
Breast cancer
Breast cancer is cancer that forms in the cells of the breasts that begin to grow out of control 1. In the U.S., breast cancer is the second most common cancer in women after skin cancer. It can occur in both men and women, but it is rare in men. Each year there are about 100 times more new cases of breast cancer in women than in men.
Currently, the average risk of a woman in the United States developing breast cancer sometime in her life is about 13%. This means there is a 1 in 8 chance she will develop breast cancer. This also means there is a 7 in 8 chance she will never have the disease.
Breast cancer mainly occurs in middle-aged and older women. The median age at the time of breast cancer diagnosis is 62. This means half of the women who developed breast cancer are 62 years of age or younger when they are diagnosed. A very small number of women diagnosed with breast cancer are younger than 45.
The American Cancer Society’s estimates for breast cancer in the United States for 2022 are 2:
- New cases:
- About 287,850 new cases of invasive breast cancer will be diagnosed in women.
- About 51,400 new cases of ductal carcinoma in situ (DCIS) will be diagnosed.
- Deaths: About 43,250 women will die from breast cancer.
- 5-Year Relative Survival: 90.6%. Relative survival is an estimate of the percentage of patients who would be expected to survive the effects of their cancer. It excludes the risk of dying from other causes. Because survival statistics are based on large groups of people, they cannot be used to predict exactly what will happen to an individual patient. No two patients are entirely alike, and treatment and responses to treatment can vary greatly.
- Breast cancer deaths as percentage of All Cancer Deaths: 7.1%.
- Rate of New Cases and Deaths per 100,000: The rate of new cases of female breast cancer was 128.3 per 100,000 women per year. The death rate was 19.9 per 100,000 women per year. These rates are age-adjusted and based on 2015–2019 cases and deaths.
- Lifetime Risk of Developing Cancer: Approximately 12.9 percent of women will be diagnosed with female breast cancer at some point during their lifetime, based on 2017–2019 data.
- In 2019, there were an estimated 3,771,795 women living with female breast cancer in the United States.
Breast cancer is the second leading cause of cancer death in women (only lung cancer kills more women each year). The chance that a woman will die from breast cancer is about 1 in 39 (about 2.6%).
Death rates from female breast cancer dropped 39% from 1989 to 2015. Since 2007, breast cancer death rates have been steady in women younger than 50, but have continued to decrease in older women. From 2013 to 2018, the death rate went down by 1% per year.
Relative survival rates are an estimate of the percentage of patients who will survive for a given period of time after a cancer diagnosis, accounting for normal life expectancy. Survival among cancer patients is compared to survival among people of the same age and race who have not been diagnosed with cancer. For example, if the 5-year relative survival rate for a specific stage of breast cancer is 90.6%, it means that women who have that cancer are, on average, about 90.6% as likely as women who don’t have that cancer to live for at least 5 years after being diagnosed. Based on the most recent data (National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) 2012–2018), relative survival rates for women diagnosed with breast cancer are 2:
- 90.6% at 5 years after diagnosis
- 86% after 10 years
- 80% after 15 years
Relative survival rates should be interpreted with caution. First, they are based on the average experience of all women and do not predict individual prognosis because many patient and tumor characteristics that influence breast cancer survival are not taken into account. Second, long-term survival rates are based on the experience of women diagnosed and treated many years ago and do not reflect the most recent improvements in early detection and treatment.
Breast cancer survival varies by stage at diagnosis
The overall 5-year relative survival rate is 99.1% for localized disease, 86.1% for regional disease, and 30% for distant-stage disease 2.
- Localized disease: There is no sign that the cancer has spread outside of the breast.
- Regional disease: The cancer has spread outside the breast to nearby structures or lymph nodes.
- Distant disease: The cancer has spread to distant parts of the body such as the lungs, liver or bones.
Survival within each stage varies by tumor size. For example, among women with regional disease, the 5-year relative survival is 95% for tumors less than or equal to 2.0 cm, 85% for tumors 2.1-5.0 cm, and 72% for tumors greater than 5.0 cm.
Breast cancer survival rates footnotes
- Women now being diagnosed with breast cancer may have a better outlook than these numbers show.
- These numbers apply only to the stage of the cancer when it is first diagnosed. They do not apply later on if the cancer grows, spreads, or comes back after treatment.
- These numbers don’t take everything into account. Survival rates are grouped based on how far the cancer has spread, but your age, overall health, how well the cancer responds to treatment, tumor grade, the presence of hormone receptors on the cancer cells, human epidermal growth factor type 2 receptor (HER2) status, and other factors can also affect your outlook.
- Survival rates for women with triple-negative breast cancer are different than those above.
- Survival rates for women with inflammatory breast cancer are different than those above.
These decreases are believed to be the result of finding breast cancer earlier through screening and increased awareness, as well as better treatments.
Substantial support for breast cancer awareness and research funding has helped created advances in the diagnosis and treatment of breast cancer. Breast cancer survival rates have increased, and the number of deaths associated with this disease is steadily declining, largely due to factors such as earlier detection, a new personalized approach to treatment and a better understanding of the disease.
Female Breast Anatomy
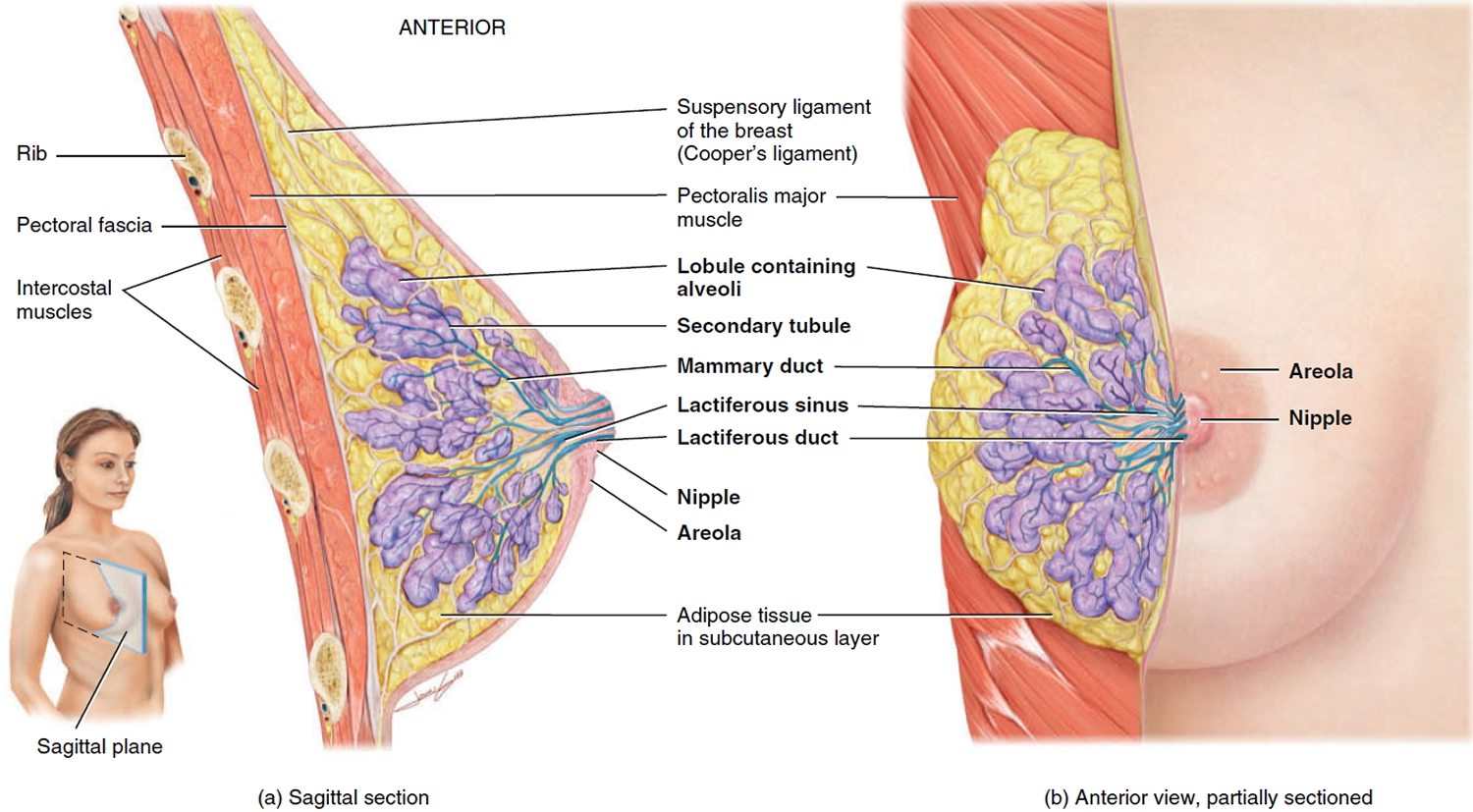
Within each breast is a mammary gland, a modified sudoriferous (sweat) gland that produces milk (Figure 1). A mammary gland consists of 15 to 20 lobes, or compartments, separated by a variable amount of adipose (fatty) tissue. In each lobe are several smaller compartments called lobules, composed of grapelike clusters of milk-secreting glands termed alveoli (small cavities) embedded in connective tissue. Contraction of myoepithelial cells surrounding the alveoli helps propel milk toward the nipples. When milk is being produced, it passes from the alveoli into a series of secondary tubules and then into the mammary ducts. Near the nipple, the mammary ducts expand slightly to form sinuses called lactiferous sinuses, where some milk may be stored before draining into a lactiferous duct. Each lactiferous duct typically carries milk from one of the lobes to the exterior.
The functions of the mammary glands are the synthesis, secretion, and ejection of milk; these functions, called lactation, are associated with pregnancy and childbirth. Milk production is stimulated largely by the hormone prolactin from the anterior pituitary, with contributions from progesterone and estrogens. The ejection of milk is stimulated by oxytocin, which is released from the posterior pituitary in response to the sucking of an infant on the mother’s nipple (suckling).
Strands of connective tissue called the suspensory ligaments of the breast (Cooper’s ligaments) run between the skin and fascia and support the breast. These ligaments become looser with age or with the excessive strain that can occur in longterm jogging or high-impact aerobics.
The breast anatomy:
- Lobules are the glands that make breast milk. Cancers that start here are called lobular cancers.
- Ducts are small canals that come out from the lobules and carry the milk to the nipple. This is the most common place for breast cancer to start. Cancers that start here are called ductal cancers.
- The nipple is the opening in the skin of the breast where the ducts come together and turn into larger ducts so the milk can leave the breast. The nipple is surrounded by slightly darker thicker skin called the areola. A less common type of breast cancer called Paget disease of the breast can start in the nipple.
- The fat and connective tissue (stroma) surround the ducts and lobules and help keep them in place. A less common type of breast cancer called phyllodes tumor can start in the stroma.
- Blood vessels and lymph vessels are also found in each breast. Angiosarcoma is a less common type of breast cancer that can start in the lining of these vessels. The lymph system is described below.
Figure 1. Normal breast (female)
Where breast cancer starts
Breast cancers can start from different parts of the breast. The most common type of breast cancer is ductal carcinoma, which begins in the cells of the lactiferous ducts that carry milk to the nipple (ductal cancers). Some breast cancers start in the glands (the cells of the lobules) that make breast milk (lobular cancers). There are also other types of breast cancer that are less common.
Ductal carcinoma in situ (DCIS) is a condition in which abnormal cells are found in the lining of the lactiferous ducts but they haven’t spread outside the lactiferous duct. Breast cancer that has spread from where it began in the ducts or lobules to surrounding tissue is called invasive breast cancer. In inflammatory breast cancer, the breast looks red and swollen and feels warm because the cancer cells block the lymph vessels in the skin.
A small number of cancers start in other tissues in the breast. These cancers are called sarcomas and lymphomas and are not really thought of as breast cancers.
Although many types of breast cancer can cause a lump in the breast, not all do. Many breast cancers are found on screening mammograms which can detect cancers at an earlier stage, often before they can be felt, and before symptoms develop. There are other symptoms of breast cancer you should watch for and report to a health care provider.
It’s also important to understand that most breast lumps are benign and not cancer (malignant). Non-cancerous breast tumors are abnormal growths, but they do not spread outside of the breast and they are not life threatening. But some benign breast lumps can increase a woman’s risk of getting breast cancer. Any breast lump or change needs to be checked by a health care professional to determine if it is benign or malignant (cancer) and if it might affect your future cancer risk.
How breast cancer spreads
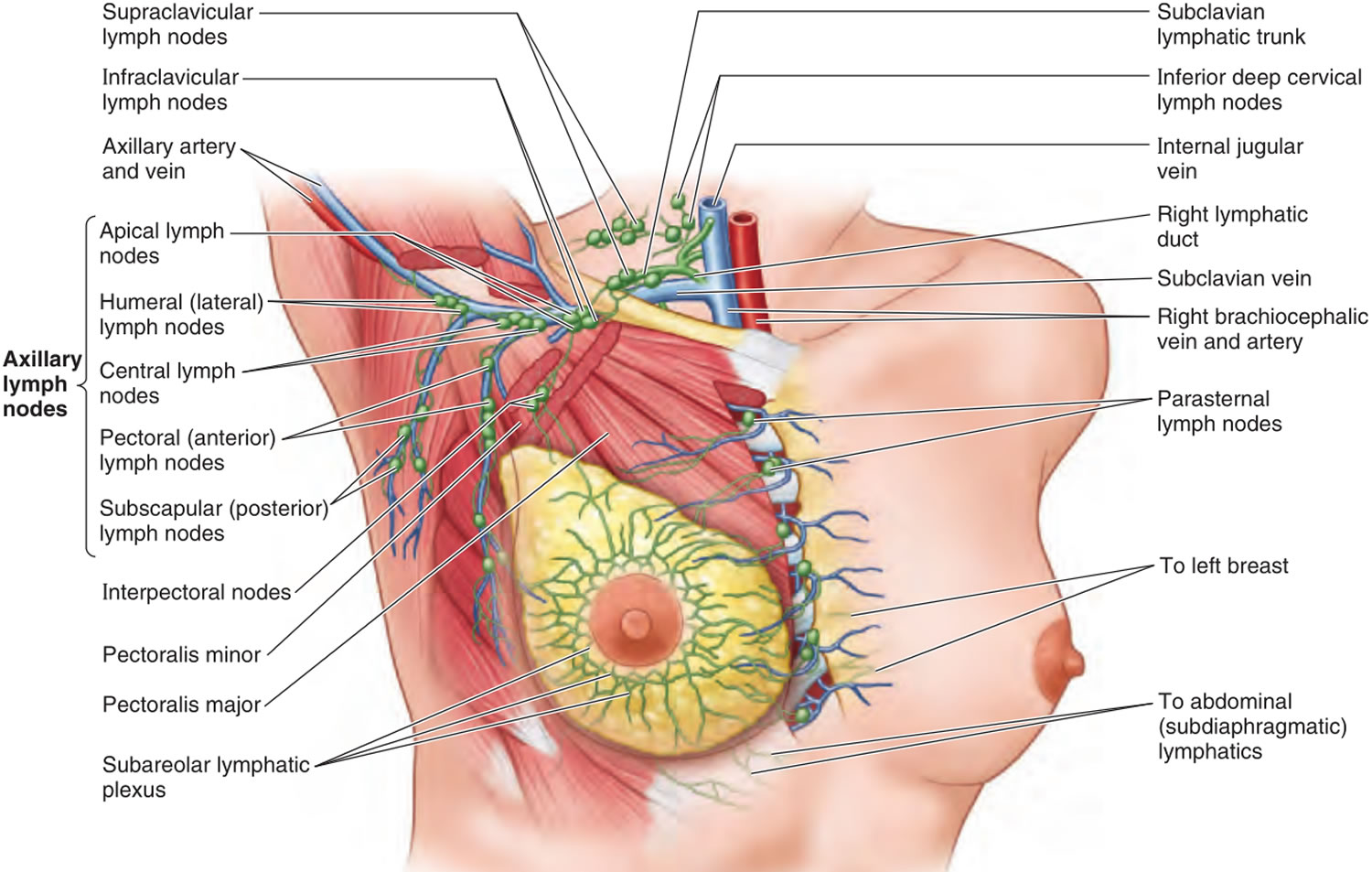
Breast cancer can spread when the cancer cells get into the blood or lymph system (see Figure 2) and are carried to other parts of the body.
The lymph system is a network of lymph (or lymphatic) vessels found throughout the body that connects lymph nodes (small bean-shaped collections of immune system cells). The clear fluid inside the lymph vessels, called lymph, contains tissue by-products and waste material, as well as immune system cells. The lymph vessels carry lymph fluid away from the breast. In the case of breast cancer, cancer cells can enter those lymph vessels and start to grow in lymph nodes. Most of the lymph vessels of the breast drain into:
- Lymph nodes under the arm (axillary nodes)
- Lymph nodes around the collar bone (supraclavicular [above the collar bone] and infraclavicular [below the collar bone] lymph nodes)
- Lymph nodes inside the chest near the breast bone (internal mammary lymph nodes)
If cancer cells have spread to your lymph nodes, there is a higher chance that the cells could have traveled through the lymph system and spread (metastasized) to other parts of your body. The more lymph nodes with breast cancer cells, the more likely it is that the cancer may be found in other organs. Because of this, finding cancer in one or more lymph nodes often affects your treatment plan. Usually, you will need surgery to remove one or more lymph nodes to know whether the cancer has spread.
Still, not all women with cancer cells in their lymph nodes develop metastases, and some women with no cancer cells in their lymph nodes develop metastases later.
Figure 2. Lymph nodes associated with breast cancer spread
 What Causes Breast Cancer
What Causes Breast Cancer
Changes or mutations in DNA can cause normal breast cells to become cancer. Certain DNA changes are passed on from parents (inherited) and can greatly increase your risk for breast cancer. Other lifestyle-related risk factors, such as what you eat and how much you exercise, can increase your chance of developing breast cancer, but it’s not yet known exactly how some of these risk factors cause normal cells to become cancer. Hormones seem to play a role in many cases of breast cancer, but just how this happens is not fully understood.
Inherited versus acquired DNA mutations
Normal breast cells become cancer because of changes (mutations) in DNA. DNA is the chemical in our cells that makes up our genes. Genes have the instructions for how our cells function. Some DNA mutations are inherited or passed to you from your parents. This means the mutations are in your cells when you are born and some mutations can greatly increase the risk of certain cancers. They cause many of the cancers that run in some families and often cause cancer when people are younger.
But most DNA changes linked to breast cancer are acquired. This means the change takes place in breast cells during a person’s life rather than having been inherited or born with them. Acquired DNA changes take place over time and are only in the breast cancer cells.
Mutated DNA can lead to mutated genes. Some genes control when our cells grow, divide into new cells, and die. Changes in these genes can cause the cells to lose normal control and are linked to cancer.
Proto-oncogenes
Proto-oncogenes are genes that help cells grow normally. When a proto-oncogene mutates (changes) or there are too many copies of it, it becomes a “bad” gene that can stay turned on or activated when it’s not supposed to be. When this happens, the cell grows out of control and makes more cells that grow out of control. This can lead to cancer. This bad gene is called an oncogene.
Think of a cell as a car. For the car to work properly, there need to be ways to control how fast it goes. A proto-oncogene normally functions in a way that’s much like a gas pedal. It helps control how and when the cell grows and divides. An oncogene is like a gas pedal that’s stuck down, which causes the cell to divide out of control.
Tumor suppression genes
Tumor suppressor genes are normal genes that slow down cell division (cell growth), repair DNA mistakes, or tell cells when to die (a process known as apoptosis or programmed cell death). When tumor suppressor genes don’t work properly, cells can grow out of control, make more cells that grow out of control, and don’t die when they should, which can lead to cancer.
A tumor suppressor gene is like the brake pedal on a car. It normally keeps the cell from dividing too quickly, just as a brake keeps a car from going too fast. When something goes wrong with the gene, such as a mutation, the “brakes” don’t work and cell division can get out of control.
Inherited gene changes
Doctors estimate that about 5 to 10 percent of breast cancers are linked to gene mutations passed through generations of a family. Certain inherited DNA mutations (changes) can dramatically increase the risk for developing certain cancers and are linked to many of the cancers that run in some families. For instance, the breast cancer genes or BRCA genes (breast cancer gene 1 = BRCA1 and breast cancer gene 2 = BRCA2) are tumor suppressor genes. When one of these breast cancer (BRCA) genes changes, it no longer suppresses abnormal cell growth, and cancer is more likely to develop. A change in one of these genes can be passed from a parent to a child.
- If you have a strong family history of breast cancer or other cancers, your doctor may recommend a blood test to help identify specific mutations in BRCA or other genes that are being passed through your family.
- Consider asking your doctor for a referral to a genetic counselor, who can review your family health history. A genetic counselor can also discuss the benefits, risks and limitations of genetic testing to assist you with shared decision-making.
Women have already begun to benefit from advances in understanding the genetic basis of breast cancer. Genetic testing can identify some women who have inherited mutations in the BRCA1 or BRCA2 tumor suppressor genes (or less commonly in other genes such as PALB2, ATM or CHEK2). These women can then take steps to reduce their risk of breast cancer and make plans to look for changes in their breasts to help find cancer at an earlier, more treatable stage. Since these mutations in BRCA 1 and BRCA 2 genes are also associated with other cancers (besides breast), women with these mutations can also consider early screening and preventive actions for other cancers.
Mutations in tumor suppressor genes like the BRCA genes are considered “high penetrance” because they often lead to cancer. Although many women with high penetrance mutations develop cancer, most cases of cancer (including breast cancer) are not caused by this kind of mutation.
More often, low-penetrance mutations or gene variations are a factor in cancer development. Each of these may have a small effect on cancer occurring in any one person, but the overall effect on the population can be large because the mutations are common, and people often have more than one at the same time. The genes involved can affect things like hormone levels, metabolism, or other things that impact risk factors for breast cancer. These genes may cause much of the risk of breast cancer that runs in families.
Acquired gene changes
Most DNA mutations related to breast cancer take place in breast cells during a woman’s life rather than having been inherited. These acquired mutations of oncogenes and/or tumor suppressor genes may result from other factors, like radiation or cancer-causing chemicals. But so far, the causes of most acquired mutations that could lead to breast cancer are still unknown. Most breast cancers have several acquired gene mutations.
Tests to spot acquired gene changes may help doctors more accurately predict the outlook (prognosis) for some women with breast cancer. For example, tests can identify women whose breast cancer cells have too many copies of the human epidermal growth factor type 2 receptor (HER2) oncogene. These cancers tend to grow and spread faster. There are drugs that target these cancer cell changes and improve outcomes for patients.
Risk factors for breast cancer
A breast cancer risk factor is anything that makes it more likely you’ll get breast cancer. But having one or even several breast cancer risk factors doesn’t necessarily mean you’ll develop breast cancer. Many women who develop breast cancer have no known risk factors other than simply being women.
Factors that are associated with an increased risk of breast cancer include 3:
- Being female. Women are much more likely than men are to develop breast cancer.
- Increasing age. Your risk of breast cancer increases as you age. Most breast cancers are found in women age 55 and older. The median age of diagnosis is slightly younger for Black women (60 years old) compared to white women 63 years old).
- Race and ethnicity. Overall, white women are slightly more likely to develop breast cancer than African American women, although the gap between them has been closing in recent years. In women under age 40, breast cancer is more common in African American women. African American women are also more likely to die from breast cancer at any age. Asian, Hispanic, and Native American women have a lower risk of developing and dying from breast cancer. Risk in different groups also varies by type of breast cancer. For example, African American women are more likely to have the less common triple-negative breast cancer.
- A personal history of having certain benign breast conditions. Women diagnosed with certain types of benign (non-cancer) breast conditions may have a higher risk of breast cancer. Some of these conditions are more closely linked to breast cancer risk than others. Doctors often divide benign breast conditions into different groups, depending on how they affect this risk.
- Non-proliferative lesions: These conditions don’t seem to affect breast cancer risk, or if they do, the increase in risk is very small. They include:
- Fibrosis and/or simple cysts (sometimes called fibrocystic changes)
- Mild hyperplasia
- Adenosis (non-sclerosing)
- Phyllodes tumor (benign)
- A single papilloma
- Fat necrosis
- Duct ectasia
- Periductal fibrosis
- Squamous and apocrine metaplasia
- Epithelial-related calcifications
- Other tumors (lipoma, hamartoma, hemangioma, neurofibroma, adenomyoepithelioma)
- Proliferative lesions without atypia (cell abnormalities): In these conditions there’s excessive growth of cells in the ducts or lobules of the breast, but the cells don’t look very abnormal. These conditions seem to raise a woman’s risk of breast cancer slightly. They include:
- Usual ductal hyperplasia (without atypia)
- Fibroadenoma
- Sclerosing adenosis
- Several papillomas (called papillomatosis)
- Radial scar
- Proliferative lesions with atypia: In these conditions, the cells in the ducts or lobules of the breast tissue grow excessively, and some of them no longer look normal. These types of lesions include:
- Atypical ductal hyperplasia (ADH)
- Atypical lobular hyperplasia (ALH)
- Breast cancer risk is about 4 to 5 times higher than normal in women with these changes. If a woman also has a family history of breast cancer and either hyperplasia or atypical hyperplasia, she has an even higher risk of breast cancer.
- Lobular carcinoma in situ (LCIS). In lobular carcinoma in situ (LCIS), cells that look like cancer cells are growing in the lobules of the milk-producing glands of the breast, but they are not growing through the wall of the lobules. LCIS is not considered to be cancer, and it typically does not spread beyond the lobule (that is, it doesn’t become invasive breast cancer) if it isn’t treated. But women with LCIS have a 7 to 12 times higher risk of developing breast cancer (which can be in either breast).
- Non-proliferative lesions: These conditions don’t seem to affect breast cancer risk, or if they do, the increase in risk is very small. They include:
- A personal history of breast cancer. If you’ve had breast cancer in one breast, you have an increased risk of developing cancer in the other breast or in another part of the same breast.
- A family history of breast cancer. About 5% to 10% of breast cancer cases are thought to be hereditary, meaning that they result directly from gene changes (mutations) passed on from a parent. If your mother, sister or daughter was diagnosed with breast cancer, particularly at a young age, your risk of breast cancer is almost double. Having 2 first-degree relatives increases her risk by about 3-fold. Women with a father or brother who has had breast cancer also have a higher risk of breast cancer. Still, the majority of people diagnosed with breast cancer have no family history of the disease.
- Inherited genes that increase cancer risk. Certain gene mutations that increase the risk of breast cancer can be passed from parents to children. The most well-known gene mutations are referred to as BRCA1 and BRCA2. In normal cells, BRCA1 and BRCA2 genes help make proteins that repair damaged DNA. Mutated versions of BRCA1 and BRCA2 genes can lead to abnormal cell growth, which can lead to cancer. These genes can greatly increase your risk of breast cancer and other cancers, but they don’t make cancer inevitable.
- If you have inherited a mutated copy of either BRCA1 or BRCA2 gene from a parent, you have a higher risk of breast cancer.
- On average, a woman with a BRCA1 or BRCA2 gene mutation has up to a 7 in 10 chance of getting breast cancer by age 80. This risk is also affected by how many other family members have had breast cancer. (It goes up if more family members are affected.)
- Women with one of these mutations are more likely to be diagnosed with breast cancer at a younger age, as well as to have cancer in both breasts.
- Women with one of these gene changes also have a higher risk of developing ovarian cancer and some other cancers. (Men who inherit one of these gene changes also have a higher risk of breast and some other cancers.)
- In the United States, BRCA mutations are more common in Jewish people of Ashkenazi (Eastern Europe) origin than in other racial and ethnic groups, but anyone can have them.
- Inherited mutations in several other genes have also been linked to breast cancer, but these account for only a small number of cases. The following gene mutations can also lead to inherited breast cancers. These gene mutations are much less common, and most of them do not increase the risk of breast cancer as much as the BRCA genes.
- ATM: The ATM gene normally helps repair damaged DNA (or helps kill the cell if the damaged can’t be fixed). Inheriting 2 abnormal copies of this gene causes the disease ataxia-telangiectasia. Inheriting one abnormal copy of this gene has been linked to a high rate of breast cancer in some families.
- PALB2: The PALB2 gene makes a protein that interacts with the protein made by the BRCA2 gene. Mutations in this gene can lead to a higher risk of breast cancer.
- TP53: The TP53 gene helps stop the growth of cells with damaged DNA. Inherited mutations of this gene cause Li-Fraumeni syndrome. People with this syndrome have an increased risk of breast cancer, as well as some other cancers such as leukemia, brain tumors, and sarcomas (cancers of bones or connective tissue). This mutation is a rare cause of breast cancer.
- CHEK2: The CHEK2 gene is another gene that normally helps with DNA repair. A CHEK2 mutation increases breast cancer risk.
- PTEN: The PTEN gene normally helps regulate cell growth. Inherited mutations in this gene can cause Cowden syndrome, a rare disorder that puts people at higher risk for both cancer and benign (non-cancer) tumors in the breasts, as well as growths in the digestive tract, thyroid, uterus, and ovaries.
- CDH1: Inherited mutations in this gene cause hereditary diffuse gastric cancer, a syndrome in which people develop a rare type of stomach cancer. Women with mutations in this gene also have an increased risk of invasive lobular breast cancer.
- STK11: Defects in this gene can lead to Peutz-Jeghers syndrome. People affected with this disorder have pigmented spots on their lips and in their mouths, polyps (abnormal growths) in the urinary and digestive tracts, and a higher risk of many types of cancer, including breast cancer.
- Radiation exposure. If you received radiation treatments to your chest as a child or young adult, your risk of breast cancer is increased. Radiation treatment in older women (after about age 40 to 45) does not seem to increase breast cancer risk.
- Being overweight or obese. Being overweight or obese after menopause increases breast cancer risk. Before menopause, a woman’s ovaries make most of her estrogen, and fat tissue makes only a small part of the total amount. After menopause (when the ovaries stop making estrogen), most estrogen comes from fat tissue. Having more fat tissue after menopause can raise estrogen levels and increase the chances of getting breast cancer. Women who are overweight also tend to have higher blood insulin levels. Higher insulin levels have been linked to some cancers, including breast cancer.
- Diabetes. Women with diabetes have a small increase in their risk of breast cancer, although scientists are not sure why.
- Not being physically active. Evidence is growing that regular physical activity reduces breast cancer risk, especially in women past menopause. The main question is how much activity is needed. Some studies have found that even as little as a couple of hours a week might be helpful, although more seems to be better. Exactly how physical activity might reduce breast cancer risk isn’t clear, but it may be due to its effects on body weight, inflammation, and hormone levels.
- Having dense breast tissue. Breasts are made up of fatty tissue, fibrous tissue, and glandular tissue. Breasts appear denser on a mammogram when they have more glandular and fibrous tissue and less fatty tissue. Women with dense breasts on mammogram have a higher risk of breast cancer than women with average breast density. Unfortunately, dense breast tissue can also make it harder to see cancers on mammograms. A number of factors can affect breast density, such as age, menopausal status, the use of certain drugs (including menopausal hormone therapy), pregnancy, and genetics.
- Beginning your period at a younger age. Beginning your period before age 12 increases your risk of breast cancer. The increase in risk may be due to a longer lifetime exposure to the hormones estrogen and progesterone.
- Beginning menopause at an older age. If you began menopause at an older age, you’re more likely to develop breast cancer. The increase in risk may be because they have a longer lifetime exposure to the hormones estrogen and progesterone.
- Having your first child at an older age. Women who give birth to their first child after age 30 may have an increased risk of breast cancer.
- Having never been pregnant. Women who have never been pregnant have a greater risk of breast cancer than do women who have had one or more pregnancies.
- Postmenopausal hormone therapy also called hormone replacement therapy (HRT) or menopausal hormone therapy. Women who take hormone therapy medications that combine estrogen and progesterone (also known as combined hormone therapy) to treat the signs and symptoms of menopause have an increased risk of breast cancer. This increase in risk is typically seen after about 4 years of use. Combined hormone therapy also increases the likelihood that the breast cancer may be found at a more advanced stage. The risk of breast cancer decreases when women stop taking these medications, although the increased risk does not go away completely.
