
What is brittle bone disease
Brittle bone disease is also known as osteogenesis imperfecta, is one of the most common inherited bone disorders, that causes weak bones that break easily. Brittle bone disease (osteogenesis imperfecta) typically involves the bones, teeth, ligaments, eyes and skin, and is characterized by fragile bones that break easily. There are at least eight recognized forms of osteogenesis imperfecta, designated type 1 through type 8. The types can be distinguished by their signs and symptoms, although their characteristic features overlap. Type 1 is the mildest form of osteogenesis imperfecta and type 2 is the most severe; other types of this condition have signs and symptoms that fall somewhere between these two extremes. Increasingly, genetic factors are used to define the different forms of osteogenesis imperfecta.
All four major types (types 1 to 4) of brittle bone disease (osteogenesis imperfecta) are caused by defects in the amount or structure of type 1 collagen, an important part of the bone matrix. The collagen problem usually results from a dominant genetic defect.
When people have brittle bone disease (osteogenesis imperfecta), all of their bones are abnormally weak. The severity of the abnormality varies enormously — from Type 2 osteogenesis imperfecta, which is usually lethal in infancy (or even before birth) to Type 1 osteogenesis imperfecta, which may be so mild that the diagnosis is not made, even in adulthood.
The milder forms of brittle bone disease (osteogenesis imperfecta), including type 1, are characterized by bone fractures during childhood and adolescence that often result from minor trauma. Fractures occur less frequently in adulthood. People with mild forms of the condition typically have a blue or grey tint to the part of the eye that is usually white (the sclera), and may develop hearing loss in adulthood. Affected individuals are usually of normal or near normal height.
Other types of brittle bone disease (osteogenesis imperfecta) are more severe, causing frequent bone fractures that may begin before birth and result from little or no trauma. Additional features of these conditions can include blue sclerae, short stature, hearing loss, respiratory problems, and a disorder of tooth development called dentinogenesis imperfecta. The most severe forms of osteogenesis imperfecta, particularly type 2, can include an abnormally small, fragile rib cage and underdeveloped lungs. Infants with these abnormalities have life-threatening problems with breathing and often die shortly after birth.
Brittle bone disease (osteogenesis imperfecta) affects an estimated 6 to 7 per 100,000 people worldwide. Approximately 25,000 to 50,000 people in the U.S. have brittle bone disease (osteogenesis imperfecta). Brittle bone disease (osteogenesis imperfecta) occurs equally among males and females and in all racial groups. Types 1 and 4 are the most common forms of osteogenesis imperfecta, affecting 4 to 5 per 100,000 people.
In the US: Incidence of brittle bone disease (osteogenesis imperfecta) by type is as follows:
- Type 1 – One per 30,000 live births
- Type 2 – One per 60,000 live births
- Type 3 – One per 70,000 live births
- Type 4 – Rare
Age of onset of symptoms (i.e. fractures) varies depending on the type, as follows:
- Type 1 – Infancy
- Type 2 – In utero
- Type 3 – Half the cases in utero, and other half in the neonatal period
- Type 4 – Usually in infancy
Brittle bone disease facts
- Brittle bone disease is a genetic disorder that is present throughout a person’s lifetime. Many people with brittle bone disease have fewer fractures after puberty when growth stops, but the genetic difference remains. Fractures and other complications occur throughout the lifespan and can increase again after menopause in women and after age 60 in men. Non-skeletal problems can be serious.
- The majority of people with brittle bone disease have a dominant mutation. When one parent has a dominantly inherited type of brittle bone disease, there is a 50 percent chance with each pregnancy that the child will have brittle bone disease. There is a 50 percent chance that the child will not have brittle bone disease.
- Although present from conception, brittle bone disease can be diagnosed at many different ages from birth into adulthood. The most severe forms are usually diagnosed at birth or shortly after. Other forms may not be diagnosed until the child has a series of broken bones or an adult has unusually low bone density. Brittle bone disease type 1, the most common and mildest form of brittle bone disease, is rarely diagnosed at birth.
- The appearance of people with brittle bone disease varies considerably. Although many people with brittle bone disease are short-statured, people with milder forms may be of near-average height and have no obvious symptoms of brittle bone disease. About 50 percent of people with brittle bone disease have tinted sclera that can range in color from nearly white to dark blue or gray. People with brittle bone disease also have variable mobility, ranging from independent walking to full-time wheelchair use.
- Brittle bone disease does not affect fertility. Many men and women who have brittle bone disease have children. Some women who have brittle bone disease may experience pregnancy complications due to skeletal problems. It is important that all young people with brittle bone disease receive information about their condition and about reproductive health.
- Children with brittle bone disease can have all types of fractures, including but not limited to spiral, rib, skull, incomplete, and displaced fractures.
- Distinguishing brittle bone disease from child abuse requires a thorough assessment by a medical professional who is familiar with the full range of brittle bone disease characteristics.
- Though fragile bones are the hallmark of brittle bone disease, many parts of the body are affected by brittle bone disease. Skeletal features include fragile bones, bone deformity, loose joints, and short stature. Non-skeletal symptoms affect the heart, skin, blood vessels, muscles, tendons, internal organs, and eyes. In addition, breathing problems, hearing loss, excessive perspiration and brittle teeth are common.
