
Funnel web spider bite
Funnel web spiders are the most venomous in the world and envenomation should be considered a life threatening emergency. Funnel web spider bite is a medical emergency; a pressure immobilisation bandage should be applied and the patient transferred to a hospital with available antivenom and resuscitation facilities 1. Funnel-web spiders are found in eastern seaboard of Australia, around Sydney, including parts of southern Queensland, South Australia and Tasmania. Funnel-web spiders are not native to the United States, although some people may keep them as exotic pets. There are over 40 species of funnel-web spiders, with 3 genera restricted to Australia, including the Hadronyche, Illawarra, and the Atrax 2. Of all Australian spiders, one species of the Atrax genera, the Atrax robustus also known as the Sydney funnel-web spider, is unquestionably the most dangerous spider in Australia and is implicated in the most human fatalities; however tree-dwelling funnel webs (Hadronyche cerberea and Hadronyche formidabilis) have the highest envenoming rates (75%), while the Sydney funnel web, Atrax robustus, accounted for only 17% (or 1% of all spider bites) 3. Funnel-web spider antivenom appears effective and safe; severe allergic reactions are uncommon.
Isbister et al 4 observed the following clinical effects of funnel web spider envenomation:
- autonomic – excessive sweating (diaphoresis) (78%), hypersalivation (44%) and goose bumps (piloerection) (12%)
- cardiovascular – hypertension (75%) and fast heart rate (tachycardia) (59%), slow heart rate (bradycardia) and hypotension (less commonly – both 10%)
- neurological – fasciculations (54%) and oral pins-and-needles sensation (paraesthesia) (17%)
- noncardiogenic pulmonary edema (54%), more common in children than adults (70% compared to 44%)
- other – agitation (47%), vomiting (41%), headache (10%).
Children may deteriorate rapidly and death may result in 1–2 hours if left untreated 5. In adults, untreated envenomation may result in death from progressive, irreversible hypotension, or possibly raised intracranial pressure resulting from cerebral edema 5.
Despite its fearsome reputation, there are only 14 recorded deaths due to funnel web spider bite, and experience has shown that many bites do not result in significant envenoming. However, when the spider does inject a dangerous quantity of venom, the effects can be rapid and severe, and death within an hour may occur. The bite is usually painful, both due to large fangs and acidic venom and the spider is usually seen. If envenoming occurs, it will develop early, starting with tingling around the lips, twitching of the tongue, then profuse salivation, lachrymation, sweating, piloerection and muscle twitching/spasms. Hypertension and tachycardia occur, and respiratory distress due to rapid development of pulmonary edema, which may be very severe and potentially lethal. In the early stages it may be mistaken for organo-phosphate poisoning. Convulsions may occur.
While the causative venom is multicomponent, the key neurotoxins are called delta-atracotoxins (delta-ACTXs) are considered to be the principal component responsible for severe envenoming in humans. Delta-atracotoxins act by slowing sodium current inactivation resulting in spontaneous repetitive firing of action potentials. This triggers the release of excessive and eventual exhaustion of predominantly sympathetic neurotransmitters leading to the characteristic biphasic clinical syndrome 6. It is interesting to note that most mammals are relatively unaffected by funnel web spider venom, but humans are very sensitive.
Since the introduction of funnel web spider antivenom in 1980, there have been no deaths reported and time required in hospital has dramatically decreased from an average of 14 days 7 to less than 2 days 8. Moreover, the antivenom is extremely safe – no cases of anaphylaxis have been reported and only one case of serum sickness has been associated with the antivenom 9. There has been only 1 death associated with Sydney funnel web spider bite and was likely a result of a delayed presentation 10.
Funnel-web spiders are medium to large in size and are dark in color, ranging from black to brown (Figure 1). Funnel-web spiders get their name from their funnel-shaped burrows they spin to trap prey. These spiders reside in cool and relatively sheltered habitats. They are often found under rocks or in rock gardens, in various shrubberies, or under logs. Some funnel web spiders even reside in trees, sometimes several meters in the air.
