What is a blood clot
Blood clots are gel-like clumps of blood. Normally, blood flows freely through veins and arteries. Blood clots are beneficial when they form in response to an injury or a cut, plugging the injured blood vessel, which stops bleeding. However, when too much clotting occurs or blood clots form inside your veins or arteries without a good reason and don’t dissolve naturally, it can cause serious complications. These blood clots can be very serious and need to be treated quickly. These blood clots may require medical attention, especially if they are in your legs or are in more critical locations, such as your lungs, heart and brain. A number of conditions can cause this type of blood clot. Staying healthy and active can help prevent them.
When a blood clot forms, it can be stationary (called a thrombosis) and block blood flow or break loose (called an embolism) and travel to various parts of the body.
There are two different types of blood clots:
- Arterial blood clots are those that form in the arteries. Once arterial clots form, they cause symptoms immediately. Because this type of clot prevents oxygen from reaching vital organs, it can cause a variety of complications like stroke, heart attack, paralysis and intense pain.
- Venous blood clots are those that form in the veins. Venous clots typically form slowly over a period of time. Symptoms of venous clots gradually become more noticeable.
Blood clots can occur in many different parts of the body, each area having different symptoms:
- Legs and arms: Symptoms of blood clots in the legs and arms vary and may include pain or cramping, swelling, tenderness, warmth to the touch and bluish- or red-colored skin. Clots that occur in larger veins are called deep vein thrombosis (DVT). Blood clots can also occur in smaller, more superficial (closer to the skin) veins.
- Heart: Common symptoms for blood clots in the heart include pain in the chest and left arm, sweating and difficulty breathing.
- Lungs: The most common symptoms include shortness of breath or difficulty breathing, chest pain and cough. Other symptoms that may or may not appear are sweating, discolored skin, swelling in the legs, irregular heartbeat and/or pulse and dizziness.
- Brain: Patients with blood clots in their brains can experience problems with their vision or speech, seizures and general weakness.
- Abdomen: Symptoms of abdominal blood clots can include severe abdominal pain, nausea, vomiting and diarrhea and/or bloody stools.
A blood clot can be life-threatening depending on the location and severity. If the clot occurs elsewhere in the body, it may cause symptoms associated with, for example, a heart attack or stroke.
Blood clots can form in, or travel to, the blood vessels in the brain, heart, kidneys, lungs, and limbs. A clot in the veins deep in the limbs is called deep vein thrombosis (DVT). DVT usually affects the deep veins of the legs. If a blood clot in a deep vein breaks off and travels through the bloodstream to the lungs and blocks blood flow, it is called a pulmonary embolism (PE). Other complications of blood clots include stroke, heart attack, kidney problems, kidney failure, and pregnancy-related problems. Treatments for blood clots include blood thinners and other medicines.
An excessive clotting disorder, also known as a hypercoagulable disorder or thrombophilia, is the tendency of some people to develop blood clots in parts of the body, such as the deep veins in the legs (called deep vein thrombosis or DVT) or the arteries of the heart (arterial thrombosis). The tendency to develop a clot may arise because of some underlying condition that develops during a person’s lifetime (acquired) or may be due to certain genes passed from parent to child (inherited).
In the U.S., as many as 900,000 people are affected by venous thromboembolism annually and about 100,000 people die each year from blood clots. Many people who develop a clot experience long-term health issues, according to the Centers for Disease Control and Prevention (CDC).
Clotting is a normal response to blood vessel or tissue injury. When there is an injury and bleeding occurs, the body stops this blood loss through a complex clotting process called hemostasis. During hemostasis, the injured blood vessel constricts to reduce blood flow, platelets adhere to the injury site and clump together to form a loose platelet plug, and the coagulation cascade is initiated. During the cascade process, the body sequentially activates coagulation factors, proteins that produce a net of fibrin threads that weave through the platelet plug and stabilize the resulting blood clot. This blood clot functions as a barrier to further blood loss, one that stays in place until the injury has healed, and eventually the clot is broken down by the body.
Usually, the body activates the clotting process, regulates its speed and volume with feedback mechanisms, and after the site has healed, breaks down the blood clot and removes it in a process called fibrinolysis. When something goes wrong with blood clot formation or breakdown, excessive blood clot formation may occur.
- Blood clot activation problems: Some conditions cause activation of the clotting process when there is no injury and no need for a blood clot to form. For example, anything that interrupts the smooth blood vessel walls, essential for unimpeded blood flow, may increase risk of blood clot formation.
- Blood clot regulation problems: Blood clot formation is carefully regulated by the body. Even as a blood clot forms to stop bleeding at the site of an injury, the body begins to activate proteins that will slow clot production, much like the brakes in a car. If blood clot production is not regulated well, excessive blood clotting may result.
- Blood clot breakdown problems: After an injury is healed, proteins are activated that break down and remove the blood clot (fibrinolysis). Dysfunction or deficiency in the breakdown proteins can cause excessive clotting.
The tendency to develop a blood clot may arise because of some underlying condition that develops during a person’s lifetime (acquired) or may be due to certain genes passed from parent to child (inherited). Acquired conditions are far more commonly the cause of clots than inherited disorders. When someone has experienced a blood clot in a vein or artery (thrombotic episode), a physical examination and thorough patient history may reveal one or more contributing factors that led to inappropriate blood clot formation.
Blood clots are rare in young, healthy people.
You’re more likely to get a blood clot if you:
- are staying in or recently left hospital – especially if you can’t move around much (like after an operation)
- are overweight
- smoke
- are using combined hormonal contraception such as the combined pill, contraceptive patch or vaginal ring
- have had a blood clot before
There are also other things that increase your risk of clots.
To reduce your risk of developing blood clots, try these tips:
- Avoid sitting for long periods. If you travel by airplane, walk the aisle periodically. For long car trips, stop and walk around frequently.
- Move. After you’ve had surgery or been on bed rest, the sooner you get up and move around, the better.
- Drink plenty of fluids when traveling. Dehydration can contribute to the development of blood clots.
- Change your lifestyle. Lose weight, lower high blood pressure, stop smoking and exercise regularly.
Blood clots can be life threatening if not treated quickly.
Symptoms of a blood clot include:
- throbbing or cramping pain, swelling, redness and warmth in a leg or arm
- sudden breathlessness, sharp chest pain (may be worse when you breathe in) and a cough or coughing up blood
Seek emergency care if you experience:
- Cough that produces bloody sputum
- A fast heartbeat
- Lightheadedness
- Difficult or painful breathing. This could be a blood clot in the lungs (pulmonary embolism), which needs to be treated immediately.
- Chest pain or tightness
- Pain extending to your shoulder, arm, back or jaw
- Sudden weakness or numbness of your face, arm or leg
- Sudden difficulty speaking or understanding speech (aphasia)
- Sudden changes in your vision
- Passing out or fainting.
Consult your doctor if you develop these signs or symptoms in an area on an arm or leg:
- Swelling
- Redness
- Pain
Blood clot causes
Blood clots form when platelets (blood components) and plasma proteins thicken, forming a semisolid mass. This process may be triggered by an injury or it can sometimes occur inside blood vessels that don’t have an obvious injury.
Once these clots form, they can travel to other parts of your body, causing harm. Factors and conditions that can cause troublesome blood clots, as well as serious conditions that are associated with blood clots, include:
- Antiphospholipid syndrome — an autoimmune disorder in which a person develops antiphospholipid antibodies such as the lupus anticoagulant or cardiolipin antibody.
- Arteriosclerosis / atherosclerosis
- Certain medications, such as oral contraceptives and hormone therapy drugs
- Deep vein thrombosis (DVT)
- Factor V Leiden
- Family history of blood clots
- Heart arrhythmias (heart rhythm problems)
- Heart attack
- Heart failure
- Obesity
- Peripheral artery disease
- Polycythemia vera
- Pregnancy
- Prolonged sitting or bed rest
- Pulmonary embolism (blood clot in an artery in the lung)
- Smoking
- Stroke
- Surgery
Risk factors developing blood clot
The risk factors for developing a venous clot are different from those for an arterial clot, and people at risk for getting one are not necessarily at risk for getting the other. Different risk factors or events can cause unnatural clotting; however, each factor may initiate clotting in a different way. There are molecules in your system that signal your body to let it know when, where, and how quickly to form a clot, and genetics plays a role in how quickly your body reacts to these signals. Certain risk factors, such as obesity, slow the flow of blood in the veins, while others, such as age, can increase the body’s natural ability to clot. Even certain medications can affect how quickly your blood clots.
Risk factors for excessive blood clotting include:
- Certain genetic disorders (see inherited conditions below)
- Atherosclerosis—the buildup of cholesterol,lipids, and calcium deposits in the walls of arteries; the deposits make the blood vessel walls less smooth, weaken them, and eventually form plaques that may rupture and lead to clots and to strokes and heart attacks.
- Diabetes
- Atrial fibrillation. Atrial fibrillation can cause blood to pool in a chamber of the heart, which can increase the risk of the blood clotting.
- Overweight, obesity, and metabolic syndrome. These conditions can contribute to atherosclerosis, which in turn can lead to excessive clotting.
- Vasculitis—inflammation of blood vessel walls may increase risk of a clot forming. Vasculitis that has healed may provide sites within blood vessels that promote formation of plaque (atherosclerosis).
- Smoking
- Staying in one position for a long time, such as being in the hospital or taking a long car or plane ride. Also known as “coach-class” syndrome, describes any situation that immobilizes someone for long periods of time, such as cramped seating during long distance travel or prolonged bed rest with an illness or hospitalization. Immobility may lead to slow or restricted blood flow (venous stasis) and an increased risk of developing a blood clot, especially in the deep veins of the legs (DVT).
- Certain cancers and cancer treatments. Cancer may cause excessive clotting for a variety of reasons: 1) tumor growth may cause external compression on a blood vessel or, in some cases, actually extend into blood vessels (for example, renal cell cancers extending into the renal veins); 2) tumor may produce substances that can initiate and/or promote clotting (e.g., a type of leukemia known as acute promyelocytic leukemia can cause DIC); 3) treatments for cancer (radiation, chemotherapy) may leave patients more susceptible to excessive clotting.
- Pregnancy or recently giving birth (postpartum)—pregnant women have high levels of platelets and clotting factors and so are at increased risk for clots.
- Immobility (including prolonged inactivity, long trips by plane or car)
- Oral contraceptives
- Trauma such as fractures or surgery—damage to blood vessels and prolonged immobilization can lead to blood clots.
- Certain surgeries
- Age (increased risk for people over age 60)
- A family history of blood clots
- Chronic inflammatory diseases
- High blood pressure
- High cholesterol
- Presence of a catheter in a central vein—disruption in the flow of blood can cause blood clots to form.
