
What is brachial plexopathy
Brachial plexopathy is a form of peripheral neuropathy that occurs when there is damage to the brachial plexus. This is an area on each side of the neck where nerve roots from the spinal cord split into each arm’s nerves. Damage to the brachial plexus results in pain, decreased movement, or decreased sensation in the arm and shoulder.
Brachial plexus
The roots (anterior rami) of spinal nerves C5–C8 and T1 form the brachial plexus, which extends inferiorly and laterally on either side of the last four cervical and first thoracic vertebrae (Figures 1 and 2). The brachial plexus passes above the first rib posterior to the clavicle and then enters the axilla (armpit).
Figure 1. Brachial plexus
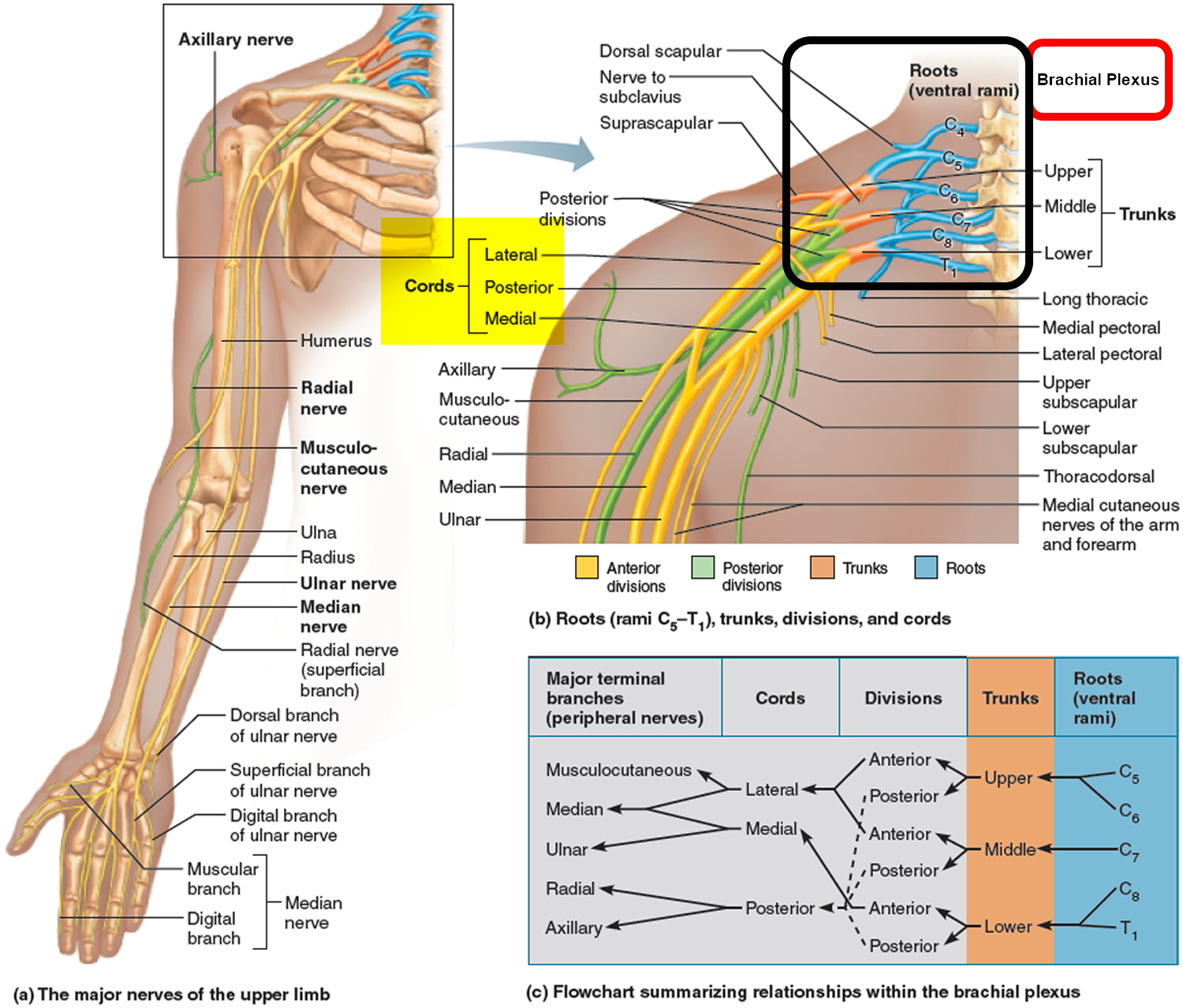
Figure 2. Brachial plexus origin and nerve branches
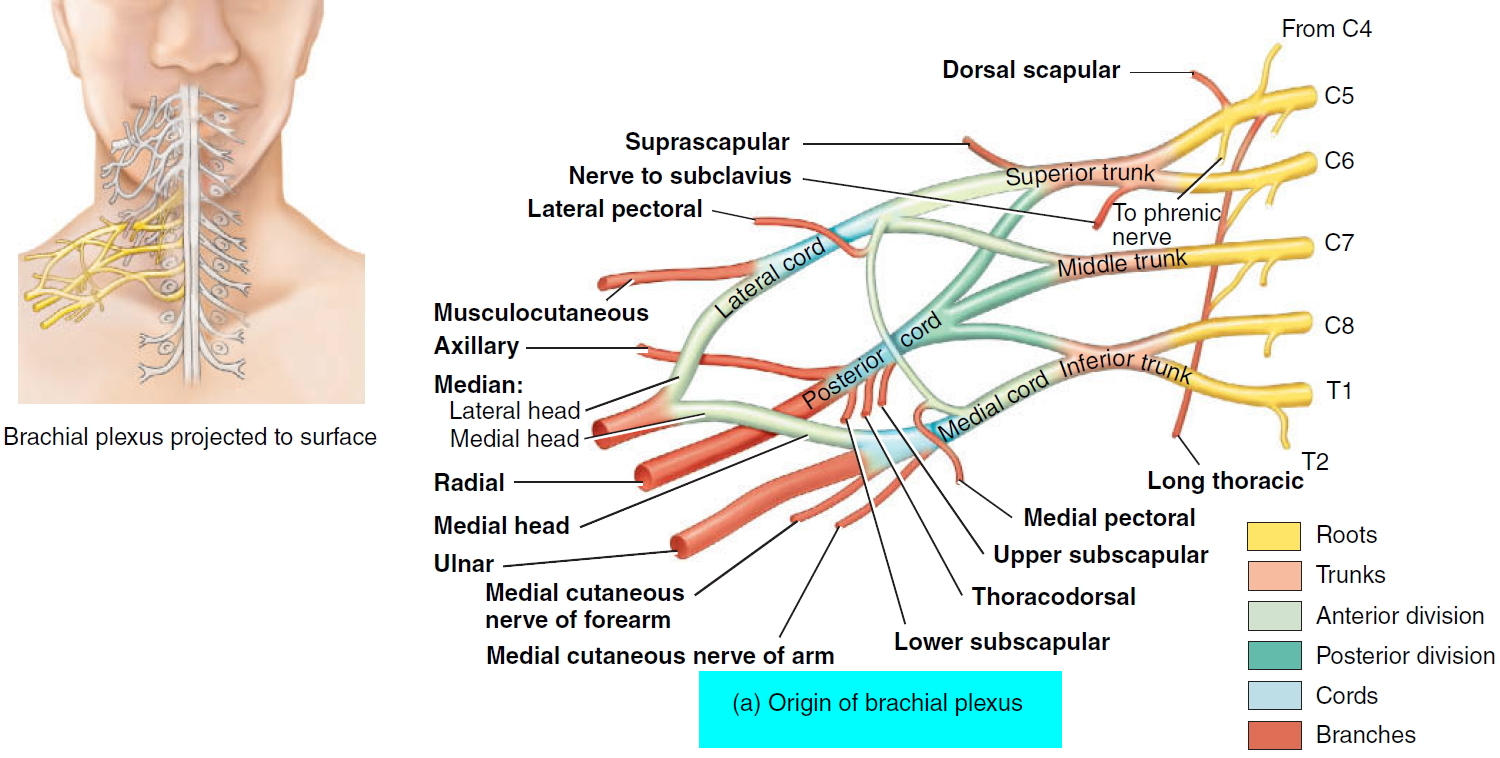 Figure 3. Brachial plexus motor and sensory innervation of the upper limb
