
Glasgow Coma Scale
Glasgow Coma Scale or GCS is a neurological scale that aims to give a reliable, objective way of recording the general level of consciousness in patients with traumatic brain injury (TBI) and to to help gauge the severity of an acute brain injury 1. The Glasgow Coma Scale (GCS) is divided into 3 categories, eye opening (E), motor response (M), and verbal response (V). The Glasgow Coma Scale score is determined by the sum of the score in each of the 3 categories, with a maximum score of 15 and a minimum score of 3, as follows:
- Glasgow Coma Scale score = eye opening (E) + motor response (M) + verbal response (V)
Based on motor responsiveness, verbal performance, and eye opening to appropriate stimuli, the Glascow Coma Scale was designed and should be used to assess the depth and duration coma and impaired consciousness. Glasgow Coma Scale helps to gauge the impact of a wide variety of conditions such as acute brain damage due to traumatic and/or vascular injuries or infections, metabolic disorders (e.g., hepatic or renal failure, hypoglycemia, diabetic ketosis), etc. Education is necessary to the proper application of the Glasgow Coma Scale 2. The predictive value of the GCS, even when applied early, is limited 3. Despite these and other limitations 4, health care practitioners continue to use Glasgow Coma Scale widely.
Glasgow Coma Scale was initially used to assess level of consciousness after head injury, and the Glasgow Coma Scale is now used by first aid, emergency medical services, and doctors as being applicable to all acute medical and trauma patients. In hospitals it is also used in monitoring chronic patients in the intensive care. The Glasgow Coma Scale was published in 1974 by Graham Teasdale and Bryan J. Jennett, professors of neurosurgery at the University of Glasgow’s Institute of Neurological Sciences at the city’s Southern General Hospital 5.
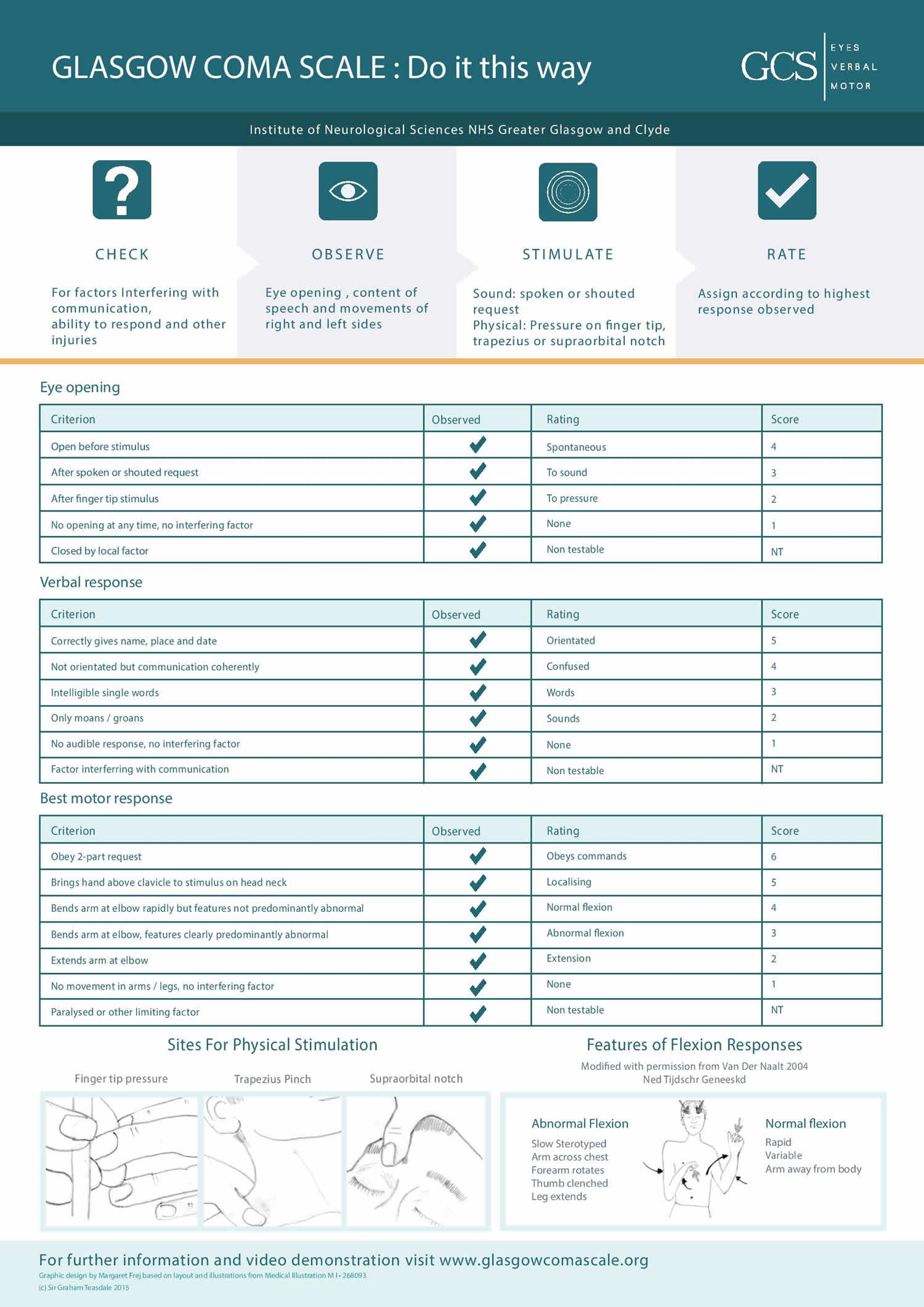
Eye Opening Response (E)
- Spontaneous–open with blinking at baseline = 4 points
- To verbal stimuli, command, speech = 3 points
- To pain only (not applied to face) = 2 points
- No response = 1 point
Verbal Response (V)
- Oriented conversation = 5 points
- Confused conversation, but able to answer questions = 4 points
- Inappropriate words = 3 points
- Incomprehensible speech or sounds = 2 points
- No response = 1 point
Motor Response (M)
- Obeys verbal commands for movement = 6 points
- Purposeful movement to painful stimuli = 5 points
- Withdraws in response to painful stimuli = 4 points
- Flexion in response to painful stimuli (decorticate posturing) = 3 points
- Extension response in response to painful stimuli (decerebrate posturing) = 2 points
- No response = 1 point
