Hodgkin’s lymphoma
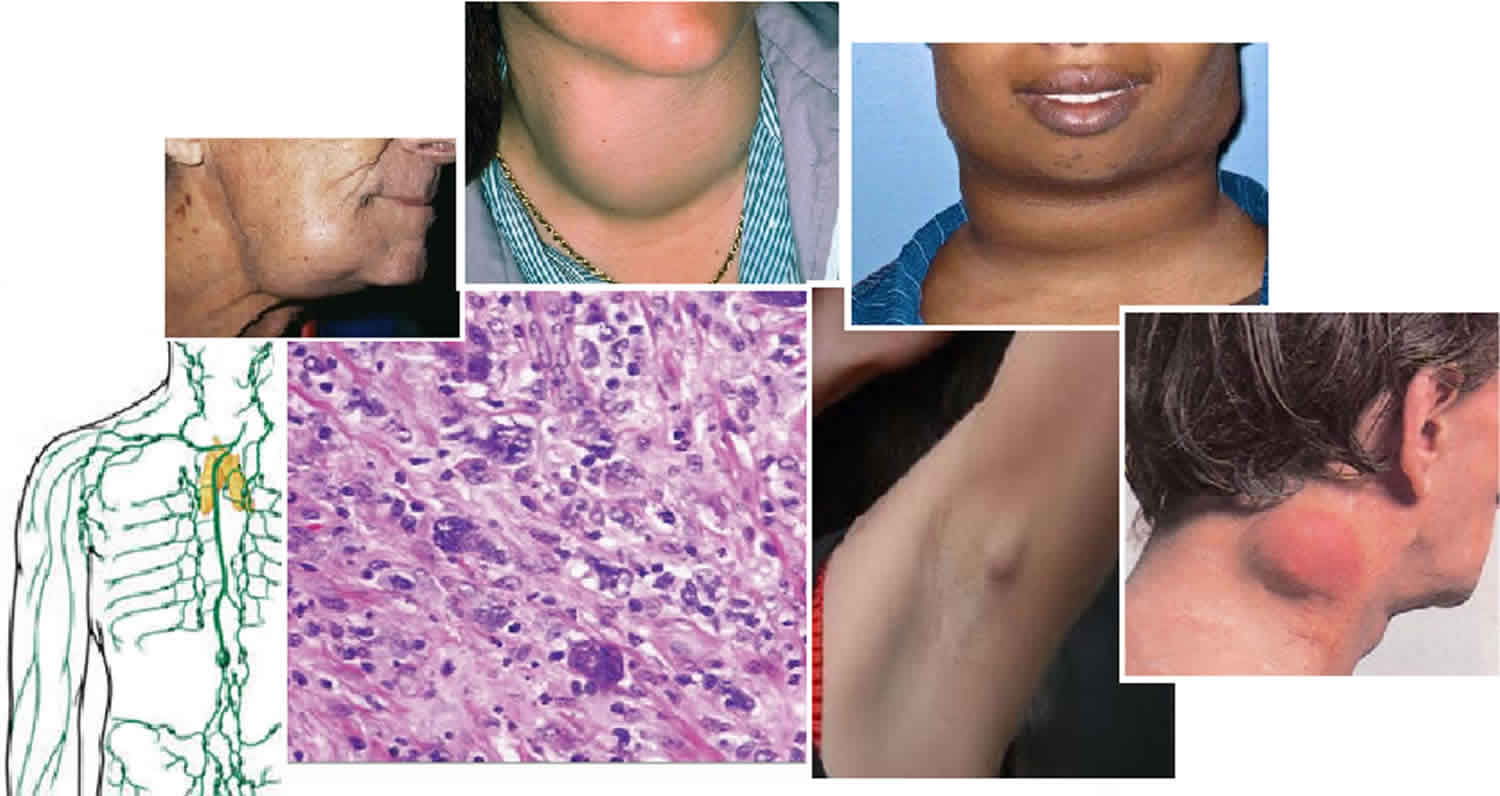
Hodgkin lymphoma also called Hodgkin’s disease is an uncommon cancer that develops in the lymphatic system that is marked by the presence of a type of cell called the Reed-Sternberg cell (see Figure 1). The two major types of Hodgkin lymphoma are classic Hodgkin lymphoma and nodular lymphocyte-predominant Hodgkin lymphoma 1. Classical Hodgkin lymphoma accounts for approximately 95% of all Hodgkin’s lymphoma, and it is further subdivided into four subgroups: nodular sclerosis Hodgkin lymphoma (NSHL), lymphocyte-rich Hodgkin lymphoma (LRHL), mixed cellularity Hodgkin lymphoma (MCHL), and lymphocyte-depleted Hodgkin lymphoma (LDHL) 2. Although Hodgkin lymphoma can start almost anywhere, most often it starts in lymph nodes in the upper part of the body. The most common sites are in the chest, neck, or under the arms. Signs and symptoms of Hodgkin lymphoma include painless, swollen lymph nodes (lymphadenopathy), an enlarged spleen, fever, weight loss, fatigue, and night sweats.
Hodgkin lymphoma is named after Dr. Thomas Hodgkin who, in 1832, described several cases of people with symptoms of a cancer involving the lymph nodes. The disease was called “Hodgkin’s disease” until it was officially renamed “Hodgkin lymphoma” in the late 20th century.
Hodgkin lymphoma is distinguished from other types of lymphoma primarily by the presence of two types of cells, referred to as Hodgkin cells and Reed-Sternberg cells, named after the scientists who first identified them. Reed-Sternberg cells are large, abnormal B lymphocytes that often have more than one nucleus and an owl-like appearance (Figure 1). Hodgkin cells are larger than normal lymphocytes, but smaller than Reed-Sternberg cells. These differences can be observed under a microscope and further identified by special pathology tests. This is important information that helps doctors determine a patient’s Hodgkin lymphoma subtype.
Hodgkin lymphoma starts when an abnormal change to the DNA of a white blood cell called a lymphocyte causes it to become a lymphoma cell that, if untreated, results in the uncontrolled growth of cancerous lymphocytes.
- These cancerous cells crowd out normal white cells, and the immune system can’t guard against infection effectively.
- Lymphoma cells grow and form masses, usually in the lymph nodes, located throughout our bodies in the lymphatic system.
- Lymphoma cells can also gather in other areas of the body where lymphoid tissue is found.
- Hodgkin lymphoma is distinguished from other types of lymphoma by the presence of Reed-Sternberg cells (named for the scientists who first identified them). Other cells associated with the disease are called Hodgkin cells.
Hodgkin lymphoma most often spreads through the lymph vessels from lymph node to lymph node. Rarely, late in the disease, it can invade the bloodstream and spread to other parts of the body, such as the liver, lungs, and/or bone marrow.
The American Cancer Society’s estimates for Hodgkin disease (Hodgkin’s lymphoma) in the United States for 2022 are 3, 4:
- New cases: About 8,540 new cases (4,570 in males and 3,970 in females)
- Deaths: About 920 deaths (550 males and 370 females)
- 5-Year Relative Survival: 89.1%. Relative survival is an estimate of the percentage of patients who would be expected to survive the effects of their cancer. It excludes the risk of dying from other causes. Because survival statistics are based on large groups of people, they cannot be used to predict exactly what will happen to an individual patient. No two patients are entirely alike, and treatment and responses to treatment can vary greatly.
- Percentage of All Cancer Deaths: 0.2%.
- Rate of New Cases and Deaths per 100,000: The rate of new cases of Hodgkin lymphoma was 2.6 per 100,000 men and women per year. The death rate was 0.3 per 100,000 men and women per year. These rates are age-adjusted and based on 2015–2019 cases and deaths.
- Lifetime Risk of Developing Cancer: Approximately 0.2 percent of men and women will be diagnosed with Hodgkin lymphoma at some point during their lifetime, based on 2017–2019 data.
- In 2019, there were an estimated 218,740 people living with Hodgkin lymphoma in the United States.
Both children and adults can develop Hodgkin lymphoma, but it is most common in early adulthood (especially in a person’s 20s). The risk of Hodgkin lymphoma rises again in late adulthood (after age 55). Overall, the average age of people when they are diagnosed is 39.
Hodgkin lymphoma is rare in children younger than 5 years of age. About 10% to 15% of cases are diagnosed in children and teenagers ages 15 to 19 years.
Survival rates have improved in the past few decades, largely due to advances in treatment. More than 75% of all newly diagnosed patients with adult Hodgkin lymphoma can be cured with combination chemotherapy and/or radiation therapy 5. The 5-year relative survival rate for all patients diagnosed with Hodgkin lymphoma is now about 89.1%, and the 10-year relative survival rate is about 80%. Certain factors such as the stage (extent) of Hodgkin lymphoma and a person’s age affect these rates.
Many types of Hodgkin’s lymphoma exist, including rare forms that are difficult for inexperienced pathologists to identify. Accurate diagnosis and staging are key to developing a treatment plan. Research shows that review of biopsy tests by pathologists who aren’t experienced with lymphoma results in a significant proportion of misdiagnoses. Get a second opinion from a specialist if needed.
Figure 1. Reed Sternberg cells seen in classical Hodgkin’s lymphoma
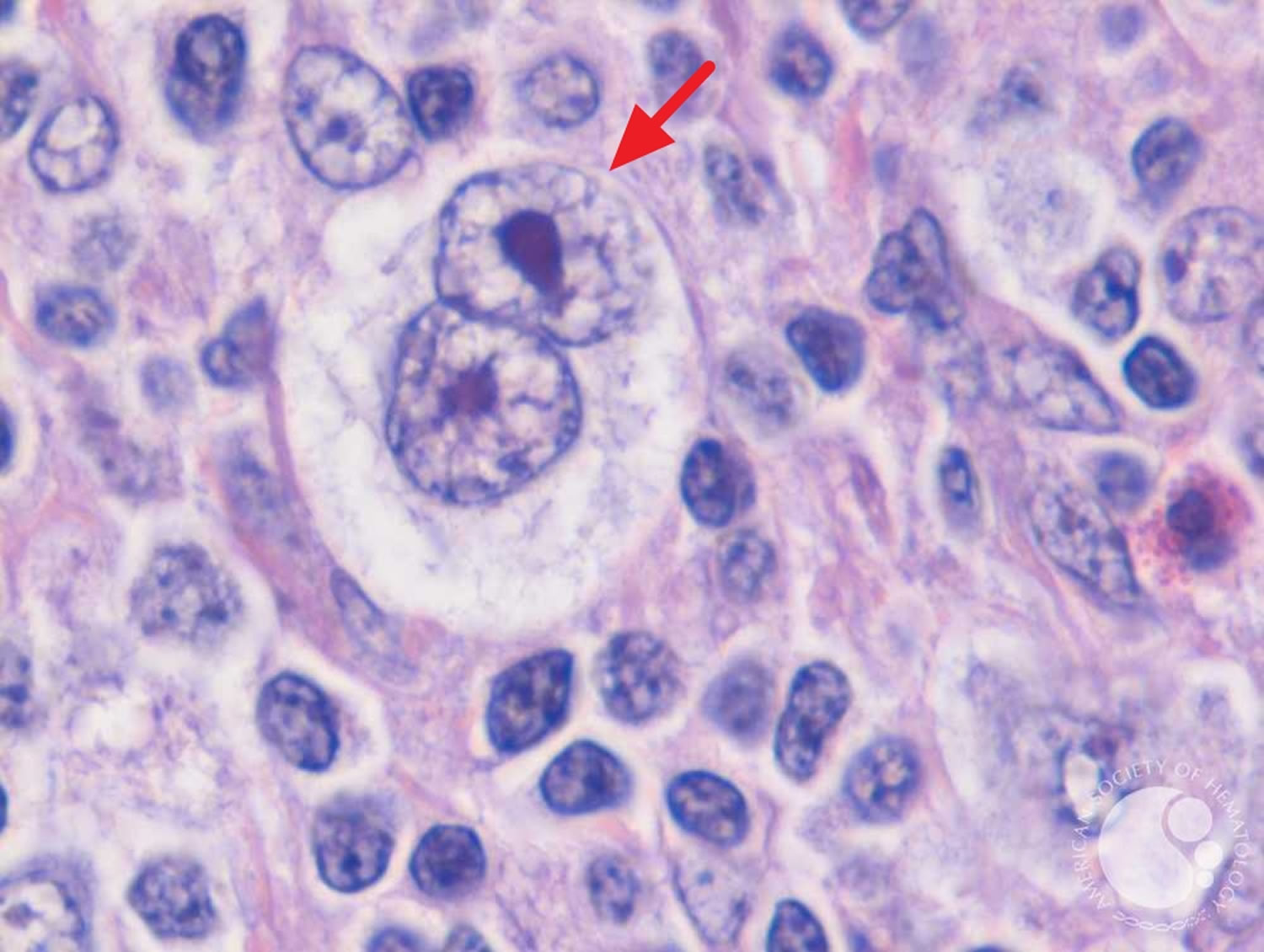
Footnote: Reed-Sternberg cells are large, abnormal lymphocytes (a type of white blood cell) that may contain more than one nucleus. Reed-Sternberg cells are found in people with Hodgkin lymphoma. Reed-Sternberg cells are also called Hodgkin and Reed-Sternberg cells.
The Lymphatic System
To understand what lymphoma is, it helps to know about the lymph system (also known as the lymphatic system). The lymph system is part of the immune system, which helps fight infections and some other diseases. The lymphatic system plays a role in:
- fighting bacteria and other infections
- destroying old or abnormal cells, such as cancer cells
The lymphatic system also helps the flow of fluids in the body.
The lymph system is made up mainly of cells called lymphocytes, a type of white blood cell. There are 2 main types of lymphocytes:
- B lymphocytes (B cells): B cells make proteins called antibodies to help protect the body from germs (bacteria and viruses).
- T lymphocytes (T cells): There are several types of T cells. Some T cells destroy germs or abnormal cells in the body. Other T cells help boost or slow the activity of other immune system cells.
