What is brain fog
“Brain fog” is a constellation of symptoms that include reduced cognition, inability to concentrate and multitask, as well as loss of short and long term memory that is inappropriate for a person’s age 1. It may include forgetfulness, spaciness, confusion, decreased ability to pay attention, an inability to focus, and difficulty in processing information 2. Remember that gradual cognitive decline from early adulthood is a fact of life.
Brain fog characterizes patients with autism spectrum disorders, neuroimmune diseases 3, celiac disease 4, chronic fatigue syndrome 5, fibromyalgia, Sjögren’s syndrome 2, mastocytosis 6, disorders of mast cell activation 7, and postural tachycardia syndrome 8, as well as “minimal cognitive impairment,” an early clinical presentation of Alzheimer’s disease 9 and other neuropsychiatric disorders 1. Moreover, patients on chemotherapy often experience brain “chemo fog” 10.
Brain “fog” may be due to inflammatory molecules, including adipocytokines and histamine released from mast cells further stimulating microglia activation, and causing focal brain inflammation.
A recent survey of the symptoms experienced by patients with mast cell disorders reported that >90% of them experienced moderate to severe brain “fog” almost daily 11 and cognitive impairment was confirmed using a validated instrument 11. Patients with mast cell disorders also experience other related neurologic 12 and psychiatric 13 symptoms. It is interesting that children with mastocytosis were reported to have increased risk of developing autism spectrum disorders compared to the general population 14. Children with autism spectrum disorders are also characterized by brain “fog” 15 and focal brain inflammation 16 with mast cell activation being implicated in their pathogenesis 17.
Even though Alzheimer’s disease has typically been associated with brain senile plaques and neurofibrillary tangles that involve amyloid-β (Aβ) and tau proteins 18, recent evidence indicates that oxidative stress/mitochondrial dysfunction 19 and inflammation 18, are possibly involved in Alzheimer’s disease. In fact the immune system and inflammation are increasingly implicated in neuropsychiatric diseases 20.
What causes brain fog
Inflammatory molecules, secreted in the brain could contribute to the pathogenesis of such diseases 21 possibly including brain “fog.” Brain expression of pro-inflammatory genes was increased in the brains of deceased patients with neuropsychiatric diseases 22.