- Use of certain drugs such as:
- Hormone replacement therapy
- Oral contraceptives
- Tamoxifen
- Heparin (which can cause heparin-induced thrombocytopenia, HIT)
- An acquired deficiency of one or more of the proteins that regulate clot formation, such as protein C, protein S, or antithrombin. When the level of these proteins drops, clot formation is less well-regulated and the risk of a clot increases.
- Disseminated intravascular coagulation (DIC)—a life-threatening, acute, acquired condition that causes tiny clots throughout the body; it uses up coagulation factors at an accelerated rate, leading to both bleeding and clotting.
- Bone marrow disorders such as myeloproliferative neoplasms (MPNs)
- Paroxysmal nocturnal hemoglobinuria (PNH)—an acquired condition that can cause hemolytic anemia, bone marrow failure, kidney failure, as well as clotting, particularly in veins in the abdomen (e.g., hepatic, portal, mesenteric, splenic, renal) and in the brain (cerebral veins)
- Lupus, an autoimmune disorder
- Elevated levels of homocysteine—can be caused by a deficiency of vitamin B12
- Heart Failure— may cause slowing of blood flow (stasis)
Inherited Conditions
Certain inherited gene mutations may predispose someone to forming blood clots.
Some of the most common inherited factors contributing to blood clots include:
- Factor V Leiden mutation (Activated protein C resistance)—a mutation in the gene that makes the factor V protein; Factor V is activated normally, but it is resistant to degradation by activated protein C, which regulates the clotting process.
- Prothrombin 20210 mutation (factor II mutation)—a mutation that results in an increased amount of prothrombin (factor II) in the circulation, which is associated with an increased risk for venous blood clots
- MTHFR mutation—a mutation in this gene may predispose someone to high levels of homocysteine, which can increase the risk of excessive clotting.
Factor V Leiden or the prothrombin G20210A mutation are relatively common in the population, but it is thought that they add only a slight increase in the risk of actually developing a problem with clotting.
Some inherited conditions are relatively rare and are usually due to genetic mutations that lead to a deficiency or dysfunction in the coagulation protein that the gene produces. Examples include:
- Antithrombin (formerly known as antithrombin III)—this is a factor that helps decrease the activity of the clotting process by inhibiting factors Xa, IXa, XIa, and thrombin. Inherited deficiency of antithrombin can lead to a clot formation.
- Protein C—helps regulate the speed of the coagulation cascade by degrading activated factors V and VIII
- Protein S—a cofactor with protein C
- Elevated factor VIII levels—persistently elevated factor VIII levels that are not associated with inflammation or other acquired conditions but are associated with an increased thrombotic risk
- Dysfibrinogenemia—abnormal fibrinogen leads to fibrin that does not break down normally. Patients with dysfibrinogenemia may have bleeding or clotting complications. Dysfibrinogenemia can be inherited or acquired.
In all of these inherited disorders (except for antithrombin deficiency), people may inherit one mutated gene copy and one normal gene copy (heterozygous) or two mutated gene copies (homozygous). If someone has two mutated gene copies, the person tends to have a more severe form of the condition, and if the person is heterozygous in more than one condition, the risk of clotting tends to be additive (and sometimes the risk is multiplied). With inherited hypercoagulable disorders, the first thrombotic episode may be seen at a relatively young age (less than 50 years of age). The patient may have recurrent thrombosis, a family history of thrombosis, and blood clots in unusual sites, such as veins of the brain, liver or kidneys.
How to prevent blood clots
If you’re at a high risk of blood clots – for example, you’re in hospital – follow the advice of your care team about preventing clots.
This may involve wearing stockings that improve your blood flow or taking medicine to reduce the risk of clots (anticoagulants).
There are also things you can do to help avoid clots.
DO
- stay active – even just taking regular walks can help
- drink plenty of water to avoid dehydration – you’re more likely to get a clot if you’re dehydrated
- try to lose weight if you’re overweight
- wear flight stockings or flight socks to improve your blood flow on long flights – a pharmacist can advise you about this
DON’T
- sit for long periods without moving, if you can avoid it
- drink lots of alcohol – this can make you dehydrated
- smoke
Blood clot signs and symptoms
The first indication that someone may have a clotting disorder may be the presence of a blood clot somewhere in the body that is blocking the flow of blood through a blood vessel (thrombotic episode). The signs and symptoms that may develop depend on the location of the clot.
Symptoms of blood clots, which vary depending upon where the clot is located:
- Heart – chest heaviness or pain, discomfort in other areas of the upper body, shortness of breath, sweating, nausea, light-headedness
- Brain – weakness of the face, arms or legs, difficulty speaking, vision problems, sudden and severe headache, dizziness
- Arm or Leg – sudden or gradual pain, swelling, tenderness and warmth
- Lung – sharp chest pain, racing heart, shortness of breath, sweating, fever, coughing up blood
- Abdomen – severe abdominal pain, vomiting, diarrhea
For example, when a blood clot is present in the deep vein of a leg (DVT), one of the most common complications, signs and symptoms may include:
- Leg pain or tenderness, usually in one leg
- Leg swelling, edema
- Discoloration of the leg
If a blood clot is blocking a blood vessel in a lung (pulmonary embolism), signs and symptoms may include:
- Sudden shortness of breath, difficulty breathing
- Chest pain or discomfort that may worsen with a deep breath or coughing
- Coughing up blood
- Rapid or irregular heartbeat
- Anxiety
- Lightheadedness or feeling faint
Blood clot in leg
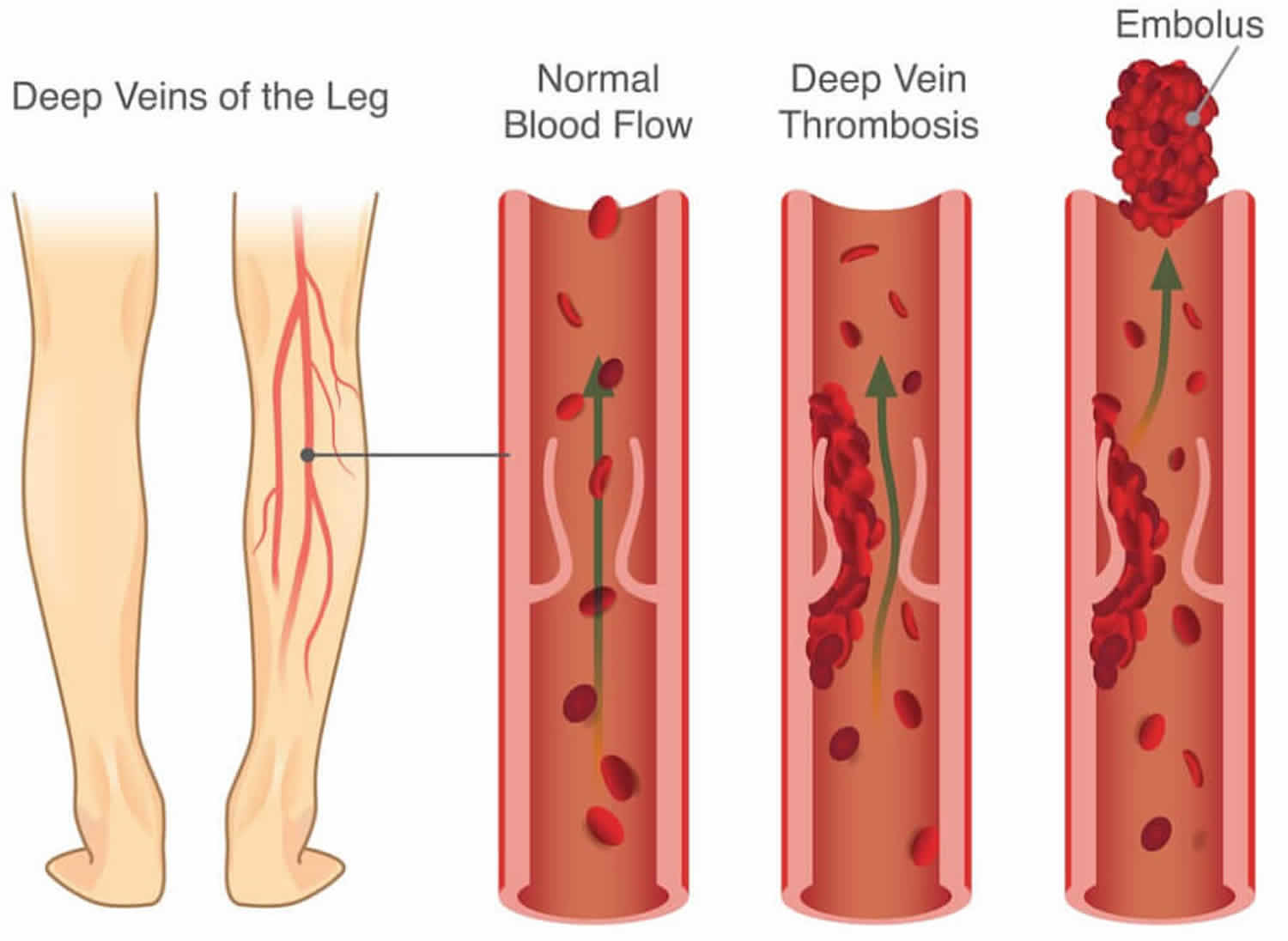
Blood clot in leg is a blood clot that develops within a deep vein in the body, usually in the leg. Deep vein thrombosis (DVT) occurs when a blood clot (thrombus) forms in one or more of the deep veins in your body, usually in your legs. Deep vein thrombosis (DVT) usually occurs in a deep leg vein, a larger vein that runs through the muscles of the calf and the thigh. Deep vein thrombosis (DVT) can cause leg pain or swelling, but also can occur with no symptoms.
Blood clot in leg can cause pain and swelling in the leg and may lead to complications such as pulmonary embolism, if a blood clot in a deep vein breaks off and travels through the bloodstream to the lungs and blocking blood flow in your lungs (see blood clot in lung below).
Deep vein thrombosis can develop if you have certain medical conditions that affect how your blood clots. It can also happen if you don’t move for a long time, such as after surgery or an accident, or when you’re confined to bed.
Figure 1. Blood clot in leg (deep vein thrombosis)

Symptoms of blood clot in leg
Deep vein thrombosis can occur without noticeable symptoms.
Blood clot in leg signs and symptoms can include:
- Swelling in the affected leg (usually your calf). Rarely, there’s swelling in both legs.
- Pain in your leg. The pain often starts in your calf and can feel like cramping or soreness.
- Red or discolored skin on the leg, particularly at the back of your leg below the knee.
- A feeling of warmth in the affected leg.