Brittle bone disease types
Brittle bone disease type 1
Brittle bone disease type 1 is the mildest and most common form of the disorder. It accounts for 50 percent of the total brittle bone disease population. Brittle bone disease type 1 is characterized with mild bone fragility, relatively few fractures, and minimal limb deformities. The child might not fracture until he or she is learning to walk.
Shoulders and elbow dislocations may occur more frequently than in healthy children.
- Some children have few obvious signs of brittle bone disease or fractures. Others experience multiple fractures of the long bones, compression fractures of the vertebrae, and chronic pain.
- The intervals between fractures may vary considerably.
- After growth is completed, the incidence of fractures decreases considerably.
- Blue sclerae are often present.
- Typically, a child’s stature may be average or slightly shorter-than-average as compared with unaffected family members, but is still within the normal range for the age.
- There is a high incidence of hearing loss. Onset occurs primarily in young adulthood, but it may occur in early childhood.
- Dentinogenesis imperfecta is often absent.
- Brittle bone disease type 1 is dominantly inherited. It can be inherited from an affected parent, or, in previously unaffected families, it results from a spontaneous mutation. Spontaneous mutations are common.
- Biochemical tests on cultured skin fibroblasts show a lower-than-normal amount of type 1 collagen. Collagen structure is normal.
- People with brittle bone disease type 1 experience the psychological burden of appearing normal and healthy to the casual observer despite needing to accommodate their bone fragility.
- The absence of obvious symptoms in some children may contribute to problems at school or with peers.
- Significant care issues that arise with brittle bone disease type 1 include gross motor developmental delays, joint and ligament weakness and instability, muscle weakness, the need to prevent fracture cycles, and the necessity of spine protection.
- Family members should carry documentation of the brittle bone disease diagnosis to avoid accusations of child abuse at emergency rooms.
- Treatment with bisphosphonates is not routinely recommended.
- The treatment plan should maximize mobility and function, increase peak bone mass, and develop muscle strength. Physical therapy, early intervention programs, and as much exercise and physical activity as possible will improve outcomes.
Brittle bone disease type 2
Brittle bone disease type 2 is the most severe form. At birth, infants with brittle bone disease type 2 have very short limbs, small chests, and soft skulls. Their legs are often in a frog-leg position. The radiologic features are characteristic and include absent or limited calvarial mineralization; flat vertebral bodies; very short, telescoped, broad femurs; beaded and often broad short ribs; and evidence of malformation of the long bones.
- Intrauterine fractures will be evident in the skull, long bones, or vertebrae.
- The sclerae are usually very dark blue or gray.
- The lungs are underdeveloped.
- Infants with brittle bone disease type 2 have low birth weights.
- Respiratory and swallowing problems are common.
- Macrocephaly may be present. Microcephaly is rarely present.
- Infants with brittle bone disease type 2 usually die within weeks of delivery. A few may survive longer. Cause of death is usually respiratory and cardiac complications.
- Brittle bone disease type 2 results from a new dominant mutation in a type 1 collagen gene or parental mosaicism. Similar extremely severe types of brittle bone disease, types 7 and 8, can be caused by recessive mutations to other genes.
- Genetic counseling is recommended for parents of a child with brittle bone disease type 2 before any future pregnancies.
- Significant care issues that arise with brittle bone disease type 2 include obtaining an accurate diagnosis, getting genetic counseling, the family’s need for emotional support, and management of respiratory and cardiac impairments. Infants with brittle bone disease type 2 who can breathe without a respirator and those with severe brittle bone disease type 3 may be candidates for treatment with bisphosphonates.
Brittle bone disease type 3
Brittle bone disease type 3 is the most severe type among children who survive the neonatal period. The degree of bone fragility and the fracture rate vary widely.
Brittle bone disease type 3 is characterized by structurally defective type 1 collagen. This poor quality type 1 collagen is present in reduced amounts in the bone matrix.
- At birth, infants generally have mildly shortened and bowed limbs, small chests, and a soft calvarium.
- Respiratory and swallowing problems are common in newborns.
- There may be multiple long-bone fractures at birth, including many rib fractures.
- Frequent fractures of the long bones, the tension of muscle on soft bone, and the disruption of the growth plates lead to bowing and progressive malformation. Children have a markedly short stature, and adults are usually shorter than 3 feet, 6 inches, or 102 centimeters.
- Spine curvatures, compression fractures of the vertebrae, scoliosis, and chest deformities occur frequently.
- The altered structure of the growth plates gives a popcorn-like appearance to the metaphyses and epiphyses.
- The head is often large relative to body size.
- A triangular facial shape, due to over development of the head and underdevelopment of the face bones, is characteristic.
- The sclerae may be white or tinted blue, purple, or gray.
- Dentinogenesis imperfecta is common but not universal.
- The majority of brittle bone disease type 3 cases result from dominant mutations in type 1 collagen genes. Often these mutations are spontaneous. Similar extremely severe types of brittle bone disease, types 7 and 8, are caused by recessive mutations to other genes.
- Genetic counseling is recommended for asymptomatic parents of a child with brittle bone disease type 3 before any future pregnancies.
