What is ivermectin
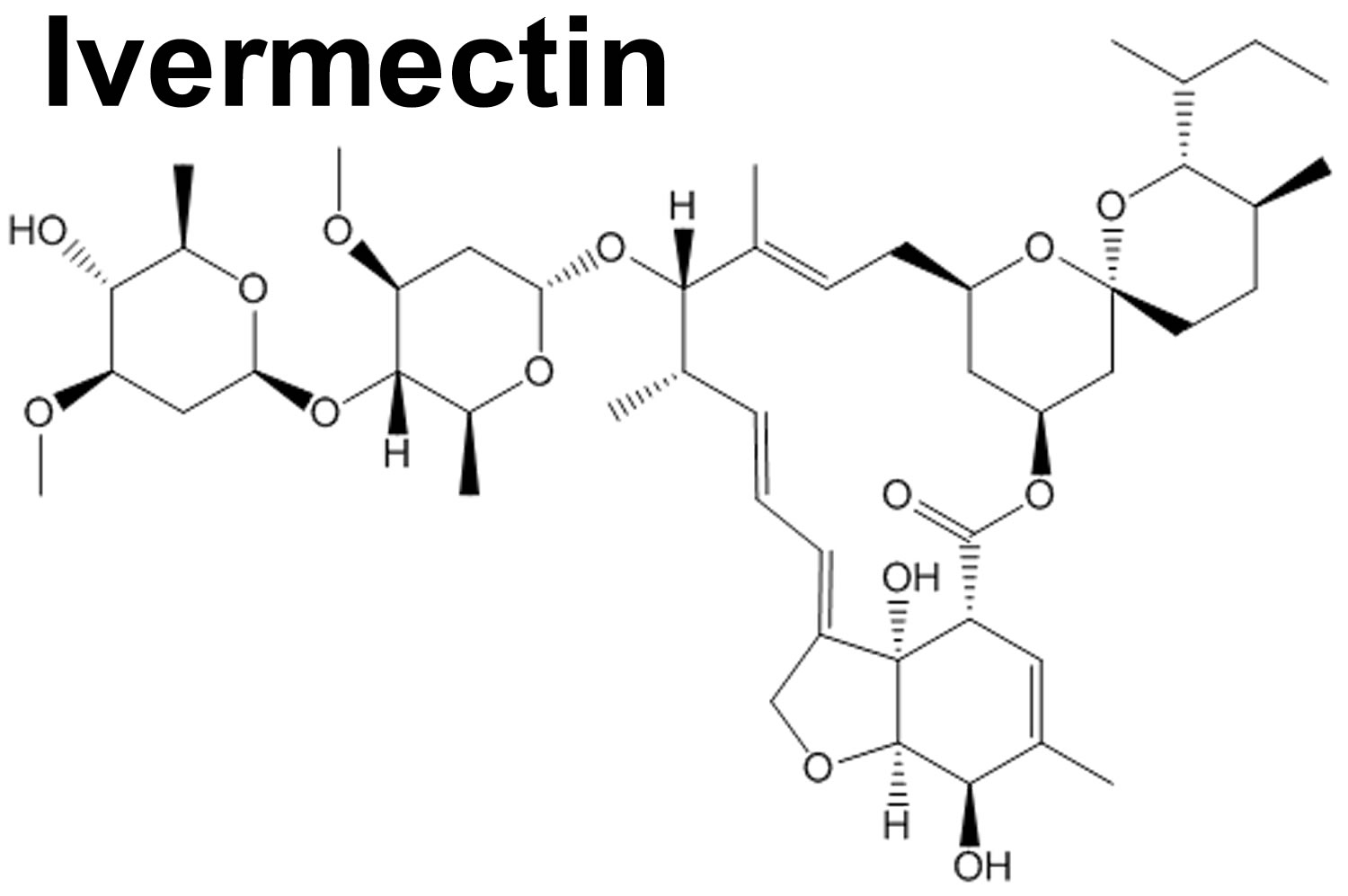
Ivermectin is an anti-parasite medication with activity against several parasitic nematodes (parasitic worms) and scabies and is the treatment of choice for onchocerciasis (also called “river blindness” because the blood-feeding flies that transmit the ultimately blinding disease inhabit lush, fertile land alongside the rivers in which they breed). Ivermectin has a broad spectrum of activity against several nematodes (Ascaris, Trichuris, Ancylostoma), cestodes (Taenia) and trematodes (Fasciola, Schistosoma). Ivermectin has particularly potent activity against onchocerciasis (river blindness) and lymphatic filariasis, which are important endemic diseases in Africa and South America. In tropical Africa, Onchocerca parasites (Onchocerca volvulus) are transmitted primarily by Dipteran blackflies of the Simulium damnosum complex, members of the Simulium neavei group also being vectors. Some game animals, notably elands and buffalo, are possible reservoir hosts. In the Western hemisphere, varieties of Simulium species bite humans and may transmit parasites. Ivermectin is a lipophilic drug that belongs to the avermectin class (mostly avermectin H2B1a with some avermectin H2B1b) of macrocyclic lactone compounds 1. Ivermectin acts as an endectocide (i.e., kills both endoparasites and ectoparasites). Ivermectin binds to and activates the glutamate-gated chloride channels of nerve and muscle cells of a wide variety of nematode (parasitic worms) and arthropod species, causing uncontrolled influx of chloride ions into the cells and leading to paralysis and death of the organism 2. Distinct from the channel opening induced by endogenous glutamate transmitter, ivermectin-activated channels open very slowly but essentially irreversibly. As a result, neurons or muscle cells remain at either hyperpolarisation or depolarization state, thereby resulting in paralysis and death of the parasites. Ivermectin does not readily pass the mammal blood-brain barrier to the central nervous system where glutamate-gated chloride channels locate, hence the hosts are relatively resistant to the effects of this agent. Ivermectin has a high safety profile in humans and livestock 3 and is one of the most commonly-used anti-helminthic drug in the livestock industry to control intestinal nematodes 1.
The large-scale administration of oral ivermectin to people has become a cornerstone in the global eradication campaign against human onchocerciasis and lymphatic filariasis 4. The recommended dose of ivermectin used to treat humans for filarial infection [i.e., 150 mg/kg body weight yields peak plasma concentrations of ca. 40–45 ng/ml] 5. At these plasma concentrations, ivermectin can significantly reduce the survival of Anopheles mosquitoes that ingest treated blood. Anopheles species shown to be susceptible to ivermectin at these concentrations include major vectors from Africa (Anopheles gambiae, Anopheles arabiensis), Southeast Asia (Anopheles campestris, Anopheles dirus, Anopheles minimus, Anopheles swandwongporni) and Latin America (Anopheles aquasalis, Anopheles darlingi). Pilot field trials in western Africa indicate that the mass drug administration of ivermectin against onchocerciasis and lymphatic filariasis can simultaneously reduce survival of Anopheles gambiae and local malaria transmission 6.