It is still not clear what triggers brain inflammation. Mounting evidence suggests that stress 22 and exposure to mold 23, especially airborne mycotoxins 24, may be involved. It is interesting that mold can potentiate histamine release from mast cells 25.
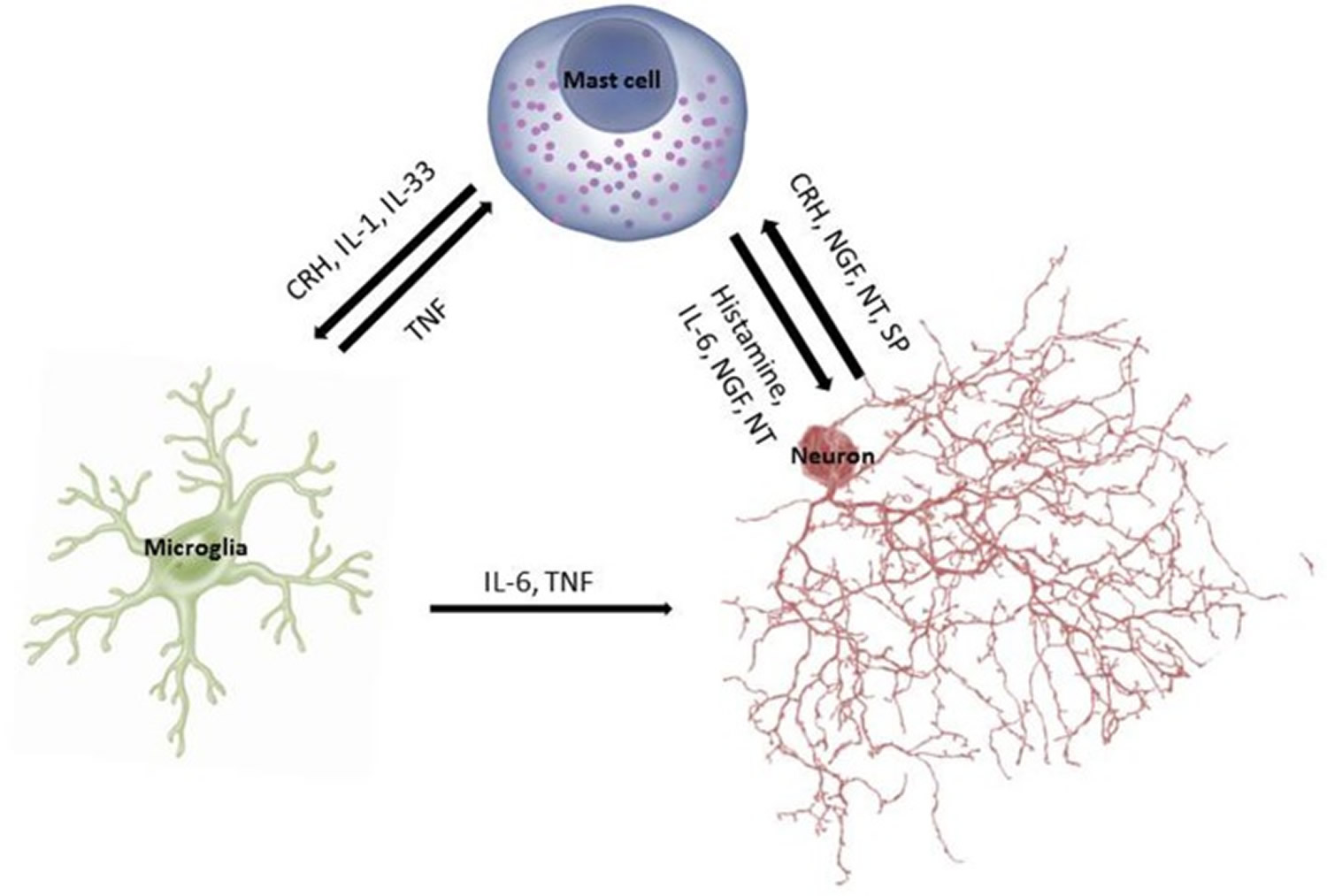
In fact, cross-talk between mast cells and microglia is being considered critical in the pathogenesis of neurodegenerative diseases 26 (see Figure 1). Microglia activation is a common finding in brains of children with autism spectrum disorders 27, as well as in other psychiatric diseases 28. Activation of microglia directly or indirectly by corticotropin-releasing hormone (CRH) could contribute to the pathogenesis of mental disorders 29.
Figure 1. Schematic representation of the cross-talk between mast cells, microglia, and neurons
Obesity
Obesity has been associated with neuropsychiatric disorders 30. Adipocytokines are involved in neuroinflammation 31 and possibly in dementia 32 including Alzheimer’s disease 33.
Mast cells have been implicated in obesity 34, obesity-related asthma 35 and in cardiovascular disease (coronary artery disease) 36, which involves local inflammation 37. Both mast cells 38 and histamine 39 have been reported to be increased in atherosclerotic coronary plaques 34. Mast cell-derived histamine is a coronary constrictor. Mast cell-derived IL-6 and TNF are independent risk factors for coronary heart disease 40 and can be released from mast cells under stress 41, which can precipitate myocardial infarction (heart attack) 42. Obesity leads to endothelial dysfunction and chronic inflammation 43, also associated with the metabolic syndrome 44.
Brain fog symptoms
Signs and symptoms of brain fog may include the following:
- Being unusually disorganized
- Confusion
- Difficulty concentrating
- Difficulty finding the right word
- Difficulty learning new skills
- Difficulty multitasking
- Fatigue
- Feeling of mental fogginess
- Short attention span
- Short-term memory problems
- Taking longer than usual to complete routine tasks
- Trouble with verbal memory, such as remembering a conversation
- Trouble with visual memory, such as recalling an image or list of words
When to see a doctor
If you experience troubling memory or thinking problems, make an appointment with your doctor. Keep a journal of your signs and symptoms so that your doctor can better understand how your memory problems are affecting your everyday life.