Figure 3. Brachial plexus motor and sensory innervation of the upper limb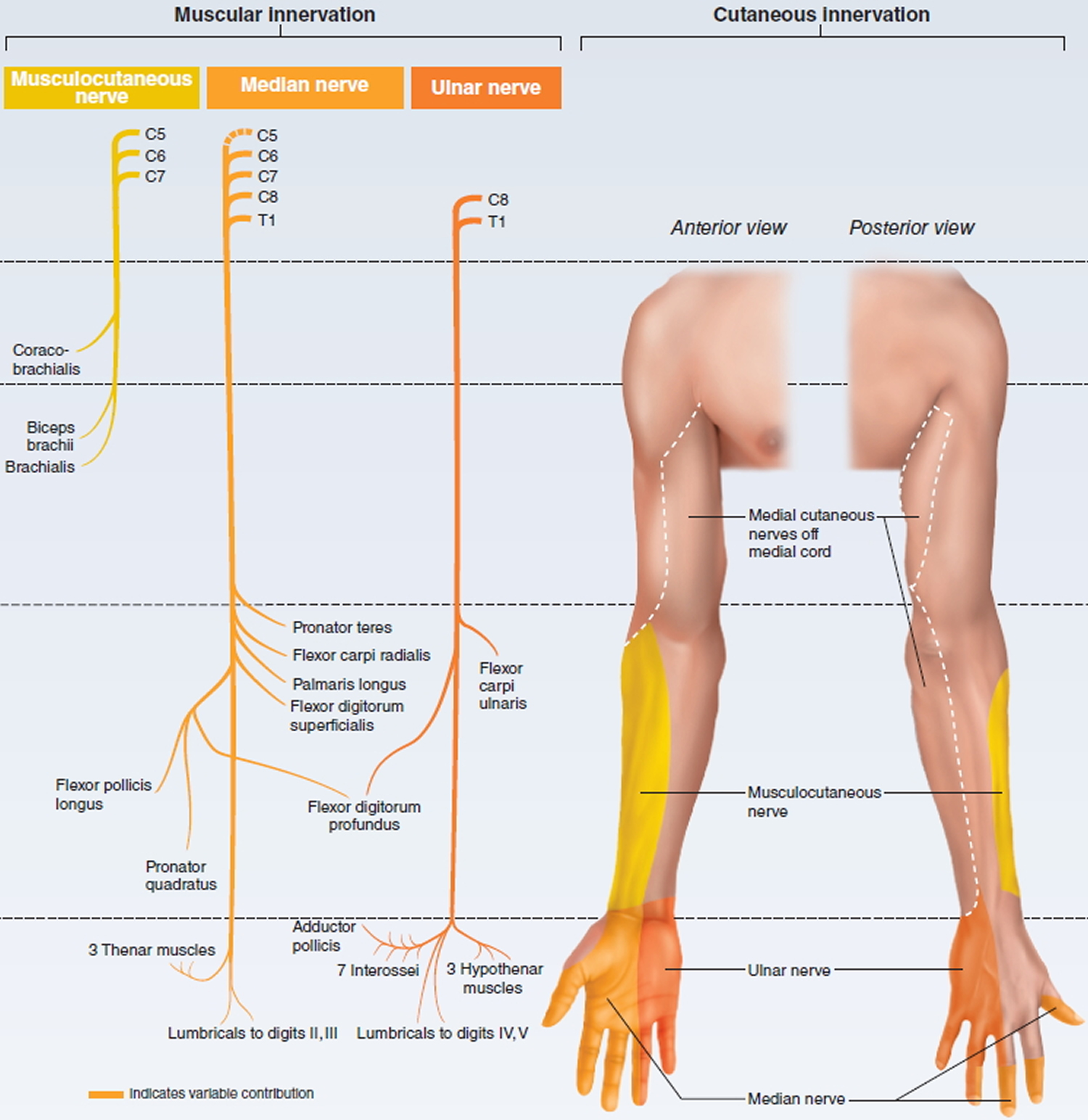
Figure 4. Erb’s palsy (C5-C6 nerve damage) waiter’s tip position
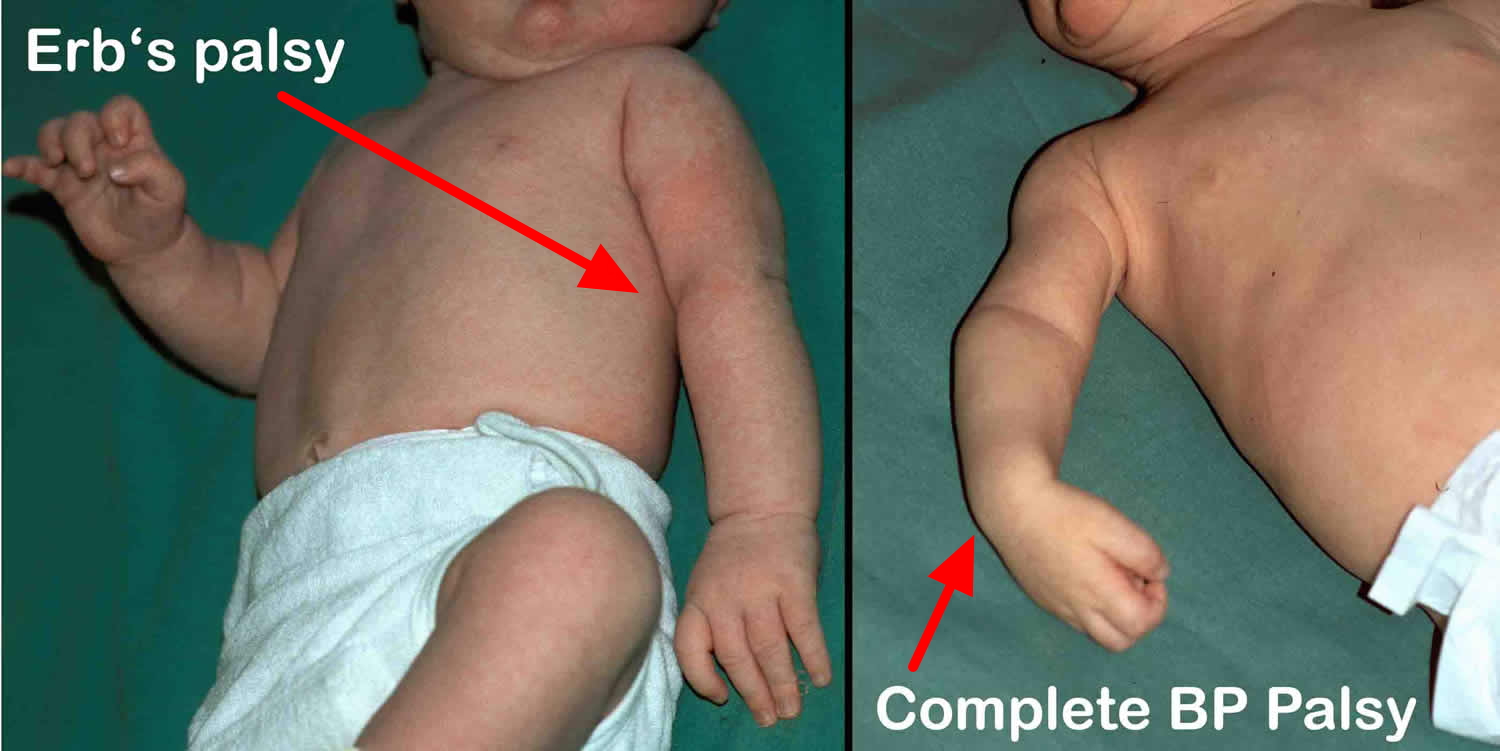
Figure 5. Klumpke’s paralysis (C8-T1 nerve damage) claw hand


Since the brachial plexus is so complex, an explanation of its various parts is helpful. As with the cervical and other plexuses, the roots are the anterior rami of the spinal nerves. The roots of several spinal nerves unite to form trunks in the inferior part of the neck. These are the superior, middle, and inferior trunks. Posterior to the clavicles, the trunks diverge into divisions, called the anterior and posterior divisions. In the axillae (armpits), the divisions unite to form cords called the lateral, medial, and posterior cords. The cords are named for their relationship to the axillary artery, a large artery that supplies blood to the upper limb. The branches of the brachial plexus form the principal nerves of the brachial plexus.
