
What is lightheadedness
Lightheadedness is a feeling that you are about to faint or “pass out.” You may sometimes feel nauseated or vomit when you are light-headed. You do not feel as if you or your surroundings are moving. Lightheadedness is different from vertigo, which is the feeling that you or things around you are spinning or tilting.
Lightheadedness usually goes away or gets better when you lie down. If lightheadedness gets worse, it can lead to lead to a feeling of almost fainting or a fainting spell (syncope).
It is common to feel lightheaded from time to time. Lightheadedness usually is not caused by a serious problem. Lightheadedness often is caused by a short-lasting drop in blood pressure and blood flow to your head that occurs when you get up too quickly from a seated or lying position (orthostatic hypotension). Ongoing light-headedness may mean you have a more serious problem that needs to be evaluated.
Call your local emergency services number anytime you think you may need emergency care. For example, call if:
- You have symptoms of a stroke. These may include:
- Sudden numbness, tingling, weakness, or loss of movement in your face, arm, or leg, especially on only one side of your body.
- Sudden vision changes.
- Sudden trouble speaking.
- Sudden confusion or trouble understanding simple statements.
- Sudden problems with walking or balance.
- A sudden, severe headache that is different from past headaches.
- You have symptoms of a heart attack. These may include:
- Chest pain or pressure, or a strange feeling in the chest.
- Sweating.
- Shortness of breath.
- Nausea or vomiting.
- Pain, pressure, or a strange feeling in the back, neck, jaw, or upper belly or in one or both shoulders or arms.
- Lightheadedness or sudden weakness.
- A fast or irregular heartbeat.
After you call your local emergency services number, the operator may tell you to chew 1 adult-strength or 2 to 4 low-dose aspirin. Wait for an ambulance. Do not try to drive yourself.
Watch closely for changes in your health, and be sure to contact your doctor call line if:
- Your lightheadedness gets worse or does not get better with home remedy.
What causes lightheadedness
Light-headedness has many causes, including:
- Allergies.
- Illnesses such as the flu or colds. Home treatment of your flu and cold symptoms usually will relieve light-headedness.
- Vomiting, diarrhea, fevers, and other illnesses that cause dehydration.
- Very deep or rapid breathing (hyperventilation).
- Anxiety and stress.
- The use of tobacco, alcohol, or illegal drugs.
Common reasons for lightheadedness include:
- Dehydration.
- Medication side effects.
- Sudden drop in blood pressure.
- Low blood sugar.
Alcohol and many prescription and non-prescription medicines can cause lightheadedness. These problems may develop from:
- Taking too much of a medicine (overmedicating).
- Alcohol and medicine interactions. This is a problem, especially for older adults, who may take many medicines at the same time.
- Misusing a medicine or alcohol.
- Drug intoxication or the effects of withdrawal.
Psychiatric causes of lightheadedness are common, particularly anxiety; therefore, anxiety and depression should be included in the patient history. In one study, about 28 percent of patients with lightheadedness reported symptoms of at least one anxiety disorder 1. In another study, one in four patients with lightheadedness met criteria for panic disorder 2. A study of patients with chronic lightheadedness showed that those with panic disorder were more likely to have neurotologic findings than those without panic disorder 3. Up to 60 percent of patients with chronic subjective lightheadedness have been reported to have an anxiety disorder 4. Depression and alcohol intoxication have also been found to overlap with lightheadedness 5.
Hyperventilation syndrome is an important cause of lightheadedness. Although the condition can be associated with anxiety disorders, many patients without anxiety experience hyperventilation. Hyperventilation is defined as breathing in excess of metabolic requirements, causing a respiratory alkalosis and lightheadedness. Patients may sigh repeatedly and may have associated symptoms, such as chest pain, paraesthesias, bloating, and epigastric pain 6.
At its most serious, lightheadedness could be a sign of heart attack or stroke. If you suspect you’re having a heart attack or stroke, seek immediate medical attention.
