
What is a cochlear implant
A cochlear implant is also called a “bionic ear,” is an electronic medical device that restores partial hearing to individuals with severe to profound hearing loss who do not benefit from a conventional hearing aid 1. Even individuals with severe or profound “nerve deafness” may be able to benefit from cochlear implants. A cochlear implant device replaces the function of the damaged inner ear. A cochlear implant is surgically implanted in the inner ear (the cochlea) and activated by a device worn outside the ear called the speech or sound processor. Unlike a hearing aid, a cochlear implant does not make sound louder or clearer. Instead, the cochlear implant device bypasses damaged parts of the auditory system and directly stimulates the nerve of hearing in the cochlea to provide sound signals to the brain, allowing individuals who are profoundly hearing impaired to receive sound.
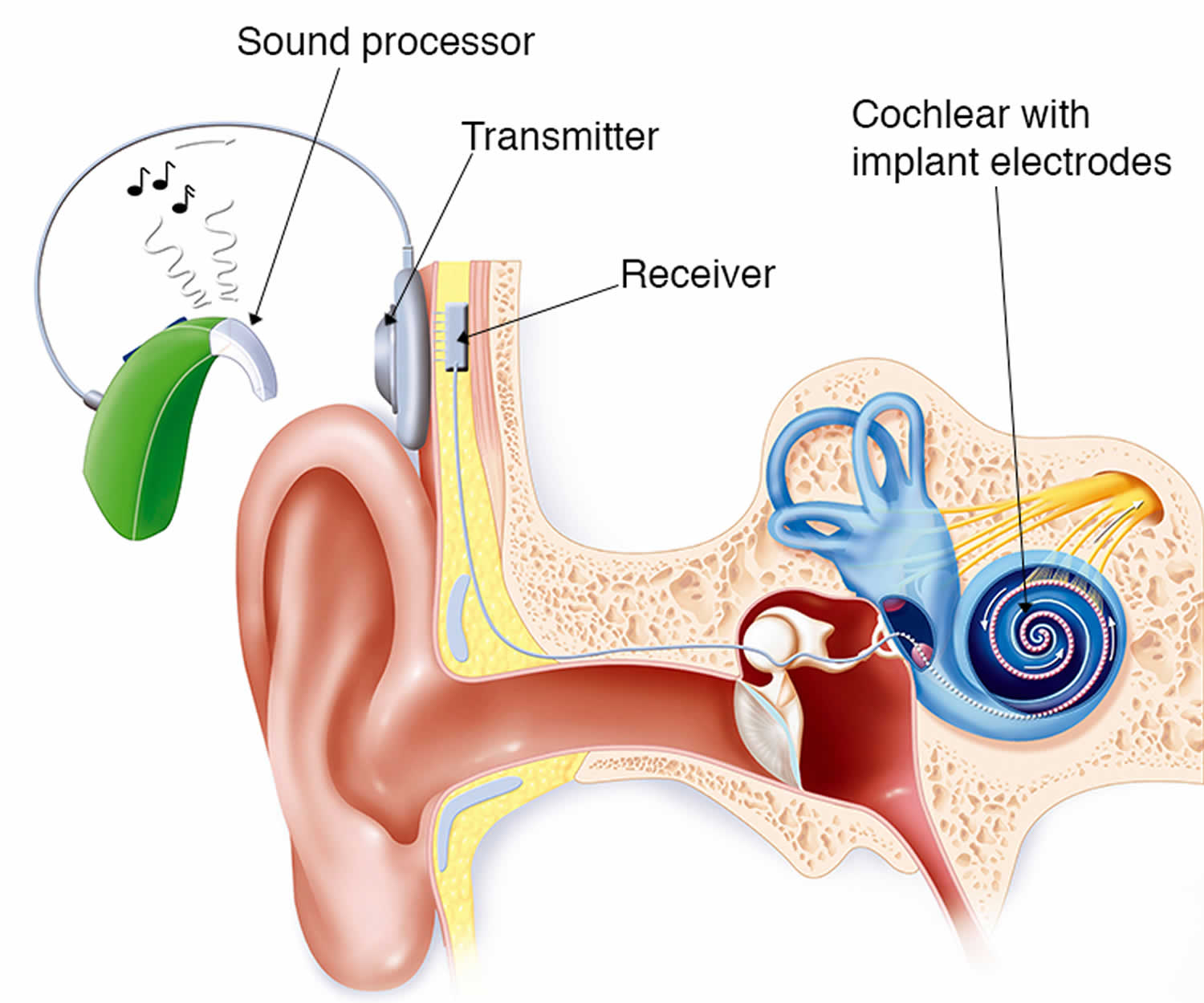
Cochlear implants usually consist of 2 main components:
- The externally worn microphone, sound processor and transmitter system.
- The implanted receiver and electrode system, which contains the electronic circuits that receive signals from the external system and send electrical currents to the inner ear.
Currently made cochlear implant devices have a magnet that holds the external system in place next to the implanted internal system. The external system may be worn entirely behind the ear or its parts may be worn in a pocket, belt pouch, or harness.
A cochlear implant works by receiving sound from the outside environment, processes it, and sends small electric currents near the auditory nerve (vestibulocochlear nerve or cranial nerve 8). These electric currents activate the auditory nerve, which then sends a signal to the brain. The brain learns to recognize this signal and the person experiences this as “hearing”.
The cochlear implant somewhat simulates natural hearing, where sound creates an electric current that stimulates the auditory nerve. However, the result is not the same as normal hearing.
The Food and Drug Administration (FDA) regulates cochlear implant devices for both adults and children and approves them only after thorough clinical investigation. You can search for FDA approved cochlear implants here: https://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ImplantsandProsthetics/CochlearImplants/ucm062882.htm
The first commercial cochlear implant devices were approved by the FDA in the mid-1980’s. However, research with this device began in the 1950’s.
- Cost of cochlear implants: More expensive than a hearing aid, the total cost of a cochlear implant, including evaluation, surgery, device, and rehabilitation can cost as much as $100,000. Fortunately, most insurance companies and Medicare provide benefits that cover the cost.
- Children and adults who are deaf or severely hard-of-hearing can be fitted for cochlear implants. As of December 2012, approximately 324,200 registered cochlear implant devices have been implanted worldwide. In the United States, roughly 58,000 cochlear implant devices have been implanted in adults and 38,000 in children.
