Herpes
Herpes is the name of a group of viruses that cause painful blisters and sores. The most common viruses are:
- Herpes simplex virus type 1 (HSV-1) and herpes simplex virus type 2 (HSV-2). Herpes simplex virus type 1 (HSV-1) usually causes cold sores or fever blisters around your mouth. Herpes simplex virus type 2 (HSV-2) usually causes sores on the genitals or sexual organs (genital herpes). Genital herpes is a sexually transmitted infection (STI). Once you’re infected, you have the virus for the rest of your life.
- Type 1 herpes simplex virus (HSV-1) usually causes oral herpes, fever blisters or cold sores. Type 1 herpes simplex virus (HSV-1) infects more than half of the U.S. population by the time they reach their 20s. HSV-1 is mainly transmitted via contact with the virus in sores, saliva or surfaces in or around the mouth. People may be exposed to HSV-1 as children due to close skin-to-skin contact with someone infected. Less commonly, HSV-1 can be transmitted to the genital area through oral-genital contact to cause genital herpes. Type 1 herpes simplex virus (HSV-1) can be transmitted from oral or skin surfaces that appear normal; however, the greatest risk of transmission is when there are active sores. People who already have HSV-1 are not at risk of reinfection, but they are still at risk of acquiring HSV-2.
- Type 2 herpes simplex virus (HSV-2) usually affects the genital area. Herpes simplex virus type 2 (HSV-2) usually causes sores on the genitals or sexual organs (genital herpes). Genital herpes is a sexually transmitted infection (STI). HSV-2 is mainly transmitted during sex through contact with genital or anal surfaces, skin, sores or fluids of someone infected with the virus. HSV-2 can be transmitted even if the skin looks normal and is often transmitted in the absence of symptoms.
- However, either HSV-1 or HSV-2 can affect almost any area of skin or mucous membrane. Once you’re infected, you have the virus for the rest of your life.
- Recurrent outbreaks of genital herpes caused by HSV-1 are often less frequent than outbreaks caused by HSV-2.
- In rare circumstances, herpes (HSV-1 and HSV-2) can be transmitted from mother to child during delivery, causing neonatal herpes.
- Herpes zoster also known as varicella zoster virus (VZV) or herpesvirus 3, the same virus that causes chickenpox initially and later on shingles. After a person recovers from chickenpox, the varicella zoster virus (VZV) stays dormant (inactive) in the body inside the nerves within dorsal root ganglia of your spinal cord. The varicella zoster virus (VZV) can reactivate years later, causing shingles.
Once you have been infected with the herpes virus, you’ll go through different stages of infection.
- Primary stage. This stage starts 2 to 8 days after you’re infected with the herpes virus. Usually, the herpes virus infection causes groups of small, painful blisters. The fluid in the blisters may be clear or cloudy. The area under the blisters will be red. The blisters break open and become open sores. You may not notice the blisters, or they may be painful. It may hurt to urinate during this stage. While most people have a painful primary stage of infection, some don’t have any symptoms. They may not even know they’re infected.
- Latent stage. During this stage, there are no blisters, sores, or other symptoms. The herpes virus is traveling from your skin into the nerves near your spine where they stay dormant.
- Shedding stage. In the shedding stage, the herpes virus starts multiplying in the nerve endings. If these nerve endings are in areas of your body that make or are in contact with body fluids, the herpes virus can get into those body fluids. This could include saliva, semen, or vaginal fluids. There are no symptoms during this stage, but the herpes virus can be spread during this time. This means that herpes is very contagious during this stage.
- Recurrences. Many people have blisters and sores that come back after the first herpes attack goes away. This is called a recurrence. Usually, the symptoms aren’t as bad as they were during the first attack. Stress, being sick, or being tired may start a recurrence. Being in the sun or having your menstrual period may also cause a recurrence. You may know a recurrence is about to happen if you feel itching, tingling, or pain in the places where you were first infected.
Herpes key facts:
- Genital herpes is a common sexually transmitted infection (STI).
- Over the past 20 years, HSV-1 and HSV-2 estimated seroprevalence has steadily declined, yet certain populations remain disproportionately affected by HSV infection.
- Infection is lifelong; currently, there is no cure for HSV infection.
- Neonatal herpes infection (birth-acquired herpes or herpes during pregnancy) is uncommon yet can result in substantial morbidity and mortality.
If you think you have herpes, see your doctor as soon as possible. It’s easier to diagnose when there are sores. You can start treatment sooner and perhaps have less pain with the infection.
There’s no cure for herpes. But medicines can help. They may be provided as a pill, cream, or a shot. Medicines such as acyclovir and valacyclovir fight the herpes virus. They can speed up healing and lessen the pain of herpes for many people. They can be used to treat a primary outbreak or a recurrent one.
If the medicines are being used to treat a recurrence, they should be started as soon as you feel tingling, burning, or itching. They can also be taken every day to prevent recurrences.
Figure 1. Herpes simplex virus (HSV)
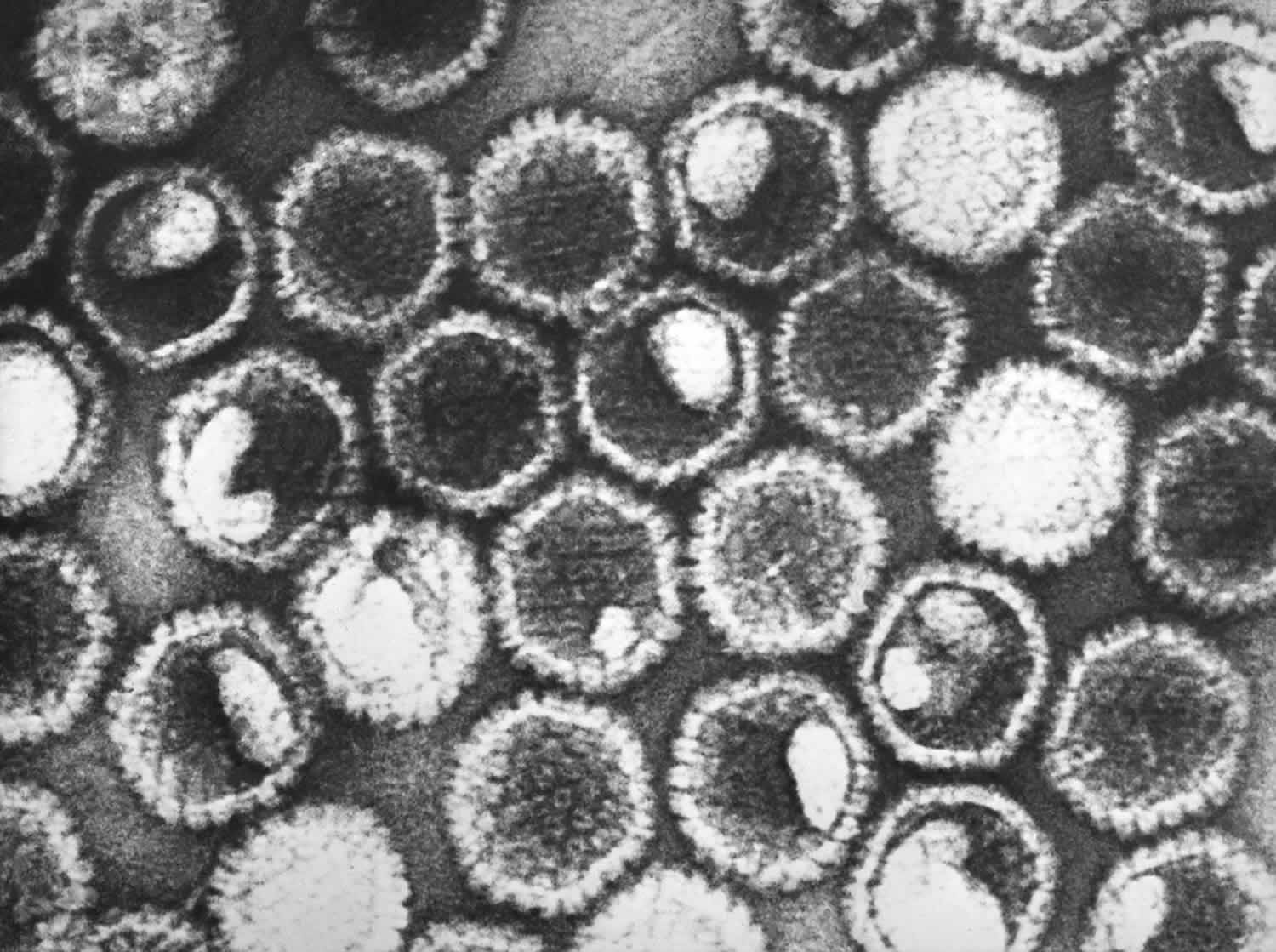
Footnote: This negatively stained transmission electron microscopic image revealed the presence of numerous herpes simplex virions. At the core of its icosahedral proteinaceous capsid, the HSV contains a double-stranded DNA linear genome.
[Source 1 ]What causes herpes?
Genital herpes is a sexually transmitted disease (STD) caused by two types of herpes viruses – herpes simplex virus type 1 (HSV-1) and herpes simplex virus type 2 (HSV-2) 2. People with HSV infections can pass along the virus even when they have no visible symptoms.
Herpes is most easily spread when blisters or sores can be seen on the infected person. But it can be spread at any time, even when the person who has herpes isn’t experiencing any symptoms. Herpes can also be spread from one place on your body to another. If you touch sores on your genitals, you can carry the virus on your fingers. Then you can pass it onto other parts of your body, including your mouth or eyes.
The herpes simplex virus type 2 (HSV-2) that causes genital herpes is usually spread from one person to another during vaginal, oral, or anal sex. The herpes simplex virus type 2 (HSV-2) can enter your body through a break in your skin. It can also enter through the skin of your mouth, penis, vagina, urinary tract opening, or anus.
Herpes simplex 1
Herpes simplex virus type 1 (HSV-1) is a version of the virus that causes cold sores or fever blisters. People may be exposed to HSV-1 as children due to close skin-to-skin contact with someone infected.
A person with HSV-1 in tissues of the mouth can pass the virus to the genitals of a sexual partner during oral sex. The newly caught infection is a genital herpes infection.
Recurrent outbreaks of genital herpes caused by HSV-1 are often less frequent than outbreaks caused by HSV-2.
Neither HSV-1 nor HSV-2 survives well at room temperature. So the virus is not likely to spread through surfaces, such as a faucet handle or a towel. But kissing or sharing a drinking glass or silverware might spread the virus.
Herpes simplex 2
Herpes simplex virus type 2 (HSV-2) is the most common cause of genital herpes. The virus can be present:
- On blisters and ulcers or the fluid from ulcers
- The moist lining or fluids of the mouth
- The moist lining or fluids of the vagina or rectum
The virus moves from one person to another during sexual activity.
Herpes symptoms
Many people who get herpes never have symptoms. Sometimes the symptoms are mild and are mistaken for another skin condition. Symptoms of genital herpes may include:
- Painful sores in the genital area, anus, buttocks, or thighs
- Itching
- Painful urination
- Vaginal discharge
- Tender lumps in the groin
During the first outbreak called primary herpes, you may experience flu-like symptoms. These include body aches, fever, and headache. Many people who have a herpes infection will have outbreaks of sores and symptoms from time to time. Symptoms are usually less severe than the primary outbreak. The frequency of outbreaks also tends to decrease over time.
Herpes prevention
The best way to prevent getting herpes is to not have sex with anyone who has the virus. It can be spread even when the person who has it isn’t showing any symptoms. If your partner has herpes, there is no way of knowing for sure that you won’t get it.
If you are infected, there is no time that is completely safe to have sex and not spread herpes. If you have herpes, you must tell your sex partner. You should avoid having sex if you have any sores. Herpes can spread from one person to another very easily when sores are present.
You should use condoms every time you have sex. They can help reduce the risk of spreading herpes. But it’s still possible to spread or get herpes if you’re using a condom.
Herpes testing
Your doctor will do a physical exam and look at the sores. He or she can do a culture of the fluid from a sore and test it for herpes. Blood tests or other tests on the fluid from a blister can also be done.
Herpes treatment
There’s no cure for herpes. But medicines such as acyclovir and valacyclovir can help fight the herpes virus. If you think you have herpes, see your doctor as soon as possible. It’s easier to diagnose when there are sores. You can start treatment sooner and perhaps have less pain with the infection.
Your doctor give you a pill, cream, or a shot. They can speed up healing and lessen the pain of herpes for many people. They can be used to treat a primary outbreak or a recurrent one.
If the medicines are being used to treat a recurrence, they should be started as soon as you feel tingling, burning, or itching. They can also be taken every day to prevent recurrences.
To soothe the pain associated with herpes:
- Take acetaminophen (Tylenol) or ibuprofen (Advil, Motrin).
- Place lukewarm or cool cloths on the sore place.
- Take lukewarm baths. (A woman may urinate in the tub at the end of the bath if she is having pain urinating. This may help dilute the urine so it doesn’t burn the sores so badly.)
- Keep the area dry and clean.
- Wear cotton underwear.
- Wear loose-fitting clothes.
Living with herpes
It’s common to feel guilty or ashamed when you are diagnosed with herpes. You may feel your sex life is ruined or that someone you thought you could trust has hurt you. You may feel sad or upset. Talk to your family doctor about how you’re feeling.
Keep in mind that herpes is very common. About 1 in 6 adults have it. Herpes may get less severe as time goes by. You can help protect your sex partner by not having sex during outbreaks and by using condoms at other times.
Shingles
Shingles also called herpes zoster or zoster, is a painful blistering rash disease caused by the varicella zoster virus (VZV) the same virus that causes chickenpox, that reactivates (wakes up) causing a painful blistering rash. If you’ve ever had chickenpox, you can get shingles. Most cases of chickenpox occur in children under age 15, but older children and adults can get it too. Chickenpox (varicella-zoster virus infection) spreads very easily from one person to another. After the chickenpox clears, the varicella-zoster virus (VZV) stays inside your body inside the nerves within dorsal root ganglia and lie dormant for years. The varicella-zoster virus (VZV) may not cause problems for many years. Eventually, it may reactivates (wakes up) and travels along nerve pathways to your skin — producing shingles (herpes zoster) — a painful, blistering rash. But, not everyone who’s had chickenpox will develop shingles. Shingles tends to cause more pain and less itching than chickenpox. As you get older, the varicella-zoster virus (VZV) may reappear as shingles. Although shingles is most common in people over age 50, anyone who has had chickenpox is at risk. Shingles (herpes zoster) often affects people with weak immunity. People with various kinds of cancer have a 40% increased risk of developing shingles. People who have had shingles rarely get it again; the chance of getting a second episode is about 1%.
Almost 1 out of 3 people in the United States will develop shingles in their lifetime. There are an estimated 1 million cases of shingles each year in this country. Anyone who has recovered from chickenpox may develop shingles; even children can get shingles. However, the risk of shingles increases as you get older. About half of all cases occur in people 60 years old or older. Older adults also are more likely to have severe disease.
Shingles can lead to severe nerve pain called postherpetic neuralgia (PHN) that can last for months or years after the rash goes away.
Shingles generally lasts between two and six weeks. Most people get shingles only once, but it is possible to get it two or more times.
There is no cure for shingles. Early treatment with medicines that fight the virus may help. These medicines may also help prevent lingering pain.
- If you think you might have shingles, talk to your doctor as soon as possible. It’s important to see your doctor no later than 3 days after the rash starts. The doctor will confirm whether or not you have shingles and can make a treatment plan. Although there is no cure for shingles, early treatment with drugs that fight the virus can help the blisters dry up faster and limit severe pain. Shingles can often be treated at home. People with shingles rarely need to stay in a hospital.
The risk of getting shingles increases with age. A vaccine can reduce your risk of getting shingles or lessen its effects. Your doctor may recommend getting this vaccine after your 50th birthday or once you reach 60 years of age. There’s another — and maybe even more important — reason for getting the shingles vaccine. If you’ve had chickenpox, you can still get shingles after getting shingles vaccine. The vaccine also lessens your risk of developing serious complications from shingles, such as life-disrupting nerve pain.
The nerve pain can last long after the shingles rash goes away. Some people have this nerve pain, called post-herpetic neuralgia (PHN), for many years. The pain can be so bad that it interferes with your everyday life. The shingles vaccine reduces your risk of developing this nerve pain, even more than it reduces your risk of getting shingles.
An anti-viral medicine may also prevent long-lasting nerve pain if your get shingles. It’s most effective when started within 3 days of seeing the rash. The anti-viral medicine can also make shingles symptoms milder and shorter.
- Shingles and chickenpox are caused by the same virus called varicella zoster virus.
- An estimated 1 million people get shingles each year in the United States.
- Anyone who has had chickenpox can get shingles, and you can get shingles at any age.
- Your risk of getting shingles and having more severe pain increases as you get older.