- A heavy ache in the affected area
Blood clot in leg (deep vein thrombosis) usually (although not always) affects one leg. The pain may be worse when you bend your foot upward towards your knee. If you develop signs or symptoms of deep vein thrombosis, contact your doctor.
If left untreated, about 1 in 10 people with a deep vein thrombosis (DVT) will develop a blood clot in lung (pulmonary embolism). A blood clot in lung (pulmonary embolism) is a very serious and life-threatening condition that requires immediate medical attention.
The warning signs and symptoms of a pulmonary embolism include:
- Sudden shortness of breath
- Chest pain or discomfort that worsens when you take a deep breath or when you cough
- Feeling lightheaded or dizzy, or fainting
- Rapid pulse
- Coughing up blood
- Sudden collapse
Both DVT and pulmonary embolism require urgent investigation and treatment.
Seek immediate medical attention if you have pain, swelling and tenderness in your leg, and you develop breathlessness and chest pain.
Blood clot in leg complications
A serious complication associated with deep vein thrombosis is pulmonary embolism.
Pulmonary embolism
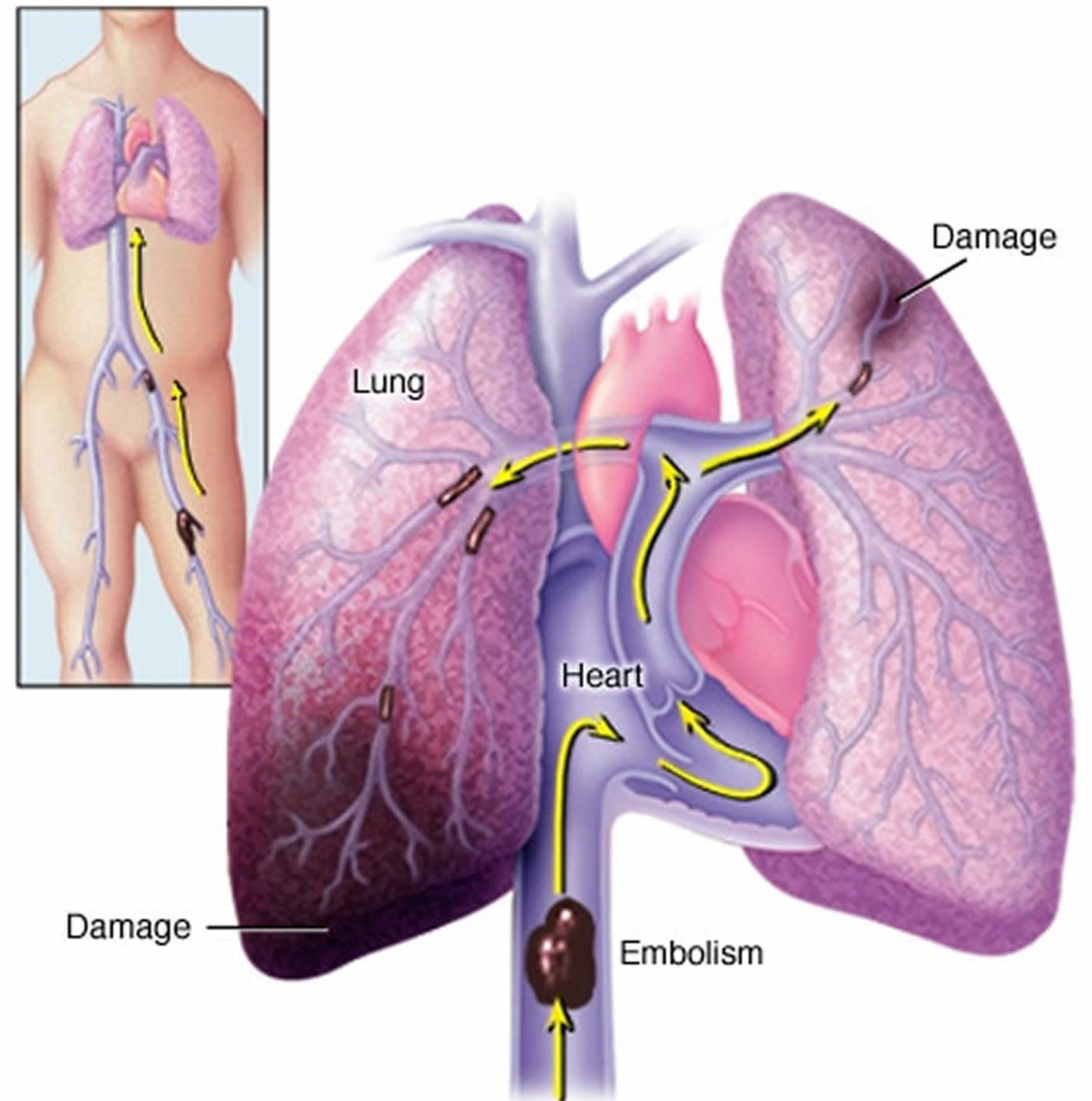
A pulmonary embolism occurs when a blood vessel in your lung becomes blocked by a blood clot (thrombus) that travels to your lung from another part of your body, usually your leg.
A pulmonary embolism can be life-threatening. It’s important to watch for signs and symptoms of a pulmonary embolism and seek medical attention if they occur. Signs and symptoms of a pulmonary embolism include:
- Sudden shortness of breath
- Chest pain or discomfort that worsens when you take a deep breath or when you cough
- Feeling lightheaded or dizzy, or fainting
- Rapid pulse
- Coughing up blood
Postphlebitic syndrome
A common complication that can occur after deep vein thrombosis is known as postphlebitic syndrome, also called post-thrombotic syndrome. This affects around 20-40% of people with a history of DVT. It’s also more likely to occur if you’re overweight or if you’ve had more than one DVT in the same leg.
If you have deep vein thrombosis (DVT), the blood clot in the vein of your calf can divert the flow of blood to other veins, causing an increase in pressure. This can affect the tissues of your calf and lead to symptoms, including:
- Persistent swelling of your legs (edema)
- Leg pain
- Skin discoloration
- Skin sores or ulcers on the calf (in severe cases)
Blood clot in leg causes
The blood clots of deep vein thrombosis can be caused by anything that prevents your blood from circulating or clotting normally, such as injury to a vein, surgery, certain medications and limited movement.
Risk factors for blood clot in leg
Many factors can increase your risk of developing deep vein thrombosis (DVT). The more you have, the greater your risk of DVT. Risk factors include:
- Inheriting a blood-clotting disorder. Some people inherit a disorder that makes their blood clot more easily. This condition on its own might not cause blood clots unless combined with one or more other risk factors.
- Prolonged bed rest, such as during a long hospital stay, or paralysis. When your legs remain still for long periods, your calf muscles don’t contract to help blood circulate, which can increase the risk of blood clots.
- Injury or surgery. Injury to your veins or surgery can increase the risk of blood clots.
- Pregnancy. Pregnancy increases the pressure in the veins in your pelvis and legs. Women with an inherited clotting disorder are especially at risk. The risk of blood clots from pregnancy can continue for up to six weeks after you have your baby.
- Birth control pills (oral contraceptives) or hormone replacement therapy. Both can increase your blood’s ability to clot.
- Being overweight or obese. Being overweight increases the pressure in the veins in your pelvis and legs.
- Smoking. Smoking affects blood clotting and circulation, which can increase your risk of DVT.
- Cancer. Some forms of cancer increase substances in your blood that cause your blood to clot. Some forms of cancer treatment also increase the risk of blood clots.
- Heart failure. This increases your risk of DVT and pulmonary embolism. Because people with heart failure have limited heart and lung function, the symptoms caused by even a small pulmonary embolism are more noticeable.
- Inflammatory bowel disease. Bowel diseases, such as Crohn’s disease or ulcerative colitis, increase the risk of DVT.
- A personal or family history of deep vein thrombosis or pulmonary embolism. If you or someone in your family has had one or both of these, you might be at greater risk of developing a DVT.
- Age. Being older than 60 increases your risk of DVT, though it can occur at any age.
- Sitting for long periods of time, such as when driving or flying. When your legs remain still for hours, your calf muscles don’t contract, which normally helps blood circulate. Blood clots can form in the calves of your legs if your calf muscles don’t move for long periods.
Blood clot in leg prevention
Measures to prevent deep vein thrombosis include:
- Avoid sitting still. If you have had surgery or have been on bed rest for other reasons, try to get moving as soon as possible. If you’re sitting for a while, don’t cross your legs, which can hamper blood flow. If you’re traveling a long distance by car, stop every hour or so and walk around.
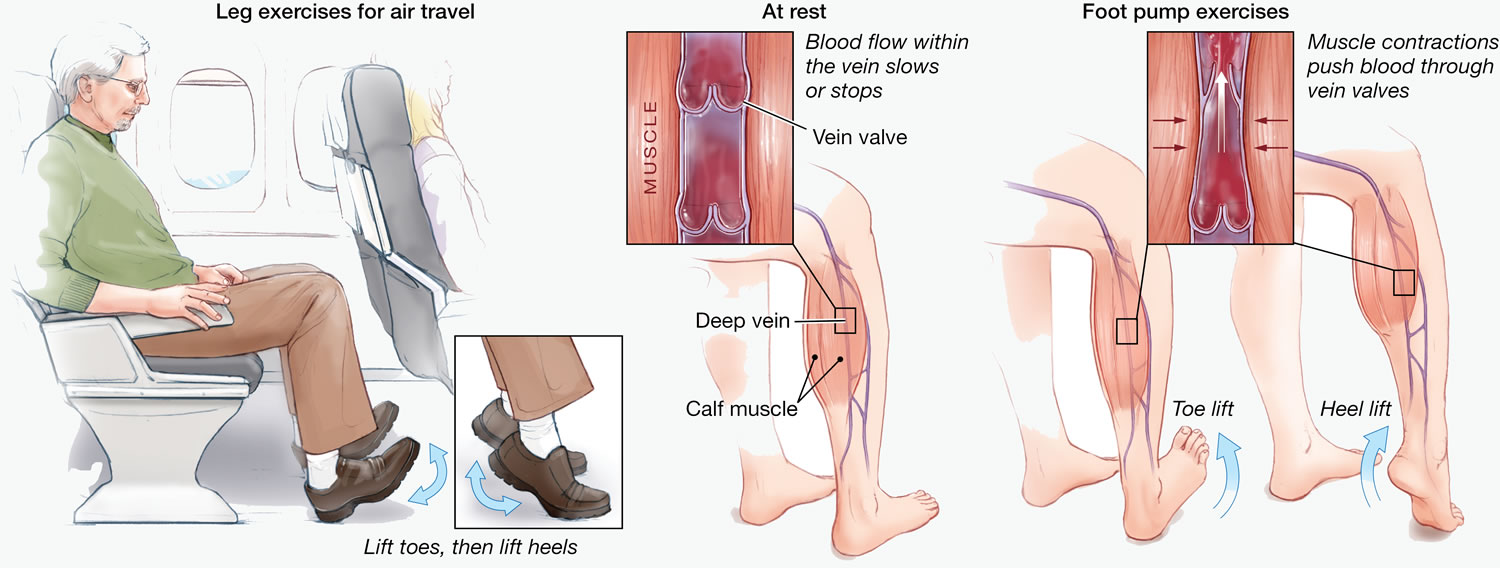
- If you’re on a plane, stand or walk occasionally. If you can’t do that, exercise your lower legs. Try raising and lowering your heels while keeping your toes on the floor, then raising your toes with your heels are on the floor.