Be sure to ask your otolaryngologists (ear, nose, and throat specialist) for written information, including brochures provided by the cochlear implant manufacturers. You need to be fully informed about the benefits and risks of cochlear implants, including how much is known about safety, reliability, and effectiveness of a device; how often you must come back to the clinic for checkups; and whether your insurance company pays for the procedure.
Inner ear anatomy
You rely on the inner ear, an intricate sensory organ, to hear and to maintain balance. The inner ear is a complex system of communicating chambers and tubes called a labyrinth. Each ear has two parts to the labyrinth—the bony (osseus) labyrinth and the membranous labyrinth (Figure 1). The bony labyrinth is a cavity within the temporal bone. The membranous labyrinth is a tube of similar shape that lies within the bony labyrinth. Between the bony and membranous labyrinths is a fluid called perilymph, which is secreted by cells in the wall of the bony labyrinth. The membranous labyrinth contains another fluid, called endolymph.
The parts of the labyrinths include three membranous semicircular ducts within three bony semicircular canals, and a cochlea. The semicircular canals and associated structures provide a sense of equilibrium (balance). The cochlea functions in hearing.
The cochlea has a bony core and a thin, bony shelf that extends out from the core and coils around it. The shelf divides the bony labyrinth of the cochlea into upper and lower compartments. The upper compartment, called the scala vestibuli, leads from the oval window to the tip of the cochlea. The lower compartment, the scala tympani, extends from the tip of the cochlea to a membrane-covered opening in the wall of the middle ear called the round window.
The part of the membranous labyrinth within the cochlea is called the cochlear duct. It lies between the two bony compartments and ends as a closed sac near the tip of the cochlea. The cochlear duct is separated from the scala vestibuli by a vestibular membrane (Reissner’s membrane) and from the scala tympani by a basilar membrane. The basilar membrane has many thousands of elastic fibers, allowing it to move in response to sound vibrations. Sound vibrations entering the perilymph at the oval window travel along the scala vestibuli and pass through the vestibular membrane and into the endolymph of the cochlear duct, where they move the basilar membrane.
After passing through the basilar membrane, the vibrations enter the perilymph of the scala tympani. Their forces are dissipated into the air in the tympanic cavity by movement of the membrane covering the round window.
The spiral organ (organ of Corti) contains the hearing receptors. It is located on the upper surface of the basilar membrane and stretches from the apex to the base of the cochlea. The receptor cells, called hair cells, are organized in rows and have many hairlike processes that project into the endolymph of the cochlear duct. Above these hair cells is a tectorial membrane attached to the bony shelf of the cochlea, passing over the receptor cells and contacting the tips of their hairs.
As sound vibrations move the basilar membrane, the hairs move back and forth against the tectorial membrane and the resulting mechanical deformation of the hairs stimulates the hair cells (Figure 3. The Cochlea). Hair cells at different locations along the length of the cochlear duct respond to different frequencies (pitch) of sound vibrations. This enables us to hear sounds of different pitch simultaneously.
Hair cells are epithelial but function somewhat like neurons. For example, when a hair cell is at rest, its membrane is polarized. When it is stimulated, selective ion channels open, depolarizing the membrane and making it more permeable to calcium ions. The hair cell has no axon or dendrites, but it has neurotransmitter-containing vesicles near its base. As calcium ions diffuse into the cell, some of these vesicles fuse with the cell membrane and release a neurotransmitter by exocytosis. The neurotransmitter stimulates the dendrites of nearby sensory neurons. In response these neurons send action potentials along the cochlear branch of the vestibulocochlear nerve to the auditory cortex of the temporal lobe of the brain.
The ear of a young person with normal hearing can detect sound waves with frequencies ranging from 20 to more than 20,000 vibrations per second. The range of greatest sensitivity is 2,000 to 3,000 vibrations per second. More-intense stimulation of the hair cells causes more action potentials per second to reach the auditory cortex, and we sense a louder sound.
Units called decibels (dB) measure sound intensity on a logarithmic scale. The decibel scale begins at 0 dB, which is the intensity of the sound that is least perceptible by a normal human ear. A sound of 10 dB is 10 times as intense as the least perceptible sound; a sound of 20 dB is 100 times as intense; and a sound of 30 dB is 1,000 times as intense. A whisper has an intensity of about 40 dB, normal conversation measures 60 to 70 dB, and heavy traffic produces about 80 dB. A sound of 120 dB, common at a rock concert, produces discomfort, and a sound of 140 dB, such as that emitted by a jet plane at takeoff, causes pain.
Frequent or prolonged exposure to sounds with intensities above 85 dB can damage hearing receptors and cause permanent hearing loss.
Auditory Pathways
The nerve fibers associated with hearing enter the auditory pathways, which pass into the auditory cortices of the temporal lobes of the cerebrum. Here they are interpreted. On the way, some of these fibers cross over, so that impulses arising from each ear are interpreted on both sides of the brain. Consequently, damage to a temporal lobe on one side of the brain does not necessarily cause complete hearing loss in the ear on that side.
Several factors cause partial or complete hearing loss. Interference with the transmission of vibrations to the inner ear is called conductive hearing loss. Conductive hearing loss may be due to plugging of the external acoustic meatus or to changes in the eardrum or auditory ossicles. For example, the eardrum may harden as a result of disease and become less responsive to sound waves, or disease or injury may tear or perforate the eardrum.
Damage to the cochlea, auditory nerve, or auditory pathways can cause sensorineural hearing loss. Loud sounds, tumors in the central nervous system, brain damage from vascular accidents, or use of certain drugs can also cause sensorineural hearing loss.
Steps in the Generation of Sensory Impulses from the Ear
- Sound waves enter external acoustic meatus.
- Sound waves cause eardrum to reproduce vibrations coming from sound source.
- Auditory ossicles amplify and transfer vibrations to end of stapes.
- Movement of stapes at oval window transfers vibrations to perilymph in scala vestibuli.
- Vibrations pass through vestibular membrane and enter endolymph of cochlear duct, where they move the basilar membrane.
- Different frequencies of vibration of basilar membrane stimulate different sets of receptor cells.
