams a day can significantly improve blood pressure and heart health. One estimate suggested that if the U.S. population dropped its sodium intake to 1,500 mg/day (1/2 teaspoon salt), overall blood pressure could decrease by 25.6%, with an estimated $26.2 billion in health care savings. Another estimate projected that achieving this goal would reduce cardiovascular disease deaths by anywhere from 500,000 to nearly 1.2 million over the next decade.
Here are the approximate amounts of sodium in a given amount of salt:
- 1/4 teaspoon salt = 575 mg sodium
- 1/2 teaspoon salt = 1,150 mg sodium
- 3/4 teaspoon salt = 1,725 mg sodium
- 1 teaspoon salt = 2,300 mg sodium
The body needs only a small amount of sodium (less than 500 milligrams per day) to function properly. That’s a mere smidgen — the amount in less than ¼ teaspoon. Very few people come close to eating less than that amount. Plus, healthy kidneys are great at retaining the sodium that your body needs.
Vitamins and minerals
An optimal diet generally provides all the vitamins, minerals, and other micronutrients needed for good health. However, many women in the U.S., and a very large percentage of poor women, do not follow optimal diets 242. Thus, for most women a daily multivitamin-multimineral supplement provides good insurance against nutritional deficiencies 243. Such supplements usually include extra iron, which is needed by the 9% to 11% of premenopausal women with iron deficiency 244.
The most firmly established benefit of vitamin supplements is that additional folic acid can reduce the risk of neural tube defects by approximately 70% 245. Current guidelines call for all women of childbearing age to take a daily supplement containing 400 to 800 micrograms (μg) of folic acid, or 4 milligrams (mg) for women with a child with a neural tube defect.
Calcium is important for the maintenance of bone strength. Precisely how much calcium is needed is a controversial question. World Health Organization (WHO) guidelines recommend an intake of 400 mg/day. In the United Kingdom, 700 mg/day is considered adequate for women aged 19 years and older. In the United States, dietary guidelines recommend that adult women receive 1,500 mg of calcium daily 246, in large part by consuming 3 servings of low-fat or fat-free dairy products a day 247. A lower-calorie, no-fat option is to get calcium from supplements.
For maintaining bone strength, other factors—including physical activity and vitamin D—are as important, or more important, than calcium. There is mounting evidence that current recommendations for vitamin D (200–600 IU/day, depending on age) are too low, and that 1,000 IU/day provides better protection against fractures and possibly heart disease and some cancers 248. Excess intake of preformed vitamin A (retinol) has been associated with an increased risk of hip fracture, possibly by competing with vitamin D 249. However, elevated risk is seen at intakes slightly higher than the current Dietary Reference Intake of 700 μg per day. Given this concern, a multivitamin that delivers much of its vitamin A as beta-carotene is preferred.
Physical activity
Stay physically active to complement eating a healthy diet. Staying active regularly is essential for good physical and mental health and wellbeing. This is true no matter how young or old you are. Physical activity has a positive impact on brain health. Based on epidemiological evidence, people who lead a physically active lifestyle have lower risk of cognitive decline. Based on randomized controlled trials, people who participate in purposeful exercise (e.g. brisk walking, cycling, strength training, group exercise classes, etc.) show beneficial changes in brain structure and function. However, in spite of the link between physical activity and brain health, there is not yet sufficient scientific evidence that physical activity can reduce risk of brain diseases that cause dementia (e.g. Alzheimer’s disease).
Despite not being able to conclude which types of exercise are better than others based on current evidence, research indicates that people who are less active can benefit their brain health by becoming more active. For example, evidence indicates that individuals who lead inactive or sedentary lifestyles stand to benefit more from an increase in physical activity than those who are already physically active and take up a new exercise regimen. Even without consensus on the optimal type of exercise, all the participants recommend that people should start thinking about the type, frequency, duration and intensity of exercise they currently get either at work or in leisure time, and consider how they could increase or vary that. If an individual is sedentary during the day, standing up and taking walking breaks is helpful.
Adults should be active most days, preferably every day. Each week, adults should do either:
- 2.5 to 5 hours of moderate intensity physical activity – such as a brisk walk, golf, mowing the lawn or swimming
- 1.25 to 2.5 hours of vigorous intensity physical activity – such as jogging, aerobics, fast cycling, soccer or netball
- an equivalent combination of moderate and vigorous activities.
Include muscle-strengthening activities as part of your daily physical activity on at least 2 days each week. This can be:
- push-ups
- pull-ups
- squats or lunges
- lifting weights
- household tasks that involve lifting, carrying or digging.
Doing any physical activity is better than doing none. If you do no physical activity right now, start by doing some, then slowly build up to the recommended amount.
Long periods of sitting can offset the benefits of being physically active, so it’s important to:
- reduce the time you spend sitting – for example, by organising walking meetings, using a standing desk, or enjoying a walk during your lunch break
- break up long periods of sitting – for example, by doing lunges or star jumps or walking around when on the phone.
Brain supplements summary
Research suggests that a diet rich in antioxidant vitamins may slow the progression of Alzheimer’s disease 155. Data on supplementation with vitamins A, B, C, D, and E vitamins are ambiguous. There are no international guidelines for dietary recommendations in Alzheimer’s disease. The conducted meta-analyses suggest that vitamins A, B, C, D, and E deficiencies may increase the risk of Alzheimer’s disease, therefore, a diet rich in vitamins A, D, C, B6, B12, and folic acid seems to be recommended in the prevention of Alzheimer’s disease. In meta-analyses of observational research, a diet rich in vitamins C and E was linked to a 20 to 25 percent lower risk of Alzheimer’s disease 174. However, in two randomized controlled trials, vitamin E or vitamin E and C supplements did not help patients with mild cognitive impairment (MCI) 175. Supplementation with both vitamins C and E failed to slow cognitive decline for women over age 65 177 although another observational study reported more promising results 178. It is possible that supplements are helpful but only for people who do not consume enough vitamin E or C through their diets. Nevertheless, current evidence suggests that vitamin C or E supplementation, alone or in combination, is unlikely to promote cognition or prevent cognitive decline in most people. In conclusion, adequate quantities of fruit and vegetables will supplement the deficiency of antioxidant vitamins, which are often deficient in patients with dementia. Further research are needed to resolving unclear issues.
References- 2019 AARP Brain Health and Dietary Supplements Survey. https://www.aarp.org/content/dam/aarp/research/surveys_statistics/health/2019/brain-health-and-dietary-supplements-report.doi.10.26419-2Fres.00318.001.pdf
- The Real Deal on Brain Health Supplements: GCBH Recommendations on Vitamins, Minerals, and Other Dietary Supplements. https://www.aarp.org/content/dam/aarp/health/brain_health/2019/06/gcbh-supplements-report-english.doi.10.26419-2Fpia.00094.001.pdf
- Serra-Majem, L., Tomaino, L., Dernini, S., Berry, E. M., Lairon, D., Ngo de la Cruz, J., Bach-Faig, A., Donini, L. M., Medina, F. X., Belahsen, R., Piscopo, S., Capone, R., Aranceta-Bartrina, J., La Vecchia, C., & Trichopoulou, A. (2020). Updating the Mediterranean Diet Pyramid towards Sustainability: Focus on Environmental Concerns. International journal of environmental research and public health, 17(23), 8758. https://doi.org/10.3390/ijerph17238758
- Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, Obarzanek E, Conlin PR, Miller ER 3rd, Simons-Morton DG, Karanja N, Lin PH; DASH-Sodium Collaborative Research Group. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med. 2001 Jan 4;344(1):3-10. doi: 10.1056/NEJM200101043440101
- Morris, M. C., Tangney, C. C., Wang, Y., Sacks, F. M., Bennett, D. A., & Aggarwal, N. T. (2015). MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimer’s & dementia : the journal of the Alzheimer’s Association, 11(9), 1007–1014. https://doi.org/10.1016/j.jalz.2014.11.009
- Hosking DE, Eramudugolla R, Cherbuin N, Anstey KJ. MIND not Mediterranean diet related to 12-year incidence of cognitive impairment in an Australian longitudinal cohort study. Alzheimers Dement. 2019 Apr;15(4):581-589. doi: 10.1016/j.jalz.2018.12.011
- Berendsen AM, Kang JH, Feskens EJM, de Groot CPGM, Grodstein F, van de Rest O. Association of Long-Term Adherence to the MIND Diet with Cognitive Function and Cognitive Decline in American Women. J Nutr Health Aging. 2018;22(2):222-229. doi: 10.1007/s12603-017-0909-0
- Chen X, Huang Y, Cheng HG. Lower intake of vegetables and legumes associated with cognitive decline among illiterate elderly Chinese: a 3-year cohort study. J Nutri Health Aging. 2012;16(6):549–552.