- The Centers for Disease Control and Prevention (CDC) recommends people age 50 and older get two doses of the shingles vaccine Shingrix (recombinant zoster vaccine), separated by 2 to 6 months, to protect against shingles and its complications. Adults 19 years and older who have weakened immune systems because of disease or therapy should also get two doses of Shingrix (recombinant zoster vaccine), as they have a higher risk of getting shingles and related complications.
Figure 2. Shingles blisters (typical early onset of herpes zoster or shingles rash with blisters in groups)

Figure 3. Shingles rash

Figure 4. Shingles rash on body – typical of herpes zoster or shingles, this image display grouped blisters with central depressions in a red, band-like distribution.

Figure 5. Shingles on face

Footnote: Shingles rash along the face or brow area may involve the eye. The varicella-zoster virus can travel through the nerve fibers and emerge in the cornea. Eye pain, redness, tearing, and blurring are common symptoms of ocular shingles. If this happens, your eye care professional may prescribe oral anti-viral treatment to reduce the risk of inflammation and scarring in the cornea. Shingles can also cause decreased sensitivity in the cornea. Corneal problems may arise months after the shingles are gone from the rest of the body. If you experience shingles in your eye, or nose, or on your face, it’s important to have your eyes examined several months after the shingles have cleared. If left untreated, this infection can lead to permanent eye damage.
You can’t catch shingles from someone. However, if you have a shingles rash, you can pass the virus to someone who has not had chickenpox (or the chickenpox vaccine) can get this virus. This would usually be a child, when this happens, the person develops chickenpox, not shingles. The virus spreads through direct contact with the rash and cannot spread through the air. Chickenpox can be dangerous for some people. Until your shingles blisters scab over, you are contagious and should avoid physical contact with anyone who hasn’t yet had chickenpox or the chickenpox vaccine, especially people with weakened immune systems, pregnant women and newborns.
If you have shingles, what can you do to prevent spreading the virus?
When you have shingles, you’re only contagious while you have blisters. To prevent spreading the virus while you have blisters, the Centers for Disease Control and Prevention (CDC) recommends that you:
- Cover the rash
- Wash your hands often and try to avoid touching the rash
- Avoid being around people for whom catching the virus could be dangerous
The varicella-zoster virus is especially dangerous for these people
- Catching this virus and getting chickenpox can be dangerous for women who are pregnant and have not had chickenpox or gotten the chickenpox vaccine. In this situation, the virus can harm the woman’s unborn baby.
Babies less than 1 month old and people who have a weak immune system can also have complications if they catch the virus. People who have a weak immune system include those who are:
- HIV positive
- Taking medicine that weakens their immune system
- Receiving chemotherapy or radiation treatments
You’re not contagious before you develop blisters or after the blisters scab over. Be sure to take precautions while you have blisters.
A person must have had chickenpox to get shingles. Some people who have had chickenpox have a higher risk of getting shingles. But, not everyone who’s had chickenpox will develop shingles.
Most people who develop shingles have only one episode during their lifetime. However, a person can have a second or even a third episode.
- One out of every three people 60 years old or older will get shingles.
- One out of six people older than 60 years who get shingles will have severe pain. The pain can last for months or even years.
- The most common complication of shingles is severe pain where the shingles rash was. This pain can be debilitating. There is no treatment or cure from this pain. As people get older, they are more likely to develop long-term pain as a complication of shingles and the pain is likely to be more severe.
- Shingles may also lead to serious complications involving the eye.
- Very rarely, shingles can also lead to pneumonia, hearing problems, blindness, brain inflammation (encephalitis), or death.
Some illnesses and medical treatments can weaken a person’s immune system and increase the risk of getting shingles. These include:
- Are 50 years of age or older
- Have an illness or injury
- Are under great stress
- Have medical conditions that keep their immune systems from working properly:
- Cancers like leukemia and lymphoma
- Human immunodeficiency virus (HIV)/AIDS
- Some cancer treatments, such as chemotherapy or radiation
- Medicine taken to prevent rejection of a transplanted organ. Immunosuppressive drugs, such as steroids and drugs that are given after organ transplantation.
- Cortisone when taken for a long time
What causes shingles?
Shingles is caused by the varicella zoster virus (VZV), the same virus that causes chickenpox. After a person recovers from chickenpox, the virus stays dormant (inactive) in the body (in the nervous system). Shingles appears when the virus wakes up. Scientists aren’t sure why the virus can reactivates or “wakes up” years later, causing shingles. A short-term weakness in immunity may cause this. Shingles is more common in older adults and in people who have weakened immune systems.
Shingles cannot be passed from one person to another. However, the virus that causes shingles, the varicella zoster virus (VZV), can spread from a person with active shingles to cause chickenpox in someone who had never had chickenpox or received chickenpox vaccine.
The varicella zoster virus (VZV) is spread through direct contact with fluid from the rash blisters caused by shingles.
A person with active shingles can spread the virus when the rash is in the blister-phase. A person is not infectious before the blisters appear. Once the rash has developed crusts, the person is no longer infectious.
Shingles is less contagious than chickenpox and the risk of a person with shingles spreading the virus is low if the rash is covered.
If you have shingles, you should:
- Cover the rash.
- Avoid touching or scratching the rash.
- Wash your hands often to prevent the spread of varicella zoster virus.
- Avoid contact with the people below until your rash has developed crusts
- pregnant women who have never had chickenpox or the chickenpox vaccine;
- premature or low birth weight infants; and
- people with weakened immune systems, such as people receiving immunosuppressive medications or undergoing chemotherapy, organ transplant recipients, and people with human immunodeficiency virus (HIV) infection.
Risk factors for shingles
Anyone who has ever had chickenpox can develop shingles. Most adults in the United States had chickenpox when they were children, before the advent of the routine childhood vaccination that now protects against chickenpox.
Factors that may increase your risk of developing shingles include:
- Being older than 50. Shingles is most common in people older than 50. The risk increases with age. Some experts estimate that half the people age 80 and older will have shingles.
- Having certain diseases. Diseases that weaken your immune system, such as HIV/AIDS and cancer, can increase your risk of shingles.
- Undergoing cancer treatments. Radiation or chemotherapy can lower your resistance to diseases and may trigger shingles.
- Taking certain medications. Drugs designed to prevent rejection of transplanted organs can increase your risk of shingles — as can prolonged use of steroids, such as prednisone.
Triggering factors for shingles
Shingles triggering factors are sometimes recognized, such as:
- Pressure on the nerve roots
- Radiotherapy at the level of the affected nerve root
- Spinal surgery
- An infection
- An injury (not necessarily to the spine)
- Contact with someone with varicella (chickenpox) or herpes zoster (shingles)
Shingles prevention
A shingles vaccine may help prevent shingles. The Centers for Disease Control and Prevention (CDC) recommends people age 50 and older get two doses of the shingles vaccine Shingrix (recombinant zoster vaccine), separated by 2 to 6 months, to protect against shingles and its complications. Adults 19 years and older who have weakened immune systems because of disease or therapy should also get two doses of Shingrix (recombinant zoster vaccine), as they have a higher risk of getting shingles and related complications.
Routine vaccination of people 50 years old and older 5:
- Whether or not they report a prior episode of herpes zoster.
- Whether or not they report a prior dose of Zostavax, a shingles vaccine that is no longer available for use in the United States.
- It is not necessary to screen, either verbally or by laboratory serology, for evidence of prior varicella.
In the United States, Shingrix (recombinant zoster vaccine) was approved by the Food and Drug Administration (FDA) in 2017. Studies suggest that Shingrix offers protection against shingles for more than five years. Shingrix is a nonliving vaccine made of a virus component. It is given in two doses, with 2-6 months between doses.
The shingles vaccine is used only as a prevention strategy. It’s not intended to treat people who currently have the disease. Talk to your doctor about which option is right for you.
Shingrix is approved and recommended for people age 50 and older, including those who’ve previously received the Zostavax vaccine or had shingles.
- The Zostavax vaccine is no longer sold in the U.S., but other countries may still use it.
The most common side effects of either shingles vaccine are redness, pain, tenderness, swelling and itching at the injection site, and headaches.
The shingles vaccine doesn’t guarantee that you won’t get shingles. But this vaccine will likely reduce the course and severity of the disease and reduce your risk of postherpetic neuralgia.
Adults 50 years old or older should talk to their healthcare professional about getting two doses of the shingles vaccine Shingrix (recombinant zoster vaccine), separated by 2 to 6 months, to protect against shingles and its complications.
- The shingles vaccine can reduce your risk of shingles and the long-term pain it can cause 6.
- Persons who have already had shingles or who have a chronic medical condition can receive the shingles vaccine.
- In a clinical trial involving thousands of adults 60 years old or older, the vaccine reduced the risk of shingles by about half. Even if the shingles vaccine doesn’t prevent you from getting shingles, it can still reduce the chance of having long-term pain or post-herpetic neuralgia (PHN).
Talk with your healthcare professional for more information and to find out if the shingles vaccine is right for you.
Adults can get vaccines at doctors’ offices, pharmacies, workplaces, community health clinics, and health departments. To find a place to get a vaccine near you, go to https://vaccinefinder.org/
Most private health insurance plans cover recommended vaccines. Check with your insurance provider for details and for a list of vaccine providers. Medicare Part D plans cover shingles vaccine, but there may be costs to you depending on your specific plan.
If you do not have health insurance, visit https://www.healthcare.gov/ to learn more about health insurance options.
Contraindications and precautions for herpes zoster vaccination
Shingrix (recombinant zoster vaccine) should NOT be administered to 5, 7:
- A person with a history of severe allergic reaction, such as anaphylaxis, to any component of this vaccine.
- A person experiencing an acute episode of herpes zoster. Shingrix is not a treatment for herpes zoster or postherpetic neuralgia (PHN). The general guidance for any vaccine is to wait until the acute stage of the illness is over and symptoms abate.
There is currently no CDC recommendation for Shingrix use in pregnancy; therefore, providers should consider delaying vaccination until after pregnancy. There is no recommendation for pregnancy testing before vaccination with Shingrix. Recombinant vaccines such as Shingrix pose no known risk to people who are breastfeeding or to their infants. Providers may consider vaccination without regard to breastfeeding status if Shingrix is otherwise indicated.
Adults with a minor acute illness, such as a cold, can receive Shingrix. Adults with a moderate or severe acute illness should usually wait until they recover before getting the vaccine.
Shingles signs and symptoms
Early signs of shingles include burning or shooting pain and tingling or itching, usually on one side of the body or face. The most common place for shingles is a band that goes around one side of your waistline. The pain can be mild to severe. Rashes or blisters appear anywhere from one to 14 days later. The rash consists of blisters that typically scab over in 7 to 10 days. The rash usually clears up within 2 to 4 weeks. If shingles appears on your face, it may affect your vision or hearing. The pain of shingles may last for weeks, months, or even years after the blisters have healed.
- The warning: Before the rash develops, people often have pain, itching, burning or tingling in the area where the rash will develop. And area of skin may feel very sensitive. This usually occurs in a small area on 1 side of the body. These symptoms can come and go or be constant. The lymph nodes draining the affected area are often enlarged and tender. Most people experience this for 1 to 5 days before the rash appears. It can last longer.
- Rash: A rash then appears in the same area. Most commonly, the rash occurs in a single stripe around either the left or the right side of the body. In other cases, the rash occurs on one side of the face. In rare cases (usually among people with weakened immune systems), the rash may be more widespread and look similar to a chickenpox rash. Shingles can affect the eye and cause loss of vision.
- Blisters: The rash soon turns into groups of clear blisters. The blisters turn yellow or bloody before they crust over (scab) and heal. The blisters tend to last 2 to 3 weeks.
- Pain: It is uncommon to have blisters without pain. Once the blisters heal, the pain tends to lessen. The pain can last for months after the blisters clear.
- Flu-like symptoms: The person may get a fever, headache, chills or upset stomach with the rash.
The chest (thoracic), neck (cervical), forehead (ophthalmic) and lumbar or sacral sensory nerve supply regions are most commonly affected at all ages. The frequency of ophthalmic herpes zoster or herpes zoster ophthalmicus (shingles affecting the eye) increases with age. Herpes zoster occasionally causes blisters inside the mouth or ears, and can also affect the genital area. Sometimes there is pain without rash—herpes zoster “sine eruptione”—or rash without pain, most often in children.
Pain and general symptoms subside gradually as the eruption disappears. In uncomplicated cases, recovery is complete within 2–3 weeks in children and young adults, and within 3–4 weeks in older patients.
Complications of shingles
The most common complication of shingles is a condition called post-herpetic neuralgia (PHN). People with post-herpetic neuralgia have severe pain in the areas where they had the shingles rash, even after the rash clears up. Post-herpetic neuralgia is diagnosed in people who have pain that persists after their rash has resolved. Some define post-herpetic neuralgia as any duration of pain after the rash resolves; others define it as duration of pain for more than 30 days, or for more than 90 days after rash onset.
The pain from post-herpetic neuralgia may be severe and debilitating, but it usually resolves in a few weeks or months. Some people can have pain from post-herpetic neuralgia for many years and can interfere with daily life.
A person’s risk of having post-herpetic neuralgia after herpes zoster increases with age. As people get older, they are more likely to develop post-herpetic neuralgia, and the pain is more likely to be severe. Post-herpetic neuralgia occurs rarely among people under 40 years of age but can occur in approximately 13% (and possibly more) of untreated people who are 60 years of age and older with herpes zoster. Older adults are more likely to have post-herpetic neuralgia and to have longer lasting and more severe pain. Other predictors of post-herpetic neuralgia include the level of pain a person has when they have the rash and the size of their rash.
Other complications of herpes zoster include:
- Shingles may also lead to serious complications involving the eye (herpes zoster ophthalmicus, when the ophthalmic division of the fifth cranial nerve is involved) may result in vision loss.
- Bacterial superinfection of the lesions, usually due to Staphylococcus aureus and, less commonly, due to group A beta hemolytic streptococcus.
- Cranial and peripheral nerve palsies. Depending on which nerves are affected, shingles can cause an inflammation of the brain (encephalitis), facial paralysis, or hearing or balance problems. Muscle weakness in about one in 20 patients. Facial nerve palsy is the most common result (Ramsay Hunt syndrome). There is a 50% chance of complete recovery, but some improvement can be expected in nearly all cases
- Deep blisters that take weeks to heal followed by scarring.
- Very rarely, shingles can also lead to pneumonia, hearing problems, blindness, brain inflammation (meningoencephalitis), hepatitis, acute retinal necrosis or death.
People with compromised or suppressed immune systems are more likely to have complications from herpes zoster. They are more likely to have severe rash that lasts longer. Also, they are at increased risk of developing disseminated herpes zoster.
Shingles (herpes zoster) in the early months of pregnancy can harm the fetus, but luckily this is rare. Shingles in late pregnancy can cause chickenpox in the fetus or newborn. Herpes zoster may then develop as an infant.
Shingles diagnosis
Shingles is usually diagnosed based on the history of pain on one side of your body, along with the telltale rash and blisters. Your doctor may also take a tissue scraping or culture of the blisters for examination in the laboratory.
Shingles treatment
There’s no cure for shingles, but prompt treatment with prescription antiviral drugs can speed healing and reduce your risk of complications. These medications include:
- Acyclovir (Zovirax)
- Valacyclovir (Valtrex)
- Famciclovir
Antiviral treatment can reduce pain and the duration of symptoms if started within one to three days after the onset of herpes zoster. Aciclovir 800 mg 5 times daily for seven days is most often prescribed. Valaciclovir and famciclovir are also useful.
In healthy children shingles is often relatively mild and may not require treatment, however, children who take courses of systemic steroids, e.g., for asthma, are rendered vulnerable for up to three months after treatment is complete – if the child develops chickenpox in this period parents should seek urgent competent advice as treatment with oral antiviral therapy will be required.
Immunocompromised patients
- Should continue on with oral antiviral therapy for two days after crusting of the lesions
- If the patient is unwell / develops widespread (disseminated) zoster, hospital admission will be needed
Management of acute herpes zoster may include:
- Rest and pain relief
- Protective ointment applied to the rash, such as petroleum jelly.
- Oral antibiotics for secondary infection
Shingles can cause severe pain, so your doctor also may prescribe:
- Capsaicin topical patch (Qutenza)
- Anticonvulsants, such as gabapentin (Neurontin)
- Tricyclic antidepressants, such as amitriptyline
- Numbing agents, such as lidocaine, delivered via a cream, gel, spray or skin patch
- Medications that contain narcotics, such as codeine
- An injection including corticosteroids and local anesthetics
Shingles generally lasts between two and six weeks. Most people get shingles only once, but it is possible to get it two or more times.