- As a receptor cell depolarizes, its membrane becomes more permeable to calcium ions.
- Inward diffusion of calcium ions causes vesicles at base of the receptor cell to release neurotransmitter.
- Neurotransmitter stimulates dendrites of nearby sensory neurons.
- Sensory impulses are triggered on fibers of the cochlear branch of vestibulocochlear nerve.
- Auditory cortices of temporal lobes interpret sensory impulses.
Figure 1. Inner ear anatomy

Figure 2. Parts of the inner ear
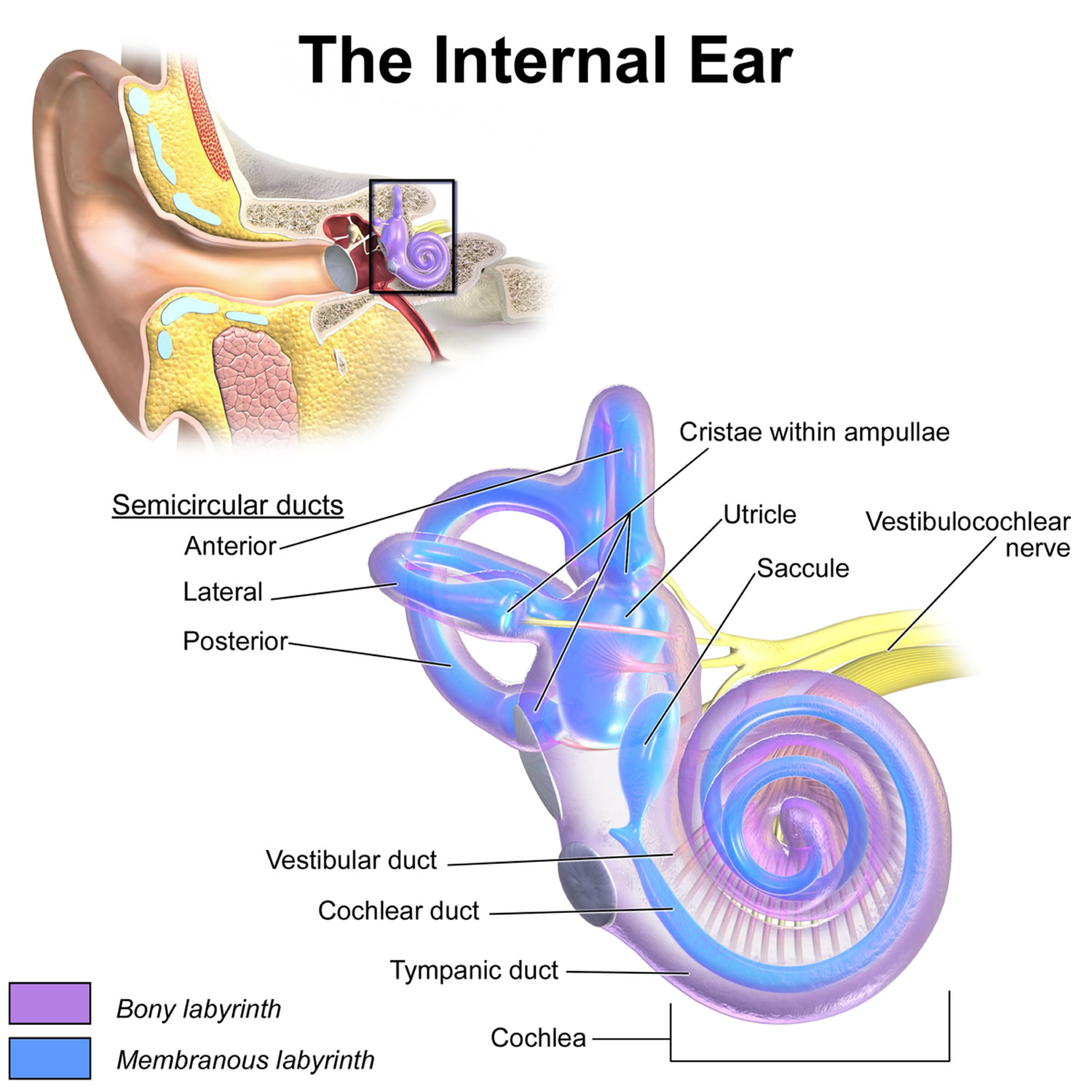
Note: A closer look at the inner ear. Perilymph separates the bony (osseous) labyrinth of the inner ear from the membranous labyrinth, which contains endolymph. Note that areas of bony labyrinth have been removed to reveal underlying structures.