- Make lifestyle changes. Lose weight and quit smoking.
- Exercise. Regular exercise lowers your risk of blood clots, which is especially important for people who sit a lot or travel frequently.
If you’re planning a long-distance plane, train or car journey (journeys of 6 hours or more), make sure you:
- drink plenty of water
- avoid drinking excessive amounts of alcohol because it can cause dehydration
- avoid taking sleeping pills because they can cause immobility
- perform simple leg exercises, such as regularly flexing your ankles
- take occasional short walks when possible – for example, during refuelling stopovers
- wear elastic compression stockings
While you’re in hospital
Everyone should have their risk of having a blood clot checked when they’re admitted to hospital, whatever type of treatment they’re having.
There are a number of things your healthcare team can do to help reduce your risk of getting DVT while you’re in hospital.
For example, they’ll make sure you have enough to drink so you don’t become dehydrated, and they’ll also encourage you to move around as soon as you’re able to.
Depending on your risk factors and individual circumstances, a number of different medications can be used to help prevent DVT. For example:
- anticoagulant medicines – such as dabigatran etexilate or fondaparinux sodium, which are often used to help prevent blood clots after certain types of surgery, including orthopaedic surgery
- low molecular weight heparin (LMWH) – often used in many cases to help prevent blood clots, including during and shortly after pregnancy
- unfractionated heparin (UFH) – often used in people with severe kidney impairment or established kidney failure
Compression stockings or compression devices are also commonly used to help keep the blood in your legs circulating.
Compression stockings are worn around your feet, lower legs and thighs, and fit tightly to encourage your blood to flow more quickly around your body.
Compression devices are inflatable and work in the same way as compression stockings, inflating at regular intervals to squeeze your legs and encourage blood flow.
Your healthcare team will usually advise you to walk regularly after you’ve been prescribed compression stockings. Keeping mobile can help prevent the symptoms of DVT returning and may help prevent or improve complications of DVT, such as post-thrombotic syndrome.
Figure 2. Blood clot in leg preventive exercise
Blood clot in leg diagnosis
To diagnose deep vein thrombosis, your doctor will ask you about your symptoms. You’ll also have a physical exam so that your doctor can check for areas of swelling, tenderness or discoloration on your skin. Depending on how likely you are to have a blood clot, your doctor might suggest tests, including:
- Ultrasound. A wandlike device (transducer) placed over the part of your body where there’s a clot sends sound waves into the area. As the sound waves travel through your tissue and reflect back, a computer transforms the waves into a moving image on a video screen. A clot might be visible in the image. Sometimes a series of ultrasounds are done over several days to determine whether a blood clot is growing or to check for a new one.
- Blood test. Almost all people who develop severe deep vein thrombosis have an elevated blood level of a substance called D dimer.
- Venography. A dye is injected into a large vein in your foot or ankle. An X-ray creates an image of the veins in your legs and feet, to look for clots. However, less invasive methods of diagnosis, such as ultrasound, can usually confirm the diagnosis.
- CT or MRI scans. Either can provide visual images of your veins and might show if you have a clot. Sometimes these scans performed for other reasons reveal a clot.
Blood clot in leg treatment
Deep vein thrombosis (DVT) treatment is aimed at preventing the clot from getting bigger and preventing it from breaking loose and causing a pulmonary embolism. Then the goal becomes reducing your chances of deep vein thrombosis happening again.
Deep vein thrombosis treatment options include:
Blood thinners (anticoagulants)
Deep vein thrombosis is most commonly treated with anticoagulants, also called blood thinners. These drugs, which can be injected or taken as pills, decrease your blood’s ability to clot. They don’t break up existing blood clots, but they can prevent clots from getting bigger and reduce your risk of developing more clots.
The injectable medications can be given as a shot under the skin or by injection into your arm vein (intravenous).
Heparin is typically given intravenously. Other similar blood thinners, such as enoxaparin (Lovenox), dalteparin (Fragmin) or fondaparinux (Arixtra), are injected under the skin.
You might receive an injectable blood thinner for a few days, after which pills such as warfarin (Coumadin, Jantoven) or dabigatran (Pradaxa) are started. Once warfarin has thinned your blood, the injectable blood thinners are stopped.
Other blood thinners can be given in pill form without the need for an injectable blood thinner. These include rivaroxaban (Xarelto), apixaban (Eliquis) or edoxaban (Savaysa).
You might need to take blood thinner pills for three months or longer. It’s important to take them exactly as your doctor instructs because taking too much or too little can cause serious side effects.
If you take warfarin, you’ll need periodic blood tests to check how long it takes your blood to clot. Pregnant women shouldn’t take certain blood-thinning medications.
Clot busters (thrombolytics)
If you have a more serious type of deep vein thrombosis or pulmonary embolism, or if other medications aren’t working, your doctor might prescribe drugs that break up clots quickly, called clot busters or thrombolytics.
These drugs are either given through an IV line to break up blood clots or through a catheter placed directly into the clot. These drugs can cause serious bleeding, so they’re generally reserved for severe cases of blood clots.
Filters
If you can’t take medicines to thin your blood, you might have a filter inserted into a large vein — the vena cava — in your abdomen. A vena cava filter prevents clots that break loose from lodging in your lungs.
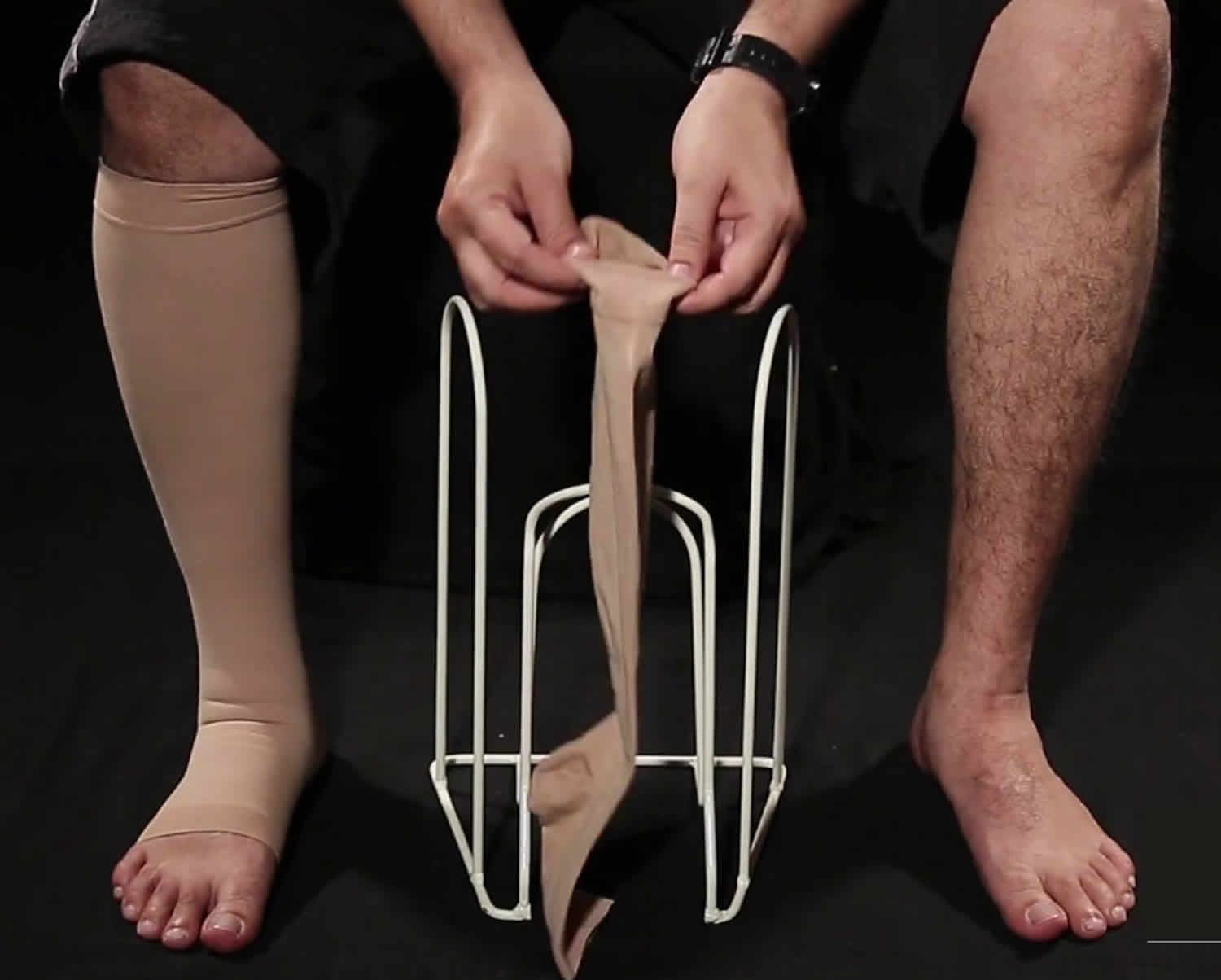
Compression stockings
To help prevent swelling associated with deep vein thrombosis, these are worn on your legs from your feet to about the level of your knees.
This pressure helps reduce the chances that your blood will pool and clot. You should wear these stockings during the day for at least two years, if possible.
Figure 3. Blood clot in leg compression stockings
Blood clot in lung
Blood clot in one of the pulmonary arteries in your lungs is also called pulmonary embolism. Blood clot in lung (pulmonary embolism) can be life-threatening if not treated quickly. Seek immediate medical attention if you experience unexplained shortness of breath, chest pain or a cough that produces bloody sputum.
In most cases, blood clot in lung (pulmonary embolism) is caused by blood clots that travel to the lungs from the legs or, rarely, other parts of the body (deep vein thrombosis or DVT). You may also have pain, redness and swelling in one of your legs (usually the calf). These are symptoms of a blood clot in your leg(s), also called deep vein thrombosis (DVT).