Shingles medication
It is best to get treatment immediately. Treatment can include:
Pain relievers to help ease the pain: The pain can be very bad, and prescription painkillers may be necessary. Your doctor also may prescribe:
- Capsaicin topical patch (Qutenza)
- Anticonvulsants, such as gabapentin (Neurontin)
- Tricyclic antidepressants, such as amitriptyline
- Numbing agents, such as lidocaine, delivered via a cream, gel, spray or skin patch
- Medications that contain narcotics, such as codeine
- An injection including corticosteroids and local anesthetics
Post-herpetic neuralgia may be difficult to treat successfully. It may respond to any of the following.
- Local anesthetic applications
- Topical capsaicin
- Tricyclic antidepressant medications such as amitriptyline
- Anti-epileptic medications gabapentin and pregabalin
- Transcutaneous electrical nerve stimulation or acupuncture
- Botulinum toxin into the affected area
- Early use of antiviral medication
Nonsteroidal anti-inflammatories (NSAIDs) and opioids are generally unhelpful.
Anti-viral medicine: This medicine may be prescribed when a doctor diagnoses shingles within 72 hours of the rash first appearing. The earlier anti-viral treatment is started, the better it works. Anti-viral medicines include famciclovir, valacyclovir, and acyclovir. These can lessen the pain and the amount of time the pain lasts.
Nerve blocks: Given for intense pain, these injections (shots) contain a numbing anesthetic and sometimes a corticosteroid.
Corticosteroids: To lower swelling and pain, some patients may get corticosteroid pills with their anti-viral medicine. This treatment is not common because it can make the rash spread.
Treatments for pain after the rash clears: Certain anti-depressants, pain relievers, anesthetic creams and patches, and anti-seizure medicines can help.
Ophthalmic zoster
- All patients with ophthalmic zoster, irrespective of age or severity of symptoms, should be prescribed oral antiviral drugs at the first sign of disease
- Patients with a red eye or visual complaints must be referred to an ophthalmologist on an urgent basis
- Those not needing referral must be reviewed after at most one week
Ramsay-Hunt syndrome
- Oral antiviral therapy must be started immediately and contact the on-call ENT (ear nose and throat) specialist
- Some advocate the use of systemic steroids – refer to local guidelines for management
Home remedies for shingles
- Get plenty of rest and eat well-balanced meals.
- Try simple exercises like stretching or walking. Check with your doctor before starting a new exercise routine.
- Apply a cool washcloth to your blisters to ease the pain and help dry the blisters.
- Cool compresses, baths or ice packs may help with the discomfort. Do not apply ice packs directly to the skin. Wrap the ice pack in a light towel and place it gently over the dressing. Wash the towel in hot water after use.
- Apply calamine lotion to the blisters.
- Cover the rash with loose, non-stick, sterile bandages.
- Wear loose cotton clothes around the body parts that hurt.
- Do things that take your mind off your pain. For example, watch TV, read, talk with friends, listen to relaxing music, or work on a hobby you like.
- Avoid stress. It can make the pain worse.
- Try not to scratch the rash. Scratching may cause scarring and infection of the blisters.
- If the blisters are open, applying creams or gels is not recommended because they might increase the risk of a secondary bacterial infection.
- After a bath or shower, gently pat yourself dry with a clean towel. Do not rub or use the towel to scratch yourself and do not share towels.
- Do not use antibiotic creams or sticking plasters on the blisters since they may slow down the healing process.
- Take an oatmeal bath or use calamine lotion to see if it soothes your skin.
- Avoid contact with people who may be more at risk, such as pregnant women who are not immune to chickenpox, people who have a weak immune system and babies less than 1 month old.
- Do not share towels, play contact sports, or go swimming.
- Share your feelings about your pain with family and friends. Ask for their understanding.
Also, you can limit spreading the virus by:
- Keeping the rash covered
- Not touching or scratching the rash
- Washing your hands often
Shingles prognosis
Most cases of shingles last 3 to 5 weeks. Shingles follows a pattern:
- The first sign is often burning or tingling pain; sometimes, it includes numbness or itching on one side of the body.
- Somewhere between 1 and 5 days after the tingling or burning feeling on the skin, a red rash will appear.
- A few days later, the rash will turn into fluid-filled blisters.
- About a week to 10 days after that, the blisters dry up and crust over.
- A couple of weeks later, the scabs clear up.
Most people get shingles only one time. But, it is possible to have it more than once.
Longterm pain and other lasting problems
After the shingles rash goes away, some people may be left with ongoing pain called post-herpetic neuralgia or PHN. The pain is felt in the area where the rash had been. For some people, post-herpetic neuralgia is the longest lasting and worst part of shingles. The older you are when you get shingles, the greater your chance of developing post-herpetic neuralgia.
The post-herpetic neuralgia pain can cause depression, anxiety, sleeplessness, and weight loss. Some people with post-herpetic neuralgia find it hard to go about their daily activities, like dressing, cooking, and eating. Talk with your doctor if you have any of these problems.
There are medicines that may help with post-herpetic neuralgia. Steroids may lessen the pain and shorten the time you’re sick. Analgesics, antidepressants, and anticonvulsants may also reduce the pain. Usually, post-herpetic neuralgia will get better over time.
Some people have other problems that last after shingles has cleared up. For example, the blisters caused by shingles can become infected. They may also leave a scar. It is important to keep the area clean and try not to scratch the blisters. Your doctor can prescribe an antibiotic treatment if needed.
See your doctor right away if you notice blisters on your face—this is an urgent problem. Blisters near or in the eye can cause lasting eye damage or blindness. Hearing loss, a brief paralysis of the face, or, very rarely, swelling of the brain (encephalitis) can also occur.
Herpes and pregnancy
Newborn infants can become infected with herpes virus during pregnancy, during labor or delivery, or after birth. Herpes type 2 virus (genital herpes) is the most common cause of herpes infection in newborn babies. But herpes type 1 virus (oral herpes) can also occur.
Newborn infants can become infected with herpes virus:
- In the uterus (this is unusual)
- Passing through the birth canal (birth-acquired herpes, the most common method of infection)
- Right after birth (postpartum) from being kissed or having other contact with someone who has herpes mouth sores
If the mother has an active outbreak of genital herpes at the time of delivery, the baby is more likely to become infected during birth. Some mothers may not know they have herpes sores inside their vagina.
Some women have had herpes infections in the past, but are not aware of it, and may pass the virus to their baby.
If your baby has any symptoms of birth-acquired herpes, including skin blisters with no other symptoms, have the baby seen by your doctor right away.
It’s important to avoid getting herpes during pregnancy. If your partner has herpes and you don’t have it, be sure to always use condoms during sexual intercourse. Your partner could pass the infection to you even if they are not currently experiencing an outbreak. If there are visible sores, avoid having sex completely until the sores have healed.
If you’re pregnant and have genital herpes, or if you have ever had sex with someone who had it, tell her doctor. Your doctor will give you an antiviral medicine to start taking toward the end of your pregnancy. This will make it less likely that you will have an outbreak at or near the time you deliver your baby.
If you have an active genital herpes infection at or near the time of delivery, you can pass it to your baby. When the baby passes through the birth canal, it may come in contact with sores and become infected with the virus. This can cause brain damage, blindness, or even death in newborns.
If you do have an outbreak of genital herpes at the time of delivery, your doctor will most likely deliver your baby by C-section. With a C-section, the baby won’t go through the birth canal and be exposed to the virus. This lessens the risk of giving herpes to your baby.
Herpes and pregnancy causes
Newborn infants can become infected with herpes virus during pregnancy, during labor or delivery, or after birth during the first 28 days after birth 8. Herpes type 2 virus (genital herpes) is the most common cause of herpes infection in newborn babies. But herpes type 1 virus (oral herpes) can also occur. Neonatal HSV infrequently occurs, with an estimated incidence of 1 in 3,000 deliveries 8, 9. In the United States, however, HSV-related neonatal deaths increased significantly between 1995 and 2017 10.
Newborn infants can become infected with herpes virus:
- In the uterus (this is unusual)
- Passing through the birth canal (birth-acquired herpes, the most common method of infection) also called intrapartum infection
- Right after birth (postpartum) from being kissed or having other contact with someone who has herpes mouth sores
The following five factors have been identified as the major influence for risk of transmission 11:
- Whether the HSV infection is primary or recurrent
- HSV antibody status of the pregnant person
- Duration of membrane rupture
- Integrity of mucocutaneous barrier (e.g. use of fetal scalp electrodes)
- Mode of the delivery (vaginal versus cesarean)
Approximately 85% of neonatal HSV infections result from intrapartum infection (a period from the onset of labor through delivery of the placenta), with the remaining cases involving HSV exposure and transmission during the intrauterine (in utero) or postpartum (postnatal) periods 11. The risk of intrapartum HSV transmission is highest among pregnant persons who newly acquire genital HSV-2 (or HSV-1) late in pregnancy when compared to women who have reactivation of genital HSV during pregnancy 8.
If the mother has an active outbreak of genital herpes at the time of delivery, the baby is more likely to become infected during birth. Some mothers may not know they have herpes sores inside their vagina.
The highest HSV transmission risk occurs when a pregnant person acquires HSV near the time of delivery 12, 13, 14. If a pregnant woman has primary genital HSV infection and is shedding HSV at the time of delivery, the risk of HSV transmission to the neonate is 10 to 30 times higher than if they are shedding HSV during a recurrent episode of genital herpes 11.
Some women have had herpes infections in the past, but are not aware of it, and may pass the virus to their baby.
If your baby has any symptoms of birth-acquired herpes, including skin blisters with no other symptoms, have the baby seen by your doctor right away.
Herpes and pregnancy prevention
Practicing safe sex can help prevent the mother from getting genital herpes.
People with cold sores (oral herpes) should not come in contact with newborn infants. To prevent transmitting the virus, caregivers who have a cold sore should wear a mask and wash their hands carefully before coming in contact with an infant.
Mothers should speak to their doctors about the best way to minimize the risk of transmitting herpes to their infant.
Herpes and pregnancy symptoms
Herpes may only appear as a skin infection. Small, fluid-filled blisters (vesicles) may appear. These blisters break, crust over, and finally heal. A mild scar may remain. Herpes infection may also spread throughout your body. This is called disseminated herpes. In this type, the herpes virus can affect many parts of your body.
- Herpes infection in the brain is called herpes encephalitis
- The liver, lungs, and kidneys may also be involved
- There may or may not be blisters on the skin
Newborn infants with herpes that has spread to the brain or other parts of the body are often very sick. Symptoms include:
- Skin sores, fluid-filled blisters
- Bleeding easily
- Breathing difficulties such as rapid breathing and short periods without breathing, which can lead to nostril flaring, grunting, or blue appearance
- Yellow skin and whites of the eyes
- Weakness
- Low body temperature (hypothermia)
- Poor feeding
- Seizures, shock, or coma
Herpes that is caught shortly after birth has symptoms similar to those of birth-acquired herpes.
Herpes the baby gets in the uterus can cause:
- Eye disease, such as inflammation of the retina (chorioretinitis)
- Severe brain damage
- Skin sores (lesions)
Herpes and pregnancy diagnosis
Tests for birth-acquired herpes include:
- Checking for the virus by scraping from vesicle or vesicle culture
- Electroencephalogram (EEG)
- MRI of the head
- Spinal fluid culture
Additional tests that may be done if the baby is very sick include:
- Blood gas analysis
- Blood coagulation studies (PT, PTT)
- Complete blood count
- Electrolyte measurements
- Tests of liver function
Herpes and pregnancy treatment
It is important to tell your doctor at your first prenatal visit if you have a history of genital herpes.
- If you have frequent herpes outbreaks, you’ll be given a medicine to take during the last month of pregnancy to treat the virus. This helps prevent an outbreak at the time of delivery.
- C-section is recommended for pregnant women who have an active outbreak of herpes sores and are in labor.
- You may have some prodromal symptoms before a sore appears. You may experience itching in the affected area, “tingling” or “pinching” sensations, muscle tenderness, shooting pains in the buttocks, legs, or groin, and nerve pain in the leg. Be sure to notify your provider if you are having these sensations.
- For women with a first-episode genital herpes infection during the third trimester of pregnancy, C-section may be offered due to the possibility of prolonged viral shedding.
Herpes virus infection in infants is generally treated with antiviral medicine given through a vein (intravenous). The baby may need to be on the medicine for several weeks.
Treatment may also be needed for the effects of herpes infection, such as shock or seizures. Because these babies are very ill, treatment is often done in the hospital intensive care unit.
Management of babies with herpes
Infants with HSV disease should be treated with parenteral acyclovir therapy in consultation with a pediatric infectious diseases specialist. Treatment duration is generally 14 days for SEM disease or 21 days for disseminated and central nervous system disease, and suppressive therapy after central nervous system disease may be indicated for up to 6 months; detailed guidelines are available for management of neonates who are delivered vaginally in the presence of maternal genital HSV lesions 15, 16. Despite improvement in outcomes with parenteral acyclovir and subsequent suppressive oral acyclovir therapy, neurodevelopmental outcomes remain poor in neonates with central nervous system herpes if present at birth 16, 17:
Recommended treatment regimen of neonatal herpes for infants with neonatal herpes limited to the skin and mucous membranes:
- Acyclovir 20 mg/kg body weight IV every 8 hours for 14 days
Recommended regimen for infants with neonatal herpes who have disseminated disease and disease involving the brain and spinal cord (CNS):
- Acyclovir 20 mg/kg body weight IV every 8 hours for 21 days
Herpes and pregnancy prognosis
Infants with systemic herpes or encephalitis often do poorly. This is despite antiviral medicines and early treatment.
In infants with skin disease, the vesicles may keep coming back, even after treatment is finished.
Affected children may have developmental delay and learning disabilities.
Genital herpes
Genital herpes is a sexually transmitted disease (STD) caused by two types of herpes viruses – herpes simplex virus type 1 (HSV-1) and herpes simplex virus type 2 (HSV-2) 18, 2. Genital herpes is a chronic, lifelong viral infection that causes recurrent genital ulcers and on rare occasions, disseminated and visceral disease 19. Most people with genital herpes do not know they have it or may have very mild symptoms. Other people have pain, itching and sores around their genitals, anus or mouth. People with genital herpes are able to spread the virus despite having very mild symptoms or no symptoms. Genital herpes can often be spread by skin-to-skin contact during vaginal, anal and oral sex.
Genital herpes is common in the United States. At least 50 million people in the United States—about one in six adults—are infected with HSV. More than one out of every six people aged 14 to 49 years have genital herpes. Genital herpes is more common in women than in men.
Genital herpes can cause outbreaks of blisters or sores on the genitals and anus. Once infected, you can continue to have recurrent episodes of symptoms throughout your life.
There are 2 types of herpes simplex virus (HSV), both viruses can affect either the lips, mouth, genital or anal areas, however:
- Herpes simplex virus type 1 (HSV1) commonly causes cold sores on the lips, mouth or face. However, most people do not have any symptoms. Most people with oral herpes were infected during childhood or young adulthood from non-sexual contact with saliva. Oral herpes caused by HSV-1 can be spread from the mouth to the genitals through oral sex. This is why some cases of genital herpes are caused by HSV-1.
- Herpes simplex virus type 2 (HSV2) causes most genital herpes in the United States 20.
Genital herpes is most easily spread when there are blisters or sores, but can still be passed even if a person has no current blisters or sores or other symptoms. Herpes simplex virus (HSV) also can be present on the skin even if there are no sores. If a person comes into contact with the herpes simplex virus (HSV) on an infected person’s skin, he or she can become infected.
In 2018, there were an estimated 18.6 million people age 18-49 years living with genital herpes caused by herpes simplex virus type 2 (HSV-2), plus several additional million persons living with genital herpes caused by herpes simplex virus type 1 (HSV-1) 21. In 2018 alone, approximately 572,000 persons 18-49 years of age newly acquired HSV-2 in the United States 21. Since genital herpes is not a nationally notifiable condition, the true prevalence (persons living with genital herpes) and incidence (new cases of genital herpes) are difficult to accurately determine.
There is no cure for genital herpes, once you’re infected, you have the virus for the rest of your life. Symptoms often show up again after the first outbreak. Medicine can ease symptoms. It also lowers the risk of infecting others. Condoms can help prevent the spread of a genital herpes infection.
Treatment the first time you have genital herpes
- You may be prescribed antiviral medicine to stop the symptoms getting worse, you need to start taking this within 5 days of the symptoms appearing. You doctor may also give you cream for the pain.
Treatment if the blisters come back
- Go to your doctor or STD clinic if you have been diagnosed with genital herpes and need treatment for an outbreak. Antiviral medicine may help shorten an outbreak by 1 or 2 days if you start taking it as soon as symptoms appear. But outbreaks usually settle by themselves, so you may not need treatment. Recurrent outbreaks are usually milder than the first episode of genital herpes. Over time, outbreaks tend to happen less often and be less severe. Some people never have outbreaks.
- Some people who have more than 6 outbreaks in a year may benefit from taking antiviral medicine for 6 to 12 months. If you still have outbreaks of genital herpes during this time, you may be referred to a specialist.