The brachial plexus provides almost the entire nerve supply of the shoulders and upper limbs (Figures 1 and 2). Five large terminal branches arise from the brachial plexus:
- (1) The axillary nerve supplies the deltoid and teres minor muscles.
- (2) The musculocutaneous nerve supplies the anterior muscles of the arm.
- (3) The radial nerve supplies the muscles on the posterior aspect of the arm and forearm.
- (4) The median nerve supplies most of the muscles of the anterior forearm and some of the muscles of the hand.
- (5) The ulnar nerve supplies the anteromedial muscles of the forearm and most of the muscles of the hand.
Brachial plexopathy causes
Damage to the brachial plexus is usually from direct injury to the nerve, stretching injuries (including birth trauma), pressure from tumors in the area (especially from lung tumors), or damage that results from radiation therapy.
Brachial plexus dysfunction may also be associated with:
- Birth defects that put pressure on the neck area
- Exposure to toxins, chemicals, or drugs
- General anesthesia, used during surgery
- Inflammatory conditions, such as those due to a virus or immune system problem
In some cases, no cause can be identified.
Radiation-induced brachial plexopathy
Radiation-induced brachial plexopathy can occur when radiotherapy is directed at the chest, axillary region, thoracic outlet, or neck for the treatment of a myriad of neoplastic diseases. Treatment technique, radiation volume and concomitant use of chemotherapy are associated with development of radiation injury to the brachial plexus 1. The frequency of radiation-induced brachial plexopathy has declined over the past 60 years and depends significantly on both the radiation dose and the proximity of the radiation volume to the underlying plexus. The current brachial plexopathy incidence is 1-2% in patients receiving a typical dose of less than 55 Gy 2. Breast carcinoma accounts for 40-75% of reported cases, followed by lung carcinoma and lymphoma 3.
When treating the axillary and supraclavicular lymph nodes with radiation therapy, it is impossible to avoid irradiating normal tissues, including the brachial plexus. While dosing regimens are designed to limit damage to healthy tissue, radiation-induced neuropathy may occur. The radiation dose; treatment technique; concomitant use of chemotherapy; surgical lymph node dissection; and underlying comorbidities such as diabetes, hypertension, obesity, and vascular disease all demonstrate significant association with the development of radiation injury to the brachial plexus 4. The mechanism is believed to be a combination of failure of cellular proliferation and localized ischemia. The net result is fibrosis of the neural and perineural soft tissues secondary to microvascular insufficiency. This, in turn, leads to ischemic damage to the axons and Schwann cells 5.
The natural course of radiation injury to the brachial plexus varies. Most commonly, brachial plexopathy develops months to years after radiation therapy and demonstrates a relatively stable course over months to years with a gradual worsening of paresthesias and pain. One third of patients deteriorate rapidly and exhibit significant weakness, lymphedema, and pain. Rarely, brachial plexopathy presents as a mild and relatively reversible set of symptoms 6. No present studies quantify the degree of disability experienced by patients with radiation induced brachial plexopathy.