Figure 1. Ivermectin for humans
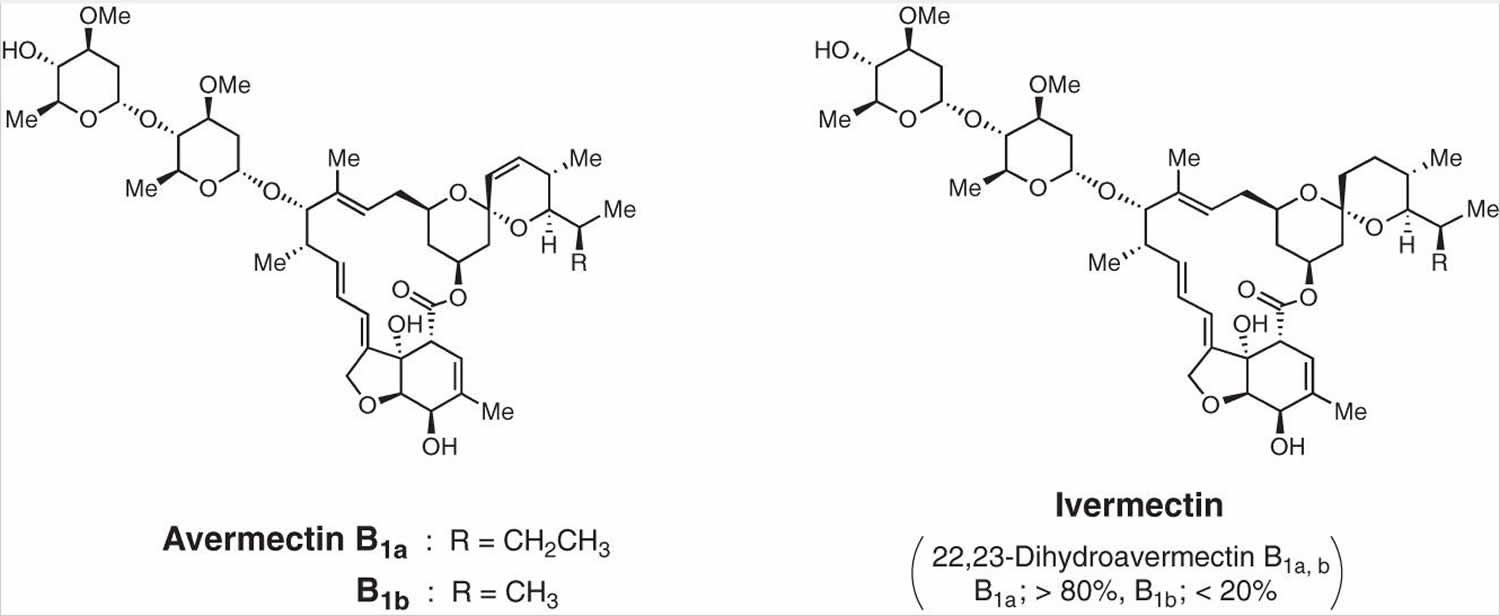
Figure 2. Ivermectin synthesis from avermectin
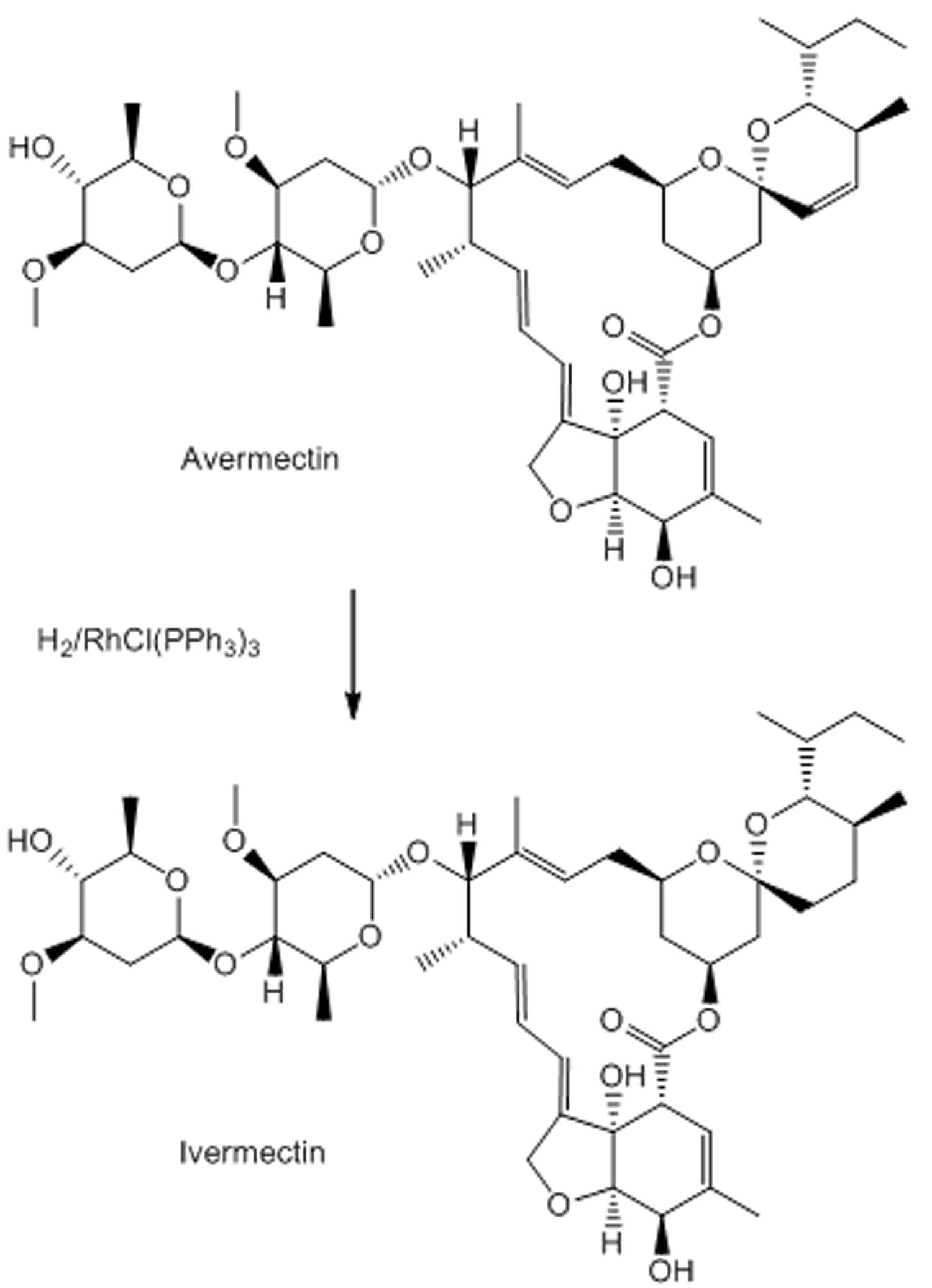
When it first appeared in the late-1970s, ivermectin, a derivative of avermectin was a truly revolutionary drug. Ivermectin was the world’s first endectocide (veterinary parasiticide), forerunner of a completely new class of antiparasitic agents, potently active against a wide range of internal and external nematodes and arthropods. Despite decades of searching around the world, the Japanese microorganism Streptomyces avermitilis remains the only source of avermectin ever found 7. Ivermectin is effective against a wide range of parasites, including gastrointestinal roundworms, lungworms, mites, lice and hornflies 8. Ivermectin is also highly effective against ticks, for example, the ixodid tick Rhipicephalus (Boophilus) microplus, one of the most important cattle parasites in the tropics and subtropics, which causes enormous economic damage. Indicative of the impact, in Brazil, where some 80% of the bovine herd is infested, losses total about $2 billion annually 9. Today, ivermectin is being used to treat billions of livestock and pets around the world, helping to boost production of food and leather products, as well as keep billions of companion animals, particularly dogs and horses, healthy. The ‘Blockbuster’ drug in the Animal Health sector, meaning that it achieved annual sales in excess of over US$1 billion, maintained that status for over 20 years 10. Ivermectin is so useful and adaptable that it is also being used off-label, sometimes, illegally, for example to treat fish lice in the aquaculture industry, where it can have a negative impact on non-target organisms 10. Ivermectin also has extensive uses in agriculture 11.