- If you think you have genital herpes, it is important to see a doctor as soon as possible. Your doctor can confirm the diagnosis with testing and start treatment. Anti-viral medication may help to prevent transmission. Talk to your doctor about this in more detail.
- If you have genital herpes, it is important to always use condoms and dental dams when having sex, even when you have no symptoms. A dental dam is a square of thin latex that can be placed over the vulva or anal area during oral sex. It is safest to avoid sex when you have blisters, sores or symptoms.
- It is also important to tell your sexual partners that you have genital herpes. Your doctor can help you decide who to tell and how to tell them.
- If you’re pregnant: It’s important to tell your obstetrician that you or a partner have had genital herpes, so that they can monitor you for symptoms and manage your pregnancy safely. There is a risk you can pass the virus on to your baby if you have a vaginal delivery during a first attack of genital herpes. If this happens you may be recommended to have a caesarean delivery.
Genital herpes cause
Genital herpes is a sexually transmitted disease (STD) caused by two types of herpes viruses – herpes simplex virus type 1 (HSV-1) and herpes simplex virus type 2 (HSV-2) 2. People with HSV infections can pass along the virus even when they have no visible symptoms.
First-episode genital herpes caused by HSV-1 has been identified with increased frequency among young women, college students, and men who have sex with men 22, 23, 24, 25, 26. Acquisition of genital HSV-1 can occur through genital-genital contact or via receptive oral sex 27, 28. In some settings, such as university campuses, HSV-1 has now replaced HSV-2 as the leading cause of first-episode genital herpes 23. One proposed reason for this shift is decreasing HSV-1 orolabial infection in childhood and early adolescence 25, with first exposure to HSV-1 occurring later in life with sexual activity. Changing sex practices in young adults, namely an increase in oral-genital sex, may also contribute to the changing epidemiology of genital herpes 25. General HSV-1 seroprevalence data, such as reported in the National Health and Nutrition Examination Survey (NHANES) studies, do not provide accurate information on genital herpes infections, since it is not possible to determine whether infection is oral or genital with a positive HSV-1 serologic test. Nevertheless, HSV-1 does contribute significantly to the burden of genital HSV, and there are likely at least several million prevalent genital HSV-1 infections in the United States 21.
How is genital herpes spread?
You can get genital herpes by having vaginal, anal, or oral sex with someone who has the disease, often he/she is unaware that he/she has HSV infection 29, 30, 31.
If you do not have herpes, you can get infected if you come into contact with the herpes virus in 32:
- A herpes sore;
- Saliva (if your partner has an oral herpes infection) or genital secretions (if your partner has a genital herpes infection);
- Skin in the oral area if your partner has an oral herpes infection, or skin in the genital area if your partner has a genital herpes infection.
You can get herpes from a sex partner who does not have a visible sore or who may not know he or she is infected. It is also possible to get genital herpes if you receive oral sex from a sex partner who has oral herpes.
- You will not get herpes from toilet seats, bedding, or swimming pools, or from touching objects around you such as silverware, soap, or towels. If you have additional questions about how herpes is spread, consider discussing your concerns with a healthcare provider.
Risk factors for genital herpes
A higher risk of getting genital herpes is linked to:
- Contact with genitals through oral, vaginal or anal sex. Having sexual contact without using a barrier increases your risk of genital herpes. Barriers include condoms and condom-like protectors called dental dams used during oral sex. Women are at higher risk of getting genital herpes. The virus can spread more easily from men to women than from women to men.
- Having sex with multiple partners. The number of people you have sex with is a strong risk factor. Contact with genitals through sex or sexual activity puts you at higher risk. Most people with genital herpes do not know they have it. Each additional sexual partner raises your risk of being exposed to the virus that causes genital herpes.
- Having a partner who has genital herpes but is not taking medicine to treat it. There is no cure for genital herpes, but medicine can help limit outbreaks.
- Certain groups within the population. Women, people with a history of sexually transmitted diseases, older people, Black people in in the United States and men who have sex with men diagnosed with genital herpes at a higher than average rate. Women are more likely to have genital herpes than are men. The virus is sexually transmitted more easily from men to women than it is from women to men. People in groups at higher risk may choose to talk to a health care provider about their personal risk.
Genital herpes prevention
The only way to avoid sexually transmitted diseases (STDs) is to not have vaginal, anal, or oral sex.
If you are sexually active, you can do the following things to lower your chances of getting genital herpes:
- Be in a long-term mutually monogamous relationship with a partner who is not infected with an STD (e.g., a partner who has been tested and has negative STD test results);
- Using latex condoms the right way every time you have sex.
Be aware that not all herpes sores occur in areas that are covered by a latex condom. Also, herpes virus can be released (shed) from areas of the skin that do not have a visible herpes sore. For these reasons, condoms may not fully protect you from getting herpes.
If you are in a relationship with a person known to have genital herpes, you can lower your risk of getting genital herpes if:
- Your partner takes an anti-herpes medication every day. This is something your partner should discuss with his or her doctor.
- You avoid having vaginal, anal, or oral sex when your partner has herpes symptoms (i.e., when your partner is having an outbreak).
Genital herpes signs and symptoms
The symptoms of genital herpes can vary widely, depending upon whether you are having an initial or recurrent episode. However, many people infected with genital herpes have no symptoms, or have very mild symptoms.
The first time a person has noticeable signs or symptoms of herpes may not be the initial episode. For example, it is possible to be infected for the first time, have few or no symptoms, and then have a recurrent outbreak with noticeable symptoms several years later. For this reason, it is often difficult to determine when the initial infection occurred, especially if a person has had more than one sexual partner. Thus, a current sexual partner may not be the source of the infection.
- Most people infected with HSV don’t know they have it because they don’t have any signs or symptoms or because their signs and symptoms are so mild.
When present, symptoms may begin about two to 12 days after exposure to the virus. If you experience symptoms of genital herpes, they may include:
- Pain or itching. You may experience pain and tenderness in your genital area until the infection clears.
- Small red bumps or tiny white blisters. These may appear a few days to a few weeks after infection.
- Ulcers. These may form when blisters rupture and ooze or bleed. Ulcers may make it painful to urinate.
- Scabs. Skin will crust over and form scabs as ulcers heal.
During an initial outbreak, you may have flu-like signs and symptoms such as swollen lymph nodes in your groin, headache, muscle aches and fever.
Differences in symptom location
Sores appear where the infection entered your body. You can spread the infection by touching a sore and then rubbing or scratching another area of your body, including your eyes.
Men and women can develop sores on the:
- Buttocks and thighs
- Anus
- Mouth
- Urethra (the tube that allows urine to drain from the bladder to the outside)
Women can also develop sores in or on the:
- Vaginal area
- External genitals
- Cervix
Men can also develop sores in or on the:
- Penis
- Scrotum
Genital herpes complications
Complications associated with genital herpes may include:
- Other sexually transmitted infections. Having genital sores increases your risk of transmitting or contracting other sexually transmitted infections, including HIV and AIDS.
- Newborn infection. Babies born to infected mothers can be exposed to the virus during the birthing process. Less often, the virus is passed during pregnancy or by close contact after delivery. Even with treatment, these newborns have a high risk of brain damage, blindness or death for the newborn.
- Bladder problems. In some cases, the sores associated with genital herpes can cause inflammation around the tube that delivers urine from your bladder to the outside world (urethra). The swelling can close the urethra for several days, requiring the insertion of a catheter to drain your bladder.
- Internal inflammatory disease. HSV infection can cause swelling and inflammation within the organs associated with sexual activity and urination. These include the ureter, rectum, vagina, cervix and uterus.
- Meningitis. In rare instances, HSV infection leads to inflammation of the membranes and cerebrospinal fluid surrounding your brain and spinal cord.
- Rectal inflammation (proctitis). Genital herpes can lead to inflammation of the lining of the rectum, particularly in men who have sex with men.
- Finger infection. An HSV infection can spread to a finger through a break in the skin causing discoloration, swelling and sores. The infections are called herpetic whitlow.
- Eye infection. HSV infection of the eye can cause pain, sores, blurred vision and blindness.
- Swelling of the brain. Rarely, HSV infection leads to inflammation and swelling of the brain, also called encephalitis.
- Infection of internal organs. Rarely, HSV in the bloodstream can cause infections of internal organs.
Persons with HSV-2 infection have a threefold increase in the risk of acquiring human immunodeficiency virus (HIV) infection 33. This may be related to open ulcers, or lymphocytes at the site of eruptions, facilitating HIV invasion during sexual contact 34.
Concurrent infection with HSV-2 and HIV increases the severity of HSV episodes and the likelihood of atypical presentations 35. The relationship between genital HSV-1 and HIV infections has not been well studied 36.
Genital herpes diagnosis
Your doctor usually can diagnose genital herpes based history of your sexual activity, a physical exam and the results of certain laboratory tests:
- Viral culture. This test involves taking a tissue sample or scraping of the sores for examination in the laboratory.
- Polymerase chain reaction (PCR) test also called nucleic acid amplification test (NAAT). PCR is used to copy your DNA from a sample of your blood, tissue from a sore or spinal fluid. The DNA can then be tested to establish the presence of HSV and determine which type of HSV you have.
- Antigen detection. The use of direct fluorescent antibody (DFA) testing offers lower sensitivity than viral culture or PCR and is not recommended 37.
- Cytologic examination: Cells infected with HSV will show characteristic changes, and these can be observed by obtaining a sample from the lesion and smearing it on a microscope slide (e.g. Tzanck smear). This test is not recommended due to low sensitivity (less than 80%) and lack of differentiation of HSV-1 from HSV-2.
- Blood test. This test analyzes a sample of your blood for the presence of HSV antibodies to detect a past herpes infection.
To confirm a diagnosis of genital herpes, your doctor will likely take a sample from an active sore. One or more tests of these samples are used to see if you have herpes simplex virus (HSV), infection and show whether the infection is HSV-1 or HSV-2.
Less often, a lab test of your blood may be used for confirming a diagnosis or ruling out other infections.
Your doctor will likely recommend that you get tested for other STDs. Your partner should also be tested for genital herpes and other STDs.
Genital herpes treatment
There’s no cure for genital herpes. Treatment with prescription antiviral medications may:
- Help sores heal sooner during an initial outbreak
- Lessen the severity and duration of symptoms in recurrent outbreaks
- Reduce the frequency of recurrence
- Minimize the chance of transmitting the herpes virus to another
Genital herpes anti-viral medications include 15, 19:
- Acyclovir (Zovirax) 400 mg orally 3 times/day for 7–10 days
- OR
- Valacyclovir (Valtrex) 1 gm orally 2 times/day for 7–10 days
- OR
- Famciclovir 250 mg orally 3 times/day for 7–10 days
* Treatment can be extended if healing is incomplete after 10 days of therapy.
Despite some evidence from animal models that early treatment may impact the long-term natural history of the infection, human trials have shown that oral acyclovir treatment of primary genital herpes does not influence the frequency of subsequent genital recurrences 38, 39.
These antiviral drugs will stop the herpes simplex virus multiplying once it reaches the skin or mucous membranes but cannot eradicate the virus from its resting stage within the nerve cells. They can therefore shorten and prevent episodes while the drug is being taken, but a single course cannot prevent future episodes.
Your doctor may prescribe anti-viral medication to help reduce the severity of genital herpes symptoms. This is most effective when started within 72 hours of the first symptoms.
If you have frequent or severe recurrent episodes there are medications available to help control them.
Other treatments being studied include:
- Imiquimod cream, an immune enhancer
- Human leukocyte interferon alpha cream.
Both appear less beneficial than conventional antiviral drugs.
Your doctor may recommend that you take the medicine only when you have symptoms of an outbreak or that you take a certain medication daily, even when you have no signs of an outbreak. These medications are usually well-tolerated, with few side effects.
- Different formulations of topical antiviral creams are available. They are not generally recommended for genital herpes.
Cold sore
Cold sores also called fever blisters or herpes labialis, are caused by a contagious virus called herpes simplex virus (HSV). Cold sores are tiny, fluid-filled blisters on and around the border of your lips (Figure 6). Cold sores may also appear on other areas of your face, such as your chin or nose. These blisters are often grouped together in patches. After the blisters break, a crust forms over the resulting sore. Cold sores usually heal in two to four weeks without leaving a scar. There are two types of herpes simplex virus. Type 1 herpes simplex virus (HSV-1) usually causes oral herpes, or cold sores. Type 1 herpes simplex virus (HSV-1) infects more than half of the U.S. population by the time they reach their 20s. Type 2 herpes simplex virus (HSV-2) usually affects the genital area. However, either HSV-1 or HSV-2 can affect almost any area of skin or mucous membrane.
Even though they are called cold sores, they have nothing to do with having a cold. You catch a cold sore by coming into close contact with someone who has a cold sore, such as by kissing. Also, not everyone who comes into contact with the virus will get a cold sore. For these people, the virus just never becomes active. But the majority of people who are exposed to a cold sore will have some sort of reaction. It may be that they get one cold sore and never have another. Or they may have cold sore outbreaks several times a year.
After the primary episode of infection, the herpes simplex virus (HSV) resides in a latent state in spinal dorsal root nerves that supply sensation to your skin. During a recurrence, the virus follows the nerves onto the skin or mucous membranes, where it multiplies, causing the clinical lesion. After each attack and lifelong, it enters the resting state.
During an attack, the herpes simplex virus (HSV) can be inoculated into new sites of skin, which can then develop blisters as well as the original site of infection.
Some people have no symptoms from the infection. But others develop painful and unsightly cold sores. Cold sores usually occur outside the mouth, on or around the lips. When they are inside the mouth, they are usually on the gums or the roof of the mouth. They are not the same as canker sores, which are not contagious.
Because cold sores are caused by a virus there is no cure for cold sores. They normally go away on their own in a few weeks. Antiviral medicines can help them heal faster. They can also help to prevent cold sores in people who often get them. Other medicines can help with the pain and discomfort of the sores. These include ointments that numb the blisters, soften the crusts of the sores, or dry them out. Protecting your lips from the sun with sunblock lip balm can also help.
Figure 6. Primary oral herpes (primary herpetic gingivostomatitis) caused by herpes simplex virus type 1
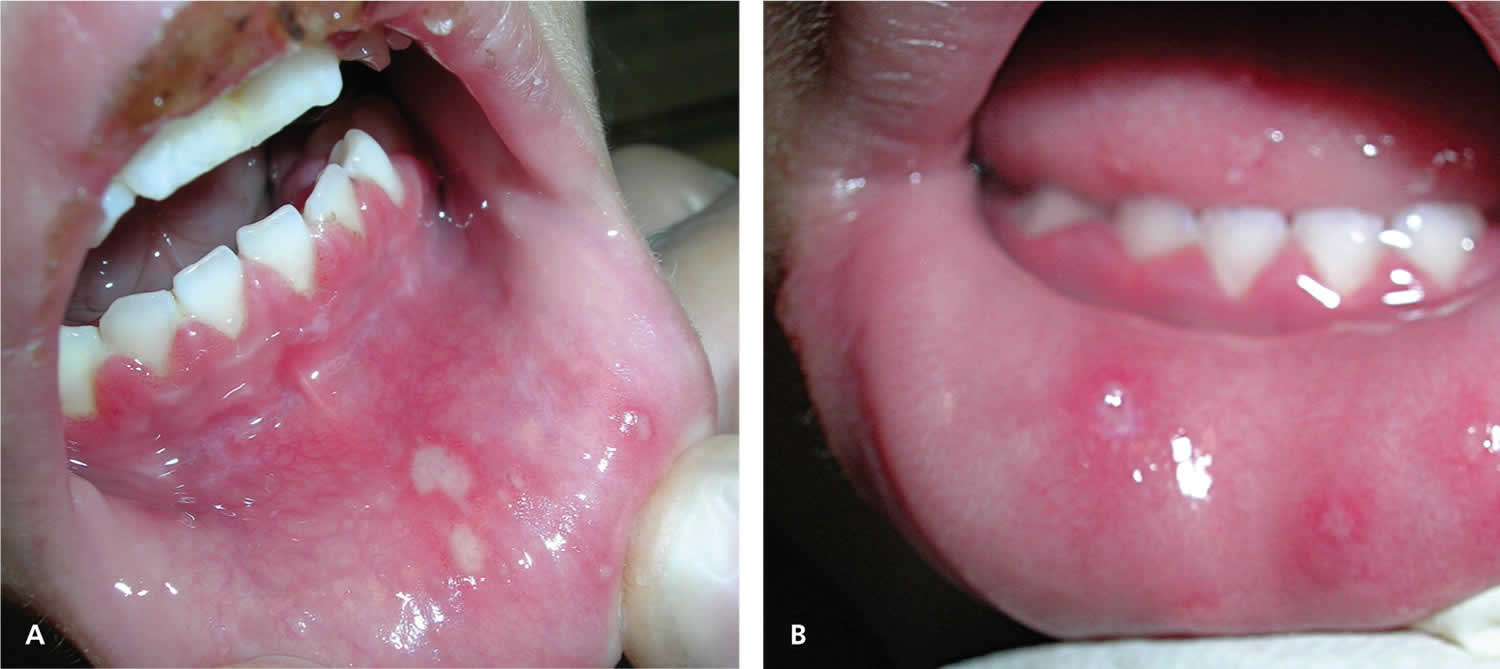
Footnote: (A) a four-year-old girl with lower lip ulcers and crusting on the upper lip, and (B) a two-year-old girl with ulcers on the lower lip and tongue. Both patients show visible gingivitis with reddened, inflamed, and swollen gums.
