What is Castleman disease
Castleman disease is a rare disease of lymph nodes and related tissues. It is also known as Castleman’s disease, giant lymph node hyperplasia and angiofollicular lymph node hyperplasia. It was first described by Dr. Benjamin Castleman in the 1950s 1. Castleman disease is not cancer. Instead, it is called a lymphoproliferative disorder. This means there is an abnormal overgrowth of cells of the lymph system that is similar in many ways to lymphomas (cancers of lymph nodes). Castleman disease may also be associated with malignancies such as Kaposi sarcoma, non-Hodgkin lymphoma, Hodgkin lymphoma, and POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy and skin changes) syndrome.
Even though Castleman disease is not officially a cancer, one form of this disease (known as multicentric Castleman disease) acts very much like lymphoma. In fact, many people with this disease eventually develop lymphomas. And like lymphoma, Castleman disease is often treated with chemotherapy or radiation therapy.
There are two main forms of Castleman disease:
- Unicentric Castleman disease.
- Multicentric Castleman disease.
Unicentric Castleman disease is a “localized” condition that is generally confined to a single set of lymph nodes, while multicentric Castleman disease is a “systemic” disease that affects multiple sets of lymph nodes and other tissues throughout the body 2. The exact underlying cause of Castleman disease is currently unknown; however, it is thought to occur sporadically in people with no family history of the condition. Treatment varies based on the form of the condition, the severity of symptoms and whether or not the affected person also has an HIV and/or human herpes virus type 8 (HHV-8) infection 3.
Patients with Castleman disease may be asymptomatic or may present with a variety of signs and symptoms. A variety of laboratory tests and imaging studies are indicated for the assessment, but the diagnosis is confirmed by histologic examination of a needle biopsy specimen from an involved lymph node.
Treatment varies depending on the type of Castleman disease: unicentric or multicentric. Surgical removal of the involved node is usually curative in unicentric disease, but is rarely curative in multicentric Castleman disease.The interleukin-6 inhibitor siltuximab is approved for multicentric Castleman disease in patients who are negative for HIV and human herpesvirus–8.
Doctors don’t know how many people are diagnosed with Castleman disease each year. Doctors do know that Castleman disease is rare, especially in people who are otherwise healthy.
The localized (unicentric) form of Castleman disease is more common than the multicentric Castleman disease. Multicentric Castleman disease is much more likely to occur in people infected with HIV. Over the past few decades, as the number of people with HIV infection has increased, the number of people diagnosed with multicentric Castleman disease has also gone up. Modern anti-viral treatments have helped people with HIV live much longer, but these drugs don’t seem to lower the chance of getting multicentric Castleman disease.
Castleman disease can affect children as well as adults. Younger people are more likely to have the localized form. Older adults and those with HIV infection are more likely to have the multicentric form.
The mean age of patients with multicentric Castleman disease is 50-65 years. Persons with HIV infection may be younger. Males account for 50%-65% of multicentric Castleman disease cases.
Lymph nodes and lymphoid tissue
To understand Castleman disease, it helps to know about the body’s lymph system.
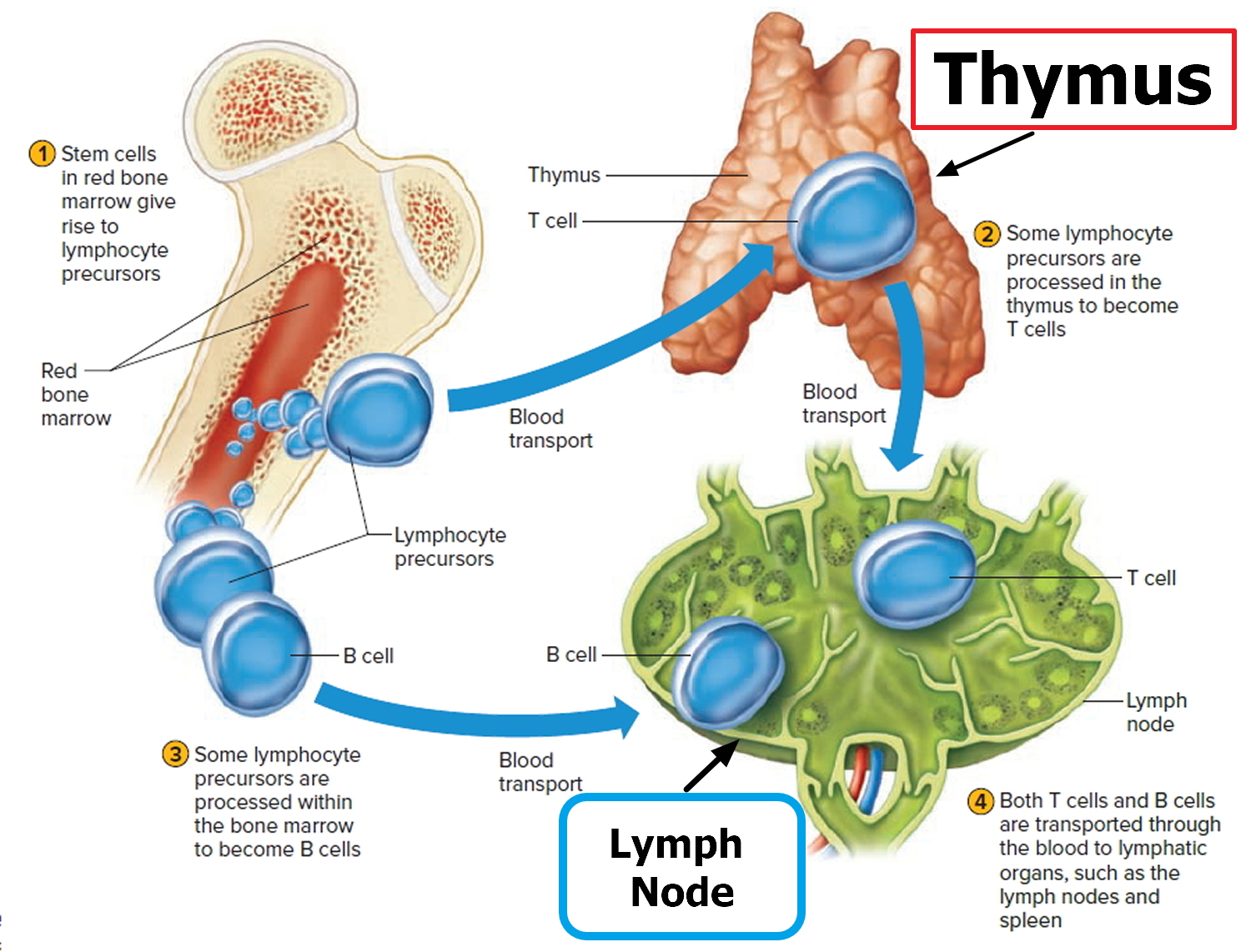
Lymphoid tissue, also known as lymphatic tissue, is the main part of the immune system. It is formed by different types of cells that work together to help the body fight infections. The main cells in lymphoid tissue are lymphocytes, a type of white blood cell. There are 2 main types of lymphocytes: B cells and T cells.