- Morris MC, Wang Y, Barnes LL, Bennett DA, Dawson-Hughes B, Booth SL. Nutrients and bioactives in green leafy vegetables and cognitive decline: Prospective study. Neurology. 2018 Jan 16;90(3):e214-e222. doi: 10.1212/WNL.0000000000004815
- Morris MC, Evans DA, Tangney CC, Bienias JL, Wilson RS. Associations of vegetable and fruit consumption with age-related cognitive change. Neurology. 2006 Oct 24;67(8):1370-6. doi: 10.1212/01.wnl.0000240224.38978.d8
- Devore EE, Kang JH, Breteler MM, Grodstein F. Dietary intakes of berries and flavonoids in relation to cognitive decline. Ann Neurol. 2012 Jul;72(1):135-43. doi: 10.1002/ana.23594
- Diet May Help Prevent Alzheimer’s. https://www.rush.edu/news/diet-may-help-prevent-alzheimers
- Davis B.A., Prall B.C. The challenges of incorporation of omega-3 fatty acids into ration components and their prevalence in garrison feeding. Military medicine. 2014;179:162–167. doi: 10.7205/MILMED-D-14-00172
- Bailes J.E., Patel V. The potential for DHA to mitigate mild traumatic brain injury. Mil. Med. 2014;179:112–116. doi: 10.7205/MILMED-D-14-00139
- Stonehouse W., Conlon C.A., Podd J., Hill S.R., Minihane A.M., Haskell C., Kennedy D. DHA supplementation improved both memory and reaction time in healthy young adults: a randomized controlled trial. Am. J. Clin. Nutr. 2013;97:1134–1143. doi: 10.3945/ajcn.112.053371
- Barrett, E., McBurney, M., & Ciappio, E. (2014). Omega-3 fatty acid supplementation as a potential therapeutic aid for the recovery from mild traumatic brain injury/concussion. Advanced Nutrition, 5(3), 268–277. doi:10.3945/an.113.005280
- Jackson P.A., Reay J.L., Scholey A.B., Kennedy D.O. DHA-rich oil modulates the cerebral haemodynamic response to cognitive tasks in healthy young adults: a near IR spectroscopy pilot study. Br. J. Nutr. 2012;107:1093–1098. doi: 10.1017/S0007114511004041
- Pandey KB, Rizvi SI. Plant polyphenols as dietary antioxidants in human health and disease. Oxidative Medicine and Cellular Longevity. 2009;2(5):270-278. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2835915/
- Dietary polyphenols and the prevention of diseases. Scalbert A, Manach C, Morand C, Rémésy C, Jiménez L. Crit Rev Food Sci Nutr. 2005; 45(4):287-306. https://www.ncbi.nlm.nih.gov/pubmed/16047496/
- Biomarkers of the intake of dietary polyphenols: strengths, limitations and application in nutrition research. Spencer JP, Abd El Mohsen MM, Minihane AM, Mathers JC. Br J Nutr. 2008 Jan; 99(1):12-22. https://www.ncbi.nlm.nih.gov/pubmed/17666146/
- Vauzour, D. (2012). Dietary polyphenols as modulators of brain functions: Biological actions and molecular mechanisms underpinning their beneficial effects. Oxidative Medicine and Cell Longevitv, 2012, 914273.
- Somerville, V., Bringans, C., & Braakhuis, A. (2017). Polyphenols and performance: A systematic review and meta-analysis. Sports Medicine, Aug, 47(8), 1589–1599. doi:10.1007/s40279-017-0675-5
- Meeusen, R. (2014). Exercise, nutrition and the brain. Sports Medicine, 44(Suppl. 1), 47–56. doi:10.1007/s40279-014-0150-5
- Decroix, L., Tonoli, C., Soares, D., Tagougui, S., Heyman, E., & Meeusen, R. (2016). Acute cocoa flavanol improves cerebral oxygenation without enhancing executive function at rest or after exercise. Journal of Applied Physiology, Nutrition and Metabolism, 41(12), 1225–1232. doi:10.1139/apnm-2016-0245
- British Journal of Nutrition, Volume 99, Issue 1, January 2008 , pp. 12-22. Biomarkers of the intake of dietary polyphenols: strengths, limitations and application in nutrition research. https://www.cambridge.org/core/journals/british-journal-of-nutrition/article/biomarkers-of-the-intake-of-dietary-polyphenols-strengths-limitations-and-application-in-nutrition-research/BBAB7EA49BCD0434EFB38098BDAA387C
- Polyphenols: food sources and bioavailability. Manach C, Scalbert A, Morand C, Rémésy C, Jiménez L. Am J Clin Nutr. 2004 May; 79(5):727-47. http://ajcn.nutrition.org/content/79/5/727.long
- Scholey A.B., French S.J., Morris P.J., Kennedy D.O., Milne A.L., Haskell C.F. Consumption of cocoa flavanols results in acute improvements in mood and cognitive performance during sustained mental effort. J. Psychopharmacol. 2010;24:1505–1514. doi: 10.1177/0269881109106923
- Bell L., Lamport D.J., Butler L.T., Williams C.M. A Review of the Cognitive Effects Observed in Humans Following Acute Supplementation with Flavonoids, and Their Associated Mechanisms of Action. Nutrients. 2015;7:10290–10306. doi: 10.3390/nu7125538
- Spencer J.P.E. Flavonoids and brain health: multiple effects underpinned by common mechanisms. Genes Nutr. 2009;4:243–250. doi: 10.1007/s12263-009-0136-3
- Lamport D.J., Pal D., Macready A.L., Barbosa-Boucas S., Fletcher J.M., Williams C.M., Spencer J.P., Butler L.T. The effects of flavanone-rich citrus juice on cognitive function and cerebral blood flow: an acute, randomised, placebo-controlled cross-over trial in healthy, young adults. Br. J. Nutr. 2017;116:2160–2168. doi: 10.1017/S000711451600430X
- Watson A.W., Haskell-Ramsay C.F., Kennedy D.O., Cooney J.M., Trower T., Scheepens A. Acute supplementation with blackcurrant extracts modulates cognitive functioning and inhibits monoamine oxidase-B in healthy young adults. J. Functional Foods. 2015;17:524–539. doi: 10.1016/j.jff.2015.06.005
- Wightman E.L., Haskell C.F., Forster J.S., Veasey R.C., Kennedy D.O. Epigallocatechin gallate, cerebral blood flow parameters, cognitive performance and mood in healthy humans: a double-blind, placebo-controlled, crossover investigation. Hum. Psychopharmacol. 2012;27:177–186. doi: 10.1002/hup.1263
- Scholey, A., Tildesley, N., Ballard, C., Wesnes, K.A., Tasker, A., Perry, E.K., & Kennedy, D.O. (2008). An extract of Salvia (sage) with anticholinesterase properties improves memory and attention in healthy older volunteers. Psychopharmacology, 198, 127–139. PubMed doi:10.1007/s00213-008-1101-3
- Nehlig, A. (2013). The neuroprotective effects of cocoa flavanol and its influence on cognitive performance. British Journal of Clinical Pharmacology, 75, 716–727. doi:10.1111/j.1365-2125.2012.04378.x
- Ried, K., Sullivan, T., Fakler, P., Frank, O., & Stocks, N. (2012). Effect of cocoa on blood pressure. Cochrane Database Systematic Reviews, (8), CD008893.
- Wightman E.L., Haskell-Ramsay C.F., Thompson K.G., Blackwell J.R., Winyard P.G., Forster J., Jones A.M., Kennedy D.O. Dietary nitrate modulates cerebral blood flow parameters and cognitive performance in humans: A double-blind, placebo-controlled, crossover investigation. Physiol. Behav. 2015;149:149–158. doi: 10.1016/j.physbeh.2015.05.035
- Presley T.D., Morgan A.R., Bechtold E., Clodfelter W., Dove R.W., Jennings J.M., Kraft R.A., King S.B., Laurienti P.J., Jack W. Acute effect of a high nitrate diet on brain perfusion in older adults. Nitric Oxide. 2011;24:34–42. doi: 10.1016/j.niox.2010.10.002
- Thompson K.G., Turner L., Prichard J., Dodd F., Kennedy D.O., Haskell C., Blackwell J.R., Jones A.M. Influence of dietary nitrate supplementation on physiological and cognitive responses to incremental cycle exercise. Respir. Physiol. Neurobiol. 2014;193:11–20. doi: 10.1016/j.resp.2013.12.015
- Glade M.J. Caffeine-Not just a stimulant. Nutrition. 2010;26:932–938. doi: 10.1016/j.nut.2010.08.004.
- McLellan T.M., Caldwell J.A., Lieberman H.R. A review of caffeine’s effects on cognitive, physical and occupational performance. Neurosci. Biobehav. Rev. 2016;71:294–312. doi: 10.1016/j.neubiorev.2016.09.001
- Ullrich S., de Vries Y.C., Kuhn S., Repantis D., Dresler M., Ohla K. Feeling smart: Effects of caffeine and glucose on cognition, mood and self-judgment. Physiol. Behav. 2015;151:629–637. doi: 10.1016/j.physbeh.2015.08.028
- Crawford C., Teo L., Lafferty L., Drake A., Bingham J.J., Gallon M.D., O’Connell M.L., Chittum H.K., Azorla S.M., Berry K. Caffeine to optimize cognitive function for military mission-readiness: a systematic review and recommendations for the field. Nutr. Rev. 2017;75:17–35. doi: 10.1093/nutrit/nux007
- Wu L, Sun D, He Y. Coffee intake and the incident risk of cognitive disorders: A dose-response meta-analysis of nine prospective cohort studies. Clin Nutr. 2017 Jun;36(3):730-736. doi: 10.1016/j.clnu.2016.05.015
- Cappelletti S, Piacentino D, Sani G, Aromatario M. Caffeine: cognitive and physical performance enhancer or psychoactive drug? Curr Neuropharmacol. 2015 Jan;13(1):71-88. doi: 10.2174/1570159X13666141210215655. Erratum in: Curr Neuropharmacol. 2015;13(4):554. Daria, Piacentino [corrected to Piacentino, Daria].