[Source 40 ]Figure 7. Cold sore on lip
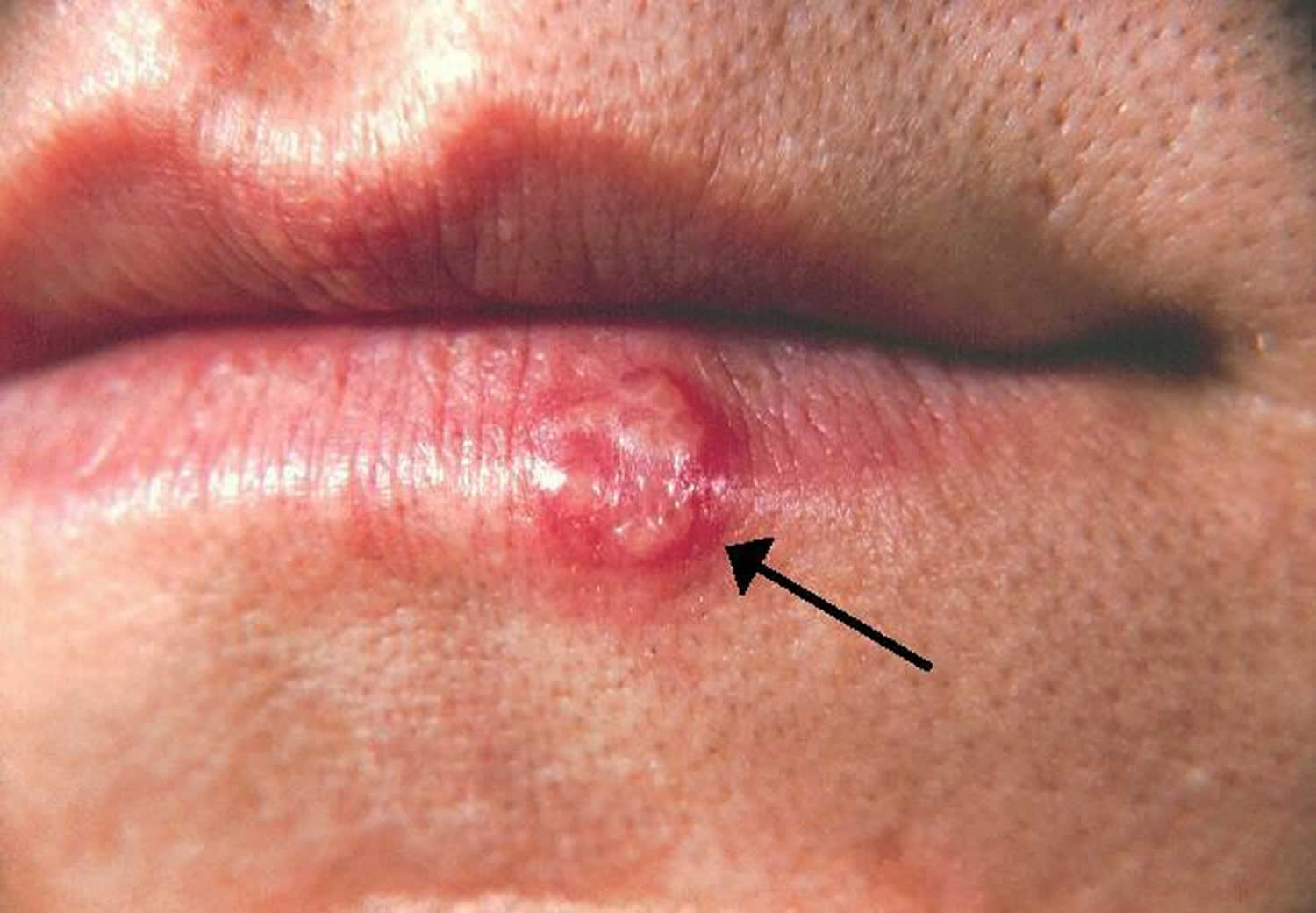
Figure 8. Recurrent herpes simplex virus

Footnote: Young girl with recurrent herpes simplex virus type 1 showing vesicles on a red base at the vermilion border.
[Source 40 ]Figure 9. Recurrent oral herpes
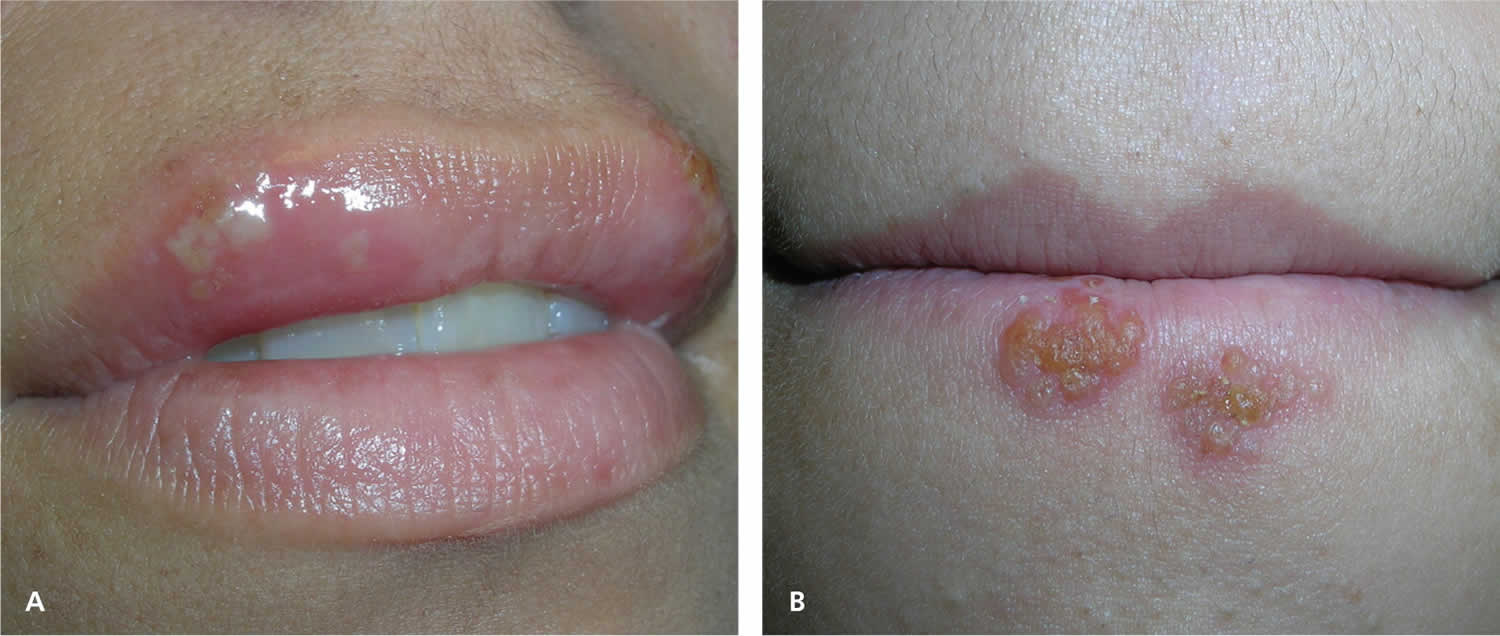
Footnote: (A) Ulcers that form after the vesicles break, as shown in an adult women with herpes labialis. (B) Recurrent herpes simplex virus type 1 in the crusting stage seen at the vermilion border.
[Source 40 ]Figure 10. Oral herpes tongue in a patient with weak immune system causing a severe and large ulcer on tongue

Figure 11. Facial herpes

Cold sores generally clear up without treatment. See your doctor if you have more severe symptoms or a weakened immune system (e.g., you have HIV, on immune suppressant medications or you are having cancer treatment):
- You have a weakened immune system
- The cold sores don’t heal within two weeks
- Symptoms are severe
- You have frequent recurrences of cold sores
- You experience irritation in your eyes
It’s also a good idea to see your doctor if:
- there are signs the cold sore is infected, such as redness around the sore, pus and a fever
- you aren’t sure you have a cold sore
- the cold sore isn’t healing, it’s spreading or you have more than one cold sore
- your cold sore has spread to near your eyes
- you get cold sores often
Antibiotics may be needed if the cold sore gets infected.
Does having cold sore mean I have a sexually transmitted infection?
Having a cold sore does not mean that you have a sexually transmitted infection (STI). Most cold sores are caused by herpes simplex virus type 1 (HSV-1). Genital herpes (a type of STD) is typically caused by HSV-2. However, it is possible to transmit HSV-1 from a cold sore to the genital area during oral sex. In short, it is possible to get genital herpes from a cold sore from oral sex.
Are cold sores herpes?
Yes. Cold sores are caused by herpes simplex virus (HSV). There are two types of herpes simplex virus. Type 1 herpes simplex virus (HSV-1) usually causes oral herpes, or cold sores. Type 1 herpes virus infects more than half of the U.S. population by the time they reach their 20s. Type 2 herpes simplex virus (HSV-2) usually affects the genital area.
Are cold sores contagious?
Yes. Cold sores are contagious even if you don’t see the sores. Cold sores are spread from person to person by close contact, such as kissing. Cold sores are caused by a herpes simplex virus (HSV-1) closely related to the one that causes genital herpes (HSV-2). Both of these viruses can affect your mouth or genitals and can be spread by oral sex.
Can you get genital herpes from a cold sore?
Yes, it is possible to get genital herpes from oral sex.
Genital herpes is caused by the herpes simplex virus (HSV). There are two types of herpes viruses — HSV-1 and HSV-2. Genital herpes is usually caused by HSV-2; oral herpes (cold sores) is usually caused by HSV-1.
However, genital herpes can also be caused by HSV-1. Someone with HSV-1 can transmit the virus through oral contact with another person’s genitals, anus, or mouth, even if they don’t have sores that are visible at the time.
Other than abstinence (not having sex) the best way to help prevent herpes is to use a condom during any type of sex (oral, vaginal, or anal). Girls should have their partners use a dental dam every time they receive oral sex to help protect against genital herpes. And if either partner has a sore, it’s best to not have sex until the sore has cleared up.
How long do cold sores last?
Cold sores usually heal in two to four weeks without leaving a scar.
There’s no cure for herpes simplex virus (HSV) infection, and the blisters may return. Antiviral medications can help cold sores heal more quickly and may reduce how often they return.
What causes cold sores?
Cold sores are caused by certain strains of the herpes simplex virus (HSV). Type 1 herpes simplex virus (HSV-1) usually causes cold sores. Type 2 herpes simplex virus (HSV-2) is usually responsible for genital herpes. However, either type can cause sores in the facial area or on the genitals. Most people who are infected with the herpes simplex virus that causes cold sores never develop signs and symptoms.
HSV-1 is typically spread through direct contact with contaminated saliva or other infected bodily secretions, as opposed to HSV-2, which is spread primarily by sexual contact.
Cold sores are most contagious when oozing blisters are present. But you can transmit the virus to others even if you don’t have blisters. Shared eating utensils, razors and towels, as well as kissing, may spread HSV-1. Oral sex can spread HSV-1 to the genitals and HSV-2 to the lips.
Primary infection appears two to 20 days after contact with an infected person. Transmission involves mucous membranes and open or abraded skin. During one study of herpes labialis, the median duration of HSV-1 shedding was 60 hours when measured by polymerase chain reaction (PCR) and 48 hours when measured by culture 41. Peak viral DNA load occurred at 48 hours, with no virus detected beyond 96 hours of onset of symptoms 41. Recurrent infections may be precipitated by various stimuli, such as stress, fever, sun exposure, extremes in temperature, ultraviolet radiation, immunosuppression, or trauma. The virus remains dormant for a variable amount of time.
Once you’ve had an episode of herpes infection, the virus lies dormant in nerve cells in your skin and may emerge as another cold sore at the same place as before. Recurrence may be triggered by:
- Viral infection or fever
- Hormonal changes, such as those related to menstruation or pregnancy.
- Stress
- Trauma, such as that caused by dental work or cuts from shaving.
- Fatigue
- Surgery.
- Exposure to sunlight and wind
- Changes in your immune system
Oral HSV-1 usually recurs one to six times per year 42. The duration of symptoms is shorter and the symptoms are less severe during a recurrence.
The likelihood of reactivation of HSV infection differs between HSV-1 and HSV-2, and between the sacral and trigeminal anatomic sites. In one study, the mean monthly frequencies of recurrence were 0.33 genital HSV-2 infections, 0.12 orolabial HSV-1 infections, 0.020 genital HSV-1 infections, and 0.001 oral HSV-2 infections 43. This shows that recurrences are more likely when HSV-1 is oral and HSV-2 is genital.
Risk factors for getting cold sores
About 90 percent of adults worldwide — even those who’ve never had symptoms of an infection — test positive for evidence of the herpes simplex virus (HSV) that causes cold sores.
People who have weakened immune systems are at higher risk of complications from the herpes simplex virus (HSV). Medical conditions and treatments that increase your risk of complications include:
- HIV/AIDS
- Severe burns
- Eczema
- Cancer chemotherapy
- Anti-rejection drugs for organ transplants
Cold sore symptoms
Cold sores signs and symptoms vary, depending on whether this is your first outbreak (primary infection) or a recurrence. Primary infection is defined as first outbreak of oral herpes in patients with no existing antibodies to HSV-1 or HSV-2. The most common location for primary oral herpes infection is inside the mouth. In primary HSV, there are painful sores anywhere inside your mouth (herpetic gingivostomatitis) . The lymph nodes in your neck may or may not be swollen. In severe cases of HSV infection, oral herpes may involve the entire lining of your mouth and both lips. These severe infections may be accompanied by fever, sore throat, foul breath, and difficulty eating.
The mouth lesions (herpetic gingivostomatitis) consist of painful vesicles on a red, swollen base that occur on the lips, gingiva, oral palate, or tongue. The lesions ulcerate (Figure 2) and the pain can be severe. Refusal to eat or drink may be a clue to the presence of oral HSV. The lesions usually heal within 10 to 14 days 42.
During first-time oral herpes infection (primary infection), some people experience:
- Fever
- Painful eroded gums
- Sore throat
- Headache
- Muscle aches
- Swollen lymph nodes
Children under 5 years old may have oral herpes inside their mouths and the lesions are commonly mistaken for canker sores. Canker sores involve only the mucous membrane and aren’t caused by the herpes simplex virus.
In recurrent herpes labialis, symptoms of tingling, pain, pins and needles sensation (paresthesias), itching, and burning of the area precede the lesions in 60 percent of persons 42. This may happen 24 to 48 hours before the cold sore actually appears. The lesions then appear as clusters of tiny blisters on the lip or vermilion border (Figures 3 and 4). The tiny blisters may have an erythematous base. The tiny blisters subsequently break open and form a crust (Figure 5). Healing begins within three to four days, and reepithelization may take seven to eight days 42. A typical oral herpes outbreak can last several days, and the blisters can take two to four weeks to heal completely without treatment. However, many people who are exposed to HSV-1 demonstrate asymptomatic seroconversion.
For recurrent oral herpes, locations include the:
- Lips.
- Nose.
- Chin.
- Cheeks.
Recurrences typically appear at the same spot each time and tend to be less severe than the first outbreak. There may also be sores inside your mouth, especially if your immune system has been affected, such as by cancer or HIV, or if you have undergone organ transplantation (Figure 6).
Additionally, some people never develop the symptoms of a primary HSV infection and may mistake a recurrent infection for a primary infection. A recurrent infection typically lasts 7-10 days. As it fades, it may leave a pink, purplish, or brownish color in lighter skin colors. In darker skin colors, HSV may fade to leave a darker brown color. People who are prone to recurrent outbreaks tend to get them 3-4 times per year.
Recurrent oral herpes usually passes through several stages:
- Tingling and itching. Many people feel an itching, burning or tingling sensation around their lips for a day or so before a small, hard, painful spot appears and blisters erupt.
- Blisters. Small fluid-filled blisters typically break out along the border where the outside edge of the lips meets the skin of the face. Cold sores can also occur around the nose or on the cheeks.
- Oozing and crusting. The small blisters may merge and then burst, leaving shallow open sores that will ooze fluid and then crust over.