The male funnel web spider has a spur on its second leg and the spinnerets (from which the spider produces silk) of both sexes are long and obvious, especially the terminal spinneret. Both sexes of funnel web spider are very aggressive. When disturbed, they will rear up ready to strike with their large, downward pointing fangs. The female funnel web spider constructs a burrow that may be 30 cm or more deep. Some use crevices in rocks or around house foundations and colonies may contain as many as 100 spiders. The male funnel web spiders tend to roam and often enter houses, particularly during the summer months and in wet weather. Funnel web spider bites may occur when the spider has taken up temporary residence in bedding, clothing or footwear, or when it is trodden on.
Funnel-web spiders have powerful, sharp fangs that have been known to penetrate fingernails and soft shoes. They are known to be the most dangerous spiders in the world. The silk entrance to the burrow of a Sydney funnel-web spider has a “vestibule-like” structure, and the spider sits just within the vestibule and senses vibrations along the silk “trip lines” and reacts to inject venom into its prey. The tree-dwelling funnel-web spiders can reach 4 to 5 cm in length, with the largest species being the Northern Tree Funnel Web Spider 11.
All funnel-web spider bites should be treated as potentially life-threatening, even though only approximately 10% to 15% of bites are venomous. Since the venom from the funnel-web spider bite is highly toxic, all species should be considered potentially dangerous 12 In all the fatalities where the gender of the spider was confirmed, the male funnel-web spider was responsible. The male species is considered to be the most venomous, and all 13 funnel web spider fatalities documented before the introduction of antivenom in 1980 have been attributed to the male spider 13. Males are more active at night and have been known to enter homes. The onset of severe envenomation is rapid. In one study, the median time to onset of envenoming was 28 minutes, and only 2 cases had onset after 2 hours. In both cases, the bites had pressure immobilization bandages applied. Death may occur in 15 minutes (small children) to 3 days 10. Younger patients and patients with underlying medical conditions have a higher incidence of death when they are bitten by a funnel-web spider.
Figure 1. Funnel web spiders
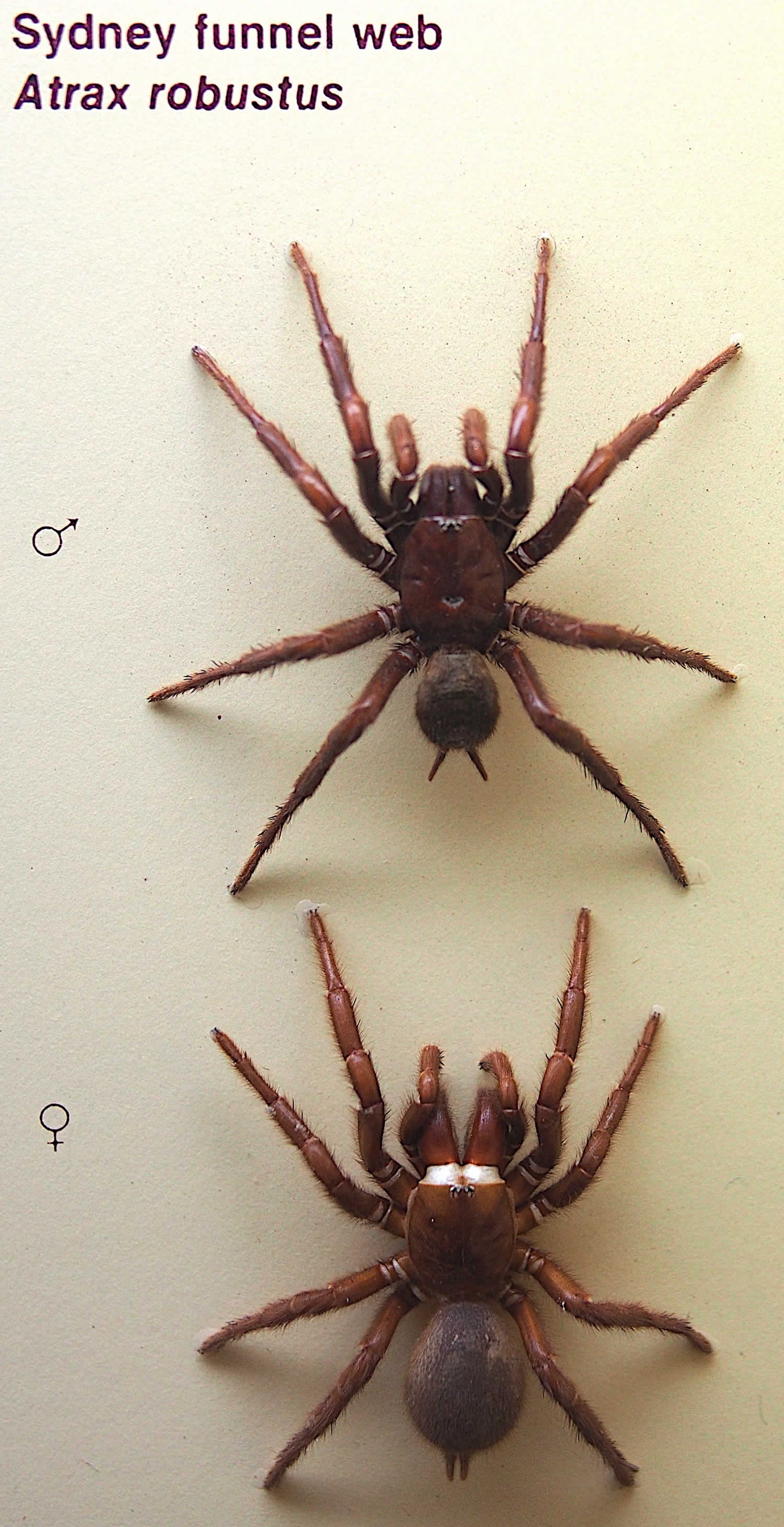
Footnote: Comparison of size and appearance of male (top) and female (bottom) Sydney funnel web spiders
Funnel web spider bite symptoms
