
What is the deltoid muscle
The deltoid muscle is a large triangular shaped muscle associated with the human shoulder girdle, explicitly located in the proximal upper arm. The shoulder girdle is composed of the following bony components:
- Proximal humerus
- Scapula – anatomic components of the scapula also include the glenoid, acromion, coracoid process
- Clavicle
The shoulder girdle musculature, in addition to the deltoid muscle itself, includes the following:
- Rotator cuff (supraspinatus, infraspinatus, teres minor, subscapularis)
- Trapezius and other periscapular stabilizing muscles
- Triceps
- Latissimus dorsi
- Pectoralis major/minor
The deltoid muscle fibers are separated into into three anatomical portions 1:
- Anterior (or clavicular fibers): the anterior deltoid muscle fibers take its origin from the lateral one-third of the clavicle as well as the anterior acromion
- Lateral (or acromial fibers): the lateral muscle fibers originate from the lateral margin of the acromion
- Posterior (or spinal fibers): the posterior deltoid muscle from the scapular spine.
The deltoid muscle origin attaches to the spine of the scapula and lateral third of the clavicle. This U-shaped origin point mirrors the insertion point for the trapezius muscle. It’s apex (or insertion) attaches to the lateral side of the body of the humerus, on a point known as the deltoid tuberosity 1.
The deltoid muscle’s function is testable in the clinical setting. It is done by manually raising the patient’s arm 15 degrees. After this, ask the patient to abduct the arm against resistance. In patients who have normal deltoid muscle function, the arm will contract, and the lateral deltoid muscle contraction will be appreciated via palpation. In patients who have a dysfunctional deltoid muscle, these clinical findings will not be present. A deltoid dysfunctional problem commonly arises due to axillary nerve palsy. Common causes of axillary nerve palsy include overuse of a crutch, surgery, or posterior shoulder dislocation from severe trauma.
The inability to abduct the arm does not specifically indicate that there is a dysfunction with the deltoid muscle. The inability to abduct the arm presents during proximal neuromuscular disorders. Neurological problems include Lambert Eaton disease 2. Muscular inflammatory processes polymyositis or dermatomyositis 3, polymyalgia rheumatica (stiffness rather than weakness), and as a side effect of aluminum hydroxide containing vaccines 4. These conditions could all present with proximal muscle weakness or with the inability to abduct the arm. Other differential diagnoses for patients with deltoid weakness include cachexia from chronic disease or malnourishment 5.
Deltoid muscle blood supply and lymphatics
The deltoid receives vascular supply from the thoracoacromial branch of the axillary artery. The thoracoacromial branch originates from the second part of the axillary artery which lies posterior to the pectoralis minor. The thoracoacromial artery contributes to the deltoid branches. It travels alongside the cephalic vein in the deltopectoral groove. The deltoid muscle also receives minor contributions from the posterior circumflex artery and the deltoid branches of the profunda brachii. Although the posterior circumflex artery is not the main supply, terminal branches cross the space between the deltoid and proximal humerus, making it vulnerable to bleeding or hematoma during an anterior approach surgery to the shoulder 6.
Lymphatic drainage of the deltoid is by the deltopectoral lymph nodes, which are located in the besides the cephalic vein within the deltopectoral groove.
Deltoid muscle nerve supply
The axillary nerve innervates the deltoid. Both C5 and C6 contribute to the axillary nerve. The axillary nerve originates from the posterior cord of the brachial plexus 7.