Today, ivermectin is being increasingly used worldwide to combat other diseases in humans, such as Strongyloidiasis (which infects some 35 million each year), scabies (which causes 300 million cases annually), Pediculosis, Gnathostomiasis and Myiasis—and new and promising properties and uses for ivermectin and other avermectin derivatives are continuing to be found 12. These include activity against another neglected tropical disease, Leishmaniasis 13. Of perhaps even greater significance is the evidence that the use of ivermectin has both direct and indirect beneficial impact on improving community health. Studies of long-term treatment with ivermectin to control Onchocerciasis have shown that use of the drug is additionally associated with significant reduction in the prevalence of infection with any soil-transmitted helminth parasites (including Ascaris, Trichuris and hookworm), most or all of which are deemed to be major causes of the morbidity arising from poor childhood nutrition and growth 14. It is also known that the prevalence of head lice is markedly reduced in children taking ivermectin tablets 15 and that scabies is markedly reduced in populations taking the drug regularly 16. Above all, ivermectin has proved to be a medicine of choice for the world’s rural poor. In many underprivileged communities throughout the tropics, intestinal worms and parasitic skin diseases are extremely common and associated with significant morbidity. They usually co-exist, with many individuals infected with both ecto- and endoparasites 17. Mass treatment of poly-parasitized populations is deemed to be the best means of control and ivermectin is the ideal drug for such interventions. A recent study in Brazil, using locally produced ivermectin, looked at the impact on internal helminthes and parasitic skin diseases. The researchers concluded that “mass treatment with ivermectin was an effective and safe means of reducing the prevalence of most of the parasitic diseases prevalent in a poor community in North-East Brazil. The effects of treatment lasted for a prolonged period of time”.
Ivermectin is typically given as one or two oral doses. Ivermectin therapy has been associated with minor, self-limiting serum aminotransferase elevations and very rare instances of clinically apparent liver injury 18.
Ivermectin for preventing and treating COVID‐19
In cell culture systems, ivermectin has activity against several viruses including the novel coronavirus known as COVID‐19 (Severe Acute Respiratory Syndrome coronavirus-type 2 [SARS-CoV-2]) virus, the cause of the global pandemic of respiratory illness 19. In the face of growing burden of severe illness posed by COVID-19, drugs with antiviral activity against SARS-CoV-2 in vitro (test tube studies) were often tried (repurposed) to improve the course and prevent death 20, 21, 22. A plausible and well‐characterized antiviral mechanism of ivermectin has been proposed to be the inhibition of nuclear translocation of viral proteins, facilitated by mammalian host importin also known as karyopherin α/β‐1 heterodimerization 21. Based on this mechanism, ivermectin binds to the importin alpha (armadillo repeat) domain causing thermal stability and a conformational change in alpha‐helicity that prevents binding to importin beta‐1 23.
Ivermectin was evaluated in several open label trials (14 studies with 1678 participants investigating ivermectin compared to no treatment, placebo, or standard of care) with suggestive evidence of benefit, but in more carefully designed, larger trials ivermectin in doses of 20 to 14 mg daily for 3 to 5 days had little or no effect in either preventing infection or ameliorating its outcome 24.
Ivermectin compared to placebo or standard of care for treating people in hospital with COVID‐19 (inpatient COVID‐19 treatment)
- Scientists are uncertain whether ivermectin compared to placebo or standard of care reduces or increases mortality and clinical worsening up to day 28 assessed as need for invasive mechanical ventilation (IMV) or need for supplemental oxygen (0 participants required supplemental oxygen; 1 study, 45 participants; very low‐certainty evidence), adverse events within 28 days and viral clearance at day seven 25. Ivermectin may have little or no effect compared to placebo or standard of care on clinical improvement up to 28 days and duration of hospitalization. No study reported quality of life up to 28 days 25.
Ivermectin compared to placebo or standard of care for outpatient COVID‐19 treatment
- Scientists are uncertain whether ivermectin compared to placebo or standard of care reduces or increases mortality up to 28 days and clinical worsening up to 14 days assessed as need for invasive mechanical ventilation or non‐invasive mechanical ventilation or high flow oxygen requirement. Researchers are uncertain whether ivermectin compared to placebo reduces or increases viral clearance at seven days. Ivermectin may have little or no effect compared to placebo or standard of care on the number of participants with symptoms resolved up to 14 days and adverse events within 28 days. None of the studies reporting duration of symptoms were eligible for primary analysis. No study reported hospital admission or quality of life up to 14 days 25.
Ivermectin compared to no treatment for prevention of COVID‐19 infection
- Researchers found one study. Mortality up to 28 days was the only outcome eligible for primary analysis. The researchers are uncertain whether ivermectin reduces or increases mortality (death rate) compared to no treatment. The study reported results for development of COVID‐19 symptoms and adverse events up to 14 days that were included in a secondary analysis due to high risk of bias. No study reported COVID‐19 infection, hospital admission, and quality of life up to 14 days.