How to get rid of brain fog
It’s not clear what causes brain fog and no cure has been identified.
There are lifestyle habits that you can adopt to maintain or potentially improve your health as you age.
These habits, spanning four categories:
- Physical health and exercise,
- Diet and nutrition,
- Cognitive activity, and
- Social engagement.
Can help keep your body and brain healthy and potentially reduce your risk of cognitive decline.
Research has suggested that combining good nutrition with mental, social and physical activities may have a greater benefit in maintaining or improving brain health than any single activity.
Get regular medical care
- Make regular appointments with your primary care doctor or specialist (neurologist, neuropsychiatrist, geriatric psychiatrist).
- Consider going to a specialized memory disorders clinic. Ask your doctor for a referral if desired.
Manage your lifestyle to optimize your health and sense of well being. Always report changes in cognition/memory and mood (depression, anxiety).
Make sure your physician knows about all the prescription and OTC (over-the-counter) medications you are taking.
Especially in patients over 65-70 years of age, a major cause of cognitive dysfunction can be side effects of drugs and drug interactions.
- Inquire about your hormonal status, thyroid function, and blood pressure.
Adopt a Health Lifestyle with Healthy Diet and Regular Exercise
Eating a heart-healthy diet benefits both your body and your brain. In general, this is a diet that is lower in saturated fats. Research in the area of the relationship between diet and cognitive functioning is somewhat limited, but it does point to the benefits of two diets in particular: the DASH (Dietary Approaches to Stop Hypertension) diet and the Mediterranean diet. These diets can help reduce heart disease and may also be able to reduce risk of dementia.
- Dietary Approaches to Stop Hypertension (DASH) diet
- Mediterranean diet
The Dietary Approaches to Stop Hypertension (DASH)
The DASH diet aims to reduce blood pressure:
- Eat foods that are low in saturated fat, total fat and cholesterol, and high in fruits, vegetables and low-fat dairy.
- Consume whole grains, poultry, fish and nuts.
- Decrease your intake of fats, red meats, sweets, sugared beverages and sodium.
The Mediterranean diet
The Mediterranean diet incorporates different principles of healthy eating that are typically found in the areas bordering the Mediterranean Sea:
- Focus on fruit, vegetables, nuts and grains.
- Replace butter with healthy fats, like olive oil.
- Limit red meat.
- Use herbs to flavor food rather than salt.
- Eat fish and poultry at least twice a week.
Stay Physically Active
Exercise regularly. Adequate physical exercise enhances cognition/memory.
Physical activity is a valuable part of any overall body wellness plan and is associated with a lower risk of cognitive decline. If it’s safe for you, engage in cardiovascular exercise to elevate your heart rate. This will increase the blood flow to your brain and body, providing additional nourishment while reducing potential dementia risk factors such as high blood pressure, diabetes and high cholesterol.
- Physical activities
- Take care of your health
Physical activities
Consider physical activities that may also be mentally or socially engaging, such as walking with a friend, taking a dance class, joining an exercise group or golfing. Incorporate activity that you enjoy so you will continue to engage in it. For example, bike riding, gardening or walking the dog. Adopting healthy exercise habits today will allow you to enjoy the lifelong benefits of regular physical activity. However, it’s never too late to start — making healthy choices at any age is beneficial to your well-being. Always consult your doctor before starting any new exercise program.
Prevent falls
- Falls are the leading cause of fatal and non-fatal injuries in older adults, and one-third of adults over age 65 fall every year.
- Falls in which your head is injured may affect your brain’s ability to function normally, causing unconsciousness, confusion and other symptoms.
- Engage in regular physical activity to improve your strength and balance and reduce your risk of falling.
- At home, cover or put objects out of the way that may increase your risk of tripping and falling, such as shoes or electrical cords.
- Turn on lights when you enter a room so you can clearly see obstacles. Consider installing extra lighting in areas that tend to be dark.
