What is hypoplastic left heart syndrome
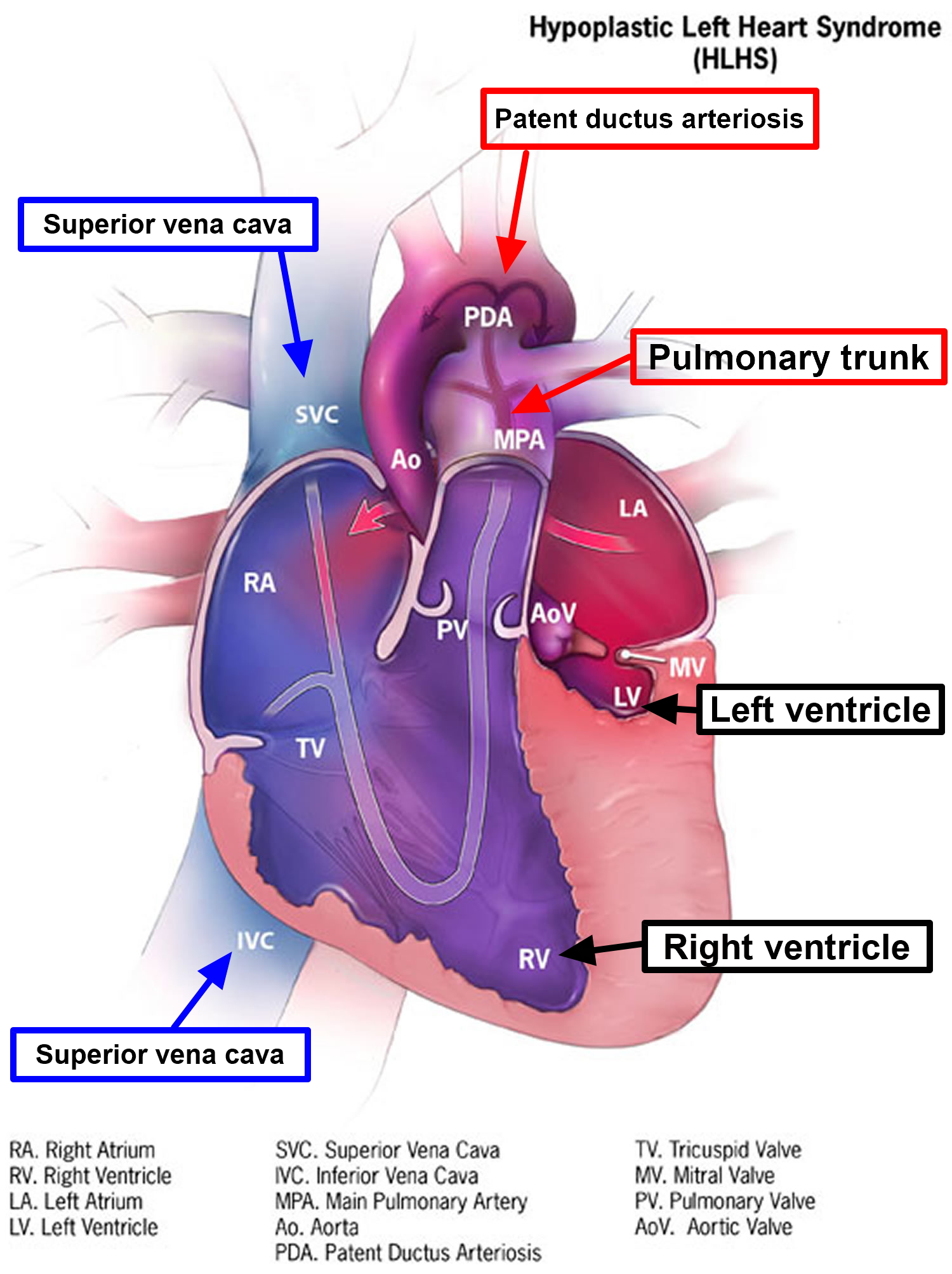
Hypoplastic left heart syndrome is a group of closely related complex and rare heart defects present at birth (congenital). In hypoplastic left heart syndrome, the left side of the heart is critically underdeveloped and is characterized by the underdevelopment (hypoplasia) of the chambers on the left side of the heart (i.e., left atrium and ventricle). In addition, the mitral valve, which connects these chambers (left atrium to left ventricle) to each other, is usually abnormally narrow (stenosis) or closed (atresia) and the aortic valve, which connects the heart to the major vessels that lead from the lungs (ascending aorta), may also be narrow or closed. Infants with hypoplastic left heart syndrome also have an abnormally narrow ascending aorta. If your baby is born with hypoplastic left heart syndrome, the left side of the heart can’t effectively pump blood to his/her body, so the right side of the heart must pump blood to the lungs and to the rest of the body.
Hypoplastic left heart syndrome is a rare disorder that affects males (67 percent) more often than females. The Centers for Disease Control and Prevention (CDC) estimates that each year about 960 babies in the United States are born with hypoplastic left heart syndrome 1. In other words, about 1 out of every 4,344 babies born in the United States each year is born with hypoplastic left heart syndrome. Hypoplastic left heart syndrome accounts for 7-9 percent of all congenital heart defects.
As with most congenital heart defects, there is no known cause. About 10% of babies with hypoplastic left heart syndrome also have other birth defects.
The problem develops before birth when the left ventricle and other structures do not grow properly, including the:
- Aorta: the blood vessel that carries oxygen-rich blood from the left ventricle to the entire body
- Entrance and exit of the ventricle
- Mitral and aortic valves
This causes the left ventricle and aorta to be poorly developed, or hypoplastic. In most cases, the left ventricle and aorta are much smaller than normal.
In babies with this condition, the left side of the heart is unable to send enough blood to the body. As a result, the right side of the heart must maintain the circulation for both the lungs and the body. The right ventricle can support the circulation to both the lungs and the body for a while, but this extra workload eventually causes the right side of the heart to fail.
The symptoms of hypoplastic left heart syndrome are present at birth (congenital). The symptoms of hypoplastic left heart syndrome are directly related to the underdevelopment of the left side of the heart and associated structures. In all cases, infants have impaired blood flow from the lungs, through the heart, and on to other parts of the body (systemic circulation). Symptoms may include difficulty breathing (dyspnea), a high-pitched noise while inhaling (rales), and grayish-blue discoloration of the skin (cyanosis) during the first 48 hours of life, which occurs because of low levels of circulating oxygen in the blood. Impaired blood flow characteristic of hypoplastic left heart syndrome results in fluid buildup in the heart, lung and various body tissues (congestive heart failure).
Infants with hypoplastic left heart syndrome may accumulate excessive acids in their blood and other body tissues (metabolic acidosis). Symptoms may include poor feeding habits, frequent vomiting, lethargy, and/or shock. When shock occurs, the symptoms may include abnormally high pulse (tachycardia) and respiration rate, respiratory distress, abnormally enlarged liver (hepatomegaly), cool moist skin, abnormally low blood pressure, and/or paleness. In most cases, if left untreated, life-threatening complications usually occur.
The progression and severity of hypoplastic left heart syndrome depend upon a structure called the ductus arteriosus, which is present in all newborns. The ductus arteriosus is a passageway that allows blood to travel from the right ventricle to the aorta and then throughout the body, bypassing the left side of the heart and the lungs. However, the ductus arteriosus closes shortly after birth forcing blood to travel through the malformed left ventricle resulting in impaired blood flow throughout the body.
The only possibility of survival is a connection between the right and the left side of the heart, or between the arteries and pulmonary arteries (the blood vessels that carry blood to the lungs). Babies are normally born with 2 of these connections:
- Foramen ovale (a hole between the right and left atrium)
- Ductus arteriosus (a small blood vessel that connects the aorta to the pulmonary artery)
Both of these connections normally close on their own a few days after birth.