The initial funnel web spider bite is usually painful and fangmarks are generally seen 14. The Sydney funnel web spider envenomation syndrome is generally characterized by two phases: the first begins within minutes of the bite, and the second when the secretions subside – typically many hours later 15. Historically deaths have occurred in either phase of envenomation.
Phase 1
Phase 1 is characterized by:
- Local effects:
- bite site may be painful for days to weeks because of direct trauma and acidity of venom but no local necrosis has been recorded
- local swelling, erythema and occasionally sweating.
- General effects:
- numbness around the mouth and spasms/fasciculation of the tongue
- nausea and vomiting, abdominal pain, acute gastric dilatation
- profuse sweating, salivation, lacrimation, piloerection
- severe dyspnea as a result of noncardiogenic pulmonary edema
- mental status can rapidly progress from confusion to irrationality or coma
- hypertension, tachycardia and vasoconstriction (hypotension may occur later)
- local and generalized muscle fasciculation and spasm which may be prolonged and violent (facial, tongue or intercostal muscles, trismus) and difficult to manage.
Phase 2
Phase 2 is characterized by:
- hypotension
- hypoventilation and apnea
- continuing acute noncardiogenic pulmonary edema
- coma, and, finally
- irreversible cardiac arrest.
Funnel web spider bite diagnosis
Spider identification is problematic and the clinician is better off recognizing the ‘toxindrome’ (the signs and symptoms associated with medically significant spider bite) than attempting to identify the spider responsible for the bite 1. Incorrect spider identification is likely to be responsible for the myth that white tailed spider (Lampona spp) bites commonly result in necrotising arachnidism 16. The term for systemic effects resulting from spider bite is ‘araneism’, or ‘arachnidism’. In addition, there are terms to describe the effects of specific spiders such as ‘latrodectism’ (red back spider) and ‘loxoscelism’ (recluse spider). The two main types of spider venom are:
- neurotoxic (affects the nervous system) – released by Latrodectus species (red back spider, widow spider) and Atrax species (funnel web spider), and
- cytotoxic or necrotic (causing damage to tissue) – released by Loxosceles species (recluse spider).
No assay is available for the clinical detection of funnel-web spider venom.
- Perform laboratory studies to assess the effects of envenomation or in consideration of differential diagnoses and coexistent conditions.
- Obtain arterial blood gas measurements, serum electrolyte levels, and creatinine clearance to assess for hypoxia, acidosis, hyperglycemia, and renal impairment.
- Measure serum glucose level in any patient with altered mental status to exclude hypoglycemia.