Figure 1. Deltoid muscle (front view)

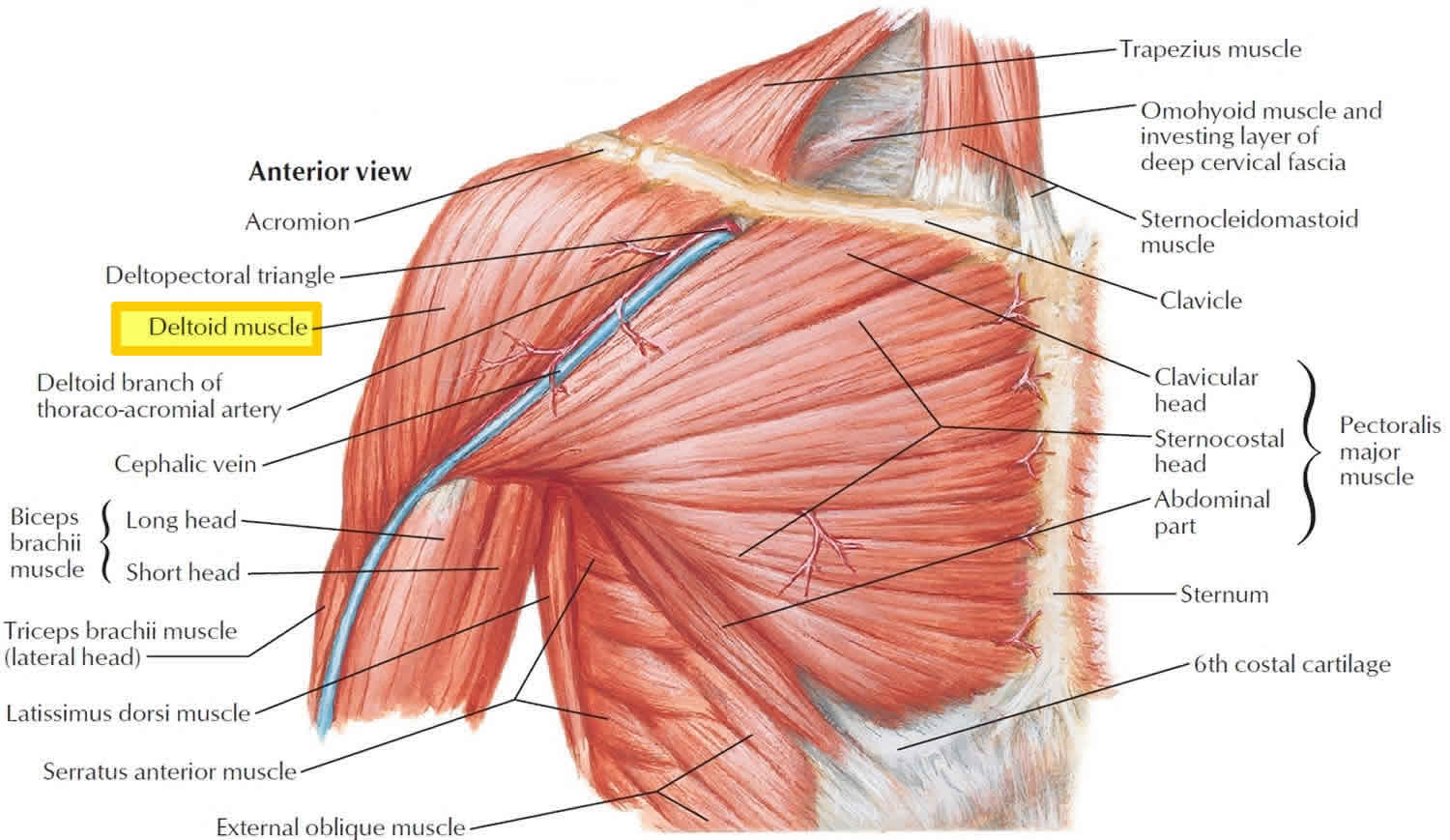
Figure 2. Deltoid muscle (back view)
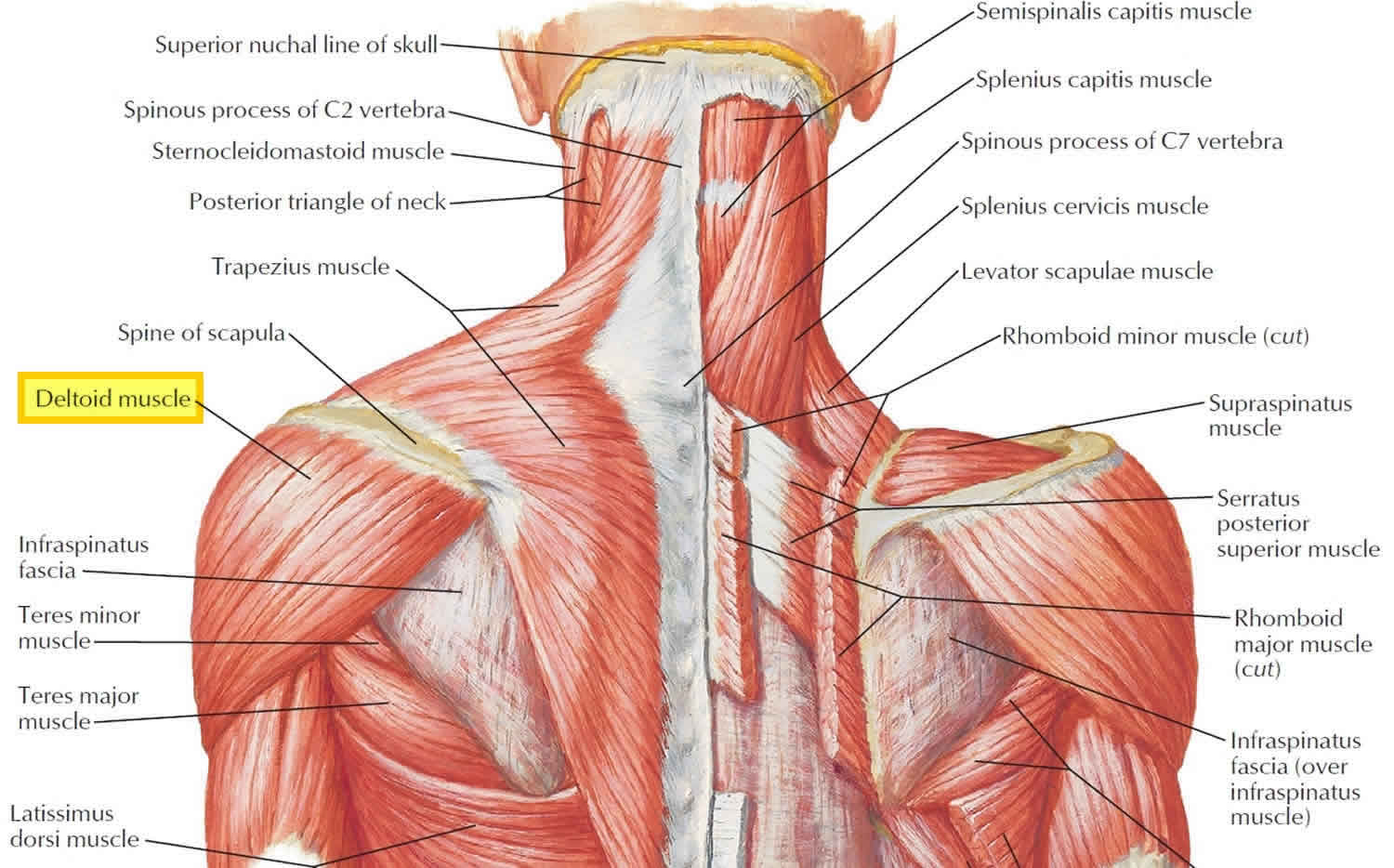
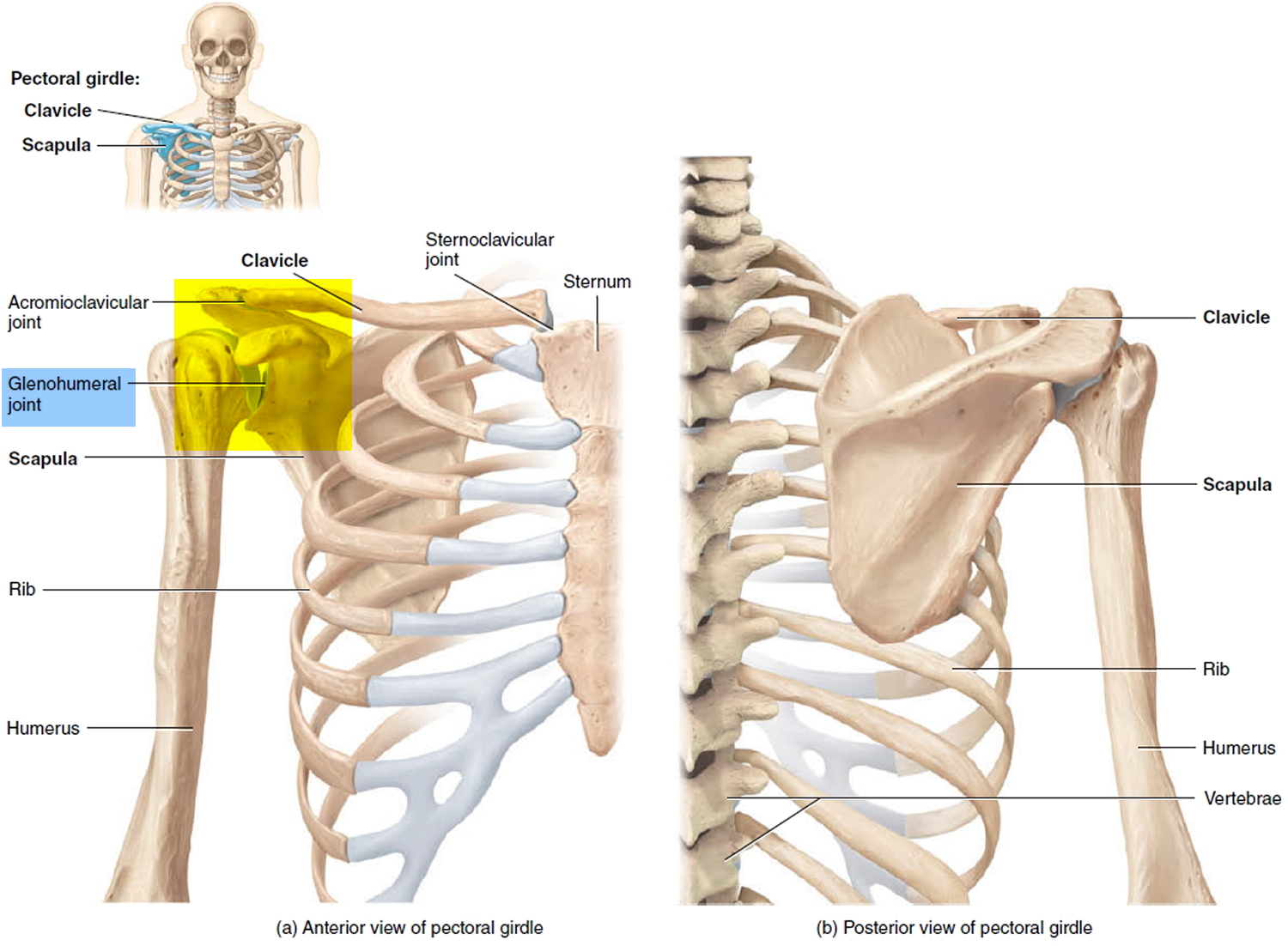
Figure 3. Shoulder girdle (pectoral girdle)
What is the action of the deltoid muscle
Deltoid muscle lateral fibers (acromial fibers) is the major abductor of the arm at shoulder joint (supraspinatus muscle assists deltoid muscle in abducting the arm beyond initial 15 degrees); anterior fibers (clavicular fibers) flex and medially rotate arm at shoulder joint; posterior fibers (spinal fibers) assist in extending and laterally rotate arm at shoulder joint. Muscles that work with the deltoid include the supraspinatus, infraspinatus, teres minor and the subscapularis. These muscles help initial abduction from 0 to 15 degrees, but also provide stabilization to the glenohumeral joint when the deltoid works to abduct past 15 degrees.
The deltoid muscle divides into three distinct parts (anterior, lateral, and posterior). When all three parts contracts simultaneously, the deltoid will assist in abducting the arm past 15 degrees 5. Deltoid muscle cannot initiate abduction because the direction of pull of the deltoid muscle is parallel to the axis of the humerus. Throughout abduction, the anterior