In babies with hypoplastic left heart syndrome, blood leaving the right side of the heart through the pulmonary artery travels through the ductus arteriosus to the aorta. This is the only way for blood to get to the body. If the ductus arteriosus is allowed to close in a baby with hypoplastic left heart syndrome, the baby may quickly die because no blood will be pumped to the body. Babies with known hypoplastic left heart syndrome are usually started on a medicine to keep the ductus arteriosus open.
Because there is little or no flow out of the left heart, blood returning to the heart from the lungs needs to pass through the foramen ovale or an atrial septal defect (a hole connecting the collecting chambers on the left and right sides of the heart) back to the right side of the heart. If there is no foramen ovale, or if it is too small, the baby could die. Babies with this problem have the hole between their atria opened, either with surgery or using a thin, flexible tube (heart catheterization).
Medication to prevent closure of the connection (ductus arteriosus) between the right and left sides, followed by either surgery or a heart transplant, is necessary to treat hypoplastic left heart syndrome. With advances in care, the outlook for babies born with hypoplastic left heart syndrome is better now than in the past.
It’s more likely that your baby would be diagnosed with hypoplastic left heart syndrome either before birth or soon after. However, you should seek medical help if you notice that your baby has the following symptoms:
- Grayish-blue skin color
- Rapid, difficult breathing
- Poor feeding
- Cold hands and feet
- Being unusually drowsy or inactive
If your baby has any of the following signs of shock, call your local emergency number right away:
- Cool, clammy skin that may be pale or gray
- A weak and rapid pulse
- Abnormal breathing that may be either slow and shallow or very rapid
- Dilated pupils
- Lackluster eyes that seem to stare
Human heart
The normal heart has four chambers. The two upper chambers, known as atria, are separated from each other by a fibrous partition known as the atrial septum. The two lower chambers are known as ventricles and are separated from each other by the ventricular septum. Valves connect the atria (left and right) to their respective ventricles. The valves allow for blood to be pumped through the chambers. The heart uses its left and right sides for different tasks. The right side blood travels from the right ventricle through the pulmonary artery to the lungs where it receives oxygen. In the lungs, oxygen enriches the blood, which then circulates to the heart’s left side through pulmonary veins and enters the left ventricle. The left side of the heart (left ventricle) pumps blood into a large vessel called the aorta, which circulates the oxygen-rich blood to the rest of the body.
In a baby without a congenital heart defect, the right side of the heart pumps oxygen-poor blood from the heart to the lungs. The left side of the heart pumps oxygen-rich blood to the rest of the body. When a baby is growing in a mother’s womb during pregnancy, there are two small openings between the left and right sides of the heart: the patent ductus arteriosus and the patent foramen ovale. Normally, these openings will close a few days after birth.