- Elevated serum creatine kinase can indicate rhabdomyolysis and should be measured.
- Complete blood count (CBC) results may demonstrate hemoconcentration, and coagulation studies may demonstrate a coagulopathy.
- A chest radiograph may demonstrate pulmonary edema.
Funnel web spider bite treatment
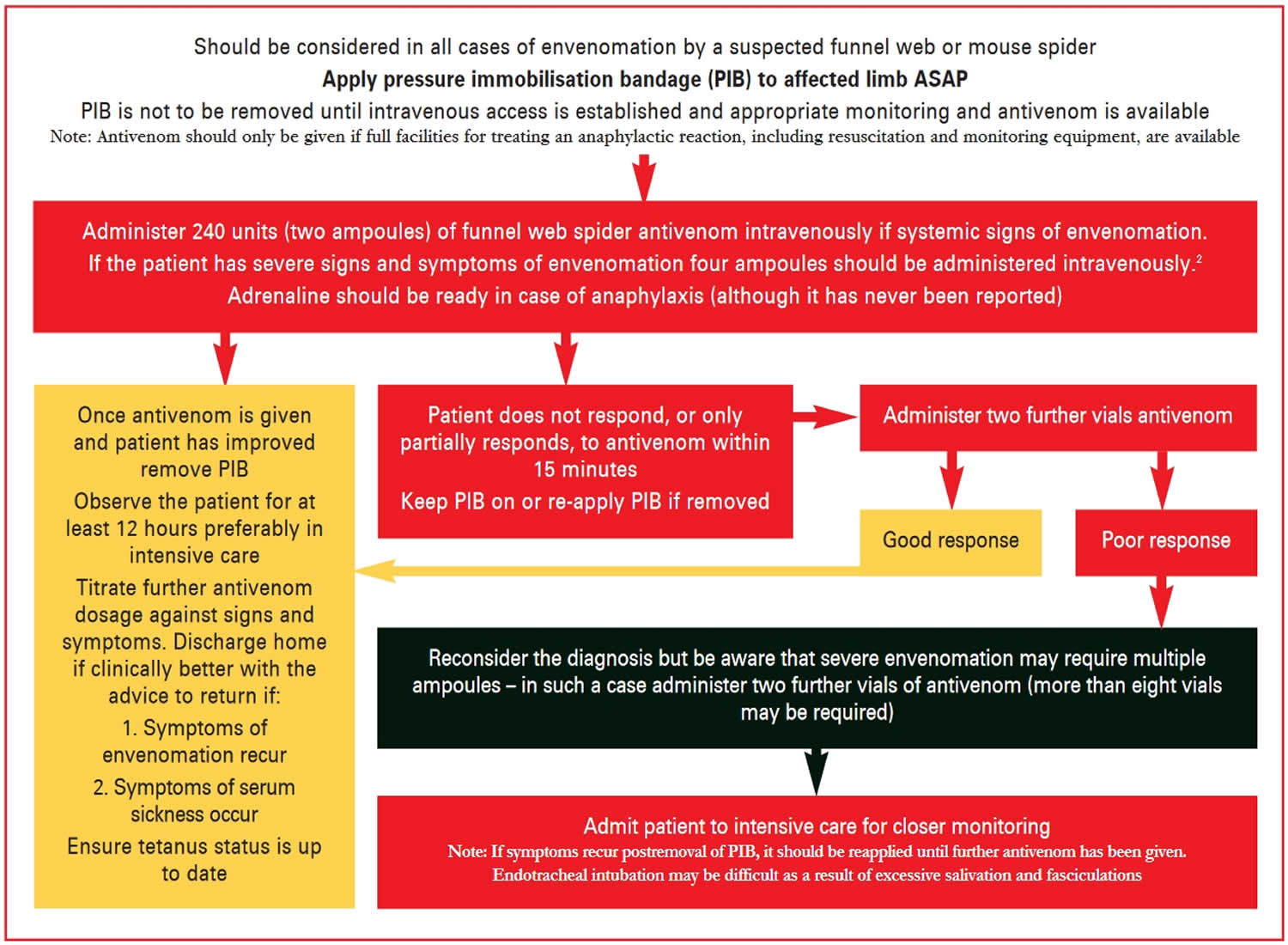
Funnel web spider antivenom is the only example of the use of rabbit IgG to treat a human envenomation 1. It was developed by Sutherland in 1980 17. Isbister et al 4 reported a severe allergy rate of 1.3%. Treatment of funnel web spider envenomation is outlined in Figure 2.