- Significant care issues that arise with brittle bone disease type 3 include the need to prevent fracture cycles; the appropriate timing of rodding surgery; scoliosis monitoring; respiratory function monitoring; the need to develop strategies to cope with short stature and fatigue; the family’s need for emotional support, especially during infancy; and the off-label use of bisphosphonates.
- It is also important to address difficulties with social integration, participation in leisure activities, and maintaining stamina.
- The treatment plan should maximize mobility and function, increase peak bone mass and muscle strength, and employ as much exercise and physical activity as possible.
Brittle bone disease type 4
People with brittle bone disease type 4 are moderately affected. Brittle bone disease type 4 can range in severity from relatively few fractures, as in brittle bone disease type 1, to a more severe form resembling brittle bone disease type 3. The diagnosis can be made at birth but often occurs later.
- The child might not fracture until he or she is walking.
- People with brittle bone disease type 4 have moderate-to-severe growth retardation, which is one factor that distinguishes them clinically from people with type 1.
- Bowing of the long bones is common, but to a lesser extent than in type 3.
- The sclerae are often light blue in infancy, but the color intensity varies. The sclerae may lighten to white later in childhood or early adulthood.
- The child’s height may be less-than-average for his or her age.
- It is common for the humerus and femur to be short
- Long bone fractures, vertebral compression, scoliosis, and ligament laxity may also be present.
- Dentinogenesis imperfecta may be present or absent.
- Brittle bone disease type 4 has an autosomal dominant pattern of inheritance. Many cases are the result of a new mutation.
- Brittle bone disease type 4 is characterized by structurally defective type 1 collagen. This poor quality type 1 collagen is present in reduced amounts in the bone matrix.
- Significant care issues that arise with brittle bone disease type 4 include the need to prevent fracture cycles; the appropriate timing of rodding surgery; scoliosis monitoring; the need to develop strategies for coping with short stature and fatigue; the family’s need for emotional support, especially during infancy; and the off-label use of bisphosphonates.
- Family members should carry documentation of the brittle bone disease diagnosis to avoid accusations of child abuse at emergency rooms.
- It is also important to address difficulties with social integration, participation in leisure activities, and maintaining stamina.
- The treatment plan should maximize mobility and function, increase peak bone mass and muscle strength, and employ as much exercise and physical activity as possible.
Microscopic studies of brittle bone disease bone identified a subset of people who are clinically within the brittle bone disease type 4 group but have distinctive patterns to their bone. Review of the clinical histories of these people uncovered other common features. As a result of this research, two types — Type 5 and Type 6 were added to the Sillence Classification. Regarding these types, it is important to note the following:
- They do not involve deficits of type 1 collagen.
- Treatment issues are similar to brittle bone disease type 4.
- Diagnosis requires specific radiographic and bone studies.
Brittle bone disease type 5
Brittle bone disease type 5 is moderate in severity. It is similar to brittle bone disease type 4 in terms of frequency of fractures and the degree of skeletal deformity. The most conspicuous feature of this type is large, hypertrophic calluses in the largest bones at fracture or surgical procedure sites. Hypertrophic calluses can also arise spontaneously.
Calcification of the interosseous membrane between the radius and ulna restricts forearm rotation and may cause dislocation of the radial head. Women with brittle bone disease type 5 anticipating pregnancy should be screened for hypertrophic callus in the iliac bone. Brittle bone disease type 5 is dominantly inherited and represents 5 percent of moderate-to-severe brittle bone disease cases.
Brittle bone disease type 6
Brittle bone disease type 6 is extremely rare. Brittle bone disease type 6 is moderate in severity and similar in appearance and symptoms to brittle bone disease type 4. Brittle bone disease type 6 is distinguished by a characteristic mineralization defect seen in biopsied bone. The mode of inheritance is probably recessive, but it has not yet been identified.
Recessively Inherited Types of brittle bone disease (Types 7 and 8):
Two recessive types of brittle bone disease, types 7 and 8, were identified in 2006. Unlike the dominantly inherited types, the recessive types of brittle bone disease do not involve mutations in the type 1 collagen genes.
These recessive types of brittle bone disease result from mutations in two genes that affect collagen:
- the cartilage-associated protein gene (CRTAP)
- the prolyl 3-hydroxylase 1 gene (LEPRE1)
Recessively inherited brittle bone disease has been discovered in people with lethal, severe and moderate brittle bone disease. There is no evidence of a recessive form of mild brittle bone disease. Recessive inheritance probably accounts for fewer than 10 percent of brittle bone disease cases.