- Estrogen therapy: Studies of the use of estrogen alone after menopause have had mixed results. Some have found a slightly higher risk, while others have found no increase in risk, or even a slight decrease in risk. If estrogen therapy does increase the risk of breast cancer, it is not by much.
- Drinking alcohol. Drinking alcohol increases the risk of breast cancer and other types of cancer. The risk increases with the amount of alcohol consumed. Women who have 1 alcoholic drink a day have a small (about 7% to 10%) increase in risk compared with those who don’t drink, while women who have 2 to 3 drinks a day have about a 20% higher risk.
- Smoking. Some studies have found that heavy tobacco smoking over a long time might be linked to a slightly higher risk of breast cancer. In some studies, the risk has been highest in certain groups, such as women who started smoking before they had their first child.
- Being taller. Many studies have found that taller women have a higher risk of breast cancer than shorter women. The reasons for this aren’t exactly clear, but it may have something to do with factors that affect early growth, such as nutrition early in life, as well as hormonal or genetic factors.
- Exposure to diethylstilbestrol (DES). From the 1940s through the early 1970s some pregnant women were given an estrogen-like drug called DES because it was thought to lower their chances of losing the baby (miscarriage). These women have a slightly increased risk of developing breast cancer. Women whose mothers took DES while they were pregnant with them may also have a slightly higher risk of breast cancer.
- Not breastfeeding. Most studies suggest that breastfeeding may slightly lower breast cancer risk, especially if it continues for a year or more. But this has been hard to study, especially in countries like the United States, where breastfeeding for this long is uncommon.
- Breast implants. Breast implants have not been linked with an increased risk of the most common types of breast cancer. However, they have been linked to a rare type of non-Hodgkin lymphoma called breast implant-associated anaplastic large cell lymphoma (BIA-ALCL), which can form in the scar tissue around the implant. This lymphoma appears to happen more often in women who have implants with textured (rough) surfaces rather than smooth surfaces. If breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) does occur after an implant, it can show up as a lump, a collection of fluid, swelling, or pain near the implant, or as a change in a breast’s size or shape.
- Birth control methods using hormones might increase breast cancer risk.
- Oral contraceptives: Most studies have found that women using oral contraceptives (birth control pills) have a slightly higher risk of breast cancer than women who have never used them. Once the pills are stopped, this risk seems to go back to normal within about 10 years.
- Birth control shots: Some studies have suggested that getting long-acting progesterone shots (such as Depo-Provera) every 3 months for birth control might increase breast cancer risk, but not all studies have found this.
- Birth control implants, intrauterine devices (IUDs), skin patches, vaginal rings: These forms of birth control also use hormones, which in theory could fuel breast cancer growth. Some studies have suggested a link between use of hormone-releasing IUDs and breast cancer risk, but few studies have looked at the use of birth control implants, patches, and rings and breast cancer risk.
Genetic testing can be done to look for inherited mutations in the BRCA1 and BRCA2 genes (or less commonly in genes such as PTEN, TP53, or others mentioned above). This might be an option for some women who have been diagnosed with breast cancer, as well as for certain women with factors that put them at higher risk for breast cancer, such as a strong family history. While genetic testing can be helpful in some cases, not every woman needs to be tested, and the pros and cons need to be considered carefully.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Breast cancer prevention
Breast cancer risk reduction for women with an average risk
Making changes in your daily life may help reduce your risk of breast cancer. Try to:
Ask your doctor about breast cancer screening. Discuss with your doctor when to begin breast cancer screening exams and tests, such as clinical breast exams and mammograms.
Talk to your doctor about the benefits and risks of screening. Together, you can decide what breast cancer screening strategies are right for you.
Become familiar with your breasts through breast self-exam for breast awareness. Women may choose to become familiar with their breasts by occasionally inspecting their breasts during a breast self-exam for breast awareness. If there is a new change, lumps or other unusual signs in your breasts, talk to your doctor promptly.
- Breast awareness can’t prevent breast cancer, but it may help you to better understand the normal changes that your breasts undergo and identify any unusual signs and symptoms.
- Avoid or limit alcohol. Alcohol increases risk of breast cancer. Even drinking small amounts of alcohol has been linked with an increase in risk. It is best not to drink alcohol at all. For women who do drink, they should have no more than 1 alcoholic drink a day. A drink is 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of 80-proof distilled spirits (hard liquor).
- Being physically active. Many studies have shown that moderate to vigorous physical activity is linked with lower breast cancer risk, so it’s important to get regular physical activity. An analysis of 35 studies found that highly active women had a 14% lower risk of developing breast cancer compared with the least active women. The American Cancer Society recommends that adults get at least 150 to 300 minutes of moderate intensity or 75 to 150 minutes of vigorous intensity activity each week (or a combination of these), preferably spread throughout the week. Getting to or exceeding the upper limit of 300 minutes is ideal.
- Breastfeeding. Breastfeeding lowers the risk of developing breast cancer, particularly if you have your children when you are younger. The longer you breastfeed the more the risk is reduced. It is not completely clear why this is. But the reduced risk might be because the ovaries don’t produce eggs so often during breastfeeding. Or it might be because breastfeeding changes the cells in the breast so they might be more resistant to changes that lead to cancer.
- Limit postmenopausal hormone therapy. Combination hormone therapy may increase the risk of breast cancer. Talk with your doctor about the benefits and risks of hormone therapy. Some women experience bothersome signs and symptoms during menopause and, for these women, the increased risk of breast cancer may be acceptable in order to relieve menopause signs and symptoms. To reduce the risk of breast cancer, use the lowest dose of hormone therapy possible for the shortest amount of time.
- Maintain a healthy weight. If your weight is healthy, work to maintain that weight. If you need to lose weight, ask your doctor about healthy strategies to accomplish this. Reduce the number of calories you eat each day and slowly increase the amount of exercise.
- Choose a healthy diet. Women who eat a Mediterranean diet supplemented with extra-virgin olive oil and mixed nuts may have a reduced risk of breast cancer. The Mediterranean diet focuses mostly on plant-based foods, such as fruits and vegetables, whole grains, legumes, and nuts. People who follow the
- Mediterranean diet choose healthy fats, such as olive oil, over butter and fish instead of red meat.
Breast cancer risk reduction for women with a high risk
If your doctor has assessed your family history and determined that you have other factors, such as a precancerous breast condition, that increase your risk of breast cancer, you may discuss options to reduce your risk, such as:
Preventive medications (chemoprevention)
Medicines such as tamoxifen and raloxifene block the action of estrogen in breast tissue. Tamoxifen might be an option even if you haven’t gone through menopause, while raloxifene is only used for women who have gone through menopause. Other drugs, called aromatase inhibitors, might also be an option for women past menopause. Aromatase inhibitors lower estrogen levels by stopping an enzyme in fat tissue called aromatase from changing other hormones into estrogen. Estrogen can fuel the growth of breast cancer cells. Aromatase inhibitors don’t stop the ovaries from making estrogen. They only lower estrogen levels in women whose ovaries aren’t making estrogen (such as women who have already gone through menopause). Because of this, they are used mainly in women who have gone through menopause already.
The aromatase inhibitors that have been shown in studies to lower breast cancer risk in postmenopausal women who are at increased risk include:
- Anastrozole (Arimidex)
- Exemestane (Aromasin)
Like tamoxifen, aromatase inhibitors are more often used to treat hormone receptor-positive breast cancer than to lower breast cancer risk.
When used to lower breast cancer risk, aromatase inhibitors are typically taken for 5 years. They are pills taken once a day.
All of these medicines can also have side effects, so it’s important to understand the possible benefits and risks of taking one of them. Doctors reserve these medications for women who have a very high risk of breast cancer. Discuss the benefits and risks with your doctor.
The most common side effects of aromatase inhibitors are symptoms of menopause, such as hot flashes, night sweats, and vaginal dryness. Aromatase inhibitors can also cause muscle and joint pain. This side effect can be serious enough to cause some women to stop taking the drugs.
Unlike tamoxifen and raloxifene, aromatase inhibitors tend to speed up bone thinning, which can lead to osteoporosis. People with osteoporosis are more likely to have broken bones. Because of this, doctors often recommend checking bone density before starting one of these drugs.
Aromatase inhibitors may raise cholesterol. Women with pre-existing heart disease who take an AI may be at higher risk of having a heart problem.
Preventive surgery
Women with a very high risk of breast cancer may choose to have their healthy breasts surgically removed (prophylactic mastectomy). They may also choose to have their healthy ovaries removed (prophylactic oophorectomy) to reduce the risk of both breast cancer and ovarian cancer. Some studies have suggested prophylactic oophorectomy might lower the risk of breast cancer as well, although not all studies have found this. Some women choose to have prophylactic oophorectomy done along with a prophylactic mastectomy. Removing the ovaries causes a woman to go into menopause. This can lead to symptoms such as hot flashes, trouble sleeping, vaginal dryness, loss of bone density, and anxiety or depression.
A prophylactic mastectomy can lower breast cancer risk by 90% or more, but it doesn’t guarantee that you will not get breast cancer. This is because it’s not possible to remove all breast cells, even with a mastectomy. The breast cells that are left behind might still go on to become cancer 4.
You might consider preventive surgery if you 4:
- Have a mutation in the BRCA1 or BRCA2 gene (or certain other genes that increase breast cancer risk) that is found by genetic testing.
- Unfortunately there’s no way to know for sure ahead of time if a woman will benefit from bilateral prophylactic mastectomy (removing both breasts before cancer is diagnosed). Most women with a BRCA1 or BRCA2 gene mutation will develop breast cancer at some point. Having a prophylactic mastectomy before the cancer develops might add many years to their lives. But not all women with BRCA1 or BRCA2 mutations develop breast cancer. For some women the surgery might not have been helpful. Although they might still get some important benefits from the surgery such as peace of mind, they would also have to deal with its aftereffects, which might include physical and emotional side effects.
- Have a strong family history of breast cancer (such as breast cancer in several close relatives, or breast cancer in at least one relative at a young age)
- Had radiation therapy to the chest before age 30
- Have (or have had) cancer in one breast (especially if you also have a strong family history)
- Some women who have already been diagnosed with breast cancer choose to have the other breast removed at the same time of surgery to remove the breast with cancer. This operation is known as a contralateral prophylactic mastectomy, can help lower their risk of developing a second breast cancer. This is more likely to be a good option for women who also have other factors that increase their risk of getting another breast cancer, such as a BRCA1 or BRCA2 mutation or a strong family history of breast cancer.
- But for women who don’t have a family history or other risk factors for breast cancer, the benefit of contralateral prophylactic mastectomy is less clear. Having breast cancer does raise your risk of getting cancer in the other breast, but this risk is still usually low, and many women overestimate this risk. And while contralateral prophylactic mastectomy lowers the risk of getting cancer in the other breast, it does not increase most women’s chances of living longer.
- Other issues might also be important when considering a contralateral prophylactic mastectomy. For example, after a mastectomy, the breasts may no longer look the same, even if a woman has breast reconstruction. Removing both breasts (possibly followed by reconstruction) can help the breasts look more symmetrical after treatment.
Like any type of surgery, a mastectomy can have risks and side effects, some of which could affect your quality of life. Because of this, preventive surgery is not usually a good option for women who are at average risk of breast cancer, or for those who are at only slightly increased risk.
For women who are known (or strongly suspected) to have a BRCA1 or BRCA2 gene mutation, a prophylactic oophorectomy (removal of the ovaries) might also be recommended as well.
Again, it’s important to talk to your health care team so that you’re well informed about the possible benefits, risks, and side effects of this type of surgery. You might also want to talk to other women who have had this surgery before deciding if it’s right for you.
Types of breast cancer
There are many types of breast cancer. The type of breast cancer is determined by the specific kind of cells in the breast that are affected. Most breast cancers are carcinomas. Carcinomas are tumors that start in the epithelial cells that line organs and tissues throughout the body. Sometimes, an even more specific term is used. For example, most breast cancers are a type of carcinoma called adenocarcinoma, which starts in cells that make up glands (glandular tissue). Breast adenocarcinomas start in the ducts (the milk ducts) or the lobules (milk-producing glands).
The most common types of breast cancer are ductal carcinoma in situ (DCIS), invasive ductal carcinoma, and invasive lobular carcinoma. The most common breast cancers such as ductal carcinoma in situ (DCIS) and invasive carcinoma are adenocarcinomas, since the cancers start in the gland cells in the milk ducts or the lobules (milk-producing glands).
Other kinds of cancers can grow in the breast, like angiosarcomas and sarcomas, which start in the cells of the muscle, fat, or connective tissue, but are not considered breast cancer since they start in different cells of the breast.
Breast cancers are also classified by certain types of proteins or genes each cancer might make. After a biopsy is done, breast cancer cells are tested for proteins called estrogen receptors and progesterone receptors, and the HER2 gene or protein. The tumor cells are also closely looked at in the lab to find out what grade it is. The specific proteins found and the tumor grade can help decide the stage of the cancer and treatment options.
Sometimes a single breast tumor can be a combination of different types. And in some very rare types of breast cancer, the cancer cells may not form a lump or tumor at all.
- Angiosarcoma
- Ductal carcinoma in situ (DCIS)
- Triple-negative breast cancer
- Inflammatory breast cancer
- Invasive lobular carcinoma
- Male breast cancer
- Paget’s disease of the breast
- Recurrent breast cancer
When a biopsy is done to find out the specific type of breast cancer, the pathologist will also check if the cancer has spread into the surrounding tissues. The following terms are used to describe the extent of the cancer:
- In situ breast cancers have not spread.
- Invasive or infiltrating cancers have spread (invaded) into the surrounding breast tissue.
Common kinds of breast cancer
The most common kinds of breast cancer are carcinomas, and are named based on where they form and how far they have spread.
Most breast cancers are carcinomas, which are tumors that start in the epithelial cells that line organs and tissues throughout the body. When carcinomas form in the breast, they are usually a more specific type called adenocarcinoma, which starts in cells in the ducts (the milk ducts) or the lobules (glands in the breast that make milk).
The type of breast cancer can also refer to whether the cancer has spread or not. In situ breast cancer (ductal carcinoma in situ or DCIS) is a pre-cancer that starts in a milk duct and has not grown into the rest of the breast tissue. The term invasive (or infiltrating) breast cancer is used to describe any type of breast cancer that has spread (invaded) into the surrounding breast tissue.
In situ cancers
Ductal Carcinoma In Situ (DCIS)
Ductal carcinoma in situ (DCIS) also known as intraductal carcinoma or Stage 0 breast cancer, is a non-invasive or pre-invasive breast cancer 5. This means the cells that line the ducts have changed to cancer cells but they have not spread through the walls of the ducts into the nearby breast tissue.
About 1 in 5 new breast cancers will be DCIS or ductal carcinoma in situ. Nearly all women with this early stage of breast cancer can be cured.
Because ductal carcinoma in situ (DCIS) hasn’t spread into the breast tissue around it, it can’t spread (metastasize) beyond the breast to other parts of the body.
DCIS is considered a pre-cancer because sometimes it can become an invasive cancer. This means that over time, DCIS may spread out of the duct into nearby tissue, and could metastasize (spread). Right now, though, there’s no good way to know for sure which will become invasive cancer and which ones won’t. So almost all women with DCIS will be treated.
In most cases, a woman with ductal carcinoma in situ (DCIS) can choose between breast-conserving surgery and simple mastectomy 6. Radiation is usually given after breast-conserving surgery. Tamoxifen or an aromatase inhibitor after surgery might also be an option if the DCIS is hormone-receptor positive 6.
Lobular carcinoma in situ (LCIS)
Lobular carcinoma in situ (LCIS) may also be called lobular neoplasia. This breast change is not a cancer, though the name can be confusing. Lobular carcinoma in situ (LCIS) is a type of breast change that is sometimes seen when a breast biopsy is done. In LCIS, cells that look like cancer cells are growing in the lining of the milk-producing glands (lobules) of the breast, but they don’t invade through the wall of the lobules.
Lobular carcinoma in situ (LCIS) is not considered to be cancer, and it typically does not spread beyond the lobule (that is, it doesn’t become invasive breast cancer) if it isn’t treated. But having LCIS does increase your risk of developing an invasive breast cancer in either breast later on, so close follow-up is important 7.
Women with LCIS have about a 7 to 12 times higher risk of developing invasive cancer in either breast. For this reason, doctors typically recommend that women with LCIS have regular breast cancer screening tests and follow-up visits with a health care provider for the rest of their lives.
LCIS and another type of breast change (atypical lobular hyperplasia) are types of lobular neoplasia. These are benign (non-cancerous) conditions, but they both increase your risk of breast cancer.
The different types of lobular carcinoma in situ (LCIS) are:
- Classic LCIS: The cells lining the lobules of the breast are smaller and are about the same size.
- Pleomorphic LCIS: The cells lining the lobules of the breast are larger and look more abnormal.
- Florid LCIS: The cells lining the lobules have grown into a large enough group that they have formed a mass, typically with an area of dead cells in the middle (called central necrosis).
Lobular carcinoma in situ (LCIS) diagnosis
Classic lobular carcinoma in situ (LCIS) usually doesn’t cause a lump that can be felt or changes that can be seen on a mammogram, although pleomorphic and florid LCIS are sometimes found this way. Most often, LCIS is found when a breast biopsy is done for another problem that’s nearby. During a biopsy, small pieces of breast tissue are removed and checked in the lab.
Lobular carcinoma in situ (LCIS) treatment
Having lobular carcinoma in situ (LCIS) does increase your risk of developing invasive breast cancer later on. But since LCIS is not a true cancer or pre-cancer, in most cases, often no treatment is needed after the biopsy 7.
Sometimes if LCIS is found using a needle biopsy, the doctor might recommend that it be removed completely (with an excisional biopsy or some other type of breast-conserving surgery) to help make sure that LCIS was the only abnormality there. This is especially true if the LCIS is described as pleomorphic or if it has necrosis (areas of dead cells), in which case it might be more likely to grow quickly.
Even after an excisional biopsy, if pleomorphic or florid LCIS is found, some doctors might recommend another, more extensive surgery to make sure it has all been removed.
Lobular carcinoma in situ (LCIS) monitoring
Close follow-up is important because women with lobular carcinoma in situ (LCIS) have the same increased risk of developing cancer in both breasts. Women should also talk to their doctor about what they can do to help reduce their breast cancer risk. Options for women at high risk of breast cancer because of LCIS may include:
- Seeing a doctor more often (such as every 6 to 12 months) for a breast exam along with the yearly mammogram. Additional imaging with breast MRI may also be recommended, especially if a woman has other factors that raise her risk of breast cancer.
- Making lifestyle changes to lower breast cancer risk.
- Taking medicine to help lower the risk of breast cancer.
- Surgery, called bilateral prophylactic mastectomy (removal of both breasts), to reduce risk. (This is more likely to be a reasonable option in women who also have other risk factors for breast cancer, such as a BRCA gene mutation.) This may be followed later by breast reconstruction.
Invasive (infiltrating) breast cancer
Breast cancers that have spread into surrounding breast tissue are known as invasive breast cancer 8.
Most breast cancers are invasive, but there are different types of invasive breast cancer. The two most common are invasive (or infiltrating) ductal carcinomas (IDC) and invasive lobular carcinoma (ILC).
Inflammatory breast cancer is also a type of invasive breast cancer.
Treatment of invasive breast cancer depends on how advanced the cancer is (the stage of the cancer) and other factors 8. Most women will have some type of surgery to remove the tumor. Depending on the type of breast cancer and how advanced it is, you might need other types of treatment as well, either before or after surgery, or sometimes both.
Invasive (infiltrating) ductal carcinoma (IDC)
Invasive (or infiltrating) ductal carcinomas (IDC) is the most common type of breast cancer. About 8 of 10 invasive breast cancers are invasive (or infiltrating) ductal carcinomas (IDC).
Invasive (or infiltrating) ductal carcinomas (IDC) starts in the cells that line a milk duct in the breast, breaks through the wall of the duct, and grows into the nearby breast tissues. At this point, it may be able to spread (metastasize) to other parts of the body through the lymph system and bloodstream.
Invasive lobular carcinoma (ILC)
Invasive lobular carcinoma (ILC) starts in the milk-producing glands (lobules). Like IDC, it can spread (metastasize) to other parts of the body. About 1 invasive breast cancer in 10 is an invasive lobular carcinoma (ILC). Invasive lobular carcinoma (ILC) may be harder to detect on physical exam as well as imaging, like mammograms, than invasive ductal carcinoma (IDC). And compared to other kinds of invasive carcinoma, about 1 in 5 women with ILC might have cancer in both breasts at the time they are diagnosed.
Special types of invasive breast cancer
There are some special types of breast cancer that are sub-types of invasive carcinoma. They are much less common than the breast cancers named above and each typically make up fewer than 5% of all breast cancers. These are often named after features seen when they are viewed under the microscope, like the ways the cells are arranged.
Some of these may have a better prognosis than standard invasive infiltrating ductal carcinoma (IDC). These include:
- Adenoid cystic (or adenocystic) carcinoma
- Low-grade adenosquamous carcinoma (this is a type of metaplastic carcinoma)
- Medullary carcinoma
- Mucinous (or colloid) carcinoma
- Papillary carcinoma
- Tubular carcinoma
Some sub-types have the same or maybe worse prognoses than standard invasive infiltrating ductal carcinoma. These include:
- Metaplastic carcinoma (most types, including spindle cell and squamous, except low grade adenosquamous carcinoma)
- Micropapillary carcinoma
- Mixed carcinoma (has features of both invasive ductal and lobular)
In general, all of these sub-types are still treated like standard invasive infiltrating ductal carcinoma.
Inflammatory breast cancer
Inflammatory breast cancer (IBC) is rare. Inflammatory breast cancer accounts for about 1% to 5% of all breast cancers. Inflammatory breast cancer differs from other types of breast cancer in its symptoms, outlook, and treatment. Symptoms include breast swelling, purple or red color of the skin, and pitting or thickening of the skin of the breast so that it may look and feel like an orange peel. Often, a lump is not felt. If you have any of these symptoms, it does not mean that you have inflammatory breast cancer, but you should see a doctor right away.
Inflammatory breast cancer has some symptoms of inflammation like swelling and redness. But infection or injury do not cause inflammatory breast cancer or the symptoms. Inflammatory breast cancer symptoms are caused by cancer cells blocking lymph vessels in the skin.
Inflammatory breast cancer differs from other types of breast cancer in several key ways:
- Inflammatory breast cancer doesn’t look like a typical breast cancer. It often does not cause a breast lump, and it might not show up on a mammogram. This makes it harder to diagnose.
- Inflammatory breast cancer tends to occur in younger women (younger than 40 years of age).
- Women with inflammatory breast cancer tend to have a worse prognosis (outcome) than women with other common types of breast cancer.
- African-American women appear to be at higher risk of inflammatory breast cancer than white women.
- Inflammatory breast cancer is more common among women who are overweight or obese.
- Inflammatory breast cancer also tends to be more aggressive—it grows and spreads much more quickly—than more common types of breast cancer.
- Inflammatory breast cancer is always at a locally advanced stage when it’s first diagnosed because the breast cancer cells have grown into the skin. (This means it at least stage 3.)
- In about 1 of every 3 cases, inflammatory breast cancer has already spread (metastasized) to distant parts of the body when it is diagnosed. This makes it harder to treat successfully.
Inflammatory breast cancer signs and symptoms
Inflammatory breast cancer (IBC) causes a number of signs and symptoms, most of which develop quickly (withing 3-6 months), including:
- Thickening (edema/swelling) of the skin of the breast
- Redness involving more than one-third of the breast
- Pitting or thickening of the skin of the breast so that it may look and feel like an orange peel
- A retracted or inverted nipple
- One breast looking larger than the other because of swelling
- One breast feeling warmer and heavier than the other
- A breast that may also be tender, painful or itchy
- Swelling of the lymph nodes under the arms or near the collarbone
If you have any of these symptoms, it does not mean that you have inflammatory breast cancer, but you should see a doctor right away. Tenderness, redness, warmth, and itching are also common symptoms of a breast infection or inflammation, such as mastitis if you’re pregnant or breastfeeding. Because these problems are much more common than inflammatory breast cancer, your doctor might at first suspect infection as a cause and treat you with antibiotics.
This may be a good first step, but if your symptoms don’t get better in 7 to 10 days, more tests need to be done to look for cancer. The possibility of inflammatory breast cancer should be considered more strongly if you have these symptoms and are not pregnant or breastfeeding, or have been through menopause.
Inflammatory breast cancer grows and spreads quickly, so the cancer may have already spread to nearby lymph nodes by the time symptoms are noticed. This spread can cause swollen lymph nodes under your arm or above your collar bone. If the diagnosis is delayed, the cancer can spread to lymph nodes in your chest or to distant sites.
If you have any of these symptoms, it does not mean that you have inflammatory breast cancer, but you should see a doctor right away. If treatment with antibiotics is started, you’ll need to let your doctor know if it doesn’t help, especially if the symptoms get worse or the affected area gets larger. Ask to see a specialist (like a breast surgeon) or you might want to get a second opinion if you’re concerned.
Inflammatory breast cancer stages
All Inflammatory breast cancers start as Stage 3 since they involve the skin. If the cancer has spread to lymph nodes around the collarbone or inside the chest, it’s stage 3C. Cancer that has spread outside the breast and nearby lymph nodes is stage 4.
Inflammatory breast cancer survival rates
Inflammatory breast cancer (IBC) is considered an aggressive cancer because it grows quickly, is more likely to have spread at the time it’s found, and is more likely to come back after treatment than other types of breast cancer. The outlook is generally not as good as it is for other types of breast cancer.
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they cannot predict what will happen in any particular person’s case. Many other factors can affect a person’s outlook, such as age, general health, treatment received, and how well the cancer responds to treatment. Your doctor can tell you how the numbers below may apply to you, as he or she is familiar with your situation.
These survival rates are based on people diagnosed years ago. Improvements in treatment since then may result in a more favorable outlook for people now being diagnosed with inflammatory breast cancer.
These numbers are based on data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, for patients who were diagnosed with inflammatory breast cancer between 1990 and 2008.
Median survival is the length of time for half of the patients in a group to have died. By definition, half of the patients in that group are still alive. It is important to remember that the median is just a kind of average used by researchers. No one is “average” and many people have much better outcomes than the median. Also, people with inflammatory breast cancer can die of other things, and these numbers don’t take that into account.
- The median survival rate for people with stage III inflammatory breast cancer is about 57 months.
- The median survival rate for people with stage IV inflammatory breast cancer is about 21 months.
Triple-negative breast cancer
Triple-negative breast cancer refers to the fact that the breast cancer cells don’t have estrogen or progesterone receptors (ER or PR) and also don’t make any or too much of the human epidermal growth factor type 2 (HER2). The breast cancer cells test “negative” on all 3 tests (negative estrogen receptor [ER], progesterone receptor [PR] and human epidermal growth factor type 2 receptor [HER2 receptor]). Your doctor uses a sample of your cancer to test the cells for these receptors. You might have this testing following a biopsy of the cancer, or after surgery to remove it. Many breast cancers have receptors for one or more of these substances (estrogen, progesterone and HER2). But triple negative breast cancers don’t have any of them. Triple-negative breast cancer accounts for about 10-15% of all breast cancers. Triple-negative breast cancers tend to be more common in women younger than age 40, who are Black, or who have a BRCA1 gene mutation 9. The BRCA1 gene is one of the gene faults that can increase the risk of breast cancer within families.
Triple-negative breast cancer differs from other types of invasive breast cancer in that it tends to grow and spread faster, has fewer treatment options, and tends to have a worse prognosis (outcome).
A rare type of breast cancer known as basal type breast cancer is usually triple negative. Some men have triple negative breast cancer but this is very rare. Most men have estrogen receptors in their cancer cells.
Triple-negative breast cancer has fewer treatment options than other types of invasive breast cancer. This is because the cancer cells do not have the estrogen or progesterone receptors or enough of the HER2 protein to make hormone therapy or targeted HER2 drugs work. Hormone treatment and the targeted cancer drug trastuzumab (Herceptin) don’t work for people with triple negative breast cancer. Because hormone therapy and anti-HER2 drugs are not choices for women with triple-negative breast cancer, chemotherapy is often used.
Triple-negative breast cancer signs and symptoms
Triple-negative breast cancer can have the same signs and symptoms as other common types of breast cancer.
Symptoms can include:
- a new lump or thickening in your breast or armpit
- a change in size, shape or feel of your breast
- skin changes in the breast such as puckering, dimpling, a rash or redness of the skin
- fluid leaking from the nipple in a woman who isn’t pregnant or breast feeding
- changes in the position of nipple
Triple-negative breast cancer diagnosis
Once a breast cancer diagnosis has been made using imaging tests and a biopsy, the cancer cells will be checked for certain proteins. If the cells do not have estrogen or progesterone receptors (ER or PR), and also do not make any or too much of the HER2 protein, the cancer is considered to be triple-negative breast cancer.
Triple-negative breast cancer treatment
The main treatments for triple negative breast cancer are surgery, chemotherapy and radiotherapy. The treatment you need depends on:
- where the cancer is
- the size of the cancer and whether it has spread (the stage)
- how abnormal the cells look under the microscope (the grade)
- your general health
If the cancer has not spread to distant sites, surgery is an option. You might have surgery to remove:
- an area of the breast (called breast conserving surgery)
- the whole breast (called mastectomy)
When you have your surgery, the surgeon usually takes out some of the lymph nodes under your arm. They test these nodes to see if they contain cancer cells. The surgeon might check the lymph nodes closest to the breast using a procedure called sentinel lymph node biopsy. Testing the lymph nodes helps to find the stage of the cancer and decide on further treatment.
Chemotherapy might be given first to shrink a large tumor, followed by surgery. Chemotherapy is often recommended after surgery to reduce the chances of the cancer coming back. Radiation might also be an option depending on certain features of the tumor and the type of surgery you had.
After breast conserving surgery you usually have radiotherapy to the rest of the breast tissue.
In cases where the cancer has spread to other parts of the body (stage 4), platinum chemotherapy, targeted drugs like a PARP inhibitor, or antibody-drug conjugate, or immunotherapy with chemotherapy might be considered.
Stages 1 to 3 triple-negative breast cancer
Surgery first: If the early-stage triple negative breast cancer tumor is small enough to be removed by surgery, then breast-conserving surgery or a mastectomy with a check of the lymph nodes may be done In certain cases, such as with a large tumor or if the lymph nodes are found to have cancer, radiation may follow surgery. You might also be given chemo after surgery (adjuvant chemotherapy) to reduce the chances of the cancer coming back. For women who have a BRCA mutation and at surgery are found to have 10:
- A tumor larger than 2cm but no bigger than 5cm
- OR
- 1 to 3 axillary (underarm) lymph nodes with cancer
The targeted drug olaparib (Lynparza) might be given for a year after adjuvant chemo. When given this way, it can help some women live longer.
Surgery second: Chemo is often given before surgery (neoadjuvant chemotherapy) by itself or with pembrolizumab (Keytruda) to shrink a large tumor and/or lymph nodes with cancer. If cancer is still found in the tissue removed by surgery after neoadjuvant chemo has been given, your doctor may recommend 10:
- an oral chemo drug called capecitabine (Xeloda) for 18 to 24 weeks. This might help some women live longer.
- more pembrolizumab after surgery (adjuvant treatment) to reduce the chances of the cancer coming back.
- the targeted drug olaparib for one year for women who have a BRCA mutation to help lower the chance of the cancer recurring. When given this way, it can help some women live longer.
Stage 4 triple-negative breast cancer
Chemo is often used first when the cancer has spread to other parts of the body (stage 4) 10. Common chemo drugs used include anthracyclines, taxanes, capecitabine, gemcitabine, eribulin, and others. Chemo drugs might be used alone or in combination.