Figure 3. The Cochlea (cross section view)
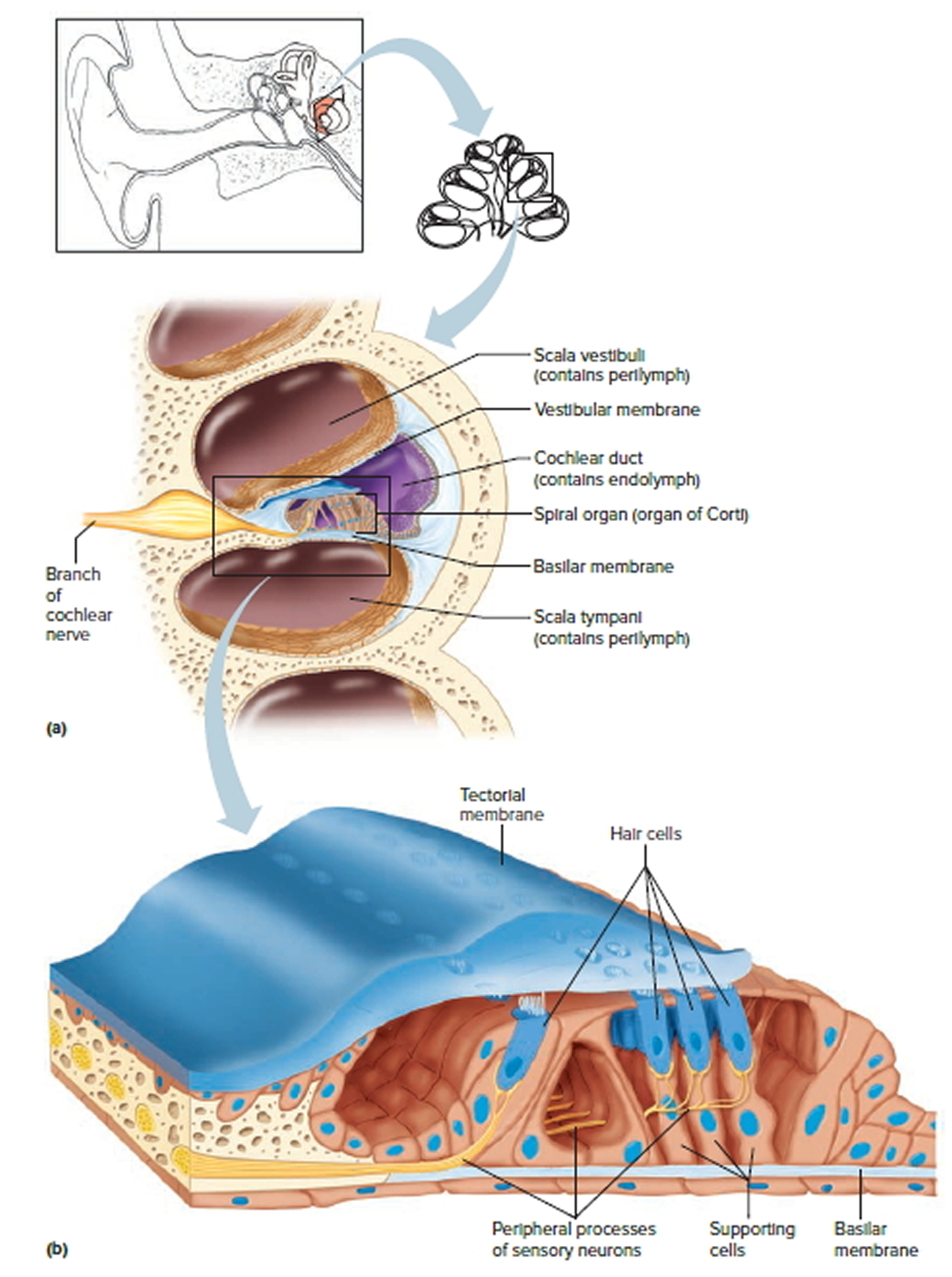
Note: a) Cross section of the cochlea. (b) The spiral organ and the tectorial membrane.
Figure 4. Cochlear implant
What is normal hearing?
Your ear consists of three parts that play a vital role in hearingthe external ear, middle ear, and inner ear.
Conductive hearing: Sound travels along the ear canal of the external ear, causing the ear drum to vibrate. Three small bones of the middle ear conduct this vibration from the eardrum to the cochlea (auditory chamber) of the inner ear.
Sensorineural hearing: When the three small bones move, they start waves of fluid in the cochlea, and these waves stimulate more than 16,000 delicate hearing cells (hair cells). As these hair cells move, they generate an electrical current in the auditory nerve. The electrical signal travels through inter-connections in the brain to specific areas of the brain that recognize it as sound.
How is hearing impaired?
Conductive Hearing Loss: A hearing loss is conductive when there is a problem with the ear canal, the eardrum, and/or the three bones connected to the eardrum. If you have disease or obstruction involving your ear canal, tympanic membrane (ear drum), or middle ear, your conductive hearing may be impaired. This causes a mechanical (conductive) blockage, preventing the full energy of the sound from reaching your inner ear. Two common reasons for this type of hearing loss are excess wax in the ear canal or fluid behind the eardrum. Medical treatment or surgery may be available for these and other forms of conductive hearing loss. Medical or surgical treatment can probably correct this or a hearing aid can be used in certain instances.
Sensorineural Hearing Loss: A hearing loss is sensorineural when it results from damage to the inner ear (cochlea) or auditory nerve, often a result of the aging process and/or noise exposure, but also may be secondary to head trauma, systemic illness or infection, or inheritance. Sounds may be unclear or too soft. Sensitivity to loud sounds may occur. Medical or surgical intervention cannot correct most sensorineural hearing losses, but hearing aids may help you reclaim some sounds you are missing as a result of nerve deafness. An inner ear problem, however, can result in a sensorineural impairment or nerve deafness. In most cases, the hair cells in the Cochlea are damaged and do not function. Although many auditory nerve fibers may be intact and can transmit electrical impulses to the brain, these nerve fibers are unresponsive because of hair cell damage inside the Cochlea. Since severe sensorineural hearing loss cannot be corrected with medicine, it can be treated only with a cochlear implant.
How does a cochlear implant work?
Cochlear implants bypass damaged hair cells in the Cochlea and convert speech and environmental sounds into electrical signals and send these signals to the hearing nerve – the vestibulocochlear nerve (cranial nerve VIII).
A cochlear implant has two main components:
- An internal component that consists of a small electronic device that is surgically implanted under the skin behind the ear, connected to electrodes that are inserted inside the cochlea.
- An external component, usually worn behind the ear, that consists of a speech processor, microphone, and battery compartment.
The microphone captures sound, allowing the speech processor to translate it into distinctive electrical signals. These signals or “codes” are transmitted across the skin via radio waves to the internal electronic stimulator. The internal stimulator then sends the signals to the implanted electrodes in the cochlea. The electrodes signals stimulate the auditory nerve fibers (vestibulocochlear nerve [cranial nerve VIII]) to send information to the brain, where it is interpreted as meaningful sound.
Why are there different kinds of cochlear implants?
Current thinking is that the inner ear responds to sound by at least two separate ways.
One theory, the place theory, says the cochlea responds greater to a simple tone at one place along its length. Another theory is that the ear responds to the timing of the sound.
Researchers, following the place theory, devised cochlear implants that separated the sound into groups. For example, they sent the lower pitches to the area of the cochlea where it seemed more responsive to lower pitches. And they sent higher pitches to the area more responsive to high pitches. Thus, they used several channels and electrodes spaced out inside the cochlea. Since there were also timing theories, researchers devised cochlear implants that made the sound signals into pulses to see if the cochlea would respond better to various kinds of pulses.
Most modern cochlear implants are versatile, in that they are somewhat capable of being adjusted to respond to sound in various ways. Audiologists try a variety of adjustments to see what works best with a particular patient.