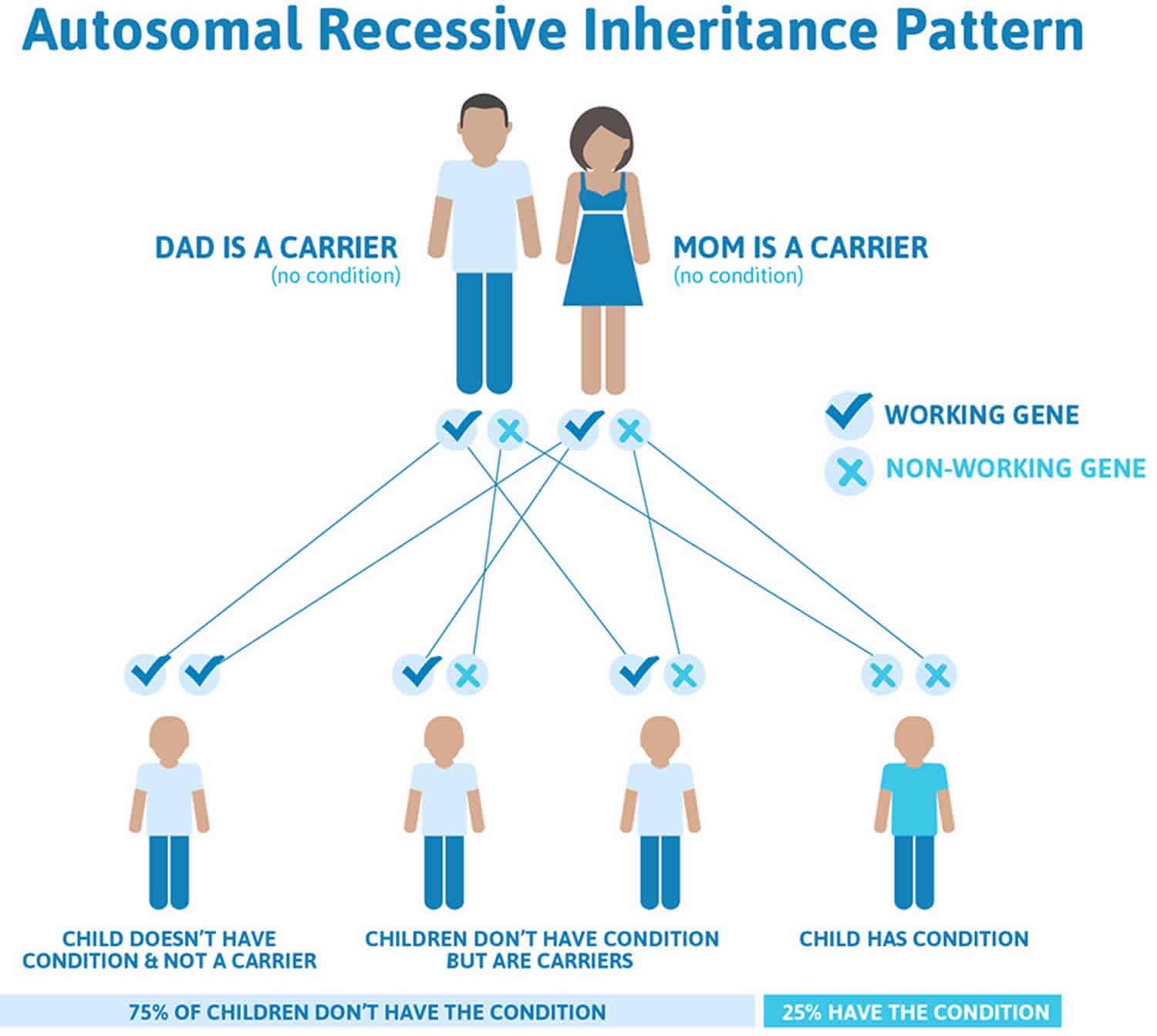
Parents of a child who has a recessive type of brittle bone disease have a 25 percent chance per pregnancy of having another child with brittle bone disease.
Unaffected siblings of a person with a recessive type have a 2 in 3 chance of being a carrier of the recessive gene.
Brittle bone disease type 7
Some cases of brittle bone disease type 7 resemble brittle bone disease type 4 in many aspects of appearance and symptoms. Other cases resemble brittle bone disease type 2, except that infants have white sclerae, small heads and round faces. It is common for leg bones, humerus and femur to be short. Short stature is common.
Coxa vara is common. Brittle bone disease type 7 results from recessive inheritance of a mutation in the CRTAP gene. Partial (10%) expression of CRTAP leads to moderate bone dysplasia. Total absence of the cartilage-associated protein has been lethal in all identified cases.
Brittle bone disease type 8
Cases of brittle bone disease type 8 are similar to brittle bone disease types 2 or 3 in appearance and symptoms except for white sclerae. Brittle bone disease type 8 is characterized by severe growth deficiency and extreme under-mineralization of the skeleton. Brittle bone disease type 8 is caused by absence or severe deficiency of prolyl 3-hydroxylase activity due to mutations in the LEPRE1 gene.
What causes brittle bone disease
Mutations in the COL1A1, COL1A2, CRTAP, and P3H1 genes cause brittle bone disease (osteogenesis imperfecta).
Mutations in the COL1A1 and COL1A2 genes are responsible for more than 90 percent of all cases of brittle bone disease (osteogenesis imperfecta). These genes provide instructions for making proteins that are used to assemble type 1 collagen. This type of collagen is the most abundant protein in bone, skin, and other connective tissues that provide structure and strength to the body.