Based on the current very low‐ to low‐certainty evidence, scientists are uncertain about the effectiveness and safety of ivermectin used to treat or prevent COVID‐19 25. The completed studies are small and few are considered high quality. Several studies are underway that may produce clearer answers in review updates. Overall, the reliable evidence available does not support the use ivermectin for treatment or prevention of COVID‐19 outside of well‐designed randomized trials.
Evaluation of ivermectin is continuing in 31 ongoing studies, and we will update this post with their results when they become available.
ICON Clinical Study Results
- Use of Ivermectin Is Associated With Lower Mortality in Hospitalized Patients With Coronavirus Disease 2019: The Ivermectin in COVID Nineteen Study 26, 27
- The ICON study, which was a multihospital retrospective cohort study, involved 280 patients, 173 patients were treated with at least one oral dose of 200 μg/kg ivermectin and 107 patients had no ivermectin treatment. Patients could also be treated with hydroxychloroquine, azithromycin, or both.
- The results from this study showed that:
- Overall mortality was significantly lower for the ivermectin group (15%) compared to the usual treatment group (25.2%) using figures from the unmatched cohort.
- Mortality for the subgroup of patients who had severe pulmonary involvement was lower in the ivermectin treatment group (38.8%) compared to the usual treatment group (80.7%) from the unmatched cohort.
- There was no significant difference between the two treatment groups regarding successful extubation rates of mechanically ventilated patients. Successful extubation is when the patient has had the breathing tube that has been used for mechanical ventilation removed and they can successfully breath on their own.
- Length of hospital stay was not significantly different between the ivermectin treatment group and the regular treatment group.
- For secondary analysis of the results propensity score matching was performed, which is when the researcher matches a person in the treatment group to a person in the non-treatment group who has similar characteristics. This reduces the effects of confounding and selection bias.
- For the propensity matched cohort figures the mortality was significantly lower in the ivermectin treatment group compared to the regular treatment group (13.3% vs 24.5%).
- The study noted that “Interpretation of these findings are tempered by the limitations of the retrospective design and the possibility of confounding” and that “Further studies in appropriately designed randomized trials are recommended before any conclusions can be made.”
- There has been feedback in regard to this study querying some of the important variables and how they may have affected the study outcome.
IVERCOR-COVID-19 trial
- Ivermectin to prevent hospitalizations in patients with COVID-19 (IVERCOR-COVID19) a randomized, double-blind, placebo-controlled trial 28
- The IVERCOR-COVID-19 trial was a randomized, double-blind, placebo controlled trial involving 501 patients. The aim of this trial was to determine whether ivermectin treatment could prevent hospitalization of individuals with early COVID-19. One group was treated with ivermectin plus standard treatment and the other group was treated with placebo with standard treatment. Patients were not allowed to take hydroxychloroquine, chloroquine or antiviral drugs.
- The results of this trial were published on 2 July 2021 showed that:
- The percentage of patients that needed hospitalization was 5.6% in the ivermectin treatment group and 8.4% in the placebo group, but the difference between the two groups was not statistically significantly
- There was no statistically significant difference in median time from patient enrollment to hospitalization between the treatment groups. The ivermectin treatment group median time to hospitalization was 3.5 days and placebo group 3 days.
- There was no statistically significant difference in mean time from study enrolment until a patient was put on invasive mechanical ventilatory support (MVS). The ivermectin treatment group was 5.25 days compared to the placebo group which was 10 days.
- The limitations in this study was noted as a:
- Low percentage of hospitalized patients
- The mean dose of ivermectin was 192.37 μg/kg/day which was below the dose proposed as probably being effective.
PRINCIPLE TRIAL
- Platform Randomised Trial of Treatments in the Community for Epidemic and Pandemic Illnesses (PRINCIPLE) 29.
- The PRINCIPLE trial is a current trial investigating treatments for COVID-19 patients in the community who are more at risk of serious illness. The study is investigating a number of different treatments including ivermectin.
- Participants in the ivermectin part of the trial will be:
- Between the age 18 and 64 years old
- With a underlying health condition or shortness of breath due to COVID-19
- Must join trial within first 14 days of covid-19 symptoms or a positive test
- Will be assigned to receive 3 day course of oral ivermectin treatment
- They will be compared to a group of patients receiving standard NHS COVID-19 care.
The ivermectin part of this trial started in June 2021 and results will be published when available.
Here’s what you need to know about Ivermectin
- Ivermectin is not FDA approved to treat COVID-19 patients. Ivermectin should not be used in patients for COVID-19, unless it is part of a clinical trial.
- With known antiviral properties, ivermectin has been shown to reduce SARS-CoV-2 replication in laboratory studies 29. Small pilot studies show that early administration with ivermectin can reduce viral load and the duration of symptoms in some patients with mild COVID-19. Even though ivermectin is used routinely in some countries to treat COVID-19, there is little evidence from large-scale randomised controlled trials to demonstrate that it can speed up recovery from the illness or reduce hospital admission 29.
- Currently there is not enough high quality evidence supporting the use of ivermectin for COVID-19 treatment 30. Clinical trials assessing ivermectin tablets for the prevention or treatment of COVID-19 in people are ongoing.
- More randomized clinical trials with a higher certainty of evidence are needed for ivermectin in the treatment COVID-19.
- Ivermectin tablets are FDA approved medicine for some types of intestinal worms and ivermectin cream is FDA approved for rosacea treatment.
- Both oral and topical ivermectin have a good safety profile at standard dosing levels.
The World Health Organization’s (WHO) Therapeutics and COVID-19 living guideline is the World Health Organization’s most up-to-date recommendations of treatments of COVID-19.
- Their recommendation is that ivermectin should not used in patients with COVID-19 unless it is in a research setting, as part of a clinical trial 31.
- This recommendation is the result of a systematic review of randomized clinical trials that used ivermectin for COVID-19. After analysing the information from these studies, they believe that there is a high degree of uncertainty on whether ivermectin is helpful or harmful in treating COVID-19.
- The uncertainty in some of the ivermectin trials for COVID-19 is due to:
- serious risk of bias
- serious risk of imprecision.
There are far fewer randomized controlled trials for ivermectin compared to other COVID treatments. The randomized controlled trials included multiple small trials, that had fewer patients enrolled and had fewer events recorded.
More randomized controlled trials are needed with higher quality of evidence to determine if ivermectin is successful at treating COVID-19.