- Natural killer (NK) cells, which attack virus-infected cells or tumor cells
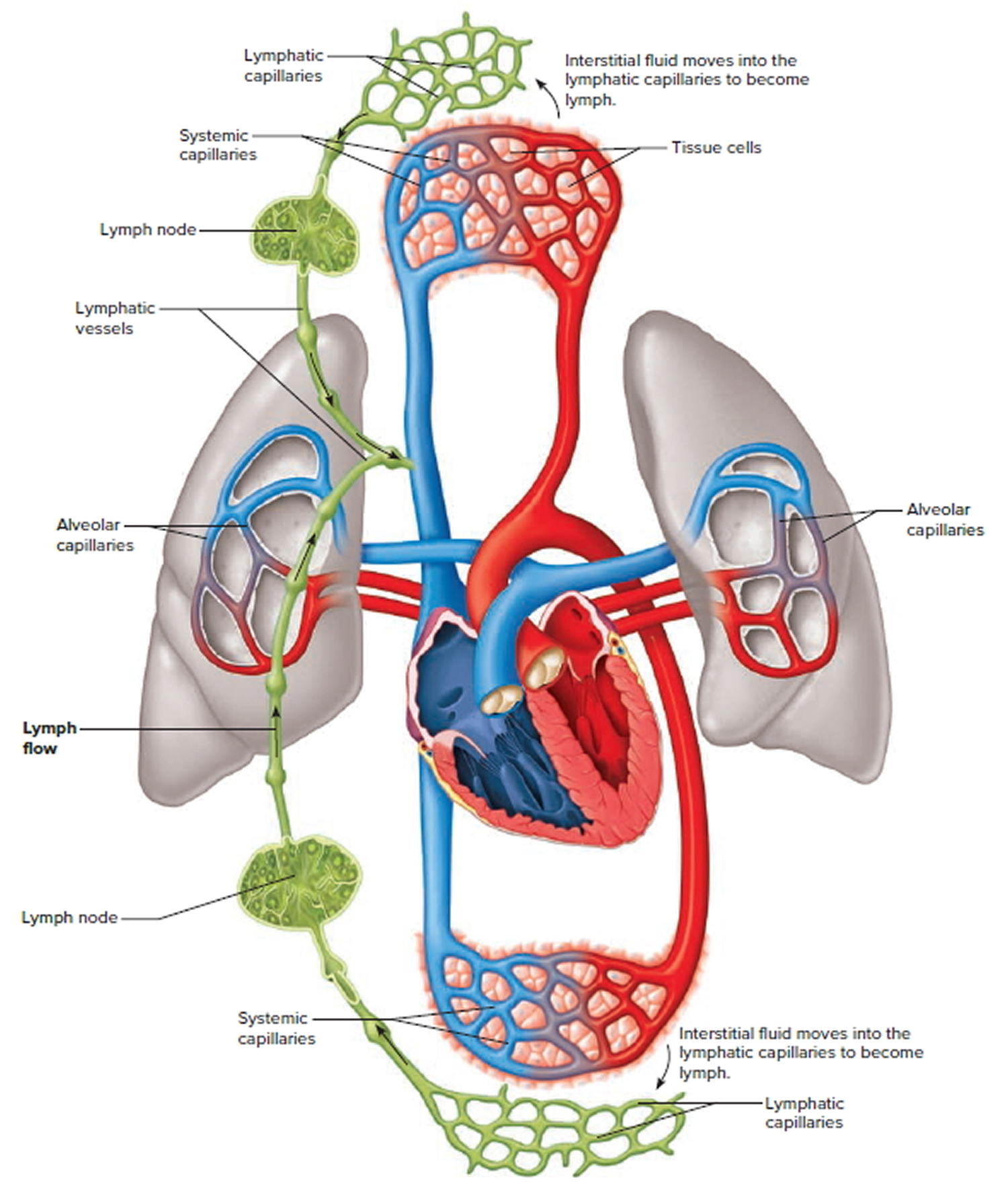
The lymphatic system is a vast collection of cells and biochemicals that travel in lymphatic vessels, and the organs and glands that produce them. The lymphatic system includes a network of vessels (like the arteries and veins that carry blood) that assist in circulating body fluids (a colorless liquid called lymph), so it is closely associated with your cardiovascular system. Lymphatic vessels transport excess fluid away from interstitial spaces in most tissues and return it to the bloodstream (Figure 4). This fluid carries food to the cells and bathes the body tissues to form tissue fluid. The fluid then collects waste products, bacteria, and damaged cells. It also collects any cancer cells if these are present. This fluid then drains into the lymph vessels. Without the lymphatic system, this fluid would accumulate in tissue spaces. Special lymphatic capillaries, called lacteals, are located in the lining of the small intestine. They absorb digested fats and transport them to the venous circulation.
The lymphatic system is a system of thin tubes and lymph nodes that run throughout the body. Lymph nodes are bean shaped glands. The thin tubes are called lymph vessels or lymphatic vessels. Tissue fluid called lymph circulates around the body in these vessels and flows through the lymph nodes.
The lymph system is an important part of your immune system. It plays a role in fighting bacteria and other infections and destroying old or abnormal cells, such as cancer cells.
The major sites of lymphoid tissue are:
- Lymph nodes: Lymph nodes are bean-sized collections of lymphocytes and other immune system cells throughout the body, including inside the chest, abdomen, and pelvis. They are connected to each other by a system of lymphatic vessels.
- Spleen: The spleen is an organ under the lower ribs on your left side. The spleen makes lymphocytes and other immune system cells. It also stores healthy blood cells and filters out damaged blood cells, bacteria, and cell waste.
- Bone marrow: The bone marrow is the spongy tissue inside certain bones. New blood cells (including some lymphocytes) are made there.
- Thymus: The thymus is a small organ behind the upper part of the breastbone and in front of the heart. Thymus is an organ in which T lymphocytes mature and multiply.
- Adenoids and tonsils: These are collections of lymphoid tissue in the back of your throat. They help make antibodies against germs that are breathed in or swallowed.
- Digestive tract: The stomach, intestines, and many other organs also have lymph tissue.
The lymphatic system has a second major function— it enables you to live in a world with different types of organisms. Some of them live in or on the human body and in some circumstances may cause infectious diseases. Cells and biochemicals of the lymphatic system launch both generalized and targeted attacks against “foreign” particles, enabling the body to destroy infectious agents. This immunity against disease also protects against toxins and cancer cells. When the immune response is abnormal, persistent infection, cancer, allergies, and autoimmune disorders may result.
The larger lymphatic vessels lead to specialized organs called lymph nodes. After leaving the lymph nodes, the vessels merge to form still larger lymphatic trunks.
Figure 2. Locations of major lymph nodes
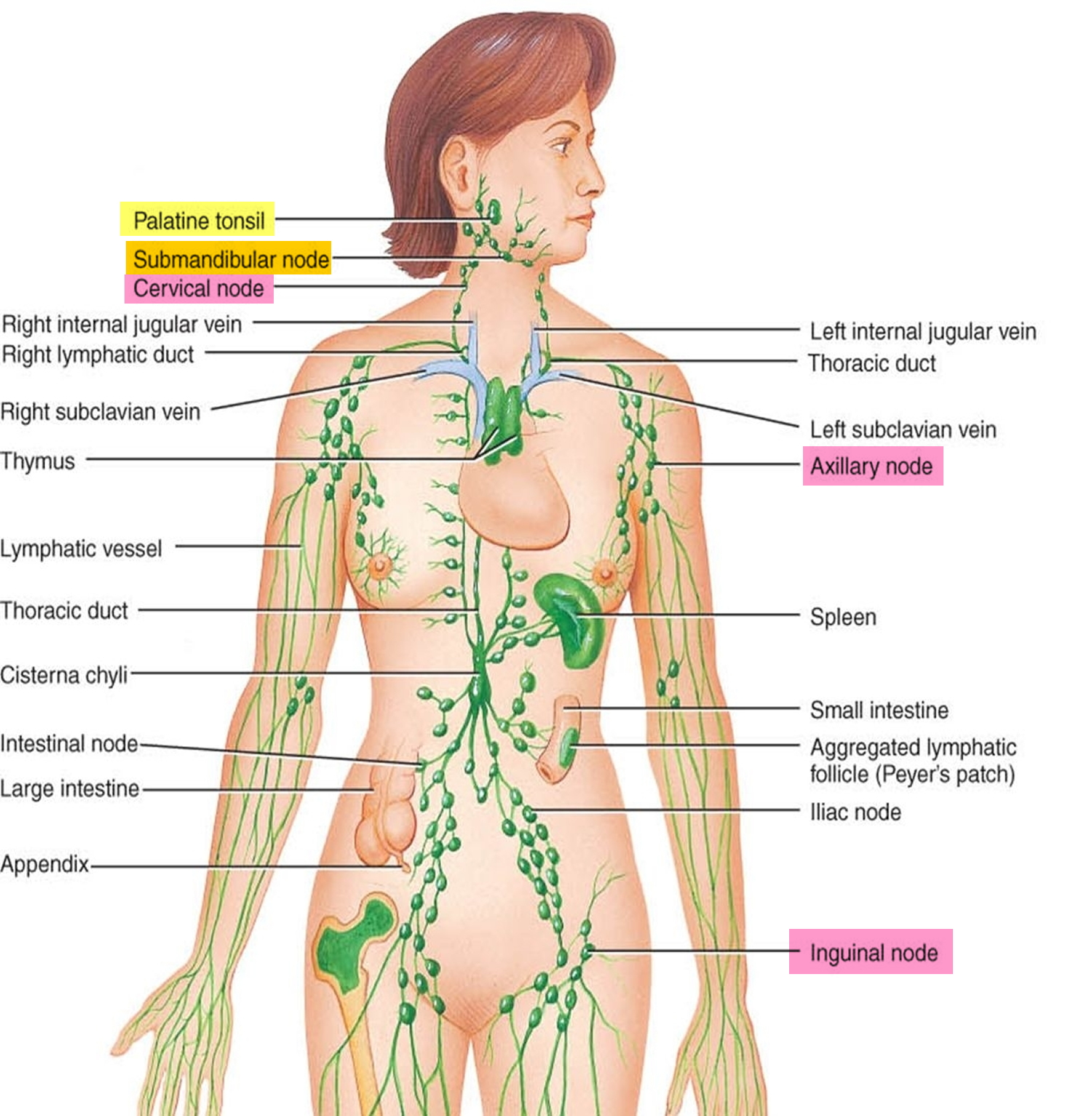
Figure 3. Functions of lymph nodes in the lymphatic system
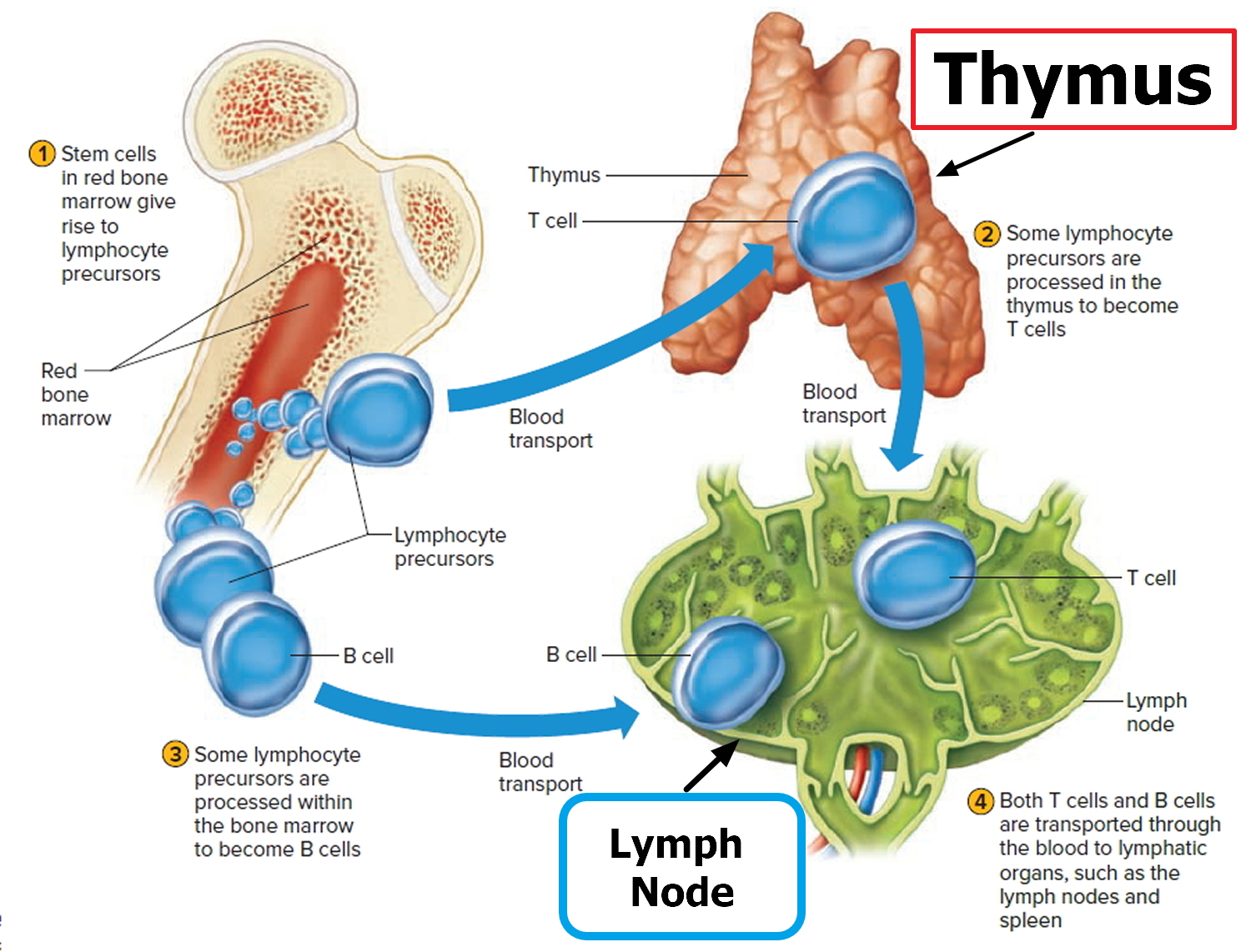
Figure 4. Schematic representation of lymphatic vessels transporting fluid from interstitial spaces to the bloodstream. Depending on its origin, lymph enters the right or left subclavian vein.
Types of Hodgkin’s lymphoma
The World Health Organization (WHO) divides Hodgkin lymphoma into two main subtypes. They are:
- Classic Hodgkin lymphoma (cHL)
- Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL)
Classic Hodgkin lymphoma (cHL) is characterized by the presence of Reed-Sternberg cells. Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is characterized by the presence of lymphocyte-predominant cells, sometimes termed “popcorn cells,” and Reed-Sternberg cells are not found.
It’s important to know your subtype since it plays a large part in determining the type of treatment you’ll receive.
Classic Hodgkin’s lymphoma
Classic Hodgkin’s lymphoma (cHL) accounts for about 95% of all cases of Hodgkin’s lymphomas in developed countries 6.
The cancer cells in Classic Hodgkin’s lymphoma (cHL) are called Reed-Sternberg cells. These cells are usually an abnormal type of B lymphocyte. Enlarged lymph nodes in people with Classic Hodgkin’s lymphoma (cHL) usually have a small number of Reed-Sternberg cells and a large number of surrounding normal immune cells. These other immune cells make up most of the enlarged lymph nodes.
Classic Hodgkin’s lymphoma has 4 subtypes:
- Nodular sclerosis Hodgkin lymphoma (NSCHL): This is the most common type of Hodgkin lymphoma in developed countries. It accounts for about 7 out of 10 cases. It is most common in teens and young adults, but it can occur in people of any age. It tends to start in lymph nodes in the neck or chest.
- Mixed cellularity Hodgkin lymphoma (MCCHL): This is the second most common type, found in about 4 out 10 cases. Mixed cellularity Hodgkin lymphoma (MCCHL) is seen mostly in people with HIV infection. It’s also found in children or the elderly . It can start in any lymph node but most often occurs in the upper half of the body.
- Lymphocyte-rich Hodgkin lymphoma: Lymphocyte-rich Hodgkin lymphoma isn’t common. It usually occurs in the upper half of the body and is rarely found in more than a few lymph nodes.
- Lymphocyte-depleted Hodgkin lymphoma: This is the least common form of Hodgkin lymphoma. Lymphocyte-depleted Hodgkin lymphoma is seen mainly in older people and those with HIV infection. It’s more aggressive than other types of Hodgkin lymphoma and likely to be advanced when first found. It’s most often in lymph nodes in the abdomen (belly) as well as in the spleen, liver, and bone marrow.