and posterior parts of the deltoid play a significant role in stabilizing the arm while the lateral head assists in raising the arm from 15 to 100 degrees. Additional functions include ambulation. The anterior head of the deltoid works with pectoralis major to flex the arm when walking. This is in contrast to the posterior part of the deltoid which works with the latissimus dorsi to extend the arm during ambulation 8.
It is also noteworthy to discuss the stabilization functions that the deltoid muscle provides. While carrying large objects while the completely adducted (such as a dead-lift movement or carrying weights), the deltoid prevents inferior displacement of the glenohumeral joint. The deltoid muscle also provides compensatory force during abduction of the arm. In a 2018 study, shoulders that had a rotator cuff tear required as much as 108.1% of the normal 193.8 Newton deltoid muscle force to stabilize and abduct the arm 79.8 degrees 9.
References- Peterson SL, Rayan GM. Shoulder and upper arm muscle architecture. J Hand Surg Am. 2011 May;36(5):881-9.
- Todisco V, Cirillo G, Capuano R, d’Ambrosio A, Tedeschi G, Gallo A. Stimulated single-fiber electromyography (sSFEMG) in Lambert-Eaton syndrome. Clin Neurophysiol Pract. 2018;3:148-150.
- Kohara N, Kuzuhara S, Kaneko T, Yamanouchi H, Toyokura Y. [Two cases of post-poliomyelitis muscular atrophy]. Rinsho Shinkeigaku. 1989 Jul;29(7):919-23.
- Israeli E, Agmon-Levin N, Blank M, Shoenfeld Y. Macrophagic myofaciitis a vaccine (alum) autoimmune-related disease. Clin Rev Allergy Immunol. 2011 Oct;41(2):163-8.
- Elzanie A, Varacallo M. Anatomy, Shoulder and Upper Limb, Deltoid Muscle. [Updated 2018 Dec 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537056
- Smith CD, Booker SJ, Uppal HS, Kitson J, Bunker TD. Anatomy of the terminal branch of the posterior circumflex humeral artery: relevance to the deltopectoral approach to the shoulder. Bone Joint J. 2016 Oct;98-B(10):1395-1398.
- Gadea F, Bouju Y, Berhouet J, Bacle G, Favard L. Deltopectoral approach for shoulder arthroplasty: anatomic basis. Int Orthop. 2015 Feb;39(2):215-25
- Klarner T, Barss TS, Sun Y, Kaupp C, Zehr EP. Preservation of common rhythmic locomotor control despite weakened supraspinal regulation after stroke. Front Integr Neurosci. 2014;8:95.
- Dyrna F, Kumar NS, Obopilwe E, Scheiderer B, Comer B, Nowak M, Romeo AA, Mazzocca AD, Beitzel K. Relationship Between Deltoid and Rotator Cuff Muscles During Dynamic Shoulder Abduction: A Biomechanical Study of Rotator Cuff Tear Progression. Am J Sports Med. 2018 Jul;46(8):1919-1926.





{kind=link}