
Ear hair removal
There are many reasons why men and women choose to remove unwanted body hair. Excess ear hair may be undesirable and in many instances cause embarrassment and low self esteem.
Ear hairs that can be found in and around the ear fall into two different categories:
- Vellus hair – tiny, short, thin, and almost invisible that grow in most places on the human body. At the ear, they are present in the very outer portion of the ear canal in the outer cartilaginous area or on the pinna itself. The density varies among individuals. When short, it is often referred to as “peach fuzz.” Strands are usually short (less than 2 mm), and the follicle is not connected to a sebaceous gland 1. Vellus hair is mostly non-pigmented. However, during and after puberty, dihyrotestosterone (DHT) present in the body causes vellus hairs on the arms, legs, faces, and in other parts of the body to grow thicker and darker, into “terminal” hair – to a greater extent in men than women 2. With aging, the normal growth cycles of hair (growth, resting, and falling out phases) get out of whack, and as a result, some hairs grow longer before they are shed.
- Tragi hairs – larger/thicker stiff terminal. They take their name from Latin (tragos ‘goat’) with reference to the characteristic tuft of hair that is often present, likened to a goat’s beard. These can be prominent in the outer portion of the ear canal, on the tragus, antitragus, and in extreme cases over the helix (Figure 1). Tragi hairs can be numerous in some people and also very prominent. This condition is more often found in men than women. In some extreme cases, the ear hair can be quite long, recorded as being 5.2 inches by the Guinness World Records in 2003 (Figure 2) for Radhakant Baijpai. Since then, the 64 year-old (in 2015) grocer’s ear hair has continued to grow, being almost 10 inches long in 2009. He said that he has no intention to cut it, having been growing since he was 18 years old.
Ear hair is generally identified as the terminal hair developing from the follicles inside the ear canal. However, in its broader sense, ear hair may include the fine vellus hair covering much of the ear (particularly at the prominent parts of the anterior ear), as well as the terminal, or tragi hair.
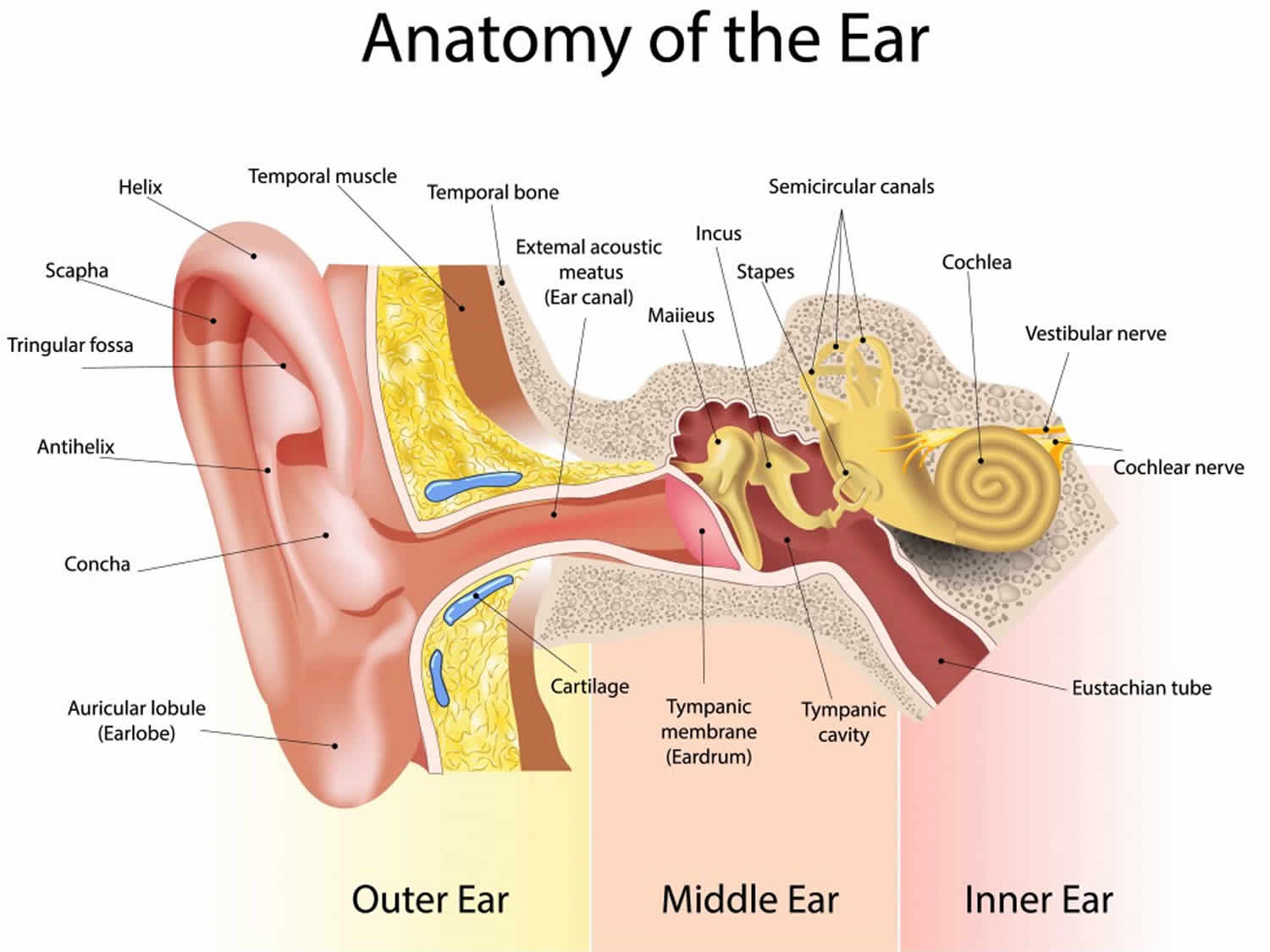