Because the clots block blood flow to the lungs, pulmonary embolism can be life-threatening. However, prompt treatment greatly reduces the risk of death. Taking measures to prevent blood clots in your legs will help protect you against pulmonary embolism.
Figure 4. Blood clot in lung (pulmonary embolism)
Blood clot in lung symptoms
Blood clot in lung (pulmonary embolism) symptoms can vary greatly, depending on how much of your lung is involved, the size of the clots, and whether you have underlying lung or heart disease.
Common blood clot in lung signs and symptoms include:
- Shortness of breath. This symptom typically appears suddenly and always gets worse with exertion.
- Chest pain. You may feel like you’re having a heart attack. The pain may become worse when you breathe deeply (pleurisy), cough, eat, bend or stoop. The pain will get worse with exertion but won’t go away when you rest.
- Cough. The cough may produce bloody or blood-streaked sputum.
Other signs and symptoms that can occur with pulmonary embolism include:
- Leg pain or swelling, or both, usually in the calf
- Clammy or discolored skin (cyanosis)
- Fever
- Excessive sweating
- Rapid or irregular heartbeat
- Lightheadedness or dizziness
Blood clot in lung causes
Pulmonary embolism occurs when a clump of material, most often a blood clot, gets wedged into an artery in your lungs. These blood clots most commonly come from the deep veins of your legs. This condition is known as deep vein thrombosis (DVT).
In most cases, multiple clots are involved but not necessarily all at once. The portions of lung served by each blocked artery are robbed of blood and may die. This is known as pulmonary infarction. This makes it more difficult for your lungs to provide oxygen to the rest of your body.
Occasionally, blockages in the blood vessels are caused by substances other than blood clots, such as:
- Fat from the marrow of a broken long bone
- Collagen or other tissue
- Part of a tumor
- Air bubbles
Risk factors for blood clot in lung
Although anyone can develop blood clots and subsequent pulmonary embolism, certain factors can increase your risk.
Medical history
You’re at higher risk if you or any of your family members have had venous blood clots or pulmonary embolism in the past. This may be due to inherited disorders that affect blood, making it more prone to clot.
In addition, some medical conditions and treatments put you at risk, such as:
- Heart disease. Cardiovascular disease, specifically heart failure, makes clot formation more likely.
- Cancer. Certain cancers — especially pancreatic, ovarian and lung cancers, and many cancers with metastasis — can increase levels of substances that help blood clot, and chemotherapy further increases the risk. Women with a personal or family history of breast cancer who are taking tamoxifen or raloxifene also are at higher risk of blood clots.
- Surgery. Surgery is one of the leading causes of problem blood clots. For this reason, medication to prevent clots may be given before and after major surgery such as joint replacement.
Prolonged immobility
Blood clots are more likely to form during periods of inactivity, such as:
- Bed rest. Being confined to bed for an extended period after surgery, a heart attack, leg fracture, trauma or any serious illness makes you more vulnerable to blood clots. When the lower extremities are horizontal for long periods, the flow of venous blood slows and blood can pool in the legs.
- Long trips. Sitting in a cramped position during lengthy plane or car trips slows blood flow in the legs, which contributes to the formation of clots.
Other risk factors
- Smoking. For reasons that aren’t well-understood, tobacco use predisposes some people to blood clot formation, especially when combined with other risk factors.
- Being overweight. Excess weight increases the risk of blood clots — particularly in women who smoke or have high blood pressure.
- Supplemental estrogen. The estrogen in birth control pills and in hormone replacement therapy can increase clotting factors in your blood, especially if you smoke or are overweight.
- Pregnancy. The weight of the baby pressing on veins in the pelvis can slow blood return from the legs. Clots are more likely to form when blood slows or pools.
Blood clot in lung complications
Blood clot in lung (pulmonary embolism) can be life-threatening. About one-third of people with undiagnosed and untreated pulmonary embolism don’t survive. When the condition is diagnosed and treated promptly, however, that number drops dramatically.
Pulmonary embolism can also lead to pulmonary hypertension, a condition in which the blood pressure in your lungs and in the right side of the heart is too high. When you have obstructions in the arteries inside your lungs, your heart must work harder to push blood through those vessels. This increases the blood pressure within these vessels and the right side of the heart, which can weaken your heart.
In rare cases, small emboli occur frequently and develop over time, resulting in chronic pulmonary hypertension, also known as chronic thromboembolic pulmonary hypertension.
Blood clot in lung prevention
Preventing clots in the deep veins in your legs (deep vein thrombosis) will help prevent pulmonary embolism. For this reason, most hospitals are aggressive about taking measures to prevent blood clots, including:
- Blood thinners (anticoagulants). These medications are often given to people at risk of clots before and after an operation — as well as to people admitted to the hospital with a heart attack, stroke or complications of cancer.
- Compression stockings. Compression stockings steadily squeeze your legs, helping your veins and leg muscles move blood more efficiently. They offer a safe, simple and inexpensive way to keep blood from stagnating during and after general surgery.
- Leg elevation. Elevating your legs when possible and during the night also can be very effective. Raise the bottom of your bed 4 to 6 inches with blocks or books.
- Physical activity. Moving as soon as possible after surgery can help prevent pulmonary embolism and hasten recovery overall. This is one of the main reasons your nurse may push you to get up, even on your day of surgery, and walk despite pain at the site of your surgical incision.
- Pneumatic compression. This treatment uses thigh-high or calf-high cuffs that automatically inflate with air and deflate every few minutes to massage and squeeze the veins in your legs and improve blood flow.
Prevention while traveling
The risk of blood clots developing while traveling is low, but increases as travel increases. If you have risk factors for blood clots and you’re concerned about traveling, talk with your doctor.
Your doctor might suggest the following to help prevent blood clots during travel:
- Drink plenty of fluids. Water is the best liquid for preventing dehydration, which can contribute to the development of blood clots. Avoid alcohol, which contributes to fluid loss.
- Take a break from sitting. Move around the airplane cabin once an hour or so. If you’re driving, stop every hour and walk around the car a couple of times.
- Do a few deep knee bends.
- Fidget in your seat. Flex your ankles every 15 to 30 minutes.
- Wear support stockings. Your doctor may recommend these to help promote circulation and fluid movement in your legs. Compression stockings are available in a range of stylish colors and textures. There are even devices, called stocking butlers, to help you put on the stockings.
Blood clot in lung diagnosis
Pulmonary embolism can be difficult to diagnose, especially in people who have underlying heart or lung disease. For that reason, your doctor will likely order one or more of the following tests.
Blood tests
Your doctor may order a blood test for the clot-dissolving substance D dimer. High levels may suggest an increased likelihood of blood clots, although other factors can also cause high D dimer levels.
Blood tests also can measure the amount of oxygen and carbon dioxide in your blood. A clot in a blood vessel in your lungs may lower the level of oxygen in your blood. In addition, blood tests may be done to determine whether you have an inherited clotting disorder.
Chest X-ray
This noninvasive test shows images of your heart and lungs on film. Although X-rays can’t diagnose pulmonary embolism and may even appear normal when pulmonary embolism exists, they can rule out conditions that mimic the disease.
Ultrasound
A noninvasive test known as duplex ultrasonography (sometimes called duplex scan, or compression ultrasonography) uses sound waves to check for blood clots in your thigh veins.
In this test, your doctor uses a wand-shaped device called a transducer to direct the sound waves to the veins being tested. These waves are then reflected back to the transducer and translated into a moving image by a computer. The absence of clots reduces the likelihood of DVT. If the upper thigh vessels are clear, the ultrasonography will also scan the veins behind the knee looking for residual clots. If clots are present, treatment likely will be started immediately.
Spiral CT scan
In a spiral (helical) CT scan, the scanner rotates around your body in a spiral — like the stripe on a candy cane — to create 3-D images. This type of CT can detect abnormalities within the arteries in your lungs with much greater precision than conventional CT scans. In some cases, contrast material is given intravenously during the CT scan to outline the pulmonary arteries.
Pulmonary angiogram
This test provides a clear picture of the blood flow in the arteries of your lungs. It’s the most accurate way to diagnose pulmonary embolism, but because it requires a high degree of skill to administer and has potentially serious risks, it’s usually performed when other tests fail to provide a definitive diagnosis.
In a pulmonary angiogram, a flexible tube (catheter) is inserted into a large vein — usually in your groin — and threaded through into your heart and on into the pulmonary arteries. A special dye is then injected into the catheter, and X-rays are taken as the dye travels along the arteries in your lungs.
One risk of this procedure is a temporary change in your heart rhythm. In addition, the dye may cause kidney damage in people with decreased kidney function.
MRI
MRI scans use radio waves and a powerful magnetic field to produce detailed images of internal structures. Because MRI is expensive, it’s usually reserved for pregnant women (to avoid radiation to the fetus) and people whose kidneys may be harmed by dyes used in other tests.
Blood clot in lung treatment
Treatment is aimed at keeping the blood clot from getting bigger and preventing new clots from forming. Prompt treatment is essential to prevent serious complications or death.
Medications
- Blood thinners (anticoagulants). These drugs prevent new clots from forming while your body works to break up the clots. Heparin is a frequently used anticoagulant that can be given through the vein or injected under the skin. It acts quickly and is often overlapped for several days with an oral anticoagulant, such as warfarin, until it becomes effective, which can take days. A newer class of anticoagulants, referred to as novel oral anticoagulants (NOACs), has been tested and approved for treatment of venous thromboembolism, including pulmonary embolism. These medications work quickly and have fewer interactions with other medications. Some NOACs have the advantage of being given by mouth, without the need for overlap with heparin. However, all anticoagulants have side effects, with bleeding being the most common.
- Clot dissolvers (thrombolytics). While clots usually dissolve on their own, there are medications given through the vein that can dissolve clots quickly. Because these clot-busting drugs can cause sudden and severe bleeding, they usually are reserved for life-threatening situations.
Surgical and other procedures
- Clot removal. If you have a very large, life-threatening clot in your lung, your doctor may suggest removing it via a thin, flexible tube (catheter) threaded through your blood vessels.
- Vein filter. A catheter can also be used to position a filter in the body’s main vein — called the inferior vena cava — that leads from your legs to the right side of your heart. This filter can help keep clots from being carried into your lungs. This procedure is typically reserved for people who can’t take anticoagulant drugs or when anticoagulant drugs don’t work well enough or fast enough. Some filters can be removed when they are no longer needed.