Take care of your health
Keep your heart healthy to help keep your brain healthy. Growing evidence suggests that many factors that increase the risk of heart disease also may increase the risk of dementia. These factors include smoking, obesity, diabetes, high cholesterol and high blood pressure.
- Visit your doctor regularly.
- Get your “numbers” checked, including weight, blood sugar, blood pressure and cholesterol. Actively seek treatment to keep yourself within healthy ranges.
- Stay physically active
- If you have diabetes, manage it properly.
- Stop smoking. If you don’t smoke, don’t start.
- Take action to minimize stress. Studies have found that regular physical activity decreases stress, increases your ability to manage stress and leads to better mood overall.
- Get enough sleep. Inadequate sleep due to conditions like insomnia or sleep apnea can result in problems with memory and thinking. Rejuvenate with sufficient sleep. If after 8-9 hours of sleep you are still tired, tell your doctor.
- Avoid excess alcohol.
- Seek professional assistance to address anxiety, depression or other mental health concerns.
- Minimize stress and anxiety:
• Set realistic expectations
• Plan ahead
• Take breaks throughout the day
• Learn relaxation exercises and practice them at regular intervals
• Balance work and leisure
• Let yourself laugh
• Talk about feelings
• Limit multi-tasking and focus on one task at a time
• Reduce caffeine and alcohol.
• Manage effectively musculoskeletal and joint pain.
Stay Mentally and Socially Active
Embrace lifestyle habits that improve your overall health, such as exercising, consuming a nutritious diet — and staying cognitively and socially active. Science suggests these may support brain health as well. It’s never too late to make changes to achieve a healthier lifestyle — or too early to start.
- Mental activities
- Social Activities
Mental activities
Mentally challenging activities, such as learning a new skill, adopting a new hobby or engaging in formal education, may have short and long-term benefits for your brain. To keep your mind active, it is important to participate in activities that expose your mind to new topics. Boost your brain power: Continue to work into retirement (part time), learn new skills, volunteer, engage in social and men.
Challenge yourself to games with strategy or high-level reading material, or determine how to approach a familiar task in a more effective way. Selecting activities you enjoy will increase the likelihood that you will continue to engage in them over time.
Another way to stay mentally active is to get as much formal education as you can, at any point in life. Formal education is classroom-based learning administered by professionally trained teachers. Engaging in this type of education will help keep your brain healthy and may protect your brain from developing dementia. This could involve taking a class at a local college or community center that teaches a new topic, skill or hobby (e.g., learning a language or how to play an instrument).
Social activities
Social engagement is associated with reduced rates of disability and mortality, and may also reduce risk for depression. Remaining socially active may support brain health and possibly delay the onset of dementia. There are many ways to stay socially active in your community, and these activities will provide the greatest connection to others.
Stay socially active
Participation in clubs, volunteer efforts and other community pursuits may be valuable in maintaining your overall health. Many of these social activities are low-cost or free, such as joining a walking group or book club in your neighborhood. Staying socially active can also be as simple as engaging with friends and family on a regular basis.
Pursue social activities that are meaningful to you. For instance, if you love animals, consider volunteering at a local shelter or with a rescue group.