Symptoms of recurrent oral herpes are typically milder than those of primary infection, with a 24-hour prodrome of tingling, burning, and itch 44. Recurrent orolabial HSV-1 infections classically affect the vermillion border of the lip (as opposed to the mouth and lips as seen in primary infection) 45.
Cold sores complications
In some people, herpes simplex virus (HSV) that causes cold sores can cause problems in other areas of the body, including:
Eye infection
Herpes simplex may cause swollen eyelids and conjunctivitis with opacity and superficial ulceration of the cornea (dendritic ulcer, best seen after fluorescein staining of the cornea). HSV infection of the eye also known as herpetic keratitis is a common cause of blindness in the United States 46, 47, 48, 49. Common symptoms are eye pain, light sensitivity, and discharge with gritty sensation in the eye. Fluorescein stain with a ultraviolet light may show a classic dendritic ulcer on the cornea (Figure 8). Without prompt treatment, scarring of the cornea may occur (Figure 9).
Figure 12. HSV infection of the eye

Footnote: Slit-lamp view of a dendritic ulcer with fluorescein uptake from herpetic keratitis.
[Source 50 ]Figure 13. Herpetic keratitis with corneal scarring
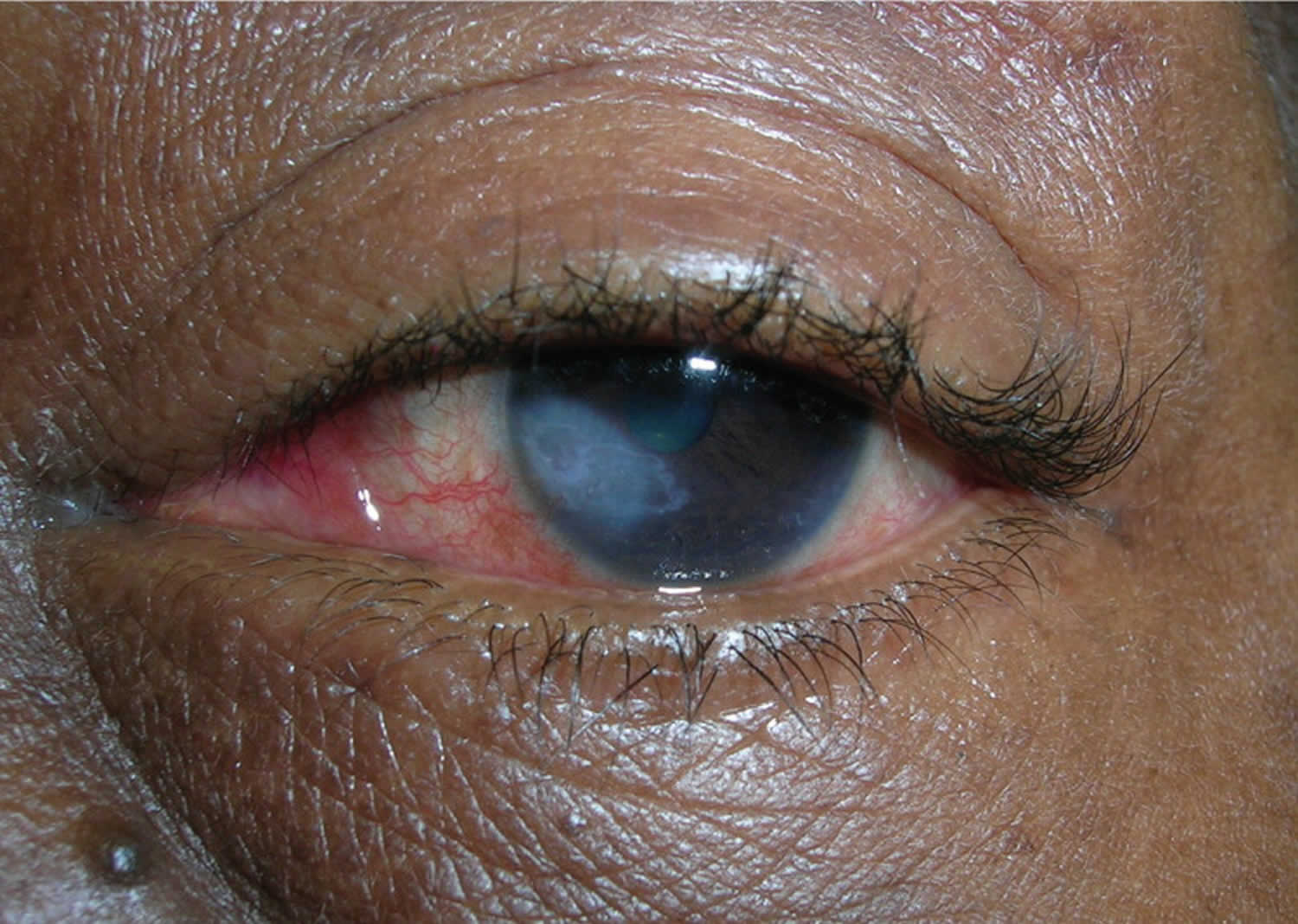
Footnote: Herpetic keratitis with corneal scarring in a 56-year-old woman
[Source 40 ]Throat infection
Throat infections may be very painful and interfere with swallowing.
Eczema herpeticum
In patients with a history of atopic dermatitis, Darier disease, Hailey-Hailey disease, mycosis fungoides, and all types of ichthyosis, herpes simplex virus (HSV) may result in severe and widespread infection, known as eczema herpeticum. The skin disease can be active or historical. Numerous blisters erupt on the face or elsewhere, associated with swollen lymph glands and fever. The increased risk is also associated with mutations in the filaggrin gene, which is seen in atopic dermatitis and ichthyosis vulgaris. Pharmaceutical risk factors for eczema herpeticum include the use of topical calcineurin inhibitors such as pimecrolimus and tacrolimus.
Erythema multiforme
A single episode or recurrent erythema multiforme is an uncommon reaction to herpes simplex. The rash of erythema multiforme appears as symmetrical plaques on hands, forearms, feet and lower legs. It is characterized by target lesions, which sometimes have central blisters. Mucosal lesions may be observed.
Nervous system
Cranial or facial nerves may be infected by herpes simplex virus (HSV), producing temporary paralysis of the affected muscles. Rarely, neuralgic pain may precede each recurrence of herpes by 1 or 2 days (Maurice syndrome). Meningitis is rare. A major risk factor for herpes encephalitis is mutations in the toll-like receptor (TLR-3) or UNC-93B genes 44. It has been postulated that these mutations inhibit normal interferon-based responses.
Widespread infection
Disseminated infection and/or persistent ulceration due to herpes simplex virus (HSV) can be serious in debilitated or immune deficient patients, for example in people with human immunodeficiency virus (HIV) infection, transplant recipients (solid organ or hematopoietic stem cells) or leukemia/lymphoma patients 51, 52.
In the immunocompromised patient population, HSV infection can result in severe and chronic infection. The most common presentation of severe and chronic HSV infection is quickly enlarging ulcerations or verrucous/pustular lesions. It is not uncommon for patients to have respiratory or gastrointestinal tract involvement and present with shortness of breath (dyspnea) or difficulty or painful swallowing (dysphagia) 53, 54, 55, 56.
Neonatal herpes
Neonatal herpes can occur when an infant is exposed to HSV during vaginal delivery. Neonatal herpes simplex virus infection is rare, occurring in an estimated 1 in 1000 newborns in the United States. However, it is a serious condition that can lead to lasting neurologic disability or death. Women with recurrent genital herpes have a low risk of vertically transmitting HSV to their newborn baby. However, risk for neonatal herpes is greatest when a mother acquires HSV for the first time in late pregnancy.
Cold sore prevention
Cold sores cannot always be avoided, but you may be able to help prevent them by treating them as at the very first sign of a cold sore (usually the tingling stage). You also can try to avoid known cold sore triggers (some of these are unavoidable).
- Sunlight
- Stress
- Hormones
- Fatigue
- Fever
- A weak immune system or changes in your immune system
Wearing sunscreen and proactively managing stress may help. Ways to reduce stress include exercising, meditating, and doing things you enjoy each day. You should also try to get 7 to 8 hours of sleep each night.
Because the herpes simplex virus (HSV) is very contagious, it is important to take the following steps to prevent spread (transmission) of the virus during the prodromal phase (burning, tingling, or itching) and active phase (presence of blisters or sores) of HSV infections:
- Avoid sharing cups and eating utensils.
- Avoid kissing and performing oral sex.
- Avoid sharing lip balm and lipstick.
- Avoid sharing razors, towels, and other personal care items.
- Wash your hands with soap and water if you touch an active lesion.
Unfortunately, the virus can still be transmitted even when someone does not have active lesions.
Cold sores diagnosis
Your doctor can usually diagnose cold sores just by looking at them (grouped vesicles or ulcers on an erythematous base). To confirm the diagnosis, he or she may take a sample from the blister for testing in a laboratory by culture or polymerase chain reaction (PCR) of a viral swab taken from fresh vesicles. The most sensitive and specific mechanism is viral polymerase chain reaction (PCR). Herpes simplex virus (HSV) serology is not very informative, as it’s positive in most individuals and thus not specific for the lesion with which they present. Viral culture, direct fluorescent antibody (DFA) assay, and Tzanck smear are alternative methods of diagnosing. It is important to note that the Tzanck smear identifies multinucleated giant cells, so it cannot distinguish between HSV and varicella zoster virus (VZV) 44. The direct fluorescent antibody (DFA) assay, however, can distinguish between the 2 entities 57.
Cold sore treatment
Cold sores generally clear up without treatment in two to four weeks. Cold sore treatment includes managing outbreaks with over-the-counter (OTC) creams to prescription drugs to home remedies that include ice packs and aloe vera gels. Which you choose will depend on how many outbreaks you have and what works best for you.
For episodic treatment, oral antiviral agents, such as acyclovir (Zovirax), valacyclovir (Valtrex) and famciclovir (Famvir), are superior to topical antiviral therapy 58. Valacyclovir and famciclovir have greater oral bioavailability and are better absorbed than acyclovir, require less frequent dosing, but are more expensive and are not approved for children 58. Topical antiviral agents such as 5% acyclovir cream/ointment (Zovirax) ± hydrocortisone (Xerese), 1% penciclovir (Denavir) cream, and 50 mg Buccal Adhesive Tablet (ABT-50 mg) can also be used for episodic treatment of herpes labialis 58. These topical agents are not effective in the prevention of recurrent herpes labialis. For chronic daily suppressive therapy, oral antivirals are the treatment of choice 58.
Prescription medicines
If you have several outbreaks a year, you should see your family doctor. They will work with you on a treatment plan that may include prescription antiviral medicine. Oral antiviral medications include:
- Acyclovir (Zovirax) – 200 mg 5 times daily for five days
- OR
- Acyclovir (Zovirax) – 400 mg 3 times daily for five days
- OR
- Famciclovir (Famvir) – as a single dose of 3 x 500 mg
- OR
- Valacyclovir (Valtrex) – 1 g 3 times daily for seven days
- OR
- Valacyclovir (Valtrex) – 2 grams twice daily for one day
Some of these products are packaged as pills to be swallowed. Others are creams to be applied to the sores several times a day. In general, the pills work better than the creams. For very severe infections, some antiviral drugs can be given with an injection. These medicines not only help speed healing, they also may prevent future outbreaks.
Topical aciclovir or penciclovir may shorten attacks of recurrent herpes simplex, provided the cream is started early enough.
Higher doses of antiviral drugs are used for eczema herpeticum or for disseminated herpes simplex.
Your doctor may also prescribe you a numbing gel if your cold sore is painful.
OTC treatments
If your outbreaks aren’t as severe or frequent, an OTC medicine should help soothe and heal your cold sore. There are a variety of OTC creams, gels, patches, lip balms, and even lasers designed to minimize symptoms and shorten the cold sore cycle. A small sampling of popular products include:
- Creams, gels and ointments containing the drugs aciclovir (Zovirax cream 5%) or penciclovir (Denavir) are available in pharmacies without a prescription. For them to be able to work, they have to be applied to the affected area every 2 to 3 hours during the daytime. The treatment lasts five days, but should not exceed 10 days 59.
- Docosanol (Abreva) is an FDA approved cream safe for people 12 years of age and older. If you begin using it at first tingle, it can shorten healing time. It also helps minimize symptoms.
- Zilactin Cold Sore Gel relieves pain and promotes healing with an active ingredient of 10% benzyl alcohol. The gel creates a protective barrier over your cold sore.
- Orajel Cold Sore Patented Treatment is a liquid treatment with touch-free applicator. It cleans the affected area and provides pain relief.
- Mederma cold sore patch uses hydrocolloid gel to boost recovery and reduce scab formation.
- Compeed Cold Sore Patch conceals your cold sore while it heals it. The patch also helps prevent speading your cold sore to others.
- Laser treatment is the latest—and priciest—treatment to enter the market. The Virulite Invisible Light Electronic Cold Sore Treatment Device is FDA approved to treat your cold sore at home. Treatments may result in clearing cold sore in a matter of days.
- Acetaminophen (Tylenol) and ibuprofen (Advil) both help relieve cold sore pain.
There is also a combination drug (Zovirax Duo) that contains both aciclovir and a mild steroid 60, 61, 62. One study looked into whether this combination drug can lower the risk of cold sore blisters and scabs forming 62. The combination drug (Zovirax Duo) that contains both aciclovir and a mild steroid was either compared with aciclovir used alone or with a non-medicated cream (placebo). The people in the study had an average of 5 to 6 cold sores per year, and their cold sores often crusted over and formed scabs. They started using the treatment as soon as they noticed the first signs of a cold sore developing. The study suggests that the combination of aciclovir and a steroid is somewhat more effective than aciclovir alone 62. In other words, compared to aciclovir alone, the combination drug (Zovirax Duo that contain both aciclovir and a mild steroid) prevented the development of blisters and scabs in an extra 7 out of 100 people 62. Topical treatments for cold sores can sometimes irritate the skin a bit, but no serious side effects occurred in the studies.
To ease the discomfort of a cold sore:
- Try other cold sore remedies. Some over-the-counter preparations contain a drying agent, such as alcohol, that may speed healing.
- Use lip balms and cream. Protect your lips from the sun with a zinc oxide cream or lip balm with sunblock. If your lips become dry, apply a moisturizing cream.
- Apply a cool compress. A cool, damp cloth may reduce redness, help remove crusting and promote healing.
- Apply pain-relieving creams. Over-the-counter creams with lidocaine or benzocaine may offer some pain relief.
Home remedies for cold sores
There are many home remedies for treating a cold sore. Some may be effective. However, there is no medical evidence that these methods can shorten healing time or provide pain relief.
- Aloe vera gel
- Vitamins C and vitamin E
- Tea tree oil
- Peppermint oil
- Lemon balm
- Vanilla extract
- Tea bag
- Ice
- Lysine. An amino acid, lysine is available as an oral supplement and as a cream.
- Propolis. Also known as synthetic beeswax, this is available as a 3 percent ointment. When applied early and often, it may shorten the duration of the breakout.
- Rhubarb and sage. A cream combining rhubarb and sage may be about as effective as acyclovir (Zovirax) cream.
- Stress reduction. If your cold sores are triggered by stress, you might want to try relaxation techniques, such as deep-breathing exercises and meditation.
Whichever treatment you choose for your cold sore, know that it has the best chance of working if you start it during the tingling stage.
Recurring cold sores treatment
Oral acyclovir is effective in suppressing herpes labialis in immunocompetent adults with frequent recurrences. In one randomized control trial, treatment with oral acyclovir (400 mg twice per day) resulted in a 53 percent reduction in the number of clinical recurrences and a 71 percent reduction in virus culture-positive recurrences compared with placebo 63. The median time to first clinically documented recurrence was 46 days for placebo courses and 118 days for acyclovir courses 63. The mean number of recurrences per four-month treatment period was 1.80 episodes per patient during placebo treatment and 0.85 episodes per patient during acyclovir treatment 63.
Treatment with oral valacyclovir (500 mg per day) for 16 weeks was compared with placebo in the suppression of herpes labialis in patients with a history of four or more recurrent lesions in the previous year 64. Results showed 60 percent of persons in the valacyclovir group were recurrence-free throughout the study period compared with 38 percent in the placebo group. The mean time to first recurrence was longer with valacyclovir (13.1 weeks) compared with placebo (9.6 weeks) 64.
In a Cochrane review of herpes labialis prevention in patients receiving treatment for cancer, acyclovir was found to be effective in the prevention of HSV infections, as measured by oral lesions or viral isolates 65. There was no evidence that valacyclovir is more effective than acyclovir. In another study, daily valacyclovir (500 mg per day) and acyclovir (400 mg twice per day) were equally effective in the prevention of recurrent HSV eye disease 66.