The interval from the last dose of radiation to the first symptom of brachial plexus disorder varies widely. The average interval range reported is 7.5 months to 6 years; however, symptoms may develop decades after treatment. Owing to this prolonged time interval and nonspecific symptoms, often an extensive workup is undergone prior to arriving at the diagnosis of radiation brachial plexopathy.
Sensory symptoms, such as numbness, paresthesia, and dysesthesia, along with swelling and weakness of the arm, are the predominant presenting symptoms. These neurologic symptoms can be progressive and may lead to a weak and edematous arm.
Most radiation brachial plexopathies are painless, but when present, pain symptoms usually are limited to the shoulder and proximal arm. Such pain usually is rated as mild to moderate in intensity. Significant pain complaints are more commonly associated with recurrent tumor than with radiation brachial plexopathy 5.
Traumatic brachial plexopathy
Trauma accounts for a large proportion of brachial plexopathies. The mechanism of an injury and the magnitude, rate, and direction of deforming forces ultimately determine the extent and location of a traumatic brachial plexopathy.
A lesion of the brachial plexus can result in motor, sensory, and sympathetic disturbances. Impairments can be transient, as in stinger or burner injuries in football players, or they may result in intractable palsy. Because of the changing arrangement of the brachial plexus as it progresses distally, injuries to it may result in diverse paralyses, anesthesias, and paresthesias, depending on the exact level of injury and the extent of injury to the various elements at that level 7.
Brachial plexopathy symptoms
Brachial plexopathy symptoms may include:
- Numbness of the shoulder, arm, or hand
- Shoulder pain
- Tingling, burning, pain, or abnormal sensations (location depends on the area injured)
- Weakness of the shoulder, arm, hand, or wrist.
Brachial plexopathy possible complications
Brachial plexopathy complications may include:
- Deformity of the hand or arm, mild to severe, which can lead to contractures
- Partial or complete arm paralysis
- Partial or complete loss of sensation in the arm, hand, or fingers
- Recurrent or unnoticed injury to the hand or arm due to diminished sensation
Brachial plexopathy diagnosis
Brachial plexopathy may be difficult to accurately diagnose, even with a meticulous investigation. This is not only because the anatomic design of the plexus pose challenges, but also because the types of lesions and injuries that occur are frequently incomplete and complex. Even so, establishing a precise anatomic diagnosis and estimating the severity of the lesion is imperative for prognostic, surgical, and rehabilitative purposes.
An exam of the arm, hand and wrist can reveal a problem with the nerves of the brachial plexus. Signs may include:
- Deformity of the arm or hand
- Difficulty moving the shoulder, arm, hand, or fingers
- Diminished arm reflexes
- Wasting of the muscles
- Weakness of hand flexing
A detailed history may help determine the cause of the brachial plexopathy. Age and sex are important, because some brachial plexus problems are more common in certain groups. For example, young men more often have inflammatory or post-viral brachial plexus disease called Parsonage-Turner syndrome.
Tests that may be done to diagnose this condition may include:
- Blood tests
- Chest x-ray
- Electromyography (EMG) to check the muscles and nerves that control the muscles
- MRI of the head, neck, and shoulder
- Nerve conduction to check how fast electrical signals move through a nerve
- Nerve biopsy to examine a piece of nerve under the microscope (rarely needed)
- Ultrasound
Brachial plexopathy treatment
Brachial plexopathy treatment is aimed at correcting the underlying cause and allowing you to use your hand and arm as much as possible. In some cases, no treatment is needed and the problem gets better on its own. A rehabilitation program may be undertaken with a physical therapist and/or an occupational therapist. The goals are to preserve range of motion (ROM), improve strength, and manage pain.
Brachial plexopathy treatment options include any of the following:
- Medicines to control pain
- Physical therapy to help maintain muscle strength.
- Braces, splints, or other devices to help you use your arm
- Nerve block, in which medicine is injected into the area near the nerves to reduce pain
- Surgery to repair the nerves or remove something pressing on the nerves
Occupational therapy or counseling to suggest changes in the workplace may be needed.