Ivermectin for humans
Ivermectin is used to treat strongyloidiasis (threadworm; infection with a type of roundworm that enters the body through the skin, moves through the airways and lives in the intestines). Ivermectin is also used to control onchocerciasis (river blindness; infection with a type of roundworm that may cause rash, bumps under the skin, and vision problems including vision loss or blindness). Ivermectin is in a class of medications called anthelmintics. It treats strongyloidosis by killing the worms in the intestines. Ivermectin treats onchocerciasis by killing the developing worms. Ivermectin does not kill the adult worms that cause onchocerciasis and therefore it will not cure this type of infection.
Ivermectin is also sometimes used to treat certain other roundworm infections, head or pubic lice infestation, and scabies (itchy skin condition caused by infestation with small mites that live under the skin). Talk to your doctor about the risks of using this medication for your condition.
Ivermectin may be prescribed for other uses; ask your doctor or pharmacist for more information.
How should ivermectin be used?
Ivermectin comes as a tablet to take by mouth. It is usually taken as a single dose on an empty stomach with water. If you are taking ivermectin to treat onchocerciasis, additional doses 3, 6, or 12 months later may be necessary to control your infection. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take ivermectin exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
Retreatment is required because ivermectin has no activity against adult onchocerca volvulus parasites which tend to reside in subcutaneous nodules. Surgical excision of these nodules may be considered to eliminate the adult reproduction of microfilariae.
Patients with crusted scabies may require two or more doses of ivermectin spaced at one to two week intervals.
If you are taking ivermectin to treat strongyloidiasis, you will need to have a stool exam at least three times during the first 3 months after your treatment to see if your infection has cleared. If your infection has not cleared, your doctor will probably prescribe additional doses of ivermectin.
Ivermectin special precautions
Appropriate studies performed to date have not demonstrated pediatric-specific problems that would limit the usefulness of ivermectin topical lotion in children. However, use is not recommended in infants younger than 6 months of age.
Appropriate studies have not been performed on the relationship of age to the effects of ivermectin topical cream in the pediatric population. Safety and efficacy have not been established.
Pregnancy Category C: Animal studies have shown an adverse effect and there are no adequate studies in pregnant women OR no animal studies have been conducted and there are no adequate studies in pregnant women.
- Two cases of the use of ivermectin during pregnancy have been reported. These reports found that the risk of fetal damage in pregnant women treated with ivermectin was no greater than control. The risk versus benefit should be considered in pregnant women heavily infected with parasites, especially during mass distribution of ivermectin in endemic areas. The advantage of treatment may outweigh any potential risk to the infant 32, 33, 34.
Breastfeeding: There are no adequate studies in women for determining infant risk when using this medication during breastfeeding. Ivermectin is excreted into human milk in low concentrations. The manufacturer recommends that treatment during nursing only occur if the risk of delayed treatment to the mother outweighs the possible risk to the infant. Weigh the potential benefits against the potential risks before taking this medication while breastfeeding.
Before taking ivermectin:
- tell your doctor and pharmacist if you are allergic to ivermectin or any other medications.
- tell your doctor and pharmacist what other prescription and nonprescription medications, vitamins, nutritional supplements, and herbal products you are taking or plan to take. Be sure to mention if you are taking medications for anxiety, mental illness or seizures; muscle relaxants; sedatives; sleeping pills; or tranquilizers. Your doctor may need to change the doses of your medications or monitor you carefully for side effects.
- tell your doctor if you have or have ever had meningitis, human African trypanosomiasis (African sleeping sickness; an infection that is spread by the bite of the tsetse fly in certain African countries), or conditions that affect your immune system, such as human immunodeficiency virus (HIV).
tell your doctor if you are pregnant, plan to become pregnant, or are breast-feeding. If you become pregnant during your treatment with ivermectin, call your doctor. - ask your doctor about the safe use of alcoholic beverages while you are taking ivermectin.
- if you are taking ivermectin for onchocerciasis, you should know that you may experience dizziness, lightheadedness, and fainting when you get up too quickly from a lying position. To avoid this problem, get out of bed slowly, resting your feet on the floor for a few minutes before standing up.if you are taking ivermectin for strongyloidiasis and have had loiasis (Loa loa infection with a type of worm that causes skin and eye problems) or if you have ever lived in or traveled to areas of West or Central Africa where loiasis is common, you should know that you may have a serious reaction. Call your doctor immediately if you experience blurred vision, head or neck pain, seizures or difficulty walking or standing.
Precautions
Cutaneous, systemic and/or ophthalmological reactions have been reported with other microfilaricidal drugs. Allergic and inflammatory reactions (the Mazzotti reaction) may occur with ivermectin, probably due to the death of the microfilariae. Patients treated with ivermectin therapy for onchocerciasis may experience these reactions in addition to clinical adverse reactions possibly, probably, or definitely related to the therapy itself. The treatment of severe Mazzotti reactions has not been subjected to controlled clinical studies. Oral or intravenous rehydration, corticosteroids, antihistamines, acetaminophen and/or aspirin have been used for treatment.
After treatment with microfilaricidal medications, patients with hyperreactive onchodermatitis (sowda) may be more likely than others to experience severe adverse reactions, especially edema and aggravation of onchodermatitis.
Serious or fatal encephalopathy has been reported rarely in patients with onchocerciasis, and heavily infected with Loa loa, either spontaneously or after treatment with ivermectin. In these patients, pain (including neck and back pain), red eye, conjunctival hemorrhage, dyspnea, urinary and/or fecal incontinence, difficulty in standing/walking, mental status changes, confusion, lethargy, stupor, seizures, or coma have been reported. This syndrome has been seen very rarely following the use of ivermectin therapy. Pretreatment assessment for loiasis and careful posttreatment follow-up should be implemented in all patients considered for treatment with ivermectin for any reason and who had exposure to Loa loa endemic areas of West and Central Africa.
The patient should be advised of the need for repeated stool examinations to document clearance of infection with Strongyloides stercoralis.
The patient should be advised that treatment with ivermectin does not kill the adult Onchocerca parasites, and therefore repeated follow-up and retreatment is usually necessary.
In immunocompromised (including HIV-infected) patients being treated for intestinal strongyloidiasis, repeated courses of therapy may be necessary. Adequate and well-controlled clinical trials have not been conducted in such patients to determine the optimal dosing regimen. Several treatments, i.e., at 2-week intervals, may be required, and cure may not be attained. Control of extraintestinal strongyloidiasis in these patients is difficult, and suppressive therapy, i.e., once per month, may be useful.
Ivermectin is extensively metabolized in the liver and should be used cautiously in patients with hepatic disease. Dosage adjustments may be needed, although specific recommendations are not currently available. The manufacturer does not recommend that ivermectin treatment be excluded in patients with liver disease.
Clinical trials of ivermectin did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger patients. Other reported clinical experience has not identified differences in responses between elderly and younger patients. In general, treatment of elderly patients should be cautious, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
Safety and effectiveness in pediatric patients weighing less than 15 kg have not been determined.