Hair growth within the ear canal itself is limited to the cartilaginous ear canal – roughly the outer 1/3 of the ear canal (Figure 3). The inner 2/3 of the ear canal, called the bony ear canal, does not have sufficient dermis and hypodermis underlying the epidermis to support the hair root in the hair follicle. Therefore, ear hair is not found in the deeper (bony) structure of the ear canal. Hair growth within the outer portion of the ear canal seems to increase and become stiffer as men age (along with an increase in nasal hair growth).
A more traditional length and location of tragi (terminal) hair just inside the ear canal opening.
Ear hair serves a protective function by filtering dust from the air and also acts to impede the entry of insects and other debris. It has been reported as well that heavy growth may prevent hearing aids from making a good seal, when needed (the topic of an upcoming post). Heavy tragi hair can sometimes create problems when making ear impressions, and often “barbering” is required because certain ear impression materials might allow the hairs to become embedded into the ear impression, potentially causing some discomfort when removing the ear impression with hair attached.
Some medical indications for hair removal include:
- Hirsutism. Hirsutism is excessive growth of “male” pattern hair that appear on the face, back, chest, abdomen, and thighs in women. Hirsutism is common and is usually a sign of an underlying endocrine disorder, most commonly, polycystic ovary syndrome (PCOS). In women with PCOS, weight gain probably contributes to its development or worsening. There are available treatments that can help decrease and slow hair growth to improve overall quality of life.
- Hypertrichosis (congenital or acquired). Hypertrichosis is excessive hair growth over and above the normal for the age, sex and race of an individual. Hypertrichosis can develop all over the body or can be isolated to small patches. Hypertrichosis may be congenital (present at birth) or acquired (arises later in life). The cause of hypertrichosis is unknown. Congenital hypertrichosis is believed to be a genetic disorder that is inherited or occurs as a result of spontaneous mutation. Acquired hypertrichosis lanuginosa sometimes occurs in people who at a later stage are diagnosed with a cancer of some form. This hair growth, also known as malignant down, is often confined to the face with long fine silky hair noticeable on the nose and eyelids, sites that are normally hairless. It is not known why a cancer causes this excessive hair growth.
There are basically 3 types of hair removal methods:
- Temporary hair removal,
- Temporary hair reduction
- Permanent hair removal.
Within each method a number of different techniques are used to achieve hair removal or reduction.