What happens in hypoplastic left heart syndrome
In hypoplastic left heart syndrome, the left side of the heart can’t properly supply blood to the body because the lower left chamber (left ventricle) is too small or in some cases it may not even exist. In addition, the valves on the left side of the heart (aortic valve and mitral valve) don’t work properly, and the main artery leaving the heart (aorta) is smaller than normal.
For the first several days of life, the right side of the heart can pump blood both to the lungs and to the rest of the body through a blood vessel that connects the pulmonary artery directly to the aorta (patent ductus arteriosus). The oxygen-rich blood returns to the right side of the heart through a natural opening (foramen ovale) between the right chambers of the heart (atria). When the foramen ovale and the ductus arteriosus are open, they are referred to as being “patent.”
If the ductus arteriosus and the foramen ovale close — which they normally do after the first day or two of life — the right side of the heart has no way to pump blood out to the body. Keeping these connections open is necessary for the baby’s survival in the first few days of life in babies with hypoplastic left heart syndrome. This will keep blood flowing to the body until the first surgical procedure is performed.
Figure 1. The anatomy of the heart chambers

Figure 2. Heart back view
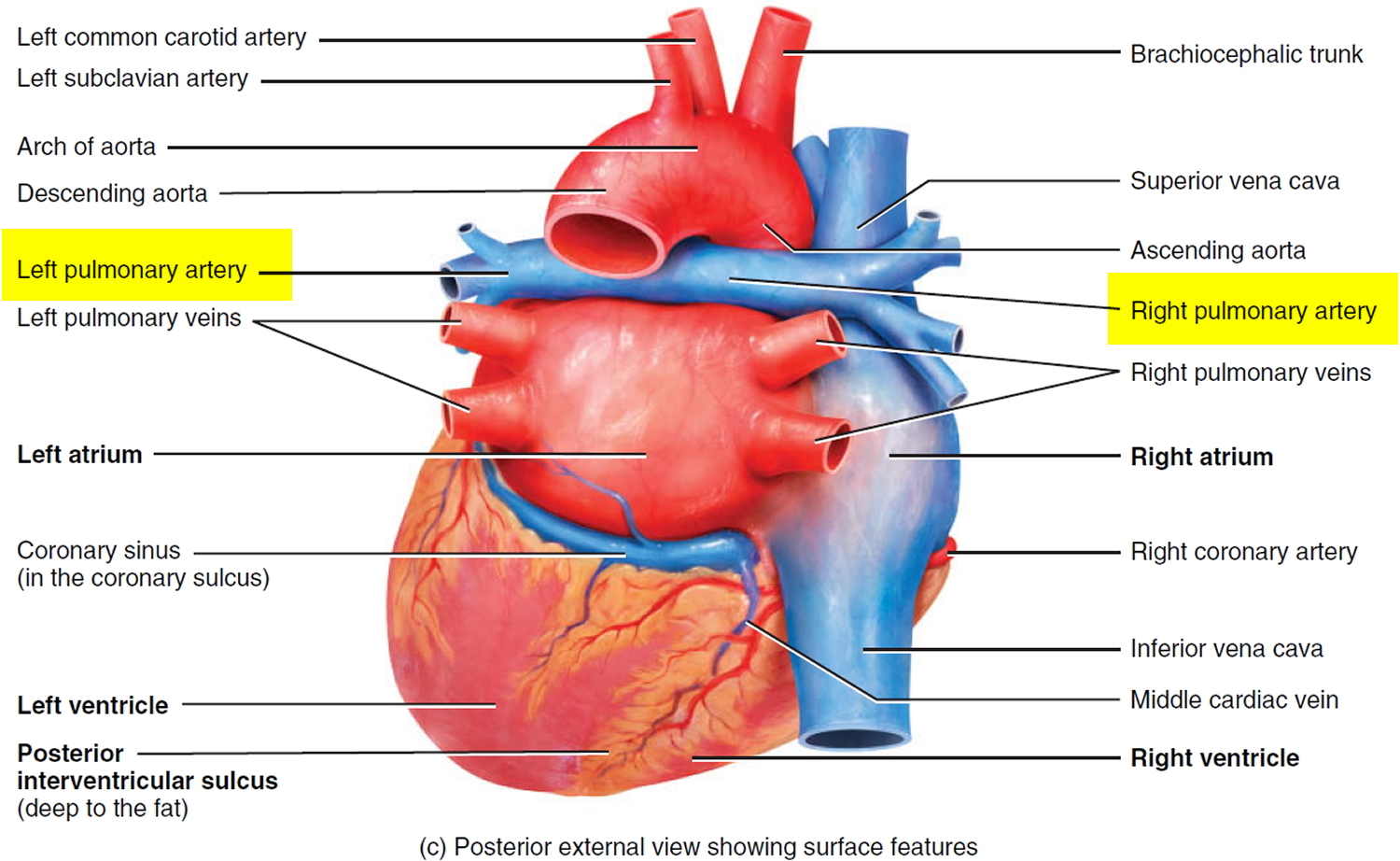
Figure 3. Normal heart blood flow

Figure 4. Heart valves function
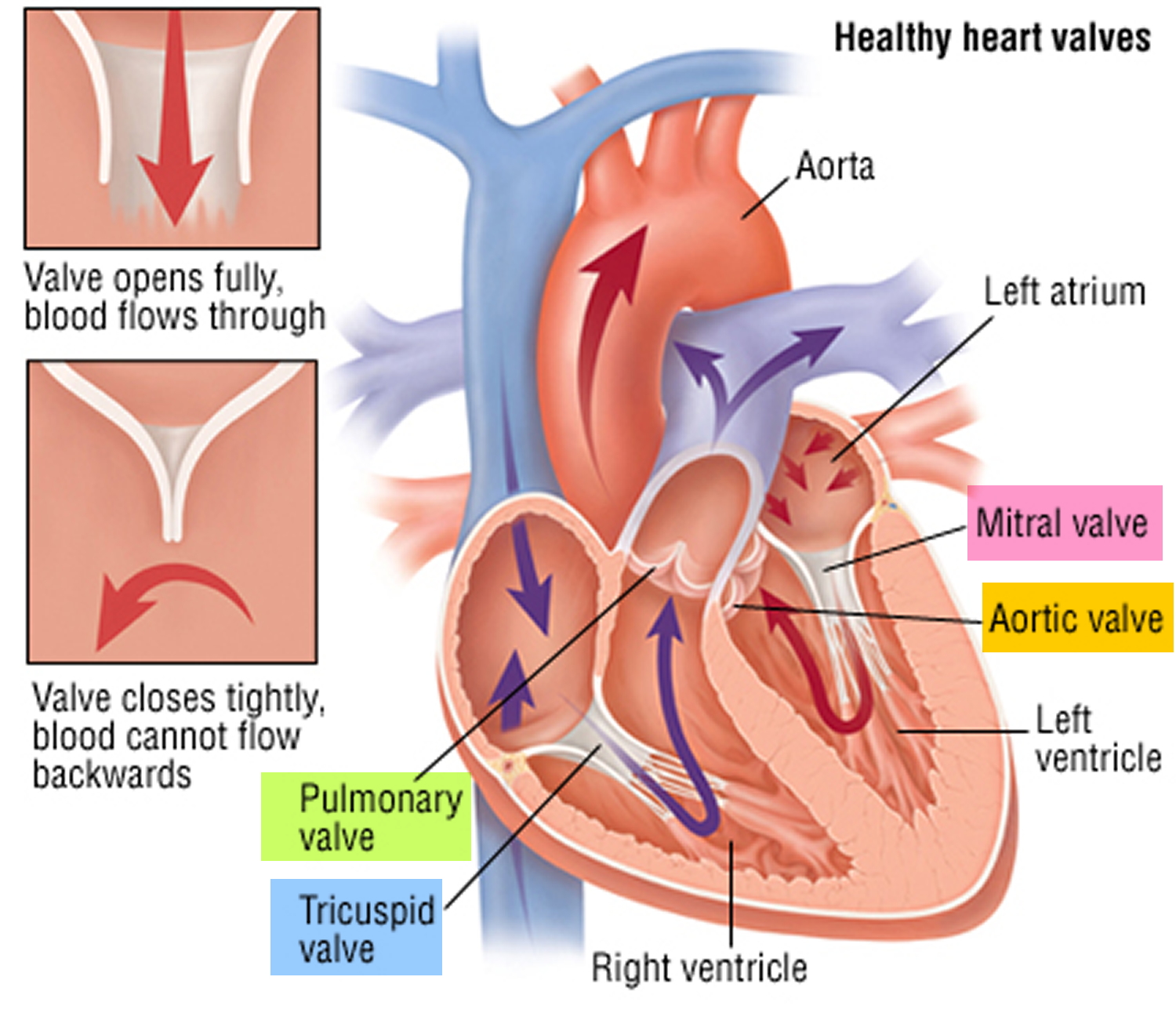
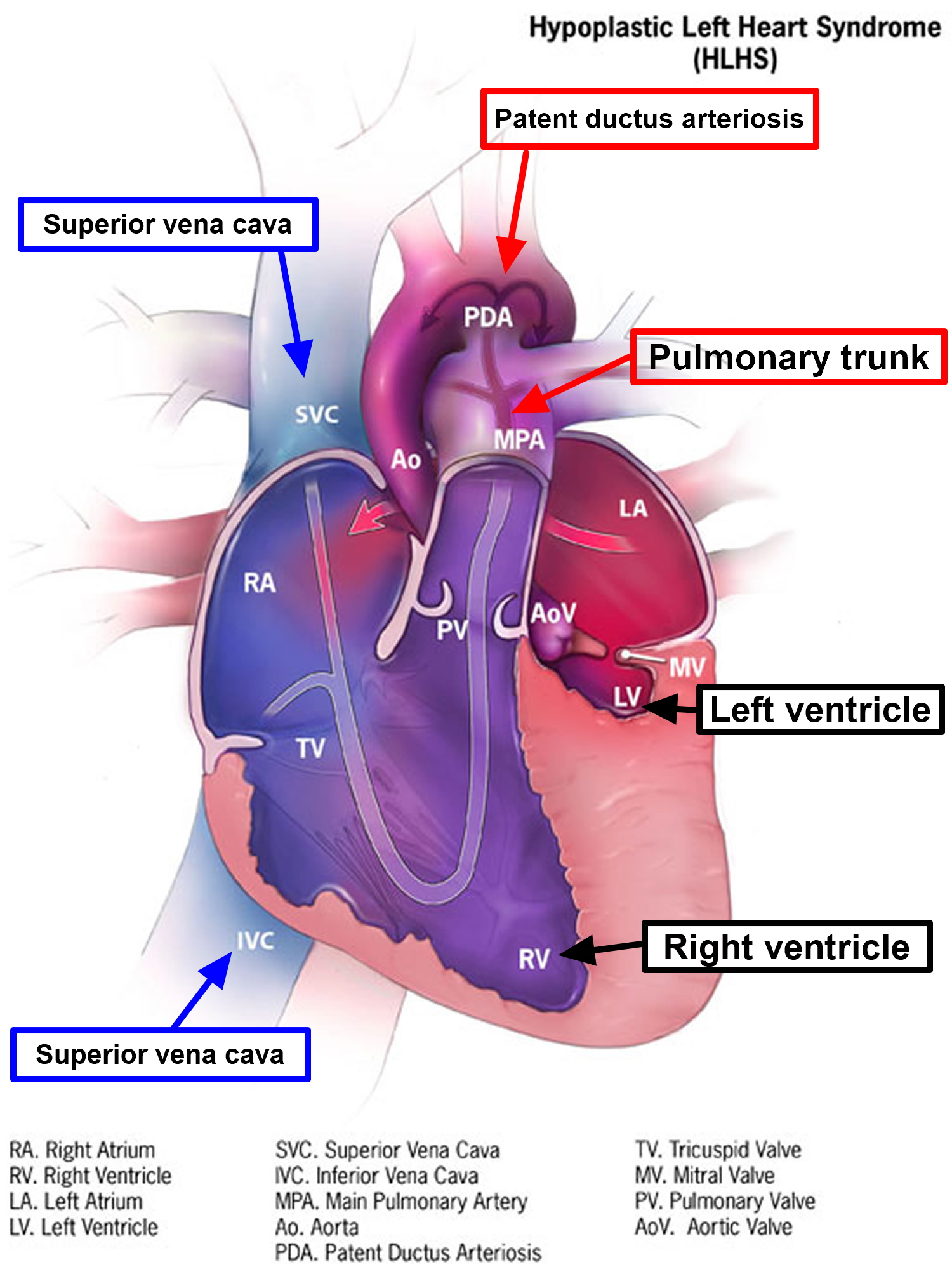
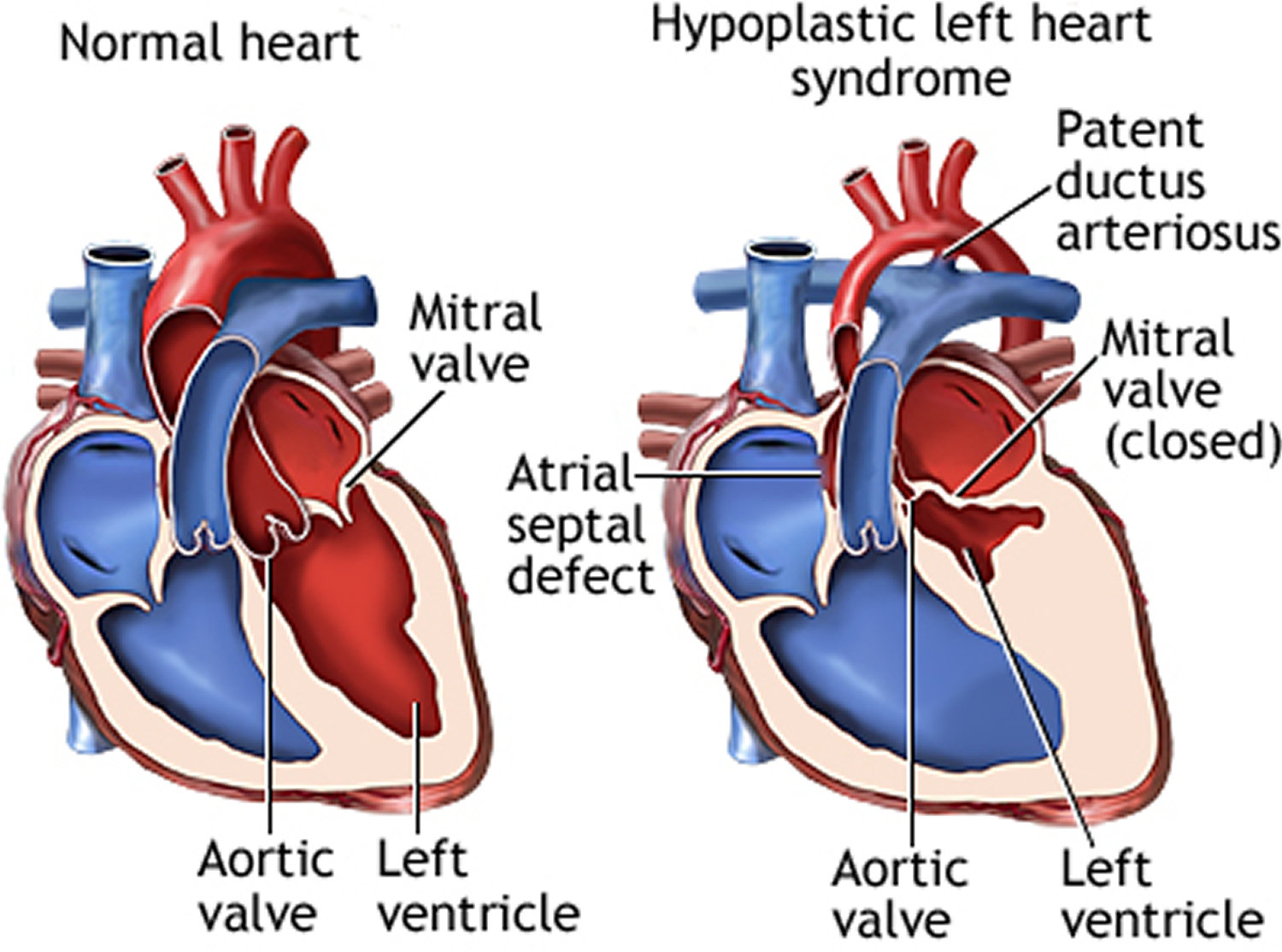
Figure 5. Hypoplastic left heart syndrome
Hypoplastic left heart syndrome possible complications
Complications include:
- Blockage of the artificial shunt
- Chronic diarrhea (from a disease called protein-losing enteropathy)
- Fluid in the abdomen (ascites) and in the lungs (pleural effusion)
- Heart failure
- Irregular, fast heart rhythms (arrhythmias)
- Strokes and other nervous system complications
- Sudden death
Hypoplastic left heart syndrome prognosis
If left untreated, hypoplastic left heart syndrome is fatal. Survival rates for the staged repair continue to rise as surgery techniques and care after surgery improve. Survival after the first stage hypoplastic left heart syndrome surgery is more than 75%.
The child’s outcome after surgery depends on the size and function of the right ventricle.
Children with hypoplastic left heart syndrome are always limited to some extent in their physical activities. Physical endurance may get worse in teenage years or young adult life, but specific restrictions on exercise are usually not necessary. Your child’s cardiologist will tell you if there are any specific forms of exercise or activities they should avoid.
Hypoplastic left heart syndrome survival rate
With treatment, many babies survive, although most will have complications later in life. Some of the complications may include:
- Tiring easily when participating in sports or other exercise
- Heart rhythm abnormalities (arrhythmias)
- Fluid buildup in the lungs, abdomen, legs and feet (edema)
- Formation of blood clots that may lead to a pulmonary embolism or stroke
- Developmental problems related to the brain and nervous system
- Need for additional heart surgery or transplantation
Although every circumstance is different, remember that many children with congenital heart defects grow up to lead healthy lives.
Hypoplastic left heart syndrome life expectancy
Without surgery, hypoplastic left heart syndrome is fatal, usually within the first few weeks of life.
Hypoplastic left heart syndrome is a complex condition, and some children will not survive all three stages of surgery. Although surgery can give a better quality of life, it is not possible to correct the heart abnormality and it’s uncertain how long children with this condition will live for. The longest survivors at present are in their late 20s. Heart transplantation may be an option for some patients, although this is rarely considered before adulthood.
Hypoplastic left heart syndrome causes
The exact cause of most cases of hypoplastic left heart syndrome is not known. It occurs for no apparent reason (sporadically) in the majority of cases. Research suggests that the interaction of many genes and other environmental factors (multifactorial inheritance) may be responsible for hypoplastic left heart syndrome. In some cases, autosomal dominant and recessive inheritance has been suggested. If your family has one child with hypoplastic left heart syndrome, the risk of having another with a similar condition is increased.
If you have one child with a congenital heart condition, there is about a 1 in 40 chance of having another child with congenital heart disease 2. However, this risk may be higher (or lower) depending on the type of congenital heart disease your child has. Because your risk of having another child with congenital heart disease is higher than it is for other people, you may be offered a special scan at an early stage in future pregnancies, to look at the baby’s heart.
Hypoplastic left heart syndrome affects a number of structures on the left side of the heart that do not fully develop, for example:
- The left ventricle is underdeveloped and too small.
- The mitral valves is not formed or is very small.
- The aortic valve is not formed or is very small.
- The ascending portion of the aorta is underdeveloped or is too small.
- Often, babies with hypoplastic left heart syndrome also have an atrial septal defect, which is a hole between the left and right upper chambers (atria) of the heart.
In most cases, the malformations associated with hypoplastic left heart syndrome occur as a result of a developmental failure during early fetal (embryonic) growth. The reason that this occurs is not fully understood. Conditions that limit blood flow from the right to left atrium during fetal development may result in underdevelopment of the left heart. Such conditions may include premature closure of the foramen ovale and fetal heart muscle disease (cardiomyopathy).