- Panza F, Solfrizzi V, Barulli MR, Bonfiglio C, Guerra V, Osella A, Seripa D, Sabbà C, Pilotto A, Logroscino G. Coffee, tea, and caffeine consumption and prevention of late-life cognitive decline and dementia: a systematic review. J Nutr Health Aging. 2015 Mar;19(3):313-28. doi: 10.1007/s12603-014-0563-8
- Baker LB, Nuccio RP, Jeukendrup AE. Acute effects of dietary constituents on motor skill and cognitive performance in athletes. Nutr Rev. 2014 Dec;72(12):790-802. doi: 10.1111/nure.12157
- Kromhout MA, Jongerling J, Achterberg WP. Relation between caffeine and behavioral symptoms in elderly patients with dementia: an observational study. J Nutr Health Aging. 2014 Apr;18(4):407-10. doi: 10.1007/s12603-013-0417-9
- Cao C, Loewenstein DA, Lin X, Zhang C, Wang L, Duara R, Wu Y, Giannini A, Bai G, Cai J, Greig M, Schofield E, Ashok R, Small B, Potter H, Arendash GW. High Blood caffeine levels in MCI linked to lack of progression to dementia. J Alzheimers Dis. 2012;30(3):559-72. doi: 10.3233/JAD-2012-111781
- Solfrizzi V, Panza F, Imbimbo BP, D’Introno A, Galluzzo L, Gandin C, Misciagna G, Guerra V, Osella A, Baldereschi M, Di Carlo A, Inzitari D, Seripa D, Pilotto A, Sabbá C, Logroscino G, Scafato E; Italian Longitudinal Study on Aging Working Group. Coffee Consumption Habits and the Risk of Mild Cognitive Impairment: The Italian Longitudinal Study on Aging. J Alzheimers Dis. 2015;47(4):889-99. doi: 10.3233/JAD-150333
- Walters ER, Lesk VE. The Effect of Prior Caffeine Consumption on Neuropsychological Test Performance: A Placebo-Controlled Study. Dement Geriatr Cogn Disord. 2016;41(3-4):146-51. doi: 10.1159/000443952
- Kamimori G.H., McLellan T.M., Tate C.M., Voss D.M., Niro P., Lieberman H.R. Caffeine improves reaction time, vigilance and logical reasoning during extended periods with restricted opportunities for sleep. Psychopharmacology (Berlin) 2015;232:2031–2042. doi: 10.1007/s00213-014-3834-5
- Aidman E., Johnson K., Paech G.M., Della Vedova C., Pajcin M., Grant C., Kamimori G.H., Mitchelson E., Hoggan B.L., Fidock J., et al. Caffeine reduces the impact of drowsiness in driving errors. Transp. Res. Part F: Traffic Psychol. Behav. 2018;54:236–247. doi: 10.1016/j.trf.2018.01.008
- Reyner L.A., Horne J.A. Early morning driver sleepiness: Effectiveness of 200 mg caffeine. Psychophysiology. 2000;37:251–256. doi: 10.1111/1469-8986.3720251
- Kahathuduwa C.N., Dassanayake T.L., Amarakoon A.M., Weerasinghe V.S. Acute effects of theanine, caffeine and theanine-caffeine combination on attention. Nutr. Neurosci. 2017 doi: 10.1080/1028415X.2016.1144845
- Brunye T.T., Mahoney C.R., Lieberman H.R., Giles G.E., Taylor H.A. Acute caffeine consumption enhances the executive control of visual attention in habitual consumers. Brain Cogn. 2010;74:186–192. doi: 10.1016/j.bandc.2010.07.006
- Soar K., Chapman E., Lavan N., Jansari A.S., Turner J.J.D. Investigating the effects of caffeine on executive functions using traditional Stroop and a new ecologically-valid virtual reality task, the Jansari assessment of Executive Functions (JEF) Appetite. 2016;105:156–163. doi: 10.1016/j.appet.2016.05.021
- Hussain S.J., Cole K.J. No Enhancement of 24-Hour Visuomotor Skill Retention by Post-Practice Caffeine Administration. PLoS ONE. 2015;10:e0129543. doi: 10.1371/journal.pone.0129543
- Pomeroy, D. E., Tooley, K. L., Probert, B., Wilson, A., & Kemps, E. (2020). A Systematic Review of the Effect of Dietary Supplements on Cognitive Performance in Healthy Young Adults and Military Personnel. Nutrients, 12(2), 545. https://doi.org/10.3390/nu12020545
- Kennedy D.O., Scholey A.B., Wesnes K.A. Modulation of cognition and mood following administration of single doses of Ginkgo biloba, ginseng, and a ginkgo/ginseng combination to healthy young adults. Physiol. Behav. 2002;75:739–751. doi: 10.1016/S0031-9384(02)00665-0
- Cui Y, Shu XO, Gao YT, Cai H, Tao MH, Zheng W. Association of ginseng use with survival and quality of life among breast cancer patients. Am J Epidemiol. 2006 Apr 1;163(7):645-53. doi: 10.1093/aje/kwj087
- Tachikawa E., Kudo K., Harada K., Kashimoto T., Miyate Y., Kakizaki A., Takahashi E. Effects of ginseng saponins on responses induced by various receptor stimuli. Euro. J. Pharmacol. 1999;369:23–32. doi: 10.1016/S0014-2999(99)00043-6
- Reay J.L., Scholey A.B., Kennedy D.O. Panax ginseng (G115) improves aspects of working memory performance and subjective ratings of calmness in healthy young adults. Hum. Psychopharmacol. 2010;25:462–471. doi: 10.1002/hup.1138
- Namgung E, Kim J, Jeong H, Hong G, Kim M, Kim RY, Kim S, Lyoo IK. Effects of Korean red ginseng on human gray matter volume and cognitive function: A voxel-based morphometry study. Hum Psychopharmacol. 2021 Mar;36(2):e2767. doi: 10.1002/hup.2767
- Park KC, Jin H, Zheng R, Kim S, Lee SE, Kim BH, Yim SV. Cognition enhancing effect of panax ginseng in Korean volunteers with mild cognitive impairment: a randomized, double-blind, placebo-controlled clinical trial. Transl Clin Pharmacol. 2019 Sep;27(3):92-97. doi: 10.12793/tcp.2019.27.3.92
- Geng J, Dong J, Ni H, Lee MS, Wu T, Jiang K, Wang G, Zhou AL, Malouf R. Ginseng for cognition. Cochrane Database Syst Rev. 2010 Dec 8;(12):CD007769. doi: 10.1002/14651858.CD007769.pub2
- D’Angelo L, Grimaldi R, Caravaggi M, Marcoli M, Perucca E, Lecchini S, Frigo GM, Crema A. A double-blind, placebo-controlled clinical study on the effect of a standardized ginseng extract on psychomotor performance in healthy volunteers. J Ethnopharmacol. 1986 Apr-May;16(1):15-22. doi: 10.1016/0378-8741(86)90063-2
- Sünram-Lea, S., Birchall, R., Wesnes, K., & Petrini, O. (2005). The effect of acute administration of 400mg of Panax ginseng on cognitive performance and mood in healthy young volunteers.https://www.semanticscholar.org/paper/The-effect-of-acute-administration-of-400mg-of-on-Sünram-Lea-Birchall/39c285a8e9cc6e24fc2d6c5ac24a917842f67416
- Sørensen H, Sonne J (1996) A double-masked study of the effects of ginseng on cognitive functions. Current Therapeutic Research 57, 959-968. https://doi.org/10.1016/S0011-393X(96)80114-7
- Moreira SC, Jansen AK, Silva FM. Dietary interventions and cognition of Alzheimer’s disease patients: a systematic review of randomized controlled trial. Dement Neuropsychol. 2020 Jul-Sep;14(3):258-282. doi: 10.1590/1980-57642020dn14-030008
- Heo JH, Lee ST, Chu K, Oh MJ, Park HJ, Shim JY, Kim M. Heat-processed ginseng enhances the cognitive function in patients with moderately severe Alzheimer’s disease. Nutr Neurosci. 2012 Nov;15(6):278-82. doi: 10.1179/1476830512Y.0000000027
- Lee ST, Chu K, Sim JY, Heo JH, Kim M. Panax ginseng enhances cognitive performance in Alzheimer disease. Alzheimer Dis Assoc Disord. 2008 Jul-Sep;22(3):222-6. doi: 10.1097/WAD.0b013e31816c92e6
- Heo JH, Lee ST, Oh MJ, Park HJ, Shim JY, Chu K, Kim M. Improvement of cognitive deficit in Alzheimer’s disease patients by long term treatment with korean red ginseng. J Ginseng Res. 2011 Nov;35(4):457-61. doi: 10.5142/jgr.2011.35.4.457
- Lho SK, Kim TH, Kwak KP, Kim K, Kim BJ, Kim SG, Kim JL, Kim TH, Moon SW, Park JY, Park JH, Byun S, Suh SW, Seo JY, So Y, Ryu SH, Youn JC, Lee KH, Lee DY, Lee DW, Lee SB, Lee JJ, Lee JR, Jeong H, Jeong HG, Jhoo JH, Han K, Hong JW, Han JW, Kim KW. Effects of lifetime cumulative ginseng intake on cognitive function in late life. Alzheimers Res Ther. 2018 May 24;10(1):50. doi: 10.1186/s13195-018-0380-0
- Hernández-García D, Granado-Serrano AB, Martín-Gari M, Naudí A, Serrano JC. Efficacy of Panax ginseng supplementation on blood lipid profile. A meta-analysis and systematic review of clinical randomized trials. J Ethnopharmacol. 2019 Oct 28;243:112090. doi: 10.1016/j.jep.2019.112090
- Coon JT, Ernst E. Panax ginseng: a systematic review of adverse effects and drug interactions. Drug Saf. 2002;25(5):323-44. doi: 10.2165/00002018-200225050-00003