Total Glasgow Coma Scale score = 15
- Total Glasgow Coma Scale score 15 is Normal
- Total Glasgow Coma Scale score 3-14 is Abnormal
Glasgow Coma Scale and Children
The Glasgow Coma Scale has limited applicability to children, especially below the age of 36 months (where the verbal performance of even a healthy child would be expected to be poor). Consequently, the Pediatric Glasgow Coma Scale or PGCS, a separate yet closely related scale, was developed for assessing young children. The Pediatric Glasgow Coma Scale still uses the three tests — eye, verbal, and motor responses — and the three values are considered separately as well as together.
Pediatric brain injuries are classified by severity using the same scoring levels as adults, i.e. 8 or lower reflecting the most severe, 9-12 being a moderate injury and 13-15 indicating a mild traumatic brain injury (TBI). As in adults, moderate and severe injuries often result in significant long-term impairments.
Table 1. Pediatric Glasgow Coma Scale for Children
| Eye Opening | |||
| Score | Age 1 Year or Older | Age 0-1 Year | |
| 4 | Spontaneously | Spontaneously | |
| 3 | To verbal command | To shout | |
| 2 | To pain | To pain | |
| 1 | No response | No response | |
| Best Motor Response | |||
| Score | Age 1 Year or Older | Age 0-1 Year | |
| 6 | Obeys command | ||
| 5 | Localizes pain | Localizes pain | |
| 4 | Flexion withdrawal | Flexion withdrawal | |
| 3 | Flexion abnormal (decorticate) | Flexion abnormal (decorticate) | |
| 2 | Extension (decerebrate) | Extension (decerebrate) | |
| 1 | No response | No response | |
| Best Verbal Response | |||
| Score | Age >5 Years | Age 2-5 Years | Age 0-2 Years |
| 5 | Oriented and converses | Appropriate words | Cries appropriately |
| 4 | Disoriented and converses | Inappropriate words | Cries |
| 3 | Inappropriate words; cries | Screams | Inappropriate crying/screaming |
| 2 | Incomprehensible sounds | Grunts | Grunts |
| 1 | No response | No response | No response |
Glasgow coma scale interpretation
A patient’s Glasgow Coma Score (GCS) should be documented on a coma scale chart. This allows for improvement or deterioration in a patient’s condition to be quickly and clearly communicated. Individual elements, as well as the sum of the Glasgow Coma Scale score, are important. The individual elements of a patient’s GCS can be documented numerically (e.g. E2V4M6) as well as added together to give a total Coma Score (e.g E2V4M6 = 12). For example, the Glasgow Coma Scale score is expressed in the form “GCS 12 = E2 V4 M6 at 07:35”. Generally, when a patient is in a decline of their Glasgow Coma Scale score, the nurse or medical staff should assess the cranial nerves and determine which of the twelve have been affected.