Risk factors for hypoplastic left heart syndrome
If you already have a child with hypoplastic left heart syndrome, you’re at a higher risk of having another baby with this condition or a similar condition. If you have one child with a congenital heart condition, there is about a 1 in 40 chance of having another child with congenital heart disease 2. However, this risk may be higher (or lower) depending on the type of congenital heart disease your child has. Because your risk of having another child with congenital heart disease is higher than it is for other people, you may be offered a special scan at an early stage in future pregnancies, to look at the baby’s heart.
Beyond family history, there are no clear risk factors for hypoplastic left heart syndrome.
Hypoplastic left heart syndrome prevention
There is no known prevention for hypoplastic left heart syndrome. As with many congenital diseases, the causes of hypoplastic left heart syndrome are uncertain and have not been linked to a mother’s disease or behavior.
However, if you have a family history of heart defects, or if you already have a child with a congenital heart defect, before getting pregnant consider talking with a genetic counselor and a cardiologist experienced in congenital heart defects.
Hypoplastic left heart syndrome symptoms
Babies born with hypoplastic left heart syndrome usually are seriously ill soon after birth. Symptoms may occur in the first few hours of life, although it may take up to a few days to develop symptoms.
Hypoplastic left heart syndrome symptoms include:
- Bluish (cyanosis) or poor skin color
- Cold hands and feet (extremities)
- Lethargy
- Poor pulse
- Poor suckling and feeding
- Cold hands and feet
- Pounding heart
- Rapid, difficult breathing
- Shortness of breath
- Being unusually drowsy or inactive
In healthy newborns, bluish color in the hands and feet is a response to cold (this reaction is called peripheral cyanosis).
A bluish color in the chest or abdomen, lips, and tongue is abnormal (called central cyanosis). It is a sign that there is not enough oxygen in the blood. Central cyanosis often increases with crying.
In a baby with hypoplastic left heart syndrome, if the natural connections between the heart’s left and right sides (foramen ovale and ductus arteriosus) are allowed to close, he or she may go into shock and may die.
Signs of cardiogenic shock include:
- Cool, clammy skin that may be pale or gray
- A weak and rapid pulse
- Abnormal breathing that may be either slow and shallow or very rapid
- Dilated pupils
- Lackluster eyes that seem to stare
A baby who is in shock may be conscious or unconscious. If you suspect your baby is in shock, immediately call your local emergency number for urgent medical assistance.
Hypoplastic left heart syndrome diagnosis
Before birth
It’s possible for a baby to be diagnosed with hypoplastic left heart syndrome while it’s still in the womb. During pregnancy, there are screening tests (also called prenatal tests,) to check for birth defects and other conditions. Hypoplastic left heart syndrome may be diagnosed during pregnancy with an ultrasound exam during the second trimester of pregnancy. Some findings from the ultrasound may make the health care provider suspect a baby may have hypoplastic left heart syndrome. If so, the health care provider can request a fetal echocardiogram, an ultrasound of the baby’s heart, to confirm the diagnosis. This test can show problems with the structure of the heart and how the heart is working with this defect.
If the diagnosis has been made before the baby is born, doctors usually recommend delivery at a hospital with a cardiac surgery center.
After birth
After your baby is born, his or her doctor may suspect a heart defect, such as hypoplastic left heart syndrome, if your baby has grayish-blue skin or has trouble breathing. Your baby’s doctor may also suspect a heart defect if he or she hears a heart murmur — an abnormal whooshing sound caused by turbulent blood flow.
A physical exam may show signs of heart failure:
- Faster than normal heart rate
- Lethargy
- Liver enlargement
- Rapid breathing
Also, the pulse at various locations (wrist, groin, and others) may be very weak. There are often (but not always) abnormal heart sounds when listening to the chest.
Tests may include:
- Cardiac catheterization
- ECG
- Echocardiogram
- X-ray of the chest
Doctors usually use an echocardiogram to diagnose hypoplastic left heart syndrome. This test uses high-pitched sound waves that bounce off your baby’s heart to produce moving images that can be viewed on a video screen. In a baby with hypoplastic left heart syndrome, the echocardiogram reveals a smaller than normal left ventricle and aorta, and it may also show abnormal mitral or aortic valves.
Because this test can track blood flow, it also shows blood moving from the right ventricle into the aorta. In addition, an echocardiogram can identify associated heart defects, such as an atrial septal defect.
Hypoplastic left heart syndrome treatment
Once the diagnosis of hypoplastic left heart is made, the baby will be admitted to the neonatal intensive care unit. A breathing machine (ventilator) may be needed to help the baby breathe. A medicine called prostaglandin E1 is used to keep blood circulating to the body by keeping the ductus arteriosus open.
These measures do not solve the problem. Hypoplastic left heart syndrome always requires surgery.
It’s not possible to correct hypoplastic left heart syndrome with surgery, but there are operations that can help your child to have a better quality of life. Hypoplastic left heart syndrome is treated through several surgical procedures or a heart transplant. Your doctor will discuss with you the treatment options for your child.
Your child will need to have several operations during their lifetime. The first stage of treatment is to keep the duct open by giving your baby an injection of drugs called prostaglandins. These drugs can occasionally interfere with your baby’s natural breathing, and in some rare cases, they may need the support of a ventilator.
Before hypoplastic left heart syndrome surgery
Your baby’s doctor may recommend several options to help manage your baby’s condition before surgery or transplant. They may include:
- Medication. The medication alprostadil (prostaglandin E1) helps dilate the blood vessels and keeps the ductus arteriosus open.
- Breathing assistance. If your baby has trouble breathing, he or she may need help from a breathing machine (ventilator), which ensures adequate oxygen delivery.
- Intravenous fluids. Your baby will receive fluids through a tube inserted into a vein.
- Feeding tube. If your baby has trouble or gets tired feeding, he or she may be fed through a feeding tube.
- Atrial septostomy. This procedure creates or enlarges the opening between the heart’s upper chambers (atria) to allow more blood flow from the right atrium to the left atrium if the foramen ovale closes. If your baby already has an atrial septal defect, an atrial septostomy may not be necessary.
Often, the initial surgery is carried out within a few days of birth. The first operation for most babies with hypoplastic left heart syndrome is called the Norwood procedure. However, some babies who are very small or very ill may not be suitable for this and may be offered the hybrid procedure.