What can I expect from a cochlear implant?
Most adult cochlear implant patients notice an immediate improvement in their communication skills. Children require time to benefit from their cochlear implant, as the brain needs to learn to correctly interpret the electrical sound input. While cochlear implants do not restore normal hearing, and benefits vary from one individual to another, most users find that cochlear implants help them communicate better through improved lip-reading. Also, 90 percent of adult cochlear implant patients are able to discriminate speech without the use of visual cues. There are many factors that contribute to the degree of benefit a user receives from a cochlear implant, including:
- How long a person has been deaf,
- The number of surviving auditory nerve fibers, and
- A patients motivation to learn to hear.
Your team will explain what you can reasonably expect. Before deciding whether your implant is working well, you need to understand clearly how much time you must commit. It is rare that patients do not benefit from a cochlear implant.
What determines the success of cochlear implants?
Many things determine the success of implantation. Some of them are:
- How long the patient has been deaf–as a group, patients who have been deaf for a short time do better than those who have been deaf a long time
- How old they were when they became deaf–whether they were deaf before they could speak
- How old they were when they got the cochlear implant–younger patients, as a group, do better than older patients who have been deaf for a long time
- How long they have used the implant
- How quickly they learn
- How good and dedicated their learning support structure is
- The health and structure of their cochlea–number of nerve (spiral ganglion) cells that they have
- Implanting variables, such as the depth and type of implanted electrode and signal processing technique
- Intelligence and communicativeness of patient
How can I help my child receive the most benefit from their cochlear implant?
- try to make hearing and listening as interesting and fun as possible
- encourage your child to make noises
- talk about things you do as you do them
- show your child that he or she can consciously use and evaluate the sounds he or she receives from his or her cochlear implant
- realize that the more committed you, your child’s teachers, and your health professionals are to helping your child, the more successful he or she will be.
What can I expect a cochlear implant to achieve in my child?
As a group, children are more adaptable and better able to learn than adults. Thus, they can benefit more from a cochlear implant. Significant hearing loss slows a child’s ability to learn to talk and affects overall language development. The vocal quality and intelligibility of speech from children using cochlear implants seems to be better than from children who only have acoustic hearing aids.
How important is the active cooperation of the patient?
Extremely important. The patient’s willingness to experience new acoustic sounds and cooperate in an auditory training program are critical to the degree of success with the implant. The duration and complexity of the training varies from patient to patient.
How is the external transmitter held in place correctly?
Usually, the transmitter and receiver contain magnets, which attract each other to stay aligned.
Can the sound processor be removed at night?
Yes. But you should turn it off to save the battery. Some users wear the sound processor all night so they can hear.
Can I use my cochlear implant while playing sports?
Probably. Most cochlear implants are durable enough to allow playing sports. However, the external parts of most are not waterproof, so you would have to remove them before swimming or other water sports. Deep water diving may harm the internal implant due to the high water pressure.
How long does it take me to get maximum benefit from a cochlear implant?
It depends a lot on you and your rehabilitation group. It depends on how long you have been without hearing. It depends on whether you could speak well before you lost your hearing. Usually, there is a rapid rise in your ability to interpret the sounds after receiving a cochlear implant. This rapid rise slows after about 3 months but continues.
What sounds can be heard with a cochlear implant?
You will probably hear most sounds of medium-to-high loudness. Patients often report that they can hear footsteps, slamming of doors, ringing telephones car engines, barking dogs, lawn mowers, and various other environmental sounds. You may hear some softer sounds too.
Will the cochlear implant help me control the loudness of my voice?
Yes. The cochlear implant usually helps the wearer control the loudness because you can hear your voice in relation to background sounds.
Do those who have a cochlear implant system use it?
Yes. Most people use their processors routinely from morning to night. Adults who have never been able to hear have the most difficult time learning spoken language and dealing with the sensation of hearing. Some of these adults may give up and stop using their cochlear implant.
Do insurance companies pay for cochlear implants?
Because cochlear implants are recognized as standard treatment for severe-to-profound nerve deafness, most insurance companies cover them. In 2004, Medicare, Medicaid, the Veteran’s Administration and other public health care plans cover cochlear implants. In 2004, more than 90 percent of all commercial health plans cover cochlear implants. Cochlear implant centers usually take the responsibility of obtaining prior authorization from the appropriate insurance company before proceeding with surgery.
Do I pay for the cochlear implant repairs?
Maybe. You will not have to pay for repairs if they are covered by a warranty or if you have insurance that covers repairs. Many health plans do not include specific benefits to cover repairs and replacement of parts for cochlear implants. However, the policy may have durable medical equipment (DME) benefits that can be applied. Read your benefits booklet for DME or prosthetic repair benefits, or check with the health plan.
My health plan has denied coverage for a cochlear implant. How can I appeal?
First, determine specifically why the cochlear implant was denied. Make sure you have the denial in writing. If you do not receive a written denial, ask for one. An appeal is most effective when structured in response to the specific reason for denial of coverage. If a specific denial reason is not provided, contact the plan and ask for clarification. Second, contact your cochlear implant center and advocacy groups and ask for help.
My health plan informs me that I have exhausted my rehabilitation benefits. How can I appeal this decision and obtain coverage for additional audiology or speech therapy services?
Many health plans have limited rehabilitation services. They have a predetermined cut-off point for post-operative cochlear implant services. However, you may be able to get extended medical benefits based on your need for more services by having your clinician argue your case. You may have an easier case if your child is the cochlear implant user. The manufacturer of your cochlear implant may help your clinician develop the case.
How can I insure my external parts against theft, damage or loss?
External parts, if purchased new, probably carry a warranty from the manufacturer against defects and materials. Usually, under such warranties, equipment lost, damaged beyond repair, or stolen will be replaced one time at no cost.
After the warranty expires, you may have some options, such as:
- buying a service contract from the implant manufacturer
- getting repair and replacement coverage through your health plan
- getting coverage through your personal home property and casualty or homeowner’s policy
What your teachers or educators need to know about your cochlear implant
- Cochlear implants do not make hearing normal.