Another serious cause of lightheadedness is bleeding (hemorrhage). Most of the time, the location of the bleeding and the need to seek medical care are obvious. But sometimes bleeding is not obvious (occult bleeding). You may have small amounts of bleeding in your digestive tract over days or weeks without noticing the bleeding. When this happens, lightheadedness and fatigue may be the first noticeable symptoms that you are losing blood. Heavy menstrual bleeding also can cause this type of lightheadedness.
Sometimes the cause of lightheadedness is an abnormal heart rhythm (arrhythmia), which can cause fainting spells (syncope). Unexplained fainting spells need to be evaluated by a doctor. You can check your heart rate by taking your pulse.
Many prescription and non-prescription medicines can cause lightheadedness or vertigo. The degree of lightheadedness or vertigo that a medicine causes will vary.
Medications commonly associated with lightheadedness from orthostatic hypotension 7:
Cardiac medications
- Alpha blockers (e.g., doxazosin [Cardura], terazosin)
- Alpha/beta blockers (e.g., carvedilol [Coreg], labetalol)
- Angiotensin-converting enzyme inhibitors
- Beta blockers
- Clonidine (Catapres)
- Dipyridamole (Persantine)
- Diuretics (e.g., furosemide [Lasix])
- Hydralazine
- Methyldopa
- Nitrates (e.g., nitroglycerin paste, sublingual nitroglycerin)
- Reserpine
Central nervous system medications
- Antipsychotics (e.g., chlorpromazine, clozapine [Clozaril], thioridazine)
- Opioids
- Parkinsonian drugs (e.g., bromocriptine [Parlodel], levodopa/carbidopa [Sinemet])
- Skeletal muscle relaxants (e.g., baclofen [Lioresal], cyclobenzaprine [Flexeril], methocarbamol [Robaxin], tizanidine [Zanaflex])
- Tricyclic antidepressants (e.g., amitriptyline, doxepin, trazodone)
Urologic medications
- Phosphodiesterase type 5 inhibitors (e.g., sildenafil [Viagra])
- Urinary anticholinergics (e.g., oxybutynin [Ditropan])
Head trauma and whiplash injuries can cause a variety of dizziness symptoms, from vertigo to lightheadedness 8. The incidence of dizziness with a head injury or vertigo initially after whiplash have been reported as high as 78 to 80 percent.12 Selected causes of dizziness are summarized in Table 1.
Table 1. Selected causes of lightheadedness
| Cause | Category of dizziness | Pathophysiology | Diagnostic criteria |
|---|---|---|---|
Benign paroxysmal positional vertigo | Vertigo | Loose otolith in semicircular canals causing a false sense of motion | Positive findings with Dix-Hallpike maneuver; episodic vertigo without hearing loss |
Hyperventilation syndrome | Lightheadedness | Hyperventilation causing respiratory alkalosis; underlying anxiety may provoke the hyperventilation | Symptoms reproduced with voluntary hyperventilation |
Meniere disease | Vertigo | Increased endolymphatic fluid in the inner ear | Episodic vertigo with hearing loss |
Migrainous vertigo (vestibular migraine) | Vertigo | Uncertain; one hypothesis is that trigeminal nuclei stimulation causes nystagmus in persons with migraine | Episodic vertigo with signs of migraine, plus photophobia, phonophobia, or aura during at least two episodes of vertigo |
Orthostatic hypotension | Presyncope | Drop in blood pressure on position change causing decreased blood flow to the brain, adverse effect of multiple medications | Systolic blood pressure decrease of 20 mm Hg, diastolic blood pressure decrease of 10 mm Hg, or a pulse increase of 30 beats per minute |
Parkinson disease | Disequilibrium | Dysfunction in gait causing imbalance and falls | Shuffling gait with reduced arm swing and possible hesitation |
Peripheral neuropathy | Disequilibrium | Decreased tactile response when walking causes patient to be unaware when feet touch the ground, leading to imbalance and falls | Decreased sensation in lower extremities, particularly the feet |
What causes lightheadedness and dizziness
Dizziness is a word that is often used to describe two different feelings, lightheadedness and vertigo. Dizziness can range from fleeting faintness to a severe balance disorder that makes normal functioning impossible. Although dizziness can occur in people of any age, it is more common among older adults. Among adults over age 65, up to 30 percent experience dizziness. A fear of dizziness can cause older adults to limit their physical and social activities. Dizziness can also lead to falls and other injuries.