- Kennedy D.O., Scholey A.B., Wesnes K.A. The dose-dependent cognitive effects of acute administration of Ginkgo biloba to healthy young volunteers. Psychopharmacology. 2000;151:416–423. doi: 10.1007/s002130000501
- Ude C., Paulke A., Nőldner M., Schubert-Zsilavecz M., Wurglics M. Plasma and brain levels of terpene trilactones in rats after an oral single dose of standardized Gingko biloba extract EGb 761(R) Planta Medica. 2011;77:259–264. doi: 10.1055/s-0030-1250286
- Gorby, H., Brownawell, A., & Falk, M. (2010). Do specific dietary constituents and supplements affect mental energy? Review of the evidence. Nutrition Reviews, 68(12), 697–718. PubMed doi:10.1111/j.1753-4887.2010.00340.x
- Kennedy D.O., Haskell C.F., Mauri P.L., Scholey A.B. Acute cognitive effects of standardised Ginkgo biloba extract complexed with phosphatidylserine. Hum. Psychopharmacol. 2007;22:199–210. doi: 10.1002/hup.837
- Vellas B, Coley N, Ousset PJ, Berrut G, Dartigues JF, Dubois B, Grandjean H, Pasquier F, Piette F, Robert P, Touchon J, Garnier P, Mathiex-Fortunet H, Andrieu S; GuidAge Study Group. Long-term use of standardised Ginkgo biloba extract for the prevention of Alzheimer’s disease (GuidAge): a randomised placebo-controlled trial. Lancet Neurol. 2012 Oct;11(10):851-9. doi: 10.1016/S1474-4422(12)70206-5
- Eckert A. Mitochondrial effects of Ginkgo biloba extract. Int Psychogeriatr. 2012 Aug;24 Suppl 1:S18-20. doi: 10.1017/S1041610212000531
- Birks J, Grimley Evans J. Ginkgo biloba for cognitive impairment and dementia. Cochrane Database Syst Rev. 2009 Jan 21;(1):CD003120. doi: 10.1002/14651858.CD003120.pub3
- Hashiguchi M, Ohta Y, Shimizu M, Maruyama J, Mochizuki M. Meta-analysis of the efficacy and safety of Ginkgo biloba extract for the treatment of dementia. J Pharm Health Care Sci. 2015 Apr 10;1:14. doi: 10.1186/s40780-015-0014-7
- Yang G, Wang Y, Sun J, Zhang K, Liu J. Ginkgo Biloba for Mild Cognitive Impairment and Alzheimer’s Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr Top Med Chem. 2016;16(5):520-8. doi: 10.2174/1568026615666150813143520
- Elsabagh S., Hartley D.E., Ali O., Williamson E.M., File S.E. Differential cognitive effects of Ginkgo biloba after acute and chronic treatment in healthy young volunteers. Psychopharmacology (Berlin) 2005;179:437–446. doi: 10.1007/s00213-005-2206-6
- Moulton P.L., Boyko L.N., Fitzpatrick J.L., Petros T.V. The effect of Ginkgo biloba on memory in healthy male volunteers. Physiol. Behave. 2001;73:659–665. doi: 10.1016/S0031-9384(01)00510-8
- Scholey A.B., Kennedy D.O. Acute, dose-dependent cognitive effects of Ginkgo biloba, Panax ginseng and their combination in healthy young volunteers differential interactions with cognitive demand. Hum. Psychopharmacol.: Clin. Expe. 2002;17:35–44. doi: 10.1002/hup.352
- Kellermann AJ, Kloft C. Is there a risk of bleeding associated with standardized Ginkgo biloba extract therapy? A systematic review and meta-analysis. Pharmacotherapy. 2011 May;31(5):490-502. doi: 10.1592/phco.31.5.490
- Heinonen T, Gaus W. Cross matching observations on toxicological and clinical data for the assessment of tolerability and safety of Ginkgo biloba leaf extract. Toxicology. 2015 Jan 2;327:95-115. doi: 10.1016/j.tox.2014.10.013
- Kennedy D.O., Haskell C.F., Robertson B., Reay J., Brewster-Maund C., Luedemann J., Maggini S., Ruf M., Zangara A., Scholey A.B. Improved cognitive performance and mental fatigue following a multi-vitamin and mineral supplement with added guarana (Paullinia cupana) Appetite. 2008;50:506–513. doi: 10.1016/j.appet.2007.10.007
- Kennedy D.O., Haskell C.F., Wesnes K.A., Scholey A.B. Improved cognitive performance in human volunteers following administration of guarana (Paullinia cupana) extract: comparison and interaction with Panax ginseng. Pharmacol. Biochem. Behave. 2004;79:401–411. doi: 10.1016/j.pbb.2004.07.014
- Weckerle C.A., Stutz M.A., Baumann T.W. Purine alkaloids in Paullinia. Phytochemistry. 2003;64:735–742. doi: 10.1016/S0031-9422(03)00372-8
- Espinola E.B., Dias R.F., Mattei R., Carlini E.A. Pharmacological activity of Guaranan (Paullinia cupana Mart) in laboratory animals. J. Ethnopharmacol. 1997;55:223–229. doi: 10.1016/S0378-8741(96)01506-1
- Haskell C.F., Kennedy D.O., Wesnes K.A., Milne A.L., Scholey A.B. A double-blind, placebo-controleld, multi-dose evaluationm of the acute behavioural effects of guarana in humans. J. Psychopharmacol. 2007;21:65–70. doi: 10.1177/0269881106063815
- Veasey R.C., Haskell-Ramsay C.F., Kennedy D.O., Wishart K., Maggini S., Fuchs C.J., Stevenson E.J. The Effects of Supplementation with a Vitamin and Mineral Complex with Guarana Prior to Fasted Exercise on Affect, Exertion, Cognitive Performance, and Substrate Metabolism: A Randomized Controlled Trial. Nutrients. 2015;7:6109–6127. doi: 10.3390/nu7085272
- Kennedy, D.O., Haskell, C.F., Wesnes, K.A., & Scholey, A.B. (2004). Improved cognitive performance in human volunteers following administration of guarana (Paullinia cupana) extract: Comparison and interaction with Panax ginseng. Pharmacology Biochemistry and Behavior, 79(3), 401–411.
- Haskell, C.F., Kennedy, D.O., Wesnes, K.A., Milne, A.L., & Scholey, A.B. (2007). A double-blind, placebo-controlled, multi-dose evaluation of the acute behavioural effects of guaraná in humans. Journal of Psychopharmacology, 21(1), 65–70. PubMed doi:10.1177/0269881106063815
- Veasey, R., Haskell-Ramsay, C., Kennedy, D., Wishart, K., Maggini, S., Fuchs, C., & Stevenson, E. (2015). The effects of supplementation with a vitamin and mineral complex with guaraná prior to fasted exercise on affect, exertion, cognitive performance, and substrate metabolism: A randomized controlled trial. Nutrients, 7(8), 6109–6127. PubMed doi:10.3390/nu7085272
- Pomportes, L., Brisswalter, J., Casini, L., Hays, A., & Davranche, K. (2017). Cognitive performance enhancement induced by caffeine, carbohydrate and guarana mouth rinsing during submaximal exercise. Nutrients, 9(6), 589. PubMed doi:10.3390/nu9060589
- De Bock, K, Eijnde, B.O., Ramaekers, M., & Hespel, P. (2004). Acute Rhodiola rosea intake can improve endurance exercise performance. International Journal of Sport Nutritioan and Exercise Metabolism, 14, 298–307. doi:10.1123/ijsnem.14.3.298
- Noreen, E., Buckley, J.G., Lewis, S.L., Brandauer, J., & Stuempfle, K.J. (2013). The effects of an acute dose of Rhodiola rosea on endurance exercise performance. Journal of Strength & Conditioning Research, 27, 839–847. PubMed doi:10.1519/JSC.0b013e31825d9799
- Kennedy, D., Pace, S., Haskell, C., Okello, E.J., Milne, A., & Scholey, A.B. (2006). Effects of cholinesterase inhibiting sage (Salvia officinalis) on mood, anxiety and performance on a psychological stressor battery. Neuropsychopharmacology, 31, 845–852. PubMed doi:10.1038/sj.npp.1300907
- Tildesley, N., Kennedy, D., Perry, E., Ballard, C.G., Wesnes, K.A., & Scholey, A.B. (2005). Positive modulation of mood and cognitive performance following administration of acute doses of Salvia lavandulaefolia essential oil to healthy young volunteers. Physiology and Behavior, 83, 699–709. PubMed doi:10.1016/j.physbeh.2004.09.010
- Kim HY, Huang BX, Spector AA. Phosphatidylserine in the brain: metabolism and function. Prog Lipid Res. 2014 Oct;56:1-18. doi: 10.1016/j.plipres.2014.06.002
- Engel RR, Satzger W, Günther W, Kathmann N, Bove D, Gerke S, Münch U, Hippius H. Double-blind cross-over study of phosphatidylserine vs. placebo in patients with early dementia of the Alzheimer type. Eur Neuropsychopharmacol. 1992 Jun;2(2):149-55. doi: 10.1016/0924-977x(92)90025-4
- Crook T, Petrie W, Wells C, Massari DC. Effects of phosphatidylserine in Alzheimer’s disease. Psychopharmacol Bull. 1992;28(1):61-6.