For women with triple negative breast cancer who have a BRCA mutation and whose cancer no longer responds to common breast cancer chemo drugs, other platinum chemo drugs (like cisplatin or carboplatin) or targeted drugs called PARP inhibitors (such as olaparib [Lynparza] or talazoparib [Talzenna]), may be considered.
For advanced triple negative breast cancer in which the cancer cells have the PD-L1 protein, the first treatment may be immunotherapy (pembrolizumab) plus chemo . The PD-L1 protein is found in about 1 out of 5 triple negative breast cancers.
For advanced triple negative breast cancer in which at least 2 other drug treatments have already been tried, the antibody-drug conjugate sacituzumab govitecan (Trodelvy) might be an option.
For advanced triple negative breast cancer in which the cancer cells show high levels of gene changes called microsatellite instability (MSI) or changes in any of the mismatch repair (MMR) genes (MLH1, MSH2, MSH6, and PMS2), immunotherapy with the drug pembrolizumab might be used. Pembrolizumab might also be an option for triple negative breast cancer that has a high tumor mutational burden (TMB-H) which is a measure of the number of gene mutations (changes) inside the cancer cells. Cells that have many gene mutations (a high TMB) might be more likely to be recognized as abnormal and attacked by the body’s immune system.
Recurrent triple-negative breast cancer
If triple negative breast cancer comes back (recurs) locally, cannot be removed with surgery, and makes the PD-L1 protein, immunotherapy with the drug pembrolizumab along with chemotherapy is an option. Other treatments might be options as well, depending on the situation.
If the cancer recurs in other parts of the body, options might include chemotherapy or the antibody-drug conjugate sacituzumab govitecan (Trodelvy).
Regardless of the stage of the cancer, participation in a clinical trial of new treatments for triple negative breast cancer is also a good option because triple negative breast cancer is uncommon and tends to have a poor prognosis (outcome) compared to other types of breast cancer, and because these studies often allow patients to have access to drugs not available for standard treatment.
Triple-negative breast cancer survival rates
Triple-negative breast cancer is considered an aggressive cancer because it grows quickly, is more likely to have spread at the time it’s found, and is more likely to come back after treatment than other types of breast cancer 9. The outlook (prognosis) is generally not as good as it is for other types of breast cancer.
Survival rates can give you an idea of what percentage of people with the same type and stage of cancer are still alive a certain amount of time (usually 5 years) after they were diagnosed. They can’t tell you how long you will live, but they may help give you a better understanding of how likely it is that your treatment will be successful.
Keep in mind that survival rates are estimates and are often based on previous outcomes of large numbers of people who had a specific cancer, but they can’t predict what will happen in any particular person’s case. These statistics can be confusing and may lead you to have more questions. Talk with your doctor about how these numbers may apply to you, as they are familiar with your situation.
5-year relative survival rates for triple-negative breast cancer 9:
- Localized disease: 91%
- Regional disease: 65%
- Distant disease: 12%
- All stages combined: 77%
The National Cancer Institute’s Surveillance, Epidemiology, and End Results [SEER]) stages definition:
- Localized disease: There is no sign that the cancer has spread outside of the breast.
- Regional disease: The cancer has spread outside the breast to nearby structures or lymph nodes.
- Distant disease: The cancer has spread to distant parts of the body such as the lungs, liver or bones.
Paget disease of the nipple
Paget disease of the nipple starts in the breast ducts and spreads to the skin of the nipple and then to the areola (the dark circle around the nipple). Paget disease of the breast is rare, accounting for only about 1-3% of all cases of breast cancer. Paget disease usually affects only one breast. In 80-90% of cases, it’s usually found along with either ductal carcinoma in situ (DCIS) or infiltrating ductal carcinoma (invasive breast cancer).
Paget disease of the breast signs and symptoms
The skin of the nipple and areola often looks crusted, scaly, and red. There may be blood or yellow fluid coming out of the nipple. Sometimes the nipple looks flat or inverted. It also might burn or itch. Your doctor might try to treat this as eczema first, and if it does not improve, recommend a biopsy.
Paget disease of the breast diagnosis
Most people with Paget disease of the breast also have tumors in the same breast. One or more of the following imaging tests may be done to check for other breast changes:
- Diagnostic mammogram
- Breast ultrasound
- Breast MRI (magnetic resonance imaging) scan
Paget disease of the breast is diagnosed by a biopsy, removing a small piece of the breast tissue and looking at it closely in the lab. In some cases, the entire nipple may be removed. Only a biopsy can show for sure that it is cancer.
Paget disease of the breast treatment
Paget disease of the breast can be treated by removing the entire breast (mastectomy) or breast-conserving surgery followed by whole-breast radiation therapy. If breast-conserving surgery is done, the entire nipple and areola area also needs to be removed. If invasive cancer is found, the lymph nodes under the arm will be checked for cancer.
If no lump is felt in the breast tissue, and your biopsy results show the cancer has not spread within the breast tissue, the outlook (prognosis) is excellent.
If the cancer has spread within the breast tissue (is invasive), the outlook is not as good, and the cancer will be staged and treated like any other invasive ductal carcinoma (IDC).
Phyllodes tumors of the breast
Phyllodes tumors also called or phylloides tumors, are rare breast tumors start in the connective (stromal) tissue of the breast, in contrast to carcinomas, which develop in the ducts or lobules 11. Phyllodes tumors are most common in women in their 40s, but women of any age can have them. Women with Li-Fraumeni syndrome (a rare, inherited genetic condition) have an increased risk for phyllodes tumors.
Phyllodes tumors are often divided into 3 groups, based on how they look under a microscope 11:
- Benign (non-cancerous) phyllodes tumors account for more than half of all phyllodes tumors. These tumors are the least likely to grow quickly or to spread.
- Borderline phyllodes tumors have features in between benign and malignant (cancerous) tumors.
- Malignant (cancerous) phyllodes tumors also called cystosarcoma phyllodes account for about 1 in 4 phyllodes tumors. These tend to grow the fastest and are the most likely to spread or to come back after treatment.
Having a phyllodes tumor does not affect your breast cancer risk. Still, you may be watched more closely and get regular imaging tests after treatment for a phyloodes tumor, because these tumors can sometimes come back after surgery.
Phyllodes tumors of the breast signs and symptoms
Phyllodes tumors are usually felt as a firm, painless breast lump, but some may hurt. They tend to grow large fairly quickly, and they often stretch the skin.
Phyllodes tumors of the breast diagnosis
Sometimes phyllodes tumors are seen first on an imaging test (like an ultrasound or mammogram), in which case they’re often hard to tell apart from fibroadenomas (common, non-cancerous breast tumors made up of both glandular tissue and stromal (connective) tissue).
Phyllodes tumors diagnosis can often be made with a core needle biopsy, but sometimes the entire tumor needs to be removed (during an excisional biopsy) to know for sure that it’s a phyllodes tumor, and whether it’s malignant or not.
Phyllodes tumors of the breast treatment
Phyllodes tumors typically need to be removed completely with surgery. Sometimes you might also have radiotherapy or chemotherapy.
If phyllodes tumor is found to be benign, an excisional biopsy might be all that is needed, as long as the tumor was removed completely.
If phyllodes tumor is borderline or malignant, a wider margin (area of normal tissue around the tumor) usually needs to be removed as well. This might be done with breast-conserving surgery (lumpectomy or partial mastectomy), in which part of the breast is removed. Or the entire breast might be removed with a mastectomy, especially if a margin of normal breast tissue can’t be taken out with breast-conserving surgery. Radiation therapy might be given to the area after surgery, especially if it’s not clear that all of the tumor was removed.
Malignant phyllodes tumors are different from the more common types of breast cancer. They are less likely to respond to some of the treatments commonly used for breast cancer, such as the hormone therapy or chemotherapy drugs normally used for breast cancer. Phyllodes tumors that have spread to other parts of the body are often treated more like sarcomas (soft-tissue cancers) than breast cancers.
Phyllodes tumors can sometimes come back in the same place. Because of this, close follow-up with frequent breast exams and imaging tests are usually recommended after treatment.
Angiosarcoma of the breast
Angiosarcoma of the breast is very rare making up less than 1% of all breast cancers. Angiosarcoma starts in cells that line blood vessels or lymph vessels. It can involve the breast tissue or the skin of the breast. Breast angiosarcoma is mostly seen in women, but men can also get this type of breast cancer. Some may be related to prior radiation therapy in that area. Many times angiosarcoma a complication of previous radiation treatment to the breast. It can happen 8-10 years after getting radiation treatment to the breast.
Angiosarcoma of the breast are divided into:
- Primary angiosarcoma
- Secondary angiosarcoma
Primary angiosarcoma of the breast starts in the breast tissue and may involve the skin of the breast. They tend to develop in younger women in their 30s or 40s.
Most secondary angiosarcomas of the breast occur due to having radiotherapy to the breast for a previous breast cancer. These cancers usually develop in older women.
Angiosarcomas tend to grow quickly and are generally difficult to treat.
Angiosarcoma of the breast signs and symptoms
Angiosarcoma can cause skin changes like purple colored nodules and/or a lump in the breast. It can also occur in the affected arms of women with lymphedema, but this is not common. Lymphedema is swelling that can develop after surgery or radiation therapy to treat breast cancer.
Angiosarcoma of the breast diagnosis
In some women breast angiosarcoma is found during breast screening. One or more of the following imaging tests may be done to check for breast changes:
- Diagnostic mammogram
- Breast ultrasound
- Breast MRI (magnetic resonance imaging) scan
Angiosarcoma is diagnosed by a biopsy, removing a small piece of the breast tissue and looking at it closely in the lab. Only a biopsy can tell for sure that it is cancer.
Angiosarcoma of the breast treatment
Angiosarcomas tend to grow and spread quickly. Angiosarcoma of the breast treatment usually includes surgery to remove the breast (mastectomy). You may also have a sentinel lymph node biopsy. This depends on whether there are abnormal lymph nodes in the armpit (axilla).
You might have chemotherapy or targeted drugs. The choice of chemotherapy drugs might be different from those usually used to treat other types of breast cancer.
Radiation might be given in certain cases of angiosarcomas that are not related to prior breast radiation.
Breast cancer in Men
Male breast cancer is a rare cancer that forms in the breast tissue of men. Though breast cancer is most commonly thought of as a woman’s disease, male breast cancer does occur. Male breast cancer is most common in older men, though it can occur at any age.
The American Cancer Society estimates for breast cancer in men in the United States for 2022 are 12:
- About 2,710 new cases of invasive breast cancer will be diagnosed
- About 530 men will die from breast cancer
Breast cancer is about 100 times less common among white men than among white women. Breast cancer is about 70 times less common among Black men than Black women. As in Black women, Black men with breast cancer tend to have a worse prognosis (outlook). For men, the lifetime risk of getting breast cancer is about 1 in 833 13.
Men diagnosed with male breast cancer at an early stage have a good chance for a cure. Still, many men delay seeing their doctors if they notice one of the usual signs or symptoms, such as a breast lump. For this reason, many male breast cancers are diagnosed when the disease is more advanced.
Types of breast cancer in men
Types of breast cancer diagnosed in men include:
- Cancer that begins in the milk ducts (ductal carcinoma). Nearly all male breast cancer is ductal carcinoma.
- Ductal carcinoma in situ (DCIS) also known as intraductal carcinoma, is considered non-invasive or pre-invasive breast cancer. In DCIS (intraductal carcinoma), cells that lined the ducts have changed to look like cancer cells. The difference between ductal carcinoma in situ (DCIS) and invasive cancer is that the cells have not spread (invaded) through the walls of the ducts into the surrounding tissue of the breast (or spread outside the breast). Ductal carcinoma in situ (DCIS) is considered a pre-cancer because some cases can go on to become invasive cancers. Right now, though, there is no good way to know for certain which cases will go on to become invasive cancers and which ones won’t. DCIS (intraductal carcinoma) accounts for about 1 in 10 cases of breast cancer in men. It is almost always curable with surgery.
- Lobular carcinoma in situ (LCIS) is also called lobular neoplasia. In lobular carcinoma in situ (LCIS), cells that look like cancer cells are growing in the lobules of the milk-producing glands of the breast, but they haven’t grown through the wall of the lobules. Lobular carcinoma in situ (LCIS) is not a true pre-invasive cancer because it does not turn into an invasive cancer if left untreated, but it is linked to an increased risk of invasive cancer in both breasts. LCIS is rarely, if ever seen in men.
- Infiltrating (or invasive) ductal carcinoma is the most common type of breast cancer. Invasive (or infiltrating) ductal carcinoma (IDC) starts in a milk duct of the breast, breaks through the wall of the duct, and grows into the fatty tissue of the breast. Once it breaks through the wall of the duct, it has the potential to spread to other parts of the body. At this point, it may be able to spread (metastasize) to other parts of the body through the lymphatic system and bloodstream. At least 8 out of 10 male breast cancers are invasive (or infiltrating) ductal carcinomas (alone or mixed with other types of invasive or in situ breast cancer). Because the male breast is much smaller than the female breast, all male breast cancers start relatively close to the nipple, so they are more likely to spread to the nipple. This is different from Paget disease as described below.
- Cancer that begins in the milk-producing glands (lobular carcinoma). Infiltrating (or invasive) lobular carcinoma (ILC) starts in the milk-producing glands (lobules). Like the invasive (or infiltrating) ductal carcinoma (IDC), infiltrating (or invasive) lobular carcinoma (ILC) can spread to other parts of the breast and body. Infiltrating (or invasive) lobular carcinoma (ILC) is very rare in men, accounting for only about 2% of male breast cancers. This is because men do not usually have much lobular (glandular) breast tissue.
- Cancer that spreads to the nipple (Paget’s disease of the nipple). It may also spread to the areola (the dark circle around the nipple). Rarely, male breast cancer forms in the milk ducts and spreads to the nipple, causing crusty, scaly skin around the nipple with areas of redness, itching, oozing, burning, or bleeding. There may also be an underlying lump in the breast. Paget disease may be associated with ductal carcinoma in situ (DCIS) or with infiltrating ductal carcinoma. Paget’s disease of the nipple is rare and accounts for about 1-3% of female breast cancers and a higher percentage (5%) of male breast cancers.
- Inflammatory breast cancer. Inflammatory breast cancer is an aggressive, but rare type of breast cancer. It makes the breast swollen, red, warm and tender rather than forming a lump. It can be mistaken for an infection of the breast. This is very rare in men. See Inflammatory Breast Cancer for more information.
There are some special types of breast cancer that are sub-types of invasive carcinoma. They are much less common than the breast cancers named above.
Some of these may have a better or worse prognosis than standard infiltrating ductal carcinoma 14.
- Adenoid cystic (or adenocystic) carcinoma
- Low-grade adenosquamous carcinoma (this is a type of metaplastic carcinoma)
- Medullary carcinoma
- Mucinous (or colloid) carcinoma
- Papillary carcinoma
- Tubular carcinoma
- Metaplastic carcinoma (including spindle cell and squamous, except low grade adenosquamous carcinoma)
- Micropapillary carcinoma
- Mixed carcinoma (has features of both invasive ductal and lobular)
In general, these sub-types are still treated like standard infiltrating carcinoma.
Where breast cancer begins in men
Everyone is born with a small amount of breast tissue. Breast tissue consists of milk-producing glands (lobules), ducts that carry milk to the nipples, and fat.
During puberty, women begin developing more breast tissue, and men do not. But because men are born with a small amount of breast tissue, they can develop breast cancer.
Most breast cancers begin in the ducts that carry milk to the nipple (ductal cancers or ductal carcinomas). Some start in the glands that make breast milk (lobular cancers or lobular carcinomas). Men have these ducts and glands, too, even though they aren’t normally functional. There are also types of breast cancer that start in other types of breast cells, but these are less common.
A small number of cancers start in other tissues in the breast. These cancers are called sarcomas and lymphomas and are not really thought of as breast cancers.
Although many types of breast cancer can cause a lump in the breast, not all do. There are other symptoms of breast cancer you should watch for and report to your doctor.
It’s also important to understand that most breast lumps are benign and not cancer (malignant). Benign breast tumors are abnormal growths, but they do not spread outside of the breast and they are not life threatening. Any breast lump or change needs to be checked by a health care provider to determine whether it is benign or malignant (cancer) and whether it might impact your future cancer risk.
Male breast cancer symptoms
Signs and symptoms of male breast cancer can include:
- A lump or thickening in your breast tissue that is nearly always painless
- Changes to the skin covering your breast, such as dimpling, puckering, redness or scaling
- Changes to your nipple, such as redness or scaling, or a nipple that begins to turn inward into the breast (called nipple retraction)
- Discharge from your nipple that may be blood stained
- Skin dimpling or puckering
- Nipple retraction (turning inward)
- Redness or scaling of the nipple or breast skin
- swelling of the breast (gynecomastia)
- Sore (ulcer) in the skin of the breast
- Lump or swelling under the arm
- Rash on or around the nipple
Sometimes a breast cancer can spread to lymph nodes under the arm or around the collar bone and cause a lump or swelling there, even before the original tumor in the breast is large enough to be felt.
These changes aren’t always caused by cancer, but if you notice any breast changes, you should see a health care professional as soon as possible.
Breast cancer in men causes
It’s not clear what causes male breast cancer.
Doctors know that male breast cancer occurs when some breast cells divide more rapidly than healthy cells do. The accumulating cells form a tumor that may spread (metastasize) to nearby tissue, to the lymph nodes or to other parts of the body.
Inherited genes that increase male breast cancer risk
Some men inherit abnormal (mutated) genes from their parents that increase the risk of breast cancer. Mutations (defects) in one of several genes, especially a gene called BRCA2, put you at greater risk of developing breast and prostate cancers. Men with a mutation in the BRCA2 gene have a lifetime risk of about 6 in 100. BRCA1 mutations can also cause breast cancer in men, but the risk is lower, about 1 in 100.
These genes (BRCA1 and BRCA2) normally make proteins that keep cells from growing abnormally — which helps prevent cancer. But mutated BRCA1 and BRCA2 genes aren’t as effective at protecting you from cancer.
Although mutations in BRCA1 and BRCA2 genes most often are found in members of families with many cases of breast and/or ovarian cancer, they have also been found in men with breast cancer who did not have a strong family history.
Mutations in CHEK2, PTEN and PALB2 genes might also be responsible for some breast cancers in men.
Meeting with a genetic counselor and undergoing genetic testing can determine whether you carry gene mutations that increase your risk of breast cancer — and if you can pass this gene along to your children, both boys and girls. Discuss the benefits and risks of genetic testing with your doctor.
Risk factors for breast cancer in men
Factors that increase the risk of male breast cancer include:
- Older age. Your risk of male breast cancer increases as you age. The peak incidence of male breast cancer occurs between the ages of 68 and 71. On average, men with breast cancer are about 72 years old when they are diagnosed.
- Exposure to estrogen. If you take estrogen-related drugs, such as those used as part of a sex-change procedure or for hormone therapy for prostate cancer, your risk of breast cancer is increased. There is concern that transgender/transsexual individuals who take high doses of estrogens as part of sex reassignment could also have a higher breast cancer risk. Still, there haven’t been any studies of breast cancer risk in transgendered individuals, so it isn’t clear what their breast cancer risk is.
- Family history of breast cancer. If you have a close family member with breast cancer, you have a greater chance of developing the disease. About 1 out of 5 men with breast cancer have a close relative, male or female, with breast cancer.
- Klinefelter’s syndrome (47 XXY or XXY male). This genetic syndrome occurs when a boy is born with more than one copy of the X chromosome, resulting in a 47,XXY karyotype. Klinefelter’s syndrome common physical features may include tall stature, reduced muscle tone, small testes (hypogonadism), delayed pubertal development and lack of secondary male sex characteristics such as decreased facial and body hair. Increased breast growth (gynecomastia) may occur later in puberty without appropriate biological care. Because of the abnormal development of the testicles, men with Klinefelter syndrome produce lower levels of certain male hormones (androgens) and more female hormones (estrogens). Klinefelter syndrome treatments include testosterone replacement therapy and breast reduction surgery. If needed, physical, speech, language, and occupational therapy may also help.
- Heavy drinking of alcoholic beverages increases the risk of breast cancer in men. This may be because of its effects on the liver.
- Liver disease. Certain conditions, such as cirrhosis of the liver, can reduce male hormones (androgens) and increase female hormones (estrogen), increasing your risk of breast cancer. Men with liver disease can also have a higher chance of developing benign male breast growth (gynecomastia) and also have an higher risk of developing breast cancer.
- Obesity. Fat cells convert androgens into estrogen. A higher number of fat cells in your body may result in increased estrogen and higher risk of breast cancer.
- Radiation exposure. If you’ve received radiation treatments to your chest, such as those used to treat cancers in the chest (like lymphoma), you’re more likely to develop breast cancer later in life.
- Testicle disease or surgery. Having inflamed testicles (orchitis), undescended testicle (cryptorchidism) or surgery to remove a testicle (orchiectomy) can increase your risk of male breast cancer.
Diagnosing male breast cancer
Your doctor may conduct a number of diagnostic tests and procedures, such as:
- Clinical breast exam. The doctor uses his or her fingertips to examine your breasts and surrounding areas for lumps or other changes. Your doctor assesses how large the lumps are, how they feel, and how close they are to your skin and muscles.
- Imaging tests. Mammogram and ultrasound can detect suspicious masses in your breast tissue.
- A mammogram is a low dose x-ray exam of the breast that allows doctors to look for changes in breast tissue. It is called a diagnostic mammogram when it is done because problems are present. A mammogram uses a machine designed to look only at breast tissue. The breast is pressed between 2 plates to flatten and spread the tissue. The compression only lasts a few seconds and may be uncomfortable briefly, but it is necessary to get a better picture. In some cases, special images known as cone or spot views with magnification are taken to make a small area of abnormal breast tissue easier to evaluate. The results of this test might suggest that a biopsy is needed to tell if the abnormal area is cancer. Mammography is often more accurate in men than women, since men do not have dense breasts or other common breast changes that might interfere with the test.
- Breast ultrasound uses sound waves to make a computer picture of the inside of the breast. Breast ultrasound is often used to look at breast changes that are found during a mammogram or physical exam. It is useful because it can often tell the difference between fluid-filled cysts (which are unlikely to be cancer) and solid masses (which might need further testing to be sure they’re not cancer). A gel is put on the skin of the breast, and a wand-like instrument called a transducer is moved over the skin. The transducer sends out sound waves and picks up the echoes as they bounce off body tissues. The echoes are made into a picture on a computer screen. You might feel some pressure as the transducer is moved across the breast, but it should not be painful.
- Breast biopsy. A fine needle is inserted into the breast to remove tissue for analysis in the laboratory. Test results can reveal whether you have breast cancer and if so, the type of breast cancer you have. If your doctor thinks you don’t need a biopsy, but you still feel there’s something wrong with your breast, follow your instincts. Don’t be afraid to talk to your doctor about this or go to another doctor for a second opinion. A biopsy is the only sure way to diagnose breast cancer.
- There are different types of breast biopsies. The type you have depends on your situation.
- Fine needle aspiration biopsy (FNA): This type of biopsy is often used to look for cancer spread in the nearby lymph nodes. The doctor uses a very thin, hollow needle attached to a syringe to withdraw (aspirate) a small amount of tissue or fluid from a suspicious area. A local anesthetic (numbing medicine) may or may not be used. The biopsy sample is then checked to see if there are cancer cells in it. If the area to be biopsied can be felt, the needle can be guided into it while the doctor is feeling it. If the lump can’t be felt easily, the doctor might watch the needle on an ultrasound screen as it moves into the area. This is called an ultrasound-guided biopsy. A fine needle aspiration biopsy is the easiest type of biopsy to have, but it can sometimes miss a cancer if the needle does not go into the cancer cells. If the results of the fine needle aspiration biopsy do not give a clear diagnosis, or your doctor still has concerns, you might need to have a second biopsy or a different type of biopsy.
- Core needle biopsy (CNB): This is the most common type of biopsy used to make a breast cancer diagnosis. The doctor uses a wide, hollow needle to take out pieces of breast tissue from a suspicious area. The needle used in this technique is larger than that used for fine needle aspiration biopsy and allows the doctor to remove larger cylinders (cores) of tissue. Several cylinders are often removed. The biopsy is done with local numbing medicine and with the doctor either feeling the abnormal area or using an imaging test (like ultrasound or MRI) to find the spot to biopsy.
- In addition to the standard core needle biopsy, there are two other types of core needle biopsy:
- Stereotactic core needle biopsy
- Vacuum-assisted core biopsy
- In addition to the standard core needle biopsy, there are two other types of core needle biopsy:
- There are different types of breast biopsies. The type you have depends on your situation.
If the results of the core needle biopsy do not give a clear diagnosis, or your doctor still has concerns, you might need to have a second biopsy or a different type of biopsy.
- Surgical (open) biopsy: Most breast cancer can be diagnosed with a needle biopsy. Rarely, surgery is needed to remove all or part of the lump for testing. Most often, the surgeon removes the entire mass or abnormal area, as well as a surrounding margin of normal-appearing breast tissue.
- There are 2 types of surgical biopsies:
- An incisional biopsy removes only part of the suspicious area, enough to make a diagnosis.
- An excisional biopsy removes the entire tumor or abnormal area, with or without trying to take out an edge of normal breast tissue (depending on the reason for the biopsy).
- There are 2 types of surgical biopsies:
- Lymph node biopsy: The doctor may also need to biopsy the lymph nodes under the arm to check them for cancer spread. This might be done at the same time as biopsy of the breast tumor, or during surgery to remove the breast tumor. This is done by needle biopsy, or with a sentinel lymph node biopsy and/or an axillary lymph node dissection.
Determining the extent of the cancer
Determining the extent (stage) of your cancer helps your doctor evaluate treatment options. Biopsy, blood tests and imaging tests can be used to stage male breast cancer.
The stages of male breast cancer
The stages of male breast cancer are:
- Stage 1. The tumor is no more than 2 centimeters (cm) in diameter (about 3/4 inch) and hasn’t spread to the lymph nodes.
- Stage 2. The tumor may be up to 5 cm (about 2 inches) in diameter and may have spread to nearby lymph nodes. Or the tumor may be larger than 5 cm but no cancer cells are found in the lymph nodes.
- Stage 3. The tumor may be larger than 5 cm (about 2 inches) in diameter and may involve several nearby lymph nodes. Lymph nodes above the collarbone may also contain cancer cells.
- Stage 4. Cancer at this stage has spread beyond the breast to distant areas, such as the bone, brain, liver or lungs.
Treatment for breast cancer in men
At present, the same treatments are used for breast cancer in men as for women.
To decide on the most appropriate treatment, doctors generally take into account:
- the type of breast cancer
- the size of the cancer and whether it has spread (the stage)
- how abnormal the cells look under the microscope (the grade)
- whether the cancer cells have receptors for particular hormones
- whether the cells have receptors for targeted cancer drug therapy
To treat your cancer, you might have one or more of the following treatments:
- surgery
- radiotherapy
- chemotherapy
- hormone therapy
- targeted cancer drug therapy.
Rare types of breast cancer
There are other rare types of breast cancer. Doctors have developed ways of grouping breast cancers into different types. They sometimes call rarer breast cancers special type, and the more common breast cancers no special type.
Most breast cancers are invasive carcinoma – no special type. Around 70 out of 100 (around 70%) of breast cancers are this type. You may see this written as NST or NOS (not otherwise specified).
Special type breast cancers have cells with particular features. These are seen when the doctor looks at the cells under the microscope.
Medullary breast cancer
Less than 1 in 5 out of every 100 breast cancers (less than 5%) are medullary breast cancers. Medullary breast cancers occur more often in younger women and in women who have inherited a faulty BRCA 1 gene.
The cancer cells tend to be bigger than in other types of breast cancer. When doctors look at these cancers under a microscope they can see a clear boundary between the tumour and the normal tissue. This type of breast tumour is also unusual because it contains white blood cells.
Doctors treat medullary breast cancer in the same way as other types of invasive breast cancer, with surgery, radiotherapy, and drug treatment. The outlook is generally very good.
Mucinous (mucoid or colloid) breast cancer
Between 1 to 2 out of every 100 breast cancers (1 to 2 %) are mucinous breast cancers. Mucinous (mucoid or colloid) breast cancer tends to be slower growing than other types and occurs more often in older women. It is less likely to spread to the lymph nodes.
Mucinous breast cancers have this name because the cancer is made up of a large amount of mucin. It can be a pure mucinous cancer or it can be a mix of mucinous and other types.
Doctors usually treat mucinous cancers in the same way as other types of breast cancer. They remove the cancer with surgery, either taking away the whole breast (mastectomy) or part of the breast (breast conserving surgery). You might have a sentinel node biopsy to see if the cancer has spread to the lymph nodes.
The outlook for mucinous breast cancer is generally very good.
Tubular breast cancer
About 2 out of every 100 breast cancers (about 2%) are the tubular type. The cancer cells look like tubes when seen under a microscope. Tubular breast cancer occurs more often in older women and the tumour is usually very small when diagnosed. It sometimes spreads to nearby lymph nodes.
Treatment is the same as for other types of invasive breast cancer. Tubular breast cancer is less likely to come back after treatment than some other types. So, the outlook is generally good.
Adenoid cystic carcinoma of the breast
Less than 1 in 100 breast cancers (less than 1%) are adenoid cystic cancer. This type of cancer is also sometimes called a cribriform cancer. It is a cancer type that is more often diagnosed in the salivary glands, but some develop in the breast tissue.
Adenoid cystic carcinoma of the breast is generally seen in older people but has been seen in people as young as 25.
Adenoid cystic breast cancer tends to be slow growing. Doctors usually recommend surgery. Most women don’t need to have the whole breast removed (a mastectomy). Instead, your doctor will just remove the area of the cancer. This operation is called breast conserving surgery.
The cancer rarely spreads elsewhere in the body. So you don’t usually need to have your lymph nodes removed. The risk of this type of tumour coming back is low, so the outlook is good.
Metaplastic breast cancer
Metaplastic breast cancer is very rare and makes up less than 5 out of 100 breast cancers (less than 5%). Metaplastic breast cancer usually occurs between the ages of 47 to 61 and is relatively more common in Hispanic or black women.
Doctors treat metaplastic cell cancers in the same way as other breast cancers. You might have surgery, chemotherapy and radiotherapy.
Some metaplastic breast tumours are triple negative. This means that the cancers don’t have receptors for oestrogen, progesterone, or HER2. So hormone therapy or targeted therapy isn’t helpful for these cancers.
Metaplastic breast cancer tends not to spread to the lymph glands. But it is more likely to spread to other parts of the body than other types of breast cancer.
Papillary breast cancer
Papillary breast cancer makes up less than 1 in 100 breast cancers (less than 1%). Papillary breast cancer tends to affect older women.
There are different types of papillary breast cancer:
- in-situ, these are early stage cancers that have not spread
- invasive, these have spread to or beyond surrounding breast tissue
- non cancerous (benign), these are also called papilloma’s
Treatment depends on the type of papillary breast cancer. You may have surgery to the breast and sometimes the lymph nodes. You may also have radiotherapy and drug treatment.
Basal type breast cancer
Basal type breast cancer has particular genetic changes in the cells. The cells make large amounts of a protein called cytokeratin 5/6.
Basal type breast cancers are often triple negative. This means that they don’t have many receptors for estrogen, progesterone, or HER2. So, hormone therapies and targeted drugs don’t work for most basal type cancers.
Doctors use other treatments, such as surgery, chemotherapy and radiotherapy, instead.
Lymphoma of the breast
Non-Hodgkin lymphomas (NHL) of the breast are rare and make up less than 1 in 100 breast cancers (less than 1%).
The most common types are B-cell lymphomas such as diffuse large B-cell lymphomas and extranodal marginal zone lymphomas. A less common type is peripheral T-cell lymphoma (PTCL).
There is a rare type of Non-Hodgkin lymphoma called breast implant associated anaplastic large cell lymphoma (BIA-ALCL). This can develop in a small number of women who have breast implants. The first sign is usually a swelling (seroma) around the breast implant. Very rarely, a lump may be felt close to the implant.