References- Theoharides TC, Stewart JM, Hatziagelaki E, Kolaitis G. Brain “fog,” inflammation and obesity: key aspects of neuropsychiatric disorders improved by luteolin. Frontiers in Neuroscience. 2015;9:225. doi:10.3389/fnins.2015.00225. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4490655/
- http://www.sjogrens.org/files/brochures/brain_fog.pdf
- Atopic conditions in search of pathogenesis and therapy. Theoharides TC. Clin Ther. 2013 May; 35(5):544-7. https://www.ncbi.nlm.nih.gov/pubmed/23642292/
- Cognitive impairment in coeliac disease improves on a gluten-free diet and correlates with histological and serological indices of disease severity. Lichtwark IT, Newnham ED, Robinson SR, Shepherd SJ, Hosking P, Gibson PR, Yelland GW. Aliment Pharmacol Ther. 2014 Jul; 40(2):160-70. https://www.ncbi.nlm.nih.gov/pubmed/24889390/
- Caught in the thickness of brain fog: exploring the cognitive symptoms of Chronic Fatigue Syndrome. Ocon AJ. Front Physiol. 2013; 4():63. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3617392/
- Targeting IL-33 in autoimmunity and inflammation. Theoharides TC, Petra AI, Taracanova A, Panagiotidou S, Conti P. J Pharmacol Exp Ther. 2015 Jul; 354(1):24-31. http://jpet.aspetjournals.org/content/354/1/24.long
- Spectrum of mast cell activation disorders. Petra AI, Panagiotidou S, Stewart JM, Conti P, Theoharides TC. Expert Rev Clin Immunol. 2014 Jun; 10(6):729-39. https://www.ncbi.nlm.nih.gov/pubmed/24784142/
- What is brain fog? An evaluation of the symptom in postural tachycardia syndrome. Ross AJ, Medow MS, Rowe PC, Stewart JM. Clin Auton Res. 2013 Dec; 23(6):305-11. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3896080/
- Neuronal dysfunction and disconnection of cortical hubs in non-demented subjects with elevated amyloid burden. Drzezga A, Becker JA, Van Dijk KR, Sreenivasan A, Talukdar T, Sullivan C, Schultz AP, Sepulcre J, Putcha D, Greve D, Johnson KA, Sperling RA. Brain. 2011 Jun; 134(Pt 6):1635-46. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3102239/
- A proposed mechanism for chemotherapy-related cognitive impairment (‘chemo-fog’). Raffa RB. J Clin Pharm Ther. 2011 Jun; 36(3):257-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3249621/
- Evidence for cognitive impairment in mastocytosis: prevalence, features and correlations to depression. Moura DS, Sultan S, Georgin-Lavialle S, Barete S, Lortholary O, Gaillard R, Hermine O. PLoS One. 2012; 7(6):e39468. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3379977/
- Neurologic symptoms and diagnosis in adults with mast cell disease. Smith JH, Butterfield JH, Pardanani A, DeLuca GC, Cutrer FM. Clin Neurol Neurosurg. 2011 Sep; 113(7):570-4. https://www.ncbi.nlm.nih.gov/pubmed/21664760/
- Neuropsychological features of adult mastocytosis. Moura DS, Georgin-Lavialle S, Gaillard R, Hermine O. Immunol Allergy Clin North Am. 2014 May; 34(2):407-22. https://www.ncbi.nlm.nih.gov/pubmed/24745683/
- Autism spectrum disorders and mastocytosis. Theoharides TC. Int J Immunopathol Pharmacol. 2009 Oct-Dec; 22(4):859-65. https://www.ncbi.nlm.nih.gov/pubmed/20074449/
- A review of research trends in physiological abnormalities in autism spectrum disorders: immune dysregulation, inflammation, oxidative stress, mitochondrial dysfunction and environmental toxicant exposures. Rossignol DA, Frye RE. Mol Psychiatry. 2012 Apr; 17(4):389-401. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3317062/