- Delwaide PJ, Gyselynck-Mambourg AM, Hurlet A, Ylieff M. Double-blind randomized controlled study of phosphatidylserine in senile demented patients. Acta Neurol Scand. 1986 Feb;73(2):136-40. doi: 10.1111/j.1600-0404.1986.tb03254.x
- Strike SC, Carlisle A, Gibson EL, Dyall SC. A High Omega-3 Fatty Acid Multinutrient Supplement Benefits Cognition and Mobility in Older Women: A Randomized, Double-blind, Placebo-controlled Pilot Study. J Gerontol A Biol Sci Med Sci. 2016 Feb;71(2):236-42. doi: 10.1093/gerona/glv109
- Vakhapova V, Cohen T, Richter Y, Herzog Y, Korczyn AD. Phosphatidylserine containing omega-3 fatty acids may improve memory abilities in non-demented elderly with memory complaints: a double-blind placebo-controlled trial. Dement Geriatr Cogn Disord. 2010;29(5):467-74. doi: 10.1159/000310330
- Cenacchi T, Bertoldin T, Farina C, Fiori MG, Crepaldi G. Cognitive decline in the elderly: a double-blind, placebo-controlled multicenter study on efficacy of phosphatidylserine administration. Aging (Milano). 1993 Apr;5(2):123-33. doi: 10.1007/BF03324139
- Heiss WD, Kessler J, Mielke R, Szelies B, Herholz K. Long-term effects of phosphatidylserine, pyritinol, and cognitive training in Alzheimer’s disease. A neuropsychological, EEG, and PET investigation. Dementia. 1994 Mar-Apr;5(2):88-98. doi: 10.1159/000106702
- Jorissen BL, Brouns F, Van Boxtel MP, Ponds RW, Verhey FR, Jolles J, Riedel WJ. The influence of soy-derived phosphatidylserine on cognition in age-associated memory impairment. Nutr Neurosci. 2001;4(2):121-34. doi: 10.1080/1028415x.2001.11747356
- Vakhapova, V., et al., Safety of phosphatidylserine containing omega-3 fatty acids in non-demented elderly: a double-blind placebo-controlled trial followed by an open-label extension. BMC.Neurol., 2011. 11:79.: p. 79
- Requena JR, Kristensson K, Korth C, Zurzolo C, Simmons M, Aguilar-Calvo P, Aguzzi A, Andreoletti O, Benestad SL, Böhm R, Brown K, Calgua B, Del Río JA, Espinosa JC, Girones R, Godsave S, Hoelzle LE, Knittler MR, Kuhn F, Legname G, Laeven P, Mabbott N, Mitrova E, Müller-Schiffmann A, Nuvolone M, Peters PJ, Raeber A, Roth K, Schmitz M, Schroeder B, Sonati T, Stitz L, Taraboulos A, Torres JM, Yan ZX, Zerr I. The Priority position paper: Protecting Europe’s food chain from prions. Prion. 2016 May 3;10(3):165-81. doi: 10.1080/19336896.2016.1175801
- Hirabayashi Y, Furuya S. Roles of l-serine and sphingolipid synthesis in brain development and neuronal survival. Prog Lipid Res. 2008 May;47(3):188-203. doi: 10.1016/j.plipres.2008.01.003
- Zhai PP, Xu LH, Yang JJ, Jiang ZL, Zhao GW, Sun L, Wang GH, Li X. Reduction of inflammatory responses by L-serine treatment leads to neuroprotection in mice after traumatic brain injury. Neuropharmacology. 2015 Aug;95:1-11. doi: 10.1016/j.neuropharm.2015.02.026
- Phase IIa L-serine Trial for eAD (LSPI-2). https://clinicaltrials.gov/ct2/show/NCT03062449
- Biemans EA, Verhoeven-Duif NM, Gerrits J, Claassen JA, Kuiperij HB, Verbeek MM. CSF d-serine concentrations are similar in Alzheimer’s disease, other dementias, and elderly controls. Neurobiol Aging. 2016 Jun;42:213-6. doi: 10.1016/j.neurobiolaging.2016.03.017
- Hashimoto K, Fukushima T, Shimizu E, Okada S, Komatsu N, Okamura N, Koike K, Koizumi H, Kumakiri C, Imai K, Iyo M. Possible role of D-serine in the pathophysiology of Alzheimer’s disease. Prog Neuropsychopharmacol Biol Psychiatry. 2004 Mar;28(2):385-8. doi: 10.1016/j.pnpbp.2003.11.009
- Nagata Y, Borghi M, Fisher GH, D’Aniello A. Free D-serine concentration in normal and Alzheimer human brain. Brain Res Bull. 1995;38(2):181-3. doi: 10.1016/0361-9230(95)00087-u
- Cox PA, Davis DA, Mash DC, Metcalf JS, Banack SA. Dietary exposure to an environmental toxin triggers neurofibrillary tangles and amyloid deposits in the brain. Proc Biol Sci. 2016 Jan 27;283(1823):20152397. doi: 10.1098/rspb.2015.2397
- Dunlop RA, Cox PA, Banack SA, Rodgers KJ. The non-protein amino acid BMAA is misincorporated into human proteins in place of L-serine causing protein misfolding and aggregation. PLoS One. 2013 Sep 25;8(9):e75376. doi: 10.1371/journal.pone.0075376
- Ko R., Low Dog T., Gorecki D.K., Cantilena L.R., Costello R.B., Evans W.J., Hardy M.L., Jordan S.A., Maughan R.J., Rankin J.W., et al. Evidence-based evaluation of potential benefits and safety of beta-alanine supplementation for military personnel. Nutr. Rev. 2014;72:217–225. doi: 10.1111/nure.12087
- Murakami T., Furuse M. The impact of taurine and beta-alanine supplemented diets on behavioral and neurochemical parameters in mice: antidepressant versus anxiolytic-like effects. Amino Acids. 2010;39:427–434. doi: 10.1007/s00726-009-0458-x
- Hoffman J.R., Landau G., Stout J.R., Dabora M., Moran D.S., Sharvit N., Hoffman M.W., Ben Moshe Y., McCormack W.P., Hirschhorn G., et al. beta-alanine supplementation improves tactical performance but not cognitive function in combat soldiers. J. Intern. Soc. Sports Nutr. 2014;11:15. doi: 10.1186/1550-2783-11-15
- Jongkees B.J., Hommel B., Kuhn S., Colzato L.S. Effect of tyrosine supplementation on clinical and healthy populations under stress or cognitive demands–A review. J. Psychiatr. Res. 2015;70:50–57. doi: 10.1016/j.jpsychires.2015.08.014
- Meeusen R., Watson P., Hasegawa H., Roelands B., Piacentini M.F. Central fatigue: the serotonin hypothesis and beyond. Sports Med. 2006;36:881–909. doi: 10.2165/00007256-200636100-00006
- Attipoe S., Zeno S.A., Lee C., Crawford C., Khorsan R., Walter A.R., Deuster P.A. Tyrosine for mitigating stress and enhamcing performance in healthy adult humans, a Rapid Evidence Assessment of the Literature. Mil. Med. 2015;180:754–765. doi: 10.7205/MILMED-D-14-00594
- Watson P., Enever S., Page A., Stockwell J., Maughan R.J. Tyrosine supplementation does not influence the capacity to perform prolonged exercise in a warm environment. Intern. J. sport nutr. Exerc. Metabol. 2012;22:363–373. doi: 10.1123/ijsnem.22.5.363
- Colzato L.S., Jongkees B.J., Sellaro R., Hommel B. Working memory reloaded: tyrosine repletes updating in the N-back task. Front. Behav. Neurosci. 2013;7:200. doi: 10.3389/fnbeh.2013.00200
- Colzato L.S., Jongkees B.J., Sellaro R., van den Wildenberg W.P., Hommel B. Eating to stop: tyrosine supplementation enhances inhibitory control but not response execution. Neuropsychologia. 2014;62:398–402. doi: 10.1016/j.neuropsychologia.2013.12.027
- Colzato L.S., de Haan A.M., Hommel B. Food for creativity: tyrosine promotes deep thinking. Psycholog. Res. 2015;79:709–714. doi: 10.1007/s00426-014-0610-4
- Steenbergen L., Sellaro R., Hommel B., Colzato L.S. Tyrosine promotes cognitive flexibility: evidence from proactive vs. reactive control during task switching performance. Neuropsychologia. 2015;69:50–55. doi: 10.1016/j.neuropsychologia.2015.01.022
- Coull N., Watkins S.L., Aldous J.W., Warren L.K., Chrismas B.C., Dascombe B., Mauger A.R., Abt G., Taylor H. Effect of tyrosine ingestion on cognitive and physical performance utilising an intermittent soccer performance test (iSPT) in a warm environment. Euro. J. Appl. Physiol. 2015;115:373–386. doi: 10.1007/s00421-014-3022-7