Hybrid procedure
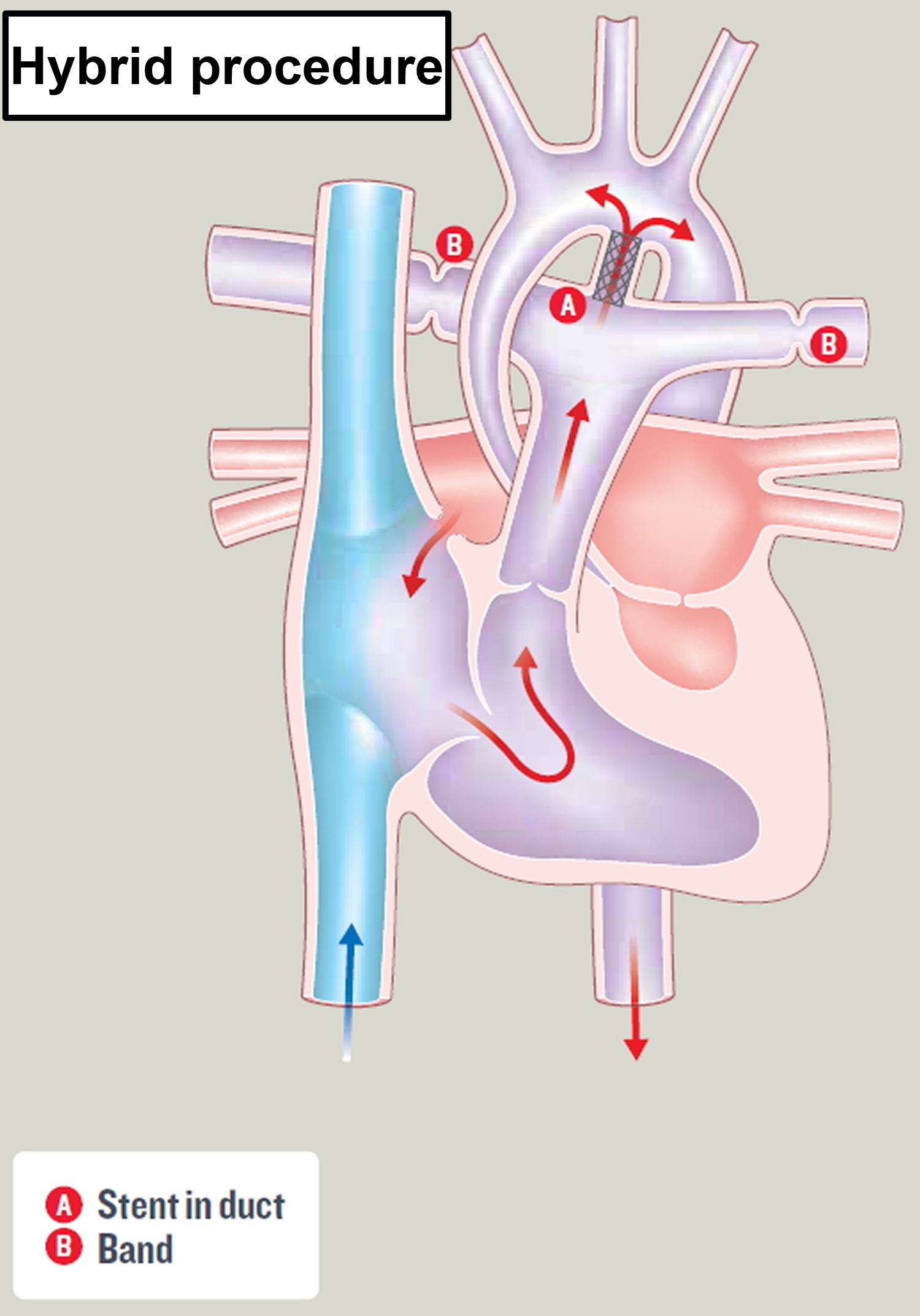
This is a technique that involves a combination of surgery and catheter treatment. The hybrid procedure helps to improve your baby’s circulation while allowing them to grow before they have more major surgery. It also helps to protect the lungs by reducing the amount of blood being delivered to them and it keeps the duct open.
Your baby will be given a general anesthetic. The surgeon will place an expandable metal mesh tube – called a stent – inside the duct, to stop it from closing. This means that blood can flow into the aorta to be delivered to the rest of the body.
Small bands are also placed around the right and left pulmonary arteries, to reduce the amount of blood flowing to the lungs. This helps to protect the lungs. After the surgery, your baby will have a scar down the center of their chest.
This is a relatively new procedure and the technique is still being evaluated. Your child’s cardiologist will discuss this with you in more detail.
Figure 6. Hybrid procedure
Hypoplastic left heart syndrome surgery
Your child will likely need several surgical procedures to treat hypoplastic left heart syndrome. Surgeons perform these procedures in three stages. These procedures are designed to create normal blood flow in and out of the heart, allowing the body to receive the oxygen-rich blood it needs.
Norwood procedure
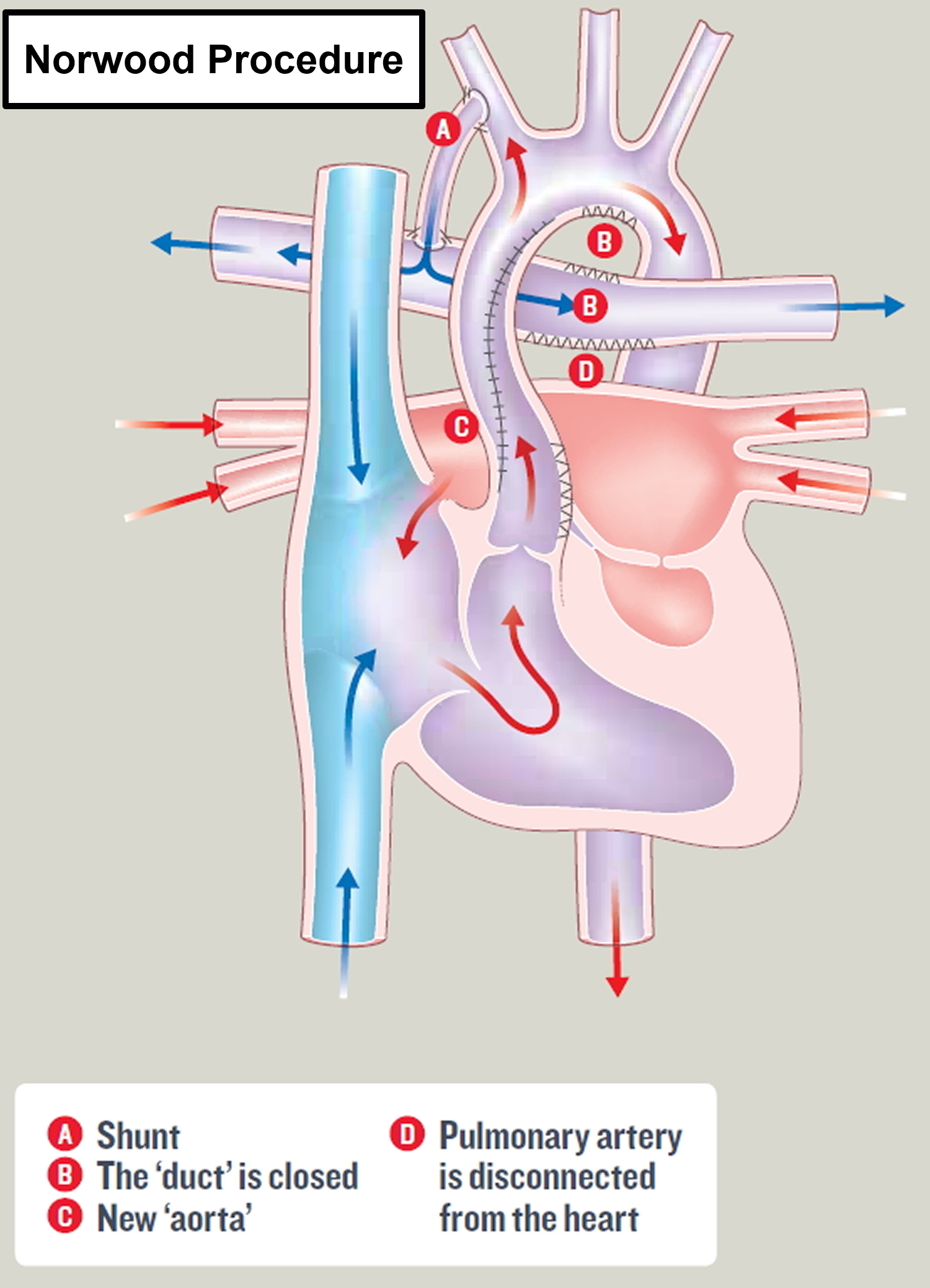
The first surgery, called the Norwood operation, occurs within the baby’s first few days of life. The Norwood procedure consists of building a new aorta by:
- Using the pulmonary valve and artery
- Connecting the hypoplastic old aorta and coronary arteries to the new aorta
- Removing the wall between the atria (atrial septum)
- Making an artificial connection from either the right ventricle or a body-wide artery to the pulmonary artery to maintain blood flow to the lungs (called a shunt)
This surgery is usually performed within the first two weeks of your child’s life. Several forms of this procedure may be performed.