Lymphoid tissue is found in many places throughout the body, including:
- Lymph nodes: bean-sized collections of lymphocytes found in small groups throughout the body, including inside the chest, abdomen, and pelvis. They can sometimes be felt under the skin in the neck, under the arms, and in the groin.
- Thymus: a small organ behind the upper part of the breastbone and in front of the heart. The thymus plays a vital role in development of T cells.
- Spleen: an organ under the lower part of the rib cage on the left side of the body. The spleen makes lymphocytes and other immune system cells to help fight infection. It also stores healthy blood cells and helps filter the blood.
- Tonsils and adenoids: collections of lymphoid tissue at the back of the throat. They help protect the body against germs that are breathed in or swallowed.
- Bone marrow: the soft inner part of certain bones that makes red blood cells, blood platelets, and white blood cells (including lymphocytes).
- Digestive tract: the stomach, intestines, and other organs, which also have lymphoid tissue.
Figure 1. Locations of major lymph nodes
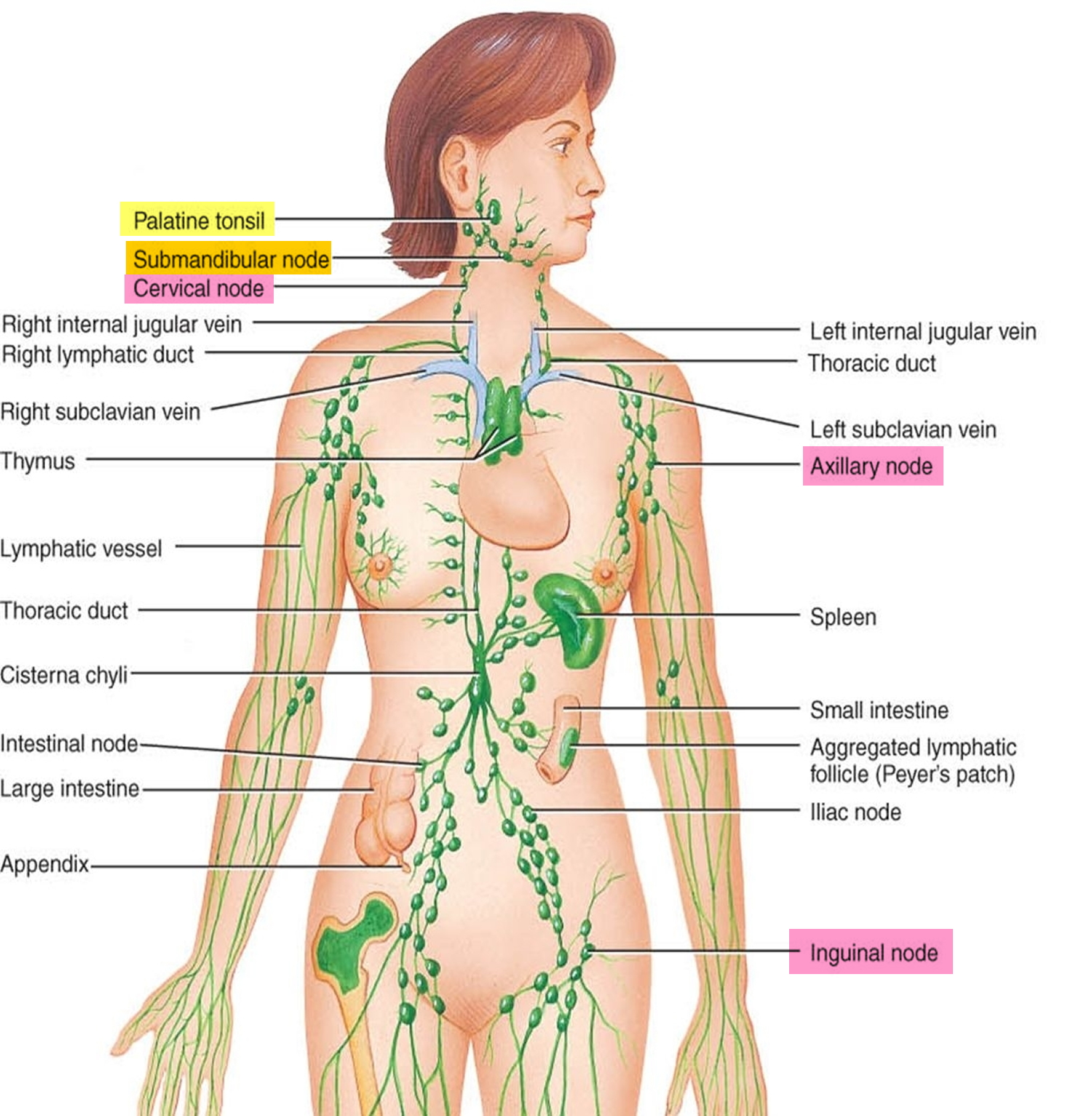
Figure 2. Functions of lymph nodes in the lymphatic system
Types of Castleman disease
Doctors can group Castleman disease in a number of ways, and they are still trying to determine which classification (or combination of them) provides the most helpful information.
Localized versus multicentric Castleman disease
The main way to classify Castleman disease is based on how much of the body it affects. The 2 main forms of Castleman disease are called localized and multicentric. They affect people very differently.
Localized (unicentric) Castleman disease
This is the more common type of Castleman disease. Localized Castleman disease only affects a single group of lymph nodes. It is not widespread. Lymph nodes in the chest or abdomen are affected most often. Castleman disease causes these lymph nodes to grow.
Enlarged lymph nodes in the chest can press on the windpipe (trachea) or smaller breathing tubes going into the lungs (bronchi), causing breathing problems. If the enlarged nodes are in the abdomen, the person might have pain, a feeling of fullness, or trouble eating. Sometimes the enlarged nodes are in places such as the neck, groin, or underarm area and are first noticed as a lump under the skin.
People with localized Castleman disease are usually cured when the affected lymph nodes are removed with surgery.
Multicentric Castleman disease
Multicentric Castleman disease affects more than one group of lymph nodes. It can also affect other organs containing lymphoid tissue. This form sometimes occurs in people infected with human immunodeficiency virus (HIV), the virus that causes AIDS. Multicentric Castleman disease is more serious than the localized type, particularly in people with HIV infection. You can read more about HIV infection in our post HIV and AIDS.
People with Multicentric Castleman disease often have problems such as serious infections, fevers, weight loss, fatigue, night sweats, and nerve damage that can cause weakness and numbness. Blood tests often show too few red blood cells (anemia) and high levels of antibodies in the blood (hypergammaglobulinemia).
Multicentric Castleman disease can weaken the body’s immune system, making it hard to fight infection. Infections in people with Multicentric Castleman disease can be very serious, even life threatening. Multicentric Castleman disease also increases the risk of developing lymphoma, a cancer of lymphoid tissue, which can often be hard to treat.