Dizziness may feel like:
- Lightheadedness, as though you might pass out
- Unsteadiness or a loss of balance
- Vertigo – vertigo is a feeling that you or your surroundings are moving when there is no actual movement. You may feel as though you are off balance, spinning, whirling, falling, or tilting. When you have severe vertigo, you may feel very nauseated or vomit. You may have trouble walking or standing, and you may lose your balance and fall.
- Floating, swimming or heavy-headedness
Dizziness is often temporary and goes away without treatment. As you talk with your doctor about your condition, try to describe your specific symptoms, how the dizziness makes you feel as it is coming on and after it has passed, what triggers it, and how long it lasts. This will help your doctor diagnose the cause and treat it.
Generally, see your doctor if you experience any recurrent, sudden, severe, or prolonged and unexplained dizziness or vertigo.
Get emergency medical care if you experience new, severe dizziness or vertigo along with any of the following:
- Sudden, severe headache
- Chest pain
- Difficulty breathing
- Numbness or paralysis of arms or legs
- Fainting
- Double vision
- Rapid or irregular heartbeat
- Confusion or slurred speech
- Stumbling or difficulty walking
- Ongoing vomiting
- Seizures
- A sudden change in hearing
- Facial numbness or weakness
In the meantime, these self-care tips may help:
- Move slowly. When you stand up from lying down, move slowly. Many people experience dizziness if they stand up too quickly.
- Drink plenty of fluids. Staying well-hydrated can help prevent or relieve several types of dizziness.
- Avoid caffeine and tobacco. By restricting blood flow, these substances can make symptoms worse.
Causes of lightheadedness and dizziness
The causes of dizziness are as varied as its symptoms. It can result from something as simple as motion sickness — the queasy feeling that you get on hairpin roads and roller coasters. Or it can be caused by an inner ear disturbance, infection, reduced blood flow due to blocked arteries or heart disease, medication side effects, anxiety, or another condition. Sometimes a cause can’t be identified.
Dizziness, particularly vertigo, occurring by itself, without any other symptoms, is generally unlikely to be a sign of a stroke.
Some causes of dizziness include:
Inner ear problems
Many cases of dizziness are caused by problems that affect the balance mechanism in your inner ear. Examples include:
- Benign paroxysmal positional vertigo (BPPV)
- Ear infection (middle ear)
- Meniere’s disease
- Migraine
Reduced blood flow
Dizziness can be caused if your brain doesn’t receive enough blood. This can occur for a variety of reasons, including:
- Arteriosclerosis / atherosclerosis
- Anemia
- Dehydration
- Hypoglycemia
- Heart arrhythmias (heart rhythm problems)
- Orthostatic hypotension (postural hypotension)
- Stroke
- Transient ischemic attack (TIA)
Certain medications
Some types of drugs cause dizziness, including some varieties of:
- Antidepressants
- Anti-seizure drugs
- Drugs to control high blood pressure
- Sedatives
- Tranquilizers
Other causes of dizziness
- Concussion
- Depression (major depressive disorder)
- Generalized anxiety disorder
- Motion sickness: First aid
- Panic attacks and panic disorder
Lightheadedness symptoms
Lightheadedness is a feeling that you are about to faint or “pass out.” You may sometimes feel nauseated or vomit when you are light-headed. You do not feel as if you or your surroundings are moving. Lightheadedness is different from vertigo, which is the feeling that you or things around you are spinning or tilting.