Blood clot in brain
A stroke is a serious life-threatening medical condition that occurs when the blood supply to part of your brain is cut off or reduced, depriving brain tissue of oxygen and nutrients. Within minutes, brain cells begin to die. Over 85% of all stroke cases is caused a blood clot in one of the blood vessels supplying the brain. The other 15% stroke cases is due to hemorrhage – where a weakened blood vessel supplying the brain bursts.
- A stroke is a medical emergency. Prompt treatment is crucial. Early action can minimize brain damage and potential complications.
- If you suspect that you or someone else is having a stroke, call your local emergency services number immediately and ask for an ambulance.
- The sooner a person receives treatment for a stroke, the less damage is likely to happen.
The good news is that strokes can be treated and prevented, and many fewer Americans die of stroke now than in the past.
Symptoms of blood clot in brain
The main symptoms of stroke can be remembered with the word F.A.S.T.:
- Face – the face may have dropped on one side, the person may not be able to smile, or their mouth or eye may have dropped.
- Arms – the person with suspected stroke may not be able to lift both arms and keep them there because of weakness or numbness in one arm.
- Speech – their speech may be slurred or garbled, or the person may not be able to talk at all despite appearing to be awake.
- Time – it’s time to dial your local emergency services number immediately if you see any of these signs or symptoms.
Paralysis or numbness of the face, arm or leg. You may develop sudden numbness, weakness or paralysis in your face, arm or leg. This often happens just on one side of your body. Try to raise both your arms over your head at the same time. If one arm begins to fall, you may be having a stroke. Also, one side of your mouth may droop when you try to smile.
Trouble with speaking and understanding. You may experience confusion. You may slur your words or have difficulty understanding speech.
Trouble with seeing in one or both eyes. You may suddenly have blurred or blackened vision in one or both eyes, or you may see double.
Headache. A sudden, severe headache, which may be accompanied by vomiting, dizziness or altered consciousness, may indicate you’re having a stroke.
Trouble with walking. You may stumble or experience sudden dizziness, loss of balance or loss of coordination.
Causes of stroke
Like all organs, the brain needs the oxygen and nutrients provided by blood to function properly. If the supply of blood is restricted or stopped, brain cells begin to die. This can lead to brain injury, disability and possibly death.
There are two main causes of strokes:
- Ischemic stroke – where the blood supply is stopped because of a blood clot, accounting for 85% of all cases
- Hemorrhagic stroke – where a weakened blood vessel supplying the brain bursts or leaked
Some people may experience only a temporary disruption of blood flow to the brain known as a transient ischaemic attack (TIA) that doesn’t cause permanent damage. This causes what’s known as a mini-stroke, often lasting between a few minutes and several hours. Transient ischaemic attacks (TIAs) should be treated urgently, as they’re often a warning sign you’re at risk of having a full stroke in the near future. Seek medical advice as soon as possible, even if your symptoms resolve.
Certain conditions increase the risk of having a stroke, including:
- high blood pressure (hypertension)
- high cholesterol
- atrial fibrillation
- diabetes
Ischemic stroke
About 85 percent of strokes are ischemic strokes. Ischemic strokes occur when the arteries to your brain become narrowed or blocked, causing severely reduced blood flow (ischemia). The most common ischemic strokes include:
- Thrombotic stroke. A thrombotic stroke occurs when a blood clot (thrombus) forms in one of the arteries that supply blood to your brain. A clot may be caused by fatty deposits (plaque) that build up in arteries and cause reduced blood flow (atherosclerosis) or other artery conditions.
- Embolic stroke. An embolic stroke occurs when a blood clot or other debris forms away from your brain — commonly in your heart — and is swept through your bloodstream to lodge in narrower brain arteries. This type of blood clot is called an embolus.
Hemorrhagic stroke
Hemorrhagic stroke occurs when a blood vessel in your brain leaks or ruptures. Brain hemorrhages can result from many conditions that affect your blood vessels. These include:
- Uncontrolled high blood pressure (hypertension)
- Overtreatment with anticoagulants (blood thinners)
- Weak spots in your blood vessel walls (aneurysms)
A less common cause of hemorrhage is the rupture of an abnormal tangle of thin-walled blood vessels (arteriovenous malformation). Types of hemorrhagic stroke include:
- Intracerebral hemorrhage. In an intracerebral hemorrhage, a blood vessel in the brain bursts and spills into the surrounding brain tissue, damaging brain cells. Brain cells beyond the leak are deprived of blood and are also damaged. High blood pressure, trauma, vascular malformations, use of blood-thinning medications and other conditions may cause an intracerebral hemorrhage.
- Subarachnoid hemorrhage. In a subarachnoid hemorrhage, an artery on or near the surface of your brain bursts and spills into the space between the surface of your brain and your skull. This bleeding is often signaled by a sudden, severe headache.
A subarachnoid hemorrhage is commonly caused by the bursting of a small sack-shaped or berry-shaped aneurysm. After the hemorrhage, the blood vessels in your brain may widen and narrow erratically (vasospasm), causing brain cell damage by further limiting blood flow.
Transient ischemic attack (TIA)
A transient ischemic attack (TIA) — sometimes known as a ministroke — is a temporary period of symptoms similar to those you’d have in a stroke. A temporary decrease in blood supply to part of your brain causes TIAs, which may last as little as five minutes.
Like an ischemic stroke, a TIA occurs when a clot or debris blocks blood flow to part of your nervous system — but there is no permanent tissue damage and no lasting symptoms.
Seek emergency care even if your symptoms seem to clear up. Having a TIA puts you at greater risk of having a full-blown stroke, causing permanent damage later. If you’ve had a TIA, it means there’s likely a partially blocked or narrowed artery leading to your brain or a clot source in the heart.
It’s not possible to tell if you’re having a stroke or a TIA based only on your symptoms. Even when symptoms last for under an hour, there is still a risk of permanent tissue damage.
Risk factors for stroke
Many factors can increase your stroke risk. Some factors can also increase your chances of having a heart attack. Potentially treatable stroke risk factors include:
- Lifestyle risk factors
- Being overweight or obese
- Physical inactivity
- Heavy or binge drinking
- Use of illicit drugs such as cocaine and methamphetamines
- Medical risk factors
- Blood pressure readings higher than 120/80 millimeters of mercury (mm Hg)
- Cigarette smoking or exposure to secondhand smoke
- High cholesterol
- Diabetes
- Obstructive sleep apnea
- Cardiovascular disease, including heart failure, heart defects, heart infection or abnormal heart rhythm
- Personal or family history of stroke, heart attack or transient ischemic attack.
- Other factors associated with a higher risk of stroke include:
- Age —People age 55 or older have a higher risk of stroke than do younger people.
- Race — African-Americans have a higher risk of stroke than do people of other races.
- Sex — Men have a higher risk of stroke than women. Women are usually older when they have strokes, and they’re more likely to die of strokes than are men.
- Hormones — use of birth control pills or hormone therapies that include estrogen, as well as increased estrogen levels from pregnancy and childbirth.
Stroke complications
A stroke can sometimes cause temporary or permanent disabilities, depending on how long the brain lacks blood flow and which part was affected. Complications may include:
- Paralysis or loss of muscle movement. You may become paralyzed on one side of your body, or lose control of certain muscles, such as those on one side of your face or one arm. Physical therapy may help you return to activities affected by paralysis, such as walking, eating and dressing.
- Difficulty talking or swallowing. A stroke might affect control of the muscles in your mouth and throat, making it difficult for you to talk clearly (dysarthria), swallow (dysphagia) or eat. You also may have difficulty with language (aphasia), including speaking or understanding speech, reading, or writing. Therapy with a speech-language pathologist might help.
- Memory loss or thinking difficulties. Many people who have had strokes experience some memory loss. Others may have difficulty thinking, making judgments, reasoning and understanding concepts.
- Emotional problems. People who have had strokes may have more difficulty controlling their emotions, or they may develop depression.
- Pain. Pain, numbness or other strange sensations may occur in the parts of the body affected by stroke. For example, if a stroke causes you to lose feeling in your left arm, you may develop an uncomfortable tingling sensation in that arm. People also may be sensitive to temperature changes, especially extreme cold, after a stroke. This complication is known as central stroke pain or central pain syndrome. This condition generally develops several weeks after a stroke, and it may improve over time. But because the pain is caused by a problem in your brain, rather than a physical injury, there are few treatments.
- Changes in behavior and self-care ability. People who have had strokes may become more withdrawn and less social or more impulsive. They may need help with grooming and daily chores.
As with any brain injury, the success of treating these complications varies from person to person.
Stroke prevention
Knowing your stroke risk factors, following your doctor’s recommendations and adopting a healthy lifestyle are the best steps you can take to prevent a stroke. If you’ve had a stroke or a transient ischemic attack (TIA), these measures might help prevent another stroke. The follow-up care you receive in the hospital and afterward also may play a role as well.
Many stroke prevention strategies are the same as strategies to prevent heart disease. In general, healthy lifestyle recommendations include:
- Controlling high blood pressure (hypertension). This is one of the most important things you can do to reduce your stroke risk. If you’ve had a stroke, lowering your blood pressure can help prevent a subsequent TIA or stroke. Exercising, managing stress, maintaining a healthy weight and limiting the amount of sodium and alcohol you eat and drink can all help to keep high blood pressure in check. In addition to recommending lifestyle changes, your doctor may prescribe medications to treat high blood pressure.
- Lowering the amount of cholesterol and saturated fat in your diet. Eating less cholesterol and fat, especially saturated fat and trans fats, may reduce the plaque in your arteries. If you can’t control your cholesterol through dietary changes alone, your doctor may prescribe a cholesterol-lowering medication.
- Quitting tobacco use. Smoking raises the risk of stroke for smokers and nonsmokers exposed to secondhand smoke. Quitting tobacco use reduces your risk of stroke.
- Controlling diabetes. You can manage diabetes with diet, exercise, weight control and medication.
- Maintaining a healthy weight. Being overweight contributes to other stroke risk factors, such as high blood pressure, cardiovascular disease and diabetes. Losing as little as 10 pounds may lower your blood pressure and improve your cholesterol levels.
- Eating a diet rich in fruits and vegetables. A diet containing five or more daily servings of fruits or vegetables may reduce your risk of stroke. Following the Mediterranean diet, which emphasizes olive oil, fruit, nuts, vegetables and whole grains, may be helpful.
- Exercising regularly. Aerobic or “cardio” exercise reduces your risk of stroke in many ways. Exercise can lower your blood pressure, increase your level of high-density lipoprotein cholesterol, and improve the overall health of your blood vessels and heart. It also helps you lose weight, control diabetes and reduce stress. Gradually work up to 30 minutes of activity — such as walking, jogging, swimming or bicycling — on most, if not all, days of the week.