Table 1. Classic Hodgkin’s Lymphoma Subtypes
| Classic Hodgkin’s Lymphoma Subtype | Characteristics |
|---|---|
| Nodular sclerosis Hodgkin lymphoma (NSCHL) | Accounts for 70 percent of classical Hodgkin lymphoma cases Most common type in young adults Involved lymph nodes contain scar tissue (sclerosis) Incidence similar in males and females Highly curable B symptoms in approximately 40 percent of cases |
| Mixed cellularity Hodgkin lymphoma (MCCHL) | Accounts for 20-25 percent of classical Hodgkin lymphoma cases Most common in older adults More common in males Prevalent in patients with HIV (human immunodeficiency virus) infection Involved lymph nodes contain Reed-Sternberg cells and several other cell types B symptoms common |
| Lymphocyte-rich Hodgkin lymphoma | Accounts for approximately 5 percent of classical Hodgkin lymphoma cases Involved lymph nodes contain numerous normal-appearing lymphocytes and Reed-Sternberg cells Usually diagnosed at an early stage More common in males B symptoms are rare |
| Lymphocyte-depleted Hodgkin lymphoma | Rarest classical Hodgkin lymphoma subtype, less than 1 percent of all classical Hodgkin lymphoma cases Involved lymph nodes contain few normal lymphocytes and numerous Reed-Sternberg cells Median age range 30-37 years Prevalent in patients with HIV infection Usually diagnosed at an advance stage B symptoms common |
Nodular lymphocyte predominant Hodgkin’s lymphoma
Nodular lymphocyte predominant Hodgkin’s lymphoma (NLPHL) accounts for about 5% of cases. The cancer cells in nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) are large cells called popcorn cells (because they look like popcorn), which are variants of Reed-Sternberg cells. You may also hear these cells called lymphocytic and histiocytic (L&H) cells.
Nodular lymphocyte predominant Hodgkin lymphoma usually starts in lymph nodes in the neck and under the arm. It can occur in people of any age, and is more common in men than in women. This type of Hodgkin’s lymphoma is treated differently from the classic Hodgkin lymphoma (cHL).
The following are some characteristics of nodular lymphocyte predominant Hodgkin’s lymphoma (NLPHL):
- Most common in 30 to 50 year-old age group
- More common in male than in female patients
- NLPHL is slow growing (indolent) and highly curable.
- Small risk (3-5 percent of cases) of transformation to aggressive non-Hodgkin lymphoma.
Hodgkin’s Lymphoma causes
The exact cause of Hodgkin’s lymphoma is unknown. Scientists have found some risk factors that make a person more likely to get Hodgkin disease, but it’s not always clear exactly how these factors might increase risk. You can not catch Hodgkin lymphoma from someone else.
Your risk of developing Hodgkin’s lymphoma is increased if:
- you have a medical condition that weakens your immune system
- you take immunosuppressant medicine
- you’ve previously been exposed to a common virus called the Epstein-Barr virus (EBV), which causes infectious mononucleosis or glandular fever. Some researchers think that infection with the Epstein-Barr virus (EBV) may sometimes cause DNA changes in B lymphocytes, leading to the development of Reed-Sternberg cells, which are the cancer cells in Hodgkin lymphoma.
You also have an increased risk of developing Hodgkin lymphoma if a first-degree relative (parent, sibling or child) has had the condition, it’s not clear if this is because of an inherited genetic fault or lifestyle factors. However, these cases are uncommon and some experts are studying whether some people have a genetic predisposition to Hodgkin lymphoma.
Hodgkin lymphoma is caused by a change (mutation) in the DNA of a type of white blood cell called B lymphocytes. The exact reason why this happens isn’t known.
DNA is the chemical in your cells that makes up your genes, which control how your cells function. You look like your parents because they are the source of your DNA. But DNA affects more than just how you look.
Some genes control when cells grow, divide into new cells, and die:
- Genes that help cells grow, divide, and stay alive are called oncogenes.
- Genes that slow down cell division or cause cells to die at the right time are called tumor suppressor genes.
Cancers can be caused by DNA changes that turn on oncogenes or turn off tumor suppressor genes.
Scientists have found many gene changes in Reed-Sternberg cells that help the cells grow and divide or live longer than they should. Reed-Sternberg cells also make substances called cytokines, which attract many other cells into the lymph node, enlarging it. In turn, these non-cancerous cells release substances that further help Reed-Sternberg cells grow.
Despite these advances, scientists do not yet know what sets off these processes. An abnormal reaction to infection with Epstein-Barr virus (EBV) or to other infections may be the trigger in some cases. But more research is needed to understand what causes Hodgkin lymphoma.
Hodgkin’s lymphoma Risk Factors
The following risk factors may increase a person’s likelihood of developing Hodgkin lymphoma:
- The Epstein-Bar virus (EBV), known for causing infectious mononucleosis, is associated with the development of Hodgkin lymphoma. The exact role of EBV in the development of Hodgkin lymphoma is not clear. Many people are infected with EBV, but very few develop Hodgkin lymphoma. Parts of the virus are found in Reed-Sternberg cells in about 1 out of 3 people with Hodgkin lymphoma. But most people with Hodgkin lymphoma have no signs of EBV in their cancer cells.
- Having a medical condition that weakens your immune system, such as being infected with human immunodeficiency virus (HIV), the virus that causes AIDS, have increased probability of developing Hodgkin lymphoma.
- Having medical treatment that weakens your immune system, for example, taking medicine to suppress your immune system after an organ transplant.
- Having previously had non-Hodgkin lymphoma, possibly because of treatment with chemotherapy or radiotherapy
- Family history of lymphoma: Brothers and sisters of young people with this disease have a higher risk for Hodgkin lymphoma. The risk is very high for an identical twin of a person with Hodgkin lymphoma. Studies found that there is a ten-fold increase of developing Hodgkin lymphoma in same-sex siblings of patients with Hodgkin lymphoma, suggesting a gene-environment interaction role in Hodgkin lymphoma predisposition 7, 8, 9. However, a family link is still uncommon – most people with Hodgkin lymphoma do not have a family history of it. It’s not clear why family history might increase risk. It might be because family members have similar childhood exposures to certain infections (such as Epstein-Barr virus), because they share inherited gene changes that make them more likely to get Hodgkin lymphoma, or some combination of these factors.
- Age: People can be diagnosed with Hodgkin lymphoma at any age, but it is most common in early adulthood (especially in a person’s 20s) and in late adulthood (after age 55).
- Gender: Hodgkin lyphoma occurs slightly more often in males than in females.
- Being very overweight (obese) – this may be more of a risk factor in women than men
- Smoking
- Geography: Hodgkin lymphoma is most common in the United States, Canada, and Europe, and is least common in African and Asian countries.
- Socioeconomic status: The risk of Hodgkin disease is greater in people with a higher socioeconomic background. The reason for this is not clear. One theory is that children from more affluent families might be exposed to some type of infection (such as Epstein-Barr virus) later in life than children from less affluent families, which might somehow increase their risk.
Hodgkin’s lymphoma prevention
Few of the known risk factors for Hodgkin lymphoma can be changed, so it’s not possible to prevent most cases of Hodgkin lymphoma at this time.
Infection with HIV, the virus that causes AIDS, is known to increase risk, so one way to limit your risk is to avoid known risk factors for HIV, such as intravenous (IV) drug use or unprotected sex with many partners.
Another risk factor for Hodgkin lymphoma is infection with the Epstein-Barr virus (the cause of infectious mononucleosis, or glandular fever), but there’s no known way to prevent this infection.
Can Hodgkin’s lymphoma be found early?
Screening tests or exams are used to look for disease in people who have no symptoms. At this time, there are no widely recommended screening tests for Hodgkin lymphoma. This is because no screening test has been shown to lower the risk of dying from this cancer. Still, in some cases Hodgkin’s lymphoma can be found early.
The best way to find Hodgkin lymphoma early is to be on the lookout for possible symptoms. The most common symptom is enlargement or swelling of one or more lymph nodes, causing a lump or bump under the skin which usually doesn’t hurt. It’s most often on the side of the neck, in the armpit, or in the groin. More often this is caused by something like an infection, not Hodgkin lymphoma, but it’s important to have such lumps checked by a doctor.
Careful, regular medical check-ups may be helpful for people with known risk factors for Hodgkin lymphoma, such as a strong family history. These people do not often get Hodgkin lymphoma, but they (and their doctors) should know about any possible symptoms and signs they might have.
Hodgkin’s lymphoma signs and symptoms
The most common early sign of Hodgkin lymphoma is painless swelling (enlargement) of one or more lymph nodes. Most people have affected lymph nodes in the upper part of their body, usually the neck or upper chest. Sometimes the affected lymph nodes are in the armpit, stomach area or groin.
Hodgkin’s lymphoma doesn’t usually hurt, but the area may become painful after drinking alcohol. The lump might grow larger over time, or new lumps might appear near it (or even in other parts of the body).
But Hodgkin lymphoma is not the most common cause of lymph node swelling. Most enlarged lymph nodes, especially in children, are caused by an infection. Lymph nodes that grow because of infection are called reactive or hyperplastic nodes. These often hurt when they are touched. If an infection is the cause, the node should return to its normal size within a few weeks after the infection goes away.
Other cancers can also cause swollen lymph nodes. If you have an enlarged lymph node, especially if you haven’t had a recent infection, it’s best to see your doctor so that the cause can be found and treated without delay, if needed.
In addition to swollen lymph nodes, other signs and symptoms of Hodgkin lymphoma may include:
- Unexplained fever (100.4°F [38ºC] or higher)
- Persistent fatigue
- Persistent cough
- Shortness of breath during normal activity
- Drenching sweats, especially at night
- Unexplained weight loss (weight loss of 10% or more of baseline weight in the previous 6 months)
- Decreased appetite
- Itchy skin (pruritus), especially after bathing or after ingesting alcohol
- Abdominal pain or swelling and feeling of fullness (due to an enlarged spleen)
- Lymph node pain after drinking alcohol
A few people with Hodgkin lymphoma have abnormal cells in their bone marrow when they’re diagnosed. This may lead to:
- persistent tiredness or fatigue
- an increased risk of infections
- excessive bleeding – such as nosebleeds, heavy periods and spots of blood under the skin
Treatment of Hodgkin’s lymphoma should relieve these symptoms within days.
B symptoms
Fever, drenching night sweats and loss of more than 10 percent of body weight over six months are sometimes termed “B symptoms.” These symptoms are significant to the prognosis and staging of the disease.
Some Hodgkin lymphoma symptoms are associated with other, less serious illnesses. However, if you’re troubled by any of the above symptoms, see your doctor.
Hodgkin’s lymphoma diagnosis
Hodgkin lymphoma can be a difficult disease to diagnose because it can be confused with some types of non-Hodgkin lymphoma. Having the correct diagnosis is important for getting the right treatment. You may want to get a second medical opinion by an experienced hematopathologist before you begin treatment. A hematopathologist is a specialist who studies blood and bone marrow cells and other tissues to help diagnose diseases of the blood, bone marrow and lymph system.
If a person has signs or symptoms that suggest Hodgkin lymphoma, exams and tests will be done to find out for sure and, if so, to determine the exact type.
Medical history and physical exam
Your doctor will want to get a thorough medical history, including information about symptoms, possible risk factors, family history, and other medical conditions.
Next, the doctor will examine you, paying special attention to the lymph nodes and other areas of the body that might be affected, including the spleen and liver. Because infections are the most common cause of enlarged lymph nodes, especially in children, the doctor will look for an infection in the part of the body near any swollen lymph nodes.
The doctor also might order blood tests to look for signs of infection or other problems. If the doctor suspects that Hodgkin lymphoma might be causing the symptoms, he or she might recommend a biopsy of a swollen lymph node.
Lymph Node Biopsy
Diagnosing Hodgkin lymphoma usually involves performing a lymph node biopsy. The entire lymph node or part of the lymph node is surgically removed using a special needle. A hematopathologist examines the sample of the lymph node under a microscope to look for the identifying characteristics of Hodgkin lymphoma. If the biopsy confirms that you have Hodgkin lymphoma, the hematopathologist will categorize the Hodgkin lymphoma into one of several subtypes. If Hodgkin and Reed-Sternberg cells are found in the lymph node sample, the hematopathologist will make a diagnosis of “classical Hodgkin lymphoma” (often abbreviated as “cHL”). There is another, less common but distinct subtype of Hodgkin lymphoma, called “nodular lymphocyte-predominant Hodgkin lymphoma” (NLPHL); a diagnosis of nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is made if the hematopathologist finds a specific type or pattern of lymphocytes that indicate this subtype of the disease.
The lymph node biopsy’s purpose is to confirm a diagnosis and:
- Identify your Hodgkin lymphoma subtype
- Develop a treatment plan
Hodgkin’s lymphoma may be difficult to diagnose because the Reed-Sternberg cells may comprise only 0.1 to 10 percent of the biopsy tissue sample, so it is important for it to be analyzed by a specialist with experience in diagnosing Hodgkin lymphoma. Pathology slides may be sent to a specialty center for confirmation of the diagnosis.
Immunophenotyping
The hematopathologist may use a lab test called immunophenotyping to distinguish Hodgkin lymphoma from other types of lymphoma or other cancerous or noncancerous conditions based on the antigens or markers on the surface of the cells, such as CD15 and CD30. These are found on the surface of the Reed-Sternberg cells in classic Hodgkin lymphoma (cHL). Tests for other proteins may point to nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL), to non-Hodgkin lymphoma (rather than Hodgkin lymphoma), or maybe to other diseases.
Staging Tests
Once your hematologist-oncologist confirms a Hodgkin lymphoma diagnosis, he or she orders more tests to stage your disease. Staging identifies the extent of your disease and where it’s located in your body.
Staging tests include:
- Imaging tests
- Blood tests
- Bone marrow tests
Imaging Tests
Imaging tests are used to look for signs of Hodgkin’s lymphoma in other areas of your body.
Imaging tests help the doctor evaluate:
- The location and distribution of enlarged lymph nodes
- Whether organs other than lymph nodes are involved
- Whether there are very large masses of tumors in one site or another
Imaging tests may include:
- Chest X-ray. Hodgkin lymphoma often enlarges lymph nodes in the chest. This can often be seen on a chest x-ray.
- CT (computed tomography) scan of the neck, chest, pelvis and abdomen (stomach area). A CT scan combines many x-rays to make detailed cross-sectional images of your body. This scan can help tell if any lymph nodes or organs in your body are enlarged. CT scans are useful for looking for Hodgkin lymphoma in the neck, chest, abdomen (belly), and pelvis.
- CT-guided needle biopsy: A CT scan can also be used to guide a biopsy needle into a suspicious area. For this procedure, a person lies on the CT scanning table while the doctor moves a biopsy needle through the skin and toward the area. CT scans are repeated until the needle is in the right place. A biopsy sample is then removed and sent to the lab to be looked at under a microscope.
- FDG-PET (fluorodeoxyglucose [FDG] positron emission tomography [PET]) of the entire body with a radioactive tracer. For a PET scan, a slightly radioactive form of sugar is put into your blood. Over time, it collects in very active cells, like cancer cells. A special camera is then used to create a picture of the parts of the body where the radioactivity collected. The picture is not detailed like a CT or MRI scan, but it can give helpful information about your whole body. PET scans can be used for many reasons in a person with Hodgkin lymphoma:
- They can help show if an enlarged lymph node contains Hodgkin lymphoma.
- They can help find small spots in the body that might be lymphoma, even if the area looks normal on a CT scan.
- They can help tell if the lymphoma is responding to treatment. Some doctors will repeat the PET scan after a few courses of chemotherapy. If it’s working, the lymph nodes will no longer take up the radioactive sugar.
- They can be used after treatment to help decide if an enlarged lymph node still has cancer or if it’s just scar tissue.
- Combination PET-CT scan. Some machines can do both a PET scan and a CT scan at the same time. This lets the doctor compare areas of higher radioactivity on the PET scan with the more detailed pictures from the CT scan. PET/CT scans often can help pinpoint the areas of lymphoma better than a CT scan alone.
- MRI (magnetic resonance imaging). Like CT scans, MRIs show detailed images of soft tissues in the body. But MRIs use radio waves and strong magnets instead of x-rays. This test is rarely used in Hodgkin lymphoma, but if the doctor is concerned about spread to the spinal cord or brain, MRI is very useful for looking at these areas.