- Benefit of an implant depends, in part, on the:
- type of communication training (total communication, auditory-oral communication, cued speech, etc.) a student used before the implant
- type of communication the student uses after the implant
- To get maximum benefit from a cochlear implant, a student will need individual training, such as:
- speech training
- lip reading training
- auditory training
- To progress with their classmates, students with cochlear implants may still need:
- special accommodation in the classroom
- preferential seating
- a note taker
- a quiet environment, away from air handlers and other noisy equipment
- a sign-language interpreter or cued speech interpreter
- Students need time to adjust and accommodate to their cochlear implants. The amount of time they need varies. During the accommodation period, students need language input from all sources they used before their implants.
- Educators should treat their students with cochlear implants as individuals, each having particular communication needs. Students don’t get equal benefits from cochlear implants.
- Students with cochlear implants may find it harder to:
- digest new and difficult subject matter
- interact in unfamiliar and complex social situations
- Educators should be aware that frequent changes to educational programs involving students with cochlear implants (program hopping) may impede learning.
- Educators can help their students in other ways to achieve full benefits from cochlear implants by:
- intervening early when there appears to be a problem
- promoting family counseling
- promoting specialized speech and language therapies
- explaining to families that speech and language are not the same thing, and that education is based on language development
- getting more information and support from local and national organizations of teachers of those with impaired hearing
- To assure that students with cochlear implants don’t fall behind their classmates, educators should frequently evaluate them and their educational settings.
- Particularly for their younger students, educators need to assure that external cochlear implant components are securely attached or removed during active school events. The components are expensive and are easily lost or damaged.
- Students will often need extra batteries, either new or recharged, for their implants to work.
- Students with cochlear implants are usually not able to interpret complex auditory signals, such as those in music.
Cochlear implant pros and cons
Cochlear implant benefits
Cochlear implants are designed only for individuals who attain almost no benefit from a hearing aid. They must be 12 months of age or older (unless childhood meningitis is responsible for deafness).
For people with cochlear implants 2:
- Hearing ranges from near normal ability to understand speech to no hearing benefit at all.
- Adults often benefit immediately and continue to improve for about 3 months after the initial tuning sessions. Then, although performance continues to improve, improvements are slower. Cochlear implant users’ performances may continue to improve for several years.
- Children may improve at a slower pace. A lot of training is needed after implantation to help the child use the new ‘hearing’ he or she now experiences.
- Most perceive loud, medium and soft sounds. People report that they can perceive different types of sounds, such as footsteps, slamming of doors, sounds of engines, ringing of the telephone, barking of dogs, whistling of the tea kettle, rustling of leaves, the sound of a light switch being switched on and off, and so on.
- Many understand speech without lip-reading. However, even if this is not possible, using the implant helps lip-reading.
- Many can make telephone calls and understand familiar voices over the telephone. Some good performers can make normal telephone calls and even understand an unfamiliar speaker. However, not all people who have implants are able to use the phone.
- Many can watch TV more easily, especially when they can also see the speaker’s face. However, listening to the radio is often more difficult as there are no visual cues available.
- Some can enjoy music. Some enjoy the sound of certain instruments (piano or guitar, for example) and certain voices. Others do not hear well enough to enjoy music.
Cochlear implant risks
General anesthesia risks
General anesthesia is drug-induced sleep. The drugs, such as anesthetic gases and injected drugs, may affect people differently. For most people, the risk of general anesthesia is very low. However, for some people with certain medical conditions, it is more risky.
Risks from the Cochlear Implant Surgical Procedure
- Injury to the facial nerve (cranial nerve VII) –this nerve goes through the middle ear to give movement to the muscles of the face. It lies close to where the surgeon needs to place the implant, and thus it can be injured during the surgery. An injury can cause a temporary or permanent weakening or full paralysis on the same side of the face as the implant.
- Meningitis –this is an infection of the lining of the surface of the brain. People who have abnormally formed inner ear structures appear to be at greater risk of this rare, but serious complication.
- Cerebrospinal fluid leakage –the brain is surrounded by fluid that may leak from a hole created in the inner ear or elsewhere from a hole in the covering of the brain as a result of the surgical procedure.
- Perilymph fluid leak –the inner ear or cochlea contains fluid. This fluid can leak through the hole that was created to place the implant.
- Infection of the skin wound.
- Blood or fluid collection at the site of surgery.
- Attacks of dizziness or vertigo.
- Tinnitus, which is a ringing or buzzing sound in the ear.
- Taste disturbances –the nerve that gives taste sensation to the tongue also goes through the middle ear and might be injured during the surgery.
- Numbness around the ear.
- Reparative granuloma –this is the result of localized inflammation that can occur if the body rejects the implant.
- There may be other unforeseen complications that could occur with long term implantation that we cannot now predict.
Risk of Bacterial Meningitis in Children with Cochlear Implants
In a 2002 study conducted by both the Centers for Disease Control and Prevention (CDC) and FDA found found that children with a cochlear implant with a positioner (a piece used in some cochlear implant models) were much more likely to get bacterial meningitis than children with other types of cochlear implants 3. The cochlear implant with a positioner was voluntarily taken off the market by the manufacturer in July 2002.
After the 2002 study was completed, the FDA continued to receive reports of bacterial meningitis in children with cochlear implants. Because of these new reports, CDC and the FDA updated the 2002 study by looking at reports that were received up to 2 years after the 2002 study ended. The purpose of this updated study was to find out if children with cochlear implants continued to be more likely to get bacterial meningitis than children of the same age group in the general population even after they had their implant in place for more than 2 years. The updated study found that even two years after implant surgery, children with cochlear implants with a positioner were at greater risk of developing bacterial meningitis than children in the general US population 4.
Recommendations from the CDC and FDA based on this study include 5:
- Children should be up-to-date on vaccines at least 2 weeks before having a cochlear implant if they are not already up-to-date on these vaccinations.
- Parents of children who have already received an implant should check with their child’s doctor to ensure that their child is up-to-date on all vaccinations.
- Doctors and other health care providers should review vaccination records of their patients who are cochlear implant recipients or candidates to ensure that they have received the recommended vaccinations based on the age-appropriate schedules for high risk people.
- Parents of children with cochlear implants should be watchful for possible signs and symptoms of meningitis and seek prompt attention for any bacterial infection their child might have. Any questions parents have about their child’s health should be discussed with the child’s doctor.