Most of the mutations that cause brittle bone disease type 1 occur in the COL1A1 gene. These genetic changes reduce the amount of type 1 collagen produced in the body, which causes bones to be brittle and to fracture easily. The mutations responsible for most cases of brittle bone disease types 2, 3, and 4 occur in either the COL1A1 or COL1A2 gene. These mutations typically alter the structure of type 1 collagen molecules. A defect in the structure of type 1 collagen weakens connective tissues, particularly bone, resulting in the characteristic features of osteogenesis imperfecta.
Mutations in the CRTAP and P3H1 genes are responsible for rare, often severe cases of osteogenesis imperfecta. Cases caused by CRTAP mutations are usually classified as type 7; when P3H1 mutations underlie the condition, it is classified as type 8. The proteins produced from these genes work together to process collagen into its mature form. Mutations in either gene disrupt the normal folding, assembly, and secretion of collagen molecules. These defects weaken connective tissues, leading to severe bone abnormalities and problems with growth.
In cases of brittle bone disease (osteogenesis imperfecta) without identified mutations in one of the genes described above, the cause of the disorder is unknown. These cases include brittle bone disease (osteogenesis imperfecta) types 5 and 6. Researchers are working to identify additional genes that may be responsible for these conditions.
Inheritance pattern
Most cases of brittle bone disease (osteogenesis imperfecta) have an autosomal dominant pattern of inheritance (see Figure 1 below), which means one copy of the altered gene in each cell is sufficient to cause the condition. Many people with type 1 or type 4 brittle bone disease (osteogenesis imperfecta) inherit a mutation from a parent who has the disorder. Most infants with more severe forms of brittle bone disease (osteogenesis imperfecta) (such as type 2 and type 3) have no history of the condition in their family. In these infants, the condition is caused by new (sporadic) mutations in the COL1A1 or COL1A2 gene.
Less commonly, brittle bone disease (osteogenesis imperfecta) has an autosomal recessive pattern of inheritance (see Figure 2 below). Autosomal recessive inheritance means two copies of the gene in each cell are altered. The parents of a child with an autosomal recessive disorder typically are not affected, but each carry one copy of the altered gene. Some cases of brittle bone disease type 3 are autosomal recessive; these cases usually result from mutations in genes other than COL1A1 and COL1A2. When brittle bone disease is caused by mutations in the CRTAP or P3H1 gene, the condition also has an autosomal recessive pattern of inheritance.
Figure 1. Autosomal dominant inheritance
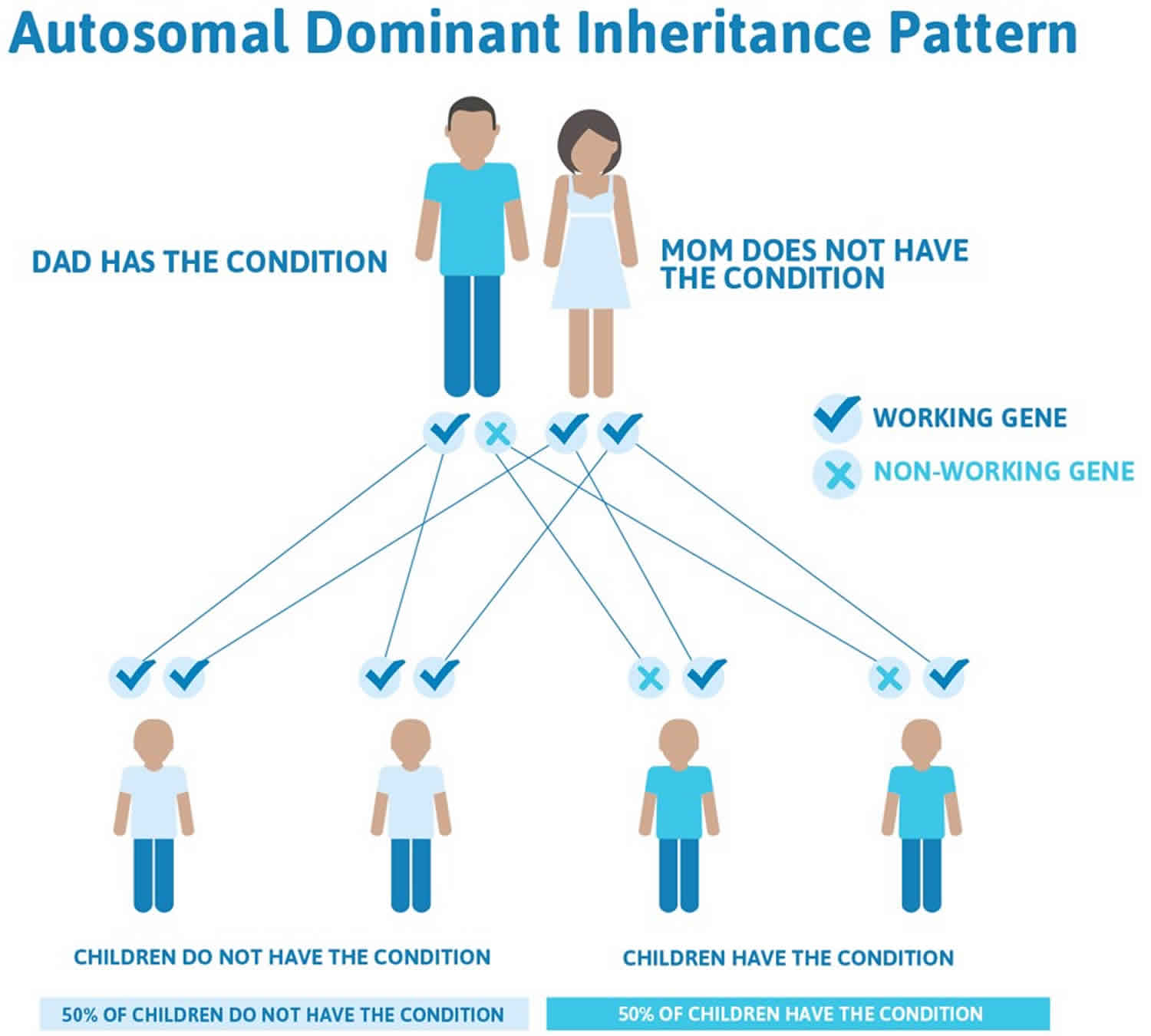
Figure 2. Autosomal recessive inheritance
Brittle bone disease symptoms
In all types of brittle bone disease (osteogenesis imperfecta), the associated symptoms vary greatly from case to case, even within families. Some affected individuals may not experience any bone fractures or only a few; other affected individuals may experience multiple fractures. brittle bone disease may range from a mild disorder with few symptoms to a severe, debilitating disorder. The age of onset of fractures also varies from case to case.