Figure 1. Ear hairs

Figure 2. Ear hair longest in the world
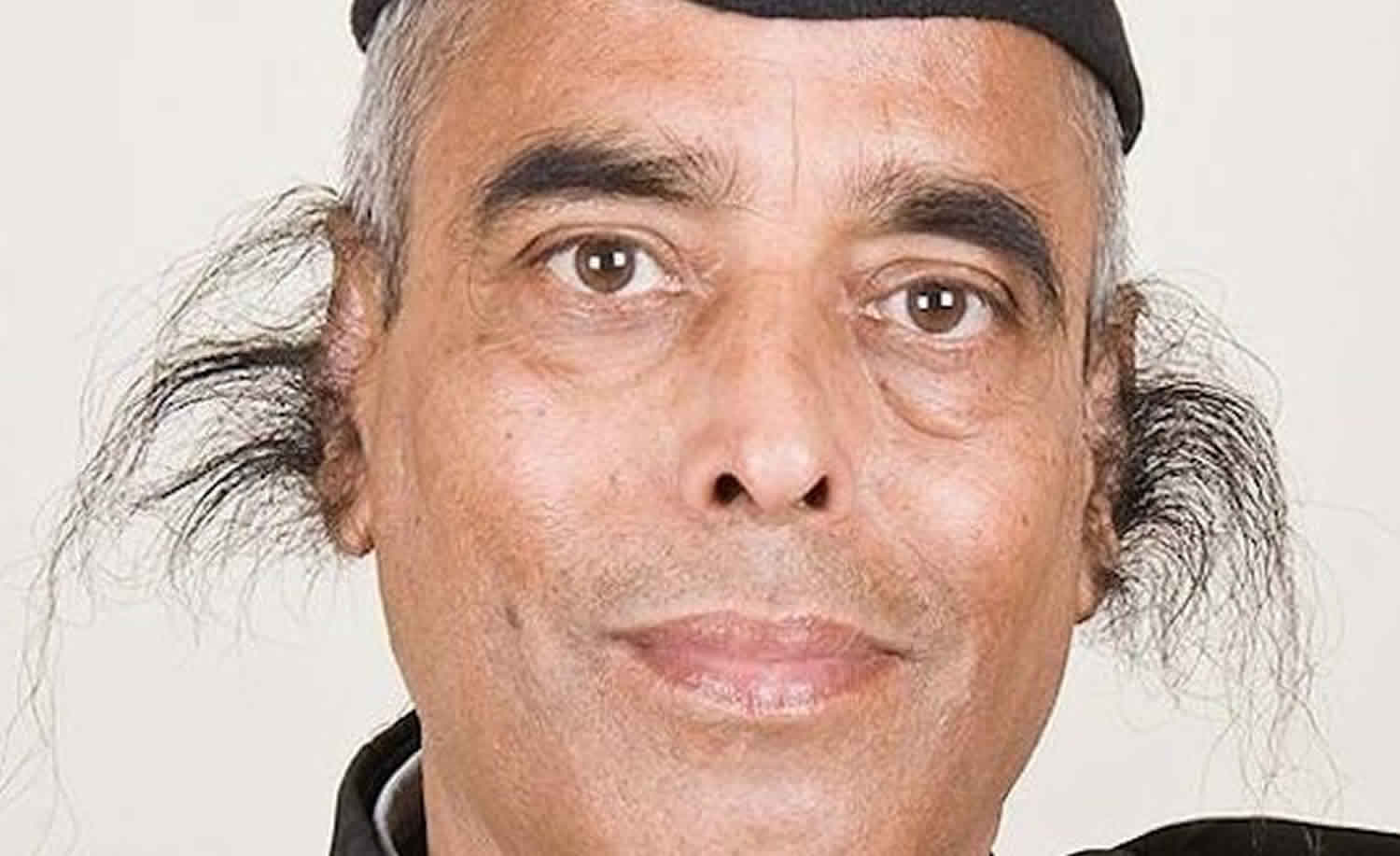
Figure 3. Ear anatomy
Temporary hair removal techniques
- Shaving. Shaving is most probably one of the oldest and most common methods of removing unwanted hair in both large and small areas. Shaving removes hair by using a razor or any other sharp bladed tool to slice the hair off at skin level. It is the method used by most men to remove facial hair on a regular, if not daily basis as part of their morning grooming. In women, shaving is the most common method used for removing hair from the underarms, legs and pubic area. The myth that shaving causes your hair to grow back thicker is not true. It may appear that hair grows back thicker but this is because the tip of the hair now has a blunt edge after being cut and as it starts to grow above the surface of the skin it not only feels stiffer but looks thicker too. Compare this to an unshaven hair where the tip has a tapered or beveled edge which makes it softer and lighter.