Figure 2. Management of potential funnel web spider bite
First aid and treatment
A summary of the recommended first aid and medical treatment for funnel web spider bite is presented in Figure 2. The key points are:
Treatment of funnel web spider envenomation 18:
- Ensure airway, breathing and circulation (ABCs) are maintained
- Supplemental oxygen (if available) should be started
- Prompt application of a pressure immobilisation bandage (PIB) to the affected limb to retard lymphatic spread of venom and promote local destruction or inactivation of the venom
- Local tissue enzymes may inactivate the venom, therefore the use of pressure immobilisation bandage may not only be helpful in delaying the onset of symptoms, but may allow for a degree of inactivation of the venom
- Transfer to hospital where antivenom and resuscitation equipment and monitoring is available
- Intravenous access should be obtained
- Pressure immobilisation bandage removal should only be performed in an appropriate resuscitation area with antivenom on hand
- If pressure immobilisation bandage has been removed and the patient deteriorates, it should be reapplied
- At the first sign of systemic envenoming due to suspected funnel web spider bite, it is advisable to give two vials of CSL Funnel Web Spider Antivenom (be prepared to give another 2–4
vials). If envenoming is already severe, start with four vials 19. Each ampoule contains 125 units of neutralizing capacity against the Sydney funnel web spider venoms. This is a freeze dried preparation. Re-constitute with approximately 6.3mL of water for injections.
Additional measures 1:
- Atropine (0.6 mg initial dose for an adult) to reduce salivation and bronchorrhea.
- Nasogastric aspiration because of gastric dilatation
- Muscle relaxants and sedatives to facilitate mechanical ventilation and control intracranial pressure
- Intubation and mechanical ventilation can assist in decreasing ventilation and gas exchange in the presence of excessive secretions and noncardiogenic pulmonary edema. (Note: entotracheal intubation can be difficult as a result of excessive salivary secretions and violent fasciculations). If secretions are not problematic and the patient is awake, noninvasive ventilation such as continuous positive airway pressure (CPAP) may be of benefit (CPAP may exacerbate hypotension).
- Fluid resuscitation should be used with caution in the event of hypotension because of noncardiogenic pulmonary edema.
- Relapse is possible and may manifest as dyspnea secondary to noncardiogenic edema, which usually responds to further antivenom (this should not be confused with iatrogenic pulmonary edema as a result of intravenous overload, particularly in children).
- If no symptoms or signs of envenomation have started 4 hours after the removal of first aid measures or postbite, the patient may be discharged (most patients presenting to hospital will not have been envenomed).
- Tetanus status should be assessed and prophylaxis provided if indicated.
Funnel web spider bite prognosis
Funnel-web spider bites can be life threatening, especially in children. They must be treated quickly with antivenin by an experienced provider. Even with appropriate and quick treatment, symptoms may last for several days to weeks. The original bite may be small and may progress to a blood blister and look like a bull’s eye. (This is similar to the appearance of a brown recluse spider bite.)
The area affected by the bite may become deeper. Additional symptoms such as fever, chills, and other signs of additional organ system involvement may develop. Deep scarring may occur and surgery may be needed to improve appearance of the scar.
Only 1 in 10 people bitten by a funnel-web spider displays signs of envenomation; however, if envenomation occurs, mortality rates are high in patients who receive no antivenom treatment. Most patients who survive until antivenom can be administered are able to make a complete recovery.
The mortality rate is difficult to determine from data from the era before antivenom. From 1927-1980, 13 deaths attributed to A robustus were reported in the medical literature and news media. No deaths have occurred since the introduction of antivenom 20.
Deaths occurred in children and adult females with bites. In all cases where the spider was identified, the culprit was the Sydney funnel-web spider,Atrax robustus. Severe envenomation, but not death, has been reported following bites by Hadronyche species.