For most people these symptoms happen many years after their implant surgery, but it could happen sooner. An in situ breast implant associated anaplastic large cell lymphoma (BIA-ALCL) is when the lymphoma hasn’t spread into other areas of the breast. The implant is removed and no further treatment is usually needed, but sometimes you may have drug treatment. The outlook is excellent for this type.
In some women the lymphoma can show as a lump in the breast. This type is called infiltrative anaplastic large cell lymphoma (i-ALCL) and it might also spread to the lymph nodes. After removing the implant, the treatment is usually chemotherapy or sometimes radiotherapy. The outlook is not so good for this type.
Signs and symptoms of breast cancer
Breast cancer typically produces no symptoms when the tumor is small and most easily treated, which is why screening is important for early detection 15. The most common physical sign is a painless lump. Sometimes breast cancer spreads to underarm lymph nodes and causes a lump or swelling, even before the original breast tumor is large enough to be felt. Less common signs and symptoms include breast pain or heaviness; persistent changes, such as swelling, thickening, or redness of the skin; and nipple abnormalities such as spontaneous discharge (especially if bloody), erosion, or retraction. Any persistent change in the breast should be evaluated by a doctor as soon as possible.
Knowing how your breasts normally look and feel is an important part of breast health. Finding breast cancer as early as possible gives you a better chance of successful treatment. But knowing what to look for does not take the place of having regular mammograms and other screening tests. Screening tests can help find breast cancer in its early stages, before any symptoms appear.
The most common symptom of breast cancer is a new lump or mass. A painless, hard mass that has irregular edges is more likely to be cancer, but breast cancers can be tender, soft, or rounded. They can even be painful. For this reason, it is important to have any new breast mass, lump, or breast change checked by a health care professional experienced in diagnosing breast diseases.
Other possible symptoms of breast cancer include:
- Swelling of all or part of a breast (even if no distinct lump is felt)
- Skin irritation, redness, dimpling or pitting of the skin over your breast, like the skin of an orange
- Breast or nipple pain
- Nipple retraction (turning inward) or newly inverted nipple
- Redness, scaliness, or thickening of the nipple or breast skin
- Nipple discharge (other than breast milk)
- Peeling, scaling, crusting or flaking of the pigmented area of skin surrounding the nipple (areola) or breast skin
Sometimes a breast cancer can spread to lymph nodes under the arm or around the collar bone and cause a lump or swelling there, even before the original tumor in the breast is large enough to be felt. Swollen lymph nodes should also be checked by a health care provider.
Although any of these symptoms can be caused by things other than breast cancer, if you have them, they should be reported to a health care professional so that the cause can be found.
Because mammograms do not find every breast cancer, it is important for you to be aware of changes in your breasts and to know the signs and symptoms of breast cancer.
Breast cancer screening for the Early Detection of Breast Cancer
Finding breast cancer early and getting state-of-the-art cancer treatment are the most important strategies to prevent deaths from breast cancer. Breast cancer that’s found early, when it’s small and has not spread, is easier to treat successfully. Getting regular screening tests is the most reliable way to find breast cancer early. The American Cancer Society has screening guidelines for women at average risk of breast cancer, and for those at high risk for breast cancer.
The goal of screening tests for breast cancer is to find it before it causes symptoms (like a lump that can be felt). Screening refers to tests and exams used to find a disease in people who don’t have any symptoms. Early detection means finding and diagnosing a disease earlier than if you’d waited for symptoms to start.
Breast cancers found during screening exams are more likely to be smaller and still confined to the breast. The size of a breast cancer and how far it has spread are some of the most important factors in predicting the prognosis (outlook) of a woman with this disease.
American Cancer Society screenings recommendations for women at average breast cancer risk
These guidelines are for women at average risk for breast cancer. For screening purposes, a woman is considered to be at average risk if she doesn’t have a personal history of breast cancer, a strong family history of breast cancer, or a genetic mutation known to increase risk of breast cancer (such as in a BRCA gene), and has not had chest radiation therapy before the age of 30. (See below for guidelines for women at high risk.)
- Women between 40 and 44 have the option to start screening with a mammogram every year.
- Women 45 to 54 should get mammograms every year.
- Women 55 and older can switch to a mammogram every other year, or they can choose to continue yearly mammograms. Screening should continue as long as a woman is in good health and is expected to live 10 more years or longer.
- All women should understand what to expect when getting a mammogram for breast cancer screening – what the test can and cannot do.
Mammograms
Regular mammograms can help find breast cancer at an early stage, when treatment is most successful. A mammogram can find breast changes that could be cancer years before physical symptoms develop. Results from many decades of research clearly show that women who have regular mammograms are more likely to have breast cancer found early, are less likely to need aggressive treatment like surgery to remove the breast (mastectomy) and chemotherapy, and are more likely to be cured.
Mammograms are not perfect. They miss some cancers. And if something is found on a screening mammogram, a woman will likely need other tests (such as more mammograms or a breast ultrasound) to find out if it is cancer. There’s also a small possibility of being diagnosed with a cancer that never would have caused any problems had it not been found during screening. This is called overdiagnosis. It’s important that women getting mammograms know what to expect and understand the benefits and limitations of screening.
In recent years, a newer type of mammogram called digital breast tomosynthesis (commonly known as three-dimensional [3D] mammography) has become much more common, although it’s not available in all breast imaging centers.
Many studies have found that 3D mammography appears to lower the chance of being called back after screening for follow-up testing. It also appears to find more breast cancers, and several studies have shown it can be helpful in women with more dense breasts. A large study is now in progress to better compare outcomes between 3D mammograms and standard (2D) mammograms.
It should be noted that 3D mammograms often cost more than 2D mammograms, and this added cost may not be covered by insurance.
The American Cancer Society breast cancer screening guidelines consider having had either a 2D or 3D mammogram as being in line with current screening recommendations 16. The American Cancer Society also believes that women should be able to choose between 2D and 3D mammography if they or their doctor believes one would be more appropriate, and that out-of-pocket costs should not be a barrier to having either one.
Clinical breast exam and breast self-exam
Research has not shown a clear benefit of regular physical breast exams done by either a health professional (clinical breast exams) or by yourself (breast self-exams). There is very little evidence that these tests help find breast cancer early when women also get screening mammograms. Most often when breast cancer is detected because of symptoms (such as a lump), a woman discovers the symptom during usual activities such as bathing or dressing. Women should be familiar with how their breasts normally look and feel and report any changes to a health care provider right away.
American Cancer Society screening recommendations for women at high risk
Women who are at high risk for breast cancer based on certain factors should get an MRI and a mammogram every year, typically starting at age 30. This includes women who 16:
- Have a lifetime risk of breast cancer of about 20% to 25% or greater, according to risk assessment tools that are based mainly on family history (see below)
- Have a known BRCA1 or BRCA2 gene mutation (based on having had genetic testing)
- Have a first-degree relative (parent, brother, sister, or child) with a BRCA1 or BRCA2 gene mutation, and have not had genetic testing themselves
- Had radiation therapy to the chest when they were between the ages of 10 and 30 years
- Have Li-Fraumeni syndrome, Cowden syndrome, or Bannayan-Riley-Ruvalcaba syndrome, or have first-degree relatives with one of these syndromes
The American Cancer Society recommends against MRI screening for women whose lifetime risk of breast cancer is less than 15%.
There’s not enough evidence to make a recommendation for or against yearly MRI screening for women who have a higher lifetime risk based on certain factors , such as:
- Having a personal history of breast cancer, ductal carcinoma in situ (DCIS), lobular carcinoma in situ (LCIS), atypical ductal hyperplasia (ADH), or atypical lobular hyperplasia (ALH)
- Having “extremely” or “heterogeneously” dense breasts as seen on a mammogram
If MRI is used, it should be in addition to, not instead of, a screening mammogram. This is because although an MRI is more likely to find cancer than a mammogram, it may still miss some cancers that a mammogram would find.
Most women at high risk should begin screening with MRI and mammograms when they are 30 and continue for as long as they are in good health. But this is a decision that should be made with a woman’s health care providers, taking into account her personal circumstances and preferences.
Tools used to assess breast cancer risk
Several risk assessment tools are available to help health professionals estimate a woman’s breast cancer risk. These tools give approximate, rather than precise, estimates of breast cancer risk based on different combinations of risk factors and different data sets.
Because the different tools use different factors to estimate risk, they may give different risk estimates for the same woman. Two models could easily give different estimates for the same person.
Risk assessment tools that include family history in first-degree relatives (parents, siblings, and children) and second-degree relatives (such as aunts and cousins) on both sides of the family should be used with the American Cancer Society guidelines to decide if a woman should have MRI screening. The use of any of the risk assessment tools and its results should be discussed by a woman with her health care provider.
Breast cancer diagnosis
Tests and procedures used to diagnose breast cancer include:
- Breast exam. Your doctor will check both of your breasts and lymph nodes in your armpit, feeling for any lumps or other abnormalities.
- Mammogram. A mammogram is an X-ray of the breast. Mammograms are commonly used to screen for breast cancer. If an abnormality is detected on a screening mammogram, your doctor may recommend a diagnostic mammogram to further evaluate that abnormality.
- Breast ultrasound. Ultrasound uses sound waves to produce images of structures deep within the body. Ultrasound may be used to determine whether a new breast lump is a solid mass or a fluid-filled cyst.
- Removing a sample of breast cells for testing (biopsy). A biopsy is the only definitive way to make a diagnosis of breast cancer. During a biopsy, your doctor uses a specialized needle device guided by X-ray or another imaging test to extract a core of tissue from the suspicious area. Often, a small metal marker is left at the site within your breast so the area can be easily identified on future imaging tests. Biopsy samples are sent to a laboratory for analysis where experts determine whether the cells are cancerous. A biopsy sample is also analyzed to determine the type of cells involved in the breast cancer, the aggressiveness (grade) of the cancer, and whether the cancer cells have hormone receptors or other receptors that may influence your treatment options.
- Breast magnetic resonance imaging (MRI). An MRI machine uses a magnet and radio waves to create pictures of the interior of your breast. Before a breast MRI, you receive an injection of dye. Unlike other types of imaging tests, an MRI doesn’t use radiation to create the images.
Other tests and procedures may be used depending on your situation.
Finding Breast Cancer During Pregnancy
Breast cancer during pregnancy is rare. But if you find a lump or notice any changes in your breasts that concern you, tell your doctor or nurse right away. There are a variety of tests a pregnant woman can have if breast cancer is suspected. And there are options for treating breast cancer if you are pregnant.
If you are pregnant and breast cancer is found, it may be called gestational breast cancer or pregnancy-associated breast cancer (PABC).
How common is breast cancer during pregnancy?
- Breast cancer is found in about 1 in every 3,000 pregnant women. But it is the most common type of cancer found during pregnancy.
Breast cancers can be harder to find when you’re pregnant
Hormone changes during pregnancy cause the breasts to change. They may become larger, lumpy, and/or tender. This can make it harder for you or your doctor to notice a lump caused by cancer until it gets quite large.
Another reason it may be hard to find breast cancers early during pregnancy is that many women put off breast cancer screening with mammograms until after the pregnancy. And because pregnancy and breastfeeding can make breast tissue denser, it can be harder to see an early cancer on a mammogram.
Because of these challenges, when a pregnant woman develops breast cancer, it’s often diagnosed at a later stage than it would be if she were not pregnant. It’s also more likely to have spread to lymph nodes.
What to look for
If you find a lump or notice any changes in your breasts that concern you, don’t ignore them. Tell your doctor or nurse right away. If your doctor doesn’t want to check it out with a mammogram, ask about other kinds of imaging tests such as ultrasound or magnetic resonance imaging (MRI). You may need to get a second opinion. Any suspicious breast changes should be checked out or even biopsied (see below) before assuming they are a normal response to pregnancy.
Are mammograms and other imaging tests safe during pregnancy?
A main concern with any imaging test during pregnancy is whether it exposes the developing fetus to radiation, which could be harmful.
Mammograms can find most breast cancers that start when a woman is pregnant, and it’s thought to be safe to have a mammogram during pregnancy. The amount of radiation needed for a mammogram is small. And the radiation is focused on the breasts, so that most of it doesn’t reach other parts of the body. For extra protection, a lead shield is placed over the lower part of the belly to help keep radiation from reaching the womb. Still, scientists can’t be certain about the
effects of even a very small dose of radiation on an unborn baby.
Ultrasound exams of the breast do not use radiation and are thought to be safe during pregnancy. This is typically an easy test to have, so it’s often the first test done to evaluate a change in the breast (such as a lump).
MRI scans do not use radiation and are thought to be safe during pregnancy. But the contrast material (dye) used in MRI can cross the placenta, the organ that connects the mother to the fetus. This dye has been linked with fetal abnormalities in lab animals. For this reason, many doctors do not recommend MRI with contrast dye during pregnancy. An MRI without contrast can be used if needed.
Other tests, such as PET scans, bone scans, and computed tomography (CT) scans are more likely to expose the fetus to radiation.
Breast biopsy during pregnancy
A new lump or abnormal imaging test result may cause concern, but a biopsy is the only way to find out if a breast change is cancer. During a biopsy a small piece of tissue is taken from the area of concern. Breast biopsies are most often done using a needle. They’re usually done as an outpatient procedure, even if you’re pregnant. The doctor uses medicine to numb just the area of the breast involved in the biopsy. This causes little risk to the fetus.
If a needle biopsy doesn’t give an answer, a surgical biopsy is typically the next step. This means taking out a piece of tissue through a small cut (incision) in the breast. Surgical biopsies are often done under general anesthesia (where drugs are used to put the patient into a deep sleep), which carries a small risk to the fetus.
Tests to stage the breast cancer
If breast cancer is found, you might need other tests to find out if cancer cells have spread within the breast or to other parts of the body. This process is called staging. Different staging tests may be needed, depending on your case.
As noted above, tests like ultrasound and MRI scans do not use radiation and are thought to be safe during pregnancy. But the contrast material (dye) sometimes used in MRI is typically not recommended during pregnancy. An MRI without contrast can be used if needed.
Chest x-rays are sometimes needed to help make treatment decisions. They use a small amount of radiation. They’re thought to be safe to have when you’re pregnant, as long as your belly is shielded.
Other tests, such as PET scans, bone scans, and computed tomography (CT) scans are more likely to expose the fetus to radiation. These tests are not often needed, especially if the cancer is thought to be just in the breast. If one of these tests is needed, doctors might be able to make adjustments to limit the amount of radiation exposure to the fetus.
Treatments are available if a pregnant woman has breast cancer. Learn about treating breast cancer during pregnancy.
Can breast cancer spread to the baby?
There are no reported cases of breast cancer spreading from the mother to the fetus. But in a very few cases, the cancer has reached the placenta (the organ that connects the mother to the fetus). This could affect the amount of nutrition the fetus gets from the mother.
Staging breast cancer
Once your doctor has diagnosed your breast cancer, he or she works to establish the extent (stage) of your cancer. Your cancer’s stage helps determine your prognosis and the best treatment options.
Complete information about your cancer’s stage may not be available until after you undergo breast cancer surgery.
Tests and procedures used to stage breast cancer may include:
- Blood tests, such as a complete blood count
- Mammogram of the other breast to look for signs of cancer
- Breast MRI
- Bone scan
- Computerized tomography (CT) scan
- Positron emission tomography (PET) scan
Not all women will need all of these tests and procedures. Your doctor selects the appropriate tests based on your specific circumstances and taking into account new symptoms you may be experiencing.
Breast cancer stages range from 0 to IV with 0 indicating cancer that is noninvasive or contained within the milk ducts. Stage IV breast cancer, also called metastatic breast cancer, indicates cancer that has spread to other areas of the body.
Breast cancer staging also takes into account your cancer’s grade; the presence of tumor markers, such as receptors for estrogen, progesterone and HER2; and proliferation factors.
Breast cancer stages
Staging is a way of describing where the cancer is located, how much the cancer has grown, and if or where it has spread. On the othr hand, breast cancer grading means how abnormal the cancer cells look under a microscope. Doctors use diagnostic tests to find out the cancer’s stage, so staging may not be complete until all the tests are finished. Knowing the stage helps the doctor to decide what kind of treatment is best and can help predict a patient’s prognosis, which is the chance of recovery. There are different stage descriptions for different types of cancer.
The earliest stage breast cancers are stage 0 (carcinoma in situ). It then ranges from stage I (1) through IV (4). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means cancer has spread more. And within a stage, an earlier letter means a lower stage. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
Your doctor might also talk about early, locally advanced or secondary breast cancer.
Tests and procedures used to stage breast cancer may include:
- Blood tests, such as a complete blood count
- Mammogram of the other breast to look for signs of cancer
- Breast MRI
- Bone scan
- Computerized tomography (CT) scan
- Positron emission tomography (PET) scan
Not all women will need all of these tests and procedures. Your doctor selects the appropriate tests based on your specific circumstances and taking into account new symptoms you may be experiencing.
TNM staging system
The most commonly used tool that doctors use to describe the stage is the American Joint Committee on Cancer (AJCC) TNM system. Doctors use the results from diagnostic tests and scans to answer these questions:
- Tumor (T): How large is the primary tumor? Where is it located?
- Node (N): Has the tumor spread to the lymph nodes? If so, where and how many?
- Metastasis (M): Has the cancer metastasized to other parts of the body? If so, where and how much?
The results are combined to determine the stage of cancer for each person.
There are 5 stages: stage 0 (zero), which is noninvasive ductal carcinoma in situ (DCIS), and stages I through IV (1 through 4), which are used for invasive breast cancer. The stage provides a common way of describing the cancer, so doctors can work together to plan the best treatments.
There are 2 types of TNM staging for breast cancer.
- First, the clinical stage is based on the results of tests done before surgery, which may include physical examination, mammogram, ultrasound, and MRI scans.
- Then, the pathologic stage also called the surgical stage is assigned based on the pathology results from the breast tissue and any lymph nodes removed during surgery. It is usually determined several days after surgery. In general, more importance is placed on the pathologic stage than the clinical stage.
In both staging systems, 7 key pieces of information are used:
- The extent (size) of the tumor (T): How large is the cancer? Has it grown into nearby areas?
- The spread to nearby lymph nodes (N): Has the cancer spread to nearby lymph nodes? If so, how many?
- The spread (metastasis) to distant sites (M): Has the cancer spread to distant organs such as the lungs or liver?
- Estrogen Receptor (ER) status: Does the cancer have the protein called an estrogen receptor?
- Progesterone Receptor (PR) status: Does the cancer have the protein called a progesterone receptor?
- Human epidermal growth factor type 2 receptor (HER2) status: Does the cancer make too much of a protein called HER2?
- Grade of the cancer (G): How much do the cancer cells look like normal cells?
Here are more details on each part of the TNM system for breast cancer:
Tumor (T)
Using the TNM system, the “T” plus a letter or number (0 to 4) is used to describe the size and location of the tumor. Some stages are divided into smaller groups that help describe the tumor in even more detail. Specific tumor stage information is listed below.
- TX: The primary tumor cannot be evaluated.
- T0 (T plus zero): There is no evidence of cancer in the breast.
- Tis: Refers to carcinoma in situ. The cancer is confined within the ducts or lobules of the breast tissue and has not spread into the surrounding tissue of the breast. There are types of breast carcinoma in situ:
- Tis (DCIS): DCIS is a noninvasive cancer, but if not removed it can develop into an invasive breast cancer later. DCIS means that cancer cells have been found in breast ducts and have not spread past the layer of tissue where they began.
- Tis (LCIS): Lobular carcinoma in situ (LCIS) describes abnormal cells found in the lobules or glands of the breast. LCIS is not cancer, but it increases the risk of developing invasive breast cancer.
- Tis (Paget’s): Paget’s disease of the nipple is a rare form of early, noninvasive cancer that is only in the skin cells of the nipple. Sometimes Paget’s disease is associated with another, invasive breast cancer. If there is also an invasive breast cancer present, it is classified according to the stage of the invasive tumor.
- T1: The invasive part of the tumor in the breast is 20 millimeters (mm) or smaller in size at its widest area. This is a little less than an inch. This stage is then broken into 3 substages depending on the size of the tumor:
- T1a is a tumor that is larger than 1 mm, but 5 mm or smaller.
- T1b is a tumor that is larger than 5 mm, but 10 mm or smaller.
- T1c is a tumor that is larger than 10 mm, but 20 mm or smaller.
- T2: The invasive part of the tumor is larger than 20 mm (>2 cm) but not larger than 50 mm (<5 cm).
- T3: The invasive part of the tumor is larger than 50 mm (>5 cm) across.
- T4: The tumor falls into 1 of the following groups:
- T4a means the tumor has grown into the chest wall.
- T4b is when the tumor has grown into the skin.
- T4c is cancer that has grown into the chest wall and the skin.
- T4d is inflammatory breast cancer.
Node (N)
The “N” in the TNM staging system stands for lymph nodes. Lymph nodes located under the arm, above and below the collarbone, and under the breastbone are called regional lymph nodes. Lymph nodes in other parts of the body are called distant lymph nodes. As explained above, if the doctor evaluates the lymph nodes before surgery, based on other tests and/or a physical examination, a letter “c” for “clinical” staging is placed in front of the “N.” If the doctor evaluates the lymph nodes after surgery, which is a more accurate assessment, a letter “p” for “pathologic” staging is placed in front of the “N.”
It’s not yet clear how much cancer in the lymph node is needed to see a change in outlook or treatment. This is still being studied, but for now, a deposit of cancer cells must contain at least 200 cells or be at least 0.2 mm across (less than 1/100 of an inch) for it to change the N stage. An area of cancer spread that is smaller than 0.2 mm (or fewer than 200 cells) doesn’t change the stage, but is recorded with abbreviations (i+ or mol+) that indicate the type of special test used to find the spread.
If the area of cancer spread is at least 0.2 mm (or 200 cells), but still not larger than 2 mm, it is called a micrometastasis (one mm is about the size of the width of a grain of rice). Micrometastases are counted only if there aren’t any larger areas of cancer spread. Areas of cancer spread larger than 2 mm are known to influence outlook and do change the N stage. These larger areas are sometimes called macrometastases, but are more often just called metastases.
The information below describes the pathologic staging.
- NX: The lymph nodes cannot be evaluated.
- N0: No cancer was found in the lymph nodes.
- N0(i+): The area of cancer spread contains fewer than 200 cells and is smaller than 0.2 mm. The abbreviation “i+” means that a small number of cancer cells (called isolated tumor cells) were seen in routine stains or when a special type of staining technique, called immunohistochemistry, was used.
- N0(mol+): Cancer cells cannot be seen in underarm lymph nodes (even using special stains), but traces of cancer cells were detected using a technique called RT-PCR. RT-PCR is a molecular test that can find very small numbers of cancer cells.
- N1: Cancer has spread to 1 to 3 axillary (underarm) lymph node(s), and/or cancer is found in internal mammary lymph nodes (those near the breast bone) on sentinel lymph node biopsy.
- N1mi: Micrometastases (tiny areas of cancer spread) in the lymph nodes under the arm. The areas of cancer spread in the lymph nodes are at least 0.2mm across, but not larger than 2mm.
- N1a: Cancer has spread to 1 to 3 lymph nodes under the arm with at least one area of cancer spread greater than 2 mm across.
- N1b: Cancer has spread to internal mammary lymph nodes on the same side as the cancer, but this spread could only be found on sentinel lymph node biopsy (it did not cause the lymph nodes to become enlarged).
- N1c: Both N1a and N1b apply.
- N2: Cancer has spread to 4 to 9 lymph nodes under the arm, or cancer has enlarged the internal mammary lymph nodes.
- N2a: Cancer has spread to 4 to 9 lymph nodes under the arm, with at least one area of cancer spread larger than 2 mm.
- N2b: Cancer has spread to one or more internal mammary lymph nodes, causing them to become enlarged.
- N3: The cancer falls within 1 of the following groups:
- N3a: Either cancer has spread to 10 or more axillary lymph nodes, with at least one area of cancer spread greater than 2 mm, OR cancer has spread to the lymph nodes under the collarbone (infraclavicular nodes), with at least one area of cancer spread greater than 2 mm.
- N3b: Either cancer is found in at least one axillary lymph node (with at least one area of cancer spread greater than 2 mm) and has enlarged the internal mammary lymph nodes, OR cancer has spread to 4 or more axillary lymph nodes (with at least one area of cancer spread greater than 2 mm), and to the internal mammary lymph nodes on sentinel lymph node biopsy.
- N3c: Cancer has spread to the lymph nodes above the collarbone (supraclavicular nodes) on the same side of the cancer with at least one area of cancer spread greater than 2 mm.
If there is cancer in the lymph nodes, knowing how many lymph nodes are involved and where they are helps doctors to plan treatment. The pathologist can find out the number of axillary lymph nodes that contain cancer after they are removed during surgery. It is not common to remove the supraclavicular or internal mammary lymph nodes during surgery. If there is cancer in these lymph nodes, treatment other than surgery, such as radiation therapy, chemotherapy, and hormonal therapy is used.
Metastasis (M)
The “M” in the TNM system indicates whether the cancer has spread to other parts of the body. Evidence of metastatic cancer means this is no longer considered early-stage or locally advanced cancer.
M followed by a 0 or 1 indicates whether the cancer has spread to distant organs — for example, the lungs, liver, or bones.
- MX: Distant spread cannot be evaluated.
- M0: No distant spread is found on x-rays (or other imaging tests) or by physical exam.
- cM0 (i+): Small numbers of cancer cells are found in blood or bone marrow (found only by special tests), or tiny areas of cancer spread (no larger than 0.2 mm) are found in lymph nodes away from the underarm, collarbone, or internal mammary areas.
- M1: Cancer has spread to distant organs (most often to the bones, lungs, brain, or liver) as seen on imaging tests or by physical exam, and/or a biopsy of one of these areas proves cancer has spread and is larger than 0.2mm.
Cancer stage grouping
Doctors assign the stage of the cancer by combining the T, N, and M classifications. Most patients are anxious to learn the exact stage of the cancer. However, it is important to keep in mind that tumor biology, including the diagnostic markers outlined above, has a significant impact on the recommended treatment plan, as well as on the prognosis. Your doctor will generally confirm the stage of the cancer when the testing after surgery is finalized, usually about 5 to 7 days after surgery. When systemic or whole body treatment is given before surgery, called neoadjuvant therapy, the stage of the cancer is primarily determined clinically. Doctors may refer to stage 1 to stage 2A cancer as early stage, and stage 2B to stage 3 as locally advanced.
Stage O (Stage Zero) breast cancer
Stage 0 or Stage zero (0) describes disease that is only in the ducts and lobules of the breast tissue and has not spread to the surrounding tissue of the breast. It is also called noninvasive cancer (Tis, N0, M0).
Figure 3. Breast cancer stage O

Stage 1A breast cancer
Stage 1A breast cancer: The tumor is small, invasive, and has not spread to the lymph nodes (T1, N0, M0).
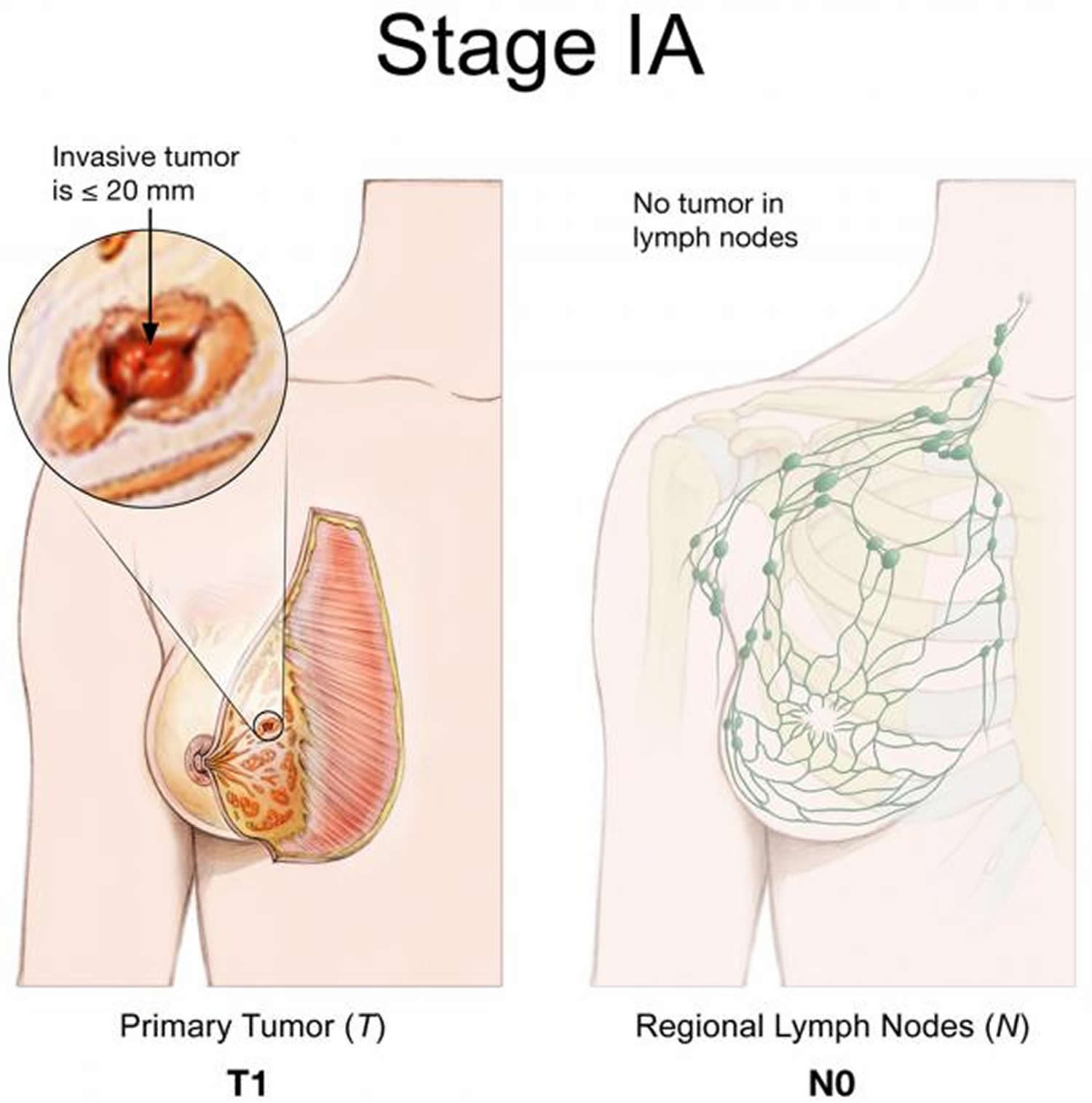 Stage 1B breast cancer
Stage 1B breast cancer
Stage 1B breast cancer: Cancer has spread only to the lymph nodes, and is larger than 0.2 mm but less than 2 mm in size. There is either no evidence of a tumor in the breast or the tumor in the breast is 20 mm or smaller (T0 or T1, N1mic, M0).