- Bone scan. A bone scan isn’t usually done unless a person is having bone pain or has lab test results that suggest the lymphoma might have reached the bones. For this test, a radioactive substance is injected into a vein. It travels to damaged areas of bone, and a special camera can then detect the radioactivity. Hodgkin lymphoma sometimes causes bone damage, which may be picked up on a bone scan. But bone scans can’t show the difference between cancers and non-cancer problems, so more tests might be needed.
Blood Tests
Blood tests are used to:
- Assess blood counts including red blood cells, white blood cells and platelets;
- Determine whether lymphoma cells are present in the blood;
- Determine whether the immunoglobulins (proteins that fight infection) made by lymphocytes are deficient or abnormal;
- Check indicators of inflammation and disease severity such as blood protein levels, uric acid levels and erythrocyte sedimentation rate (ESR);
- Assess kidney and liver functions;
- Some women may have a pregnancy test.
Your doctor might also suggest other blood tests to look for signs of certain infections:
- HIV test: This may be done if you have abnormal symptoms that might be related to HIV infection.
- Hepatitis B and C virus test: Certain chemo drugs could cause problems if you have these infections.
Bone Marrow Tests
Your doctor may decide to examine your bone marrow to see whether the disease has spread to the bone marrow. Your doctor will decide if this procedure is necessary based on certain features such as the location of the disease in your body. Bone marrow testing may not be required for patients with early-stage disease and low-risk clinical features.
- Bone marrow testing involves two steps usually done at the same time in a doctor’s office or a hospital:
- A bone marrow aspiration to remove a liquid sample of bone marrow
Tests of heart and lung function
These tests might be done if certain chemo drugs that could affect the heart or the lungs are going to be used.
- An echocardiogram (an ultrasound of the heart) or a MUGA scan can be used to check heart function.
- Lung (pulmonary) function tests (PFTs) can be used to see how well the lungs are working.
Hodgkin Lymphoma Staging
Doctors use physical examinations, imaging tests, blood test and, sometimes, bone marrow tests to determine the extent of the disease. This determination is called “staging.” The stages of Hodgkin lymphoma tell you about the number and places in the body that are affected by lymphoma. Knowing the stage of Hodgkin lymphoma helps your doctor to decide what treatment you need.
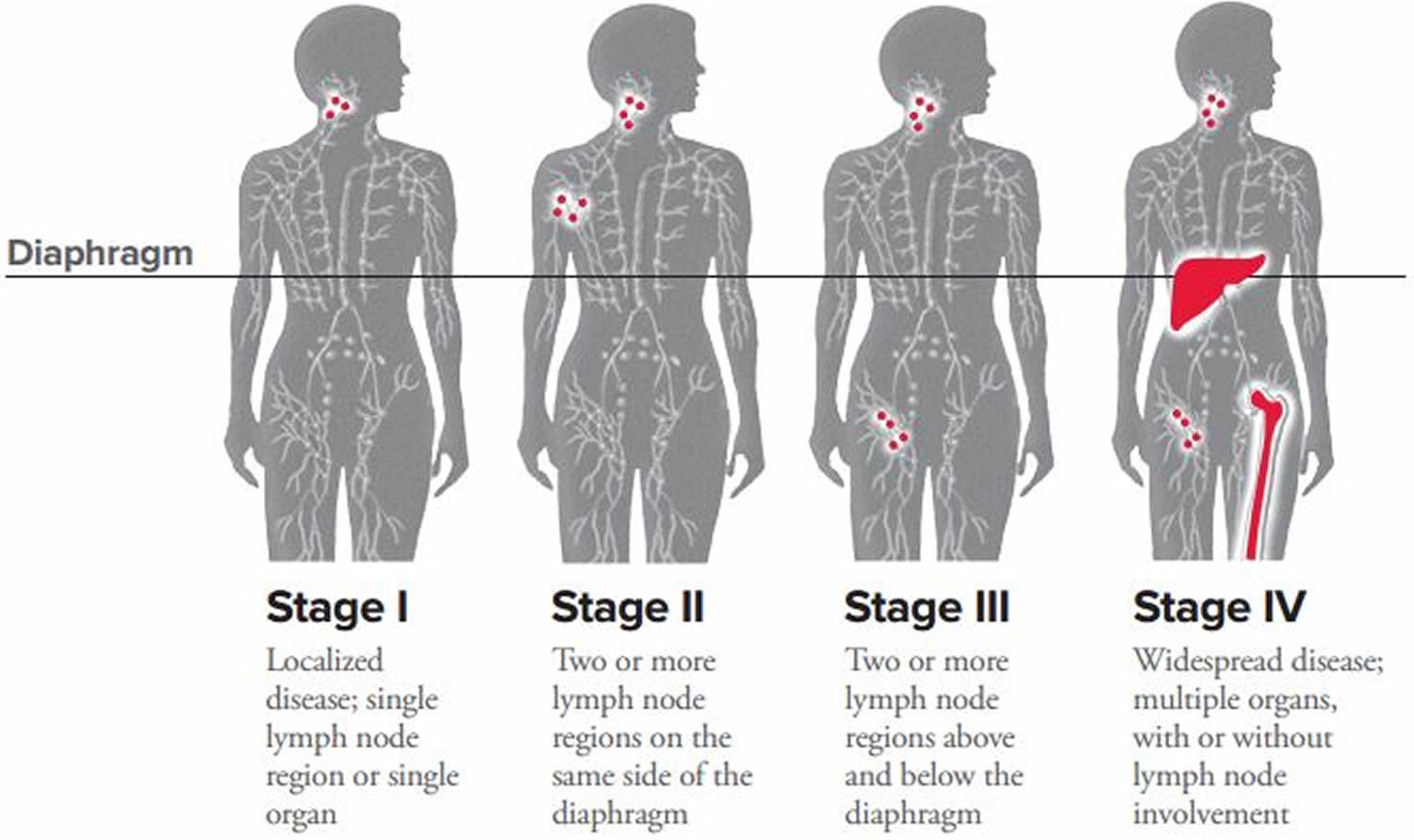
Staging for Hodgkin lymphoma is based the Lugano classification, which is based on the older Ann Arbor system. It has 4 stages, labeled 1, 2, 3, and 4. Or these can be simplified into limited or advanced stage.
- Limited stage generally means you have stage 1 or stage 2A Hodgkin lymphoma.
- Advanced stage means you have stage 2B, 3 or stage 4 Hodgkin lymphoma. Some people with stage 2 bulky lymphoma might have advanced disease, depending on their circumstances.
Other modifiers may also be used to describe the Hodgkin lymphoma stage:
- Bulky disease. This term is used to describe tumors in the chest that are at least ⅓ as wide as the chest, or tumors in other areas that are at least 10 centimeters (about 4 inches) across. It’s usually labeled by adding the letter X to the stage. It’s especially important for stage 2 lymphomas, because bulky disease may require more intensive treatment.
- A vs. B. Each stage may also be assigned a letter A or B to indicate whether you’re experiencing symptoms of Hodgkin’s lymphoma:
- The letter A means that you don’t have any significant symptoms as a result of the cancer.
- The Letter B is added (for example stage 3B) if a person has any of these B symptoms:
- Loss of more than 10% of body weight over the previous 6 months (without dieting)
- Unexplained fever of at least 100.4°F (38°C)
- Drenching night sweats
- If a person has any B symptoms, it usually means the lymphoma is more advanced, and more intensive treatment is often recommended. If no B symptoms are present, the letter A is added to the stage.
- Category E: The patient has Hodgkin lymphoma cells in organs or tissues outside the lymphatic system.
- Category S: The patient has Hodgkin lymphoma cells in the spleen.
Your treatment depends on your stage and category. Patients who fall into the B category usually need more aggressive treatment than A category patients do.
How doctors work out your Hodgkin’s lymphoma stage
Hodgkin lymphoma generally starts in the lymph nodes. If it spreads, it’s usually to another set of nearby lymph nodes. It can invade (grow into) nearby organs as well. Rarely, Hodgkin lymphoma will start in an organ other than lymph nodes, such as a lung.
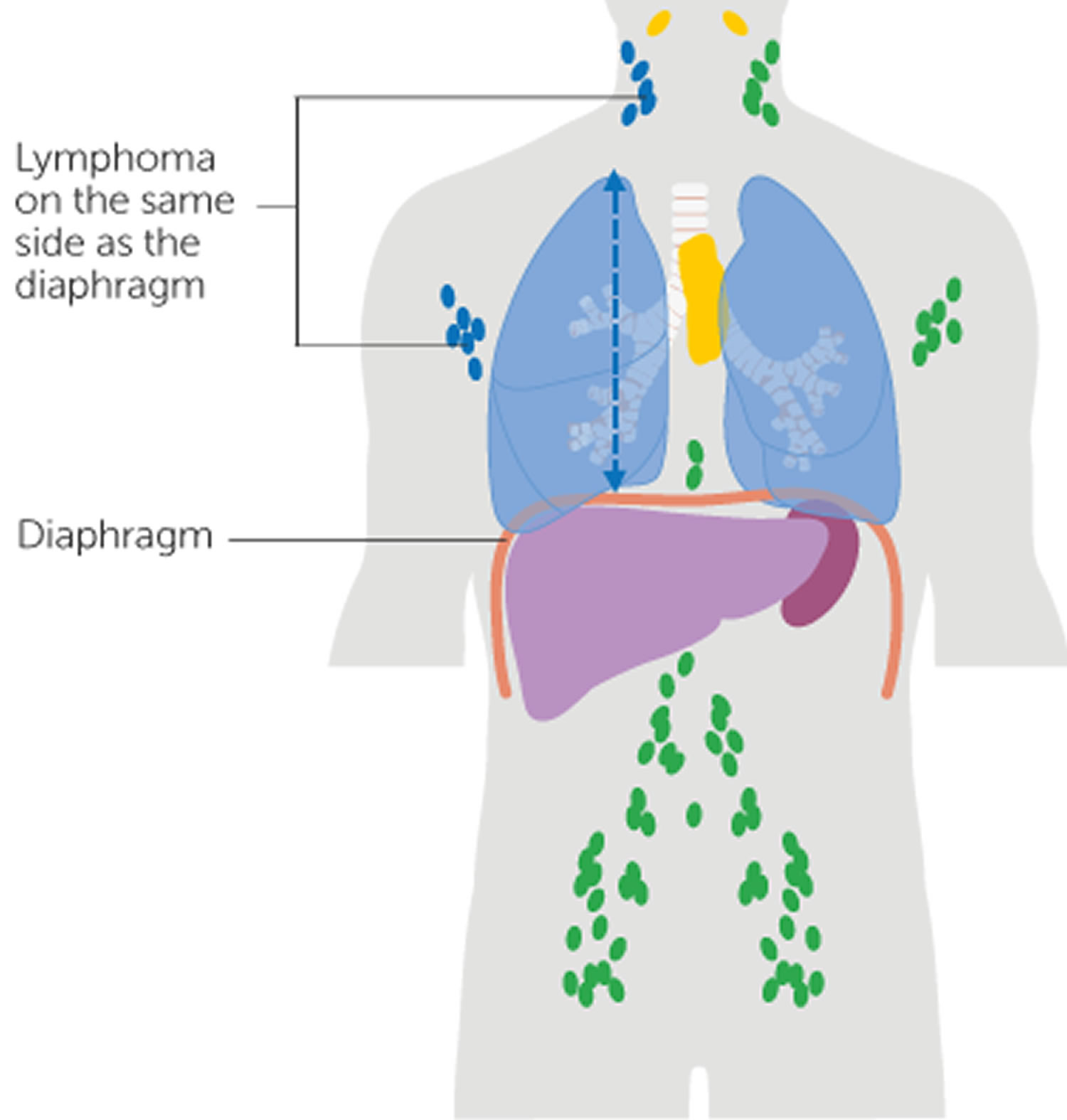
Doctors look at whether the Hodgkin lymphoma is on one side, or both sides of the diaphragm. And whether it is inside or outside of the lymphatic system. They will measure the size of the lymphoma. They do this by carrying out various tests, such as a CT or PET scan. They will also check whether you have any symptoms.
- The diaphragm. The diaphragm is the big breathing muscle that separates the chest from the tummy (abdominal) area. Doctors use the diaphragm as a guide because it is about halfway down the body.
- Inside or outside of the lymphatic system. Doctors look at whether the lymphoma is affecting:
- the lymph nodes and organs of the lymphatic system – these are called lymphatic sites. Lymphatic sites include a group of lymph nodes or an organ of the lymphatic system, such as the thymus or spleen.
- areas outside of the lymphatic sites – called extranodal (or extralymphatic) sites. Extranodal sites include the lungs, liver, blood, bone marrow, kidneys, brain and spinal cord.
- Your doctor may use the letter E after the stage number if you have lymphoma outside of the lymphatic system. Your doctor or nurse can explain what this means in your situation.
- B symptoms. Your doctor will add the letter B to your stage (for example, stage 1B) if you have any of the following symptoms:
- heavy sweating at night
- high temperatures that come and go, often at night
- unexplained weight loss, more than a tenth (10%) of your body weight in the last 6 months
- People with B symptoms may need more treatment than those without them.
- If you don’t have any of these symptoms your doctor will add the letter A to your stage (for example, stage 2A).
- Bulky disease means you have either:
- a lymph node that is 10 cm or more
- lymphoma in the center of your chest (mediastinum) which is at least a third of the width of your chest.