Microscopic subtypes of Castleman disease
Castleman disease can also be classified based on how the lymph node tissue looks under a microscope. These are called microscopic subtypes.
- The hyaline vascular type is most common. It tends to be localized, in which case people often have few symptoms and usually have a good outlook, but in rare cases it can be multicentric.
- The plasma cell type is more likely to cause symptoms and to be multicentric, but it is sometimes localized.
- The mixed subtype shows areas of both hyaline vascular and plasma cell types. It occurs less often.
- The plasmablastic type was recognized more recently. Like the plasma cell type, it is usually multicentric, usually causes symptoms, and has a less favorable outlook.
In choosing treatments, doctors believe that the microscopic type is less important than whether the disease is localized or multicentric.
Infection with certain viruses plays a role in at least some cases of Castleman disease.
Multicentric Castleman disease is more common in people infected with HIV, the virus that causes AIDS. Doctors sometimes group patients with multicentric Castleman disease into those who are infected with HIV (HIV positive) and those who are not infected (HIV negative).
In recent years, it’s become clear that another virus, known as human herpesvirus-8 (HHV-8) or Kaposi sarcoma herpesvirus (KSHV), is often found in the lymph node cells of people with multicentric Castleman disease. In fact, HHV-8 is found in the lymph nodes of nearly all Castleman disease patients who are HIV positive. Some doctors have suggested classifying Castleman disease based on whether the cells contain HHV-8.
Outlook (Prognosis) for People With Castleman Disease
Survival rates are often used by doctors as a standard way of discussing a person’s outlook (prognosis).
It’s hard to get accurate numbers on the outlook for people with Castleman disease because it is rare. Most statistics on the disease come from small numbers of patients who were treated at a single center or hospital. These numbers might not accurately reflect the outcomes for all people with Castleman disease.
The numbers below come from a study of nearly 200 people treated for Castleman disease in many different centers. The study divided people into groups based on whether the Castleman disease was unicentric or multicentric, its microscopic subtype, and whether the patient was infected with HIV (HIV+) or not infected (HIV-).
The 3-year disease-free survival rate refers to the percentage of patients who were still alive and had no signs of Castleman disease at least 3 years after it was diagnosed. Of course, many people went much longer than 3 years without any signs of Castleman disease (and many were likely cured).
| Type of Castleman Disease | 3-Year Disease-Free Survival |
| Unicentric, hyaline vascular, HIV- | 93% |
| Unicentric, plasma cell or mixed, HIV-, OR Multicentric, hyaline vascular, HIV- | 79% |
| Multicentric, plasma cell, HIV- | 46% |
| HIV+ (multicentric) | 28% |
Even when taking the factors above into account, disease-free survival rates are at best rough estimates. If you have Castleman disease, your doctor can tell you how well these numbers might apply to you, as he or she knows your situation best.
Castleman disease causes
The exact underlying cause of Castleman disease is poorly understood. The main feature of Castleman disease is an overgrowth of lymphocytes (immune cells) called B cells. The cause of this overgrowth is not known for sure, but it seems to be related to problems with the way a person’s immune system is working. Many people with Castleman disease have abnormally high blood levels of certain substances made by immune system cells. However, some scientists suspect that an increased production of interleukin-6 (IL-6) by the immune system may contribute to the development of Castleman disease. IL-6 is a substance normally produced by cells within the lymph nodes that helps coordinate the immune response to infection. Increased production of IL-6 may result in an overgrowth of lymphatic cells, leading to many of the signs and symptoms of Castleman disease. But it’s not clear what causes the high levels of IL-6.
It has also been found that a virus called human herpes virus type 8 (also known as HHV-8, Kaposi’s sarcoma-associated herpesvirus, or KSHV) is present in many people with multicentric Castleman disease, specifically. HHV-8 is found in nearly all people who are HIV-positive and develop multicentric Castleman disease, and in up to 60% of affected people without HIV. The HHV-8 virus may possibly cause multicentric Castleman disease by making its own IL-6. HHV-8 can cause infected cells to make a form of IL-6, which could explain how it leads to Castleman disease.
Many people are infected with HHV-8, but in people with normal immune systems the virus doesn’t seem to cause problems. People infected with HIV, however, often have weakened immune systems, which might allow HHV-8 to grow and cause problems. This could explain why people infected with HIV are more likely get multicentric Castleman disease. Still, some people with HIV who develop multicentric Castleman disease do not have weakened immune systems, so it’s not clear if this is the only reason.
HHV-8 hasn’t been found in all cases of multicentric Castleman disease. And it’s not clear what causes the localized (unicentric) form of Castleman disease. Researchers are still looking for the causes of Castleman disease in these other cases.
Risk Factors for Castleman Disease
A risk factor is anything that might change a person’s chance of getting a disease. But having a risk factor, or even several, doesn’t mean that you will get the disease, and having few or no risk factors doesn’t mean you won’t get the disease.
Most patients with Castleman disease don’t have any known risk factors.
The only clear risk factor for Castleman disease is infection with HIV, the virus that causes AIDS. The multicentric form of Castleman disease is much more common in people with HIV infection, particularly in those who have developed AIDS. This might be because these people tend to have weakened immune systems, which allows for the growth of another virus known as HHV-8. It’s not clear if people who have weakened immune systems for other reasons are also at increased risk.
The incidence of multicentric Castleman disease has increased with better antiretroviral therapy for the management of HIV infection. On multivariate analysis, risk factors for the development of multicentric Castleman disease included the following 4:
- Nadir CD4 count higher than 200/µL
- Increased age
- No previous antiretroviral therapy exposure
- Nonwhite ethnicity
Castleman disease signs and symptoms
Castleman disease can cause a variety of signs and symptoms or can remain asymptomatic. If symptoms do occur, they are often like those seen with other diseases, such as infections, autoimmune diseases, or even some types of cancer. Because of this, doctors might not suspect Castleman disease at first.
Unicentric Castleman disease and multicentric Castleman disease tend to present differently.
Unicentric or localized Castleman disease is generally asymptomatic but may present as follows:
The localized form of Castleman disease often starts as an enlarged lymph node. If the node is just under the skin, such as in the neck or underarm area, it might be seen or felt as a lump. But if it’s in the chest or abdomen (belly), it might not be noticed until it grows large enough to cause other symptoms:
- Localized lymphadenopathy with resultant compressive symptoms. An enlarged node in the chest might press on the windpipe, which could cause trouble breathing, wheezing, a cough, or a feeling of fullness in the chest. An enlarged node in the abdomen can cause trouble eating, pain, or just a feeling of fullness.
- Systemic manifestations like those of multicentric Castleman disease.
In general, most people with localized Castleman disease feel well otherwise. In fact, some people have no symptoms at all, and the Castleman disease is only found when the doctor does a test for another reason. On the other hand, some people with localized Castleman disease can also have some of the other symptoms listed below.
Signs and symptoms of multicentric Castleman disease may include multiple lymphadenopathy and/or the following systemic manifestations, although some cases (<10%) are asymptomatic:
People with multicentric Castleman disease have more than one area of enlarged lymph nodes. The enlarged nodes can be in the chest or abdomen, but multicentric Castleman disease often affects lymph nodes in the groin, the underarm area, and on the sides of the neck, which can often be seen or felt as lumps under the skin.