Herpetic whitlow
Herpetic whitlow also known as digital herpes simplex, finger herpes, or hand herpes, is a painful herpes simplex virus (HSV) infection occurring on the fingers or around the fingernails. Herpetic whitlow is usually seen in children who suck their thumbs and adolescents and young adults following genital herpes exposure 67. In children, herpetic whitlow tends to co-occur with gingivostomatitis aphthosa. Infections with HSV (herpes simplex virus) are very contagious and are easily spread by direct contact with infected skin lesions. Oral secretions are usually a source of infection, so, among adults, health care workers (medical or dental) who are exposed to patients’ oral mucosa while not wearing gloves and athletes engaging in contact sports (e.g., rugby players or wrestlers) are at risk for viral exposure 68. Herpes simplex virus infection usually appears as small blisters or sores around the mouth, nose, genitals, and buttocks, though infections can develop almost anywhere on the skin. Furthermore, these tender sores may recur periodically in the same sites.
People develop herpetic whitlow when they come into contact with areas already infected with HSV, either on their own bodies or on someone else’s body. Usually, there is a break in the skin, especially a torn cuticle at the base of the fingernail, which allows the virus to enter the finger tissue and establish an infection. HSV-1 causes approximately 60% of herpetic whitlow infections, while HSV-2 causes the remaining 40%.
Herpetic whitlow can affect people of all ages, of all races, and of both sexes. However, it is more common in children and in dental and medical workers. Children often contract herpetic whitlow as a result of thumb- or finger-sucking when they have a herpes infection of the lips or mouth. Dental and medical workers may contract herpetic whitlow by touching the contagious lesions of a patient with herpes simplex virus infection. In these groups of people—children and health care workers—herpetic whitlow is most commonly caused by HSV-1. In everyone else, herpetic whitlow is usually caused by infection with HSV-2.
Herpetic whitlow should be distinguished from other infectious diseases (e.g., bacterial whitlow) because of the different treatments required 69. There is no cure for herpes simplex virus infection. Antiviral medication has been widely accepted as effective in reducing the duration of symptoms in primary infection and in recurrent episodes. However, there are no controlled studies showing the optimal doses of antiviral agents for treating herpetic whitlow 70.
Untreated herpes simplex virus infections will go away on their own, but medications can reduce the symptoms and shorten the duration of outbreaks.
Figure 14. Herpetic whitlow
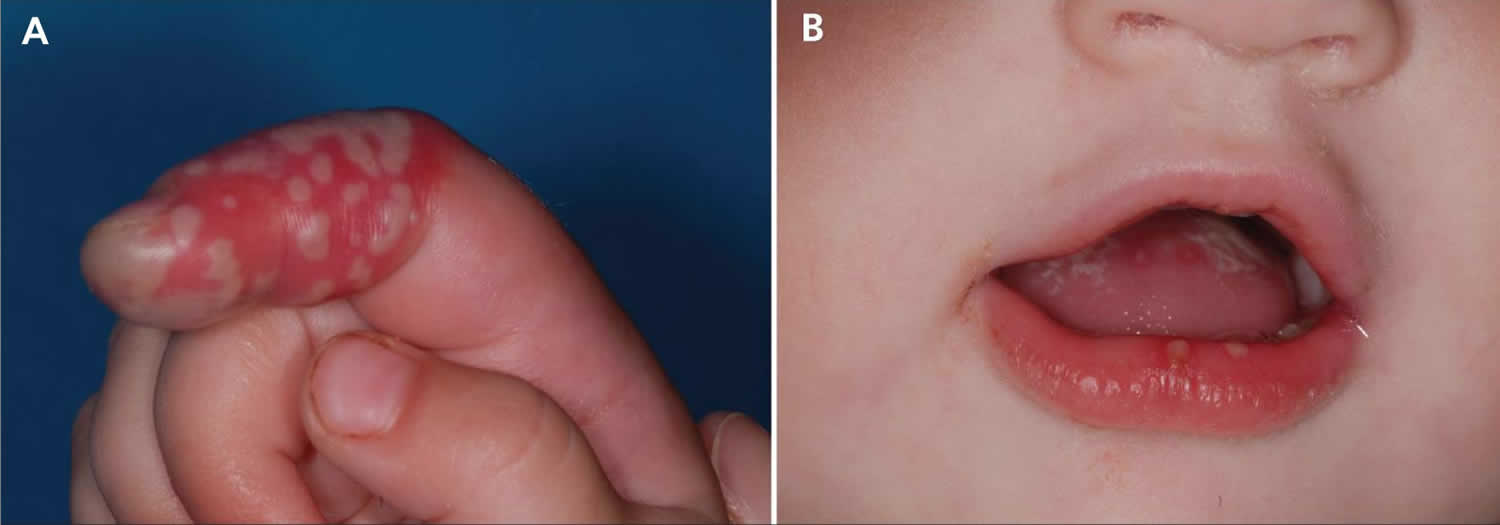
Footnote: (A) Swelling and redness with grouped vesicular lesions and pustulation on the right forefinger of a 14-month-old girl. (B) The patient also presented with gingivitis and stomatitis, appearing as vesicles with a red halo and discrete ulcers on her lower lip and tongue.
[Source 67 ]Figure 15. Herpetic whitlow thumb

Footnote: Severely painful herpetic whitlow with large vesicles on the thumb
[Source 71 ]Figure 16. Herpetic whitlow finger

Is herpetic whitlow contagious?
Yes. Infections with herpes simplex virus (HSV) are very contagious and are easily spread by direct contact with infected skin lesions. Because herpes simplex virus infections are very contagious, it is important to take the following steps to prevent spread (transmission) of the virus during the prodrome phase (burning, tingling, or itching) and active phase (presence of blisters or sores) of herpetic whitlow:
- Avoid sharing towels and other personal care items
- Cover the affected finger with a bandage
- Wear gloves if you are a health care provider
- Don’t pop any blisters—it may make the condition worse
Unfortunately, the herpes simplex virus can still be transmitted even when someone does not have active lesions. However, this is very unusual for patients with herpetic whitlow.
Herpetic whitlow causes
Herpetic whitlow is caused by one of two types of herpes simplex virus (HSV), members of the Herpesvirales family of double-stranded DNA viruses 72.
- Type 1 HSV is mainly associated with oral and facial infections
- Type 2 HSV is mainly associated with genital and rectal infections (anogenital herpes)
However, either virus can affect almost any area of skin or mucous membrane.
After the primary episode of infection, HSV (herpes simplex virus) resides in a latent state in spinal dorsal root nerves that supply sensation to the skin. During a recurrence, the virus follows the nerves onto the skin or mucous membranes, where it multiplies, causing the clinical lesion. After each attack and lifelong, it enters the resting state.
During an attack, the virus can be inoculated into new sites of skin, which can then develop blisters as well as the original site of infection.
Primary attacks of Type 1 HSV infections occur mainly in infants and young children. In crowded, underdeveloped areas of the world, nearly all children have been infected by the age of 5. In less crowded places, the incidence is lower; for example, less than half of university entrants in Britain have been infected. Type 2 HSV infections occur mainly after puberty and are often transmitted sexually.
HSV is transmitted by direct or indirect contact with someone with active herpes simplex, which is infectious for 7–12 days. Asymptomatic shedding of the virus in saliva or genital secretions can also lead to transmission of HSV, but this is infrequent, as the amount shed from inactive lesions is 100 to 1000 times less than when it is active. The incubation period is 2–12 days.
Minor injury helps inoculate herpes simplex virus (HSV) into the skin. For example:
- A thumb sucker may transmit the virus from their mouth to their thumb.
- A health-care worker may develop herpetic whitlow (paronychia)
- A rugby player or wrestler may get a cluster of blisters on one cheek (‘scrumpox’).
Herpetic whitlow signs and symptoms
The most common locations for herpetic whitlow include:
- Thumb
- Index finger
- Other fingers
Approximately 2–20 days after initial exposure to the herpes simplex virus, the infected area develops burning, tingling, and pain (prodromal phase). Over the next week or 2, the finger becomes red and swollen. Small (1–3 mm) fluid-filled blisters develop, often clustered together on a bright red base. The infection usually involves just one finger but has rarely been noted to involve several fingers. Vesicles usually coalesce into large, honeycomb-like bullae. They may spread proximally and may involve the nail bed where hemorrhagic or purpuric lesions may be noted. Patients will often report a disproportionate intensity of pain, particularly if there is nailbed involvement. Fever, lymphadenitis, epitrochlear and axillary lymphadenopathy may be present. Rarely, lymphedema of the hand and forearm may be present, although reports favor bacterial superinfection in most of these cases.
Vesicular fluid is clear early on but may become turbid, seropurulent, or hemorrhagic as it progresses. There will never be frank pus unless a bacterial superinfection is present. In immunocompromised patients (particularly AIDS with CD4 less than 50), ulceration and necrosis may be seen.The blisters usually rupture and scab over, leading to complete healing after an additional 2 weeks.
Other symptoms occasionally associated with the primary infection of herpetic whitlow include:
- Fever
- Red streaks radiating from the finger (lymphangitis)
- Swollen lymph nodes in the elbow or underarm area
If a person contracts herpetic whitlow from himself or herself (autoinoculation), then he or she is likely to have a primary herpes simplex virus infection of the mouth area or of the genital area.
Repeat (recurrent) herpes simplex virus infections are often milder than the primary infection, though they look alike. A recurrent infection typically lasts 7–10 days. Recurrent herpetic whitlow is rare.
However, people with recurrent herpes simplex virus infections may report that the skin lesions are preceded by sensations of burning, itching, or tingling (prodrome). About 24 hours after the prodrome symptoms begin, the actual lesions appear as one or more small blisters, which eventually open up and become scabbed over.
Triggers of recurrent herpes simplex virus infections include:
- Fever or illness
- Sun exposure
- Hormonal changes, such as those due to menstruation or pregnancy
- Stress
- Trauma
- Surgery
In many cases, no reason for the eruption is evident.
The vesicles tend to be smaller and more closely grouped in recurrent herpes, compared to primary herpes. They usually return to roughly the same site as the primary infection.
- Recurrent Type 1 HSV can occur on any site, most frequently the face, particularly the lips (herpes simplex labialis).
- Recurrent Type 2 HSV may also occur on any site, but most often affects the genitals or buttocks.
Itching or burning is followed an hour or two later by an irregular cluster of small, closely grouped, often umbilicated vesicles on a red base. They normally heal in 7–10 days without scarring. The affected person may feel well or suffer from fever, pain and have enlarged local lymph nodes.
Herpetic vesicles are sometimes arranged in a line rather like shingles and are said to have a zosteriform distribution, particularly when affecting the lower chest or lumbar region.
White patches or scars may occur at the site of recurrent HSV attacks and are more evident in those with the skin of color.
Herpetic whitlow diagnosis
Most herpes simplex virus infections are easy for doctors to diagnose. On occasion, however, a swab from the infected skin may be sent to the laboratory for viral culture, which takes a few days to grow or PCR (polymerase chain reaction enzyme-linked immunosorbent assay). A Tzank test consists of scraping the floor of a herpetic vesicle, staining the specimen, and looking for multinucleated “balloon” giant cells, with as high as approximately 70% sensitivity and high specificity for the disease 73. Blood tests may also be performed, but herpes simplex virus serology is not very informative, as it’s positive in most individuals and thus not specific for the lesion with which they present.
Herpetic whitlow treatment
Symptomatic relief and avoidance of secondary infection are the mainstays of therapy for herpetic whitlow. If you develop a tender, painful sore on the finger, see a doctor, especially if it is not going away or if it seems to be getting worse. You should definitely seek medical attention if you have a finger sore as well as typical symptoms of oral or genital herpes.
There is no cure for herpes simplex virus infection.
Untreated herpes simplex virus infections will go away on their own, but medications can reduce the symptoms and shorten the duration of outbreaks. The natural course of the infection in an immunocompetent patient is a spontaneous resolution of symptoms in 2 to 4 weeks 74.
Although herpetic whitlow symptoms will eventually go away on their own, your physician may prescribe antiviral medications in order to help relieve symptoms and to prevent spread of the infection to other people:
- Acyclovir pills
- Valacyclovir pills
- Famciclovir pills
- Topical acyclovir ointment
These medications are usually taken for 7–14 days.
More severe herpetic whitlow may require oral antibiotic pills if the area(s) are also infected with bacteria.
While there are few studies specific to herpetic whitlow, antivirals have been shown to shorten the duration of symptoms by up to 4 days in one study and decreased days of positive viral culture. Data is especially favorable if the antiviral is started within 48 hours of onset of symptoms. For recurrent herpetic whitlow, suppressive therapy with an antiviral agent may be helpful. Treatment with acyclovir, famciclovir, or valacyclovir has not been specifically compared. Antibiotics must be considered in a secondarily infected digit.
Viral shedding is present until the epidermal lesion is healed, so patients should be counseled on the importance of wearing gloves or another protective barrier. The patient should also be counseled that the chance of recurrence is about 30% to 50%.
Although it is rare, recurrent herpetic whitlow can be treated with the same oral antiviral medications:
- Acyclovir pills
- Valacyclovir pills
- Famciclovir pills
- Topical acyclovir ointment
People who experience early signs (prodromes) before recurrent infections may benefit from episodic treatment, by starting to take medication after the onset of tingling and burning but before the appearance of blisters and sores.
Very rarely, individuals may have recurrent herpetic whitlow outbreaks that are frequent enough or severe enough to justify suppressive therapy, in which medications are taken every day in order to decrease the frequency and severity of attacks.
Incision and drainage should not be performed as it provides no symptomatic relief and may cause viremia and bacterial superinfection 74. There have been reports of significant pain relief following nail segment excision for decompression of vesicles along the nail bed 75.
Herpetic whitlow natural treatment
Acetaminophen (paracetamol) or ibuprofen may help reduce fever and pain caused by the herpes simplex virus sores. Applying cool compresses or ice packs may also relieve some of the swelling and discomfort.
Because herpes simplex virus infections are very contagious, it is important to take the following steps to prevent spread (transmission) of the virus during the prodrome phase (burning, tingling, or itching) and active phase (presence of blisters or sores) of herpetic whitlow:
- Avoid sharing towels and other personal care items
- Cover the affected finger with a bandage
- Wear gloves if you are a health care provider
- Don’t pop any blisters—it may make the condition worse
Unfortunately, the herpes simplex virus can still be transmitted even when someone does not have active lesions. However, this is very unusual for patients with herpetic whitlow.
Herpetic whitlow prognosis
Herpetic finger infection is classically self-limited and usually resolve in 2 to 4 weeks for primary infection. After the acute stage, the pain abates, and the vesicles begin to dry and crust. Usually, the pain resolves in about 14 days, and remaining skin changes continue to heal after that. Fingers and nails typically completely heal with no further issues, although there are reports of residual scarring, numbness, and hypersensitivity.
A recurrent outbreak due to latent sensory ganglion infection has been noted in up to 30% to 50% of cases.
References- Centers for Disease Control and Prevention Public Health Image Library. Dr. Fred Murphy & Sylvia Whitfield, 1975.
- Genital Herpes – CDC Detailed Fact Sheet. https://www.cdc.gov/std/herpes/stdfact-herpes-detailed.htm
- Shingles. https://www.cdc.gov/dotw/shingles
- Shingles Vaccination. https://www.cdc.gov/vaccines/vpd/shingles/public/shingrix/index.html
- Shingrix Recommendations. https://www.cdc.gov/vaccines/vpd/shingles/hcp/shingrix/recommendations.html
- What You Need to Know About Shingles and the Shingles Vaccine. https://www.cdc.gov/vaccines/hcp/adults/downloads/fs-shingles.pdf
- Harpaz R, Ortega-Sanchez IR, Seward JF. Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2008;57(RR-5):1-30; quiz CE32-34.