Lightheadedness diagnosis
Diagnosing the cause of lightheadedness can be difficult because symptoms are often nonspecific and the differential diagnosis is broad. However, a few simple questions and physical examination tests can help narrow the possible diagnoses.
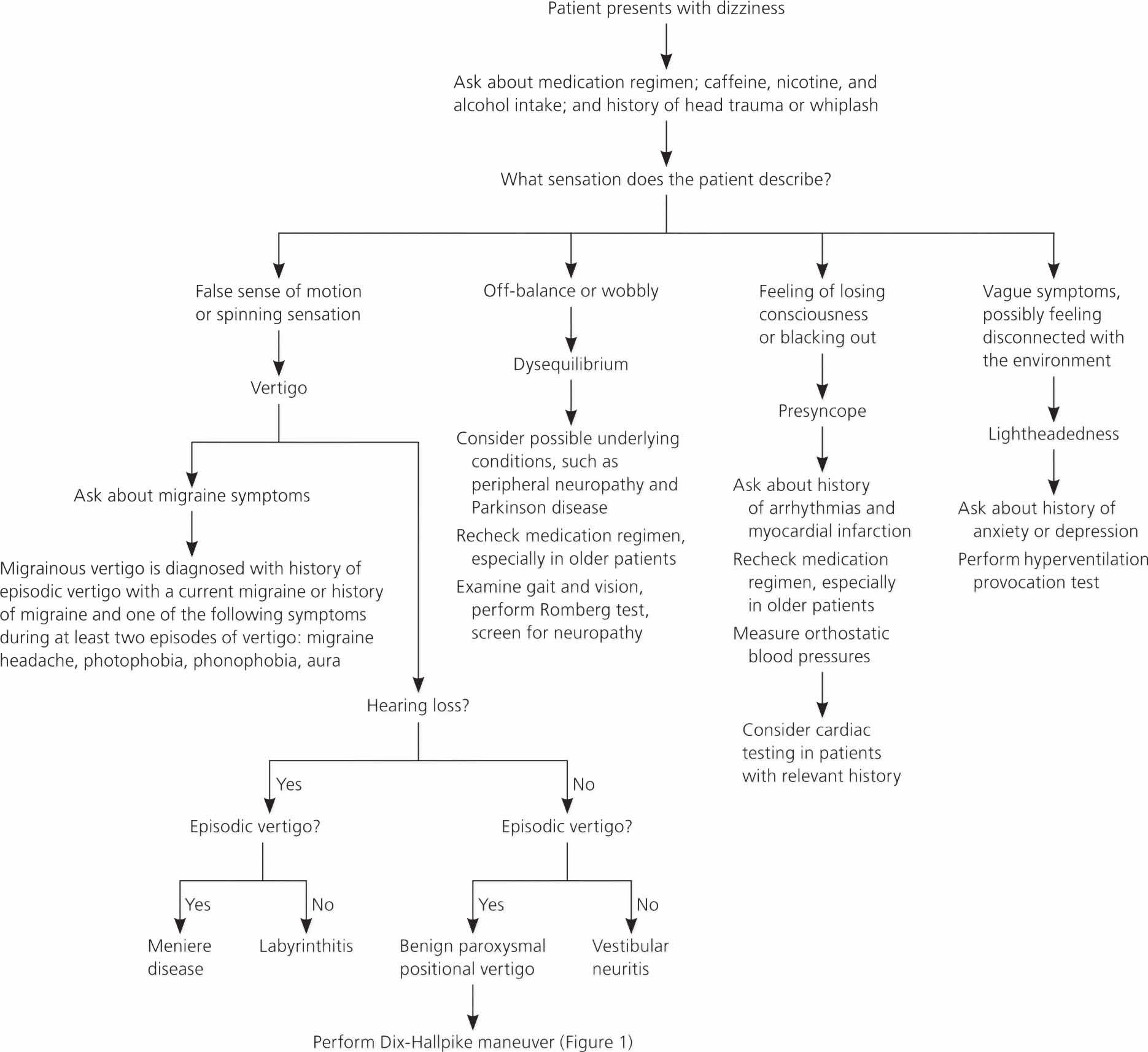
Figure 1. Algorithm for the initial evaluation of a patient with dizziness
Physical examination
The main goal of the physical examination is to reproduce the patient’s lightheadedness in the office. There are a few simple physical examination tests that can be performed to aid in this goal.