- Drinking alcohol in moderation, if at all. Alcohol can be both a risk factor and a protective measure for stroke. Heavy alcohol consumption increases your risk of high blood pressure, ischemic strokes and hemorrhagic strokes. However, drinking small to moderate amounts of alcohol, such as one drink a day, may help prevent ischemic stroke and decrease your blood’s clotting tendency. Alcohol may also interact with other drugs you’re taking. Talk to your doctor about what’s appropriate for you.
- Treating obstructive sleep apnea (OSA). Your doctor may recommend an overnight oxygen assessment to screen for OSA — a sleep disorder in which the oxygen level intermittently drops during the night. Treatment for OSA includes oxygen at night or wearing a small device in your mouth to help you breathe.
- Avoiding illegal drugs. Certain street drugs, such as cocaine and methamphetamines, are established risk factors for a TIA or a stroke. Cocaine reduces blood flow and can narrow the arteries.
Preventive medications
If you’ve had an ischemic stroke or TIA, your doctor may recommend medications to help reduce your risk of having another stroke. These include:
- Anti-platelet drugs. Platelets are cells in your blood that form clots. Anti-platelet drugs make these cells less sticky and less likely to clot. The most commonly used anti-platelet medication is aspirin. Your doctor can help you determine the right dose of aspirin for you. Your doctor might also consider prescribing Aggrenox, a combination of low-dose aspirin and the anti-platelet drug dipyridamole to reduce the risk of blood clotting. If aspirin doesn’t prevent your TIA or stroke, or if you can’t take aspirin, your doctor may instead prescribe an anti-platelet drug such as clopidogrel (Plavix).
- Anticoagulants. These drugs, which include heparin and warfarin (Coumadin, Jantoven), reduce blood clotting. Heparin is fast acting and may be used over a short period of time in the hospital. Slower acting warfarin may be used over a longer term. Warfarin is a powerful blood-thinning drug, so you’ll need to take it exactly as directed and watch for side effects. Your doctor may prescribe these drugs if you have certain blood-clotting disorders, certain arterial abnormalities, an abnormal heart rhythm or other heart problems. Other newer blood thinners may be used if your TIA or stroke was caused by an abnormal heart rhythm.
Stroke diagnosis
To determine the most appropriate treatment for your stroke, your emergency team needs to evaluate the type of stroke you’re having and the areas of your brain affected by the stroke. They also need to rule out other possible causes of your symptoms, such as a brain tumor or a drug reaction. Your doctor may use several tests to determine your risk of stroke, including:
- Physical examination. Your doctor will ask you or a family member what symptoms you’ve been having, when they started and what you were doing when they began. Your doctor then will evaluate whether these symptoms are still present. Your doctor will want to know what medications you take and whether you have experienced any head injuries. You’ll be asked about your personal and family history of heart disease, transient ischemic attack and stroke. Your doctor will check your blood pressure and use a stethoscope to listen to your heart and to listen for a whooshing sound (bruit) over your neck (carotid) arteries, which may indicate atherosclerosis. Your doctor may also use an ophthalmoscope to check for signs of tiny cholesterol crystals or clots in the blood vessels at the back of your eyes.
- Blood tests. You may have several blood tests, which tell your care team how fast your blood clots, whether your blood sugar is abnormally high or low, whether critical blood chemicals are out of balance, or whether you may have an infection. Managing your blood’s clotting time and levels of sugar and other key chemicals will be part of your stroke care.
- Computerized tomography (CT) scan. A CT scan uses a series of X-rays to create a detailed image of your brain. A CT scan can show a hemorrhage, tumor, stroke and other conditions. Doctors may inject a dye into your bloodstream to view your blood vessels in your neck and brain in greater detail (computerized tomography angiography). There are different types of CT scans that your doctor may use depending on your situation.
- Magnetic resonance imaging (MRI). An MRI uses powerful radio waves and magnets to create a detailed view of your brain. An MRI can detect brain tissue damaged by an ischemic stroke and brain hemorrhages. Your doctor may inject a dye into a blood vessel to view the arteries and veins and highlight blood flow (magnetic resonance angiography, or magnetic resonance venography).
- Carotid ultrasound. In this test, sound waves create detailed images of the inside of the carotid arteries in your neck. This test shows buildup of fatty deposits (plaques) and blood flow in your carotid arteries.
- Cerebral angiogram. In this test, your doctor inserts a thin, flexible tube (catheter) through a small incision, usually in your groin, and guides it through your major arteries and into your carotid or vertebral artery. Then your doctor injects a dye into your blood vessels to make them visible under X-ray imaging. This procedure gives a detailed view of arteries in your brain and neck.
- Echocardiogram. An echocardiogram uses sound waves to create detailed images of your heart. An echocardiogram can find a source of clots in your heart that may have traveled from your heart to your brain and caused your stroke. You may have a transesophageal echocardiogram (TEE). In this test, your doctor inserts a flexible tube with a small device (transducer) attached into your throat and down into the tube that connects the back of your mouth to your stomach (esophagus). Because your esophagus is directly behind your heart, a transesophageal echocardiogram can create clear, detailed ultrasound images of your heart and any blood clots.
Treating a stroke
Treatment depends on the type of stroke you have, including which part of the brain was affected and what caused it.
Emergency treatment for stroke depends on whether you’re having an ischemic stroke blocking an artery — the most common kind — or a hemorrhagic stroke that involves bleeding into the brain.
Strokes are usually treated with medication. This includes medicines to prevent and dissolve blood clots, reduce blood pressure and reduce cholesterol levels.
In some cases, procedures may be required to remove blood clots. Surgery may also be required to treat brain swelling and reduce the risk of further bleeding in cases of hemorrhagic strokes.
Ischemic stroke
To treat an ischemic stroke, doctors must quickly restore blood flow to your brain.
Emergency treatment with medications
Therapy with clot-busting drugs must start within 4.5 hours if they are given into the vein — and the sooner, the better. Quick treatment not only improves your chances of survival but also may reduce complications. You may be given:
- Intravenous injection of tissue plasminogen activator (tPA). This injection of recombinant tissue plasminogen activator (tPA), also called alteplase, is considered the gold standard treatment for ischemic stroke. An injection of tPA is usually given through a vein in the arm. This potent clot-busting drug ideally is given within three hours. In some instances, tPA can be given up to 4.5 hours after stroke symptoms begin. This drug restores blood flow by dissolving the blood clot causing your stroke, and it may help people who have had strokes recover more fully. Your doctor will consider certain risks, such as potential bleeding in the brain, to determine if tPA is appropriate for you.
Emergency endovascular procedures
Doctors sometimes treat ischemic strokes with procedures performed directly inside the blocked blood vessel. These procedures must be performed as soon as possible, depending on features of the blood clot:
- Medications delivered directly to the brain. Doctors may insert a long, thin tube (catheter) through an artery in your groin and thread it to your brain to deliver tPA directly into the area where the stroke is occurring. This is called intra-arterial thrombolysis. The time window for this treatment is somewhat longer than for intravenous tPA, but is still limited.
- Removing the clot with a stent retriever. Doctors may use a catheter to maneuver a device into the blocked blood vessel in your brain and trap and remove the clot. This procedure is particularly beneficial for people with large clots that can’t be completely dissolved with tPA, though this procedure is often performed in combination with intravenous tPA.
Several large and recent studies suggest that, depending on the location of the clot and other factors, endovascular therapy might be the most effective treatment. Endovascular therapy has been shown to significantly improve outcomes and reduce long-term disability after ischemic stroke.
Other procedures
To decrease your risk of having another stroke or transient ischemic attack, your doctor may recommend a procedure to open up an artery that’s narrowed by plaque. Doctors sometimes recommend the following procedures to prevent a stroke. Options will vary depending on your situation:
- Carotid endarterectomy. In a carotid endarterectomy, a surgeon removes plaques from arteries that run along each side of your neck to your brain (carotid arteries). In this procedure, your surgeon makes an incision along the front of your neck, opens your carotid artery and removes plaque that blocks the carotid artery. Your surgeon then repairs the artery with stitches or a patch made from a vein or artificial material (graft). The procedure may reduce your risk of ischemic stroke. However, a carotid endarterectomy also involves risks, especially for people with heart disease or other medical conditions.
- Angioplasty and stents. In an angioplasty, a surgeon usually accesses your carotid arteries through an artery in your groin. Here, your surgeon can gently and safely navigate to the carotid arteries in your neck. A balloon is then inflated to expand the narrowed artery. Then a stent can be inserted to support the opened artery.
Hemorrhagic strokes
As with ischemic strokes, some people who have had a hemorrhagic stroke will also be offered medication to lower their blood pressure and prevent further strokes.
If you were taking anticoagulants before you had your stroke, you may also need treatment to reverse the effects of the medication and reduce your risk of further bleeding.
Surgery
Occasionally, emergency surgery may be needed to remove any blood from the brain and repair any burst blood vessels. This is usually done using a surgical procedure known as a craniotomy.
During a craniotomy, a section of the skull is cut away to allow the surgeon access to the cause of the bleeding. The surgeon will repair any damaged blood vessels and ensure there are no blood clots present that may restrict the blood flow to the brain.
After the bleeding has been stopped, the piece of bone removed from the skull is replaced, often by an artificial metal plate.
Surgery for hydrocephalus
Surgery can also be carried out to treat a complication of haemorrhagic strokes called hydrocephalus.
This is where damage resulting from a stroke causes cerebrospinal fluid to build up in the cavities (ventricles) of the brain, causing symptoms such as headaches, sickness, drowsiness, vomiting and loss of balance.
Hydrocephalus can be treated by surgically placing an artificial tube called a shunt into the brain to allow the fluid to drain properly.
Stroke recovery and rehabilitation
After emergency treatment, stroke care focuses on helping you recover as much function as possible and return to independent living. The impact of your stroke depends on the area of the brain involved and the amount of tissue damaged.
If your stroke affected the right side of your brain, your movement and sensation on the left side of your body may be affected. If your stroke damaged the brain tissue on the left side of your brain, your movement and sensation on the right side of your body may be affected. Brain damage to the left side of your brain may cause speech and language disorders.
In addition, if you’ve had a stroke, you may have problems with breathing, swallowing, balancing and vision.
Most stroke survivors receive treatment in a rehabilitation program. Your doctor will recommend the most rigorous therapy program you can handle based on your age, overall health and degree of disability from your stroke. Your doctor will take into consideration your lifestyle, interests and priorities, and the availability of family members or other caregivers.
Your rehabilitation program may begin before you leave the hospital. After discharge, you might continue your program in a rehabilitation unit of the same hospital, another rehabilitation unit or skilled nursing facility, an outpatient unit, or your home.