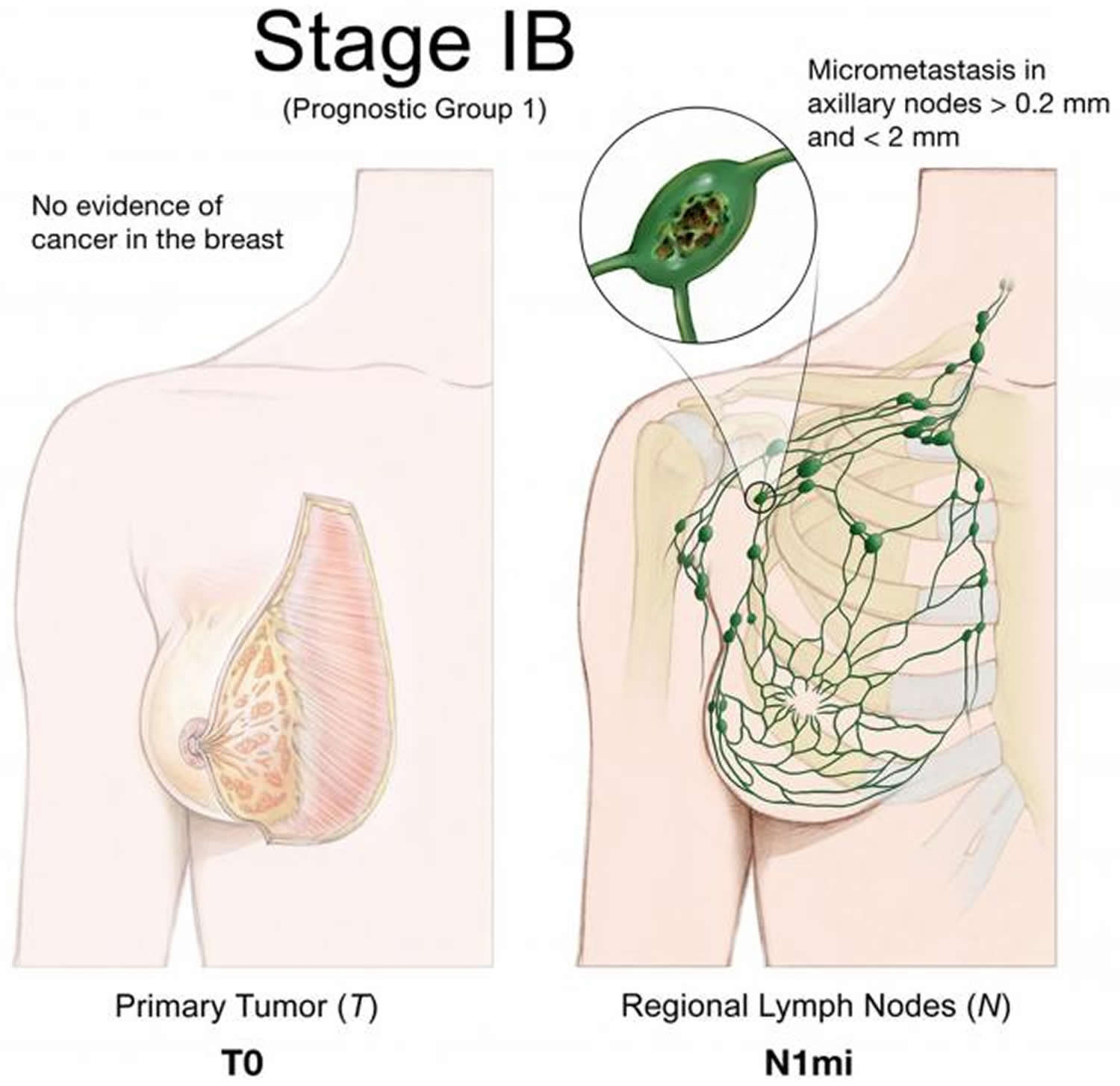
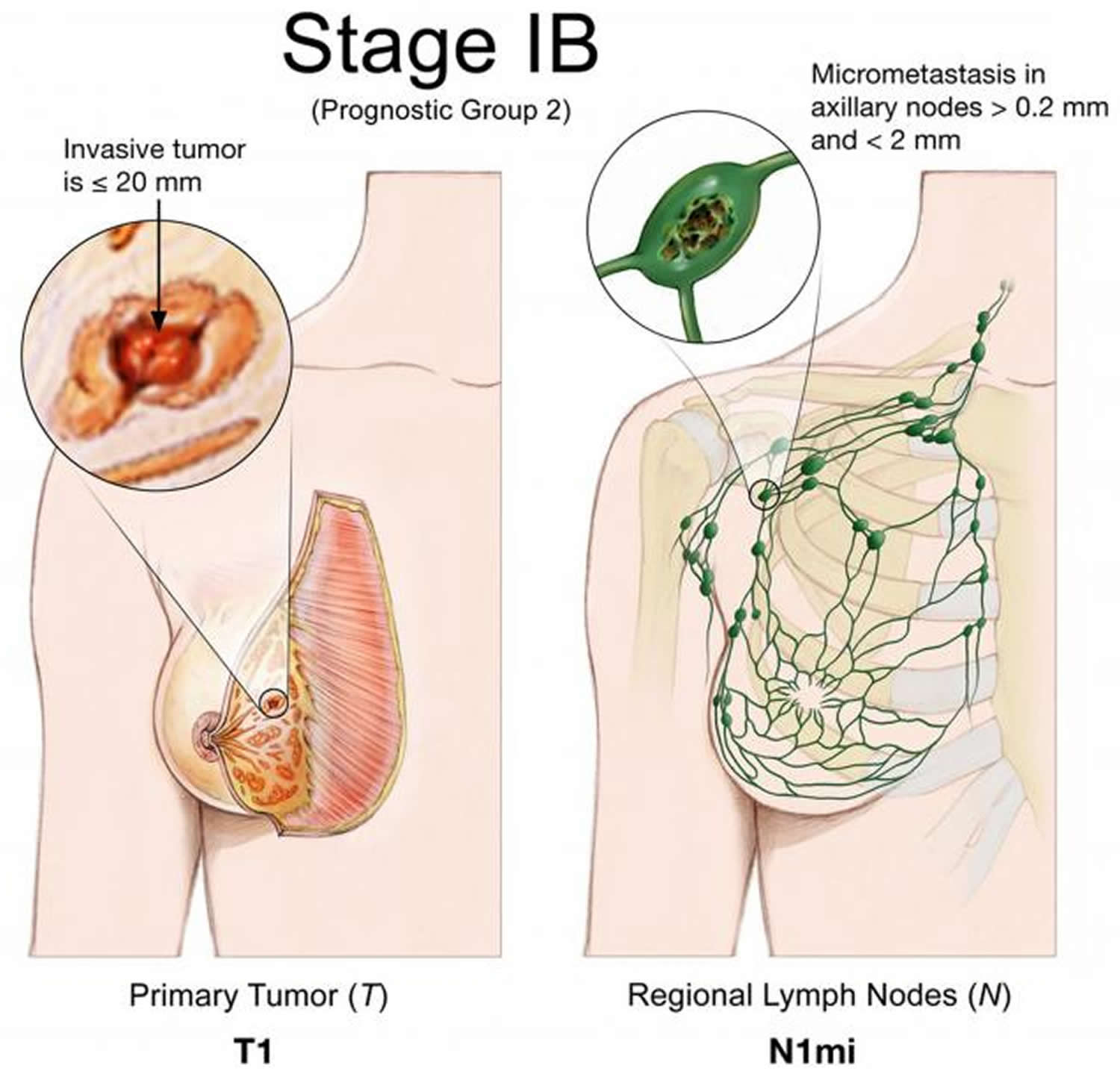 Stage 2A breast cancer
Stage 2A breast cancer
Stage 2A breast cancer: Any 1 of these conditions:
- There is no evidence of a tumor in the breast, but the cancer has spread to the axillary lymph nodes but not to distant parts of the body. (T0, N1, M0).
- The tumor is 20 mm or smaller and has spread to the axillary lymph nodes (T1, N1, M0).
- The tumor is larger than 20 mm but not larger than 50 mm and has not spread to the axillary lymph nodes (T2, N0, M0).
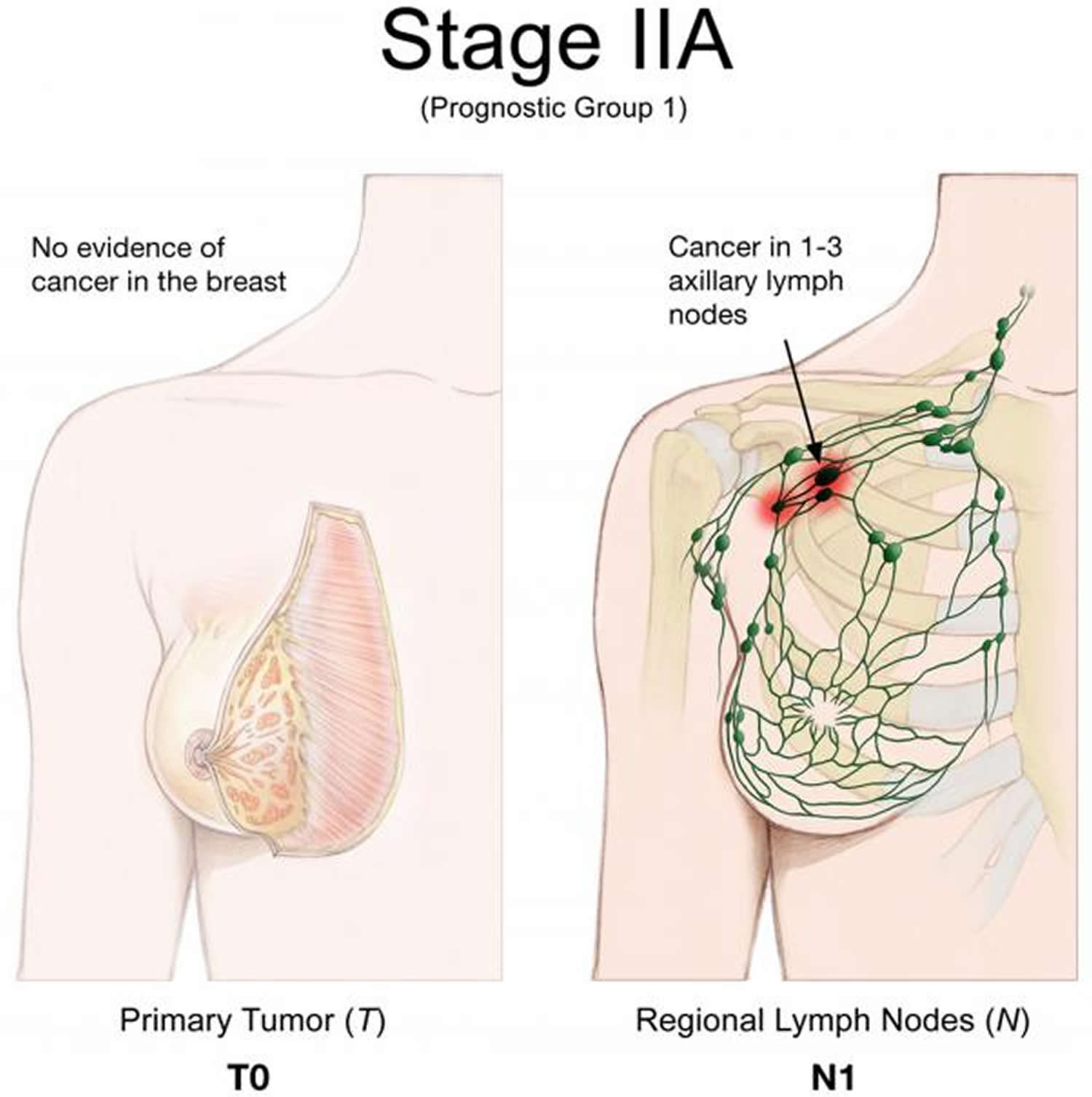
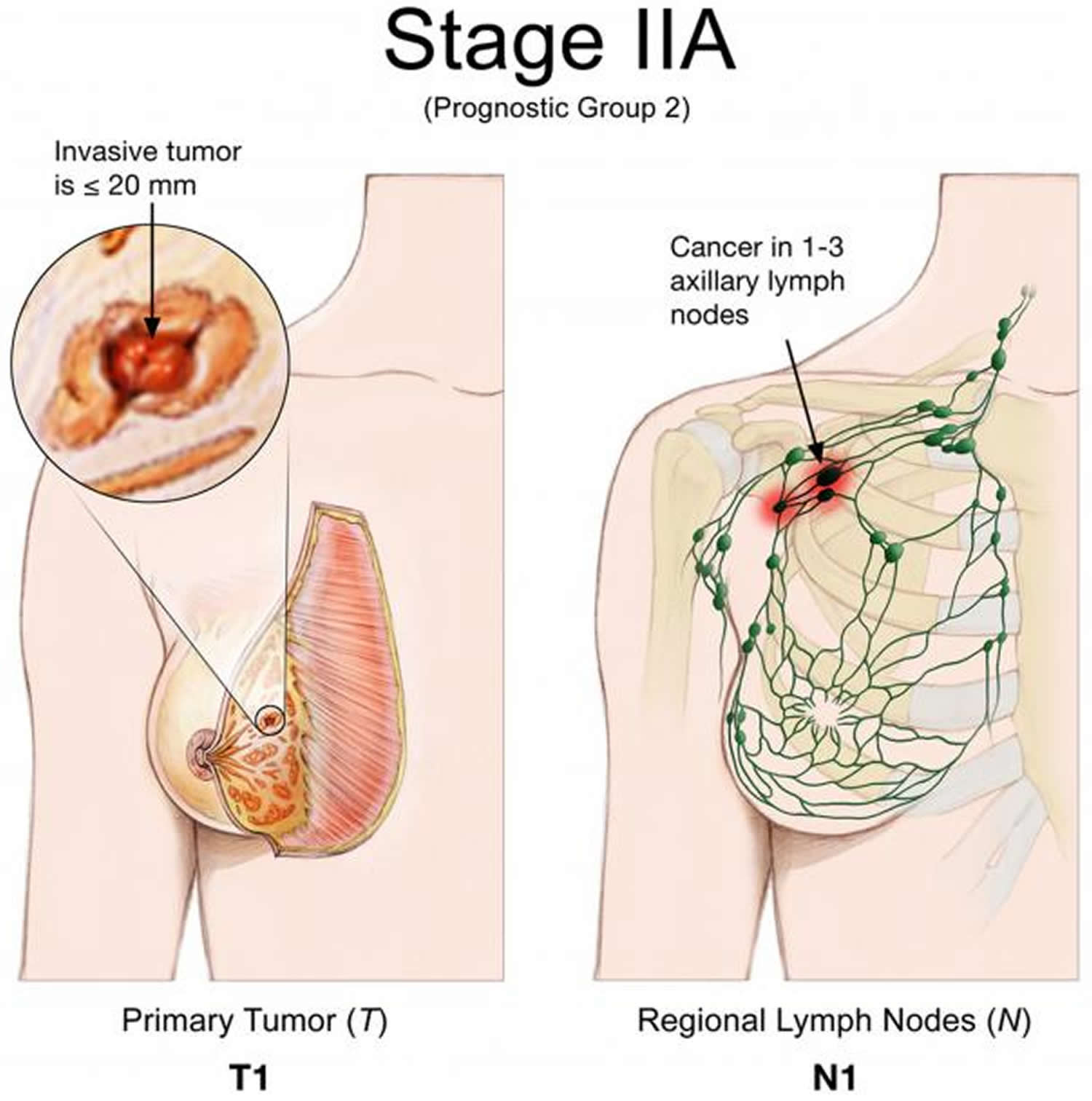
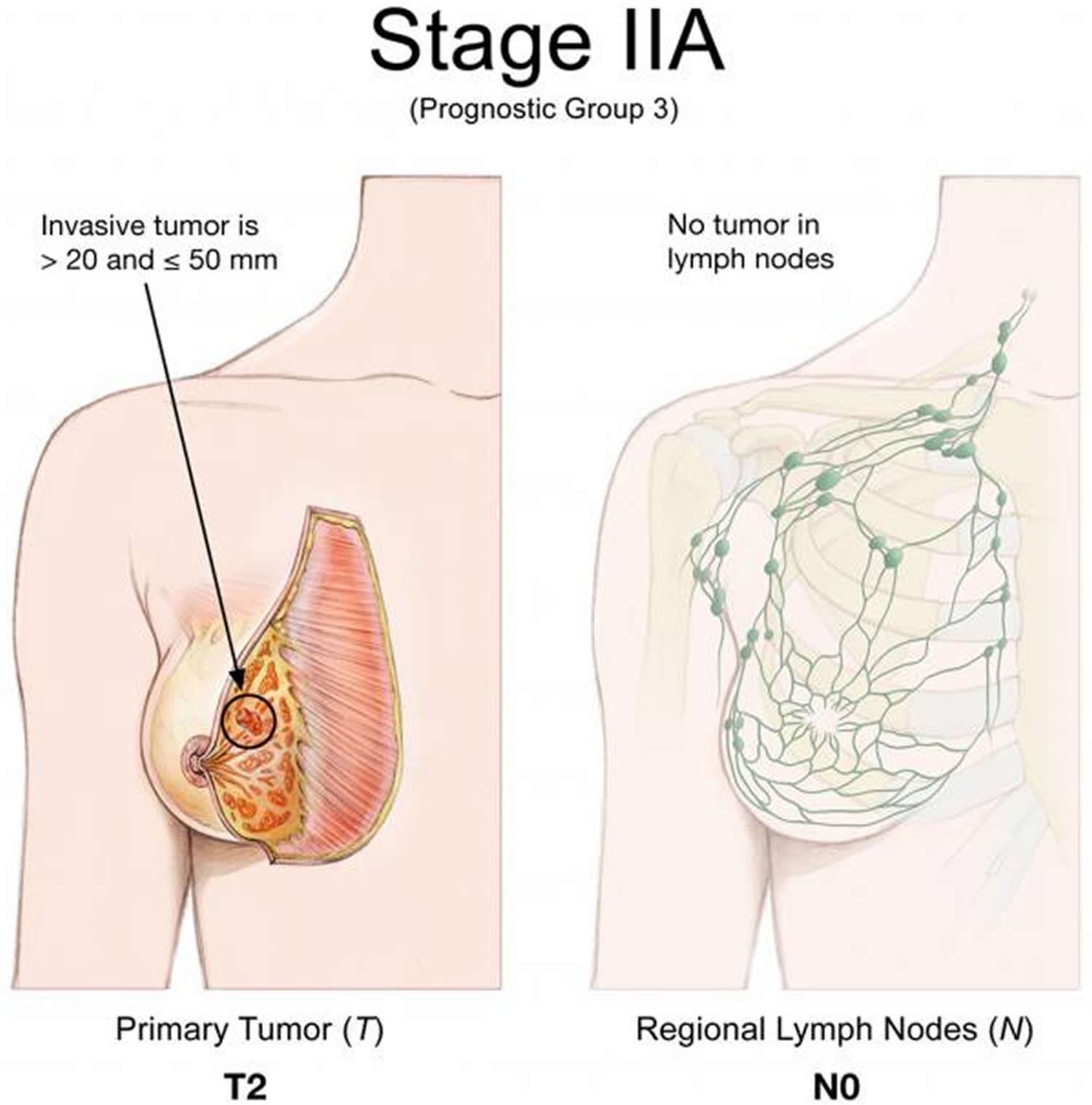
Stage 2B breast cancer
Stage 2B breast cancer: Either of these conditions:
- The tumor is larger than 20 mm but not larger than 50 mm and has spread to 1 to 3 axillary lymph nodes (T2, N1, M0).
- The tumor is larger than 50 mm but has not spread to the axillary lymph nodes (T3, N0, M0).
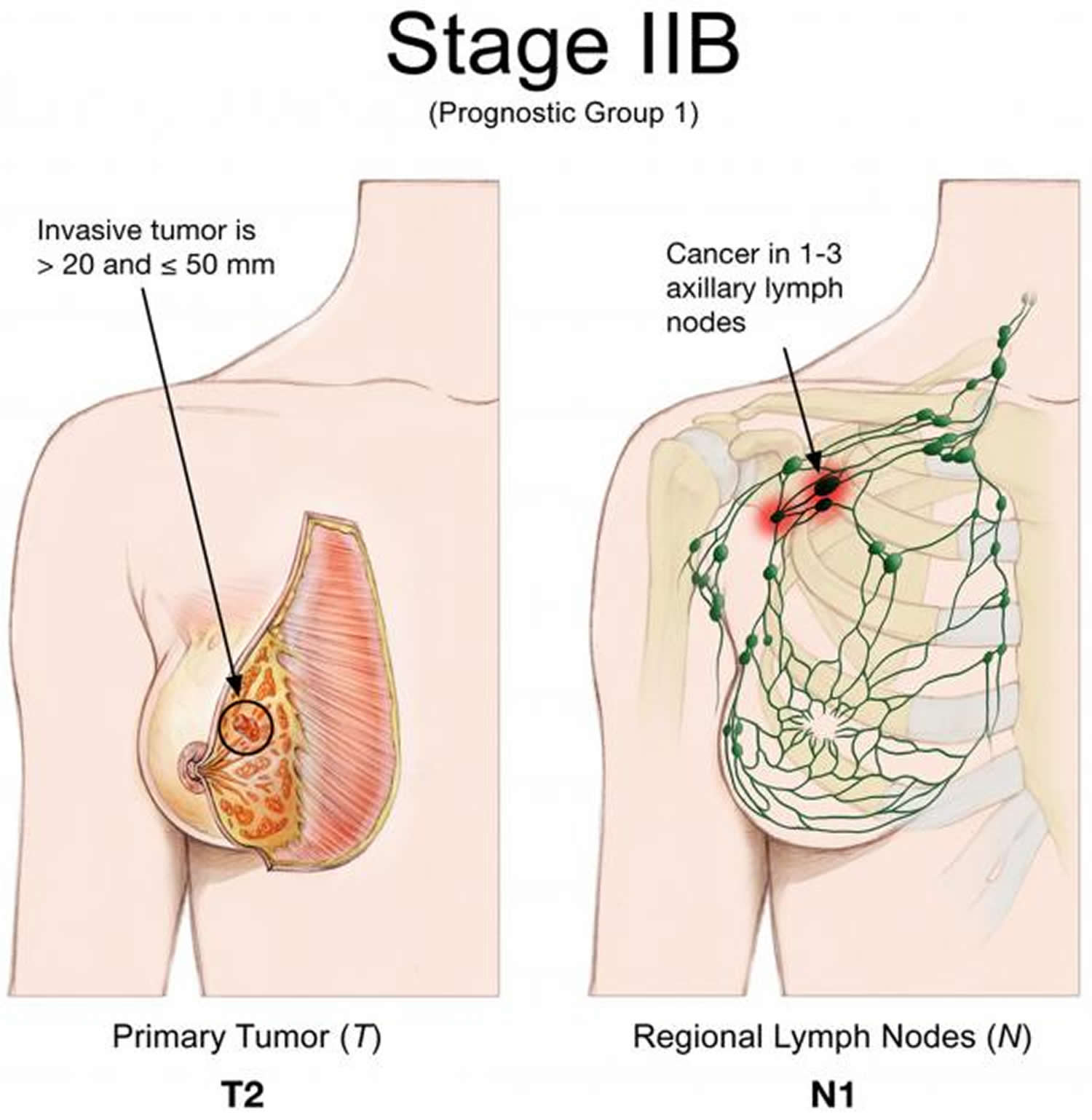
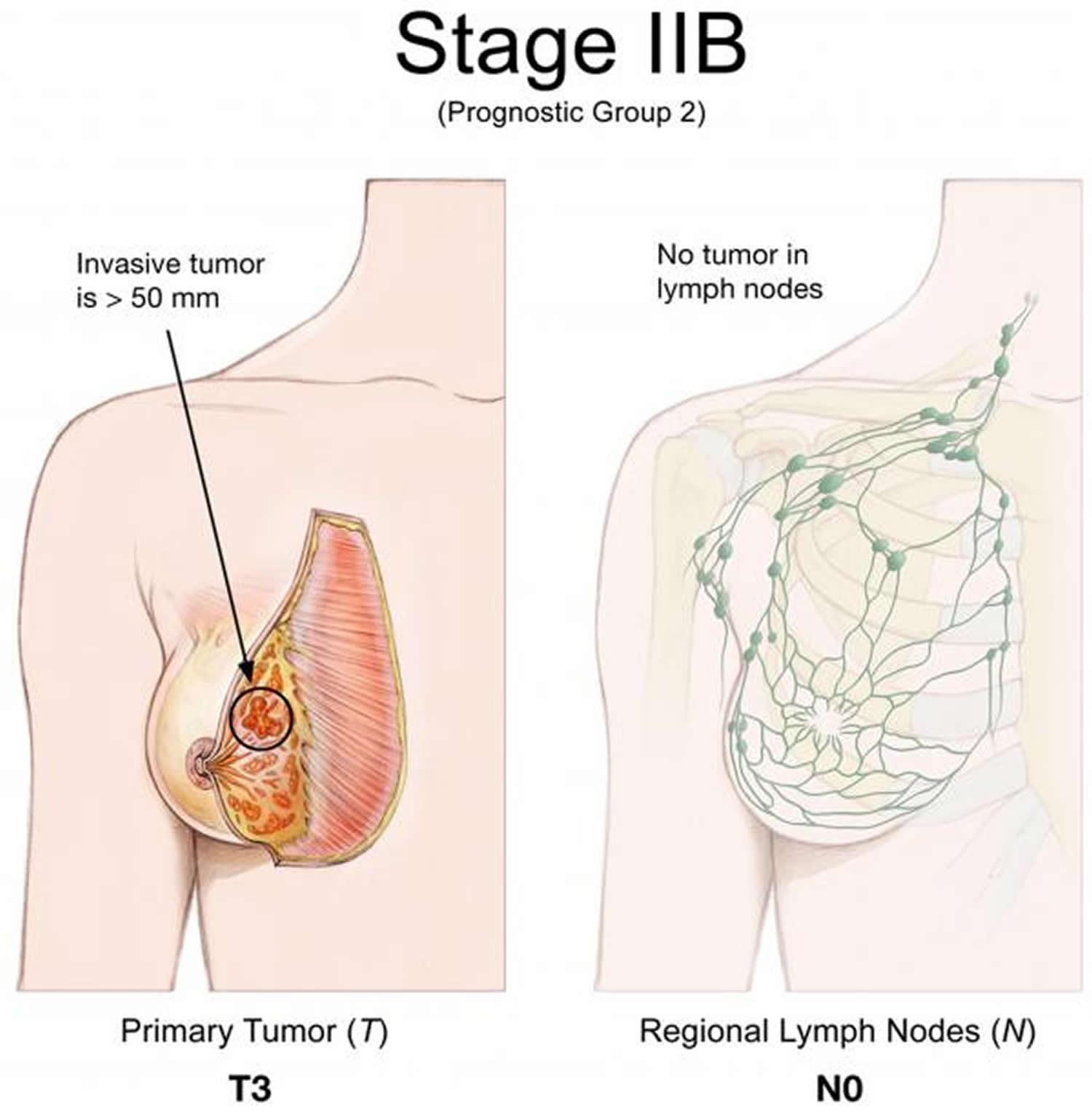
Stage 3A breast cancer
Stage 3A breast cancer: The cancer of any size has spread to 4 to 9 axillary lymph nodes, but not to other parts of the body (T0, T1, T2 or T3, N2, M0). Stage IIIA may also be a tumor larger than 50 mm that has spread to 1 to 3 lymph nodes (T3, N1, M0).