- Chemical depilation. Depilatory creams typically contain calcium thioglycolate and barium sulfate and are effective though they may irritate the skin.
- Epilation. Epilation is the term used to describe removal of body hair, including the hair root, by means of mechanical device, tweezer, or wax. It is the most effective method for temporarily removing hair.
- Waxing. Waxing is the most effective method of epilation because it removes hair completely from the hair shaft from below the skin’s surface in large quantities. Waxing is one of the most effective methods for temporary hair removal. It is unknown what the long-term effects of repeated waxing have on hair growth but the repeated damage to the hair follicles may result in permanent reduction of unwanted hair. Caution needs to be exercised in people using oral retinoids (isotretinoin and acitretin). Waxing should not be performed until treatment with these medications has been stopped for at least 6 months to 1 year. Waxing whilst taking these medications may cause tearing of the skin and possible scarring. Individuals using topical retinoids (e.g. Retin A®) should stop the medication 3-4 weeks prior to waxing to avoid skin injury and soreness. Waxing should not be performed on skin that is irritated, sunburned or broken.
- Plucking. Plucking is performed using hand-held or electrical tweezers. Hand-held tweezers are best used for removing the occasional coarse hair or a small group of hairs, such as those found on the eyebrows, chin or nipples. Electrical tweezers including the Epilady® range of products are designed to remove unwanted hair from both small and large areas. Some of these products are dual action epilators and both pluck and shave at the same time.
- Threading. Threading is an ancient method of hair removal. The technique involves a long loop of cotton thread that is twisted and rolled along the surface of the skin. Hair is caught within the entwined coils and pulled from their roots as the thread rolls along. It is used to give clean lines and is good for shaping eyebrows and removing hair from the upper lip and other facial areas. It is considered to be less painful than plucking, waxing and sugaring. To women in the Middle East and India it is a basic skill learnt from an early age. It is also available in most Western countries.
- Abrasives. Abrasives work by physically rubbing away hair form the skin surface. Abrasives used include pumice stones and devices or gloves made from fine sandpaper. This method is irritating to the skin and is seldom used these days.
- Sugaring. Sugaring is similar to waxing but instead of using wax a sugar mixture is used. The sugar mixture is made up of sugar, lemon juice and water heated together to form a paste. Like waxing, a thin layer of sugar paste is applied to the skin and a cotton strip placed on top. The strip is then pulled back sharply against the direction of the hair growth. Sugaring is a suitable alternative to waxing for people sensitive to wax.
Temporary hair reduction techniques
- Eflornithine HCl cream. Eflornithine works by blocking the enzyme ornithine decarboxylase that stimulates hair growth. Eflornithine HCl cream 13.9% has been shown to slow the rate of hair growth in animal and human studies. Studies with eflornithine cream have been limited to treating unwanted hair on the face, around the lips and chin. Eflornithine HCl cream slows the rate of hair growth and is often used in combination with other hair removal techniques to maintain a hair-free complexion. In two double-blind placebo controlled trials, 35% of patients treated with eflornithine cream show significant improvement after 24 weeks of treatment compared with 9% of patients treated with placebo. Differences between the treatment and placebo groups could be seen as early on as 4 weeks after starting treatment in some patients, whilst in other patients, differences were not apparent until after 8 weeks of treatment. It appears that the longer eflornithine is used, the better it works. Over time the need for additional hair removal techniques to maintain a hair-free complexion may reduce. However, the treatment is not effective for everyone.
- Laser-assisted. The Nd:Yag laser, Alexandrite laser, and diode laser are the most efficacious hair removal lasers 3, 4, 5.
- Intense pulsed light sources.
Permanent hair removal techniques
Electrolysis and laser hair epilation are the only hair removal methods that may provide a permanent result.