First, blood pressure should be measured while the patient is in a supine position and again at least one minute after the patient stands. A systolic blood pressure decrease of 20 mm Hg, diastolic blood pressure decrease of 10 mm Hg, or pulse increase of 30 beats per minute is indicative of orthostatic hypotension 9.
The Dix-Hallpike maneuver (watch the Youtube video below) is diagnostic for benign paroxysmal positional vertigo (BPPV) if positive, but does not rule it out if negative. The maneuver is performed on a flat examination table. While the patient is in a seated position, the physician turns the patient’s head 45 degrees to one side, then rapidly lays the patient into a supine position with the head hanging about 20 degrees over the end of the table and observes the patient’s eyes for approximately 30 seconds. The maneuver is repeated with the head turned to the opposite side. Nystagmus is diagnostic of vestibular debris in the ear that is facing down, closest to the examination table. There is usually a latent period of a few seconds before the patient develops nystagmus, and a sensation of vertigo for up to one minute 10. The sensitivity of the Dix-Hallpike maneuver is 50 to 88 percent for BPPV 11.
Lesions of the labyrinth and cranial nerve VIII (vestibulocochlear) commonly produce spontaneous nystagmus. Saccadic eye movements associated with a patient’s smooth ocular pursuit of the physician’s finger as it moves slowly left, right, up, and down may be associated with a central cause, such as brainstem or cerebellar disease. The head impulse test involves asking the patient to remain focused on a target while the physician moves the patient’s head back and forth rapidly. Eye movement to one side with a refixation saccade (rapid oscillatory eye movement that occurs as the eye fixes on an object) is indicative of a lesion on the side to which the eyes move. Bilateral refixation movements commonly occur with ototoxicity. Another test that can elicit nystagmus involves the patient leaning forward 30 degrees while the physician shakes the patient’s head back and forth vigorously for 20 seconds. The presence of nystagmus indicates a peripheral cause in the ipsilateral direction of the nystagmus 10.
Other physical examination tests include the Romberg test and observation of gait (watch Youtube video below). Swaying toward one side with the Romberg test is indicative of vestibular dysfunction in the ipsilateral side. Also, a patient’s gait will lean toward the side of a vestibular lesion. Ataxia is indicative of cerebellar dysfunction, and the patient’s gait is usually slow, wide-based, and irregular 10. Observation of gait is also important to detect symptoms suggestive of parkinsonism in patients presenting with disequilibrium 12. In early Parkinson disease, gait is usually slower with smaller steps and reduced arm swing, and progresses to freezing and hesitation in later stages of the disease 13. Screening for peripheral neuropathy is also important in patients presenting with disequilibrium 12.
If hyperventilation syndrome is suspected, the diagnosis can be confirmed by having the patient rapidly take 20 deep inhalations and exhalations, in an attempt to reproduce symptoms 10.
A thorough cardiovascular examination should be performed in all patients with dizziness. However, tests such as electrocardiography, Holter monitor testing, and carotid Doppler testing should be performed only if an underlying cardiac cause is suspected based on other findings or known cardiac disease 11.
Additional testing
In general, laboratory testing and radiography are not beneficial in the work-up of patients with lightheadedness when no other neurologic abnormalities are present 14. Laboratory studies, including complete blood count (CBC), metabolic panels, and thyroid function tests, have very low yield in diagnosing a cause of dizziness. In one meta-analysis, only 26 of 4,538 patients (0.6 percent) had laboratory abnormalities that explained their dizziness 11.