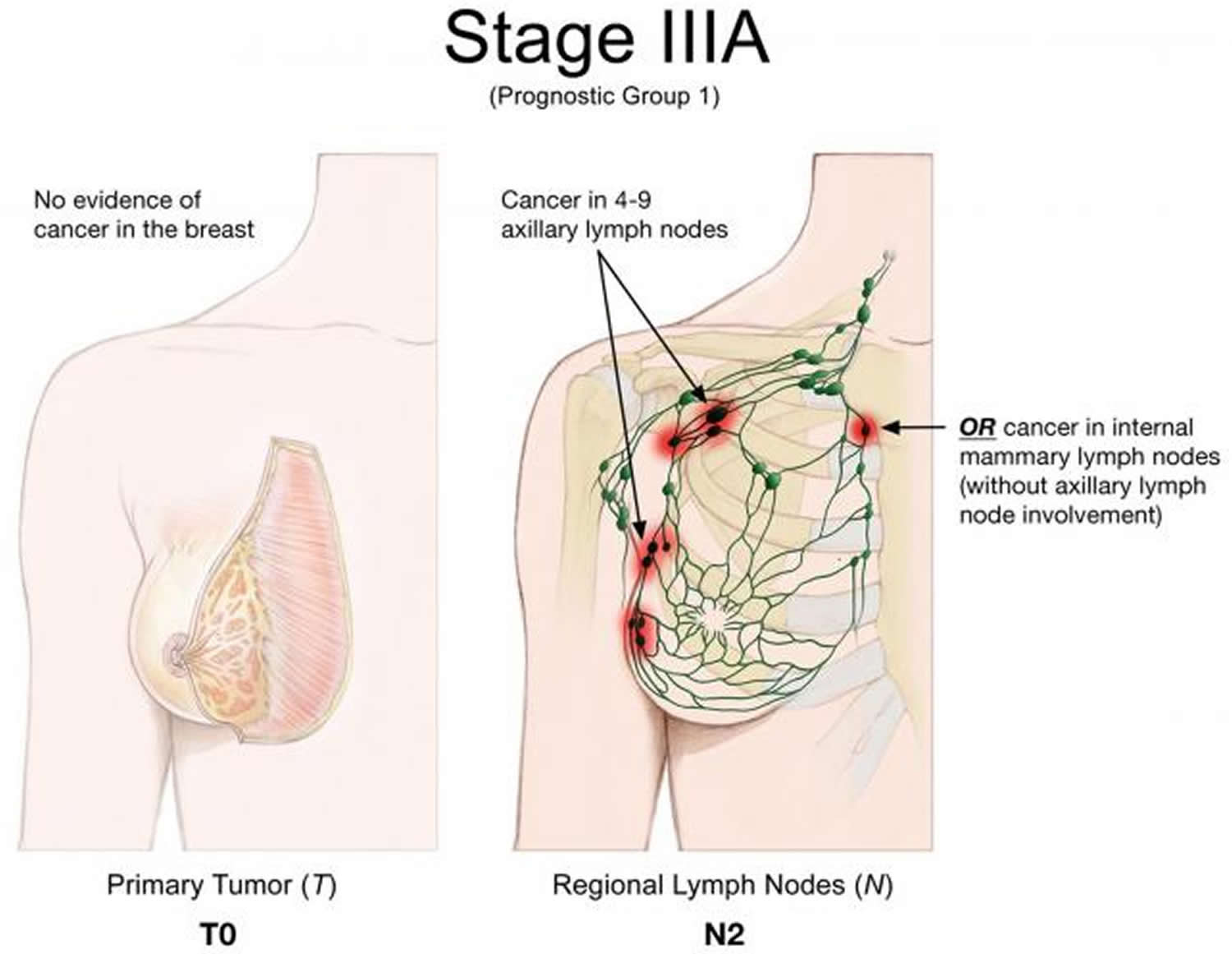
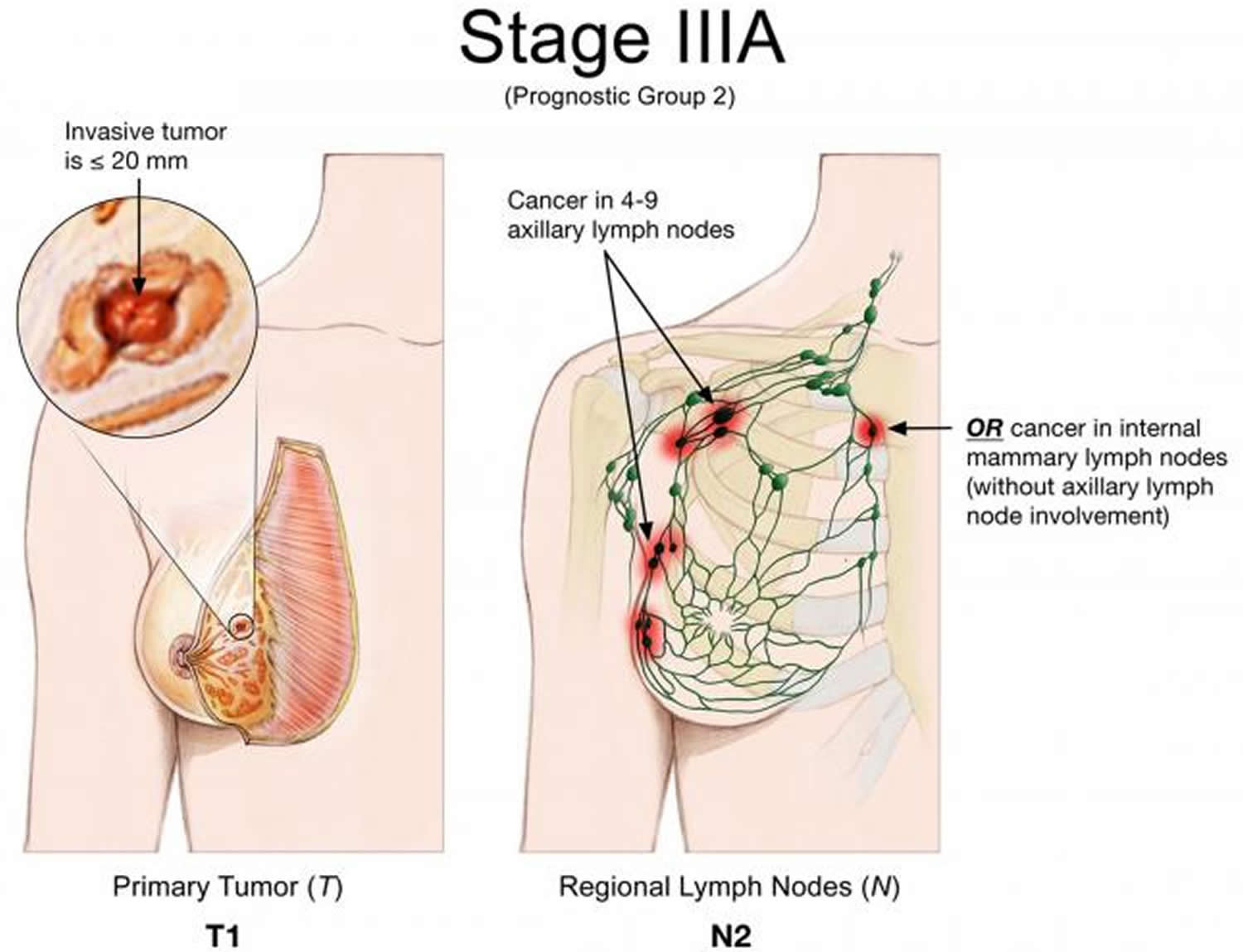
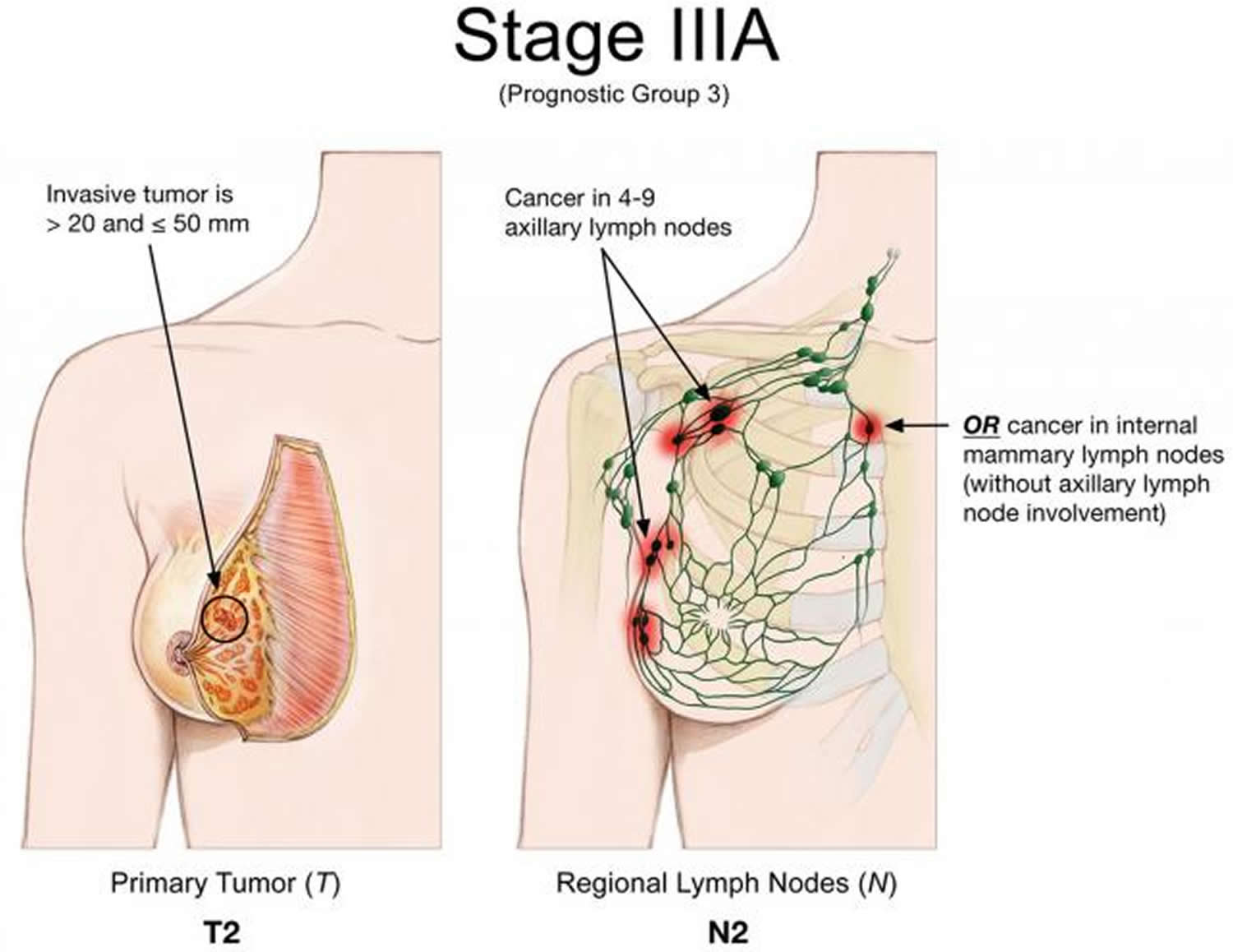
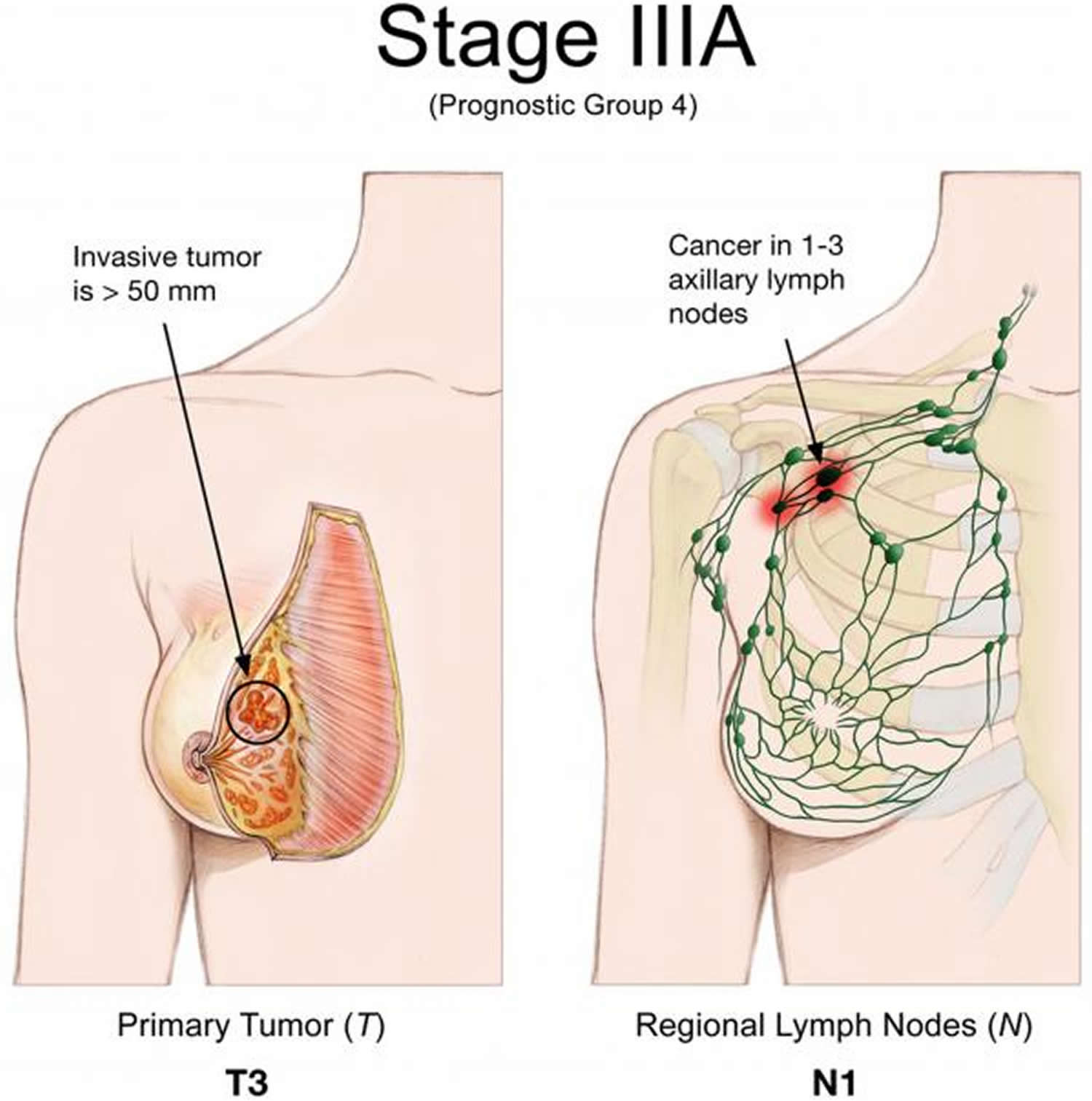
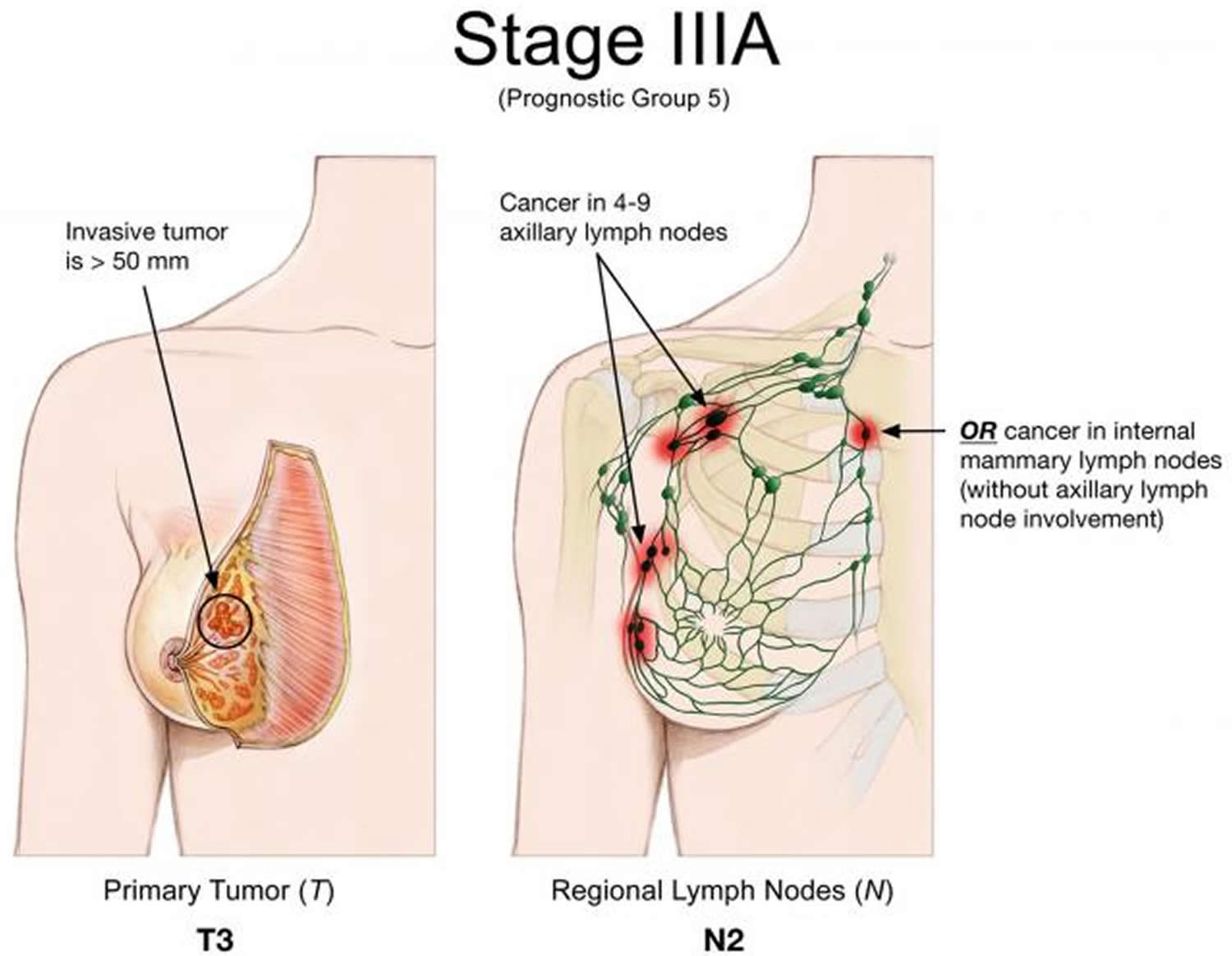
Stage 3B breast cancer
Stage 3B: The tumor has spread to the chest wall or caused swelling or ulceration of the breast or is diagnosed as inflammatory breast cancer. It may or may not have spread to the lymph nodes under the arm, but it has not spread to other parts of the body (T4; N0, N1 or N2; M0).
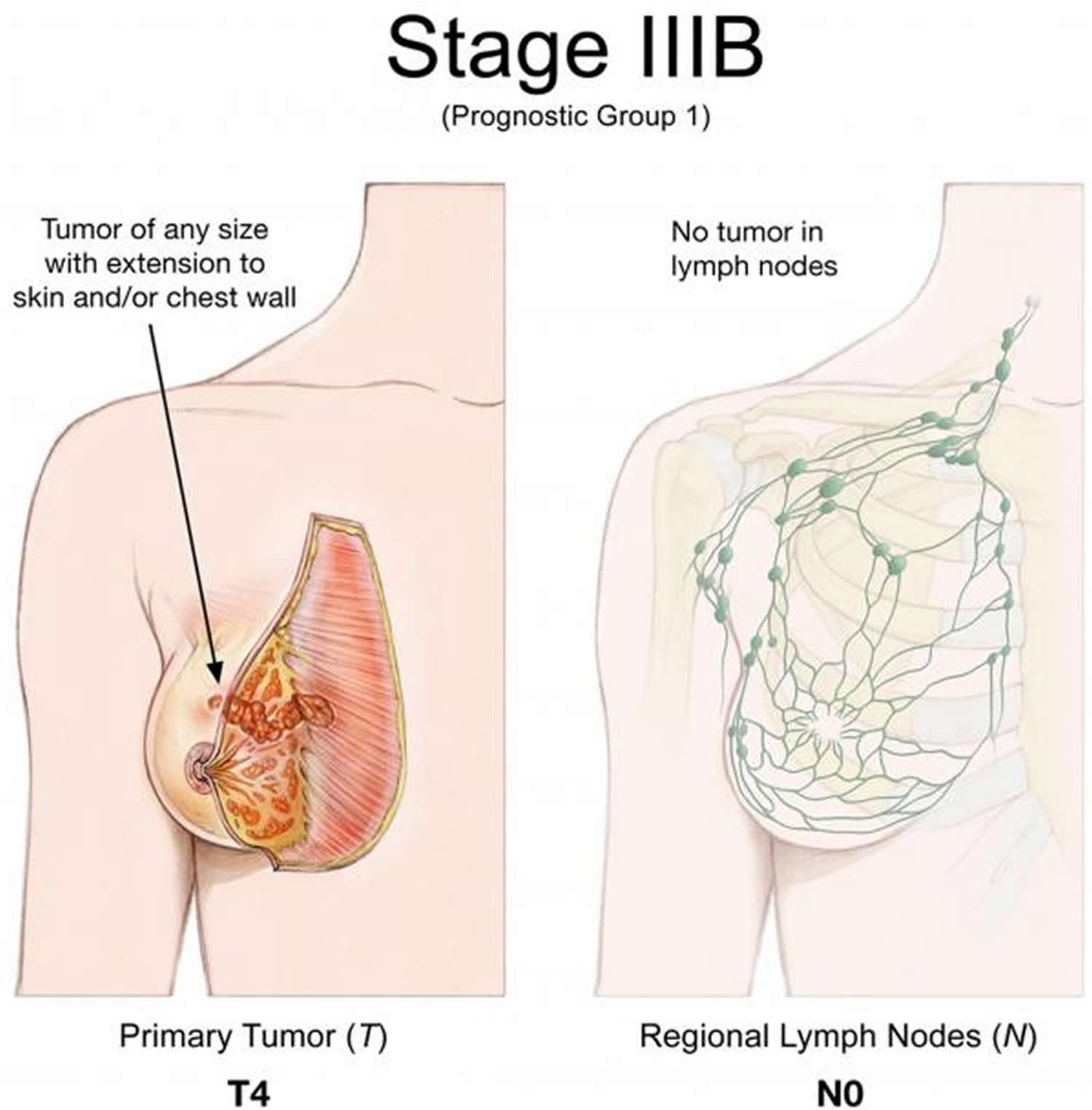
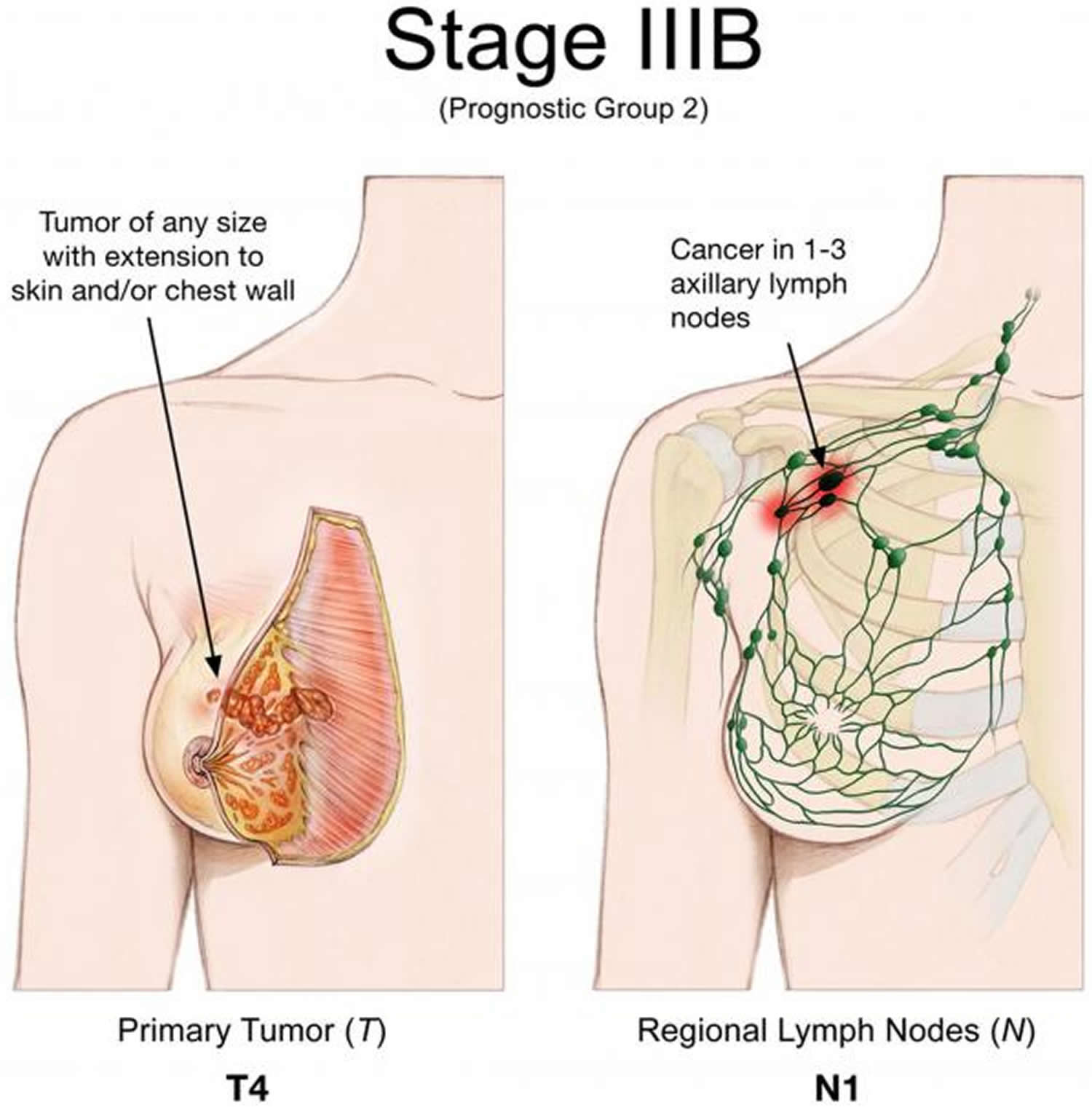
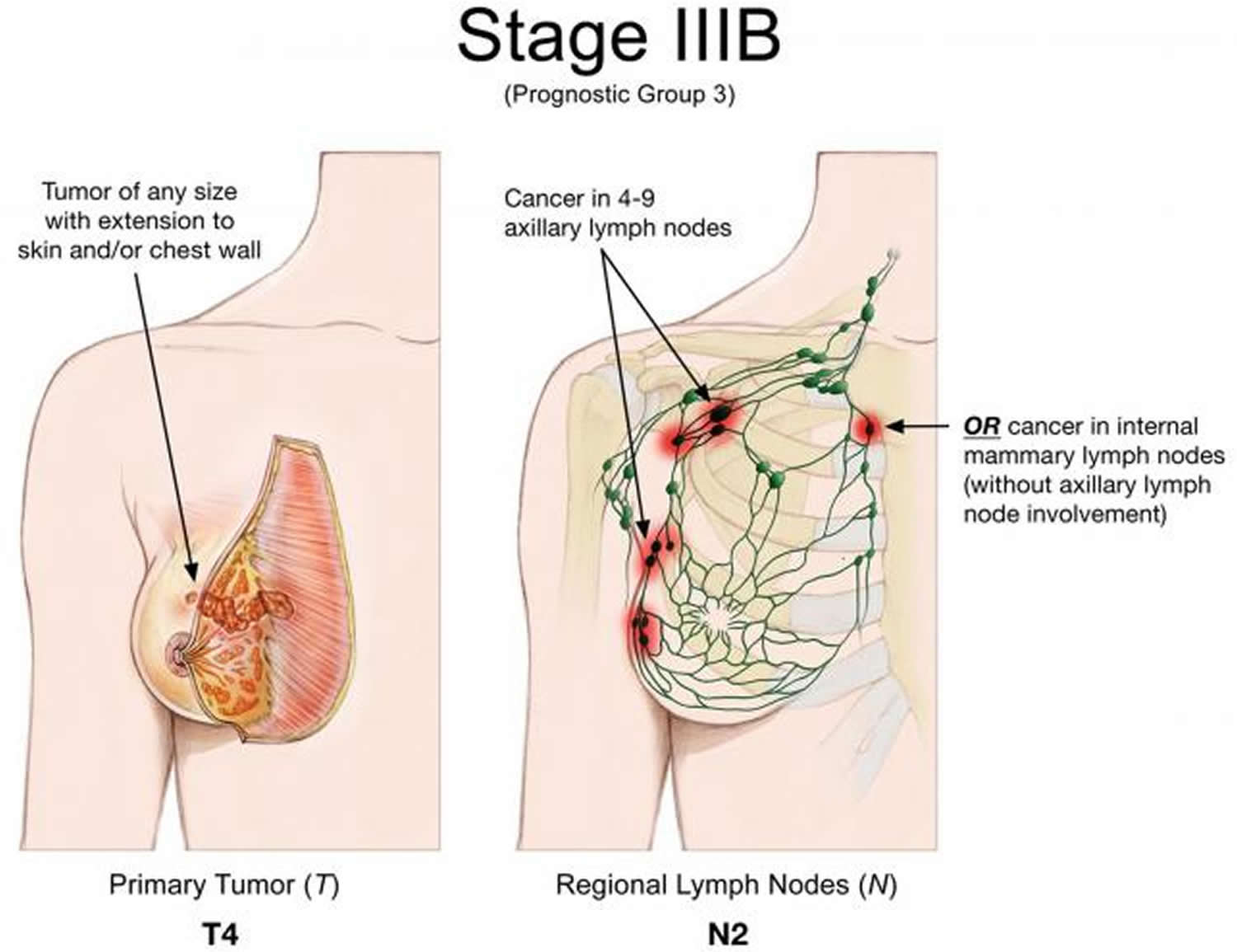 Stage 3C breast cancer
Stage 3C breast cancer
Stage 3C breast cancer: A tumor of any size that has not spread to distant parts of the body but has spread to 10 or more axillary lymph nodes or the lymph nodes in the N3 group (any T, N3, M0).
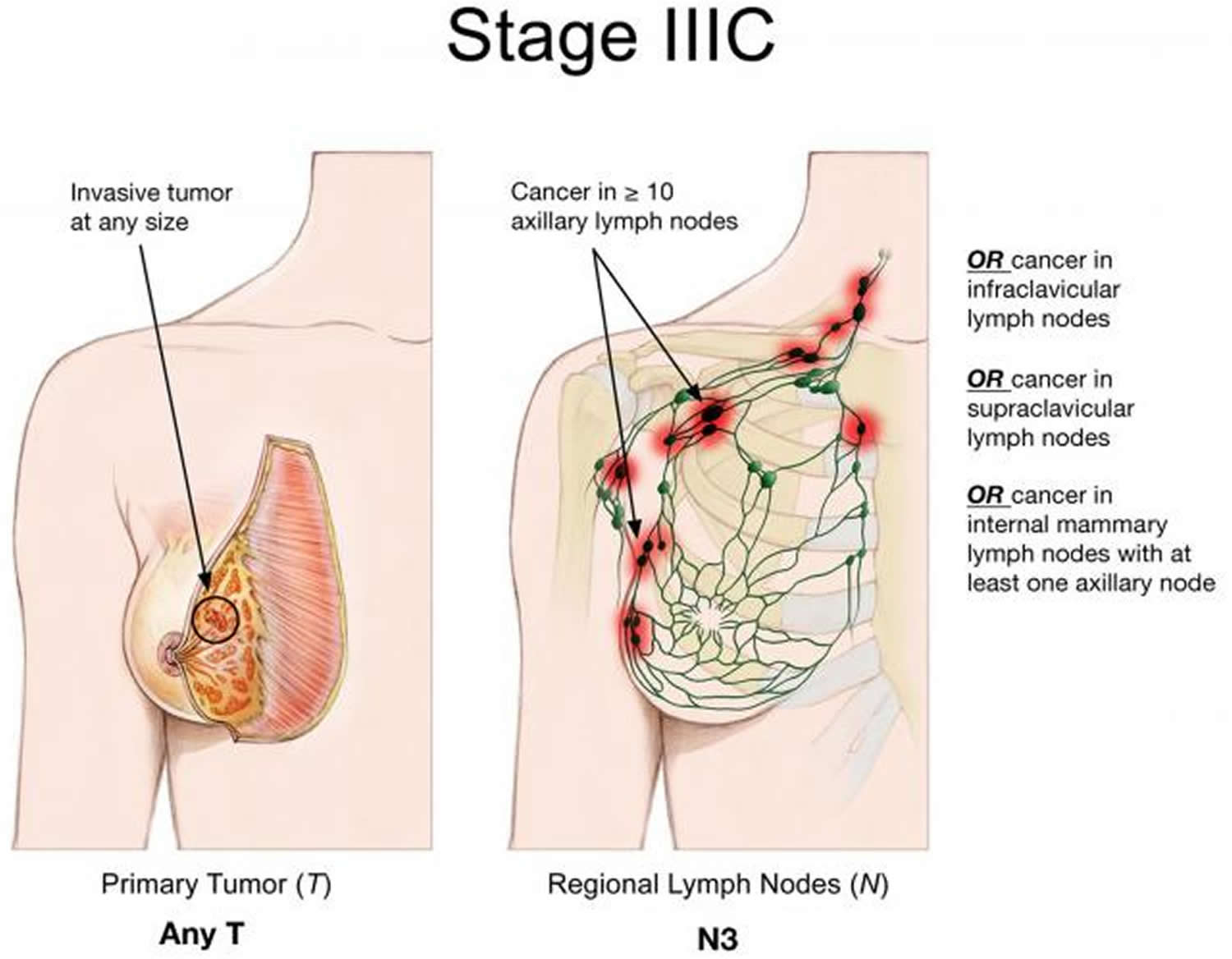 Stage 4 Metastatic breast cancer
Stage 4 Metastatic breast cancer
Stage 4 (metastatic) breast cancer: The tumor can be any size and has spread to other organs, such as the bones, lungs, brain, liver, distant lymph nodes, or chest wall (any T, any N, M1). Metastatic cancer spread found when the cancer is first diagnosed occurs about 5% to 6% of the time. This may be called de novo metastatic breast cancer. Most commonly, metastatic breast cancer is found after a previous diagnosis of early breast cancer.
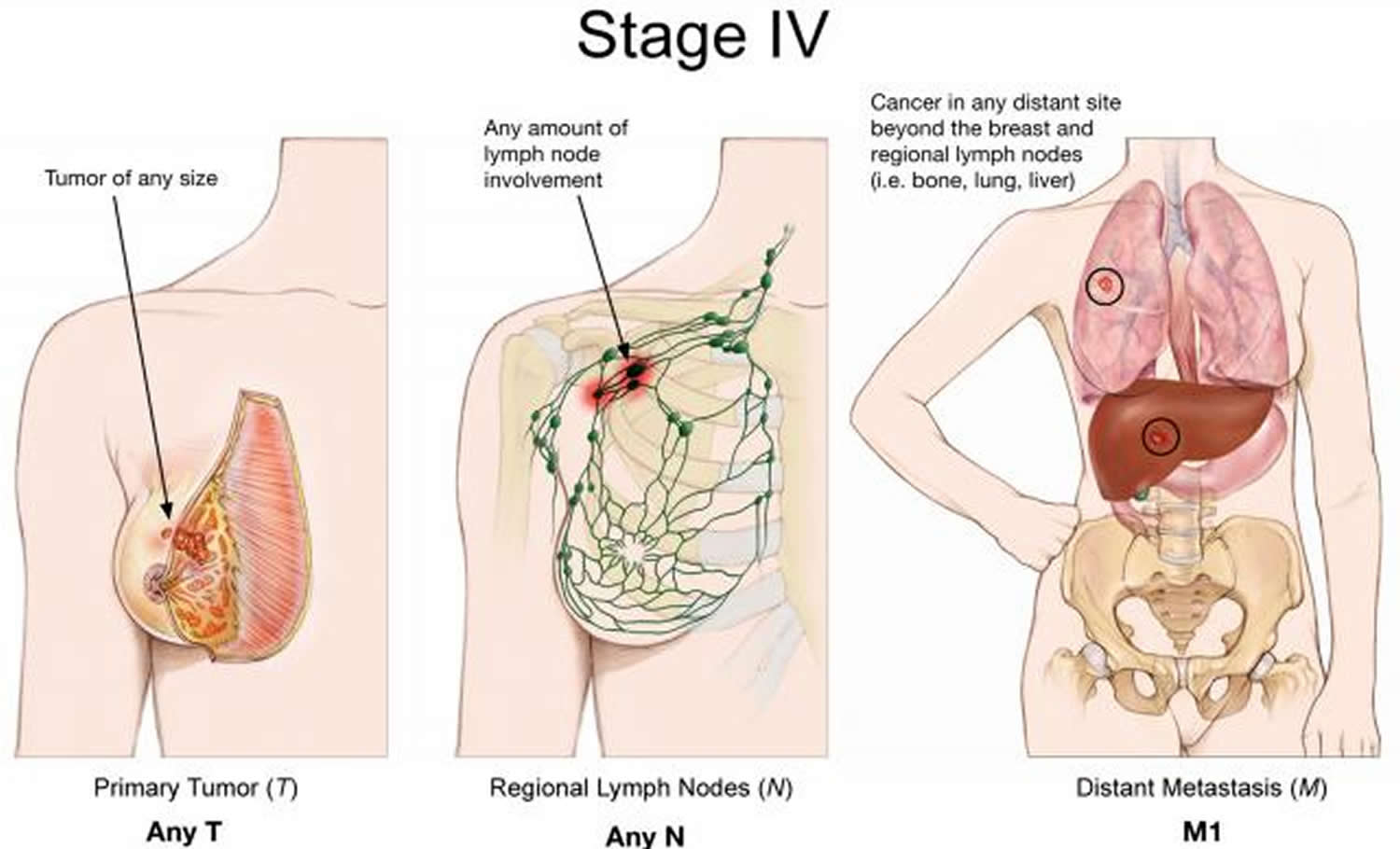
Recurrent breast cancer
Recurrent breast cancer is cancer that has come back after treatment, and can be described as local, regional, and/or distant. If the cancer does return, there will be another round of tests to learn about the extent of the recurrence. These tests and scans are often similar to those done at the time of the original diagnosis.