- Parents of children with cochlear implants should also be watchful for signs and symptoms of an ear infection, which can include ear pain, fever, and decreased appetite. Parents should seek prompt medical attention for these signs and symptoms.
- Parents should talk about the risks and benefits of cochlear implants with their child’s doctor and should discuss whether their child has certain medical conditions that might make him or her more likely to get meningitis.
Other Risks Associated with the Use of Cochlear Implants
People with a cochlear implant:
- May hear sounds differently. Sound impressions from an implant differ from normal hearing, according to people who could hear before they became deaf. At first, users describe the sound as “mechanical”, “technical”, or “synthetic”. This perception changes over time, and most users do not notice this artificial sound quality after a few weeks of cochlear implant use.
- May lose residual hearing. The implant may destroy any remaining hearing in the implanted ear.
- May have unknown and uncertain effects. The cochlear implant stimulates the nerves directly with electrical currents. Although this stimulation appears to be safe, the long term effect of these electrical currents on the nerves is unknown.
- May not hear as well as others who have had successful outcomes with their implants.
- May not be able to understand language well. There is no test a person can take before surgery that will predict how well he or she will understand language after surgery.
- May have to have it removed temporarily or permanently if an infection develops after the implant surgery. However, this is a rare complication.
- May have their implant fail. In this situation, a person with an implant would need to have additional surgery to resolve this problem and would be exposed to the risks of surgery again.
- May not be able to upgrade their implant when new external components become available. Implanted parts are usually compatible with improved external parts. That way, as advances in technology develop, one can upgrade his or her implant by changing only its external parts. In some cases, though, this won’t work and the implant will need changing.
- May not be able to have some medical examinations and treatments. These treatments include:
- MRI imaging. MRI is becoming a more routine diagnostic method for early detection of medical problems. Even being close to an MRI imaging unit will be dangerous because it may dislodge the implant or demagnetize its internal magnet. FDA has approved some implants, however, for some types of MRI studies done under controlled conditions.
- neurostimulation.
- electrical surgery.
- electroconvulsive therapy.
- ionic radiation therapy.
- Will depend on batteries for hearing. For some devices new or recharged batteries are needed every day.
- May damage their implant. Contact sports, automobile accidents, slips and falls, or other impacts near the ear can damage the implant. This may mean needing a new implant and more surgery. It is unknown whether a new implant would work as well as the old one.
- May find them expensive. Replacing damaged or lost parts may be expensive.
- Will have to use it for the rest of life. During a person’s lifetime, the manufacturer of the cochlear implant could go out of business. Whether a person will be able to get replacement parts or other customer service in the future is uncertain.
- May have lifestyle changes because their implant will interact with the electronic environment. An implant may
- set off theft detection systems
- set off metal detectors or other security systems
- be affected by cellular phone users or other radio transmitters
- have to be turned off during take offs and landings in aircraft
- interact in unpredictable ways with other computer systems
- Will have to be careful of static electricity. Static electricity may temporarily or permanently damage a cochlear implant. It may be good practice to remove the processor and headset before contact with static generating materials such as children’s plastic play equipment, TV screens, computer monitors, or synthetic fabric. For more details regarding how to deal with static electricity, contact the manufacturer or implant center.
- Have less ability to hear both soft sounds and loud sounds without changing the sensitivity of the implant. The sensitivity of normal hearing is adjusted continuously by the brain, but the design of cochlear implants requires that a person manually change sensitivity setting of the device as the sound environment changes.
- May develop irritation where the external part rubs on the skin and have to remove it for a while.
- Can’t let the external parts get wet. Damage from water may be expensive to repair and the person may be without hearing until the implant is repaired. Thus, the person will need to remove the external parts of the device when bathing, showering, swimming, or participating in water sports.
- May hear strange sounds caused by its interaction with magnetic fields, like those near airport passenger screening machines.
Cochlear implant surgery
What happens before cochlear implant surgery?
Otolaryngologists (ear, nose, and throat or ENT specialists) perform cochlear implant surgery, although not all of them do this procedure. Your local doctor can refer you to a cochlear implant clinic for an evaluation. The implant team (otolaryngologist, audiologist, nurse, and others) will determine your candidacy for a cochlear implant and review what you may expect as a result of the cochlear implant. The implant team will also conduct a series of tests, including:
Ear (otologic) evaluation: The otolaryngologist examines the ear canal and middle ear to ensure that no active infection or other abnormality precludes the implant surgery.
Physical examination: Your otolaryngologist also performs a physical examination to identify any potential problems with the use of general anesthesia needed for the implant procedure.
Hearing (audiologic) evaluation: The audiologist performs extensive hearing tests to find out how much you can hear with and without a hearing aid.
X-ray (radiographic) evaluation: Special X-rays are taken, usually computerized tomography (CT) or magnetic resonance imaging (MRI) scans, to evaluate your inner ear anatomy. The CT scan helps the doctor see if the cochlea has a normal shape. This scan is especially important if the patient has a history of meningitis because it helps see if there is new bone growth in the cochlea that could interfere with the insertion of the cochlear implant. This scan also may indicate which ear should be implanted.
What happens during cochlear implant surgery?
Cochlear implant surgery is usually performed as an outpatient procedure under general anesthesia. An incision is made behind the ear to open the mastoid bone leading to the middle ear space. Once the middle ear space is exposed, an opening is made in the cochlea and the implant electrodes are inserted. The electronic device at the base of the electrode array is then placed under the skin behind the ear.
What happens after cochlear implant surgery?
Immediately after waking, a patient may feel:
- pressure or discomfort over his (or her) implanted ear
- dizziness
- sick to the stomach (have nausea)
- disoriented or confused for a while
- a sore throat for a while from the breathing tube used during general anesthesia
Then, a patient can expect to:
- keep the bandages on for a while
- have the bandages be stained with some blood or fluid
- go home in about a day after surgery
- have stitches for a while
- get instructions about caring for the stitches, washing the head, showering, and general care and diet
- have an appointment in about a week to the stitches removed and have the implant site examined
- have the implant “turned on” (activated) about 3-6 weeks later
Several weeks after surgery, your cochlear implant team places the signal processor, microphone, and implant transmitter outside your ear and adjusts them. They teach you how to look after the system and how to listen to sound through the implant. There are many causes of hearing loss and some patients may take longer to fit and require more training due to individual differences. Your team will ask you to come back to the clinic for regular checkups and readjustment of the speech processor as needed.