Multicentric Castleman disease can also affect lymphoid tissue of internal organs, causing the liver, spleen, or other organs to enlarge. Enlarged organs might be seen or felt as masses under either side of the rib cage. They can also cause problems eating or a sense of fullness (or even pain) in the abdomen.
In addition, people with either type of Castleman disease can have other symptoms (although these symptoms are much more common in people with multicentric Castleman disease:
- Fever
- Night sweats (that soak the sheets)
- Weight loss
- Loss of appetite
- Weakness
- Fatigue
- Shortness of breath, cough
- Nausea and vomiting
- Numbness and weakness (neuropathy)
- Leg edema
- Skin rashes
- Hemangiomata
- Pemphigus
- Kaposi sarcoma
Some of these symptoms might come and go over time.
Other conditions associated with multicentric Castleman disease include the following:
- Amyloidosis
- POEMS (polyradiculoneuropathy, organomegaly, endocrinopathy, monoclonal plasma cell proliferative disorder, and skin changes) syndrome
- Autoimmune disease
- Hemolytic anemia
- Immune thrombocytopenic purpura (ITP)
- Acquired factor VIII deficiency
Some of these signs and symptoms symptoms might remit and relapse over time.
Amyloidosis, a condition in which abnormal proteins build up in tissues around the body, can occur in Castleman disease. This can lead to kidney damage; heart damage; nerve damage; and intestinal problems, mainly diarrhea. If the Castleman disease is treated successfully, the amyloidosis may improve or disappear.
Anemia can lead to problems such as fatigue and shortness of breath.
“B” symptoms, including severe fatigue, night sweats, fever, weight loss, and anorexia are typically present. These symptoms are typically driven by overproduction of interleukin-6 (IL-6). Overproduction of IL-6 also results in an acute-phase reaction, with elevation of the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level, elevated fibrinogen, thrombocytosis, and hypogammaglobinemia on laboratory testing.
Castleman disease diagnosis
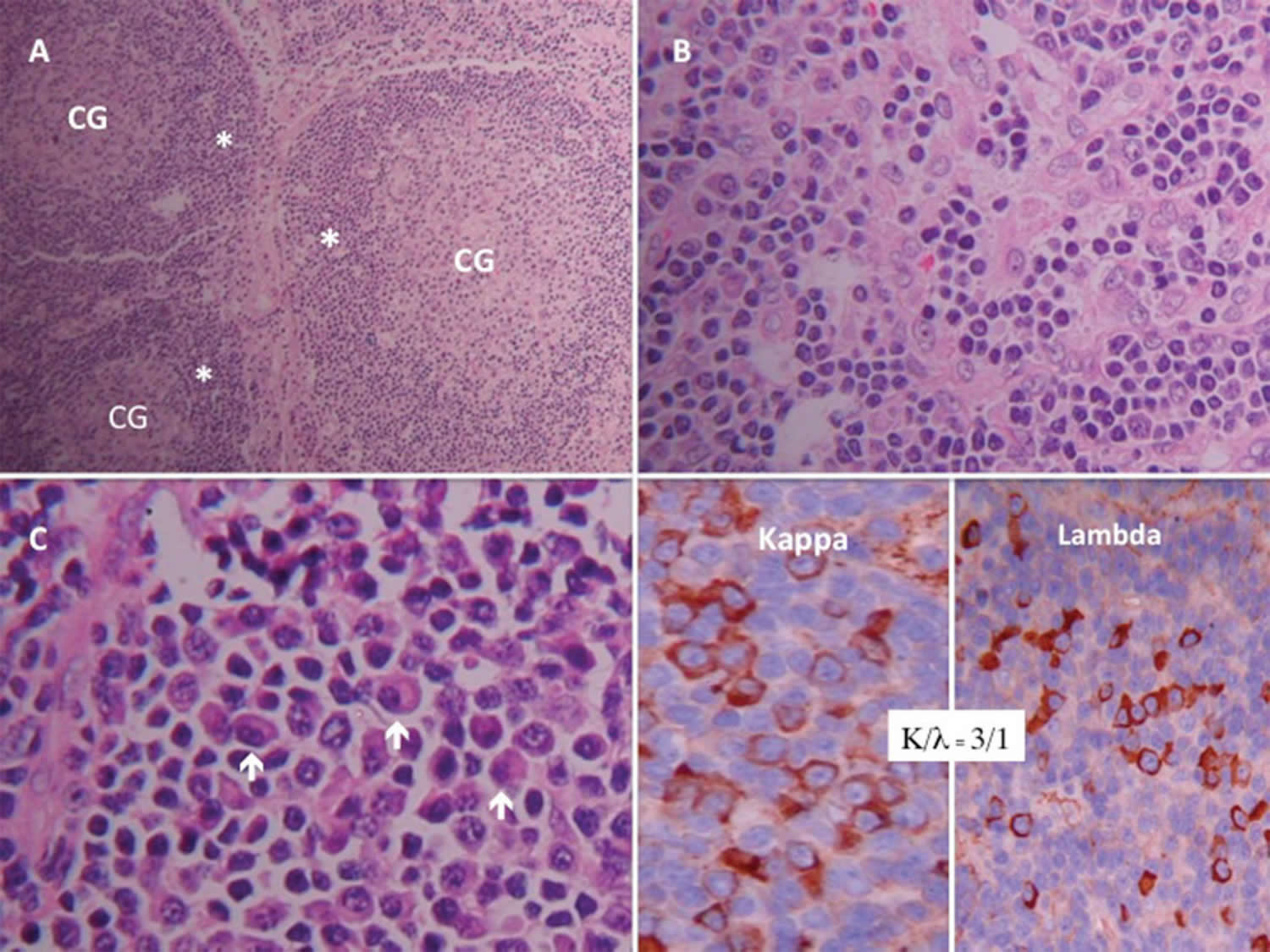
Castleman disease should be suspected in patients who present with peripheral lymphadenopathy, fever, splenomegaly, and an elevated C-reactive protein (CRP) level. The diagnosis is confirmed by histologic examination of needle biopsy specimen from an involved lymph node. Histopathologically, Castleman disease is identfied by polyclonal nodal expansions that usually leave the structure of the underlying lymph node at least partially intact and histologic features that are consistent with the hyaline vascular or plasma cell variants.
Castleman disease is rare, and its symptoms are often like those caused by other diseases (including infections, autoimmune diseases, and lymphomas), so doctors often suspect it is something else at first. The actual diagnosis of Castleman disease is made when doctors remove an affected lymph node and look at it under a microscope. This procedure, known as a biopsy, is described below.
IgH gene rearrangement studies should be performed on the lymph node specimen to rule out a clonal disorder (eg, occult lymphoma).
Chest radiography and other imaging findings are nonspecific.