Every person’s stroke recovery is different. Depending on your condition, your treatment team may include:
- Doctor trained in brain conditions (neurologist)
- Rehabilitation doctor (physiatrist)
- Nurse
- Dietitian
- Physical therapist
- Occupational therapist
- Recreational therapist
- Speech pathologist
- Social worker
- Case manager
- Psychologist or psychiatrist
- Chaplain
How do you know if you have a blood clot?
What blood clot feels like or your symptoms differ depending on the location and type of your blood clot. Your doctor will usually begin by asking you about your symptoms and obtain your medical history, as this may provide information about factors that caused the clot. Your doctor will also perform a physical examination. In an emergency situation where patients may be unable to describe their symptoms, doctors may send patients for testing immediately after a physical examination.
Blood clot diagnosis
Your doctor will investigate the underlying cause of the clotting (thrombotic) episode and will try to determine your risk of recurrent blood clots. Your doctor may do an extensive workup to find a cause if you have repeated thrombotic episodes and/or if you’re young (less than 50 years old) and/or if the blood clot occurs in an unusual site in the body.
Initial testing is usually performed to determine if a person has or has had a blood clot (thrombotic episode) and, if so, to help determine the person’s risk of a repeat thrombotic episode. Although it may be fairly simple to identify that a person has a clot, identification of the underlying cause may take more time and effort. This is because several of the diagnostic tests that need to be done are affected by an existing or recent blood clot and by any blood-thinning (anticoagulant) therapy that is given.
Often, the healthcare practitioner may have to order a few tests and treat the person’s existing blood clot first. Several weeks or months later, when the person is able to come off of anticoagulant therapy, the the healthcare practitioner can order other tests to finish the evaluation of the cause of the clotting. Follow-up testing is important in helping to determine a person’s risk of developing recurrent blood clots.
Imaging Tests
One or more of the following imaging studies may be used to detect the presence of a blood clot and/or examine blood vessels:
- Venous ultrasound: This test is usually the first step for confirming a venous blood clot. Sound waves are used to create a view of your veins. A Doppler ultrasound may be used to help visualize blood flow through your veins. If the results of the ultrasound are inconclusive, venography or MR angiography may be used.
- Venogram. A venogram may be used if the results of a D-dimer test and ultrasound scan can’t confirm a diagnosis of DVT (deep vein thrombosis). During a venogram, a liquid called a contrast dye is injected into a vein in your foot. The dye travels up the leg and can be detected by X-ray, which will highlight a gap in the blood vessel where a clot is stopping the flow of blood.
- CT Angiography of the chest: If your doctor suspects you have a pulmonary embolism, you may undergo a CT angiography scan. The most common cause of a pulmonary embolism is a fragment from a leg or pelvic clot that has broken off and traveled through the veins to the lung. You may be sent for a chest x-ray if your doctor believes you may have a condition other than a blood clot.
- CT angiography of the abdomen and pelvis: This type of CT scan may be used if your doctor suspects a blood clot somewhere in your abdomen or pelvis. It may also be used to rule out other conditions that cause the same symptoms as blood clots.
- CT angiography of the head and neck: If you are exhibiting the symptoms of a stroke, your doctor will order an emergency CT scan of the head in order to confirm the presence of a clot. In some cases, your doctor may order a cerebral angiography exam. A carotid ultrasound could also be performed to see if a fragment from a blood clot in your neck has traveled to your brain.
- Magnetic resonance imaging (MRI).
Blood clots may cause symptoms that mimic other diseases or conditions. You may undergo additional testing to rule out other conditions.
Laboratory tests
Routine laboratory tests include:
- Routine coagulation tests:
- Partial Thromboplastin Time (PTT, aPTT),
- Prothrombin Time (PT),
- Fibrinogen
- D-dimer: D-dimer is one of the protein fragments produced when a blood clot gets dissolved in the body. It is normally undetectable or detectable at a very low level unless the body is forming and breaking down blood clots. Then, its level in the blood can significantly rise. This test detects D-dimer in the blood.
As to other tests, the following general guide is used to determine what tests should be performed based on patient age and personal and family history.
- If a person has a first episode of venous thrombosis at an age younger than 50, or has a history of recurrent clotting episodes, or has a parent, sibling or child (first-degree relative) with documented thromboembolism at age younger than 50, then a test panel is often performed, including factor V Leiden mutation and prothrombin gene G20210A mutation, antiphospholipid antibodies (including lupus anticoagulant work-up), homocysteine, protein C, protein S and antithrombin. If results of these tests are not revealing, additional tests may be needed to rule out rare causes of clotting disorders.
- If a person has a first episode of venous thrombosis at an age older than 50 without known acquired risk factors and there is no personal or family history of recurrent episodes, then a limited test panel is often performed, including factor V Leiden mutation and prothrombin gene G20210A mutation, antiphospholipid antibodies (including lupus anticoagulant) and homocysteine.
The table below lists some of the tests in alphabetical order. Not all of the tests listed in the table are needed for each person with excessive clotting disorders. If somebody has been diagnosed as having a blood clot in a vein (venous thrombosis), the first step is to rule out obvious acquired causes, such as major surgery (e.g., orthopedic), trauma, immobilization, congestive heart failure, cancer, myeloproliferative neoplasms, or nephrotic syndrome.
Table 1. Laboratory Tests for Excessive Blood Clotting
| Test | Description | Ordered When/To | Abnormal Results May Indicate |
|---|---|---|---|
| Anticardiolipin antibodies (Includes cardiolipin antibody, beta-2 glycoprotein antibody, and lupus anticoagulant) | Detects the presence of one or more of these antibodies | To evaluate recurrent blood clots and/or miscarriages | Antiphospholipid syndrome |
| Antithrombin Activity | Measures the activity of antithrombin | To evaluate someone for recurrent blood clots; to detect acquired or inherited deficiency | Low activity may increase risk of clots. |
| Antithrombin Antigen | Measures quantity of antithrombin | When results from the test for activity are consistently low | Decreased production or increased use of factor; may increase thrombotic risk. |
| D-dimer | Detects or measures the level of a specific type of fibrin degradation product | Used to detect and evaluate for the presence of a blood clot | If elevated, indicates recent clotting activity; may be due to condition such as a thromboembolism or DIC (disseminated intravascular coagulation). |
| Factor V Leiden mutation (may include activated protein C resistance testing) | Identifies a genetic mutation that results in formation of an activated Factor V that resists degradation by activated protein C | When an inherited risk factor is suspected as a cause of a blood clot | The presence of the mutation increases the risk of thrombosis. |
| Fibrinogen | Tests measure the function and the amount of fibrinogen | As part of an evaluation for a clotting disorder | If low, may indicate decreased production or increased use; may be elevated with inflammation; it is an acute phase reactant. |
| Flow cytometry | Presence of certain surface proteins on blood red cells and white cells | When paroxysmal nocturnal hemoglobinuria (PNH) is suspected | Increased risk of venous thrombosis (abdominal and cerebral veins) |
| Homocysteine | Measures the level in blood | To determine a cause of recurrent blood clots | If elevated, increased cardiac risk and risk of thrombosis. |
| Lupus Anticoagulant (LA) (Panel of tests may include LA-sensitive PTT, Dilute Russell Viper Venom Test (DRVVT), and/or Platelet Neutralization Procedure (PNP)) | Panel of tests used to check for Lupus anticoagulant | To evaluate someone with recurrent blood clots and/or miscarriages; when results of the PTT are prolonged | When PTT or LA sensitive PTT and DRVVT are prolonged, it suggests LA, usually confirmed with additional testing; if present, increased risk of thrombosis. |
| Methylenetetrahydrofolate Reductase (MTHFR) | Identifies genetic mutation | Used when the homocysteine level is elevated with no clear acquired etiology | Presence of the mutation confers an increased risk for developing elevated homocysteine levels. |
| Protein C Activity | Function of protein C | To evaluate someone for recurrent blood clots; may be acquired or inherited deficiency or dysfunction | Protein C helps regulate blood clot formation by degrading activated Factors V and VIII. If activity is low, there is an increased risk of thrombosis. |
| Protein C Antigen | Quantity of protein C | Tested when protein C activity is low. | If decreased, may be due to inherited or acquired condition; increased risk of thrombosis. |
| Protein S Activity | Function of protein S | As part of an evaluation of recurrent blood clots; may be acquired or inherited deficiency or dysfunction | Protein S is a cofactor that helps protein C regulate clot formation. Low activity may increase risk of excess clotting. |
| Protein S Antigen (free and total) | Quantity of total and free protein S | Tested when protein S activity is low. | Only free protein S is available to assist protein C; total protein S includes free protein S and inactive bound protein S. If low, increases risk of clotting. |
| Prothrombin 20210 mutation | Detects inherited genetic mutation | When a person has recurrent blood clots and an inherited risk factor is suspected | If present, increases risk of thrombosis. |
| PTT (Partial Thromboplastin Time) | Measures the time it takes for a clot to form in a blood sample after reagents are added | As part of an initial workup; screens for lupus anticoagulant; also used to monitor anticoagulant therapy | A prolonged PTT suggests need for further tests; may indicate nonspecific inhibitor (such as lupus anticoagulant). |
Blood clot treatment
Blood clots are treated differently depending on the location of the clot and your health. If you are experiencing symptoms and suspect you may have a blood clot, see a doctor immediately.
There have been many research advances that have improved the prevention and treatment of blood clots. Some current treatments include:
- Anticoagulants – medicine that prevents clots from forming
- Thrombolytics – medicine that dissolves blood clots
- Catheter-directed thrombolysis – a procedure in which a long tube, called a catheter, is surgically inserted and directed toward the blood clot where it delivers clot-dissolving medication
- Thrombectomy – surgical removal of a clot.
Arterial clots:
People diagnosed with arterial disease who are at risk for developing a clot in their arteries may have several doctors involved in their care, including a cardiologist (a doctor who specializes in conditions of the heart), a neurologist, and possibly a hematologist.
Your doctor may recommend that you undergo catheter-directed thrombolysis, a procedure that delivers “clot busting” drugs to the site of the clot, or have surgery to remove the clot. These treatments are meant to manage clots aggressively since arterial clots can block blood flow to vital organs. They are typically only used in life-threatening or emergency cases.
Venous clots:
If you are diagnosed with a venous clot, your doctor may refer you to a hematologist, a doctor who specializes in treating blood diseases.
If you are diagnosed with a deep venous clot, you will be put on blood thinning medication to help thin your blood and allow it to pass more easily past the site of the clot.
Your doctor may ask you to undergo a procedure called inferior vena cava filter placement. This is recommended for patients who are at high risk for blood clots. A filter is placed into your vein to help prevent blood clot fragments from traveling through the veins to the heart or lungs.





{kind=link}