- Kishore K., Ray K., Anand J.P., Thakur L., Kumar S., Panjwani U. Tyrosine ameliorates heat induced delay in event related potential P300 and contingent negative variation. Brain Cogn. 2013;83:324–329. doi: 10.1016/j.bandc.2013.09.005
- Jongkees B.J., Sellaro R., Beste C., Nitsche M.A., Kuhn S., Colzato L.S. L-Tyrosine administration modulates teh effect of transcranial direct current stimulation on working memory in healthy humans. Cortex. 2017:103–114. doi: 10.1016/j.cortex.2017.02.014
- Kahathuduwa CN, Dassanayake TL, Amarakoon AMT, Weerasinghe VS. Acute effects of theanine, caffeine and theanine-caffeine combination on attention. Nutr Neurosci. 2017 Jul;20(6):369-377. doi: 10.1080/1028415X.2016.1144845
- White DJ, de Klerk S, Woods W, Gondalia S, Noonan C, Scholey AB. Anti-Stress, Behavioural and Magnetoencephalography Effects of an L-Theanine-Based Nutrient Drink: A Randomised, Double-Blind, Placebo-Controlled, Crossover Trial. Nutrients. 2016 Jan 19;8(1):53. doi: 10.3390/nu8010053
- Kim TI, Lee YK, Park SG, Choi IS, Ban JO, Park HK, Nam SY, Yun YW, Han SB, Oh KW, Hong JT. l-Theanine, an amino acid in green tea, attenuates beta-amyloid-induced cognitive dysfunction and neurotoxicity: reduction in oxidative damage and inactivation of ERK/p38 kinase and NF-kappaB pathways. Free Radic Biol Med. 2009 Dec 1;47(11):1601-10. doi: 10.1016/j.freeradbiomed.2009.09.008
- Park SK, Jung IC, Lee WK, Lee YS, Park HK, Go HJ, Kim K, Lim NK, Hong JT, Ly SY, Rho SS. A combination of green tea extract and l-theanine improves memory and attention in subjects with mild cognitive impairment: a double-blind placebo-controlled study. J Med Food. 2011 Apr;14(4):334-43. doi: 10.1089/jmf.2009.1374
- Camfield DA, Stough C, Farrimond J, Scholey AB. Acute effects of tea constituents L-theanine, caffeine, and epigallocatechin gallate on cognitive function and mood: a systematic review and meta-analysis. Nutr Rev. 2014 Aug;72(8):507-22. doi: 10.1111/nure.12120
- Owen GN, Parnell H, De Bruin EA, Rycroft JA. The combined effects of L-theanine and caffeine on cognitive performance and mood. Nutr Neurosci. 2008 Aug;11(4):193-8. doi: 10.1179/147683008X301513
- Kelly SP, Gomez-Ramirez M, Montesi JL, Foxe JJ. L-theanine and caffeine in combination affect human cognition as evidenced by oscillatory alpha-band activity and attention task performance. J Nutr. 2008 Aug;138(8):1572S-1577S. doi: 10.1093/jn/138.8.1572S
- Dodd FL, Kennedy DO, Riby LM, Haskell-Ramsay CF. A double-blind, placebo-controlled study evaluating the effects of caffeine and L-theanine both alone and in combination on cerebral blood flow, cognition and mood. Psychopharmacology (Berl). 2015 Jul;232(14):2563-76. doi: 10.1007/s00213-015-3895-0
- Nishida K, Yasuda E, Nagasawa K, Fujimoto S. Altered levels of oxidation and phospholipase C isozyme expression in the brains of theanine-administered rats. Biol Pharm Bull. 2008 May;31(5):857-60. doi: 10.1248/bpb.31.857
- Cho HS, Kim S, Lee SY, Park JA, Kim SJ, Chun HS. Protective effect of the green tea component, L-theanine on environmental toxins-induced neuronal cell death. Neurotoxicology. 2008 Jul;29(4):656-62. doi: 10.1016/j.neuro.2008.03.004
- Hartley L, Flowers N, Holmes J, Clarke A, Stranges S, Hooper L, Rees K. Green and black tea for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2013 Jun 18;2013(6):CD009934. doi: 10.1002/14651858.CD009934.pub2
- Lyon MR, Kapoor MP, Juneja LR. The effects of L-theanine (Suntheanine®) on objective sleep quality in boys with attention deficit hyperactivity disorder (ADHD): a randomized, double-blind, placebo-controlled clinical trial. Altern Med Rev. 2011 Dec;16(4):348-54.
- Rogers PJ, Smith JE, Heatherley SV, Pleydell-Pearce CW. Time for tea: mood, blood pressure and cognitive performance effects of caffeine and theanine administered alone and together. Psychopharmacology (Berl). 2008 Jan;195(4):569-77. doi: 10.1007/s00213-007-0938-1
- Siamwala JH, Dias PM, Majumder S, Joshi MK, Sinkar VP, Banerjee G, Chatterjee S. L-theanine promotes nitric oxide production in endothelial cells through eNOS phosphorylation. J Nutr Biochem. 2013 Mar;24(3):595-605. doi: 10.1016/j.jnutbio.2012.02.016
- Johnson EJ, Russell RM. Beta-Carotene. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:115-20.
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. Washington, DC: National Academy Press; 2001. https://www.nap.edu/read/10026/chapter/1
- Solomons NW. Vitamin A. In: Bowman B, Russell R, eds. Present Knowledge in Nutrition. 9th ed. Washington, DC: International Life Sciences Institute; 2006:157-83.
- Ross CA. Vitamin A. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:778-91.
- Mielech, A., Puścion-Jakubik, A., Markiewicz-Żukowska, R., & Socha, K. (2020). Vitamins in Alzheimer’s Disease-Review of the Latest Reports. Nutrients, 12(11), 3458. https://doi.org/10.3390/nu12113458
- Wołoszynowska-Fraser M.U., Kouchmeshky A., McCaffery P. Vitamin A and Retinoic Acid in Cognition and Cognitive Disease. Annu. Rev. Nutr. 2020;40:247–272. doi: 10.1146/annurev-nutr-122319-034227
- Sodhi R.K., Singh N. Retinoids as potential targets for Alzheimer’s disease. Pharmacol. Biochem. Behav. 2014;120:117–123. doi: 10.1016/j.pbb.2014.02.016
- Shahar S., Lee L.K., Rajab N., Lim C.L., Harun N.A., Noh M.F.N.M., Then S.-M., Jamal R. Association between vitamin A, vitamin E and apolipoprotein E status with mild cognitive impairment among elderly people in low-cost residential areas. Nutr. Neurosci. 2013;16:6–12. doi: 10.1179/1476830512Y.0000000013
- Yuan C., Fondell E., Ascherio A., Okereke O.I., Grodstein F., Hofman A., Willett W.C. Long-Term Intake of Dietary Carotenoids Is Positively Associated with Late-Life Subjective Cognitive Function in a Prospective Study in US Women. J. Nutr. 2020;150:1871–1879. doi: 10.1093/jn/nxaa087
- Péneau S., Galan P., Jeandel C., Ferry M., Andreeva V., Hercberg S., Kesse-Guyot E., The SUVI MAX 2 Research Group. Fruit and vegetable intake and cognitive function in the SU.VI.MAX 2 prospective study. Am. J. Clin. Nutr. 2011;94:1295–1303. doi: 10.3945/ajcn.111.014712
- Vitamin A. https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional
- Kennedy D.O., Stevenson E.J., Jackson P.A., Dunn S., Wishart K., Bieri G., Barella L., Carne A., Dodd F.L., Robertson B.C., et al. Multivitamins and minerals modulate whole-body energy metabolism and cerebral blood-flow during cognitive task performance: a double-blind, randomised, placebo-controlled trial. Nutr. Metabol. 2016;13:11. doi: 10.1186/s12986-016-0071-4
- Kennedy D.O. B Vitamins and the Brain: Mechanisms, Dose and Efficacy–A Review. Nutrients. 2016;8:68. doi: 10.3390/nu8020068
- Bryan J., Calvaresi E., Hughes D. Short-term folate, vitamin B-12 or vitamin B-6 supplementation slightly affects memory performance but not mood in women of various ages. J. Nutr. 2002;132:1345–1356. doi: 10.1093/jn/132.6.1345
- Traber MG. Vitamin E. In: Shils ME, Shike M, Ross AC, Caballero B, Cousins R, eds. Modern Nutrition in Health and Disease. 10th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2006;396-411.