Death occurs between 15 minutes and 3 days following the bite. In children, death is usually early and caused by pulmonary edema. In adults, death usually occurs later and is caused by persistent hypotension and cardiovascular collapse. In the late 1970s, 2 deaths occurred despite modern intensive care units. Death in these cases occurred from multisystem organ failure days after the bite 21.
References- Spider bites – Assessment and management. Australian Family Physician Vol. 38, No. 11, November 2009 https://www.racgp.org.au/afp/200911/200911braithberg.pdf
- Binstead JT, Nappe TM. Funnel Web Spider Toxicity. [Updated 2019 Dec 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535394
- Isbister GK, Gray MR, Balit CR, et al. Funnel web spider bite: A systematic review of recorded clinical cases. Med J Aust 2005;182:407–11.
- Isbister GK, Gray MR. A prospective study of 750 definite spider bites, with expert spider identification. Quart J Med 2002;95:723–31.
- Sutherland SK, Tibballs J. The genera Atrax and Hadronyche, funnel-web spiders. In: Australian animal toxins: The creatures, their toxins and care of the poisoned patient. Melbourne: Oxford University Press, 2001; 402–64.
- Graudins A, Wllson D, Alewood PF, et al. Cross reactivity of Sydney funnel web spider antivenom: Neutralisation of the in vitro toxicity of other Australian funnel web (Atrax and Hadronyche) spider venoms. Toxicon 2002;40:259–66.
- Fisher MM, Raftos J, McGuiness RT, et al. Funnel web spider (Atrax robustus) antivenom. Early clinical experience. Med J Aust 1981;2:525–526.
- Sutherland SK, Tibballs J. The genera Atrax and Hadronyche, funnel web spiders. Australiananimal toxins: the creatures, their toxins andthe care of the poisoned patient. Melbourne:Oxford University Press 2001;402–464.
- Miller MK, Whyte IM, Dawson AH. Serum sickness from funnel web spider antivenom. Med J Aust 1999;171:54.
- Isbister GK, Gray MR, Balit CR, Raven RJ, Stokes BJ, Porges K, Tankel AS, Turner E, White J, Fisher MM. Funnel-web spider bite: a systematic review of recorded clinical cases. Med. J. Aust. 2005 Apr 18;182(8):407-11.
- Atkinson RK, Walker P. The effects of season of collection, feeding, maturation and gender on the potency of funnel-web spider (Atrax infensus) venom. Aust J Exp Biol Med Sci. 1985 Oct;63 ( Pt 5):555-61.
- Isbister GK. Antivenom efficacy or effectiveness: the Australian experience. Toxicology. 2010 Feb 09;268(3):148-54.
- Sutherland SK, Tibballs J. The genera Atrax and Hadronyche, funnel web spiders. Australian animal toxins: the creatures, their toxins and the care of the poisoned patient. Melbourne: Oxford University Press 2001;402–464.
- The funnel web and common spider bites. Australian Family Physician Vol. 33, No. 4, April 2004 https://www.racgp.org.au/afpbackissues/2004/200404/20040413nimo.pdf
- Sutherland SK, Tibballs J. The genera Atrax andHadronyche, funnel web spiders. Australiananimal toxins: the creatures, their toxins andthe care of the poisoned patient. Melbourne:Oxford University Press 2001;402–464.
- Isbister G, Gray MR. White-tail spider bite: A prospective study of 130 definite bites by Lampona species. Med J Aust 2003;179:199–202.
- Sutherland SK. Antivenom to the venom of the male Sydney funnel-web spider Atrax robustus. Preliminary report. Med J Aust 1980;2:437–41.
- Nimorakiotakis B, Winkel KD. The funnel web and common spider bites. Aust Fam Physician 2004;33:244–51.
- CSL Antivenom Handbook. CSL Funnel Web Spider Antivenom. http://www.toxinology.com/generic_static_files/cslavh_antivenom_funweb.html
- Isbister GK, Gray MR, Balit CR, Raven RJ, Stokes BJ, Porges K, et al. Funnel-web spider bite: a systematic review of recorded clinical cases. Med J Aust. 2005 Apr 18. 182(8):407-411.
- Fisher MM, Carr GA, McGuinness R, Warden JC. Atrax robustus envenomation. Anaesth Intensive Care. 1980 Nov. 8(4):410-20.





{kind=link}