People with brittle bone disease experience frequent broken bones from infancy through puberty. The frequency typically decreases in the young adult years but may increase again later in life. Respiratory problems including asthma are often seen. Other medical characteristics and issues include:
- Bone deformity, and bone pain.
- Short stature.
- Spine curves.
- Low Bone Density.
- Loose joints, ligament laxity and muscle weakness are common.
- Distinctive features of the skull including late closing fontanels, and head circumference greater than average.
- Hearing loss may begin in the early 20s and by middle age is present in more than 50% of people with brittle bone disease.
- Brittle teeth (called dentinogenesis imperfecta) are seen in 50% of people who have brittle bone disease
- Respiratory problems including asthma; may be aggravated by chest wall deformity and/or spine deformity.
- Vision problems including myopia and risk for retinal detachment
- Skin hyperlaxity; easy bruising.
- Cardiac issues.
- Fatigue.
- Basilar Invagination a serious neurological problem is seen in some people with the more severe forms of brittle bone disease.
- Skin, blood vessels and internal organs may be fragile.
Brittle bone disease exhibits wide variation in appearance and severity. Severity is described as mild, moderate, or severe. The most severe forms lead to early death. Clinical features (observable signs) such as fracture frequency, muscle strength or extraskeletal problems vary widely not only between types, but within types, and even within the same family. Some features are age dependent.
Brittle bone disease type 1
Brittle bone disease type 1 is the most common and usually the mildest form of brittle bone disease. In most cases, it is characterized by multiple bone fractures usually occurring during childhood through puberty. Fractures usually begin when an affected child begins to walk; fractures during the newborn (neonatal) period are rare. The frequency of fractures usually declines after puberty. Repeated fractures may result in slight malformation of the bones of the arms and legs (e.g., bowing of the tibia and femur).
A distinguishing feature associated with brittle bone disease type 1 is bluish discoloration of the whites of the eyes (blue sclera). In some cases, individuals with brittle bone disease type I may develop abnormalities affecting the middle and/or inner ears contributing to, or resulting in, hearing impairment (i.e., conductive and/or sensorineural hearing loss). Hearing loss occurs most often in the third decade of life; however, it can occur as early as the second decade or as late as the seventh.
Individuals with brittle bone disease type 1 may have a triangular facial appearance and an abnormally large head (macrocephaly). In approximately 50 percent of cases, individuals with brittle bone disease type 1 will experience growth deficiencies after birth (postnatal), resulting in mild short stature (e.g., affected individuals will be shorter than unaffected family members). Approximately 20 percent of adults with brittle bone disease type 1 develop abnormal sideways or front-to-back curvature of the spine (scoliosis or kyphosis).
Additional symptoms associated with brittle bone disease type 1 include loose (hyperextensible) joints, low muscle tone (hypotonia), and thin skin that bruises easily.
Some researchers believe that a subgroup of brittle bone disease type 1 exists in which affected individuals experience dental abnormalities in addition to the abovementioned features.
Brittle bone disease type 2
Brittle bone disease type 2 is the most severe type of osteogenesis imperfecta. Affected infants often experience life-threatening complications at, or shortly after, birth. Infants with brittle bone disease type 2 have low birth weight, abnormally short arms and legs (limbs), and bluish discoloration of the whites of the eyes (blue sclera). In addition, affected infants may have extremely fragile bones and numerous fractures present at birth. The ribs and long bones of the legs of affected infants are often malformed.
Infants with brittle bone disease type 2 often have underdeveloped lungs and an abnormally small upper chest (thorax) that may result in life-threatening respiratory insufficiency. In some cases, affected infants may experience congestive heart failure.
Infants with brittle bone disease type 2 may also have a small, narrow nose; a small jaw (micrognathia); and an abnormally soft top of the skull (calvaria) with abnormally large soft spots (large fonatanelle). Affected infants may also have abnormally thin, fragile skin and low muscle tone (hypotonia).