Medical conditions such as diabetes and kidney disease can damage nerves. In these cases, treatment is also directed at the underlying medical condition.
Surgery is reserved for patients in whom symptoms persist despite appropriate conservative treatment 8. Brachial plexus injuries are not always reparable, however, and in such cases, neurotizations or nerve transfers may offer a better functional outcome 9.
Physical therapy
Therapeutic modalities should focus on pain reduction, strengthening, preservation of range of motion, and limiting lymphedema. The interventions and modalities should address underlying impairments, as follows:
- Weakness: Assign therapeutic exercise to enhance flexibility and strength of the shoulder girdle paracervical and parathoracic muscles. The glenohumeral joint may require a sling for sitting or standing activities to reduce the degree of glenohumeral joint subluxation and discomfort.
- Pain: Use caution when considering the application of heat and cold if the sensation in the extremity is impaired. Transcutaneous electrical nerve stimulation therapy may be considered for pain control.
- Lymphedema: Educate the patient. Perform manual lymphatic therapy and motorized intermittent pneumatic compression therapy; use graded pressure upper extremity garments.
- Range of motion: Emphasis should be placed on a home exercise program to preserve range of motion and strength.
Occupational therapy
Assess basic and instrumental activities of daily living and provide appropriate adaptive equipment.
Provide fine motor skills training, if the lower plexus is involved.
Recommend sensory and motor re-education techniques.
Consider using a flexor hinge tenodesis orthosis with or without long opponens orthosis if it allows the patient to be functionally prehensile.
Recreational therapy
Focus on enjoyable activities that help to preserve range of motion and retain or build strength while limiting pain and discomfort.
Brachial plexopathy prognosis
A good recovery is possible if the cause is identified and properly treated. In some cases, there is partial or complete loss of movement or sensation. Nerve pain may be severe and may last for a long time.
References- Platteaux N, Dirix P, Hermans R, Nuyts S. Brachial plexopathy after chemoradiotherapy for head and neck squamous cell carcinoma. Strahlenther Onkol. 2010 Sep. 186(9):517-20.
- Delanian S, Lefaix JL, Pradat PF. Radiation-induced neuropathy in cancer survivors. Radiother Oncol. 2012 Dec. 105(3):273-82.
- Fathers E, Thrush D, Huson SM, Norman A. Radiation-induced brachial plexopathy in women treated for carcinoma of the breast. Clin Rehabil. 2002 Mar. 16(2):160-5.
- Phan C, Mindrum M, Silverman C, Paris K, Spanos W. Matched-control retrospective study of the acute and late complications in patients with collagen vascular diseases treated with radiation therapy. Cancer J. 2003 Nov-Dec. 9(6):461-6.
- Dumitru D, Zwarts MJ. Brachial plexopathies and proximal mononeuropathies. Dumitru D, Amato AA, Zwarts MJ. Electrodiagnostic Medicine. 2nd. Philadephia: Hanley & Belfus; 2002. 777-836.
- Dropcho EJ. Neurotoxicity of radiation therapy. Neurol Clin. 2010 Feb. 28(1):217-34.
- Sköld MK, Svensson M, Tsao J, Hultgren T, Landegren T, Carlstedt T, et al. Karolinska institutet 200-year anniversary. Symposium on traumatic injuries in the nervous system: injuries to the spinal cord and peripheral nervous system – injuries and repair, pain problems, lesions to brachial plexus. Front Neurol. 2011. 2:29.
- Dafydd H, Lin CH. Hand reanimation. Curr Rev Musculoskelet Med. 2014 Mar. 7 (1):76-82.
- Wang SF, Li PC, Xue YH, Yiu HW, Li YC, Wang HH. Contralateral C7 nerve transfer with direct coaptation to restore lower trunk function after traumatic brachial plexus avulsion. J Bone Joint Surg Am. 2013 May 1. 95(9):821-7, S1-2.





{kind=link}