Ivermectin dosage for humans
Each ivermectin dose should be taken on an empty stomach with a full (8 oz) glass of water.
A recent pharmacokinetics study reports that following a high-fat meal absorption was significantly higher (about 2.5 times) than in the fasted state.
Adult Dose for Onchocerciasis
- 0.15 mg/kg orally once every 12 months
- Patients with heavy ocular infection may require retreatment every 6 months. Retreatment may be considered at intervals as short as 3 months.
Dosage guidelines based on body weight:
- 15 to 25 kg: 3 mg orally one time
- 26 to 44 kg: 6 mg orally one time
- 45 to 64 kg: 9 mg orally one time
- 65 to 84 kg: 12 mg orally one time
- 85 kg or more: 0.15 mg/kg orally one time
Adult Dose for Strongyloidiasis
- 0.2 mg/kg orally once
- In immunocompromised (including HIV) patients, the treatment of strongyloidiasis may be refractory requiring repeated treatment (i.e., every 2 weeks) and suppressive therapy (i.e., once a month), although well-controlled studies are not available. Cure may not be achievable in these patients.
Dosage guidelines based on body weight:
- 15 to 24 kg: 3 mg orally one time
- 25 to 35 kg: 6 mg orally one time
- 36 to 50 kg: 9 mg orally one time
- 51 to 65 kg: 12 mg orally one time
- 66 to 79 kg: 15 mg orally one time
- 80 kg or more: 0.2 mg/kg orally one time
Adult Dose for Ascariasis
- 0.2 mg/kg orally once
Adult Dose for Cutaneous Larva Migrans
- 0.2 mg/kg orally once
Adult Dose for Filariasis
- 0.2 mg/kg orally once
Study (n=26,000) of mass treatment in Papua, New Guinea:
- Bancroftian filariasis: 0.4 mg/kg orally once yearly (with a single annual dose of diethylcarbamazine 6 mg/kg), for 4 to 6 years
Adult Dose for Scabies
- 0.2 mg/kg orally once, and repeated in 2 weeks
- Ivermectin therapy may be combined with a topical scabicide.
Pediatric Dose for Filariasis
Study (n=26,000) of mass treatment in Papua, New Guinea:
- Bancroftian filariasis: 5 years or older: 0.4 mg/kg orally once yearly (with a single annual dose of diethylcarbamazine 6 mg/kg), for 4 to 6 years
Renal Dose Adjustments
- Data not available
Liver Dose Adjustments
- Data not available
What should I do if I forget a dose?
Ivermectin is usually taken as a single dose. Tell your doctor if you do not take your medication.
Ivermectin Topical Application Route
Ivermectin Topical Application is available only with your doctor’s prescription.
Ivermectin Topical Application is available in the following dosage forms:
- Cream
- Lotion
Rare side effects
- burning, itching, redness, or stinging of the skin
- burning, dry, or itching eyes
- dandruff
- discharge or excessive tearing
- dry skin
- redness, pain, or swelling of the eye, eyelid, or inner lining of the eyelid
Other side effects not listed may also occur in some patients. If you notice any other effects, check with your healthcare professional.
Ivermectin Topical Dosage
The dose of Ivermectin Topical Application will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of this medicine. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of Ivermectin Topical Application that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
For topical dosage form (cream):
- For rosacea:
- Adults—Apply to the affected area(s) of the face once a day.
- Children—Use and dose must be determined by your doctor.
For topical dosage form (lotion):
- For head lice:
- Adults, teenagers, and children 6 months of age and older—Apply directly to dry hair and scalp one time only.
- Infants younger than 6 months of age—Use is not recommended.
Ivermectin for head lice
- Ivermectin 0.5% topical lotion is used to treat head lice infestations.
To use Sklice™ topical lotion:
- Use Sklice™ on the hair and scalp only. Keep the medicine out of your eyes, nose, mouth, and vagina. If the medicine gets in your eyes, rinse them well with water.
- Wash your hands before and after using this medicine.
- Apply the medicine directly to dry hair (up to 1 tube) closest to the scalp and then apply outwards. Completely cover your entire head. Leave the medicine on the hair and scalp for 10 minutes.
- After 10 minutes, rinse your hair with warm water and dry with a clean towel. Comb hair with a fine-toothed comb to remove any nits (eggs) or nit shells. They look like small white dots.
- If live lice are seen 7 days after using this medicine, tell your doctor right away.
- Do not use this medicine again without talking to your doctor first.
- Children will need an adult to apply the medicine for them.
- Throw away any unused medicine left in the tube after each use.
- Do not use cosmetics and other hair products on the treated hair and scalp areas.
Precautions
For patients using Sklice™:
- Head lice can be easily spread from one person to another by direct contact with clothing, hats, bandannas, scarves, bedding, towels, washcloths, ribbons, hair bands, helmets, hairbrushes and combs, or hairs from infected persons. All members of your household should be checked for head lice and should receive treatment if they are found to be infected. If you have any questions about this, check with your doctor.
- To prevent spread of lice: Dry-clean or wash your clothes, bedding, and personal items (including washcloths, towels, hats, scarves, combs, brushes, hairpieces, and wigs) in hot, soapy water.
- Do not use this medicine for a hair or scalp problem that has not been checked by your doctor.
Ivermectin for rosacea
- Ivermectin 1% topical cream is used to treat lesions of rosacea. Rosacea is a skin disease that causes redness and pimples on your nose, cheeks, chin, and forehead.
To use Soolantra™ topical cream:
- This medicine is for use on the skin only. Do not get it in your eyes, mouth, or vagina. Do not use it on skin areas that have cuts or scrapes. If it does get on these areas, rinse it off right away.
- Wash your hands before and after using this medicine.
- Use a pea-sized amount for each affected area of the face (forehead, chin, nose, cheeks).
- Spread a thin layer and avoid the eyes and lips.
Precautions
For patients using Soolantra™:
- If your skin problem does not improve within a few days or if it becomes worse, check with your doctor.
- Do not use this medicine for a skin problem that has not been checked by your doctor.
- If you have any questions about this, check with your doctor.
Ivermectin side effects
Ivermectin is well tolerated compared to other microfilaricidal agents (i.e., thiabendazole, diethylcarbamazine). Adverse reactions (i.e., pruritus, fever, rash, myalgia, headache) occur commonly during the first 3 days after treatment and appear to be related to the extent of parasitic infection and systemic mobilization and killing of microfilariae. The majority of reactions can usually be treated with aspirin, acetaminophen and/or antihistamines. Adverse effects tend to occur with lesser frequency during periods of retreatment.