Brittle bone disease type 2 has been subdivided into three subgroups (A, B, and C) based upon small differences in bone formation seen only on x-rays (radiographic features).
Brittle bone disease type 3
Brittle bone disease type 3 is characterized by extremely fragile bones, multiple fractures, and malformed bones. Multiple fractures are often present at birth. Fractures and malformation of various bones (most often the ribs and long bones) may become worse (progressive malformation) as affected infants and children age.
Progressive malformation of various bones may result in short stature, sideways and front-to-back curvature of the spine (scoliosis and kyphosis), and malformation of the area where the bone in the back of the skull (occipital bone) and the top of the spine meet (basilar impression). In some cases, affected individuals may develop pulmonary insufficiency and respiratory problems. In severe cases, progressive bone malformation may result in affected individuals requiring wheelchairs.
Infants with brittle bone disease type 3 may have a slight blue discoloration to the whites of the eyes (blue sclera) at birth. In most cases, the bluish tinge fades during the first year of life. Affected infants may have a triangular facial appearance due to an abnormally prominent forehead (frontal bossing) and an abnormally small jaw (micrognathia). In some cases, hearing impairment and brittle, discolored teeth (dentinogenesis imperfecta) may also be present.
Brittle bone disease type 4
Individuals with brittle bone disease type 4 have fragile bones that often fracture easily. Fractures are more common before puberty. Affected individuals experience mild to moderate bone malformation and are usually shorter than average. Affected individuals may develop sideways and front-to-back curvature of the spine (scoliosis and kyphosis).
Individuals with brittle bone disease type 4 may have a triangular facial appearance. In most cases, the whites of the eyes (sclera) are normal or pale blue during infancy. As an affected infant ages, the pale blue discoloration of the sclera fades. Affected individuals may also experience hearing impairment and brittle, discolored teeth (dentinogenesis imperfecta).
Brittle bone disease type 5
Brittle bone disease type 5 is moderate in severity and is similar to type 4 in appearance and symptoms. Identifying features include hypertrophic calluses that may form at fracture or surgical procedure sites and restricted forearm rotation due to calcification of the membrane between the radius and ulna.
Brittle bone disease type 6
Brittle bone disease type 6 is another moderate form and is similar to type 4 in appearance. This is an extremely rare form. It is distinguished by a characteristic mineralization defect that can be seen in biopsied bone.
Brittle bone disease life expectancy
With good medical management and supportive care, the majority of people who have brittle bone disease will lead healthy, productive lives and can expect an average life span.
Permanent deformity of the extremities may occur. Brain damage may result from skull fractures. The disorder can be fatal. The disease is grouped by type:
- Brittle bone disease type 1 (most common & mild form): Mild – Compatible with normal life expectancy. Fractures occur throughout life, but deformity is uncommon. Features include blue sclerae, hypermobile joints, hearing loss and scoliosis.
- Brittle bone disease type 2 (most severe form): Lethal – Most, but not all, die in early childhood. Severe deformity is common, and infants generally do not survive long after birth.
- Brittle bone disease type 3 (severe form): Progressive deforming – Decreased life expectancy. It is characterized by bones that fracture easily and also bend. By the age of 6 years, the child has usually had multiple fractures and developed severe deformities. Children surviving till adulthood usually have short stature and disability.
- Brittle bone disease type 4: Moderately severe – Compatible with normal life expectancy. In terms of severity lies somewhere in between types 1 and 3. Fractures are common before puberty. Sclerae are pale blue and become normal in color in adult life.
Brittle bone disease diagnosis
Broken bones that occur from little or no trauma are often the first indication that an infant or child may have brittle bone disease. Babies with moderate or severe forms of brittle bone disease are often born with broken bones. Children with milder brittle bone disease (Type 1) often sustain their first broken bone as a result of normal activity—during a diaper change, while being lifted or burped, or when they begin standing and walking. Some very mild cases of brittle bone disease type 1 are not diagnosed until the teen or adult years.
Brittle bone disease remains primarily a clinical diagnosis. A physician, usually a geneticist, who is familiar with all types of brittle bone disease, can often diagnose the condition based on the presence of fractures and other clinical features. A family history for the disorder and/or genetic testing can confirm a diagnosis. Additional blood and urine tests are often used to rule out other disorders such as hypophosphatasia or rickets.
The more severe forms of brittle bone disease can be diagnosed prenatally, based upon specialized tests such as ultrasound, amniocentesis, and/or chorionic villus sampling (CVS). Ultrasound can detect bowing, fractures, shortening or other bone abnormalities. But even when ultrasound is done by a highly qualified professional, it may not be possible to pinpoint the type of brittle bone disease or differentiate between type 2 or Type 3. During amniocentesis, a sample of fluid that surrounds the developing fetus is removed and studied. During chorionic villus sampling (CVS), a tissue sample is removed from a portion of the placenta. Chromosomal studies performed on this fluid or tissue sample may reveal the genetic mutation that causes brittle bone disease.