- Vitamin E. https://ods.od.nih.gov/factsheets/VitaminE-HealthProfessional
- Von Arnim C.A.F., Herbolsheimer F., Nikolaus T., Peter R., Biesalski H.K., Ludolph A.C., Riepe M., Nagel G., The ActiFE Ulm Study Group Dietary Antioxidants and Dementia in a Population-Based Case-Control Study among Older People in South Germany. J. Alzheimer Dis. 2012;31:717–724. doi: 10.3233/JAD-2012-120634
- Lopes da Silva S, Vellas B, Elemans S, Luchsinger J, Kamphuis P, Yaffe K, Sijben J, Groenendijk M, Stijnen T. Plasma nutrient status of patients with Alzheimer’s disease: Systematic review and meta-analysis. Alzheimers Dement. 2014 Jul;10(4):485-502. doi: 10.1016/j.jalz.2013.05.1771
- Rijpma A, Meulenbroek O, Olde Rikkert MG. Cholinesterase inhibitors and add-on nutritional supplements in Alzheimer’s disease: a systematic review of randomized controlled trials. Ageing Res Rev. 2014 Jul;16:105-12. doi: 10.1016/j.arr.2014.06.002
- Dysken MW, Sano M, Asthana S, Vertrees JE, Pallaki M, Llorente M, Love S, Schellenberg GD, McCarten JR, Malphurs J, Prieto S, Chen P, Loreck DJ, Trapp G, Bakshi RS, Mintzer JE, Heidebrink JL, Vidal-Cardona A, Arroyo LM, Cruz AR, Zachariah S, Kowall NW, Chopra MP, Craft S, Thielke S, Turvey CL, Woodman C, Monnell KA, Gordon K, Tomaska J, Segal Y, Peduzzi PN, Guarino PD. Effect of vitamin E and memantine on functional decline in Alzheimer disease: the TEAM-AD VA cooperative randomized trial. JAMA. 2014 Jan 1;311(1):33-44. doi: 10.1001/jama.2013.282834. Erratum in: JAMA. 2014 Mar 19;311(11):1161
- Monacelli F., Acquarone F.M.E., Giannotti C., Borghi R., Nencioni A. Vitamin C, Aging and Alzheimer’s Disease. Nutrients. 2017;9:670. doi: 10.3390/nu9070670
- Choudhry F., Howlett D.R., Richardson J.C., Francis P.T., Williams R.J. Pro-oxidant diet enhances β/γ secretase-mediated APP processing in APP/PS1 transgenic mice. Neurobiol. Aging. 2012;33:960–968. doi: 10.1016/j.neurobiolaging.2010.07.008
- Li FJ, Shen L, Ji HF. Dietary intakes of vitamin E, vitamin C, and β-carotene and risk of Alzheimer’s disease: a meta-analysis. J Alzheimers Dis. 2012;31(2):253-8. doi: 10.3233/JAD-2012-120349
- Xu W, Tan L, Wang HF, Jiang T, Tan MS, Tan L, Zhao QF, Li JQ, Wang J, Yu JT. Meta-analysis of modifiable risk factors for Alzheimer’s disease. J Neurol Neurosurg Psychiatry. 2015 Dec;86(12):1299-306. doi: 10.1136/jnnp-2015-310548
- Fitzpatrick-Lewis D, Warren R, Ali MU, Sherifali D, Raina P. Treatment for mild cognitive impairment: a systematic review and meta-analysis. CMAJ Open. 2015 Dec 1;3(4):E419-27. doi: 10.9778/cmajo.20150057
- Farina N, Isaac MG, Clark AR, Rusted J, Tabet N. Vitamin E for Alzheimer’s dementia and mild cognitive impairment. Cochrane Database Syst Rev. 2012 Nov 14;11(11):CD002854. doi: 10.1002/14651858.CD002854.pub3. Update in: Cochrane Database Syst Rev. 2017 Jan 27;1:CD002854
- Kang JH, Cook NR, Manson JE, Buring JE, Albert CM, Grodstein F. Vitamin E, vitamin C, beta carotene, and cognitive function among women with or at risk of cardiovascular disease: The Women’s Antioxidant and Cardiovascular Study. Circulation. 2009 Jun 2;119(21):2772-80. doi: 10.1161/CIRCULATIONAHA.108.816900
- Fotuhi M, Zandi PP, Hayden KM, Khachaturian AS, Szekely CA, Wengreen H, Munger RG, Norton MC, Tschanz JT, Lyketsos CG, Breitner JC, Welsh-Bohmer K. Better cognitive performance in elderly taking antioxidant vitamins E and C supplements in combination with nonsteroidal anti-inflammatory drugs: the Cache County Study. Alzheimers Dement. 2008 May;4(3):223-7. doi: 10.1016/j.jalz.2008.01.004
- Agarwal P., Holland T.M., Wang Y., Holtzman D.M., Morris M.C. Association of Strawberries and Anthocyanidin Intake with Alzheimer’s Dementia Risk. Nutrients. 2019;11:3060. doi: 10.3390/nu11123060
- Bjelakovic G, Nikolova D, Gluud LL, Simonetti RG, Gluud C. Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Cochrane Database Syst Rev. 2012 Mar 14;(3):CD007176. doi: 10.1002/14651858.CD007176.pub2
- Abner EL, Schmitt FA, Mendiondo MS, Marcum JL, Kryscio RJ. Vitamin E and all-cause mortality: a meta-analysis. Curr Aging Sci. 2011 Jul;4(2):158-70. doi: 10.2174/1874609811104020158
- Kristal AR, Darke AK, Morris JS, Tangen CM, Goodman PJ, Thompson IM, Meyskens FL Jr, Goodman GE, Minasian LM, Parnes HL, Lippman SM, Klein EA. Baseline selenium status and effects of selenium and vitamin e supplementation on prostate cancer risk. J Natl Cancer Inst. 2014 Mar;106(3):djt456. doi: 10.1093/jnci/djt456
- Mangialasche F, Solomon A, Kåreholt I, Hooshmand B, Cecchetti R, Fratiglioni L, Soininen H, Laatikainen T, Mecocci P, Kivipelto M. Serum levels of vitamin E forms and risk of cognitive impairment in a Finnish cohort of older adults. Exp Gerontol. 2013 Dec;48(12):1428-35. doi: 10.1016/j.exger.2013.09.006
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids. Washington, DC: National Academy Press, 2000. https://www.nap.edu/catalog/9810/dietary-reference-intakes-for-vitamin-c-vitamin-e-selenium-and-carotenoids
- Levine M, Wang Y, Padayatty SJ, Morrow J. A new recommended dietary allowance of vitamin C for healthy young women. Proc Natl Acad Sci U S A. 2001 Aug 14;98(17):9842-6. doi: 10.1073/pnas.171318198
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academy Press, 2010.
- Anglin RE, Samaan Z, Walter SD, McDonald SD. Vitamin D deficiency and depression in adults: systematic review and meta-analysis. Br J Psychiatry. 2013 Feb;202:100-7. doi: 10.1192/bjp.bp.111.106666
- Calvo MS, Whiting SJ, Barton CN. Vitamin D fortification in the United States and Canada: current status and data needs. Am J Clin Nutr. 2004 Dec;80(6 Suppl):1710S-6S. doi: 10.1093/ajcn/80.6.1710S
- Taylor CL, Patterson KY, Roseland JM, Wise SA, Merkel JM, Pehrsson PR, Yetley EA. Including food 25-hydroxyvitamin D in intake estimates may reduce the discrepancy between dietary and serum measures of vitamin D status. J Nutr. 2014 May;144(5):654-9. doi: 10.3945/jn.113.189811
- Yetley EA. Assessing the vitamin D status of the US population. Am J Clin Nutr. 2008 Aug;88(2):558S-564S. doi: 10.1093/ajcn/88.2.558S
- Vitamin D for Milk and Milk Alternatives. https://www.fda.gov/food/food-additives-petitions/vitamin-d-milk-and-milk-alternatives
- Littlejohns TJ, Henley WE, Lang IA, Annweiler C, Beauchet O, Chaves PH, Fried L, Kestenbaum BR, Kuller LH, Langa KM, Lopez OL, Kos K, Soni M, Llewellyn DJ. Vitamin D and the risk of dementia and Alzheimer disease. Neurology. 2014 Sep 2;83(10):920-8. doi: 10.1212/WNL.0000000000000755
- Dursun E, Gezen-Ak D. Vitamin D basis of Alzheimer’s disease: from genetics to biomarkers. Hormones (Athens). 2019 Mar;18(1):7-15. doi: 10.1007/s42000-018-0086-5
- Annweiler C, Fantino B, Gautier J, Beaudenon M, Thiery S, Beauchet O. Cognitive effects of vitamin D supplementation in older outpatients visiting a memory clinic: a pre-post study. J Am Geriatr Soc. 2012 Apr;60(4):793-5. doi: 10.1111/j.1532-5415.2011.03877.x
- Rossom R.C., Espeland M.A., Manson J.E., Dysken M.W., Johnson K.C., Lane R.S., Leblanc E.S., Lederle F.A., Masaki K.H., Margolis K.L. Calcium and vitamin D supplementation and cognitive impairment in the women’s health initiative. J. Am. Geriatr. Soc. 2012;60:2197–2205. doi: 10.1111/jgs.12032
- An Evaluation of the Effect of Vitamin D Supplementation on the Cognitive Function of Older Subjects With Low Levels of This Vitamin. https://clinicaltrials.gov/ct2/show/study/NCT02381600
- Effect of Vitamin D on Cognitive Decline of Patients With Memory Complaint (D-COG). https://clinicaltrials.gov/ct2/show/study/NCT02185222
- Lifestyle Intervention Program for Cognitive Impairment. https://clinicaltrials.gov/ct2/show/study/NCT02741804
- Can Vitamin D3 Improve Cognitive Function in Individuals With Type 2 Diabetes? (THINK-D). https://clinicaltrials.gov/ct2/show/study/NCT02416193
- DO-HEALTH / Vitamin D3 – Omega3 – Home Exercise – Healthy Ageing and Longevity Trial (DO-HEALTH). https://clinicaltrials.gov/ct2/show/NCT01745263
- Vitamin D and Omega-3 Trial (VITAL). https://clinicaltrials.gov/ct2/show/NCT01169259
- A Large Randomized Trial of Vitamin D, Omega-3 Fatty Acids and Cognitive Decline (VITAL-Cog). https://clinicaltrials.gov/ct2/show/NCT01669915
- Annweiler C, Herrmann FR, Fantino B, Brugg B, Beauchet O. Effectiveness of the combination of memantine plus vitamin D on cognition in patients with Alzheimer disease: a pre-post pilot study. Cogn Behav Neurol. 2012 Sep;25(3):121-7. doi: 10.1097/WNN.0b013e31826df647
- Annweiler C, Fantino B, Parot-Schinkel E, Thiery S, Gautier J, Beauchet O. Alzheimer’s disease–input of vitamin D with mEmantine assay (AD-IDEA trial): study protocol for a randomized controlled trial. Trials. 2011 Oct 20;12:230. doi: 10.1186/1745-6215-12-230