Ivermectin may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- dizziness
- loss of appetite
- nausea
- vomiting
- stomach pain or bloating
- diarrhea
- constipation
- weakness
- sleepiness
- uncontrollable shaking of a part of the body
- chest discomfort
If you are taking ivermectin to treat onchocerciasis, you may also experience the following side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- swelling of the eyes, face, arms, hands, feet, ankles, or lower legs
- joint pain and swelling
- painful and swollen glands of the neck, armpit or groin
- rapid heartbeat
- eye pain, redness, or tearing
- swelling of the eye or eyelids
- abnormal sensation in the eyes
Some side effects can be serious. If you experience any of these symptoms, call your doctor immediately:
- fever
- blistering or peeling skin
- rash
- hives
- itching
Ivermectin may cause other side effects. Call your doctor if you have any unusual problems while taking this medication.
Some side effects of ivermectin may occur that usually do not need medical attention. These side effects may go away during treatment as your body adjusts to the medicine. Also, your health care professional may be able to tell you about ways to prevent or reduce some of these side effects. Check with your health care professional if any of the following side effects continue or are bothersome or if you have any questions about them:
More common—for the treatment of river blindness (onchocerciasis) only
- fever, itching or skin rash
- joint or muscle pain
- painful and tender glands in neck, armpits, or groin
- rapid heartbeat
Less common—for the treatment of river blindness (onchocerciasis) only
- headache
- swelling of the face, hands, arms, feet, or legs
Less common—for the treatment of strongyloidiasis only
- diarrhea
- dizziness
- skin rash or itching
Rare—for the treatment of river blindness (onchocerciasis) only
- Lightheadedness when getting up from a lying or sitting position
Rare—for the treatment of strongyloidiasis only
- loss of appetite
- shaking or trembling
- sleepiness
Ocular
Ocular side effects have included eyelid edema, anterior uveitis, blurred vision, conjunctivitis, limbitis, punctate opacity, keratitis, abnormal sensation in the eyes, and chorioretinitis/choroiditis; however, these effects are also associated with the disease onchocerciasis. Loss of vision has occurred rarely but usually resolved without corticosteroid treatment. Conjunctival hemorrhage has been reported during postmarketing experience in patients treated for onchocerciasis.
Other
Worsening of Mazzotti reactions, including arthralgia, synovitis, lymph node enlargement and tenderness, pruritus, skin involvement (including edema, papular and pustular or frank urticarial rash), and fever, has been reported during the first 4 days following treatment for onchocerciasis.
Nervous system
Nervous system side effects have included dizziness, headache, somnolence, vertigo, and tremor. Serious or fatal encephalopathy has been reported rarely in patients with onchocerciases, and heavily infected with Loa loa, either spontaneously or after treatment with ivermectin. Seizures have been reported during postmarketing experience.
Gastrointestinal
Gastrointestinal side effects have included anorexia, constipation, diarrhea, nausea, vomiting, and abdominal distention.
Other
Other side effects have included asthenia, fatigue, abdominal pain, chest discomfort, facial edema, and peripheral edema.
Hematologic
Hematologic side effects have included decreased leukocyte count (3%), eosinophilia (3%), and increased hemoglobin (1%). Hematomatous swellings associated with prolonged prothrombin times have been reported, but the clinical significance is unknown. Leukopenia and anemia have been reported in at least one patient.
Hepatic
Hepatic side effects have included elevated ALT and/or AST. Elevated liver enzymes, elevated bilirubin, and hepatitis have been reported during postmarketing experience.
Cardiovascular
Cardiovascular side effects have included tachycardia and orthostatic hypotension. EKG changes, including prolonged PR interval, flattened T waves and peaked T waves, have been reported in single cases. Hypotension (primarily orthostatic hypotension) has been reported during postmarketing experience.
Dermatologic
Dermatologic side effects have included pruritus, rash, and urticaria. Toxic epidermal necrolysis and Stevens-Johnson syndrome have been reported during postmarketing experience.
Respiratory
Respiratory side effects have included worsening bronchial asthma, laryngeal edema, and dyspnea.
Musculoskeletal
Musculoskeletal side effects have included myalgia.
Renal
Renal side effects have included rare transient proteinuria.
Hepatotoxicity
Single dose therapy with ivermectin has been associated with a low rate of serum aminotransferase elevations. A single case of clinically apparent liver injury has been reported after ivermectin use 35. The onset of injury occurred 1 month after a single dose and was characterized by a hepatocellular pattern of serum enzyme elevations without jaundice. Recovery was rapid and complete. The mechanism by which it might cause liver injury is unknown 36.
Symptoms of overdose may include:
- rash
- hives
- seizure
- headache
- tingling of hands or feet
- weakness
- loss of coordination
- stomach pain
- nausea
- vomiting
- diarrhea
- dizziness
- shortness of breath
- swelling of the face, arms, hands, feet, ankles, or lower legs.
- Dreyer SM, Morin KJ, Vaughan JA. Differential susceptibilities of Anopheles albimanus and Anopheles stephensi mosquitoes to ivermectin. Malaria Journal. 2018;17:148. doi:10.1186/s12936-018-2296-3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5883420/
- Ivermectin: a potent new antiparasitic agent. Campbell WC, Fisher MH, Stapley EO, Albers-Schönberg G, Jacob TA. Science. 1983 Aug 26; 221(4613):823-8.
- Ivermectin, ‘wonder drug’ from Japan: the human use perspective. Crump A, Ōmura S. Proc Jpn Acad Ser B Phys Biol Sci. 2011; 87(2):13-28.
- Rebollo MP, Bockarie MJ. Toward the elimination of lymphatic filariasis by 2020: treatment update and impact assessment for the endgame. Expert Rev Anti Infect Ther. 2013;11:723–731. doi: 10.1586/14787210.2013.811841
- Canga AG, Prieto AMS, Liebana MJD, Martinez NG, Vega MS, Vieitez JJG. The pharmacokinetics and interactions of ivermectin in humans—a mini-review. AAPS J. 2008;10:42–46. doi: 10.1208/s12248-007-9000-9
- Sylla M, Kobylinski KC, Gray M, Chapman PL, Sarr MD, Rasgon JL, et al. Mass drug administration of ivermectin in south-eastern Senegal reduces the survivorship of wild-caught, blood fed malaria vectors. Malar J. 2010;9:365. doi: 10.1186/1475-2875-9-365
- The life and times of ivermectin – a success story. Omura S, Crump A. Nat Rev Microbiol. 2004 Dec; 2(12):984-9.