Table 2. Hodgkin Lymphoma Stages
| Stage 1 Hodgkin’s lymphoma |
|
| Stage 2 Hodgkin’s lymphoma |
In both cases, the 2 sites of lymphoma are on the same side of the diaphragm. |
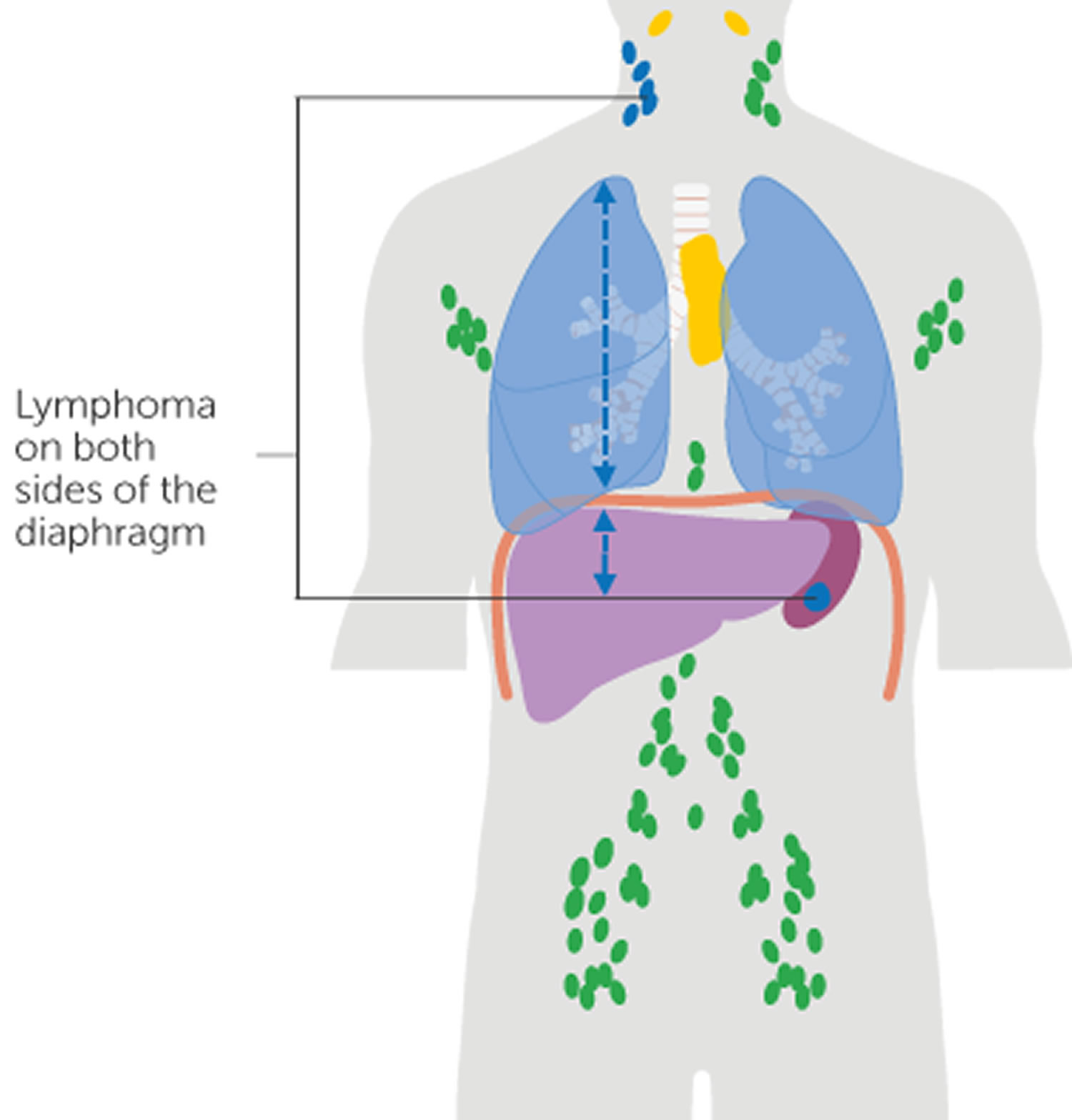
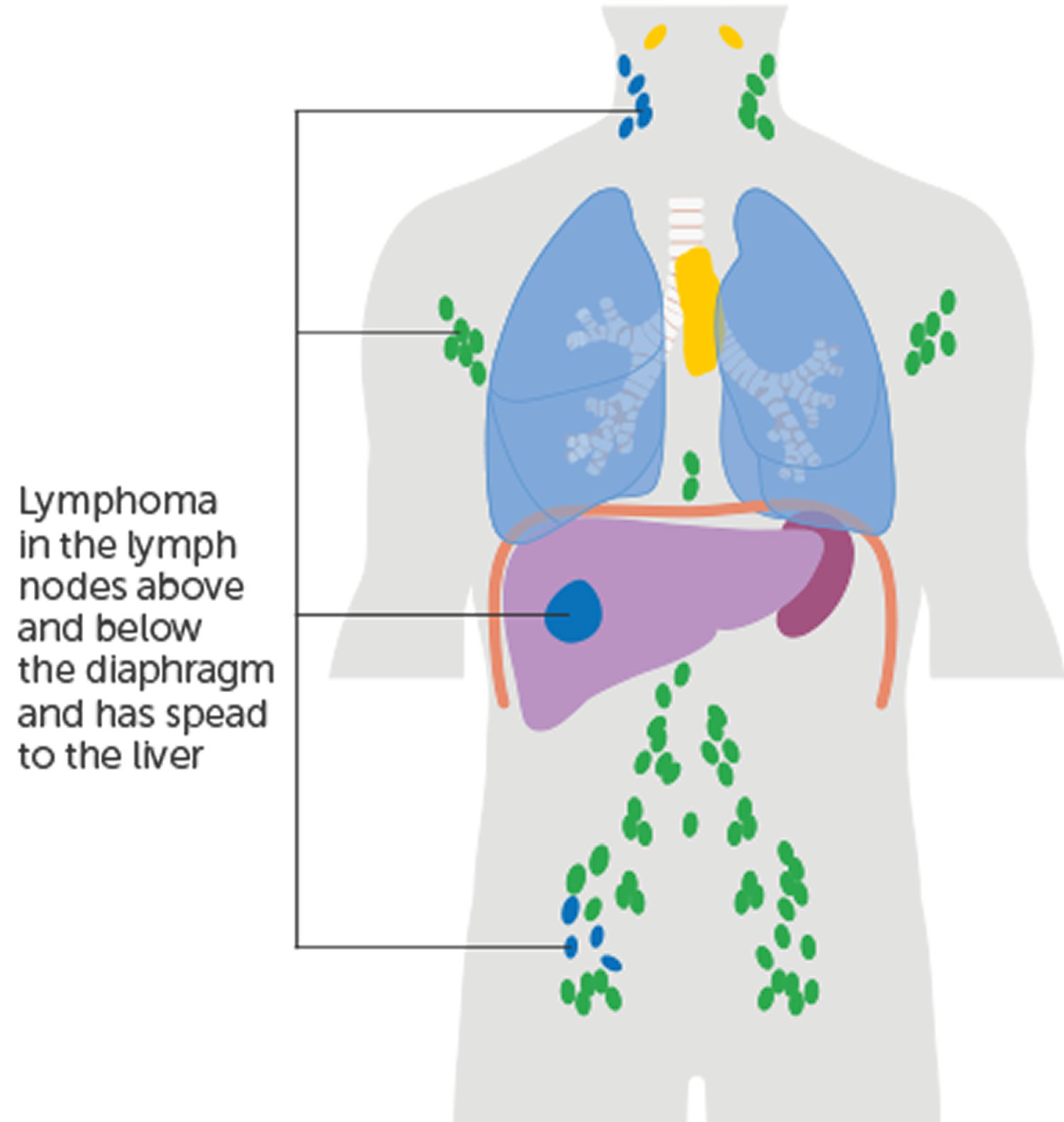
| Stage 3 Hodgkin’s lymphoma | Stage 3 Hodgkin’s lymphoma means that you have Hodgkin lymphoma cells on both sides of the diaphragm (above and below). One example is that the lymphoma is in lymph nodes on both sides of the diaphragm. Another example is that the lymphoma is in lymph nodes above the diaphragm, as well as lymphoma in the spleen. |
| Stage 4 Hodgkin’s lymphoma | Stage 4 Hodgkin’s lymphoma has spread widely into at least one organ outside of the lymph system, such as the liver, bone marrow, or lungs. Stage 4 Hodgkin’s lymphoma means one of the following:
|
Hodgkin Lymphoma Stages
Stage 1 Hodgkin’s lymphoma
Stage 1 Hodgkin’s lymphoma means that you have one of the following:
- Hodgkin lymphoma cells found in a single lymph node region (this can include single lymph node or a group of adjacent nodes) or in lymphoid organ such as the thymus above the diaphragm, OR
- Hodgkin lymphoma cells found in one organ or site outside the lymphatic system in an extranodal site (1E).

Stage 2 Hodgkin’s lymphoma
Stage 2 Hodgkin’s lymphoma means one of the following:
- Hodgkin lymphoma cells found in two or more lymph node regions on the same side of the diaphragm, either above or below, OR
- Hodgkin lymphoma cells found in a lymph node area and a nearby organ outside the lymphatic system (an extranodal site), on the same side of the diaphragm (2E)
In both cases, the 2 sites of lymphoma are on the same side of the diaphragm.
Stage 3 Hodgkin’s lymphoma
Stage 3 Hodgkin’s lymphoma means that you have Hodgkin lymphoma cells on both sides of the diaphragm (above and below). One example is that the lymphoma is in lymph nodes on both sides of the diaphragm. Another example is that the lymphoma is in lymph nodes above the diaphragm, as well as lymphoma in the spleen.
Stage 4 Hodgkin’s lymphoma
Stage 4 Hodgkin’s lymphoma has spread widely into at least one organ outside of the lymph system, such as the liver, bone marrow, or lungs.
Stage 4 Hodgkin’s lymphoma means one of the following:
- Hodgkin lymphoma cells have spread widely into one or more organs outside the lymphatic system (for example the liver, bones or lungs) and possibly into nearby lymph nodes, OR
- Hodgkin lymphoma cells found in one organ outside the lymphatic system (extranodal site) and also in distant lymph nodes
Resistant or recurrent Hodgkin lymphoma
Resistant or recurrent Hodgkin’s lymphoma is not part of the formal staging system, but doctors or nurses might use these terms to describe what’s going on with the lymphoma in some cases.
- The terms resistant or progressive disease are used when the lymphoma does not go away or progresses (grows) while you’re being treated.
- Recurrent or relapsed disease means that Hodgkin’s lymphoma went away with treatment, but it has now come back. If the lymphoma returns, it might be in the same place where it started or in another part of the body. This can happen shortly after treatment or years later.
Your doctors will not stage resistant or recurrent Hodgkin’s lymphoma in the same way as when you were first diagnosed. But you can still have more treatment and this will often work well. Your treatment may include a stem cell transplant.
Hodgkin Lymphoma Treatment Planning
Hodgkin lymphoma cases are generally classified into the three subgroups described below.
- Early-stage favorable: stage 1 to 2 with no unfavorable risk factors
- Early-stage unfavorable: stage 1 to 2 with one or more of the following unfavorable risk factors:
- Bulky disease: a mass in the chest that is one-third the width of the chest, or any lymph node mass greater than 10 centimeters
- Involvement of 3 or more lymph nodes
- B symptoms: fever, drenching night sweats and/or unexplained weight loss greater than 10 percent of body weight over 6 months
- Extranodal disease: involvement of an organ outside the lymphatic system
- Erythrocyte sedimentation rate (ESR) of 50 or higher
- Bulky disease: a mass in the chest that is one-third the width of the chest, or any lymph node mass greater than 10 centimeters
- Advanced stage: stage 3 to 4
- Seven factors (Adverse Prognostic Factors for Advanced-Stage) provide a basis for recommending either aggressive or less-intensive treatment options
- Adverse Prognostic Factors for Advanced-Stage Classical Hodgkin Lymphoma:
- Being male
- Age 45 or older
- Stage 4 disease
- Albumin level below 4 g/dL (grams per deciliter)
- Hemoglobin level below 10.5 g/dL
- Leukocytosis: white blood cell count greater than 15,000/mm³
- Lymphocytopenia: lymphocyte count less than 8% of the white blood cell count and/or lymphocyte count less than 600/mm³
The International Prognostic Score (IPS) assigns a point for each adverse prognostic factors present at diagnosis. The International Prognostic Score (IPS) helps doctors to determine the course of treatment and the prognosis for patients with advanced-stage (stage 3 to 4) disease.
Table 3. International Prognostic Index for Hodgkin lymphoma
| Hodgkin lymphoma International Prognostic Score |
|---|
| Criteria |
| Age > 45 |
| Male sex |
| Serum albumin concentration < 4.0 g per dL (40 g per L) |
| Hemoglobin concentration < 10.5 g per dL (105 g per L) |
| Ann Arbor stage 4 disease† Leukocytosis (≥ 15,000 μL [15 × 109 white blood cells per L]) Lymphopenia (< 600 lymphocytes per μL [0.6 × 109 per L], or < 8% of total white blood cell count) |
| Total score____ |
| Five-year overall survival rate based on number of criteria from International Prognostic Index/Score |
| Score 0 = 89% |
| Score 1 = 90% |
| Score 2 = 81% |
| Score 3 = 78% |
| Score 4 = 61% |
| Score ≥ 5 = 56% |
Footnote: Each criterion = 1 point.
† Ann Arbor stage 4 = noncontiguous extralymphatic involvement.
Hodgkin’s lymphoma Treatment
Which Hodgkin’s lymphoma treatments are right for you depends on the type and stage of your disease, your overall health, and your preferences. Treatment for Hodgkin lymphoma is changing due to new drugs and research findings from clinical trials. Therefore, before treatment begins, it is important to consider getting a second opinion at a center with a Hodgkin lymphoma expert.
It’s important that your doctor is experienced in treating patients with Hodgkin lymphoma or works in consultation with a Hodgkin lymphoma specialist. This type of specialist is called a hematologist-oncologist.
Hodgkin lymphoma is considered one of the most curable forms of cancer. Hodgkin lymphoma can usually be treated successfully with chemotherapy alone or chemotherapy followed by radiotherapy. Occasionally, chemotherapy may be combined with steroid medicine. Overall, treatment for Hodgkin lymphoma is highly effective and most people with the condition are eventually cured. For many people with Hodgkin lymphoma, starting treatment helps them focus on moving ahead and looking forward to recovery.
More than 80 percent of all patients diagnosed with Hodgkin lymphoma can be cured by current treatment approaches. The cure rate is higher, approaching 90 percent, in younger patients and in those with early-stage favorable Hodgkin lymphoma. Even in cases of advanced stage Hodgkin lymphoma, the disease is often highly curable.
Most patients become long-term survivors of Hodgkin’s lymphoma. Other treatment goals are to:
- Maximize cures in all stages of the disease
- Minimize both short-term and long-term side effects and complications
- Weigh the risks of toxicity against treatment benefits
Types of Hodgkin’s lymphoma treatment
Doctors use several types of approaches and treatment combinations for adults and children with Hodgkin lymphoma, some at different stages:
- Chemotherapy
- Radiotherapy also known as “radiation therapy”
- Monoclonal Antibody Therapy
- Immunotherapy
- Stem cell transplantation also known as bone marrow transplant
- Your doctor may suggest that you participate in a clinical trial. Clinical trials can involve therapy with new drugs and new drug combinations or new approaches to stem cell transplantation.
After initial clinical staging for Hodgkin lymphoma, patients with early favorable disease or early unfavorable disease are treated with ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) chemotherapy with or without involved-field or nodal radiation.
Patients with advanced-stage disease are primarily treated with chemotherapy alone, although subsequent radiation therapy may be applied for initial bulky disease (≥10 cm mediastinal mass) or for residual adenopathy (>2.5 cm) with positive findings after a postchemotherapy positron emission tomography (PET) scan 11. Treatment regimen preferences and application, as well as relative risks, differ regionally.
Patients with Hodgkin lymphoma who are older than 60 years may have more treatment-related morbidity and mortality; maintaining the dose intensity of standard chemotherapy may be difficult 12. Other therapies have been proposed for elderly patients too frail to withstand conventional regimens, but no randomized trials have been conducted with these regimens 13. Twenty-seven previously untreated patients older than 60 years, judged by the investigator to be in poor condition and unable to undergo chemotherapy, received brentuximab vedotin. A 92% overall response rate and 73% complete remission rate were reported 14. Brentuximab vedotin has been combined with dacarbazine 15 or sequentially with AVD (doxorubicin, vinblastine, dacarbazine) 16, reporting acceptable toxicities in an elderly population. A retrospective review of 287 patients aged 60 years or older with early-stage favorable Hodgkin lymphoma in two German Hodgkin Study Group trials (HD10 and HD13) showed increased bleomycin-induced lung toxicity with more than two cycles of exposure to bleomycin 17.
Table 4. Treatment Options for Adult Hodgkin Lymphoma
| Prognostic Group | Treatment Options |
|---|---|
| Early favorable classic Hodgkin lymphoma | Chemotherapy with or without radiation therapy |
| Early unfavorable classic Hodgkin lymphoma | Chemotherapy with or without radiation therapy |
| Advanced classic Hodgkin lymphoma | Chemotherapy |
| Recurrent classic Hodgkin lymphoma | Nivolumab or pembrolizumab |
| Brentuximab vedotin | |
| Brentuximab vedotin plus nivolumab | |
| Chemotherapy with stem cell transplant | |
| Combination chemotherapy | |
| Radiation therapy | |
| Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) | Watchful waiting/active surveillance |
| Radiation therapy | |
| Chemotherapy | |
| Rituximab | |
| Hodgkin lymphoma during pregnancy | Watchful waiting |
| Radiation therapy | |
| Chemotherapy |
Pretreatment Considerations
Adults of childbearing age and parents of children diagnosed with Hodgkin lymphoma should ask their doctors for information that may lessen the risk of infertility.