Surgeons reconstruct the aorta and connect it directly to the heart’s lower right chamber (right ventricle). Surgeons insert a tube (shunt) that connects the aorta to the arteries leading to the lungs (pulmonary arteries), or they place a shunt that connects the right ventricle to the pulmonary arteries. This procedure allows the right ventricle to effectively pump blood to both the lungs and the body.
In some cases, doctors may perform a hybrid procedure. Surgeons implant a stent in the ductus arteriosus to maintain the opening between the pulmonary artery and aorta, place bands around the pulmonary arteries to reduce blood flow to the lungs, and create an opening between the atria of the heart.
After this procedure, your baby’s skin will still have a blue cast because oxygen-rich blood and oxygen-poor blood continue to mix within the heart. Once your baby successfully passes through this stage of treatment, the odds of survival may increase, but he or she may still be at risk of death due to complications.
After the surgery, your baby will have a vertical scar in the centre of the chest, along the breast bone. Most babies are allowed home within a few weeks. Your baby will need to take daily medicines and be closely followed by a pediatric cardiologist, who will determine when the second stage of surgery should be done.
What are the risks of the Norwood procedure?
Most babies survive this first stage of surgery, but there is a small risk that your baby may have brain damage or internal bleeding. Kidney damage can also occur, but this usually recovers with treatment. Your pediatric cardiologist or cardiac surgeon will discuss in details your child’s individual risk with you before surgery.
Figure 7. The Norwood Procedure
Glenn shunt
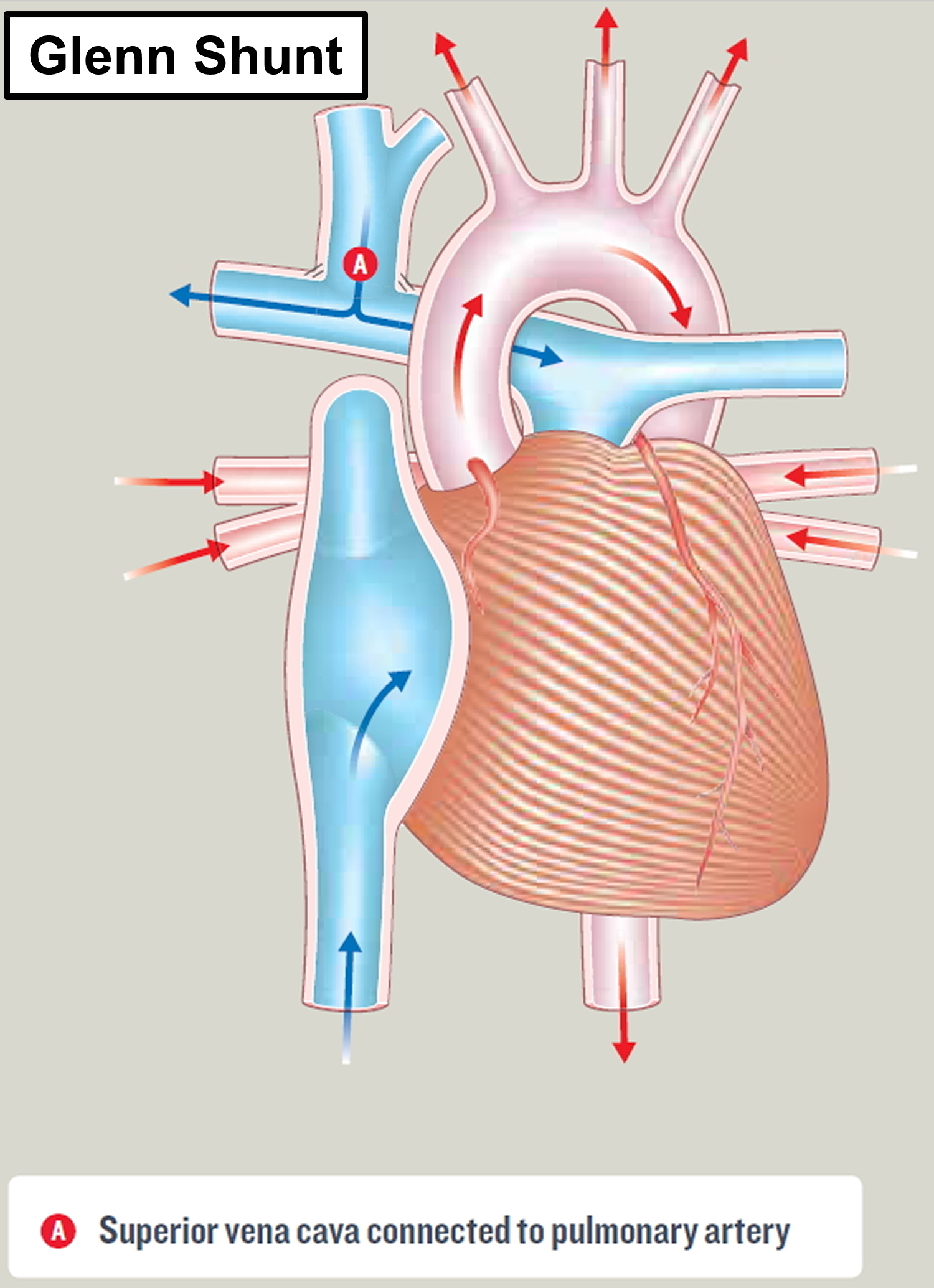
Stage II of the operation is called the Glenn shunt (cavopulmonary shunt) or hemi-Fontan procedure. The surgery is most often done when the child is 3 to 6 months of age. In this procedure, doctors remove the first shunt attached to the pulmonary arteries, and then connect the major vein carrying blue blood from the top half of the body (the superior vena cava) directly to blood vessels to the lungs (pulmonary arteries) to get oxygen. If surgeons previously performed a hybrid procedure, they’ll conduct additional steps during this procedure.
This procedure reduces the work of the right ventricle by allowing it to pump blood mainly to the aorta. It also allows most of the oxygen-poor blood returning from the body to flow directly into the lungs without a pump.
After this procedure, all the blood returning from the upper body is sent to the lungs, so blood with more oxygen is pumped to the aorta to supply organs and tissues throughout the body.
During stages I and II, the child may still appear somewhat blue (cyanotic).
What are the risks of a Glenn (cavopulmonary) shunt operation?
Most children survive this surgery, but they may become more blue and short of breath on exertion as they grow. The risk of death and other complications – such as narrowing where the superior vena cava has been joined to the pulmonary artery, brain damage, stroke or internal bleeding – varies based on the exact type of heart condition your child has. Other possible complications include pleural effusion (fluid around the lungs) and kidney damage. Your pediatric cardiologist or cardiac surgeon will discuss in details your child’s individual risk with you before surgery.