Can a patient hear immediately after the operation?
No. Without the external transmitter part of the implant a patient cannot hear. The clinic will give the patient the external components about a month after the implant surgery in the first programming session.
Why is it necessary to wait 3 to 6 weeks after the operation before receiving the external transmitter and sound processor?
The waiting period provides time for the operative incision to heal completely. This usually takes 3 to 6 weeks. After the swelling is gone, your clinician can do the first fitting and programming.
What happens during the initial programming session?
An audiologist adjusts the sound processor to fit the implanted patient, tests the patient to ensure that the adjustments are correct, determines what sounds the patient hears, and gives information on the proper care and use of the device.
Is it beneficial if a family member participates in the training program?
Yes! A family member should be included in the training program whenever possible to provide assistance. The family member should know how to manage the operations of the sound processor.
Do patients have more than one implant?
Usually, patients have only one ear implanted, though a few patients have implants in both ears.
Cochlear implant vs hearing aid
Hearing aids can be useful in treating conductive deafness but are less beneficial for sensorineural hearing loss. They increase the intensity of airborne sounds and may modify the sound spectrum to suit the patient’s particular pattern of hearing loss at higher or lower frequencies. However, the receptor cell-neural pathway system must still be intact and functioning for the sound to be perceived, so hearing aids are useless in sensorineural hearing loss.
Hearing aids vary in price according to style, features, and local market prices. Price can range from hundreds of dollars to more than $2,500 for a programmable, digital hearing aid. Purchase price should not be the only consideration in buying a hearing aid. Product reliability and customer service can save repair costs and decrease frustration of a malfunctioning hearing aid.
There are many different types of hearing aid, including:
- Behind the ear hearing aids (the most common type) – hearing aids that go around the top and back of the ear
- In the ear hearing aids – small hearing aids that fit in the opening of the ear
- In the canal hearing aids – very small hearing aids that fit a bit further into the opening of the ear, so they’re just visible
- Completely in-the-canal – least visible hearing aids
- Open fit receiver-in-the-ear (RITE) hearing aids are a newer design, and while still placed over the ear, they are extremely small and nearly invisible.
The best hearing aid for you depends upon your particular hearing loss and listening needs, the size and shape of your ear and ear canal, and the dexterity of your hands. Many hearing aids have tele-coil “T” switches for telephone use and public sound systems.
Other options, such as FM systems and Bluetooth devices in conjunction with hearing aids, may provide the best benefit for some patients.
An audiologist can discuss with you the potential benefits of using a hearing aid, recommend a device and fit you with it.
Federal regulation prohibits any hearing aid sale unless the buyer has first received a physicians evaluation, so you will need to see your doctor before you purchase a hearing aid. However, the regulation also says that if you are over 18 and aware of the recommendation for a medical exam, you may sign a waiver to forego it.
An otolaryngologist, audiologist, or independent dispenser can dispense aids. Hearing aids should be custom-fit to your ear and hearing needs. Mail-order hearing aids typically cannot be custom-fit.
Will I need a hearing aid for each ear?
Usually, if you have hearing loss in both ears, using two hearing aids is best. Listening in a noisy environment is difficult with amplification in one ear only, and it is more difficult to distinguish where sounds are coming from.
Figure 5. Hearing aid styles

Note: Many choices of hearing aid styles are available, including the following: completely in the canal (A), in the canal (B), in the ear (C), behind the ear (D), receiver in canal or receiver in the ear (E), and open fit (F).
Bone anchored hearing aids
A bone anchored hearing aid may be an option if you have hearing loss caused by sound being unable to reach your inner ear.
This type of hearing aid is attached to your skull during a minor operation. It picks up sound and sends it to the inner ear by vibrating the bones near your ear.
It can be clipped on and off – for example, it’s removed at night and when you swim or take a shower. Some newer types are held onto the head with magnets instead of a connector through the skin.
Figure 6. Bone anchored hearing aid

Bone conduction hearing devices
Bone conduction hearing devices is becoming increasingly used instead of bone anchored hearing aids (BAHA) because of how the technology has improved over the years.
A bone conduction hearing device is an alternative to a regular hearing aid for those with problems in their outer or middle ears. It transfers sound by bone vibration directly to the cochlea, bypassing the outer and the middle ear. This means it is useful for conductive and mixed hearing losses. A bone conduction hearing device relies on a working cochlea to send sound to the brain.
A bone conduction hearing device may be considered when a conventional hearing aid cannot be worn, (for example due to irritated or collapsed ear canals), or when a hearing aid does not give effective benefit.
A bone conduction hearing device offers amplification without an ear mould in the ear. This makes them more comfortable if you experience discomfort or infections in your ear. Some people also report that they have a more natural sound than conventional hearing aids for the same reason. They do not restore your hearing to normal, but can make managing in everyday situations easier.
A bone conduction hearing device is compatible with hearing loop (telecoil) systems. You can select to pick up sound through the microphone, through the loop, or through a combination of both microphone and loop. This means you can take advantage of assistive listening devices, neckloops or switching to ‘T’ in places displaying the ‘T’ symbol. The bone conduction hearing device processor may have the telecoil feature integrated within it. Otherwise a telecoil accessory can be plugged into the processor when needed.
References- Cochlear Implants. https://www.entnet.org//content/cochlearimplants
- Benefits and Risks of Cochlear Implants. https://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ImplantsandProsthetics/CochlearImplants/ucm062843.htm
- Risk of Bacterial Meningitis in Children with Cochlear Implants. New England Journal of Medicine; July 31, 2003; Volume 349:435-445 https://www.nejm.org/doi/full/10.1056/NEJMoa031101
- Bacterial Meningitis Among Children With Cochlear Implants Beyond 24 Months After Implantation. Pediatrics; February 2006; Volume 117:2:284-289 http://pediatrics.aappublications.org/content/117/2/284.full
- Risk of Bacterial Meningitis in Children with Cochlear Implants. https://www.cdc.gov/ncbddd/hearingloss/meningitis.html





{kind=link}