Finding the Best Treatment Approach
The goal of Hodgkin lymphoma treatment is to cure the disease.
- The treatment your doctor recommends is based on several factors, including:
- Your disease subtype
- Your disease stage and category
- Whether your disease is either refractory (the disease does not respond to treatment) or relapsed (the disease has recurred after treatment)
- Your age
- Whether you have coexisting diseases or conditions (for example, heart disease, kidney disease, diabetes)
As you develop a treatment plan with your doctor, be sure to discuss:
- The results you can expect from treatment
- The potential side effects, including long-term effects and late-term effects
- The possibility of participating in a clinical trial, where you may have access to advanced medical treatment that may be more beneficial to you than standard treatment
You may find it helpful to bring a loved one with you to your doctor’s visits for support, to take notes and to ask follow-up questions. It’s a good idea to prepare questions you’d like to ask when you visit your doctor. You can also record your conversations with your doctor and listen more closely when you get home.
Chemotherapy Drug Combinations
Chemotherapy (chemo) is a drug treatment that uses chemicals to kill lymphoma cells. Chemotherapy (chemo) is the main treatment for most people with Hodgkin lymphoma (other than some people with nodular lymphocyte-predominant Hodgkin lymphoma, or NLPHL). Chemotherapy drugs travel through your bloodstream and can reach nearly all areas of your body and destroy cancer cells wherever they may be. Chemotherapy (chemo) can be given in a number of different ways, depending on the stage of your lymphoma. If doctors think your lymphoma is curable, you’ll normally receive chemotherapy through a drip directly into a vein (intravenous chemotherapy). If a cure is unlikely, you may only need to take chemotherapy tablets to help relieve your symptoms.
Chemotherapy is often combined with radiation therapy in people with early-stage classical type Hodgkin’s lymphoma. Radiation therapy is typically done after chemotherapy. In advanced Hodgkin’s lymphoma, chemotherapy may be used alone or combined with radiation therapy.
Children and young adults with Hodgkin lymphoma are usually treated with combination chemotherapy and involved field radiation therapy.
Chemo is given in cycles that include a period of treatment followed by a rest period to give the body time to recover. In general, each cycle lasts for several weeks.
Most chemo treatments are given in the doctor’s office, clinic, or hospital outpatient department, but some may require a hospital stay.
Common chemotherapy drug combinations used to treat children and young adults include:
- ABVD: doxorubicin (Adriamycin®), bleomycin (Blenoxane®), vinblastine (Velban®), dacarbazine (DTIC-Dome®). ABVD is the most common regimen used in the United States.
- AV-PC: doxorubicin (Adriamycin®), vincristine (Oncovin®), prednisone and cyclophosphamide (Cytoxan®)
- ABVE: doxorubicin (Adriamycin®), bleomycin (Blenoxane®), vincristine (Oncovin®), and etoposide (Etopophos®, Toposar®, VePesid®, VP-16)
- ABVE-PC: doxorubicin (Adriamycin®), bleomycin (Blenoxane®), vincristine (Oncovin®), etoposide (Etopophos®, Toposar®, VePesid®, VP-16), prednisone and cyclophosphamide (Cytoxan®)
- BEACOPP: bleomycin (Blenoxane®), etoposide (Etopophos®, Toposar®, VePesid®, VP-16), doxorubicin (Adriamycin®), cyclophosphamide (Cytoxan®), vincristine (Oncovin®), procarbazine (Matulane®) and prednisone
- OEPA: vincristine (Oncovin®), etoposide (Etopophos®, Toposar®, VePesid®, VP-16), prednisone, and doxorubicin (Adriamycin®)
- Stanford V: Doxorubicin (Adriamycin), Mechlorethamine (nitrogen mustard), Vincristine, Vinblastine, Bleomycin, Etoposide and Prednisone
- Another drug that can be considered as chemo is brentuximab vedotin (Adcetris). This is an antibody-drug conjugate, which is a monoclonal antibody attached to a chemo drug.
Early-stage classical Hodgkin lymphoma (cHL)
- Chemotherapy combinations
- ABVD (Adriamycin® [doxorubicin], bleomycin, vinblastine, dacarbazine)
- Escalated BEACOPP (bleomycin, etoposide, Adriamycin [doxorubicin], cyclophosphamide, Oncovin® [vincristine], procarbazine, prednisone)
- Combination chemotherapy is administered with or without radiation therapy.
Advanced-stage classical Hodgkin lymphoma (cHL)
- Chemotherapy combinations
- A+AVD (Adcetris® [brentuximab vedotin], Adriamycin [doxorubicin], vinblastine, dacarbazine)
- ABVD
- ABVD followed by escalated BEACOPP
- Occasionally, chemotherapy is followed by involved-site radiation therapy (ISRT).
Side effects of chemotherapy depend on the drugs you’re given. Common side effects are nausea, vomiting and hair loss. The most significant side effect of chemotherapy is potential damage to your bone marrow. This can interfere with the production of healthy blood cells and cause the following problems:
- fatigue
- breathlessness
- increased vulnerability to infection
- bleeding and bruising more easily
If you experience these problems, treatment may need to be delayed so you can produce more healthy blood cells. Growth factor medicines can also stimulate the production of blood cells.
Other possible side effects of chemotherapy include:
- diarrhea
- loss of appetite
- mouth ulcers
- tiredness
- skin rashes
- infertility, which may be temporary or permanent
Serious long-term complications can occur, such as heart damage, lung damage and other cancers, such as leukemia.
If regular chemotherapy is unsuccessful or Hodgkin lymphoma returns after treatment, you may have a course of chemotherapy at a higher dose.
However, this intensive chemotherapy destroys your bone marrow, leading to the problems mentioned above. You’ll need a stem cell or bone marrow transplant to replace the damaged bone marrow.
Table 5. Chemotherapy Regimens Used to Treat Hodgkin Lymphoma
| Combination Name | Drugs Included | Prognostic Group |
|---|---|---|
| ABVD | Doxorubicin, bleomycin, vinblastine, and dacarbazine | Early favorable classic Hodgkin’s lymphoma |
| Early unfavorable classic Hodgkin’s lymphoma | ||
| AVD | Doxorubicin, vinblastine, and dacarbazine | Early favorable classic Hodgkin’s lymphoma |
| Advanced classic Hodgkin’s lymphoma | ||
| BEACOPP | Bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone | Early unfavorable classic Hodgkin’s lymphoma |
| Advanced classic Hodgkin’s lymphoma | ||
| GVD | Gemcitabine, vinorelbine, and liposomal doxorubicin | Recurrent classic Hodgkin’s lymphoma |
| ICE | Ifosfamide, carboplatin, and etoposide | Recurrent classic Hodgkin’s lymphoma |
| MOPP | Mechlorethamine, vincristine, procarbazine, and prednisone | Advanced classic Hodgkin’s lymphoma |
Radiation therapy
Radiation therapy also known as “radiotherapy”, uses high-energy beams, such as X-rays and protons, to kill cancer cells. Radiation therapy is most often used to treat early-stage Hodgkin lymphoma, where the cancer is only in 1 part of the body. Involved-site radiation therapy (ISRT) is sometimes used to treat Hodgkin’s lymphoma. It selectively treats the lymph nodes where the cancer started and the cancerous masses near those nodes. With a special machine, carefully focused beams of radiation are directed at the cancer. This is also called “external beam therapy” (EBT). The size of the targeted area is restricted to minimize radiation exposure to adjacent, uninvolved organs, and to decrease the side effects associated with radiation therapy.
For classical Hodgkin’s lymphoma (cHL), radiation therapy is often used after chemotherapy. People with early-stage nodular lymphocyte-predominant Hodgkin’s lymphoma may undergo radiation therapy alone.
During radiation therapy, you lie on a table and a large machine moves around you, directing the energy beams to specific points on your body. Radiation can be aimed at affected lymph nodes and the nearby area of nodes where the disease might progress. The length of radiation treatment varies, depending on the stage of the disease. A typical treatment plan might have you going to the hospital or clinic five days a week for several weeks. At each visit, you undergo a 30-minute radiation treatment. For example, radiation therapy treatment is normally given in short daily sessions, Monday to Friday, over several weeks. You shouldn’t have to stay in hospital between appointments.
With careful planning, the exposure of uninvolved organs can be either reduced or avoided during radiation therapy. Imaging techniques such as magnetic resonance imaging (MRI), positron emission tomography-computed tomography (PET-CT), and other specialized imaging techniques can enhance treatment planning.
Radiotherapy itself is painless, but it can have some significant side effects. These can vary and will be directly related to the part of your body being treated. For example, treatment to your throat can lead to a sore throat, while treatment to the head can lead to hair loss.
Other common side effects include:
- tiredness
- nausea and vomiting
- dry mouth
- loss of appetite
Most side effects are temporary, but there’s a risk of long-term problems, including infertility and permanently darkened skin in the treatment area. More-serious risks include heart disease, stroke, thyroid problems and other cancers, such as breast or lung cancer.
Steroid medicine
Steroid medicine is sometimes used in combination with chemotherapy as a more intensive treatment for advanced Hodgkin lymphoma, or if initial treatment hasn’t worked.
The steroid medicine is given intravenously, usually at the same time as your chemotherapy.
Common side effects of steroid medicine include:
- increased appetite, which can lead to weight gain
- indigestion
- problems sleeping
- feeling agitated
The side effects of steroid medicine usually start to improve once treatment finishes.
Monocolonal Antibody Therapy
This is a type of targeted therapy. When the body’s immune system identifies something harmful, such as bacteria or a virus, it produces antibodies. Antibodies are proteins that help fight infection. Monoclonal antibodies are a type of protein made in the laboratory that can bind to only one substance. By design, they can only attack a specific target, typically a substance on cancer cells (though sometimes they are designed to bind to a substance on immune cells, in order to improve their function). This targeting can reduce damage to normal, healthy cells.
In patients with classical Hodgkin’s lymphoma, the malignant Hodgkin and Reed-Sternberg cells typically express a protein called CD30. Brentuximab vedotin (Adcetris®) is an anti-CD30 antibody attached to a chemotherapy drug. It binds to cells that express CD30 and then enters the cancer cells. Once inside the cancer cells, it releases the chemotherapy drug. By targeting only cells that express CD30, fewer normal cells are harmed.
Brentuximab vedotin, given intravenously (IV), is approved for the treatment of adult patients with previously untreated Stage 3 or 4 classical Hodgkin lymphoma (cHL), in combination with doxorubicin, vinblastine, and dacarbazine. The drug is also approved for other indications such as some cases of relapsed Hodgkin’s lymphoma and certain other lymphomas with CD30 expression.
Rituximab (Rituxan®) is a monoclonal antibody designed to bind to cells expressing CD20. Rituximab is often combined with chemotherapy drugs. Rituximab (Rituxan®) is not used to treat classical Hodgkin’s lymphoma (cHL) because, in this subtype of the disease, the lymphoma cells do not usually express CD20. However, it is sometimes used to treat nodular lymphocyte predominant Hodgkin’s lymphoma (NLPHL) because CD20 is expressed by the lymphoma cells in this subtype of the disease. In rituximab therapy, the monoclonal antibodies attach to and kill the lymphoma cells.
Immunotherapy
Immunotherapy uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer. This cancer treatment is a type of biologic therapy. Immunotherapy can be used to treat some people with Hodgkin lymphoma.
Immune checkpoint inhibitors (PD-1 and PD-L1 inhibitor therapy) are a type of immunotherapy. Checkpoints are molecules found on T-cells, a type of white blood cell. PD-1 is a protein on the surface of T cells that helps keep the body’s immune responses in check. PD-L1 is a protein found on some types of cancer cells. T cells circulate throughout the body looking for signs of infection and diseases, including cancer. When a T cell comes across any type of cell, it probes (looks for) certain proteins on the cell’s surface. If the T cell determines that it is a normal, healthy cell, it moves on to check other cells. If the proteins indicate that the cell is foreign or cancerous, the T cell attacks it. But cancer cells can sometimes send misleading signals to these checkpoints, telling the T cells that they are not harmful. When PD-1 attaches to PD-L1, it stops the T cell from killing the cancer cell.
Checkpoint inhibitors (PD-1 and PD-L1 inhibitors) work by blocking the signals that cancer cells send to T cells. Checkpoint inhibitors (PD-1 and PD-L1 inhibitors) keep PD-1 and PD-L1 proteins from attaching to each other. When the signals are blocked, it is more likely the T cells will distinguish the cancer cells from healthy cells and allows the T cells to kill cancer cells.
Nivolumab (Opdivo®) and pembrolizumab (Keytruda®) are checkpoint inhibitors (PD-1 inhibitors), both given by IV, that can be used for some patients with Hodgkin lymphoma that has become refractory (come back or spread during treatment), or that has relapsed (returned) after completing other treatments. They are also used to treat certain other types of cancer in which their effects on the immune system can be helpful.
Nivolumab is FDA-approved for the treatment of adult patients with classical Hodgkin lymphoma that has relapsed or progressed after:
- Autologous hematopoietic stem cell transplantation (HSCT) and brentuximab vedotin, OR
- 3 or more lines of systemic therapy that includes autologous hematopoietic stem cell transplantation (HSCT).
Pembrolizumab is FDA-approved for the treatment of adult and pediatric patients with refractory classical Hodgkin lymphoma or who have relapsed after 3 or more prior lines of therapy.
Bone marrow transplant
Bone marrow transplant also known as stem cell transplant, is a treatment to replace your diseased bone marrow with healthy stem cells that help you grow new bone marrow. A bone marrow transplant may be an option if Hodgkin’s lymphoma returns despite treatment.
There are two main types of stem cell transplantation:
- Autologous stem cell transplantation, a procedure in which your own blood stem cells are removed, frozen and stored for later use. Next you receive high-dose chemotherapy and radiation therapy to destroy cancerous cells in your body. Finally your stem cells are thawed and injected into your body through your veins. The stem cells help build healthy bone marrow.
- Allogeneic stem cell transplantation, a procedure in which patients receive stem cells from a donor after they undergo intensive chemotherapy. Allogeneic stem cell transplantation has been successful in some patients with Hodgkin’s lymphoma after several relapses of the disease, but it is not commonly used as a treatment for Hodgkin lymphoma. It is generally only done if a patient relapses after an autologous transplant.
People who undergo bone marrow transplant may be at increased risk of infection.
In almost all cases, autologous stem cell transplantation is used for Hodgkin’s lymphoma. It remains the standard therapy for relapsed and refractory cases of Hodgkin lymphoma.
The first step is to collect the patient’s own stem cells after initial treatment is completed and the patient is in remission. The stem cells are removed from the patient’s bone marrow (inside the bones), and are frozen and stored until they are needed for the transplant. The patient is then given high doses of chemotherapy to destroy any lymphoma cells not killed during the initial treatment. After the high-dose chemotherapy is completed, the stem cells are returned to the patient’s bloodstream by IV infusion (similar to a blood transfusion). The goal is to “rescue” the bone marrow from the effects of the high doses of chemotherapy, reintroducing healthy stem cells into the system in order to restore normal blood cell production.
Brentuximab vedotin is sometimes also given to patients before the bone marrow transplant, or, in select patients, it is administered as maintenance treatment after autologous stem cell transplantation
Allogeneic stem cell transplantation has been successful in some patients with Hodgkin lymphoma after several relapses of the disease, but it is not commonly used as a treatment for Hodgkin lymphoma. It is generally only done if a patient relapses after an autologous transplant.