- Suzuki M, Yoshioka M, Hashimoto M, Murakami M, Noya M, Takahashi D, Urashima M. Randomized, double-blind, placebo-controlled trial of vitamin D supplementation in Parkinson disease. Am J Clin Nutr. 2013 May;97(5):1004-13. doi: 10.3945/ajcn.112.051664
- Vitamin D. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional
- Vitamin D. https://www.mayoclinic.org/drugs-supplements-vitamin-d/art-20363792
- Limongi F., Siviero P., Bozanic A., Noale M., Veronese N., Maggi S. The Effect of Adherence to the Mediterranean Diet on Late-Life Cognitive Disorders: A Systematic Review. J. Am. Med. Dir. Assoc. 2020;21:1402–1409. doi: 10.1016/j.jamda.2020.08.020
- Grammatikopoulou M.G., Goulis D.G., Gkiouras K., Theodoridis X., Gkouskou K.K., Evangeliou A., Dardiotis E., Bogdanos D.P. To Keto or Not to Keto? A Systematic Review of Randomized Controlled Trials Assessing the Effects of Ketogenic Therapy on Alzheimer Disease. Adv. Nutr. 2020:073. doi: 10.1093/advances/nmaa073
- Masood W, Annamaraju P, Uppaluri KR. Ketogenic Diet. [Updated 2020 Dec 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499830
- Krikorian R, Shidler MD, Dangelo K, Couch SC, Benoit SC, Clegg DJ. Dietary ketosis enhances memory in mild cognitive impairment. Neurobiol Aging. 2012 Feb;33(2):425.e19-27. doi: 10.1016/j.neurobiolaging.2010.10.006
- Broom GM, Shaw IC, Rucklidge JJ. The ketogenic diet as a potential treatment and prevention strategy for Alzheimer’s disease. Nutrition. 2019 Apr;60:118-121. doi: 10.1016/j.nut.2018.10.003
- Oh R, Gilani B, Uppaluri KR. Low Carbohydrate Diet. [Updated 2021 May 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537084
- Liu Y.H., Gao X., Na M., Kris-Etherton P., Mitchell D.C., Jensen G.L. Dietary pattern, diet quality, and dementia: A systematic review and meta-analysis of prospective cohort studies. J. Alzheimer Dis. 2020;78:151–158. doi: 10.3233/JAD-200499
- Kheirouri S., Alizadeh M. Dietary Inflammatory Potential and the Risk of Neurodegenerative Diseases in Adults. Epidemiol. Rev. 2019;41:109–120. doi: 10.1093/epirev/mxz005
- Moreira S.C., Jansen A.K., Silva F.M. Dietary interventions and cognition of Alzheimer’s disease patients: A systematic review of randomized controlled trial. Dement. Neuropsychol. 2020;14:258–282. doi: 10.1590/1980-57642020dn14-030008
- Haider S., Schwarzinger A., Stefanac S., Soysal P., Smith L., Veronese N., Dorner T.E., Grabovac I. Nutrientsal supplements for neuropsychiatric symptoms in people with dementia: A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry. 2020;35:1285–1291. doi: 10.1002/gps.5407
- https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf
- The Skinny on Fats. https://www.heart.org/en/health-topics/cholesterol/prevention-and-treatment-of-high-cholesterol-hyperlipidemia/the-skinny-on-fats
- Jakobsen, M.U., et al., Intake of carbohydrates compared with intake of saturated fatty acids and risk of myocardial infarction: importance of the glycemic index. Am J Clin Nutr, 2010. 91(6): p. 1764-8.
- Institute of Medicine, Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients). Washington, DC: National Academy Press; 2005.
- Jones PJH, Rideout T. Lipids, sterols, and their metabolites. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2014.
- Jones PJH, Papamandjaris AA. Lipids: cellular metabolism. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:132-48.
- Harris WS. Omega-3 fatty acids. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:577-86.
- Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med (Maywood). 2008 Jun;233(6):674-88. doi: 10.3181/0711-MR-311
- Wang C, Chung M, Lichtenstein A, Balk E, Kupelnick B, DeVine D, et al. Effects of omega-3 fatty acids on cardiovascular disease. Summary, evidence report/technology assessment no. 94. (Prepared by the Tufts New England Medical Center Evidence-based Practice Center, Boston, MA.) AHRQ Publication No. 04-E009-1. Agency for Healthcare Research and Quality, 2004. https://archive.ahrq.gov/downloads/pub/evidence/pdf/o3cardio/o3cardio.pdf
- Harris WS, Davidson MH. RE: Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst. 2014 Apr;106(4):dju019. doi: 10.1093/jnci/dju019
- Brasky TM, Darke AK, Song X, Tangen CM, Goodman PJ, Thompson IM, Meyskens FL Jr, Goodman GE, Minasian LM, Parnes HL, Klein EA, Kristal AR. Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst. 2013 Aug 7;105(15):1132-41. doi: 10.1093/jnci/djt174
- Harris WS. Are n-3 fatty acids still cardioprotective? Curr Opin Clin Nutr Metab Care. 2013 Mar;16(2):141-9. doi: 10.1097/MCO.0b013e32835bf380
- Agency for Healthcare Research and Quality. Omega-3 fatty acids and cardiovascular disease – 2015. https://effectivehealthcare.ahrq.gov/products/fatty-acids-cardiovascular-disease/research-protocol
- Harris WS. The omega-3 index as a risk factor for coronary heart disease. Am J Clin Nutr. 2008 Jun;87(6):1997S-2002S. doi: 10.1093/ajcn/87.6.1997S
- Metcalf RG, Cleland LG, Gibson RA, Roberts-Thomson KC, Edwards JR, Sanders P, Stuklis R, James MJ, Young GD. Relation between blood and atrial fatty acids in patients undergoing cardiac bypass surgery. Am J Clin Nutr. 2010 Mar;91(3):528-34. doi: 10.3945/ajcn.2009.28302
- James M, Proudman S, Cleland L. Fish oil and rheumatoid arthritis: past, present and future. Proc Nutr Soc. 2010 Aug;69(3):316-23. doi: 10.1017/S0029665110001564
- Abdelhamid AS, Brown TJ, Brainard JS, Biswas P, Thorpe GC, Moore HJ, Deane KH, Summerbell CD, Worthington HV, Song F, Hooper L. Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2020 Feb 29;3(2):CD003177. doi: 10.1002/14651858.CD003177.pub5
- Weylandt KH, Serini S, Chen YQ, Su HM, Lim K, Cittadini A, Calviello G. Omega-3 Polyunsaturated Fatty Acids: The Way Forward in Times of Mixed Evidence. Biomed Res Int. 2015;2015:143109. doi: 10.1155/2015/143109
- Casula M, Soranna D, Catapano AL, Corrao G. Long-term effect of high dose omega-3 fatty acid supplementation for secondary prevention of cardiovascular outcomes: A meta-analysis of randomized, placebo controlled trials [corrected]. Atheroscler Suppl. 2013 Aug;14(2):243-51. doi: 10.1016/S1567-5688(13)70005-9. Erratum in: Atheroscler Suppl. 2014 Mar;233(1):122.
- Agency for Healthcare Research and Quality. Omega-3 fatty acids and cardiovascular disease: an updated systematic review. 2016. https://effectivehealthcare.ahrq.gov/products/fatty-acids-cardiovascular-disease/research
- Siscovick DS, Barringer TA, Fretts AM, Wu JH, Lichtenstein AH, Costello RB, Kris-Etherton PM, Jacobson TA, Engler MB, Alger HM, Appel LJ, Mozaffarian D; American Heart Association Nutrition Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Epidemiology and Prevention; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; and Council on Clinical Cardiology. Omega-3 Polyunsaturated Fatty Acid (Fish Oil) Supplementation and the Prevention of Clinical Cardiovascular Disease: A Science Advisory From the American Heart Association. Circulation. 2017 Apr 11;135(15):e867-e884. doi: 10.1161/CIR.0000000000000482
- National Institutes of Health. Dietary Supplement Label Database. 2015.
- U.S. Food and Drug Administration. Fish: what pregnant women and parents should know. 2014. https://www.fda.gov/food/consumers/advice-about-eating-fish
- ConsumerLab.com. Product review: fish oil and omega-3 fatty acid supplements review (including krill, algae, calamari, green-lipped mussel oil). 2021. https://www.consumerlab.com/reviews/fish-oil-supplements-review/omega3
- Stampfer MJ, Hu FB, Manson JE, Rimm EB, Willett WC. Primary prevention of coronary heart disease in women through diet and lifestyle. N Engl J Med. 2000 Jul 6;343(1):16-22. doi: 10.1056/NEJM200007063430103
- Skerrett, P. J., & Willett, W. C. (2010). Essentials of healthy eating: a guide. Journal of midwifery & women’s health, 55(6), 492–501. https://doi.org/10.1016/j.jmwh.2010.06.019
- Looker AC, Dallman PR, Carroll MD, Gunter EW, Johnson CL. Prevalence of iron deficiency in the United States. JAMA. 1997 Mar 26;277(12):973-6. doi: 10.1001/jama.1997.03540360041028
- Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. MRC Vitamin Study Research Group. Lancet. 1991 Jul 20;338(8760):131-7.
- Institute of Medicine. Dietary reference intakes: calcium, phosphorous, magnesium, vitamin D, and fluoride. National Academy Press; 1997
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. Dietary guidelines for Americans 2005. Washington, DC: U.S. Department of Agriculture; 2005.
- Stechschulte SA, Kirsner RS, Federman DG. Vitamin D: bone and beyond, rationale and recommendations for supplementation. Am J Med. 2009 Sep;122(9):793-802. doi: 10.1016/j.amjmed.2009.02.029
- Feskanich D, Singh V, Willett WC, Colditz GA. Vitamin A intake and hip fractures among postmenopausal women. JAMA. 2002 Jan 2;287(1):47-54. doi: 10.1001/jama.287.1.47





{kind=link}