Breast cancer grade
The grade describes how a cancer cell looks under the microscope and whether they are similar or very different to normal cells. You might hear your doctor use the terms well differentiated, moderately differentiated, or poorly differentiated. A pathologist checks the cancer cells for features that can help predict how likely the cancer is to grow and spread. These include:
- the arrangement of the cells in relation to each other
- whether they form tubules (gland formation)
- how similar they look to normal breast cells (the nuclear grade)
- how many of the cells are dividing (the mitotic count)
These features taken together tell how differentiated the cancer is and the grade.
- Low grade (grade 1) the cells look similar to normal breast cells and are slow growing. These are well differentiated cancers. They are arranged in small tubules for ductal cancer and cords for lobular cancer. These cancers tend to grow and spread slowly and have a good outlook (prognosis).
- Intermediate grade (grade 2) the cells look quite different to normal breast cells. They are moderately differentiated. This means the features and outlook (prognosis) are somewhere between well and poorly differentiated.
- High grade (grade 3) the cells look very different to normal breast cells and are faster growing, these are poorly differentiated cancers that have abnormal features. They tend to grow and spread more quickly and have a worse outlook (prognosis).
Low grade cancers tend to grow more slowly than high grade. High grade cancers are more likely to come back after they have first been treated. But the grade can only give a guide to how any individual cancer will behave and individual cancers may behave differently.
Breast cancer treatment
Your doctor determines your breast cancer treatment options based on your type of breast cancer, its stage and grade, size, and whether the cancer cells are sensitive to hormones. Your doctor also considers your overall health and your own preferences.
Most women undergo surgery for breast cancer and also receive additional treatment before or after surgery, such as chemotherapy, hormone therapy or radiation.
There are many options for breast cancer treatment, and you may feel overwhelmed as you make complex decisions about your treatment. Consider seeking a second opinion from a breast specialist in a breast center or clinic. Talk to other women who have faced the same decision.
Breast cancer surgery
Operations used to treat breast cancer include:
Removing the breast cancer (lumpectomy). During a lumpectomy, which may be referred to as breast-conserving surgery or wide local excision, the surgeon removes the tumor and a small margin of surrounding healthy tissue.
A lumpectomy may be recommended for removing smaller tumors. Some people with larger tumors may undergo chemotherapy before surgery to shrink a tumor and make it possible to remove completely with a lumpectomy procedure.
Removing the entire breast (mastectomy). A mastectomy is an operation to remove all of your breast tissue. Most mastectomy procedures remove all of the breast tissue — the lobules, ducts, fatty tissue and some skin, including the nipple and areola (total or simple mastectomy).
Newer surgical techniques may be an option in selected cases in order to improve the appearance of the breast. Skin-sparing mastectomy and nipple-sparing mastectomy are increasingly common operations for breast cancer.
Removing a limited number of lymph nodes (sentinel node biopsy). To determine whether cancer has spread to your lymph nodes, your surgeon will discuss with you the role of removing the lymph nodes that are the first to receive the lymph drainage from your tumor.
If no cancer is found in those lymph nodes, the chance of finding cancer in any of the remaining lymph nodes is small and no other nodes need to be removed.
Removing several lymph nodes (axillary lymph node dissection). If cancer is found in the sentinel lymph nodes, your surgeon will discuss with you the role of removing additional lymph nodes in your armpit.
Removing both breasts. Some women with cancer in one breast may choose to have their other (healthy) breast removed (contralateral prophylactic mastectomy) if they have a very increased risk of cancer in the other breast because of a genetic predisposition or strong family history.
Most women with breast cancer in one breast will never develop cancer in the other breast. Discuss your breast cancer risk with your doctor, along with the benefits and risks of this procedure.
Complications of breast cancer surgery depend on the procedures you choose. Breast cancer surgery carries a risk of pain, bleeding, infection and arm swelling (lymphedema).
You may choose to have breast reconstruction after surgery. Discuss your options and preferences with your surgeon.
Consider a referral to a plastic surgeon before your breast cancer surgery. Your options may include reconstruction with a breast implant (silicone or water) or reconstruction using your own tissue. These operations can be performed at the time of your mastectomy or at a later date.
Radiation therapy
Radiation therapy uses high-powered beams of energy, such as X-rays and protons, to kill cancer cells. Radiation therapy is typically done using a large machine that aims the energy beams at your body (external beam radiation). But radiation can also be done by placing radioactive material inside your body (brachytherapy).
External beam radiation of the whole breast is commonly used after a lumpectomy. Breast brachytherapy may be an option after a lumpectomy if you have a low risk of cancer recurrence.
Doctors may also recommend radiation therapy to the chest wall after a mastectomy for larger breast cancers or cancers that have spread to the lymph nodes.
Breast cancer radiation can last from three days to six weeks, depending on the treatment. A doctor who uses radiation to treat cancer (radiation oncologist) determines which treatment is best for you based on your situation, your cancer type and the location of your tumor.
Side effects of radiation therapy include fatigue and a red, sunburn-like rash where the radiation is aimed. Breast tissue may also appear swollen or more firm. Rarely, more-serious problems may occur, such as damage to the heart or lungs or, very rarely, second cancers in the treated area.
Chemotherapy
Chemotherapy uses drugs to destroy fast-growing cells, such as cancer cells. If your cancer has a high risk of returning or spreading to another part of your body, your doctor may recommend chemotherapy after surgery (adjuvant chemotherapy) to decrease the chance that the cancer will recur.
Chemotherapy is sometimes given before surgery (neoadjuvant chemotherapy) in women with larger breast tumors. The goal is to shrink a tumor to a size that makes it easier to remove with surgery.
Chemotherapy is also used in women whose cancer has already spread to other parts of the body (metastatic breast cancer). Sometimes, if cancer spreads to the spinal fluid, which surrounds and cushions the brain and spinal cord, chemo may be given directly into in this area (called intrathecal chemotherapy). Chemotherapy may be recommended to try to control the cancer and decrease any symptoms the cancer is causing.
In most cases, chemo has the greatest effect when more than one drug is used at a time. Often, combinations of 2 or 3 drugs are used. Doctors use many different combinations, and it’s not clear that any particular drug combination is the best.
Adjuvant and neoadjuvant chemo drugs 17:
- Anthracyclines, such as doxorubicin (Adriamycin) and epirubicin (Ellence)
- Taxanes, such as paclitaxel (Taxol) and docetaxel (Taxotere)
- 5-fluorouracil (5-FU) or capecitabine (Xeloda)
- Cyclophosphamide (Cytoxan)
- Carboplatin (Paraplatin)
Chemo drugs for breast cancer that has spread (metastatic breast cancer) 17:
- Taxanes: Paclitaxel (Taxol), docetaxel (Taxotere), and albumin-bound paclitaxel (Abraxane)
- Ixabepilone (Ixempra)
- Eribulin (Halaven)
- Anthracyclines: Doxorubicin (Adriamycin), liposomal doxorubicin (Doxil), and epirubicin (Ellence)
- Platinum agents (Cisplatin, carboplatin)
- Vinorelbine (Navelbine)
- Capecitabine (Xeloda)
- Gemcitabine (Gemzar)
- Antibody drug conjugates (Ado-trastuzumab emtansine [Kadcyla], Fam-trastuzumab deruxtecan [Enhertu], Sacituzumab govitecan [Trodelvy])
Although drug combinations are often used to treat early breast cancer, advanced breast cancer often is treated with single chemo drugs. Still, some combinations, such as paclitaxel plus gemcitabine, are commonly used to treat metastatic breast cancer.
For cancers that are HER2-positive, one or more drugs that target HER2 may be used with chemo.
Chemotherapy side effects depend on the drugs you receive. Common side effects include hair loss, nausea, vomiting, fatigue and an increased risk of developing an infection. Rare side effects can include premature menopause, infertility (if premenopausal), damage to the heart and kidneys, nerve damage (neuropathy), and, very rarely, blood cell cancer (e.g., myelodysplastic syndromes, acute myeloid leukemia).
Certain chemo drugs, such as capecitabine (Xeloda) and liposomal doxorubicin (Doxil), can irritate the palms of the hands and the soles of the feet. This is called hand-foot syndrome. Early symptoms include numbness, tingling, and redness. If it gets worse, the hands and feet can become swollen and uncomfortable or even painful. The skin may blister, leading to peeling or even open sores. There is no specific treatment, although some creams or steroids given before chemo may help. These symptoms gradually get better when the drug is stopped or the dose is lowered. The best way to prevent severe hand-foot syndrome is to tell your doctor when symptoms first come up, so that the drug dose can be changed or other medicines can be given.
Many women who are treated with chemotherapy for breast cancer report a slight decrease in mental functioning called ‘chemo brain’. They may have some problems with concentration and memory, which may last a long time. Although many women have linked this to chemo, ‘chemo brain’ is also has been seen in women who did not get chemo as part of their treatment. Still, most women function well after treatment. In studies that have found chemo brain to be a side effect of treatment, the symptoms most often last for a few years.
Hormone therapy
Hormone therapy — perhaps more properly termed hormone-blocking therapy — is often used to treat breast cancers that are sensitive to hormones. Doctors sometimes refer to these cancers as estrogen receptor positive (ER positive) and progesterone receptor positive (PR positive) cancers.
Hormone therapy can be used before or after surgery or other treatments to decrease the chance of your cancer returning. If the cancer has already spread, hormone therapy may shrink and control it.
Treatments that can be used in hormone therapy include:
- Medications that block hormones from attaching to cancer cells (selective estrogen receptor modulators)
- Tamoxifen blocks estrogen from connecting to the cancer cells and telling them to grow and divide. While tamoxifen acts like an anti-estrogen in breast cells, it acts like an estrogen in other tissues, like the uterus and the bones. Because of this, it is called a selective estrogen receptor modulator (SERM). It can be used to treat women with breast cancer who have or have not gone through menopause. Tamoxifen can be used in several ways:
- In women at high risk of breast cancer, tamoxifen can be used to help lower the risk of developing breast cancer.
- For women who have been treated with breast-conserving surgery for ductal carcinoma in situ (DCIS) that is hormone receptor-positive, taking tamoxifen for 5 years lowers the chance of the DCIS coming back in the same breast. It also lowers the chance of getting an invasive breast cancer or another DCIS in both breasts.
- For women with hormone receptor-positive invasive breast cancer treated with surgery, tamoxifen can help lower the chances of the cancer coming back and improve the chances of living longer. It can also lower the risk of a new cancer developing in the other breast. Tamoxifen can be started either after surgery (adjuvant therapy) or before surgery (neoadjuvant therapy). When given after surgery, it is usually taken for 5 to 10 years. This drug is used mainly for women with early-stage breast cancer who have not yet gone through menopause. If you have gone through menopause, aromatase inhibitors (see below) are often used instead.
- For women with hormone-positive breast cancer that has spread to other parts of the body, tamoxifen can often help slow or stop the growth of the cancer, and might even shrink some tumors.
- Toremifene (Fareston) is another selective estrogen receptor modulator (SERM) that works in a similar way, but it is used less often and is only approved to treat post-menopausal women with metastatic breast cancer. It is not likely to work if tamoxifen has already been used and has stopped working. These drugs are pills, taken by mouth.
- The most common side effects of tamoxifen and toremifene are:
- Hot flashes
- Vaginal dryness or discharge
- Changes in the menstrual cycle
- When tamoxifen treatment starts, a small number of women with cancer that has spread to the bones might have a tumor flare (the tumor gets bigger for a short time) which can cause bone pain. This usually decreases quickly, but in some rare cases a woman may also develop a high calcium level in the blood that is hard to control. If this happens, the treatment may need to be stopped for a time.
- Rare, but more serious side effects are also possible:
- If a woman has gone through menopause, selective estrogen receptor modulators (SERMs) can increase her risk of developing endometrial cancer and uterine sarcoma. Tell your doctor right away about any unusual vaginal bleeding (a common symptom of this cancer). Most uterine bleeding is not from cancer, but this symptom always needs quick attention.
- Blood clots are another uncommon, but serious side effect. They usually form in the legs (called deep vein thrombosis or DVT), but sometimes a piece of clot in the leg may break off and end up blocking an artery in the lungs (pulmonary embolism or PE). Call your doctor or nurse right away if you develop pain, redness, or swelling in your lower leg (calf), shortness of breath, or chest pain, because these can be symptoms of a DVT or PE. Rarely, tamoxifen has been associated with strokes in postmenopausal women, so tell your doctor if you have severe headaches, confusion, or trouble speaking or moving.
- Eye problems, such as cataracts, are sometimes seen when taking tamoxifen. It is important to tell your doctor right away if you are having any new trouble with your eyesight.
- Bones can be affected. Depending on a woman’s menopausal status, tamoxifen can have different effects on the bones. In pre-menopausal women, tamoxifen can cause some bone thinning, but in post-menopausal women it often strengthens bones to some degree. The benefits of taking these drugs outweigh the risks for almost all women with hormone receptor-positive breast cancer.
- Tamoxifen blocks estrogen from connecting to the cancer cells and telling them to grow and divide. While tamoxifen acts like an anti-estrogen in breast cells, it acts like an estrogen in other tissues, like the uterus and the bones. Because of this, it is called a selective estrogen receptor modulator (SERM). It can be used to treat women with breast cancer who have or have not gone through menopause. Tamoxifen can be used in several ways:
- Selective estrogen receptor degrader (SERD) such as Fulvestrant (Faslodex) is a drug that attaches to and breaks down estrogen receptors. Fulvestrant (Faslodex) acts like an anti-estrogen throughout the body. When given to pre-menopausal women it must be combined with a luteinizing-hormone releasing hormone (LHRH) agonist to turn off the ovaries. Fulvestrant (Faslodex) is given by 2 injections into the buttocks (bottom). For the first month, the 2 shots are given 2 weeks apart. After that, they are given once a month.
- Fulvestrant can be given:
- Alone to treat advanced breast cancer that has not been treated with other hormone therapy.
- Alone to treat advanced breast cancer after other hormone drugs (like tamoxifen and often an aromatase inhibitor) have stopped working.
- In combination with a CDK 4/6 inhibitor or PI3K inhibitor to treat metastatic breast cancer as initial hormone therapy or after other hormone treatments have been tried.
- Common short-term side effects of fulvestrant can include:
- Hot flashes and/or night sweats
- Headache
- Mild nausea
- Bone pain
- Injection site pain
- Fulvestrant can be given:
- Medications that stop the body from making estrogen after menopause (aromatase inhibitors). Aromatase inhibitors work by preventing aromatase from making estrogen. Aromatase inhibitors are useful for women who have gone through menopause, although they can also be used in pre-menopausal women when they are combined with ovarian suppression (see below).
- These aromatase inhibitors are pills taken every day to treat breast cancer:
- Letrozole (Femara)
- Anastrozole (Arimidex)
- Exemestane (Aromasin)
- The most common side effects of aromatase inhibitors are:
- Hot flashes
- Vaginal dryness
- Bone and joint pain
- Muscle pain
- Aromatase inhibitors tend to have side effects different from tamoxifen. They don’t cause uterine cancers and very rarely cause blood clots. They can, however, cause muscle pain and joint stiffness and/or pain. The joint pain may be similar to a feeling of having arthritis in many different joints at one time. Options for treating this side effect include, stopping the AI and then switching to a different aromatase inhibitor, taking a medicine called duloxetine (Cymbalta), or routine exercise with nonsteroidal anti-inflammatory drugs (NSAIDs). But the muscle and joint pain has led some women to stop treatment. If this happens, most doctors recommend using tamoxifen to complete 5 to 10 years of hormone treatment.
- Because aromatase inhibitors drastically lower the estrogen level in women after menopause, they can also cause bone thinning, sometimes leading to osteoporosis and even fractures. If you are taking an aromatase inhibitor, your bone density may be tested regularly and you may also be given bisphosphonates (zoledronic acid [Zometa] for example) or denosumab (Xgeva, Prolia), to strengthen your bones.
- These aromatase inhibitors are pills taken every day to treat breast cancer:
- Ovarian suppression. There are several ways to remove or shut down the ovaries to treat breast cancer:
- Oophorectomy: Surgery to remove the ovaries. This is permanent and is also called ovarian ablation.
- Luteinizing hormone-releasing hormone (LHRH) agonists: These drugs are used more often than oophorectomy. They stop the signal that the body sends to the ovaries to make estrogen, which causes temporary menopause. Common LHRH drugs include goserelin (Zoladex) and leuprolide (Lupron). They can be used alone or with other hormone drugs (tamoxifen, aromatase inhibitors, fulvestrant) as hormone therapy in pre-menopausal women.
- Chemotherapy drugs: Some chemo drugs can damage the ovaries of pre-menopausal women so they no longer make estrogen. Ovarian function can return months or years later in some women, but in others the damage to the ovaries is permanent and leads to menopause.
- For pre-menopausal women, removing or shutting down the ovaries (ovarian suppression), which are the main source of estrogen, is effectively making them post-menopausal. All of these methods can cause symptoms of menopause, including hot flashes, night sweats, vaginal dryness, and mood swings.
- Ovarian suppression along with tamoxifen or an aromatase inhibitor might be recommended for women whose breast cancer is at high risk of coming back.
After surgery, hormone therapy can be given to reduce the risk of the cancer coming back. Taking an aromatase inhibitor, either alone or after tamoxifen, has been shown to work better than taking just tamoxifen for 5 years.
These hormone therapy schedules are known to be helpful for women who are post-menopausal when diagnosed:
- Tamoxifen for 2 to 3 years, followed by an aromatase inhibitor for 2 to 3 years (5 years total of treatment)
- Tamoxifen for 2 to 3 years, followed by an aromatase inhibitor for 5 years (7 to 8 years of treatment)
- Tamoxifen for 4½ to 6 years, followed by an aromatase inhibitor for 5 years (9½ to 11 years of treatment)
- Tamoxifen for 5 to 10 years
- An aromatase inhibitor for 5 to 10 years
- An aromatase inhibitor for 2 to 3 years, followed by tamoxifen for 2 to 3 years (5 years total of treatment)
- For women who are unable to take an aromatase inhibitor, tamoxifen for 5 to 10 years is an option
For most post-menopausal women whose cancers are hormone receptor-positive, most doctors recommend taking an aromatase inhibitor at some point during adjuvant (after surgery) therapy. Standard treatment is to take these drugs for about 5 years, or to take in sequence with tamoxifen for 5 to 10 years. For women at a higher risk of recurrence, hormone treatment for longer than 5 years may be recommended. Tamoxifen is an option for some women who cannot take an aromatase inhibitor. Taking tamoxifen for 10 years is considered more effective than taking it for 5 years, but you and your doctor will decide the best schedule of treatment for you.
These therapy schedules are known to be helpful for women who are pre-menopausal when diagnosed:
- Tamoxifen (with or without ovarian suppression) for 5 to 10 years.
- Tamoxifen (with or without ovarian suppression) for 5 years followed by an aromatase inhibitor for 5 years if you have gone through menopause.
- Aromatase inhibitor plus some sort of ovarian suppression (see above) for 5 to 10 years.
If you have early-stage breast cancer and had not gone through menopause when you were first diagnosed, your doctor might recommend taking tamoxifen first, and then taking an aromatase inhibitor later if you go through menopause during treatment. Another option is ovarian suppression by getting a drug called a luteinizing hormone-releasing hormone (LHRH) agonist, which turns off the ovaries, along with an aromatase inhibitor. Pre-menopausal women should not take an aromatase inhibitor alone for breast cancer treatment because it is unsafe and can increase hormone levels.
Targeted therapy drugs
Targeted drug therapy uses medicines that are directed at (target) proteins on breast cancer cells that help them grow, spread, and live longer. Targeted drugs work to destroy cancer cells or slow down their growth. As an example, several targeted therapy drugs focus on a protein that some breast cancer cells overproduce called human epidermal growth factor receptor 2 (HER2). The protein helps breast cancer cells grow and survive. By targeting cells that make too much HER2, the drugs can damage cancer cells while sparing healthy cells.
Targeted therapy drugs that focus on other abnormalities within cancer cells are available. And targeted therapy is an active area of cancer research.
Your cancer cells may be tested to see whether you might benefit from targeted therapy drugs. Some medications are used after surgery to reduce the risk that the cancer will return. Others are used in cases of advanced breast cancer to slow the growth of the tumor.
Immunotherapy for breast cancer
Immunotherapy is the use of medicines to boost a person’s own immune system to recognize and destroy cancer cells more effectively. Immunotherapy typically works on specific proteins involved in the immune system to enhance the immune response. An important part of the immune system is its ability to keep itself from attacking normal cells in the body. To do this, it uses proteins (or “checkpoints”) on immune cells that need to be turned on (or off) to start an immune response. Breast cancer cells sometimes use these checkpoints to avoid being attacked by the immune system. Drugs that target these checkpoint proteins (immune checkpoint inhibitors), help restore the immune response against breast cancer cells.
Immune checkpoint inhibitors for breast cancer include:
- PD-1 inhibitor
- Pembrolizumab (Keytruda) for breast cancer is a drug that targets PD-1 (a protein on immune system T cells that normally helps keep them from attacking other cells in the body). By blocking PD-1, these drugs boost the immune response against breast cancer cells. This can often shrink tumors.
- Pembrolizumab (Keytruda) can be used with chemotherapy to treat triple-negative breast cancer:
- Before and after surgery for stage 2 or 3 cancers
- That has come back (recurred) locally but can’t be removed by surgery
- That has spread to other parts of the body.
- Pembrolizumab (Keytruda) is given as an intravenous (IV) infusion, typically every 3 or 6 weeks. In certain situations, your doctor might test your cancer cells for the PD-L1 protein to show that the cancer is more likely to respond to treatment with pembrolizumab.
- Possible side effects of immune checkpoint inhibitors can include fatigue, cough, nausea, skin rash, poor appetite, constipation, and diarrhea. Other, more serious side effects occur less often.
- Infusion reactions: Some people might have an infusion reaction while getting these drugs. This is like an allergic reaction, and can include fever, chills, flushing of the face, rash, itchy skin, feeling dizzy, wheezing, and trouble breathing. It’s important to tell your doctor or nurse right away if you have any of these symptoms while getting these drugs.
- Autoimmune reactions: These drugs remove one of the protections on the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands, kidneys, or other organs.
It’s very important to report any new side effects to your health care team quickly. If serious side effects do occur, treatment may need to be stopped and you may get high doses of corticosteroids to suppress your immune system.
Treatment of Ductal Carcinoma in Situ (DCIS)
Ductal carcinoma in situ (DCIS) means the cells that line the milk ducts of the breast have become cancer, but they have not spread into surrounding breast tissue.
DCIS is considered non-invasive or pre-invasive breast cancer. DCIS can’t spread outside the breast, but it still needs to be treated because it can sometimes go on to become invasive breast cancer (which can spread).
In most cases, a woman with DCIS can choose between breast-conserving surgery (BCS) and simple mastectomy. But sometimes a mastectomy might be a better option.
Breast-conserving surgery (BCS)
In breast-conserving surgery (BCS), the surgeon removes the tumor and a small amount of normal breast tissue around it. Lymph node removal is not usually needed with breast-conserving surgery. It might be done after the first surgery if an area of invasive cancer is found. The chances an area of DCIS contains invasive cancer goes up with tumor size and how fast the cancer is growing. If lymph nodes are removed, this is usually done as a sentinel lymph node biopsy.
If breast-conserving surgery (BCS) is done, it is usually followed by radiation therapy. This lowers the chance of the cancer coming back in the same breast (either as more DCIS or as an invasive cancer). Breast-conserving surgery (BCS) without radiation therapy is not a standard treatment, but it might be an option for older women, women with other significant health problems, or women who had small areas of low-grade DCIS that were removed with large enough cancer-free surgical margins.
Many women with early-stage breast cancer, like DCIS, can choose between breast-conserving surgery (BCS) and mastectomy. The main advantage of BCS is that a woman keeps most of her breast. Some women might worry that having less extensive surgery might raise their risk of the cancer coming back. But studies following thousands of women for more than 20 years show that when BCS is done with radiation in women with early-stage cancer , survival is the same as having a mastectomy.
Mastectomy
Simple mastectomy (removal of the entire breast) may be needed if the area of DCIS is very large, if the breast has several separate areas of DCIS in different quadrants (multicentric), or if breast-conserving surgery cannot remove the DCIS completely (that is, the breast-conserving surgery specimen and re-excision specimens still have cancer cells in or near the surgical margins). If a mastectomy is needed for any of the reasons stated above, many doctors will do a sentinel lymph node biopsy along with the mastectomy because there is a higher chance that invasive cancer might be found. If an area of invasive cancer is found in the tissue removed during a mastectomy, the doctor won’t be able to go back and do sentinel lymph node biopsy later, and as a result may have to do a full axillary lymph node dissection instead.
Women having a mastectomy for DCIS typically don’t need radiation therapy and may choose to have breast reconstruction right away or later.
Hormone therapy after surgery
If the DCIS is hormone receptor-positive (estrogen or progesterone), treatment with tamoxifen (for any woman) or an aromatase inhibitor, such as exemestane or anastrozole, (for women past menopause) for 5 years after surgery can lower the risk of another DCIS or invasive cancer developing in either breast. If you have hormone receptor-positive DCIS, discuss the reasons for and against hormone therapy with your doctor.
Treatment of Lobular Carcinoma in Situ (LCIS)
Lobular carcinoma in situ (LCIS) means abnormal cells are in the lobules of the breast. In lobular carcinoma in situ (LCIS), cells that look like cancer cells are growing in the lining of the milk-producing glands (lobules) of the breast, but they don’t invade through the wall of the lobules. Lobular carcinoma in situ (LCIS) is sometimes grouped with ductal carcinoma in situ (DCIS) as a type of non-invasive breast cancer, but LCIS is different from DCIS and is not cancer. LCIS is not considered cancer, and it typically does not spread beyond the lobule (that is, it doesn’t become invasive breast cancer) if it isn’t treated. But having LCIS does increase your risk of later developing an invasive breast cancer in either breast. Women with LCIS have about a 7 to 12 times higher risk of developing invasive cancer in either breast. For this reason, doctors typically recommend that women with LCIS have regular breast cancer screening tests and follow-up visits with a health care provider for the rest of their lives.
The different types of LCIS are:
- Classic LCIS: The cells lining the lobules of the breast are smaller and are about the same size.
- Pleomorphic LCIS: The cells lining the lobules of the breast are larger and look more abnormal.
- Florid LCIS: The cells lining the lobules have grown into a large enough group that they have formed a mass, typically with an area of dead cells in the middle (called central necrosis).
Classic LCIS usually doesn’t cause a lump that can be felt or changes that can be seen on a mammogram, although pleomorphic and florid LCIS are sometimes found this way. Most often, LCIS is found when a breast biopsy is done for another problem that’s nearby. During a biopsy, small pieces of breast tissue are removed and checked in the lab.
Does LCIS need to be treated?
Having LCIS does increase your risk of developing invasive breast cancer later on. But since LCIS is not a true cancer or pre-cancer, often no treatment is recommended. Sometimes if a needle biopsy result shows LCIS , the doctor might recommend that it be removed completely (with an excisional biopsy or some other type of breast-conserving surgery) to help make sure that LCIS was the only thing there. This is especially true if the LCIS is described as pleomorphic or if it has necrosis (areas of dead cells), in which case it might be more likely to grow quickly.
With LCIS, close follow-up is very important. This usually includes a yearly mammogram and a breast exam. Close follow-up of both breasts is important because women with LCIS in one breast have the same increased risk of developing cancer in both breasts. There isn’t enough evidence to recommend getting routine magnetic resonance imaging (MRI) in addition to mammograms for all women with LCIS, but it’s reasonable for women with LCIS to talk with their doctors about their other risk factors and the benefits and limits of being screened yearly with MRI.
Most of the time, LCIS is only a risk factor for developing breast cancer, except in a certain kind of LCIS, called pleomorphic LCIS. This type may be more likely to turn into invasive cancer than most types of LCIS. Some doctors feel that this kind of LCIS needs to be removed completely with surgery.
Newer evidence is suggesting LCIS may be more of a pre-cancer than we thought. More research is being done.
Options for women at high risk of breast cancer because of LCIS may include:
- Seeing a health care provider more often (such as every 6 to 12 months) for a breast exam along with the yearly mammogram. Additional imaging with breast MRI may also be recommended, especially if a woman has other factors that raise her risk of breast cancer.
- Making lifestyle changes to lower breast cancer risk.
- Taking medicine to help lower the risk of breast cancer.
- Surgery, called bilateral prophylactic mastectomy (removal of both breasts), to reduce risk. This is more likely to be a reasonable option in women who also have other risk factors for breast cancer, such as a BRCA gene mutation. This may be followed later by breast reconstruction.
Can you lower your risk of invasive breast cancer?
If you have LCIS, you may want to consider taking a hormone medicine such as tamoxifen, raloxifene, or aromatase inhibitors to help reduce your risk of breast cancer. You might also want to consider taking part in a clinical trial for breast cancer prevention, or discussing other possible prevention strategies (such as getting to a healthy weight or starting an exercise program) with your doctor.
Because LCIS is linked to an increased risk of cancer in both breasts, some women with LCIS choose to have a bilateral simple mastectomy (removal of both breasts but not nearby lymph nodes) to lower this risk. This is more likely to be a reasonable option in women who also have other risk factors for breast cancer, such as a BRCA gene mutation or a strong family history. This may be followed by delayed breast reconstruction.
Treatment of Breast Cancer Stages 1-3
The stage (extent) of your breast cancer is an important factor in making decisions about your treatment.
Most women with breast cancer in stages 1, 2, or 3 are treated with surgery, often followed by radiation therapy. Many women also get some kind of drug therapy. In general, the more the breast cancer has spread, the more treatment you will likely need. But your treatment options are affected by your personal preferences and other information about your breast cancer, such as:
- If the cancer cells contain hormone receptors (that is, if the cancer is ER-positive or PR-positive)
- If the cancer cells have large amounts of the HER2 protein (that is, if the cancer is HER2-positive)
- How fast the cancer is growing (measure by grade or Ki-67)
- Your overall health
- If you have gone through menopause or not
Talk with your doctor about how these factors can affect your treatment options.
What type of drug treatment(s) might I get?