Brittle bone disease treatment
There is no cure for brittle bone disease, but there are ways to manage the symptoms. Despite the obstacles, many people who have brittle bone disease lead productive and fulfilling lives well into their adult years. The goal of all treatment is to minimize fractures, enhance independent function, and promote general health. Medical care for children and adults who have brittle bone disease involves an interdisciplinary team. This can include a primary care doctor, orthopedists, endocrinologists, geneticists, rehabilitation specialists, neurologists and pulmonologists. Treatment may include fracture care, physical therapy, surgical procedures, medications, life style features and mobility aides.
Fracture Care
Casting, splinting and bracing broken bones can help them heal properly. However long periods of immobility can further weaken bones and lead to muscle loss, weakness, and more fractures. Many orthopedists prefer to treat fractures with short term immobilization in lightweight casts, splints, or braces to allow some movement as soon as possible after the fracture.
A procedure in which metal rods are surgically placed in the long bones to prevent fractures (rodding) is often used to treat individuals with brittle bone disease. Plastic braces are replacing plaster casts as protective devices because they permit greater freedom of movement and can be used in water. Inflatable suits can provide added protection, especially to very young children.
Physical Therapy and Safe Exercise
Exercise and physical therapy programs have proven beneficial in strengthening muscles, increasing weight-bearing capacity, and reducing the tendency to fracture. Physical therapy in the water (hydrotherapy) has also been proven helpful since moving around in water lessens the chance of fracture. Individuals with brittle bone disease should consult with their physicians and physical therapists to determine a safe and appropriate exercise program.
Goals for physical therapy include expanding and maintaining function and promoting independence. A typical program includes muscle strengthening and aerobic conditioning. Physical therapy often begins in infancy to counteract the delay in motor skill development many children experience due to brittle bone disease related muscle weakness. Adaptive devices may be needed. Occupational therapy can help with fine motor skills and selection of adaptive equipment for daily living. As a child with brittle bone disease grows older and gains more independence, he or she will benefit from continued physical activity, such as adapted physical education. Adults with brittle bone disease also benefit from safe, regular exercise to maintain bone and muscle mass. Swimming and water therapy are particularly well-suited for people with brittle bone disease of all ages, as they allow independent movement with little fracture risk. Walking is also excellent exercise for those who are able (with or without mobility aids).
Surgery
Surgery may be needed to repair a broken bone, correct bone deformities such as bowing, stabilize the spine or repair tiny bones in the middle ear and improve hearing. Many children with brittle bone disease undergo a surgical procedure known as rodding, in which metal rods are inserted into the long bones to control fractures and improve deformities that interfere with function. Both non-expandable and expandable rods are available.
Medications
Bisphosphonate drugs, which are currently approved by the Food and Drug Administration (FDA) to prevent and treat osteoporosis are used off label to increase bone density in children and adults with moderate and severe brittle bone disease. Other drugs that were developed to treat osteoporosis are also used to prevent age-related bone loss in adults who have brittle bone disease. Teriparatide (a drug based on the parathyroid hormone) is one of them. Treatments under study include growth hormone, and gene therapies. The search continues for a drug treatment that is specific for brittle bone disease.
Healthy Lifestyle
People with brittle bone disease benefit from a healthy lifestyle that includes safe exercise and a nutritious diet. Adequate intake of nutrients, such as Vitamin D and calcium is necessary to maintain bone health, however, extra-large doses of these nutrients are not recommended.
Maintaining a healthy weight is important since extra weight adds stress to the skeleton, heart and lungs and reduces the ability to move easily. In addition, people with brittle bone disease should avoid smoking, second hand smoke, excessive alcohol or caffeine consumption and steroid medications, all of which reduce bone density.
Other treatments that focus on brittle bone disease related symptoms include:
- Hearing aids
- Crowns for brittle teeth
- Supplemental oxygen for people with breathing problems
- Mobility aids such as walkers, crutches, canes and wheelchairs
Are there precautions to take when caring for people with brittle bone disease?
- Never pull or push on a limb, or bend it into an awkward position not even to take an x-ray.
- Use caution when inserting IVs, taking blood pressure, or performing other medical procedures to avoid causing injury.
- Always dose medicines to the size, NOT the age of short statured adults.
- When a fracture is suspected, minimize handling of the affected limb.
- Respect the opinions, advice, or instructions provided by parents, children, and adults with brittle bone disease. Based on experience they give good directions for the safest ways to lift, carry or reposition. Having dealt with dozens of fractures and medical procedures, even children have a good sense of when a bone is broken even before x-rays are taken.
- Handle babies with extra care. Although there are handling techniques and precautions, it is in the child’s best interest to be held and touched and encouraged to explore independent movement to the greatest extent possible. Immobility increases bone loss and decreases muscle mass, leading to weakness, bone fragility, and more fractures.
- Lift a baby with brittle bone disease by placing one hand under the buttocks and legs, and the other hand under the shoulders, neck and head.
- Do not lift the baby from under the armpits.
- Do not lift by the ankles to change a diaper; rather slide a hand under the buttocks.
- Babies do not need to be kept on a pillow or soft surface. Encourage babies to explore independent movement.
- Supporting infants in a variety of positions (e.g., side lying, stomach lying) develops muscles that will help with sitting and standing later on.





{kind=link}