- Focal brain inflammation and autism. Theoharides TC, Asadi S, Patel AB. J Neuroinflammation. 2013 Apr 9; 10():46. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3626551/
- Is a subtype of autism an allergy of the brain? Theoharides TC. Clin Ther. 2013 May; 35(5):584-91. https://www.ncbi.nlm.nih.gov/pubmed/23688533/
- Neuroinflammation in Alzheimer’s disease. Heneka MT, Carson MJ, El Khoury J, Landreth GE, Brosseron F, Feinstein DL, Jacobs AH, Wyss-Coray T, Vitorica J, Ransohoff RM, Herrup K, Frautschy SA, Finsen B, Brown GC, Verkhratsky A, Yamanaka K, Koistinaho J, Latz E, Halle A, Petzold GC, Town T, Morgan D, Shinohara ML, Perry VH, Holmes C, Bazan NG, Brooks DJ, Hunot S, Joseph B, Deigendesch N, Garaschuk O, Boddeke E, Dinarello CA, Breitner JC, Cole GM, Golenbock DT, Kummer MP. Lancet Neurol. 2015 Apr; 14(4):388-405. https://www.ncbi.nlm.nih.gov/pubmed/25792098/
- Abnormal mitochondrial dynamics in the pathogenesis of Alzheimer’s disease. Zhu X, Perry G, Smith MA, Wang X. J Alzheimers Dis. 2013; 33 Suppl 1():S253-62. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4097015/
- Cytokines in bipolar disorder: a systematic review and meta-analysis. Munkholm K, Vinberg M, Vedel Kessing L. J Affect Disord. 2013 Jan 10; 144(1-2):16-27. https://www.ncbi.nlm.nih.gov/pubmed/22749156/
- Brain cytokines and neuropsychiatric disorders. Theoharides TC, Weinkauf C, Conti P. J Clin Psychopharmacol. 2004 Dec; 24(6):577-81. https://www.ncbi.nlm.nih.gov/pubmed/15538117/
- Decreased mitochondrial function and increased brain inflammation in bipolar disorder and other neuropsychiatric diseases. Theoharides TC, Zhang B, Conti P. J Clin Psychopharmacol. 2011 Dec; 31(6):685-7. https://www.ncbi.nlm.nih.gov/pubmed/22020358/
- Neurologic and neuropsychiatric syndrome features of mold and mycotoxin exposure. Empting LD. Toxicol Ind Health. 2009 Oct-Nov; 25(9-10):577-81. https://www.ncbi.nlm.nih.gov/pubmed/19854819/
- Detection of mycotoxins in patients with chronic fatigue syndrome. Brewer JH, Thrasher JD, Straus DC, Madison RA, Hooper D. Toxins (Basel). 2013 Apr 11; 5(4):605-17. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3705282/
- The indoor microfungus Trichoderma viride potentiates histamine release from human bronchoalveolar cells. Larsen FO, Clementsen P, Hansen M, Maltbaek N, Gravesen S, Skov PS, Norn S. APMIS. 1996 Sep; 104(9):673-9. https://www.ncbi.nlm.nih.gov/pubmed/8972692/
- Mast cells, glia and neuroinflammation: partners in crime? Skaper SD, Facci L, Giusti P. Immunology. 2014 Mar; 141(3):314-27. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3930370/
- Transcriptome analysis reveals dysregulation of innate immune response genes and neuronal activity-dependent genes in autism. Gupta S, Ellis SE, Ashar FN, Moes A, Bader JS, Zhan J, West AB, Arking DE. Nat Commun. 2014 Dec 10; 5():5748. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4270294/
- The immune theory of psychiatric diseases: a key role for activated microglia and circulating monocytes. Beumer W, Gibney SM, Drexhage RC, Pont-Lezica L, Doorduin J, Klein HC, Steiner J, Connor TJ, Harkin A, Versnel MA, Drexhage HA. J Leukoc Biol. 2012 Nov; 92(5):959-75. https://www.ncbi.nlm.nih.gov/pubmed/22875882/
- Corticotropin-releasing hormone, microglia and mental disorders. Kritas SK, Saggini A, Cerulli G, Caraffa A, Antinolfi P, Pantalone A, Rosati M, Tei M, Speziali A, Saggini R, Conti P. Int J Immunopathol Pharmacol. 2014 Apr-Jun; 27(2):163-7. https://www.ncbi.nlm.nih.gov/pubmed/25004828/