Patients who are intubated are unable to speak, and their verbal score cannot be assessed. They are evaluated only based on eye opening and motor scores, and the suffix T is added to their score to indicate intubation. In intubated patients, the maximum Glasgow Coma Scale score is 10T and the minimum score is 2T. Tracheal intubation and severe facial/eye swelling or damage make it impossible to test the verbal and eye responses. In these circumstances, the score is given as 1 with a modifier attached e.g. “E1C” where “C” = closed, or “V1T” where T = tube. A composite might be “GCS 5TC”. This would mean, for example, eyes closed because of swelling = 1, intubated = 1, leaving a motor score of 3 for “abnormal flexion”. Often the 1 is left out, so the scale reads Ec or Vt.
The Glasgow Coma Scale is often used to help define the severity of traumatic brain injury (TBI). Mild head injuries are generally defined as those associated with a GCS score of 13-15, and moderate head injuries are those associated with a GCS score of 9-12. A GCS score of 8 or less defines a severe head injury. These definitions are not rigid and should be considered as a general guide to the level of injury.
Every brain injury is different, but generally, brain injury is classified as:
- Severe Head Injury: Glasgow Coma Score 8 or less
- Moderate Head Injury: Glasgow Coma Score 9-12
- Mild Head Injury: Glasgow Coma Score 13-15
Mild brain injuries can result in temporary or permanent neurological symptoms and neuroimaging tests such as CT scan or MRI may or may not show evidence of any damage.
Moderate and severe brain injuries often result in long-term impairments in cognition (thinking skills), physical skills, and/or emotional/behavioral functioning.
Brain injury is classified as:
- Glasgow Coma Scale 8-15 and somnolence: Sleepy, easy to wake
- Glasgow Coma Scale 8-15 and stupor: Hypnoid, hard to wake
- Glasgow Coma Scale 13-15: Mild Head Injury
- Glasgow Coma Scale 9–12: Moderate Head Injury
- Glasgow Coma Scale 3–8: Coma = No eye opening, no ability to follow commands and no word verbalizations
- Glasgow Coma Scale ≤ 8: Severe Head Injury
- Glasgow Coma Scale 7-8: Light coma; Coma Grade I
- Glasgow Coma Scale 5-6: Light coma; Coma Grade II
- Glasgow Coma Scale 4: Deep coma; Coma Grade III
- Glasgow Coma Scale 3: Deep coma; Coma Grade IV
Limitations of the Glasgow Coma Scale
Factors like drug use, alcohol intoxication, shock, or low blood oxygen can alter a patient’s level of consciousness. These factors could lead to an inaccurate score on the Glasgow Coma Scale.
References- Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975 Mar 1. 1(7905):480-4.
- Rowley G, Fielding K. Reliability and accuracy of the Glasgow Coma Scale with experienced and inexperienced users. Lancet 1991; 337:535-538
- Waxman K, Sundine MJ, Young RF. Is early prediction of outcome in severe head injury possible? Arch Surg 1991; 126:1237-1242
- Eisenberg HM. Outcome after head injury: Part I: general Considerations, in Becker DP, Povlishock JR (eds): Central Nervous System Trauma Status Report, 1985. Washington, DC: U.S. Government Printing Office, 1988:271-280
- Teasdale G, Jennett B. Assessment of coma and impaired conciousness: a practical scale. Lancet. 1974; 2:81-84.





{kind=link}