Treating Classic Hodgkin Lymphoma by Stage
Treatment options for classic Hodgkin lymphoma depend on many factors, including:
- The type of Hodgkin lymphoma
- The stage (extent) of the Hodgkin lymphoma
- Whether or not the disease is bulky (large)
- Whether the disease is causing B symptoms
- Results of blood tests and other lab tests
- A person’s age
- A person’s overall health
- Personal preferences
Based on these factors, a person’s treatment might be a little different from the general outline below.
Stage 1 Hodgkin’s lymphoma treatment
Treatment for stage 1 Hodgkin lymphoma is usually 2 to 4 cycles of chemotherapy. You might also have radiotherapy.
Treatment for many patients is chemotherapy (usually 2 to 4 cycles of the ABVD regimen), followed by radiation to the initial site of the disease (involved site radiation therapy [ISRT]). Another option is chemotherapy alone (usually for 3 to 6 cycles) in selected patients.
Doctors often order a PET/CT scan after a few courses of chemo to see how well the treatment is working and to determine how much more treatment (if any) is needed.
If a person can’t have chemotherapy because of other health issues, radiation therapy alone may be an option.
For those who don’t respond to treatment, chemo using different drugs or high-dose chemo (and possibly radiation) followed by a stem cell transplant may be recommended. Treatment with an immunotherapy drug such as brentuximab vedotin (Adcetris), nivolumab (Opdivo), or pembrolizumab (Keytruda) might be another option.
Stage 2 Hodgkin’s lymphoma treatment
Treatment for stage 2 Hodgkin lymphoma is usually 2 to 4 cycles of chemotherapy. You might also have radiotherapy.
Treatment is generally more intense than that for favorable disease. It typically starts with chemotherapy (usually with the ABVD regimen for 4 to 6 cycles or other regimens such as 3 cycles of Stanford V).
PET/CT scans are often done after several cycles of chemo to see if (and how much) more treatment is needed. This is often followed by more, and maybe different, chemo. Radiation therapy (involved field radiation therapy [IFRT]) is usually given to the sites of the tumor at this point, especially if it was bulky disease.
For those who don’t respond to treatment, chemo using different drugs or high-dose chemo (and possibly radiation) followed by a stem cell transplant may be recommended. Treatment with an immunotherapy drug such as brentuximab vedotin (Adcetris), nivolumab (Opdivo), or pembrolizumab (Keytruda) might be another option.
Stage 3 Hodgkin’s lymphoma treatment
Treatment for stage 3 Hodgkin lymphoma, is generally between 6 to 8 cycles of chemotherapy. You might have steroids as part of this. And you may also have radiotherapy.
Doctors generally treat stage 3 Hodgkin lymphoma with chemotherapy using more intense regimens than that used for earlier stages. The ABVD regimen (for at least 6 cycles) is often used, but some doctors favor more intense treatment with the Stanford V regimen for 3 cycles, or up to 8 cycles of the BEACOPP regimen if there are several unfavorable prognostic factors. Another option for some people might be chemo plus the drug brentuximab vedotin (Adcetris).
PET/CT scans might be used during or after chemo to assess how much more treatment you need. Depending on the results of the scans, more chemo may be given. Radiation therapy may be given after chemo, especially if there were any large tumor areas.
For those whose Hodgkin lymphoma doesn’t respond to treatment, chemo using different drugs or high-dose chemo (and possibly radiation) followed by a stem cell transplant may be recommended. Treatment with an immunotherapy drug such as brentuximab vedotin (Adcetris), nivolumab (Opdivo), or pembrolizumab (Keytruda) might be another option.
Stage 4 Hodgkin’s lymphoma treatment
Treatment for stage 4 Hodgkin lymphoma is usually between 6 to 8 cycles of chemotherapy. You might have steroids as part of this. And you may also have radiotherapy.
Doctors generally treat stage 4 Hodgkin lymphoma with chemotherapy using more intense regimens than that used for earlier stages. The ABVD regimen (for at least 6 cycles) is often used, but some doctors favor more intense treatment with the Stanford V regimen for 3 cycles, or up to 8 cycles of the BEACOPP regimen if there are several unfavorable prognostic factors. Another option for some people might be chemo plus the drug brentuximab vedotin (Adcetris).
PET/CT scans might be used during or after chemo to assess how much more treatment you need. Depending on the results of the scans, more chemo may be given. Radiation therapy may be given after chemo, especially if there were any large tumor areas.
For those whose Hodgkin lymphoma doesn’t respond to treatment, chemo using different drugs or high-dose chemo (and possibly radiation) followed by a stem cell transplant may be recommended. Treatment with an immunotherapy drug such as brentuximab vedotin (Adcetris), nivolumab (Opdivo), or pembrolizumab (Keytruda) might be another option.
Treatment Response Monitoring
During treatment, patients need to be monitored to check their response to therapy. Response to treatment is important in predicting long-term outcomes. Patients who fail to reach complete remission with first-line treatment have a worse prognosis, so there is great value in identifying these patients early in the course of their disease.
Imaging tests are used to distinguish between tumor and fibrous (scar) tissue. PET-CT scans help doctors determine if the disease is responding to treatment. PET-CT has become the standard method for assessment of treatment response in most types of lymphoma.
The Deauville score, based on a five-point scale developed in 2009, is now an internationally recognized way of using PET-CT to assess treatment response. This scale determines the “FDG uptake” (the absorption of this radioactive material by tissues) in the involved sites. The Deauville score is then used to determine if any treatment modifications are needed.
Table 6. Deauville Score for Assessing PET-CT Scans
| PET-CT finding | Score |
|---|---|
| No FDG uptake related to lymphoma | 1 |
| FDG uptake at lymphoma site is ≤ mediastinum FDG uptake | 2 |
| FDG uptake at lymphoma site is > mediastinum FDG uptake but < liver FDG uptake | 3 |
| FDG uptake at lymphoma site is > liver FDG uptake at any site | 4 |
| FDG uptake at lymphoma site is substantially > liver FDG uptake or new FDG uptake sites found | 5 |
Abbreviations: FDG = fluorodeoxyglucose; PET-CT = positron emission tomography/computed tomography
[Source 19 ]Treatment Options for Nodular Lymphocyte-Predominant Hodgkin lymphoma (NLPHL)
Nodular lymphocyte predominant Hodgkin’s lymphoma (NLPHL) is a rare subtype of Hodgkin lymphoma that accounts for only about 5 percent of all Hodgkin lymphoma cases. The cancer cells in NLPHL are a variant of Reed-Sternberg cells. They are larger and are sometimes called “popcorn” cells because their unique shape is similar to pieces of popcorn.
Nodular lymphocyte predominant Hodgkin’s lymphoma (NLPHL) tends to progress more slowly than classical Hodgkin’s lymphoma (cHL), so the treatment approach is usually different. About 75 percent of patients with NLPHL have stage I disease at diagnosis. It is rare for NLPHL patients to have B symptoms or disease involvement outside of the lymph nodes, and mediastinal masses and bulky disease are also rare.
Because NLPHL is associated with an excellent long-term survival rate, the risk of overtreatment is an important consideration for these patients. Overtreatment may lead to problems and harmful side effects from cancer therapies that are not needed. One option for some patients is the “watch-and-wait” approach, in which the patient is closely monitored for disease progression without getting any treatment until symptoms appear or begin to change. Another option for early-stage NLPHL without any B symptoms or bulky disease is the use of radiation therapy alone.
Combination chemotherapy may be needed in more advanced stages of the disease, with rituximab (Rituxan®) added to the regimen in some cases.
Common treatments used in NLPHL include:
- ABVD + rituximab (Adriamycin® [doxorubicin], bleomycin, vinblastine, dacarbazine + rituximab)
- CHOP + rituximab (cyclophosphamide, doxorubicin, vincristine, prednisone + rituximab)
- CVP + rituximab (cyclophosphamide, vinblastine, prednisone + rituximab)
- Rituximab (Rituxan®) alone
Nodular lymphocyte predominant Hodgkin’s lymphoma (NLPHL) can sometimes recur many years (or even decades) after initial treatment. In a small percentage of patients, it can transform into diffuse large B-cell lymphoma (DLBCL), a type of non-Hodgkin lymphoma that is usually aggressive. For patients with a suspected relapse of NLPHL, another biopsy should be considered to rule out transformation to DLBCL. Patients with refractory or relapsed NLPHL can be treated with a second-line therapy that includes rituximab, either with or without chemotherapy or radiation therapy.
Treatments for Relapsed or Refractory Hodgkin’s lymphoma
Most patients with classical Hodgkin’s lymphoma (cHL) are cured by their initial (first-line) treatment. However, in a significant percentage of patients—especially those with advanced-stage Hodgkin lymphoma—the disease relapses or is refractory. Relapse means the disease comes back after a remission following treatment. Refractory means the disease has not responded to treatment. For these patients, Hodgkin lymphoma is still potentially curable.
For patients who are not cured with initial therapy, second-line treatment options include:
- Alternate chemotherapy combinations
- Monoclonal antibody therapy with brentuximab vedotin
- Checkpoint inhibitors, nivolumab and pembrolizumab
- Autologous stem cell transplantation
Alternate Chemotherapy Combinations. Traditional chemotherapy-based regimens include:
- ICE (ifosfamide, carboplatin, etoposide)
- DHAP (dexamethasone, High-dose Ara-C [cytarabine], Platinol [cisplatin])
- ESHAP (etoposide, methylprednisolone, high-dose cytarabine, cisplatin)
- IGEV (ifosfamide, gemcitabine, vinorelbine)
- GDP (gemcitabine, dexamethasone, Platinol [cisplatin])
- GVD (gemcitabine, vinorelbine, liposomal doxorubicin)
Brentuximab vedotin (Adcetris®) is a monoclonal antibody drug combination given intravenously (IV). Brentuximab vedotin is approved by the FDA for the treatment of adult patients with previously untreated stage III or stage IV classical Hodgkin lymphoma (cHL), in combination with chemotherapy (doxorubicin, vinblastine and dacarbazine). It is also approved for classical Hodgkin lymphoma (cHL) patients at high risk of relapse or progression as postautologous hematopoietic stem cell transplantation (auto-HSCT) consolidation and for classical Hodgkin lymphoma (cHL) patients after failure of auto-HSCT or after failure of at least two prior multi-agent chemotherapy regimens in patients who are not auto-HSCT candidates.
As a second-line therapy, brentuximab vedotin can be used:
- Alone, as a single agent
- In combination with chemotherapy
- In combination with checkpoint inhibitors
- As maintenance therapy after an autologous stem cell transplantation
Nivolumab (Opdivo®) is a checkpoint inhibitor given by IV, is FDA-approved for the treatment of adult patients with classical Hodgkin’s lymphoma (cHL) that has relapsed or progressed after:
- Autologous stem cell transplantation and brentuximab vedotin, OR
- 3 or more lines of systemic therapy that included autologous stem cell transplant
Pembrolizumab (Keytruda®) is a checkpoint inhibitor given IV. It is approved by the FDA for the treatment of adult and pediatric patients with refractory classical Hodgkin’s lymphoma (cHL), or who have relapsed after 3 or more prior lines of therapy.
Refractory Hodgkin lymphoma treatment
Treatment for Hodgkin lymphoma should remove all traces of the lymphoma. After treatment, the doctor will do tests such as PET/CT scans to look for any signs of Hodgkin lymphoma. If Hodgkin lymphoma is still there, most experts think that more of the same treatment is unlikely to cure it.
Sometimes, radiation therapy to an area of disease that remains after chemotherapy might be curative. Using a different combination of chemo drugs is another option. If radiation alone was the initial treatment, using chemo (with or without more radiation) might also be curative.
If Hodgkin lymphoma is still there after these treatments, most doctors would recommend high-dose chemo (and possibly radiation) followed by an autologous stem cell transplant, if it can be done. If cancer still remains after this, an allogeneic stem cell transplant may be an option.
Another option, either instead of or after a stem cell transplant, may be treatment with an immunotherapy drug, such as brentuximab vedotin (Adcetris), nivolumab (Opdivo), or pembrolizumab (Keytruda).
Recurrent or relapsed Hodgkin lymphoma treatment
If Hodgkin lymphoma comes back (recurs) after treatment, further treatment depends on where the lymphoma comes back, on how long it has been since the initial treatment, and on what the initial treatment was.
If the initial treatment was radiation therapy alone, chemotherapy is usually given for recurrent disease.
If chemotherapy without radiation therapy was used first, and the cancer comes back only in the lymph nodes, radiation to the lymph nodes can be done, with or without more chemo. Chemo with different drugs may be another option.
Radiation usually cannot be repeated in the same area. If, for example, Hodgkin lymphoma in the chest was treated with radiation and it comes back in the chest, it usually can’t be treated with more radiation to the chest. This holds true no matter how long ago the radiation was first given.
If the lymphoma returns after many years, using the same or different chemo drugs (possibly along with radiation) might still cure it. On the other hand, Hodgkin lymphoma that recurs soon after treatment may need more intensive treatment. For example, if the Hodgkin lymphoma has returned within a few months of the original treatment, high-dose chemo (and possibly radiation) followed by an autologous stem cell transplant may be recommended.
If the Hodgkin lymphoma still remains after an autologous transplant, an allogeneic stem cell transplant may be an option. Another option, either instead of or after a stem cell transplant, may be treatment with an immunotherapy drug, such as brentuximab vedotin (Adcetris), nivolumab (Opdivo), or pembrolizumab (Keytruda).
Lastly, most experts agree that treatment in a clinical trial should be considered for Hodgkin lymphoma that is resistant to treatment or comes back (relapses) after treatment.
Clinical Trials
A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
A clinical trial may be an option when it comes to finding the right treatment for your child’s cancer. Your child may have access to new or improved therapies under study and not yet on the market. Discuss with your child’s doctor the possibility of taking part in a clinical trial, where treatment is administered in a safe, closely monitored environment.
Advances in treating childhood Hodgkin lymphoma, which have improved the cure rate and quality of life for survivors, are due, in large part, to the research of pediatric cooperative groups. The focus of ongoing research and clinical trials is to
- Further improve the cure rate, especially for children with advanced Hodgkin’s lymphoma
- Minimize the risk of long-term and late effects associated with treatment (for example, infertility, impaired cardiac function and secondary cancers).
Survivorship and Special Healthcare Needs
After treatment, most children can expect to have full and productive lives. Many survivors return to school, attend college, enter the workforce, marry and become parents.
You may want to consider a survivorship program for your child that focuses on life after cancer. Many comprehensive cancer centers around the country offer these programs.
Follow-Up Care
Your child should visit his or her pediatrician or doctor at least once a year for a complete physical exam and any additional needed tests. Your child’s oncologist should also regularly examine your child.
Regular doctor visits are encouraged to:
- Enable doctors to assess the full effect of therapy
- Detect and treat disease recurrence
- Identify and manage long-term and late effects of treatment
Your pediatrician should recommend a schedule for having your child’s learning skills assessed. If your child appears to be experiencing learning disabilities, special education methods can help.
Coordination between your child’s pediatrician and oncologist is important for the best care possible. Some treatment centers offer comprehensive follow-up care clinics for childhood cancer survivors.
Long-Term and Late Effects of Treatment
Some side effects of cancer treatment, such as fatigue, can linger for months or years after therapy. Some medical conditions like heart disease and other cancers may not appear until years after treatment ends. Long-term and late effects can affect your child’s physical, mental and cognitive (brain function) health.