- Corey L, Wald A. Maternal and neonatal herpes simplex virus infections. N Engl J Med. 2009 Oct 1;361(14):1376-85. doi: 10.1056/NEJMra0807633. Erratum in: N Engl J Med. 2009 Dec 31;361(27):2681. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2780322
- Matthias J, du Bernard S, Schillinger JA, Hong J, Pearson V, Peterman TA. Estimating Neonatal Herpes Simplex Virus Incidence and Mortality Using Capture-recapture, Florida. Clin Infect Dis. 2021 Aug 2;73(3):506-512. doi: 10.1093/cid/ciaa727
- Slutsker JS, Schillinger JA. Assessing the Burden of Infant Deaths Due to Herpes Simplex Virus, Human Immunodeficiency Virus, and Congenital Syphilis: United States, 1995 to 2017. Sex Transm Dis. 2021 Aug 1;48(8S):S4-S10. doi: 10.1097/OLQ.0000000000001458
- Kimberlin DW, Baley J; Committee on Infectious Diseases; Committee on Fetus and Newborn. Guidance on management of asymptomatic neonates born to women with active genital herpes lesions. Pediatrics. 2013 Feb;131(2):383-6. doi: 10.1542/peds.2012-3217
- Pinninti SG, Kimberlin DW. Maternal and neonatal herpes simplex virus infections. Am J Perinatol. 2013 Feb;30(2):113-9. doi: 10.1055/s-0032-1332802
- Brown ZA, Selke S, Zeh J, Kopelman J, Maslow A, Ashley RL, Watts DH, Berry S, Herd M, Corey L. The acquisition of herpes simplex virus during pregnancy. N Engl J Med. 1997 Aug 21;337(8):509-15. doi: 10.1056/NEJM199708213370801
- Brown ZA, Wald A, Morrow RA, Selke S, Zeh J, Corey L. Effect of serologic status and cesarean delivery on transmission rates of herpes simplex virus from mother to infant. JAMA. 2003 Jan 8;289(2):203-9. doi: 10.1001/jama.289.2.203
- Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021 Jul 23;70(4):1-187. doi: 10.15585/mmwr.rr7004a1
- Kimberlin DW, Whitley RJ, Wan W, Powell DA, Storch G, Ahmed A, Palmer A, Sánchez PJ, Jacobs RF, Bradley JS, Robinson JL, Shelton M, Dennehy PH, Leach C, Rathore M, Abughali N, Wright P, Frenkel LM, Brady RC, Van Dyke R, Weiner LB, Guzman-Cottrill J, McCarthy CA, Griffin J, Jester P, Parker M, Lakeman FD, Kuo H, Lee CH, Cloud GA; National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study Group. Oral acyclovir suppression and neurodevelopment after neonatal herpes. N Engl J Med. 2011 Oct 6;365(14):1284-92. doi: 10.1056/NEJMoa1003509
- James SH, Kimberlin DW. Neonatal herpes simplex virus infection: epidemiology and treatment. Clin Perinatol. 2015 Mar;42(1):47-59, viii. doi: 10.1016/j.clp.2014.10.005
- Schiffer JT, Corey L. New concepts in understanding genital herpes. Curr Infect Dis Rep. 2009 Nov;11(6):457-64. doi: 10.1007/s11908-009-0066-7
- Genital Herpes. https://www.cdc.gov/std/treatment-guidelines/herpes.htm
- Gnann JW Jr, Whitley RJ. CLINICAL PRACTICE. Genital Herpes. N Engl J Med. 2016 Aug 18;375(7):666-74. doi: 10.1056/NEJMcp1603178
- Spicknall IH, Flagg EW, Torrone EA. Estimates of the Prevalence and Incidence of Genital Herpes, United States, 2018. Sex Transm Dis. 2021 Apr 1;48(4):260-265. doi: 10.1097/OLQ.0000000000001375
- Ryder N, Jin F, McNulty AM, Grulich AE, Donovan B. Increasing role of herpes simplex virus type 1 in first-episode anogenital herpes in heterosexual women and younger men who have sex with men, 1992-2006. Sex Transm Infect. 2009 Oct;85(6):416-9. doi: 10.1136/sti.2008.033902
- Roberts CM, Pfister JR, Spear SJ. Increasing proportion of herpes simplex virus type 1 as a cause of genital herpes infection in college students. Sex Transm Dis. 2003 Oct;30(10):797-800. doi: 10.1097/01.OLQ.0000092387.58746.C7
- James M. Sizemore, Jr, Fred Lakeman, Richard Whitley, Annalee Hughes, Edward W. Hook III, The Spectrum of Genital Herpes Simplex Virus Infection in Men Attending a Sexually Transmitted Disease Clinic, The Journal of Infectious Diseases, Volume 193, Issue 7, 1 April 2006, Pages 905–911, https://doi.org/10.1086/500841
- Heather Bradley, Lauri E. Markowitz, Theda Gibson, Geraldine M. McQuillan, Seroprevalence of Herpes Simplex Virus Types 1 and 2—United States, 1999–2010, The Journal of Infectious Diseases, Volume 209, Issue 3, 1 February 2014, Pages 325–333, https://doi.org/10.1093/infdis/jit458
- Bernstein DI, Bellamy AR, Hook EW 3rd, Levin MJ, Wald A, Ewell MG, Wolff PA, Deal CD, Heineman TC, Dubin G, Belshe RB. Epidemiology, clinical presentation, and antibody response to primary infection with herpes simplex virus type 1 and type 2 in young women. Clin Infect Dis. 2013 Feb;56(3):344-51. doi: 10.1093/cid/cis891
- Cherpes TL, Meyn LA, Hillier SL. Cunnilingus and vaginal intercourse are risk factors for herpes simplex virus type 1 acquisition in women. Sex Transm Dis. 2005 Feb;32(2):84-9. doi: 10.1097/01.olq.0000151414.64297.46
- William E. Lafferty, Lois Downey, Connie Celum, Anna Wald, Herpes Simplex Virus Type 1 as a Cause of Genital Herpes: Impact on Surveillance and Prevention, The Journal of Infectious Diseases, Volume 181, Issue 4, April 2000, Pages 1454–1457, https://doi.org/10.1086/315395
- Gregory J. Mertz, Asymptomatic Shedding of Herpes Simplex Virus 1 and 2: Implications for Prevention of Transmission, The Journal of Infectious Diseases, Volume 198, Issue 8, 15 October 2008, Pages 1098–1100, https://doi.org/10.1086/591914
- Mertz GJ, Benedetti J, Ashley R, Selke SA, Corey L. Risk factors for the sexual transmission of genital herpes. Ann Intern Med. 1992 Feb 1;116(3):197-202. doi: 10.7326/0003-4819-116-3-197
- Mertz GJ, Schmidt O, Jourden JL, Guinan ME, Remington ML, Fahnlander A, Winter C, Holmes KK, Corey L. Frequency of acquisition of first-episode genital infection with herpes simplex virus from symptomatic and asymptomatic source contacts. Sex Transm Dis. 1985 Jan-Mar;12(1):33-9. doi: 10.1097/00007435-198501000-00007
- Ribes JA, Steele AD, Seabolt JP, Baker DJ. Six-year study of the incidence of herpes in genital and nongenital cultures in a central Kentucky medical center patient population. J Clin Microbiol. 2001 Sep;39(9):3321-5. doi: 10.1128/JCM.39.9.3321-3325.2001
- Freeman EE, Weiss HA, Glynn JR, Cross PL, Whitworth JA, Hayes RJ. Herpes simplex virus 2 infection increases HIV acquisition in men and women: systematic review and meta-analysis of longitudinal studies. AIDS. 2006 Jan 2;20(1):73-83. doi: 10.1097/01.aids.0000198081.09337.a7
- Corey L. Synergistic copathogens–HIV-1 and HSV-2. N Engl J Med. 2007 Feb 22;356(8):854-6. doi: 10.1056/NEJMe068302. Erratum in: N Engl J Med. 2007 Apr 5;356(14):1487.
- Leeyaphan C, Surawan TM, Chirachanakul P, Prasertworonun N, Punyaratabandhu P, Omcharoen V, Jiamton S. Clinical characteristics of hypertrophic herpes simplex genitalis and treatment outcomes of imiquimod: a retrospective observational study. Int J Infect Dis. 2015 Apr;33:165-70. doi: 10.1016/j.ijid.2015.02.002
- Tan DH, Kaul R, Walsmley S. Left out but not forgotten: Should closer attention be paid to coinfection with herpes simplex virus type 1 and HIV? Can J Infect Dis Med Microbiol. 2009 Spring;20(1):e1-7. doi: 10.1155/2009/965263
- Johnston C, Corey L. Current Concepts for Genital Herpes Simplex Virus Infection: Diagnostics and Pathogenesis of Genital Tract Shedding. Clin Microbiol Rev. 2016 Jan;29(1):149-61. doi: 10.1128/CMR.00043-15
- Efstathiou S, Field HJ, Griffiths PD, Kern ER, Sacks SL, Sawtell NM, Stanberry LR. Herpes simplex virus latency and nucleoside analogues. Antiviral Res. 1999 Apr;41(3):85-100. doi: 10.1016/s0166-3542(99)00003-0
- Simmons A, Field HJ. Can HSV latency be conquered by current antiviral therapies? Sex Transm Infect. 1998 Feb;74(1):1-2.
- Nongenital Herpes Simplex Virus. Am Fam Physician. 2010;82(9):1075-1082. https://www.aafp.org/pubs/afp/issues/2010/1101/p1075.html
- Boivin G, Goyette N, Sergerie Y, Keays S, Booth T. Longitudinal evaluation of herpes simplex virus DNA load during episodes of herpes labialis. J Clin Virol. 2006 Dec;37(4):248-51. doi: 10.1016/j.jcv.2006.09.006
- Cernik C, Gallina K, Brodell RT. The treatment of herpes simplex infections: an evidence-based review. Arch Intern Med. 2008 Jun 9;168(11):1137-44. doi: 10.1001/archinte.168.11.1137
- Lafferty WE, Coombs RW, Benedetti J, Critchlow C, Corey L. Recurrences after oral and genital herpes simplex virus infection. Influence of site of infection and viral type. N Engl J Med. 1987 Jun 4;316(23):1444-9. doi: 10.1056/NEJM198706043162304
- Saleh D, Yarrarapu SNS, Sharma S. Herpes Simplex Type 1. [Updated 2022 Aug 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482197
- Williams C, Wells J, Klein R, Sylvester T, Sunenshine R; Centers for Disease Control and Prevention (CDC). Notes from the field: outbreak of skin lesions among high school wrestlers–Arizona, 2014. MMWR Morb Mortal Wkly Rep. 2015 May 29;64(20):559-60. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4584520
- Chaabane S, Harfouche M, Chemaitelly H, Schwarzer G, Abu-Raddad LJ. Herpes simplex virus type 1 epidemiology in the Middle East and North Africa: systematic review, meta-analyses, and meta-regressions. Sci Rep. 2019 Feb 4;9(1):1136. doi: 10.1038/s41598-018-37833-8
- Fedoreyev SA, Krylova NV, Mishchenko NP, Vasileva EA, Pislyagin EA, Iunikhina OV, Lavrov VF, Svitich OA, Ebralidze LK, Leonova GN. Antiviral and Antioxidant Properties of Echinochrome A. Mar Drugs. 2018 Dec 15;16(12):509. doi: 10.3390/md16120509
- Marchi S, Trombetta CM, Gasparini R, Temperton N, Montomoli E. Epidemiology of herpes simplex virus type 1 and 2 in Italy: a seroprevalence study from 2000 to 2014. J Prev Med Hyg. 2017 Mar;58(1):E27-E33. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5432775
- Finger-Jardim, F, Avila, EC, da Hora, VP, Gonçalves, CV, de Martinez, AMB, Soares, MA. Prevalence of herpes simplex virus types 1 and 2 at maternal and fetal sides of the placenta in asymptomatic pregnant women. Am J Reprod Immunol. 2017; 78:e12689. https://doi.org/10.1111/aji.12689
- Usatine RP, Smith MA, Chumley H, Mayeaux EJ Jr, Tysinger J, eds. The Color Atlas of Family Medicine. New York, NY: McGraw-Hill; 2009:83.
- Pfaff F, Groth M, Sauerbrei A, Zell R. Genotyping of herpes simplex virus type 1 by whole-genome sequencing. J Gen Virol. 2016 Oct;97(10):2732-2741. doi: 10.1099/jgv.0.000589
- van Oeffelen L, Biekram M, Poeran J, Hukkelhoven C, Galjaard S, van der Meijden W, Op de Coul E. Update on Neonatal Herpes Simplex Epidemiology in the Netherlands: A Health Problem of Increasing Concern? Pediatr Infect Dis J. 2018 Aug;37(8):806-813. doi: 10.1097/INF.0000000000001905
- Kolawole OM, Amuda OO, Nzurumike C, Suleiman MM, Ikhevha Ogah J. Seroprevalence and Co-Infection of Human Immunodeficiency Virus (HIV) and Herpes Simplex Virus (HSV) Among Pregnant Women in Lokoja, North-Central Nigeria. Iran Red Crescent Med J. 2016 Aug 10;18(10):e25284. doi: 10.5812/ircmj.25284
- El Hayderi L, Rübben A, Nikkels AF. The alpha-herpesviridae in dermatology : Herpes simplex virus types I and II. Hautarzt. 2017 Dec;68(Suppl 1):1-5. English. doi: 10.1007/s00105-016-3919-7
- Li Z, Breitwieser FP, Lu J, Jun AS, Asnaghi L, Salzberg SL, Eberhart CG. Identifying Corneal Infections in Formalin-Fixed Specimens Using Next Generation Sequencing. Invest Ophthalmol Vis Sci. 2018 Jan 1;59(1):280-288. doi: 10.1167/iovs.17-21617
- El Hayderi L, Rübben A, Nikkels AF. Alpha-Herpesviridae in der Dermatologie : Herpes-simplex-Virus Typ I und II [The alpha-herpesviridae in dermatology : Herpes simplex virus types I and II. German version]. Hautarzt. 2017 Mar;68(3):181-186. German. doi: 10.1007/s00105-016-3929-5
- Giraldo D, Wilcox DR, Longnecker R. The Type I Interferon Response and Age-Dependent Susceptibility to Herpes Simplex Virus Infection. DNA Cell Biol. 2017 May;36(5):329-334. doi: 10.1089/dna.2017.3668
- Leung AKC, Barankin B. Herpes Labialis: An Update. Recent Pat Inflamm Allergy Drug Discov. 2017;11(2):107-113. doi: 10.2174/1872213X11666171003151717
- Glaxo Operations UK. ZOVIRAX Labialis, 50 mg/g, Crème Aciclovir (Package Insert) (2012).
- InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. How effective are creams and tablets for the treatment of cold sores? 2018 Jul 12. Available from: https://www.ncbi.nlm.nih.gov/books/NBK525789
- Chen F, Xu H, Liu J, Cui Y, Luo X, Zhou Y, Chen Q, Jiang L. Efficacy and safety of nucleoside antiviral drugs for treatment of recurrent herpes labialis: a systematic review and meta-analysis. J Oral Pathol Med. 2017 Sep;46(8):561-568. https://doi.org/10.1111/jop.12534
- Arain N, Paravastu SC, Arain MA. Effectiveness of topical corticosteroids in addition to antiviral therapy in the management of recurrent herpes labialis: a systematic review and meta-analysis. BMC Infect Dis. 2015 Feb 21;15:82. doi: 10.1186/s12879-015-0824-0
- Rooney JF, Straus SE, Mannix ML, Wohlenberg CR, Alling DW, Dumois JA, Notkins AL. Oral acyclovir to suppress frequently recurrent herpes labialis. A double-blind, placebo-controlled trial. Ann Intern Med. 1993 Feb 15;118(4):268-72. doi: 10.7326/0003-4819-118-4-199302150-00004
- Baker D, Eisen D. Valacyclovir for prevention of recurrent herpes labialis: 2 double-blind, placebo-controlled studies. Cutis. 2003 Mar;71(3):239-42.
- Glenny AM, Fernandez Mauleffinch LM, Pavitt S, Walsh T. Interventions for the prevention and treatment of herpes simplex virus in patients being treated for cancer. Cochrane Database Syst Rev. 2009 Jan 21;(1):CD006706. doi: 10.1002/14651858.CD006706.pub2
- Miserocchi E, Modorati G, Galli L, Rama P. Efficacy of valacyclovir vs acyclovir for the prevention of recurrent herpes simplex virus eye disease: a pilot study. Am J Ophthalmol. 2007 Oct;144(4):547-51. doi: 10.1016/j.ajo.2007.06.001
- Hoff NP, Gerber PA. Herpetic whitlow. CMAJ. 2012;184(17):E924. doi:10.1503/cmaj.111741 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3503926
- Wu IB, Schwartz RA. Herpetic whitlow. Cutis 2007;79:193–6
- Richert B, André J. Nail disorders in children: diagnosis and management. Am J Clin Dermatol 2011;12:101–12
- Bowling JC, Saha M, Bunker CB. Herpetic whitlow: a forgotten diagnosis. Clin Exp Dermatol 2005;30:609–10
- Usatine RP, Smith MA, Chumley H, Mayeaux EJ Jr, Tysinger J, eds. The Color Atlas of Family Medicine. New York, NY: McGraw-Hill; 2009:517.
- Foti C, Romita P, Mascia P, Miragliotta G, Calvario A. Atypical Herpetic Whitlow: A Diagnosis to Consider. Endocr Metab Immune Disord Drug Targets. 2017;17(1):3-4.
- Gathier PJ, Schönberger TJ. A man with an infected finger: a case report. J Med Case Rep. 2015 May 23;9:119.
- Betz D, Fane K. Herpetic Whitlow. [Updated 2019 Feb 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482379
- Richert B, André J. Nail disorders in children: diagnosis and management. Am J Clin Dermatol. 2011 Apr 01;12(2):101-12.





{kind=link}