Figure 1. Castleman disease chest X-ray
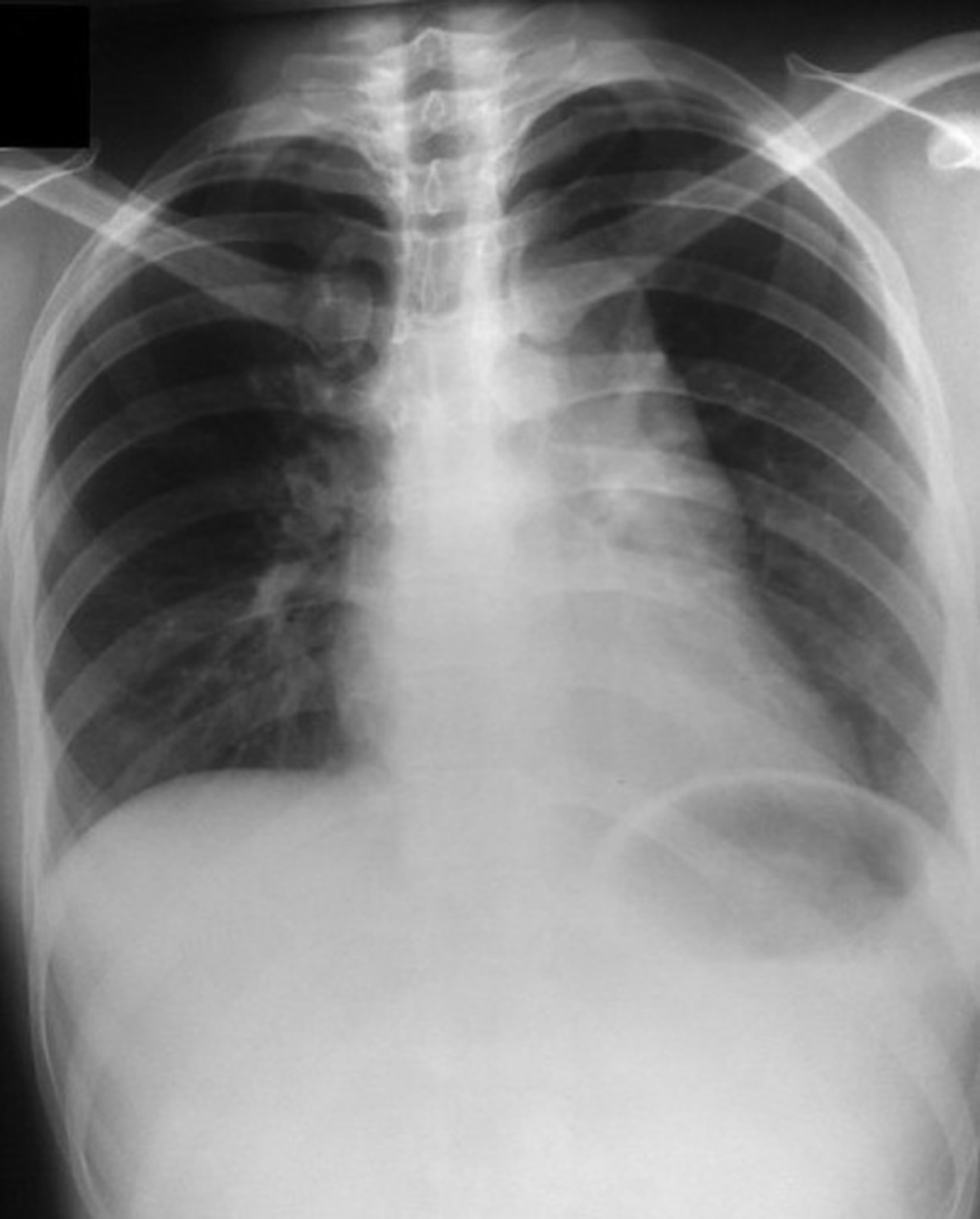

Note: Chest radiographs show a lobulated soft tissue density obscuring the aortic knob and extending down to the level of the left atrial appendage. The mass appears to be located in the anterior mediastinum on the lateral view.
Figure 2. Castleman disease CT scan (axial non-contrast)
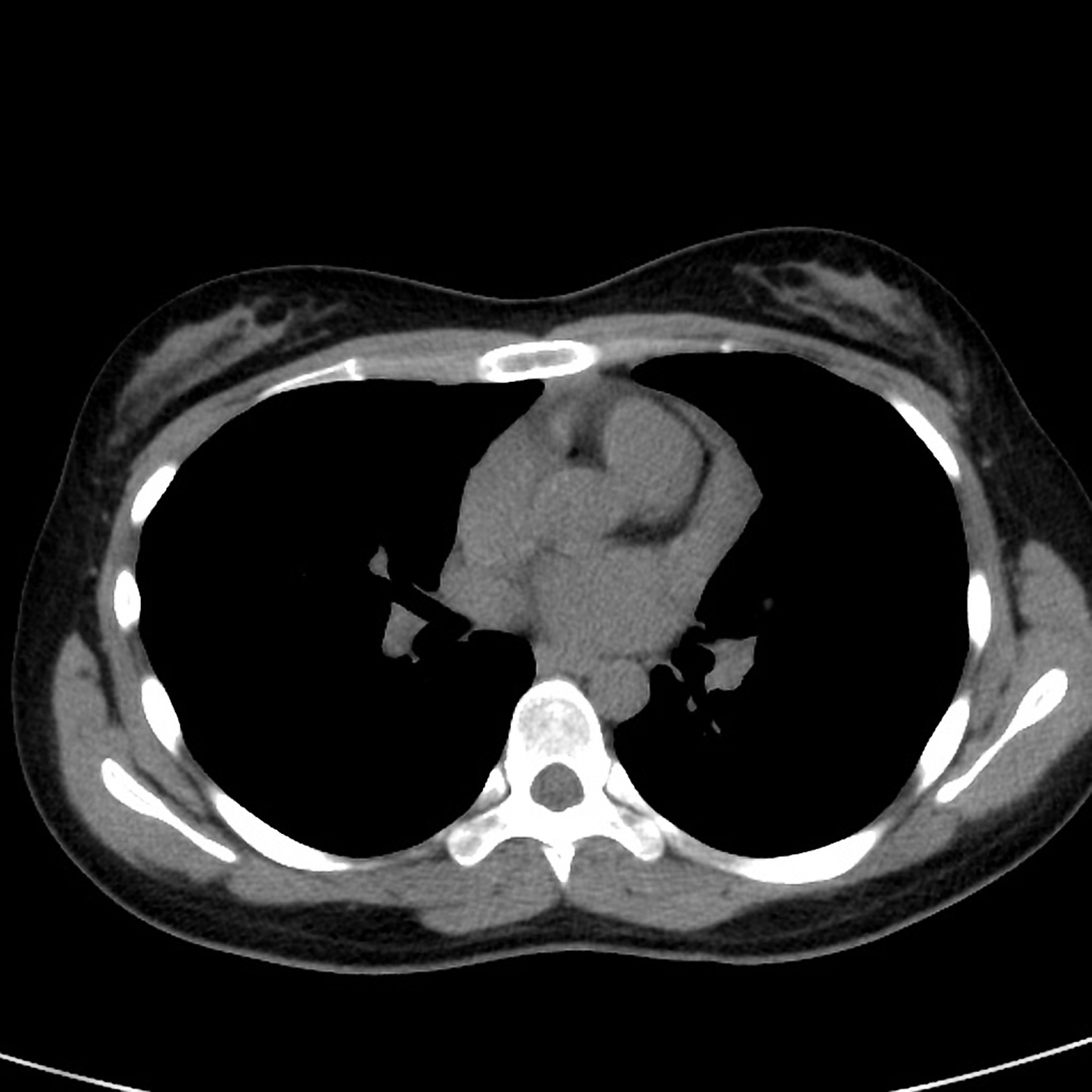
Figure 3. Castleman disease CT scan (axial with contrast)
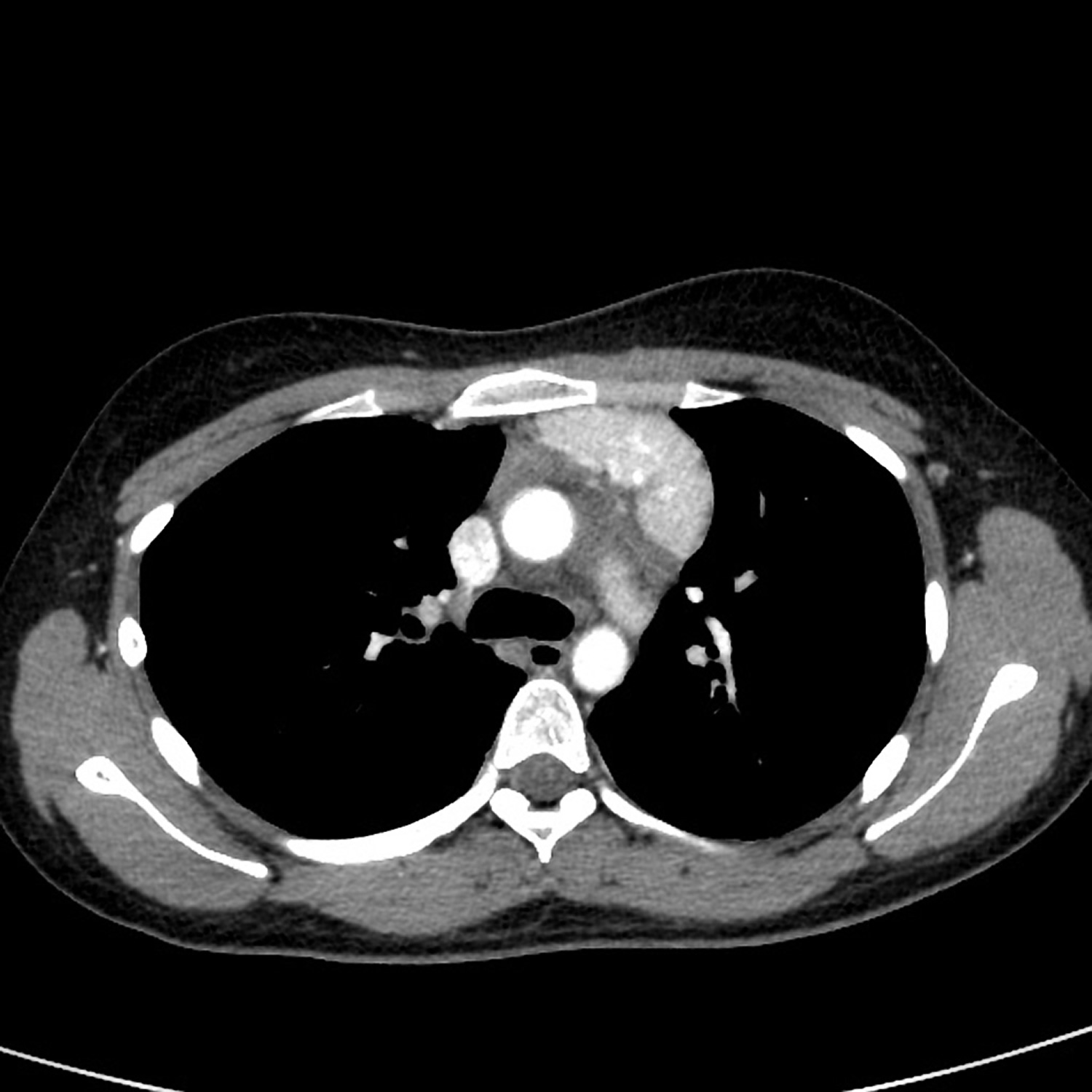
Note: There is an intensely enhancing, non-calcified, lobulated mass, measuring approximately 2.4 x 5.9 x. 6.7 cm ( AP x W x CC), in the left anterior mediastinum at the level of the aortic arch extending to the left lateral aspect of the main pulmonary artery.
Castleman disease radiology
In patients with multicentric Castleman disease, the chest radiograph may show bilateral reticular or ground-glass opacities, mediastinal widening, and/or bilateral pleural effusions.
Chest computed tomography (CT) scans may demonstrate lymphadenopathy of multiple enlarged mediastinal and hilar lymph nodes (1-3 cm in diameter). Lung parenchymal findings may be seen, including subpleural nodules, interlobular septal thickening, peribronchovascular thickening, ground-glass opacities, and patchy rounded areas of consolidation. Small to moderate bilateral pleural effusions may also be present.
CT scanning of the neck, abdomen, and pelvis, with and without contrast, may also be helpful.
Multicentric Castleman disease is positron emission tomography (PET)–avid, usually with a relatively low standardized uptake value of 2.5-5 5. PET scans are helpful in finding small collections of fast-growing cells that might not be visible on a CT scan. PET is not often used to diagnose Castleman disease, but sometimes it can help the doctor determine the cause of enlarged lymph nodes. Currently, PET scanning is more often used for staging.
For a PET scan, a form of radioactive sugar (known as fluorodeoxyglucose or FDG) is injected into the blood. (The amount of radioactivity used is very low and will pass out of the body over the next day or so.) After about an hour, you are moved onto a table in the PET scanner. You lie on the table for about 30 minutes while a special camera creates a picture showing areas of radioactivity in the body.
Any cancer cells in the body will be growing quickly, so they absorb large amounts of the radioactive sugar. Although Castleman disease cells don’t take up the sugar as much as cancer cells, they do seem to take it up more than normal cells. The picture from a PET scan is not detailed like a CT or MRI scan, but it can provide helpful information about your whole body.
Often the PET scan is combined with a CT scan, which is more detailed. This helps the doctor determine if abnormal areas seen on the CT scan are Castleman disease, cancer, or something else.