Electronystagmography tests vestibular function by using electrodes to detect nystagmus. The test has a reported sensitivity of 69 to 74 percent and specificity of 81 to 83 percent for peripheral vestibular disorders. For central vestibular disorders, sensitivity has been reported as high as 81 percent and specificity as high as 93 percent 11.
Lightheadedness treatment
Home remedy
- Lie down for 1 or 2 minutes when you feel lightheaded. After lying down, sit up slowly and remain sitting for 1 to 2 minutes before slowly standing up.
- Avoid movements, positions, or activities that have made you light-headed in the past.
- Get plenty of rest, especially if you have a cold or flu, which can cause lightheadedness.
- Make sure you drink plenty of fluids, especially if you have a fever or have been sweating.
- Do not drive or put yourself and others in danger while you feel light-headed.
Table 2 summarizes the treatment of selected causes of lightheadedness and Youtube video below illustrates the Epley maneuver, an effective treatment for BPPV 15.
Table 2. Treatment for Selected Causes of Dizziness
| Cause | Treatment | Comments |
|---|---|---|
Vertigo | ||
Benign paroxysmal positional vertigo | Meclizine (Antivert), 25 to 50 mg orally every four to six hours | Commonly used to reduce symptoms of acute episodes of vertigo, although there are no randomized controlled trials to support its use; use of vestibular suppressants can lead to brainstem compensation and prolong vertiginous symptoms |
Epley maneuver (canalith repositioning) | Main benign paroxysmal positional vertigo treatment; safe and effective compared with placebo | |
Vestibular rehabilitation | Series of head and neck exercises that can be performed daily at home; video demonstration available below. | |
Evidence for balance therapy (e.g., tai chi, Wii Fit) is accumulating | ||
Meniere disease | Salt restriction (less than 1 to 2 g of sodium per day) and/or diuretics (most commonly, hydrochlorothiazide/triamterene [Dyazide]) | No large-scale randomized controlled trials to support these therapies |
Intratympanic dexamethasone or gentamicin | Referral to an otolaryngologist required; in one small study, dexamethasone resolved symptoms in 82 percent of patients; in a larger study, gentamicin resolved symptoms in 80.7 percent of patients 16 | |
Endolymphatic sac surgery | Referral to an otolaryngologist required | |
Vestibular neuritis | Methylprednisolone (Depo-Medrol), initially 100 mg orally daily then tapered to 10 mg orally daily over three weeks | In a randomized controlled trial, methylprednisolone was more effective in improving peripheral vestibular function than valacyclovir (Valtrex) in patients with vestibular neuritis 17 |
Migrainous vertigo | Migraine prophylaxis with serotonin 5-HT1 receptor agonists (triptans) | Treatment based on expert opinion, not randomized controlled trials |
Presyncope | ||
Orthostatic hypotension | Review medication regimen | This is the first step, especially in older patients; rehydration (even increased water intake) can improve symptoms, especially in those with autonomic failure |
Midodrine (Proamatine) titrated up to 10 mg orally three times daily | Alpha-1 agonist metabolite; to avoid supine hypertension, the third dose should be given by 6 p.m.; should be used only in severely impaired patients; in placebo-controlled trials, midodrine was associated with increased standing blood pressures and fewer orthostatic symptoms compared with placebo 18 | |
Fludrocortisone, initially 0.1 mg orally daily, titrated up weekly until peripheral edema develops or to a maximal dosage | Mineralocorticoids, such as fludrocortisone, are used to increase sodium and water retention; monitor blood pressure, potassium level, and for symptoms of heart failure | |