- Adolescent-Onset Depression: Are Obesity and Inflammation Developmental Mechanisms or Outcomes? Byrne ML, O’Brien-Simpson NM, Mitchell SA, Allen NB. Child Psychiatry Hum Dev. 2015 Dec; 46(6):839-50. https://www.ncbi.nlm.nih.gov/pubmed/25666100/
- Obesity, adipokines and neuroinflammation. Aguilar-Valles A, Inoue W, Rummel C, Luheshi GN. Neuropharmacology. 2015 Sep; 96(Pt A):124-34. https://www.ncbi.nlm.nih.gov/pubmed/25582291/
- Adipokines: a link between obesity and dementia? Kiliaan AJ, Arnoldussen IA, Gustafson DR. Lancet Neurol. 2014 Sep; 13(9):913-23. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4228955/
- Altered serum levels of adipokines and insulin in probable Alzheimer’s disease. Khemka VK, Bagchi D, Bandyopadhyay K, Bir A, Chattopadhyay M, Biswas A, Basu D, Chakrabarti S. J Alzheimers Dis. 2014; 41(2):525-33. https://www.ncbi.nlm.nih.gov/pubmed/24625795/
- Mast cells squeeze the heart and stretch the gird: their role in atherosclerosis and obesity. Theoharides TC, Sismanopoulos N, Delivanis DA, Zhang B, Hatziagelaki EE, Kalogeromitros D. Trends Pharmacol Sci. 2011 Sep; 32(9):534-42. https://www.ncbi.nlm.nih.gov/pubmed/21741097/
- Do mast cells link obesity and asthma? Sismanopoulos N, Delivanis DA, Mavrommati D, Hatziagelaki E, Conti P, Theoharides TC. Allergy. 2013 Jan; 68(1):8-15. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3515712/
- Impact of obesity on cardiovascular health. Chrostowska M, Szyndler A, Hoffmann M, Narkiewicz K. Best Pract Res Clin Endocrinol Metab. 2013 Apr; 27(2):147-56. https://www.ncbi.nlm.nih.gov/pubmed/23731877/
- Role of mast cells in atherosclerosis: a classical inflammatory disease. Spinas E, Kritas SK, Saggini A, Mobili A, Caraffa A, Antinolfi P, Pantalone A, Tei M, Speziali A, Saggini R, Conti P. Int J Immunopathol Pharmacol. 2014 Oct-Dec; 27(4):517-21. https://www.ncbi.nlm.nih.gov/pubmed/25572731/
- Association between myocardial infarction and the mast cells in the adventitia of the infarct-related coronary artery. Laine P, Kaartinen M, Penttilä A, Panula P, Paavonen T, Kovanen PT. Circulation. 1999 Jan 26; 99(3):361-9. http://circ.ahajournals.org/content/99/3/361.long
- Elevation of the plasma histamine concentration in the coronary circulation in patients with variant angina. Sakata Y, Komamura K, Hirayama A, Nanto S, Kitakaze M, Hori M, Kodama K. Am J Cardiol. 1996 May 15; 77(12):1121-6. https://www.ncbi.nlm.nih.gov/pubmed/8644672/
- Inflammation and atherosclerosis. Libby P, Ridker PM, Maseri A. Circulation. 2002 Mar 5; 105(9):1135-43. http://circ.ahajournals.org/content/105/9/1135.long
- Stress-induced interleukin-6 release in mice is mast cell-dependent and more pronounced in Apolipoprotein E knockout mice. Huang M, Pang X, Karalis K, Theoharides TC. Cardiovasc Res. 2003 Jul 1; 59(1):241-9. https://www.ncbi.nlm.nih.gov/pubmed/12829195/
- Stress triggers coronary mast cells leading to cardiac events. Alevizos M, Karagkouni A, Panagiotidou S, Vasiadi M, Theoharides TC. Ann Allergy Asthma Immunol. 2014 Apr; 112(4):309-16. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4288814/
- Obesity, inflammation and endothelial dysfunction. Iantorno M, Campia U, Di Daniele N, Nistico S, Forleo GB, Cardillo C, Tesauro M. J Biol Regul Homeost Agents. 2014 Apr-Jun; 28(2):169-76. https://www.ncbi.nlm.nih.gov/pubmed/25001649/
- Relationship between adipoq gene polymorphism and lipid levels and diabetes. Sun Y, Li DG, Li Q, Huang L, He Z, Zhang F, Wang CB. J Biol Regul Homeost Agents. 2015 Jan-Mar; 29(1):221-7. https://www.ncbi.nlm.nih.gov/pubmed/25864761/





{kind=link}