Most women with breast cancer in stages 1, 2 or 3 will get some kind of drug therapy as part of their treatment. This may include:
- Chemotherapy
- Hormone therapy (tamoxifen, an aromatase inhibitor, or one followed by the other)
- HER2 targeted drugs, such as trastuzumab (Herceptin), pertuzumab (Perjeta), or abemaciclib (Verzenio)
- Immunotherapy
- Some combination of these
The types of drugs that might work best depend on the tumor’s hormone receptor status, HER2 status, and other factors.
Treating stage 1 breast cancer
These breast cancers are still relatively small and either have not spread to the lymph nodes or have spread to only a tiny area in the sentinel lymph node (the first lymph node to which cancer is likely to spread).
Surgery
Surgery is the main treatment for stage I breast cancer. These cancers can be treated with either breast-conserving surgery (BCS; sometimes called lumpectomy or partial mastectomy) or mastectomy. The nearby lymph nodes will also need to be checked, either with a sentinel lymph node biopsy (SLNB) or an axillary lymph node dissection (ALND).
In some cases, breast reconstruction can be done at the same time as the surgery to remove the cancer. But if you will need radiation therapy after surgery, it is better to wait to get reconstruction until after the radiation is complete.
Radiation therapy
If breast-conserving surgery (BCS) is done, radiation therapy is usually given after surgery to lower the chance of the cancer coming back in the breast and to also help women live longer.
In a separate group, women who are at least 65 years old may consider breast-conserving surgery (BCS) without radiation therapy if ALL of the following are true:
- The tumor was 3 cm (a little more than 1 inch) or less across and it has been removed completely.
- None of the lymph nodes removed contained cancer.
- The cancer is ER-positive or PR-positive, and hormone therapy will be given.
Radiation therapy given to women with these characteristics still lowers the chance of the cancer coming back, but it has not been shown to help them live longer.
If you had a mastectomy, you are less likely to need radiation therapy, but it might be given depending on the details of your specific cancer. You should discuss if you need radiation treatment with your doctor. You might be sent to a doctor who specializes in radiation (a radiation oncologist) for evaluation.
Systemic therapy (chemo and other drugs)
If a woman has a hormone receptor-positive (ER-positive or PR-positive) breast cancer, most doctors will recommend hormone therapy (tamoxifen or an aromatase inhibitor, or one followed by the other) as an adjuvant (after surgery) treatment, no matter how small the tumor is. Women with tumors larger than 0.5 cm (about ¼ inch) across may be more likely to benefit from it. Hormone therapy is typically given for at least 5 years.
If the tumor is larger than 0.5 cm (about 1/4 inch) across, chemo after surgery (adjuvant chemotherapy) is sometimes recommended. A woman’s age when she is diagnosed may help in deciding if chemo should be offered or not. Some doctors may suggest chemo for smaller tumors as well, especially if they have any unfavorable features (a cancer that is growing fast; hormone receptor-negative, HER2-positive; or having a high score on a gene panel such as Oncotype DX).
After surgery, some women with HER2-positive cancers will be treated with trastuzumab (with or without pertuzumab) for up to 1 year.
Many women with HER2-positive cancers will be treated with neoadjuvant (before surgery) chemo and trastuzumab (with or without pertuzumab) followed by surgery and more trastuzumab (with or without pertuzumab) for up to 1 year. If after neoadjuvant therapy, residual cancer is found during surgery, trastuzumab may be changed to a different drug, called ado-trastuzumab emtansine, which is given every 3 weeks for 14 doses.
For women with a BRCA mutation and hormone-positive, HER2-negative breast cancer who received neoadjuvant chemotherapy but still have residual cancer at the time of surgery, the targeted drug olaparib might be given after surgery. It is usually given for one year. When given this way, it can help some women live longer.
Treating stage 2 breast cancer
Stage 2 breast cancers are larger than stage 1 cancers and/or have spread to a few nearby lymph nodes.
Local therapy (surgery and radiation therapy)
Stage 2 breast cancers are treated with either breast-conserving surgery (BCS; sometimes called lumpectomy or partial mastectomy) or mastectomy. The nearby lymph nodes will also be checked, either with a sentinel lymph node biopsy or an axillary lymph node dissection.
Women who have BCS are treated with radiation therapy after surgery. Women who have a mastectomy are typically treated with radiation if the cancer is found in the lymph nodes. Some patients who have a sentinel lymph node biopsy that shows cancer in a few lymph nodes might not have the rest of their lymph nodes removed to check for more cancer. In these patients, radiation may be discussed as a treatment option after mastectomy.
If you were initially diagnosed with stage 2 breast cancer and were given a systemic treatment such as chemotherapy or hormone therapy before surgery, radiation therapy might be recommended if cancer is found in the lymph nodes during mastectomy. A radiation oncologist may talk with you to see if radiation would be helpful.
If chemotherapy is also needed after surgery, the radiation will be delayed until the chemo is done.
In some women, breast reconstruction can be done during the surgery to remove the cancer. But if you will need radiation after surgery, it is better to wait to get reconstruction until after the radiation is complete.
Systemic therapy (chemo and other drugs)
Systemic therapy (drugs that travel to almost every part of the body) is recommended for some women with stage 2 breast cancer. Some systemic therapies are given before surgery (neoadjuvant therapy), and others are given after surgery (adjuvant therapy). For some women, systemic therapy will be started before surgery and then continued after surgery. Neoadjuvant treatments are a good option for women with large tumors, because they can shrink the tumor before surgery, possibly enough to make breast-conserving surgery an option.
Neoadjuvant treatment is also a preferable option for women with triple-negative breast cancer or HER2-positive breast cancer because the treatment given after surgery is often chosen depending on how much cancer is still in the breast and/or lymph nodes at the time of surgery. Some women with early-stage cancer who get neoadjuvant treatment might live longer if the cancer completely goes away with that treatment.
To help decide which women with stage 2 hormone receptor-positive, HER2-negative breast cancer will benefit from chemotherapy, a gene panel test such as Oncotype DX may be done on the tumor sample.
The drugs used will depend on the woman’s menopause status, as well as tumor test results. Treatment might include:
- Chemotherapy: Chemo can be given before and/or after surgery.
- HER2 targeted drugs: Some women with HER2-positive cancers will be treated with adjuvant (after surgery) chemotherapy with trastuzumab with or without pertuzumab for up to 1 year. Many women with HER2-positive cancers will be treated first with trastuzumab (with or without pertuzumab) followed by surgery and then more trastuzumab (with or without pertuzumab) for up to a year. If after neoadjuvant therapy, residual cancer is found at the time of surgery, the targeted drug, ado-trastuzumab emtansine, may be used instead of trastuzumab. It is given every 3 weeks for 14 doses. For women with hormone receptor-positive cancer found in the lymph nodes after completing 1 year of trastuzumab, the doctor might also recommend additional treatment with an oral targeted drug called neratinib for 1 year.
- Hormone therapy: If the cancer is hormone receptor-positive, hormone therapy (tamoxifen, an aromatase inhibitor or one followed by the other) is typically used. It can be started before surgery, but because it continues for at least 5 years, it needs to be given after surgery as well.
- Targeted drug therapy: For women with early-stage breast cancer that is hormone receptor-positive, HER2-negative, has cancer in the lymph nodes, and has a high chance of coming back, the targeted drug abemaciclib can be given after surgery along with tamoxifen or an AI. It is a pill typically given for 2 years twice a day. For women who have a BRCA mutation with a hormone receptor-positive, HER2-negative tumor who still have cancer in the tissue removed at surgery after neoadjuvant chemo, the targeted drug olaparib might be given for one year to help lower the chance of the cancer recurring. When given this way, it can help some women live longer.
- Immunotherapy: Women with triple-negative breast cancer might get the immunotherapy drug, pembrolizumab, before surgery and then again after surgery.
Treating stage 3 breast cancer
In stage 3 breast cancer, the tumor is large (more than 5 cm or about 2 inches across) or growing into nearby tissues (the skin over the breast or the muscle underneath), or the cancer has spread to many nearby lymph nodes.
If you have inflammatory breast cancer: Stage 3 cancers also include some inflammatory breast cancers that have not spread beyond nearby lymph nodes. Treatment of these cancers can be slightly different from the treatment of other stage 3 breast cancers. You can find more details in our section about treatment for inflammatory breast cancer.
There are two main approaches to treating stage 3 breast cancer:
Starting with neoadjuvant therapy
Most often, these cancers are treated with neoadjuvant (before surgery) chemotherapy. For HER2-positive tumors, the targeted drug trastuzumab is given as well, often along with pertuzumab (Perjeta). This may shrink the tumor enough for a woman to have breast-conserving surgery (BCS). If the tumor doesn’t shrink enough, a mastectomy is done. Nearby lymph nodes will also need to be checked. A sentinel lymph node biopsy is often not an option for stage 3 cancers, so an axillary lymph node dissection is usually done.
Often, radiation therapy is needed after surgery. If breast reconstruction is planned, it is usually delayed until after radiation therapy is done. For some, additional chemo is given after surgery as well.
After surgery, some women with HER2-positive cancers will be treated with trastuzumab (with or without pertuzumab) for up to a year. Many women with HER2-positive cancers will be treated first with trastuzumab (with or without pertuzumab) followed by surgery and then more trastuzumab (with or without pertuzumab) for up to a year. If after neoadjuvant therapy, any residual cancer is found at the time of surgery, ado-trastuzumab emtansine may be used instead of trastuzumab. It is given every 3 weeks for 14 doses. For women with hormone receptor-positive cancer that is in the lymph nodes, who have completed a year of trastuzumab, the doctor might also recommend additional treatment with an oral targeted drug called neratinib for a year.
Women with hormone receptor-positive (ER-positive or PR-positive) breast cancers will also get adjuvant hormone therapy which can typically be taken at the same time as trastuzumab.
For women with hormone receptor-positive, HER2-negative breast cancer that is in the lymph nodes, and has a high chance of coming back, abemaciclib can be given after surgery along with tamoxifen or an AI. It is a pill typically given twice a day for 2 years.
For women who have a BRCA mutation and hormone receptor-positive, HER2-negative breast cancer and still have cancer in the tissue removed at surgery after neoadjuvant chemo, the targeted drug olaparib might be given for one year to help lower the chance of the cancer recurring. When given this way, it can help some women live longer.
Neoadjuvant treatment is a preferable option for women with stage 3 triple-negative breast cancer or HER2-positive breast cancer because the treatment given after surgery is chosen depending on how much cancer is still in the breast and/or lymph nodes at the time of surgery. Some women with stage 3 cancer who get neoadjuvant treatment might live longer if the cancer goes away completely with that treatment.
Women with triple-negative breast cancer might get the immunotherapy drug, pembrolizumab, before surgery and then again after surgery.
Online tools to help make decisions
To help decide if adjuvant therapy is right for you, you might want to visit the Mayo Clinic website at www.mayoclinic.com and type “adjuvant therapy for breast cancer” into the search box. You will find a page that will help you to understand the possible benefits and limits of adjuvant therapy.
Other online guides, such as www.adjuvantonline.com, are designed to be used by health care professionals. This website provides information about your risk of the cancer returning within the next 10 years and what benefits you might expect from hormone therapy and/or chemotherapy.
Starting with surgery
Surgery first is an option for some women with stage 3 cancers. Because these tumors are fairly large and/or have grown into nearby tissues, this usually means getting a mastectomy. For women with fairly large breasts, breast-conserving surgery (BCS) may be an option if the cancer hasn’t grown into nearby tissues. Sentinel lymph node biopsy may be an option for some patients, but most will need an axillary lymph node dissection. Surgery is usually followed by adjuvant chemotherapy, and/or hormone therapy, and/or targeted drug therapy, and/or HER2-positive treatment (trastuzumab, pertuzumab, or neratinib) depending on the traits of the cancer cells. Radiation is recommended after surgery.
Treatment of Inflammatory Breast Cancer
Inflammatory breast cancer is an uncommon type of invasive breast cancer that typically makes the skin on the breast look red and feel warm. It also may give the breast skin a thick, pitted appearance that looks a lot like an orange peel. These changes are caused by cancer cells blocking lymph vessels in the skin.
Because inflammatory breast cancer has reached these lymph vessels and has caused changes in the skin, it is considered to be at least a stage 3 breast cancer when it is diagnosed. Inflammatory breast cancer that has spread to other parts of the body is considered stage 4. These cancers typically grow quickly and can be challenging to treat.
Regardless of the stage of the cancer, participation in a clinical trial of new treatments for inflammatory breast cancer is also a good option because inflammatory breast cancer is rare, has a poor prognosis (outcome), and these studies often allow access to drugs not available for standard treatment.
Treating stage 3 inflammatory breast cancer
Inflammatory breast cancer that has not spread outside the breast or nearby lymph nodes is stage 3. Treatment usually starts with chemotherapy (chemo) to try to shrink the tumor. If the cancer is HER2-positive, targeted therapy is given along with the chemo. This is typically followed by surgery (mastectomy and lymph node dissection) to remove the cancer. Radiation therapy often follows surgery. Sometimes, more chemo may be given after surgery but before radiation. If the cancer is hormone receptor-positive , hormone therapy is given as well (usually after all chemo has been given). Combining these treatments has improved survival significantly over the years.
Chemotherapy (possibly along with targeted therapy)
Chemo drugs enter the bloodstream and circulate throughout the body to reach and destroy cancer cells wherever they are, so chemo is considered a type of systemic therapy. It treats both the main tumor as well as any cancer cells that have broken off and spread to lymph nodes or other parts of the body.
Using chemo before surgery is called neoadjuvant or preoperative treatment. Most women with inflammatory breast cancer will receive two types of chemo drugs (although not necessarily at the same time):
- An anthracycline, such as doxorubicin (Adriamycin) or epirubicin (Ellence)
- A taxane, such as paclitaxel (Taxol) or docetaxel (Taxotere)
Other chemo drugs may be used as well.
If the cancer is HER2-positive (the cancer cells make too much of a protein called HER2), the targeted therapy drug trastuzumab (Herceptin) is usually given, sometimes along with another targeted drug, pertuzumab (Perjeta). These drugs can lead to heart problems when given with an anthracycline, so one option is to give the anthracycline first (without trastuzumab or pertuzumab), followed by treatment with a taxane and trastuzumab (with or without pertuzumab).
For inflammatory breast cancer that is triple-negative, the immunotherapy drug pembrolizumab can be given with chemo before surgery (neoadjuvant treatment) and then continued by itself after surgery (adjuvant treatment).
For women who have:
- a BRCA mutation AND
- triple-negative or HER2-negative inflammatory breast cancer AND
- residual cancer in the tissue removed by surgery after neoadjuvant chemo
The targeted drug olaparib (Lynparza) might be given to lower the risk of the cancer recurring. It is typically given for one year. When given this way, olaparib can help some women live longer.
Surgery and further treatments
If the cancer improves with chemo, surgery is typically the next step. The standard operation is a modified radical mastectomy, where the entire breast and the lymph nodes under the arm are removed. Because inflammatory breast cancer affects so much of the breast and skin, breast-conserving surgery (partial mastectomy or lumpectomy) and skin-sparing mastectomy are not options. It isn’t clear that sentinel lymph node biopsy (where only one or a few nodes are removed) is reliable in inflammatory breast cancer, so it is also not an option.
If the cancer does not respond to chemo (and the breast is still very swollen and red), surgery cannot be done. Either other chemo drugs will be tried, or the breast may be treated with radiation. Then if the cancer responds (the breast shrinks and is no longer red), surgery may be an option.
If breast radiation isn’t given before surgery, it is given after surgery, even if no cancer is thought to remain. This is called adjuvant radiation. It lowers the chance that the cancer will come back. Radiation is usually given 5 days a week for 6 weeks, but in some cases a more intense treatment (twice a day) can be used instead. Depending on how much tumor was found in the breast after surgery, radiation might be delayed until further chemo and/or targeted therapy (such as trastuzumab) is given. If breast reconstruction is to be done, it is usually delayed until after the radiation therapy that most often follows surgery.
Treatment after surgery often includes additional (adjuvant) systemic treatment. This can include chemo, targeted therapy, hormone therapy (tamoxifen or an aromatase inhibitor) if the cancer cells have hormone receptors, the oral chemo drug capecitabine (Xeloda) if the cancer is triple-negative, the PARP inhibitor olaparib (Lynparza) if the woman has a BRCA mutation,and/or trastuzumab, pertuzumab or ado-trastuzumab emtansine if the cancer is HER2-positive.
Treating stage 4 inflammatory breast cancer
Patients with metastatic (stage 4) inflammatory breast cancer are treated with systemic therapy. This may include:
- Chemotherapy
- Hormonal therapy (if the cancer is hormone receptor-positive)
- Targeted therapy with a drug that targets HER2 (if the cancer is HER2-positive)
- Immunotherapy if the cancer makes a protein called PD-L1
- Targeted drug therapy with a PARP inhibitor called olaparib if the woman has a BRCA mutation
One or more of these treatments might be used. Many times, a targeted drug is given along with chemotherapy or with hormone therapy. Surgery and radiation may also be options in certain situations.
Treatment of Stage 4 (Metastatic) Breast Cancer
Stage 4 cancers have spread (metastasized) beyond the breast and nearby lymph nodes to other parts of the body. When breast cancer spreads, it most commonly goes to the bones, liver, and lungs. It may also spread to the brain or other organs.
For women with stage 4 breast cancer, systemic drug therapies are the main treatments. Treatment options for stage 4 breast cancer may include:
- Hormone therapy
- Chemotherapy (chemo)
- Targeted drugs
- Immunotherapy
- Some combination of these
Surgery and/or radiation therapy may be useful in certain situations (see below).
Treatment can often shrink tumors (or slow their growth), improve symptoms, and help some women live longer. These cancers are considered incurable.
Systemic (drug) treatments for stage 4 breast cancer
The types of drugs used for stage 4 breast cancer depend on the hormone receptor status, the HER2 status of the cancer and sometimes gene mutations that might be found.
- Hormone receptor-positive cancers: Women with hormone (estrogen or progesterone) receptor-positive cancers are sometimes treated first with hormone therapy (tamoxifen or an aromatase inhibitor). This may be combined with a targeted drug such as a CDK4/6 inhibitor, everolimus, or a PI3K inhibitor.
- Women who haven’t yet gone through menopause are often treated with tamoxifen or with medicines that keep the ovaries from making hormones along with other drugs.
- Hormone receptor-negative cancers: Chemo is the main treatment for women with hormone (estrogen and progesterone) receptor-negative cancers, because hormone therapy isn’t helpful for these cancers.
- HER2-positive cancers: The first therapy given is usually chemotherapy in combination with trastuzumab (Herceptin) and pertuzumab (Perjeta), both HER2 targeted drugs. If the cancer grows, other options might include:
- an antibody-drug conjugate
- a kinase inhibitor with an anti-HER2 drug or with a chemo drug or both
- other HER2 targeted drugs with chemo
- Hormone therapy might be added to these drug combinations if the cancer is also hormone-receptor positive.
- HER2-negative cancers in women with a BRCA gene mutation: These women are typically treated with a targeted drug called a PARP inhibitor, such as olaparib or talazoparib. Chemotherapy drugs and hormone drugs are also very helpful in treating these cancers.
- HER2-negative breast cancers in women with a PIK3CA gene mutation: About 30% to 40% of metastatic estrogen receptor-positive breast cancers have a PIK3CA gene mutation. Alpelisib is a targeted drug known as a PIK3 inhibitor that can be used along with the hormone drug fulvestrant to treat postmenopausal women with advanced hormone receptor-positive breast cancer. For this drug to work, there must be a PIK3CA mutation found on a biopsy done on the tumor tissue or of the cancer cells in the blood (liquid biopsy).
- Triple-negative breast cancer: An immunotherapy drug along with chemotherapy might be used in people with advanced triple-negative breast cancer whose tumor makes the PD-L1 protein. The PD-L1 protein is found is about 1 in 5 women with triple-negative breast cancer. For women with triple-negative breast cancer and a BRCA mutation, drugs called PARP inhibitors (like olaparib or talazoparib) may be considered. For breast cancers in which the cancer cells show high levels of gene changes called microsatellite instability (MSI) or changes in any of the mismatch repair (MMR) genes (MLH1, MSH2, MSH6, and PMS2), immunotherapy with the drug pembrolizumab might be used. Pembrolizumab might also be an option for triple-negative breast cancer that has other gene or protein changes. For triple-negative breast cancer that does not have any specific gene or protein changes, chemo alone or the antibody-drug conjugate sacituzumab govitecan (Trodelvy) might be an option.
Treatment often continues until the cancer starts growing again or until side effects become unacceptable. If this happens, other drugs might be tried.
Local or regional treatments for stage 4 breast cancer
Although systemic drugs are the main treatment for stage IV breast cancer, local and regional treatments such as surgery, radiation therapy, or regional chemotherapy are sometimes used as well. These can help treat breast cancer in a specific part of the body, but they are very unlikely to get rid of all of the cancer. These treatments are more likely to be used to help prevent or treat symptoms or complications from the cancer.
Radiation therapy and/or surgery may also be used in certain situations, such as:
- When the breast tumor is causing an open wound in the breast (or chest)
- To treat a small number of metastases in a certain area, such as the brain
- To help prevent bone fractures
- When an area of cancer spread is pressing on the spinal cord
- To treat a blood vessel blockage in the liver
- To provide relief of pain or other symptoms
In some cases, regional chemo (where drugs are delivered directly into a certain area, such as into the fluid around the brain and spinal cord, called intrathecal chemo) may be useful as well.
If your doctor recommends such local or regional treatments, it is important that you understand the goal—whether it is to try to cure the cancer or to prevent or treat symptoms.
Relieving symptoms of advanced breast cancer
Treatment to relieve symptoms depends on where the cancer has spread. For example, pain from bone metastases may be treated with radiation therapy, drugs called bisphosphonates such as pamidronate (Aredia) or zoledronic acid (Zometa), or the drug denosumab (Xgeva).
Advanced cancer that progresses during treatment
Treatment for advanced breast cancer can often shrink the cancer or slow its growth (sometimes for many years), but after a time, it tends to stop working. Further treatment options at this point depend on several factors, including previous treatments, where the cancer is located, a woman’s menopause status, general health, desire to continue getting treatment, and whether the hormone receptor status and HER2 status have changed on the cancer cells.
Progression while on hormone therapy
For hormone (estrogen or progesterone) receptor-positive cancers that were being treated with hormone therapy, switching to another type of hormone therapy sometimes helps. For example, if either letrozole (Femara) or anastrozole (Arimidex) were given, using exemestane, possibly with everolimus (Afinitor), may be an option. Another option might be using fulvestrant (Faslodex) or a different aromatase inhibitor, along with a CDK inhibitor. If the cancer has a PIK3CA mutation and has grown while being treated with an aromatase inhibitor, fulvestrant with alpelisib might be considered. If the cancer is no longer responding to any hormone drugs, chemotherapy immunotherapy, or PARP inhibitors might be options depending on specific features of the cancer or any gene changes that might be present.
Progression while on chemotherapy
If the cancer is no longer responding to one chemo regimen, trying another may be helpful. Many different drugs and combinations can be used to treat breast cancer. However, each time a cancer progresses during treatment, it becomes less likely that further treatment will have an effect. Sometimes, other options include adding an immunotherapy drug to the chemo or using a PARP inhibitor alone depending on specific features of the cancer or any gene changes that might be present.
Progression while getting HER2 drugs
HER2-positive cancers that no longer respond to trastuzumab (Herceptin) might respond to other drugs that target the HER2 protein. Options for women with HER2-positive cancers might include:
- Pertuzumab (Perjeta) with chemo and trastuzumab
- Ado-trastuzumab emtansine (Kadcyla)
- Fam-trastuzumab deruxtecan (Enhertu)
- Margetuximab (Margenza) with chemo
- Lapatinib (Tykerb) and the oral chemo drug capecitabine
- Lapatinib and an aromatase inhibitor (for hormone receptor-positive cancers)
- Neratinib (Nerlynx) and the chemo drug capecitabine (this combination can be helpful for cancers that have spread to the brain)
- Tucatinib (Tukysa), trastuzumab, and the chemo drug capecitabine (this combination can be helpful for cancers that have spread to the brain)
Because current treatments are very unlikely to cure metastatic breast cancer, if you are in otherwise good health, you may want to think about taking part in a clinical trial testing a newer treatment.
Treatment of Recurrent Breast Cancer
For some women, breast cancer may come back after treatment – sometimes years later. This is called a recurrence. Recurrence can be local (in the same breast or in the surgery scar), regional (in nearby lymph nodes), or in a distant area. Cancer that is found in the opposite breast without any cancer elsewhere in the body is not a recurrence—it is a new cancer that requires its own treatment.
Treating local recurrence
For women whose breast cancer has recurred locally, treatment depends on their initial treatment.
- If you had breast-conserving surgery (lumpectomy), a local recurrence in the breast is usually treated with mastectomy.
- If the initial treatment was mastectomy, recurrence near the mastectomy site is treated by removing the tumor whenever possible. This is often followed by radiation therapy if not given before.
In either case, hormone therapy, targeted therapy (like trastuzumab), immunotherapy, chemotherapy, or some combination of these may be used after surgery and/or radiation therapy. These drugs might also be used if surgery or radiation are not options.
Treating regional recurrence
When breast cancer comes back in nearby lymph nodes (such as those under the arm or around the collar bone), it is treated by removing those lymph nodes, if possible. This may be followed by radiation aimed at the area if it was not given before. Systemic treatment (such as chemo, targeted therapy, or hormone therapy) may be considered after surgery as well.
Treating distant recurrence
In general, women whose breast cancer comes back in other parts of the body, such as the bones, lungs, or brain, are treated the same way as those found to have stage 4 breast cancer in these organs when they were first diagnosed. The only difference is that treatment may or may not include treatments or drugs a woman has already had.
Recurrent breast cancer can sometimes be hard to treat. If you are in otherwise good health, you might want to think about taking part in a clinical trial testing a newer treatment.
Treatment of breast cancer in men
To determine your male breast cancer treatment options, your doctor considers your cancer’s stage, your overall health and your preferences. Male breast cancer treatment often involves surgery and may also include other treatments.
Surgery
The goal of surgery is to remove the tumor and surrounding breast tissue. The procedures include:
- Removal of breast tissue and surrounding lymph nodes (modified radical mastectomy). The surgeon removes all of your breast tissue, including the nipple and areola, and some underarm lymph nodes.
- Removal of one lymph node for testing (sentinel lymph node biopsy). The doctor identifies the lymph node most likely to be the first place your cancer cells would spread. That lymph node is removed and analyzed. If no cancer cells are found, there is a good chance that your breast cancer hasn’t spread beyond your breast tissue.
Radiation therapy
Radiation therapy uses high-energy beams to kill cancer cells. In male breast cancer, radiation therapy may be used after surgery to eliminate any remaining cancer cells in the breast, chest muscles or armpit.
During radiation therapy, radiation comes from a large machine that moves around your body, directing the energy beams to precise points on your chest.
Chemotherapy
Chemotherapy uses medications to kill cancer cells. These medications may be administered through a vein in your arm (intravenously), in pill form or by both methods.
Your doctor might recommend chemotherapy after surgery to kill any cancer cells that might have spread outside your breast. Chemotherapy may also be an option for men with advanced breast cancer.
Hormone therapy
Most men with male breast cancer have tumors that rely on hormones to grow (hormone-sensitive). If your cancer is hormone-sensitive, your doctor may recommend hormone therapy.
Hormone therapy for male breast cancer often involves the medication tamoxifen, which is also used for women. Other hormone therapy medications used in women with breast cancer haven’t been shown to be effective for men.
Coping and support
A breast cancer diagnosis can be overwhelming. And just when you’re trying to cope with the shock and the fears about your future, you’re asked to make important decisions about your treatment.
Every person finds his or her own way of coping with a cancer diagnosis. Until you find what works for you, it might help to:
- Learn enough about your breast cancer to make decisions about your care. If you’d like to know more about your breast cancer, ask your doctor for the details of your cancer — the type, stage and hormone receptor status. Ask for good sources of up-to-date information on your treatment options. Knowing more about your cancer and your options may help you feel more confident when making treatment decisions. Still, some women may not want to know the details of their cancer. If this is how you feel, let your doctor know that, too.
- Talk with other breast cancer survivors. You may find it helpful and encouraging to talk to others in your same situation. Contact the American Cancer Society to find out about support groups in your area and online.
- Find someone to talk about your feelings with. Find a friend or family member who is a good listener, or talk with a clergy member or counselor. Ask your doctor for a referral to a counselor or other professional who works with cancer survivors.
- Keep your friends and family close. Your friends and family can provide a crucial support network for you during your cancer treatment.
As you begin telling people about your breast cancer diagnosis, you’ll likely get many offers for help. Think ahead about things you may want assistance with, whether it’s having someone to talk to if you’re feeling low or getting help preparing meals.
Maintain intimacy with your partner. In Western cultures, women’s breasts are associated with attractiveness, femininity and sexuality. Because of these attitudes, breast cancer may affect your self-image and erode your confidence in intimate relationships. Talk to your partner about your insecurities and your feelings.
Supportive (palliative) care
Palliative care is specialized medical care that focuses on providing relief from pain and other symptoms of a serious illness. Palliative care specialists work with you, your family and your other doctors to provide an extra layer of support that complements your ongoing care. Palliative care can be used while undergoing other aggressive treatments, such as surgery, chemotherapy or radiation therapy.
When palliative care is used along with all of the other appropriate treatments, people with cancer may feel better and live longer.
Palliative care is provided by a team of doctors, nurses and other specially trained professionals. Palliative care teams aim to improve the quality of life for people with cancer and their families. This form of care is offered alongside curative or other treatments you may be receiving.
References- What Is Breast Cancer? https://www.cancer.org/cancer/breast-cancer/about/what-is-breast-cancer.html
- Cancer Stat Facts: Female Breast Cancer. https://seer.cancer.gov/statfacts/html/breast.html
- Breast cancer. https://www.mayoclinic.org/diseases-conditions/breast-cancer/symptoms-causes/syc-20352470
- Preventive Surgery to Reduce Breast Cancer Risk. https://www.cancer.org/cancer/breast-cancer/risk-and-prevention/preventive-surgery-to-reduce-breast-cancer-risk.html
- Ductal Carcinoma In Situ (DCIS). https://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/types-of-breast-cancer/dcis.html
- Ductal Carcinoma In Situ (DCIS). https://www.cancer.org/cancer/breast-cancer/about/types-of-breast-cancer/dcis.html
- Lobular Carcinoma in Situ (LCIS). https://www.cancer.org/cancer/breast-cancer/non-cancerous-breast-conditions/lobular-carcinoma-in-situ.html
- Invasive Breast Cancer (IDC/ILC). https://www.cancer.org/cancer/breast-cancer/about/types-of-breast-cancer/invasive-breast-cancer.html
- Triple-negative Breast Cancer. https://www.cancer.org/cancer/breast-cancer/about/types-of-breast-cancer/triple-negative.html
- Treatment of Triple-negative Breast Cancer. https://www.cancer.org/cancer/breast-cancer/treatment/treatment-of-triple-negative.html
- Phyllodes Tumors of the Breast. https://www.cancer.org/cancer/breast-cancer/non-cancerous-breast-conditions/phyllodes-tumors-of-the-breast.html
- Breast. https://cancerstatisticscenter.cancer.org/#!/cancer-site/Breast
- Key Statistics for Breast Cancer in Men. https://www.cancer.org/cancer/breast-cancer-in-men/about/key-statistics.html
- What Is Breast Cancer in Men? https://www.cancer.org/cancer/breast-cancer-in-men/about/what-is-breast-cancer-in-men.html
- https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2017-2018.pdf
- American Cancer Society Recommendations for the Early Detection of Breast Cancer. https://www.cancer.org/cancer/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html
- Chemotherapy for Breast Cancer. https://www.cancer.org/cancer/breast-cancer/treatment/chemotherapy-for-breast-cancer.html





{kind=link}