Fludrocortisone and midodrine can be used in combination if either agent alone fails to control symptoms | ||
Pseudoephedrine, 30 to 60 mg orally daily Paroxetine (Paxil), 20 mg orally daily | These drugs are options when midodrine and fludrocortisone are ineffective | |
Desmopressin (DDAVP), 5 to 40 mcg intranasally daily | Nondrug therapy includes replacement of fluids, rising slowly from lying or sitting positions, sleeping with the head of the bed elevated, increasing salt intake, and regular exercise | |
Disequilibrium | Treatment of underlying cause (e.g., peripheral neuropathy, Parkinson disease) | Because disequilibrium is generally a symptom of an underlying condition, treatment of the condition improves symptoms of disequilibrium |
Lightheadedness | ||
Hyperventilation syndrome | Breathing control exercises, rebreathing into a small paper bag | Reverses hypocapnia-related symptoms |
Beta blockers | Treats associated symptoms, such as palpitations and sweating; not for use in patients with asthma | |
Antianxiety agents (e.g., selective serotonin reuptake inhibitors) or short-term use of benzodiazepines | For use in patients with underlying anxiety | |
- Wiltink J, Tschan R, Michal M, et al. Dizziness: anxiety, health care utilization and health behavior. J Psychosom Res. 2009;66(5):417–424
- Yardley L, Owen N, Nazareth I, et al. Panic disorder with agoraphobia associated with dizziness. J Nerv Ment Dis. 2001;189(5):321–327
- Teggi R, Caldirola D, Bondi S, et al. Vestibular testing in patients with panic disorder and chronic dizziness. Acta Otorhinolaryngol Ital. 2007;27(5):243–247
- Staab JP, Ruckenstein MJ. Expanding the differential diagnosis of chronic dizziness. Arch Otolaryngol Head Neck Surg. 2007;133(2):170–176
- Nagy E, Claussen CF, Bencze G, et al. Depressive disorders in relation to neurootological complaints. Int Tinnitus J. 2004;10(1):58–64
- Gardner WN. The pathophysiology of hyperventilation disorders. Chest. 1996;109(2):516–534.
- Gupta V, Lipsitz LA. Orthostatic hypotension in the elderly: diagnosis and treatment. Am J Med. 2007;120(10):841–847
- Dizziness: A Diagnostic Approach. Am Fam Physician. 2010 Aug 15;82(4):361-368. https://www.aafp.org/afp/2010/0815/p361.html
- McGee S, Abernethy WB III, Simel DL. The rational clinical examination. Is this patient hypovolemic? JAMA. 1999;281(11):1022–1029
- Goebel JA. The ten-minute examination of the dizzy patient. Semin Neurol. 2001;21(4):391–398
- Hoffman RM, Einstadter D, Kroenke K. Evaluating dizziness. Am J Med. 1999;107(5):468–478
- Kroenke K, Lucas CA, Rosenberg ML, et al. Causes of persistent dizziness. Ann Intern Med. 1992;117(11):898–904
- Ebersbach G, Sojer M, Valldeoriola F, et al. Comparative analysis of gait in Parkinson’s disease, cerebellar ataxia and subcortical arteriosclerotic encephalopathy. Brain. 1999;122(pt 7):1349–1355.
- Wasay M, Dubey N, Bakshi R. Dizziness and yield of emergency head CT scan: is it cost effective? Emerg Med J. 2005;22(4):312
- Hilton M, Pinder D. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo. Cochrane Database Syst Rev. 2004;(2):CD003162
- De Beer L, Stokroos R, Kingma H. Intratympanic gentamicin therapy for intractable Ménière’s disease. Acta Otolaryngol. 2007;127(6):605–612
- Strupp M, Zingler VC, Arbusow V, et al. Methylprednisolone, valacy-clovir, or the combination for vestibular neuritis. N Engl J Med. 2004;351(4):354–361
- Low PA, Gilden JL, Freeman R, et al. Efficacy of midodrine vs placebo in neurogenic orthostatic hypotension. [published correction appears in JAMA. 1997;278(5):388]. JAMA. 1997;277(13):1046–1051





{kind=link}