Most childhood survivors of lymphoma don’t develop significant long-term or late effects of treatment. However, for some patients the effects can be severe.
Long-Term and Late Effects of Chemotherapy
Children treated for lymphoma may be at increased risk for:
- Fatigue
- Growth delays
- Thyroid dysfunction
- Hearing loss
- A secondary cancer
Some long-term and late effects become evident with maturation (puberty), growth and the normal aging process. Early intervention and healthy lifestyle practices (not smoking, good nutrition, exercise, regular screenings and follow-up) may have a positive effect on the occurrence and/or severity of long-term and late effects.
Long-Term and Late Effects of Radiation Therapy
Girls (as well as women under age 30) who had radiation to the breast area are at risk for developing breast cancer 15 to 20 years after treatment. Male survivors of childhood cancer are at risk for developing secondary cancers, but they don’t have as high a risk for developing breast cancer as female childhood cancer survivors do.
Girls who had radiation therapy in the chest (mediastinal) area should:
- Perform monthly breast self-examinations
- Have yearly breast examinations by a healthcare professional
- Have early baseline mammograms within 8 to 10 years after therapy or by age 40, whichever occurs earlier.
- Have breast MRIs in addition to mammography for women who received irradiation of the chest when they were between 10 and 30 years of age.
Both girls and boys who’ve undergone mediastinal radiation therapy should have baseline testing for heart function. This should be followed by testing every three to five years after treatment or more regularly if any abnormalities are found.
Returning to School
Learning disabilities can begin during treatment or appear months or years after treatment. Educate family members, friends, school personnel and healthcare providers about your child’s possible long-term and late effects of treatment. Talk with teachers about your child’s needs before he or she returns to school. Work with your child’s teachers and medical providers to develop a program tailored to his or her needs that features baseline testing, special accommodations and long-term planning.
Hodgkin’s lymphoma survival rates
The numbers below come from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program based on how far the cancer has spread. The SEER database, however, does not group cancers by the Lugano classification (stage 1, stage 2, stage 3, etc.). Instead, it groups cancers into localized, regional, and distant stages 20:
- Localized: The cancer is limited to one lymph node area, one lymphoid organ, or one organ outside the lymph system.
- Regional: The cancer reaches from one lymph node area to a nearby organ, is found in two or more lymph node areas on the same side of the diaphragm, or is considered bulky disease.
- Distant: The cancer has spread to distant parts of the body, such as the lungs, liver, or bone marrow, or to lymph node areas above and below the diaphragm.
Table 7. 5-year relative survival rates for Hodgkin lymphoma
| Surveillance, Epidemiology, and End Results (SEER) Stage | 5-Year Relative Survival Rate |
|---|---|
| Localized | 92% |
| Regional | 94% |
| Distant | 82% |
| All SEER stages combined | 88% |
Footnote: A relative survival rate compares people with the same type and stage of Hodgkin’s lymphoma to people in the overall population. For example, if the 5-year survival rate for a specific stage of Hodgkin lymphoma is 92%, it means that people who have that cancer are, on average, about 92% as likely as people who don’t have that cancer to live 5 years after being diagnosed.
- These numbers are based on people diagnosed with Hodgkin lymphoma between 2011 and 2017.
- These numbers apply only to the stage of the cancer when it is first diagnosed. They do not apply later on if the cancer grows, spreads, or comes back after treatment.
- These numbers don’t take everything into account. Survival rates are grouped based on how far the cancer has spread, but your age, overall health, how well the cancer responds to treatment, and other prognostic factors (described below) can also affect your outlook.
- People now being diagnosed with Hodgkin lymphoma may have a better outlook than these numbers show. Treatments improve over time, and these numbers are based on people who were diagnosed and treated at least five years earlier.
Hodgkin’s lymphoma prognosis
Hodgkin’s lymphoma prognosis depends on several prognostic factors, including disease stage. Hodgkin’s lymphoma stage is currently only one factor in the prognostic indices used for pretreatment risk stratification and assessment. The 5-year overall survival in stage 1 or 2a is approximately 90%; on the other hand, stage 4 disease has a 5-year overall survival of approximately 60% 1.
Along with the stage of the Hodgkin lymphoma, other factors can affect a person’s prognosis (outlook). For example, having some factors means the lymphoma is likely to be more serious 21:
- Having B symptoms or bulky disease
- Being older than 45
- Being male
- Having a high white blood cell count (above 15,000)
- Having a low red blood cell count (hemoglobin level below 10.5)
- Having a low blood lymphocyte count (below 600)
- Having a low blood albumin level (below 4)
- Having a high erythrocyte sedimentation rate, or ESR (over 30 in someone with B symptoms, or over 50 for someone without B symptoms)
Some of these factors are used to help divide stage 1 or 2 Hodgkin lymphoma into favorable and unfavorable groups, which can affect how intense the treatment needs to be (see Hodgkin’s lymphoma staging above).
Hodgkin’s Lymphoma Survival by Stage
Cancer stage at diagnosis, which refers to extent of a cancer in the body, determines treatment options and has a strong influence on the length of survival. In general, if the cancer is found only in the part of the body where it started it is localized (sometimes referred to as stage 1). If it has spread to a different part of the body, the stage is regional or distant. For Hodgkin lymphoma, 15.6% are diagnosed at the local stage. The 5-year survival for localized Hodgkin lymphoma is 92.4%.
Remember, these survival rates are only estimates – they can’t predict what will happen to any individual person. We understand that these statistics can be confusing and may lead you to have more questions. Talk to your doctor to better understand your specific situation.
- Stage 1 Hodgkin lymphoma the 5-year survival rate is about 92.4%.·
- Stage 2 Hodgkin lymphoma the 5-year survival rate is about 95%.
- Stage 3 Hodgkin lymphoma the 5-year survival rate is about 86.4%.
- Stage 4 Hodgkin lymphoma has a 5-year survival rate of about 79.8%.
Based on data from SEER (Surveillance, Epidemiology, and End Results Program at the National Cancer Institute) 2012–2018, percent surviving 5 Years is 89.1% 4.
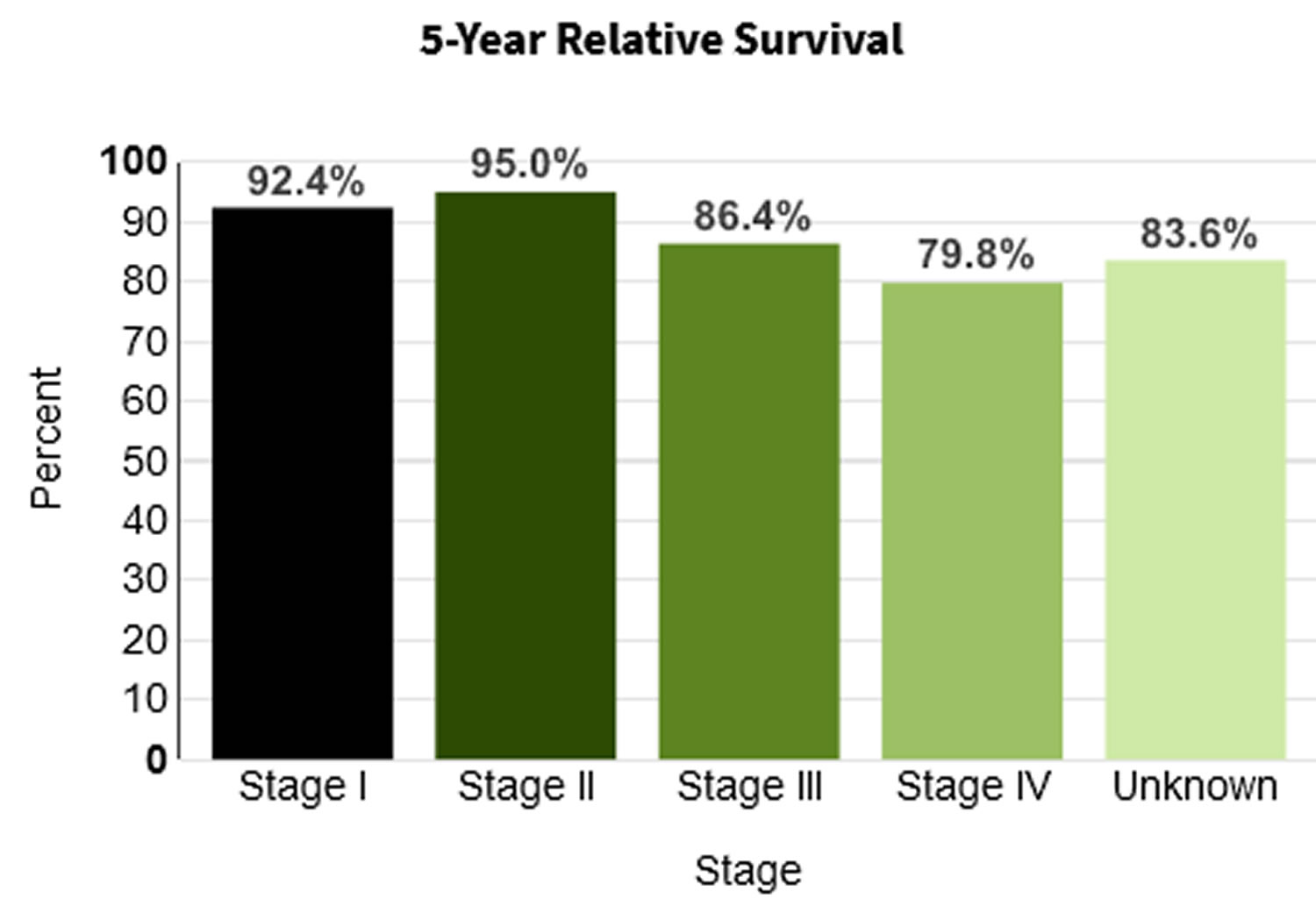
- Kaseb H, Babiker HM. Hodgkin Lymphoma. [Updated 2022 Mar 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499969
- What Is Hodgkin Lymphoma? https://www.cancer.org/cancer/hodgkin-lymphoma/about/what-is-hodgkin-disease.html
- American Cancer Society: Cancer Facts and Figures 2022. American Cancer Society, 2022. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2022/2022-cancer-facts-and-figures.pdf
- Hodgkin Lymphoma — Cancer Stat Facts. https://seer.cancer.gov/statfacts/html/hodg.html
- Brenner H, Gondos A, Pulte D. Ongoing improvement in long-term survival of patients with Hodgkin disease at all ages and recent catch-up of older patients. Blood. 2008 Mar 15;111(6):2977-83. doi: 10.1182/blood-2007-10-115493
- Hodgkin Lymphoma Subtypes. http://www.lls.org/lymphoma/hodgkin-lymphoma/diagnosis/hodgkin-lymphoma-subtypes
- PDQ Pediatric Treatment Editorial Board. Childhood Hodgkin Lymphoma Treatment (PDQ®): Health Professional Version. 2022 Apr 8. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65726
- Lyapichev KA, You MJ. Unusual presentation of classic Hodgkin lymphoma. Blood. 2019 Jan 31;133(5):502. doi: 10.1182/blood-2018-10-878058
- Milgrom, S. A., Elhalawani, H., Lee, J., Wang, Q., Mohamed, A., Dabaja, B. S., Pinnix, C. C., Gunther, J. R., Court, L., Rao, A., Fuller, C. D., Akhtari, M., Aristophanous, M., Mawlawi, O., Chuang, H. H., Sulman, E. P., Lee, H. J., Hagemeister, F. B., Oki, Y., Fanale, M., … Smith, G. L. (2019). A PET Radiomics Model to Predict Refractory Mediastinal Hodgkin Lymphoma. Scientific reports, 9(1), 1322. https://doi.org/10.1038/s41598-018-37197-z
- Hodgkin Lymphoma Staging. http://www.lls.org/lymphoma/hodgkin-lymphoma/diagnosis/hodgkin-lymphoma-staging
- Engert A, Haverkamp H, Kobe C, Markova J, Renner C, Ho A, Zijlstra J, Král Z, Fuchs M, Hallek M, Kanz L, Döhner H, Dörken B, Engel N, Topp M, Klutmann S, Amthauer H, Bockisch A, Kluge R, Kratochwil C, Schober O, Greil R, Andreesen R, Kneba M, Pfreundschuh M, Stein H, Eich HT, Müller RP, Dietlein M, Borchmann P, Diehl V; German Hodgkin Study Group; Swiss Group for Clinical Cancer Research; Arbeitsgemeinschaft Medikamentöse Tumortherapie. Reduced-intensity chemotherapy and PET-guided radiotherapy in patients with advanced stage Hodgkin’s lymphoma (HD15 trial): a randomised, open-label, phase 3 non-inferiority trial. Lancet. 2012 May 12;379(9828):1791-9. https://doi.org/10.1016/S0140-6736(11)61940-5
- Evens AM, Hong F. How can outcomes be improved for older patients with Hodgkin lymphoma? J Clin Oncol. 2013 Apr 20;31(12):1502-5. doi: 10.1200/JCO.2012.47.3058
- Kolstad A, Nome O, Delabie J, Lauritzsen GF, Fossa A, Holte H. Standard CHOP-21 as first line therapy for elderly patients with Hodgkin’s lymphoma. Leuk Lymphoma. 2007 Mar;48(3):570-6. doi: 10.1080/10428190601126610
- Forero-Torres, A., Holkova, B., Goldschmidt, J., Chen, R., Olsen, G., Boccia, R. V., Bordoni, R. E., Friedberg, J. W., Sharman, J. P., Palanca-Wessels, M. C., Wang, Y., & Yasenchak, C. A. (2015). Phase 2 study of frontline brentuximab vedotin monotherapy in Hodgkin lymphoma patients aged 60 years and older. Blood, 126(26), 2798–2804. https://doi.org/10.1182/blood-2015-06-644336
- Friedberg JW, Forero-Torres A, Bordoni RE, Cline VJM, Patel Donnelly D, Flynn PJ, Olsen G, Chen R, Fong A, Wang Y, Yasenchak CA. Frontline brentuximab vedotin in combination with dacarbazine or bendamustine in patients aged ≥60 years with HL. Blood. 2017 Dec 28;130(26):2829-2837. doi: 10.1182/blood-2017-06-787200
- Evens AM, Advani RH, Helenowski IB, Fanale M, Smith SM, Jovanovic BD, Bociek GR, Klein AK, Winter JN, Gordon LI, Hamlin PA. Multicenter Phase II Study of Sequential Brentuximab Vedotin and Doxorubicin, Vinblastine, and Dacarbazine Chemotherapy for Older Patients With Untreated Classical Hodgkin Lymphoma. J Clin Oncol. 2018 Oct 20;36(30):3015-3022. doi: 10.1200/JCO.2018.79.0139
- Böll B, Goergen H, Behringer K, Bröckelmann PJ, Hitz F, Kerkhoff A, Greil R, von Tresckow B, Eichenauer DA, Bürkle C, Borchmann S, Fuchs M, Diehl V, Engert A, Borchmann P. Bleomycin in older early-stage favorable Hodgkin lymphoma patients: analysis of the German Hodgkin Study Group (GHSG) HD10 and HD13 trials. Blood. 2016 May 5;127(18):2189-92. doi: 10.1182/blood-2015-11-681064
- PDQ Adult Treatment Editorial Board. Adult Hodgkin Lymphoma Treatment (PDQ®): Health Professional Version. 2022 May 26. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK66038
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390(10091):298–310
- Surveillance, Epidemiology, and End Results Program. https://seer.cancer.gov/
- Survival Rates for Hodgkin Lymphoma. https://www.cancer.org/cancer/hodgkin-lymphoma/detection-diagnosis-staging/survival-rates.html





{kind=link}