- Burg R.W., Miller B.M., Baker E.E., Birnbaum J., Currie S.A., Hartman R., Kong Y.L., Monaghan R.L., Olson G., Putter I., Tunac J.B., Wallick H., Stapley E.O., Oiwa R., Ōmura S. (1979) Avermectins, new family of potent anthelmintic agents: producing organisms and fermentation. Antimicrob. Agents Chemother. 15 (3), 361–367
- Grisi L., Massard C.L., Moya-Borja G.E., Pereira J.B. (2002) Impacto econômico das principais ectoparasitoses em bovinos no Brasil. Hora Veterinária 21, 8–10
- CRUMP A, ŌMURA S. Ivermectin, “Wonder drug” from Japan: the human use perspective. ŌMURA S, ed. Proceedings of the Japan Academy Series B, Physical and Biological Sciences. 2011;87(2):13-28. doi:10.2183/pjab.87.13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3043740/
- Ōmura S. (2008) Ivermectin: 25 years and still going strong. Int. J. Antimicrob. Agents 31, 91–98
- Geary T.G. (2005) Ivermectin 20 years on: maturation of a wonder drug. Trends Parasitol. 21 (11), 530–532
- dos Santos A.R., Falcão C.A., Muzitano M.F., Kaiser C.R., Rossi-Bergmann B., Férézou J.P. (2009) Ivermectin-derived leishmanicidal compounds. Bioorg. Med. Chem. 17 (2), 496–502
- Moncayo AL, Vaca M, Amorim L, et al. Impact of Long-Term Treatment with Ivermectin on the Prevalence and Intensity of Soil-Transmitted Helminth Infections. Bethony J, ed. PLoS Neglected Tropical Diseases. 2008;2(9):e293. doi:10.1371/journal.pntd.0000293. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2553482/
- Dunne C.L., Malone C.J., Whitworth J.A. (1991) A field study of the effects of ivermectin on ectoparasites of Man. Trans. R. Soc. Trop. Med. Hyg. 85, 550–551
- Bockarie M.J., Alexander N.D., Kazura J.W., Bockarie F., Griffin L., Alpers M.P. (2000) Treatment with ivermectin reduces the high prevalence of scabies in a village in Papua New Guinea. Acta Trop. 75, 127–130
- Heukelbach J. (2004) Ectoparasites—the underestimated realm. Lancet 363, 889–891
- Olivia Veit, Bernhard Beck, Michael Steuerwald, Christoph Hatz; First case of ivermectin-induced severe hepatitis, Transactions of The Royal Society of Tropical Medicine and Hygiene, Volume 100, Issue 8, 1 August 2006, Pages 795–797, https://doi.org/10.1016/j.trstmh.2006.02.003
- Kinobe, R. T., & Owens, L. (2021). A systematic review of experimental evidence for antiviral effects of ivermectin and an in silico analysis of ivermectin’s possible mode of action against SARS-CoV-2. Fundamental & clinical pharmacology, 35(2), 260–276. https://doi.org/10.1111/fcp.12644
- Heidary F, Gharebaghi R. Ivermectin: a systematic review from antiviral effects to COVID‐19 complementary regimen. J. Antibiot. (Tokyo). 2020;73:593‐602. 10.1038/s41429-020-0336-z
- Jans DA, Wagstaff KM. Ivermectin as a broad‐spectrum host‐directed antiviral: the real deal? Cells. 2020;9(9):2100‐10.3390/cells9092100
- Formiga FR, Leblanc R, Reboucas JDS et al. Ivermectin: an award‐winning drug with expected antiviral activity against COVID‐19. J. Control Release. 2020; 329: 758–761. 10.1016/j.jconrel.2020.10.009
- Lundberg L, Pinkham C, Baer A et al. Nuclear import and export inhibitors alter capsid protein distribution in mammalian cells and reduce Venezuelan Equine Encephalitis Virus replication. Antiviral Res. 2013;100:662‐672. 10.1016/j.antiviral.2013.10.004
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Ivermectin. [Updated 2021 Apr 9]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548921
- Popp, M., Stegemann, M., Metzendorf, M. I., Gould, S., Kranke, P., Meybohm, P., Skoetz, N., & Weibel, S. (2021). Ivermectin for preventing and treating COVID-19. The Cochrane database of systematic reviews, 7(7), CD015017. https://doi.org/10.1002/14651858.CD015017.pub2
- Rajter, J. C., Sherman, M. S., Fatteh, N., Vogel, F., Sacks, J., & Rajter, J. J. (2021). Use of Ivermectin Is Associated With Lower Mortality in Hospitalized Patients With Coronavirus Disease 2019: The Ivermectin in COVID Nineteen Study. Chest, 159(1), 85–92. https://doi.org/10.1016/j.chest.2020.10.009
- Ortega-Guillén, E., Meneses, G., & Coila, E. (2021). Remarks About Retrospective Analysis of Ivermectin Effectiveness on Coronavirus Disease 2019 (ICON Study). Chest, 159(5), 2110–2111. https://doi.org/10.1016/j.chest.2020.10.088
- Vallejos, J., Zoni, R., Bangher, M. et al. Ivermectin to prevent hospitalizations in patients with COVID-19 (IVERCOR-COVID19) a randomized, double-blind, placebo-controlled trial. BMC Infect Dis 21, 635 (2021). https://doi.org/10.1186/s12879-021-06348-5
- Ivermectin to be investigated in adults aged 18+ as a possible treatment for COVID-19 in the PRINCIPLE trial. https://www.principletrial.org/news/ivermectin-to-be-investigated-as-a-possible-treatment-for-covid-19-in-oxford2019s-principle-trial
- Drug treatments for covid-19: living systematic review and network meta-analysis BMJ 2021; 373 :n967 doi:10.1136/bmj.n967
- Rochwerg B, Agarwal A, Siemieniuk R A, Agoritsas T, Lamontagne F, Askie L et al. A living WHO guideline on drugs for covid-19 BMJ 2020; 370 :m3379 doi:10.1136/bmj.m3379
- Pacque M, Munoz B, Poetschke G, Foose J, Greene BM, Taylor HR “Pregnancy outcome after inadvertent ivermectin treatment during community-based distribution.” Lancet 336 (1990): 1486-9
- Chippaux JP, Gardon-Wendel N, Gardon J, Ernould JC “Absence of any adverse effect of inadvertent ivermectin treatment during pregnancy.” Trans R Soc Trop Med Hyg 87 (1993): 318
- Ette EI, Thomas WO, Achumba JI “Ivermectin: a long-acting microfilaricidal agent.” DICP 24 (1990): 426-33
- First case of ivermectin-induced severe hepatitis. Trans R Soc Trop Med Hyg. 2006 Aug;100(8):795-7. Epub 2006 May 8. https://www.ncbi.nlm.nih.gov/pubmed/16682062
- Ivermectin. https://livertox.nih.gov/Ivermectin.htm





{kind=link}