Laboratory Studies
Laboratory studies used in the workup of Castleman disease, and characteristic findings, include the following:
- Complete blood cell (CBC) count – Anemia (usually mild to moderate, occasionally, the hemoglobin level is <8 g/dL), thrombocytosis
- Liver function tests (LFT) – Hypoalbuminemia
- Serum protein electrophoresis, with immunofixation and quantitative immunoglobulins – Polyclonal hypergammaglobulinemia
- Erythrocyte sedimentation rate (ESR) – Usually elevated
- Serologies for hepatitis B, human herpesvius–8 (HHV-8), and HIV; with quantitative assays if initial results are positive
- Interleukin-6 (IL-6), lactate dehydrogenase (LDH), and C-reactive protein (CRP) levels – Usually elevated
- Vascular endothelial growth factor (VEGF) – May be elevated
Lymph Node Biopsy
A doctor might suspect you have Castleman disease based on your symptoms or the results of exams or tests, but it can only be diagnosed by removing an enlarged lymph node and examining it under the microscope. This procedure is called a biopsy. Different types of biopsies can be used, based on where the lymph node is.
Excisional or incisional biopsy: If the lymph node is near the skin surface, a surgeon can often remove the node using local anesthesia (numbing medicine). The surgeon cuts the skin over the enlarged lymph node, removes the node, and then stitches the cut closed. If the procedure removes the entire lymph node, it is called an excisional biopsy. If only part of the node is removed, it is called an incisional biopsy.
If the lymph node is in the chest or the abdomen, the surgeon might need to make a large incision to get into either of these places. This type of surgery might require general anesthesia (where you are in a deep sleep), but it might be needed to learn why the lymph node is enlarged.
Sometimes, lymph nodes in the chest can be removed by mediastinoscopy. In this procedure, a small cut is made in the front of the neck and a thin, hollow, lighted tube (called a mediastinoscope) is inserted behind the sternum (breast bone) and in front of the windpipe to look at the area. Special instruments can be passed through this tube to remove all or part of a lymph node.
The same type of procedure can be used to sample lymph nodes in the abdomen. In this case, the test is known as laparoscopy. The doctor makes a small cut in the abdomen and inserts a thin, hollow, lighted tube (called a laparoscope) and other instruments to look at the area and remove all or part of a lymph node.
Fine needle aspiration (FNA) or core needle biopsy: Sometimes lymph nodes are biopsied by putting a hollow needle into the node to remove a small amount of tissue. In a fine needle aspiration (FNA) biopsy, the doctor uses a very thin needle to withdraw (aspirate) a small amount of tissue from the enlarged node. For a core needle biopsy, the doctor uses a larger needle to remove a slightly larger piece of tissue.
Doctors have found that diagnosing Castleman disease by needle biopsy is sometimes possible, but biopsy methods that remove larger samples of tissue are usually recommended because they are thought to be more accurate.
Lab tests of biopsy samples
All biopsy specimens are looked at under a microscope by a pathologist (a doctor specially trained to diagnose disease), who studies the size and shape of the cells and how they are arranged. Since Castleman disease is so rare, the pathologist might ask another pathologist with special training in diagnosing blood and lymph node diseases (called a hematopathologist) to look at the biopsy.
Sometimes it’s hard to tell if the lymph node is affected by Castleman disease or by lymphoma. In these cases, other tests might be done on the lymph node tissue to help figure this out. Some tests look at the proteins on the surface of the cells, while others look for gene or chromosome changes within the cells. Examples of these lab tests include:
- Immunohistochemistry
- Flow cytometry
- Cytogenetics
- Fluorescent in situ hybridization (FISH)
- Polymerase chain reaction (PCR)
How is Castleman Disease Staged?
When talking about cancer, the stage is a description of how far it has spread. The stage helps doctors determine the best treatment and the likely outlook (prognosis) for the patient. Most cancers have a formal staging system that lets doctors sum up the extent of the cancer.
Since Castleman disease is not a cancer, it doesn’t have a formal staging system. Instead, doctors use other important pieces of information to help decide on the best treatment and to give them an idea of how well a patient might do.
The most important factor when deciding on treatment is whether the Castleman disease is localized/unicentric or multicentric. Localized/unicentric Castleman disease affects only a single lymph node (or lymph node group). The multicentric type affects 2 or more groups of lymph nodes in different parts of the body. It may also affect internal organs like the spleen or liver. Tests are done to see what lymph nodes and organs are affected to learn which type of Castleman disease a patient has. These tests often include some of the imaging tests such as a chest x-ray and either a CT scan or MRI of the chest and abdomen.
Another factor is the microscopic subtype of the Castleman disease, which is a description of the patterns of cells seen under the microscope in the biopsy sample.
A third important factor is whether or not the patient is infected with the human immunodeficiency virus (HIV), the virus that causes AIDS. Just about all people infected with HIV who develop Castleman disease will have the multicentric form of the disease.
Castleman disease treatment
Treatment varies depending on the type of Castleman disease: unicentric or multicentric. Surgical removal of the involved node is usually curative in unicentric disease, but is rarely curative in multicentric Castleman disease. Splenectomy can result in a transient symptomatic improvement in some patients.
There is no standard therapy for multicentric Castleman disease, and clinical practice varies.
Unicentric Castleman Disease
Surgery is usually curative. In patients whose lesions cannot be completely resected, outcomes remain favorable. Partially resected masses may remain stable and asymptomatic for many years.
Patients with unresectable diseases with compressive symptoms can be treated as described for HIV-negative multicentric Castleman disease.
Systemic steroids can provide symptomatic relief but do not predictably reduce tumor size.
Radiation therapy with 30-45 Gy can result in complete and partial remission rates of 40% and 10%, respectively, but can cause radiation-induced fibrosis that makes subsequent surgical intervention more difficult 6.
Multicentric Castleman Disease
There is no standard therapy for multicentric Castleman disease and clinical practice varies. Patients with multicentric Castleman disease should be encouraged to enroll in clinical trials, whenever available. If no clinical trial is available, therapy depends on HIV/HHV-8 status and then on the clinical aggressiveness of the disease. Treatment options are discussed below.
IL-6–directed therapy
Especially in HIV/HHV-8–negative patients with mild symptoms and no organ failure, immunotherapy with monoclonal antibodies directed at IL-6 (siltuximab) or the IL-6 receptor (tocilizumab) was reported to yield a 2-year overall survival rates and relapse-free rates of 94%-95% and 79%-85%, respectively 7.
Siltuximab is often preferred, based on its benefit in the only randomized trial 8. A case report by Patel et al 9 describes an exceptional response to siltuximab in a patient whose pretreatment serum IL-6 levels were normal, but in whom next-generation sequencing demonstrated a missense mutation in the Janus Kinase 1 (JAK1) gene, which codes for a crucial signaling component of the IL-6/IL-6 receptor/gp130 machinery. Treatment with siltuximab in their patient resulted in a complete response lasting 7 years.
Anti–IL-6–directed treatment is continued until progression of disease in order to maintain the response and prevent an early relapse.