- Electrolysis. Electrolysis involves the insertion of a small fine needle into the hair follicle, followed by a small electrical current that damages and eventually destroys the hair follicle. There are 3 different methods (modalities) to achieve this:
- Galvanic electrolysis: Galvanic electrolysis uses direct current electrolysis, which means a direct electric current is passed down a needle into the hair follicle where it creates a chemical reaction. This reaction converts tissue saline into sodium hydroxide, a caustic agent that then destroys the hair bulb.
- Thermolysis: Thermolysis uses a high frequency alternating current that is passed down through the needle to the hair follicle. The high frequency causes vibration in the cells of the hair follicle to produce enough heat to cauterize the hair bulb.
- Blend method: Blend method combines both the galvanic and thermolysis modalities.
No clinical trials have been carried out to compare the methods and any claims of one method being more effective over the other is based on anecdotal evidence only.
Electrolysis
Effectiveness of electrolysis is dependent on the skill of the technician (electrologist) performing the procedure. Proper electrolysis requires accurate needle insertion technique and use of appropriate intensity and duration of current. The technician, based on the patient’s pain threshold, sets the intensity measured in milliamps, and the duration of the current is controlled by how long the technician presses down on the hand or foot pedal. A common estimate of effectiveness is that 25% of treated hair don’t regrow.
Electrolysis is a very slow method of hair removal that may also be prolonged by having to do repeat insertions into the hair follicle. It may take a minute or more to remove each hair using galvanic electrolysis.
The amount of pain experienced during the procedure is dependent on the individual’s pain threshold. Topical anesthetic creams applied one hour before the procedure may help to reduce discomfort. However, it is desirable to maintain some sensation as the pain is related to the amount of damage to the hair follicle.
Who is suitable for electrolysis?
Almost anyone wanting to remove unwanted hair is a candidate for electrolysis. For men and women electrolysis is usually a safe and permanent process of hair removal. However, it is should not be used for patients with pacemakers because it can interrupt the electronics to cause potentially dangerous heart rhythms.
Electrolysis complications
Some degree of redness about treated hair follicles for a few days is not uncommon.
Potential risks of electrolysis include scarring and increased or reduced pigmentation i.e. brown or white marks.
Secondary local infection with bacteria (impetigo) or reactivation of herpes simplex are also possible complications.
Lasers
Lasers can be used to remove excessive and cosmetically disabling hair due to hypertrichosis or hirsutism. Laser treatments remove dark hair quickly, and it may take 3 to 6 months before regrowth is evident. Several treatment cycles are required with the spacing between treatments depends on the body area being treated. Laser treatments are less painful and much quicker than electrolysis. Complications are rare but superficial burns, pigmentary changes and even scarring may occur. Increased growth of fine dark hair in untreated areas close to the treated ones has been reported. Both increased and reduced localised sweating have been reported after treatment.
Suitable devices include long-pulsed ruby and alexandrite lasers, a diode (810nm), millisecond Nd:YAG and non-laser intense pulsed light.
References- Marks, James G; Miller, Jeffery (2006). Lookingbill and Marks’ Principles of Dermatology (4th ed.). Elsevier Inc.
- Jackson, Scott; Nesbitt, Lee T. (April 25, 2012). Differential Diagnosis for the Dermatologist. Springer Science & Business Media.
- Goldberg DJ. One-year follow-up results of hair removal using an 810 nm diode laser. J Cosmet Dermatol. 2018 Oct;17(5):775-778.
- Nistico SP, Del Duca E, Farnetani F, Guida S, Pellacani G, Rajabi-Estarabadi A, Nouri K. Removal of unwanted hair: efficacy, tolerability, and safety of long-pulsed 755-nm alexandrite laser equipped with a sapphire handpiece. Lasers Med Sci. 2018 Sep;33(7):1479-1483.
- Shokeir H, Samy N, Mahmoud H, Elsaie ML. Evaluation of Topical Capislow Extract and Long Pulsed Nd-YAG Laser in the Treatment of Idiopathic Hirsutism. J Lasers Med Sci. 2018 Spring;9(2):128-133.





{kind=link}