Figure 8. Glenn shunt (cavopulmonary shunt)
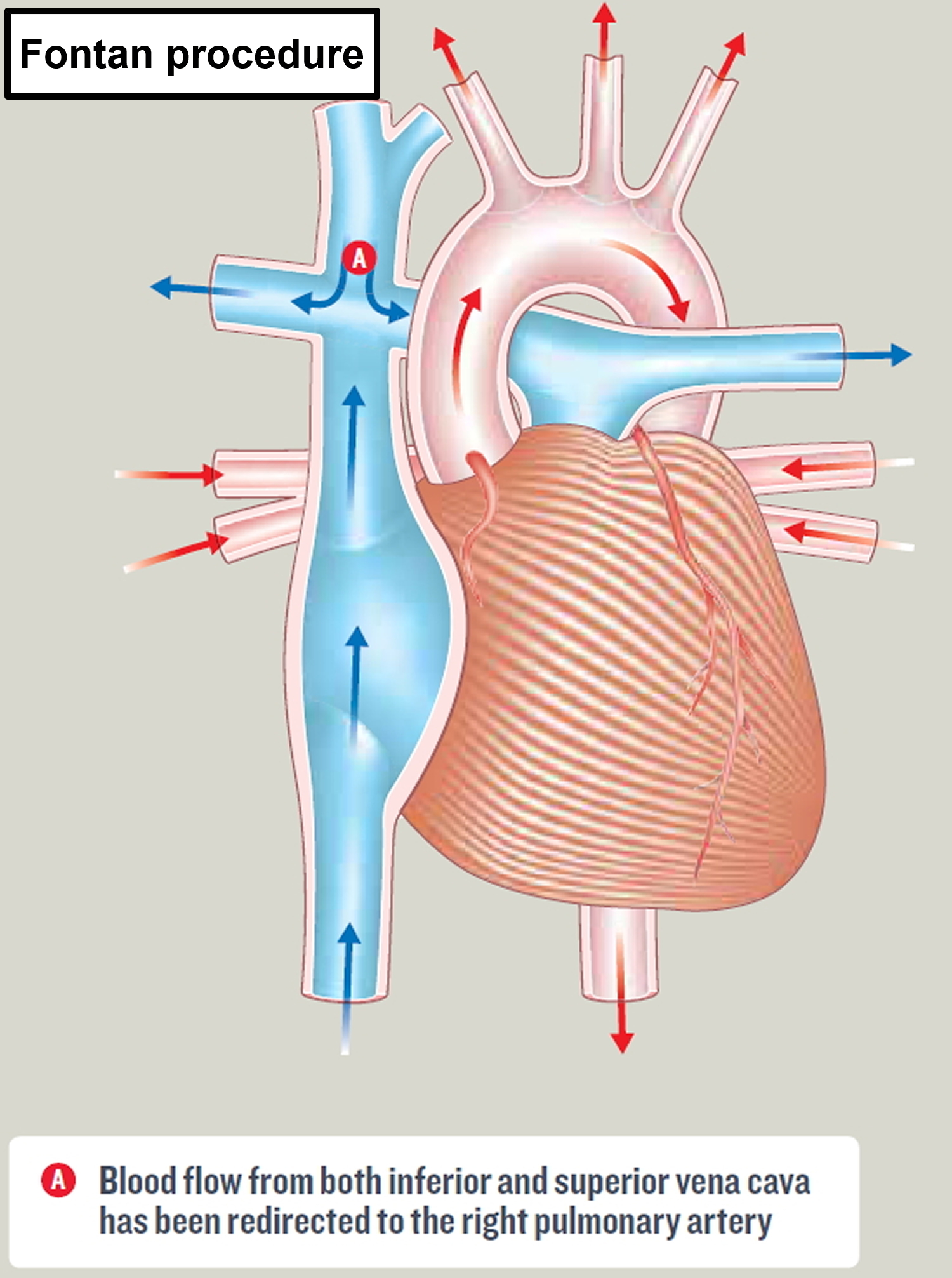
Fontan procedure
Stage III, the final step, is called the Fontan procedure. This surgery is usually performed when the baby is 18 months to 4 years old. The purpose of this operation is to improve the amount of oxygen in the blood and in most cases to improve exercise capacity. This is achieved by connecting both the inferior and superior vena cava to the pulmonary artery. The pulmonary arteries then transport the blood into the lungs. The right ventricle now serves only as the pumping chamber for the body (no longer the lungs and the body). This procedure allows the rest of the oxygen-poor blood returning from the body to flow to the lungs. After this procedure, there’s no mixing of oxygen-rich and oxygen-poor blood in the heart, and your child’s skin will no longer look blue. After this final step, the child is no longer cyanotic and has a normal oxygen level in the blood. A Fontan-type operation will not make your child’s heart normal, but – if the operation is successful – it should allow an adequate blood supply to the lungs to allow your child to grow.
Many modifications to the original Fontan operation technique have been developed, including: a modified Fontan, a fenestrated Fontan, and total cavopulmonary connection. Any type of Fontan operation is a major operation. Your child’s cardiac surgeon will explain exactly which operation your child needs.
Some people may need more surgeries in their 20s or 30s if they develop hard to control arrhythmias or other complications of the Fontan procedure.
Some doctors consider heart transplantation an alternative to the 3 step surgery, especially when the heart defects are complex. But there are few donated hearts available for small infants.
Babies with hypoplastic left heart syndrome can be considered for a transplant. While awaiting a heart transplant, your baby may require medications until a donor heart becomes available.
What are the risks of the Fontan-type procedure?
Most children survive this surgery. The risk of death and major complications – such as brain damage – varies depending on the exact type of heart condition your child has. Other possible complications include pleural effusion (fluid around the lungs), pericardial effusion (fluid around the heart), and kidney damage. Some children can develop heart rhythm disturbances which need to be treated with medicines, or less commonly with a pacemaker. The length of time your child will need to stay in hospital will vary, depending on how well he or she recovers after surgery. There is an increased risk of developing a blood clot after the surgery, so most children will need to take either warfarin or aspirin to help prevent this.
Figure 9. Fontan procedure (total cavopulmonary connection)
Follow-up care
After surgery or a transplant, your baby will need lifelong follow-up care with a cardiologist trained in congenital heart diseases to monitor his or her heart health. Various complications may occur over time and may require further treatment or medications.
Some medications may be necessary to regulate heart function. If your baby receives a heart transplant, anti-rejection medications will be necessary for the rest of his or her life to combat rejection of the new heart.
Your child’s cardiologist will tell you whether your child needs to take preventive antibiotics before certain dental or other procedures to prevent infections. In some cases, he or she may also recommend that your child limit physical activity.
Your doctor will likely recommend that you continue to have regular follow-up appointments with a cardiologist trained in congenital heart diseases as an adult. If you’re a woman and you’re considering pregnancy, discuss pregnancy risks with your doctor.
Coping and support
Caring for a baby with a serious heart problem, such as hypoplastic left heart syndrome, can be challenging. Here are some strategies that may help make it easier:
- Seek support. Ask for help from family members and friends. Talk with your child’s cardiologist about support groups and other types of assistance that are available near you.
- Record your baby’s health history. It will be important to write down your baby’s diagnosis, medications, surgery and other procedures and the dates they were performed, as well as the name and phone number of your child’s cardiologist, emergency contact numbers for your child’s doctors and hospital, and any other important information about your baby’s care. It’s also important to include a copy of the operative report from your child’s surgeon in your records. This information will help you recall the care your child has received, and it will be useful for doctors who are unfamiliar with your baby to review his or her complex health history.
- Talk about your concerns. As your child grows, you may worry about activities in which he or she can safely participate. Talk with the cardiologist about which activities are best for your child. If some are off-limits, encourage your child in other pursuits rather than focusing on what he or she can’t do. If other issues about your child’s health concern you, discuss them with your child’s cardiologist, too.
- Parker SE, Mai CT, Canfield MA, et al; for the National Birth Defects Prevention Network. Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol. 2010;88:1008-16.
- Gill HR, Splitt M, Sharland K, Simpson JM. 2003. Patterns of recurrence of congenital heart disease: An analysis of 6,640 consecutive pregnancies evaluated by detailed fetal echocardiography. Journal of the American College of Cardiology; 42: 923-9.





{kind=link}