Anti-CD20 monoclonal antibody therapy
If neither siltuximab nor tocilizumab is available, experts recommend the anti-CD20 monoclonal antibody rituximab, which affects IL-6 production. Rituximab may be administered or without steroids and/or chemotherapy and may be used regardless of HIV status and typically yields a good response, especially when used along with chemotherapy. However, rituximab therapy occasionally worsens Kaposi sarcoma, which must be carefully considered in HIV-positive patients with high viral load, low CD4 count, and active Kaposi sarcoma 10.
Cytotoxic chemotherapy
Cytotoxic chemotherapy has been used with agents such as vinblastine and etoposide, both as single agents, yielding symptomatic relief and a partial response in almost all patients 11.
However, symptoms recur when treatment is stopped, necessitating intermittent maintenance therapy, often lifelong. Thus, combination chemotherapy is usually preferred to monotherapy when chemotherapy is given. Etoposide is often used with rituximab in HIV/HHV-8–positive patients with organ dysfunction and aggressive disease.
Medication Summary
Various therapies have been used for multicentric Castleman disease, including the following:
- Intravenous immunoglobulin (IVIG)
- Antivirals that target human herpesvirus–8 (HHV-8),
- Angiogenesis inhibitors (eg, thalidomide)
- Corticosteroids for inflammation
- Chemotherapy
- Agents that decrease interleukin-6 (IL-6).
Siltuximab (Sylvant) is the only biologic approved by the US Food and Drug Administration (FDA) for multicentric Castleman disease 12. Siltuximab is a monoclonal antibody that binds IL-6. Other drugs with anti-IL-6 actions that are used off-label include tocilizumab and rituximab. Tocilizumab is an IL-6 antagonist, while rituximab targets CD20 and affects IL-6 production.
Immunomodulators
Class Summary
Agents that decrease IL-6 production or actions are emerging for multicentric Castleman disease.
Siltuximab (Sylvant)
Siltuximab is a monoclonal antibody that binds IL-6 and prevents the binding of IL-6 to both soluble and membrane-bound IL-6 receptors. It is approved by the FDA with an indication for multicentric Castleman disease in patients who are negative for HIV and human herpesvirus-8.
Tocilizumab (Actemra)
Tocilizumab is an IL-6 receptor antagonist. It has been used off-label for multicentric Castleman disease.
Rituximab (Rituxan)
Rituximab is a humanized monoclonal antibody that binds to CD20 antigen, which results in decreased IL-6 production. It has been used off-label for multicentric Castleman disease.
Treatment in HIV/HHV-8–positive patients
In most HIV/HHV-8–positive patients, experts often suggest a combination of ganciclovir plus rituximab, with etoposide added for symptomatic or aggressive disease 13.
Antiretroviral therapy therapy is often included with the above combination regimen in patients with a low CD4 count, higher HIV load, and/or active Kaposi sarcoma.
Other therapies with limited efficacy data include the following:
- Antiviral therapy (ganciclovir, cidofovir, interferon alpha)
- Bortezomib: Shown to have activity in the plasma cell variant of Castleman disease 14
- Thalidomide plus rituximab: Has also been shown to induce some responses 15
Long-Term Monitoring
Disease response is assessed with imaging and laboratory data after about 4 cycles of therapy. A second round may be administered upon a partial response. IL-6–directed therapy should be given continuously.
Monitoring at periodic intervals (2-4 months) with a history and physical examination and serum biomarkers (including IL-6, CRP, serum free light chain assay, quantitative immunoglobulins) is often done. Generally, annual imaging can be discontinued after 5 years if the patient remains disease-free.
References- Castleman B, Iverson L, Menendez VP. Localized mediastinal lymphnode hyperplasia resembling thymoma. Cancer. 1956 Jul-Aug. 9(4):822-30.
- Jennifer R Brown, MD, PhD; Jon C Aster, MD; Nikhil C Munshi, MD. Unicentric Castleman’s disease. UpToDate.
- Yu L, Tu M, Cortes J, Xu-Monette ZY, Miranda RN, Zhang J, et al. Clinical and pathological characteristics of HIV- and HHV-8-negative Castleman disease. Blood. 2017 Mar 23. 129 (12):1658-1668.
- Casper C. The aetiology and management of Castleman disease at 50 years: translating pathophysiology to patient care. Br J Haematol. 2005 Apr. 129(1):3-17.
- Barker R, Kazmi F, Stebbing J, Ngan S, Chinn R, Nelson M, et al. FDG-PET/CT imaging in the management of HIV-associated multicentric Castleman’s disease. Eur J Nucl Med Mol Imaging. 2009 Apr. 36(4):648-52.
- Chronowski GM, Ha CS, Wilder RB, Cabanillas F, Manning J, Cox JD. Treatment of unicentric and multicentric Castleman disease and the role of radiotherapy. Cancer. 2001 Aug 1. 92(3):670-6.
- Kawabata H, Tomosugi N, Kanda J, Tanaka Y, Yoshizaki K, Uchiyama T. Anti-interleukin 6 receptor antibody tocilizumab reduces the level of serum hepcidin in patients with multicentric Castleman’s disease. Haematologica. 2007 Jun. 92(6):857-8.
- van Rhee F, Wong RS, Munshi N, Rossi JF, Ke XY, Fosså A, et al. Siltuximab for multicentric Castleman’s disease: a randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2014 Aug. 15(9):966-74.
- Patel M, Ikeda S, Pilat SR, Kurzrock R. JAK1 Genomic Alteration Associated With Exceptional Response to Siltuximab in Cutaneous Castleman Disease. JAMA Dermatol. 2017 May 1. 153 (5):449-452.
- Bower M. How I treat HIV-associated multicentric Castleman disease. Blood. 2010 Nov 25. 116(22):4415-21.
- Scott D, Cabral L, Harrington WJ Jr. Treatment of HIV-associated multicentric Castleman’s disease with oral etoposide. Am J Hematol. 2001 Feb. 66(2):148-50.
- Wong RS, Casper C, Munshi N, et al. A Multicenter, Randomized, Double-Blind, Placebo-Controlled Study Of The Efficacy and Safety Of Siltuximab, An Anti-Interleukin-6 Monoclonal Antibody, In Patients With Multicentric Castleman’s Disease. Blood. Nov 15 2013. 122(21):505.
- Uldrick TS, Polizzotto MN, Aleman K, O’Mahony D, Wyvill KM, Wang V, et al. High-dose zidovudine plus valganciclovir for Kaposi sarcoma herpesvirus-associated multicentric Castleman disease: a pilot study of virus-activated cytotoxic therapy. Blood. 2011 Jun 30. 117(26):6977-86.
- Sobas MA, Alonso Vence N, Diaz Arias J, Bendaña Lopez A, Fraga Rodriguez M, Bello Lopez JL. Efficacy of bortezomib in refractory form of multicentric Castleman disease associated to poems syndrome (MCD-POEMS variant). Ann Hematol. 2010 Feb. 89(2):217-9.
- Wang X, Ye S, Xiong C, Gao J, Xiao C, Xing X. Successful treatment with bortezomib and thalidomide for POEMS syndrome associated with multicentric mixed-type Castleman’s disease. Jpn J Clin Oncol. 2011 Oct. 41(10):1221-4.





{kind=link}