
Lumbar radiculopathy
Lumbar radiculopathy commonly called lumbosacral radiculopathy, is a term used to describe a pain syndrome caused by compression or irritation of lumbosacral nerve roots in your lower back or lumbar spine 1. Lumbosacral radiculopathy can be caused by lumbar disc herniation, degeneration of the spinal vertebra, and narrowing of the foramen from which the nerves exit the spinal canal. Lumbosacral radiculopathy symptoms include low back pain that radiates into the lower extremities in a dermatomal pattern. Other accompanying symptoms can include numbness, weakness, and loss of reflexes, although the absence of these symptoms does not exclude a diagnosis of lumbosacral radiculopathy 2.
Lumbar spine anatomy
The anatomy of the lumbar epidural space is the key to understanding the mechanism of lumbosacral radiculopathic pain. The sinuvertebral nerves innervate structures in the lumbar epidural space; these nerves originate distal to the dorsal root ganglion, then run back through the intervertebral foramen to supply the arteries, venous plexi, and lymphatics. At the inner aspect of the intervertebral foramen, the sinuvertebral nerves divide into ascending and descending branches that freely communicate with corresponding branches from the segment above, from the segment below, and from the opposite side.
The sinuvertebral nerve supplies the posterior longitudinal ligament, superficial annulus fibrosus, epidural blood vessels, anterior dura mater, dural sleeve, and posterior vertebral periosteum. The 2 structures capable of transmitting neuronal impulses that result in the experience of pain are the sinuvertebral nerve and the nerve root. The posterior rami of the spinal nerves supply the apophyseal joints above and below the nerve as well as the paraspinous muscles at multiple levels.
Herniation of the intervertebral disc can cause impingement of the above neuronal structures, thus causing pain. The presence of disc material in the epidural space is thought to initially result in direct toxic injury to the nerve root by chemical mediation and then exacerbation of the ensuing intraneural and extraneural swelling, which results in venous congestion and conduction block. Notably, the size of the disc herniation has not been found to be related to the severity of the patient’s pain.
Pain is also believed to be mediated by inflammatory mechanisms that involve substances such as phospholipase A2, nitric oxide, and prostaglandin E. These mediators are all found in the nucleus pulposus itself. Phospholipase A2 has been found in high concentrations in herniated lumbar discs; this substance acts on cell membranes to release arachidonic acid, a precursor to other prostaglandins and leukotrienes that further advance the inflammatory cascade. Additionally, leukotriene B4 and the substance thromboxane B2 have been found to have direct nociceptive stimulatory roles.
From a biomechanical standpoint, the lumbar intervertebral discs are highly susceptible to herniation because they are exposed to tremendous forces, principally by the magnification of the forces that result from the lever effect of the human arm in lifting; the forces generated by the upper trunk mechanics with rotation, flexion/extension, and side-bending on the discs below; and by the vertical forces associated with the upright position. Because each intervertebral disc is a fluid system, hydraulic pressure is generated whenever a load is placed on the axial skeleton. The hydraulic pressure mechanisms then multiply the force on the annulus fibrosus of the intervertebral disc to make it 3-5 times that which is exerted on the axial skeleton.
Figure 1. Spinal cord segments
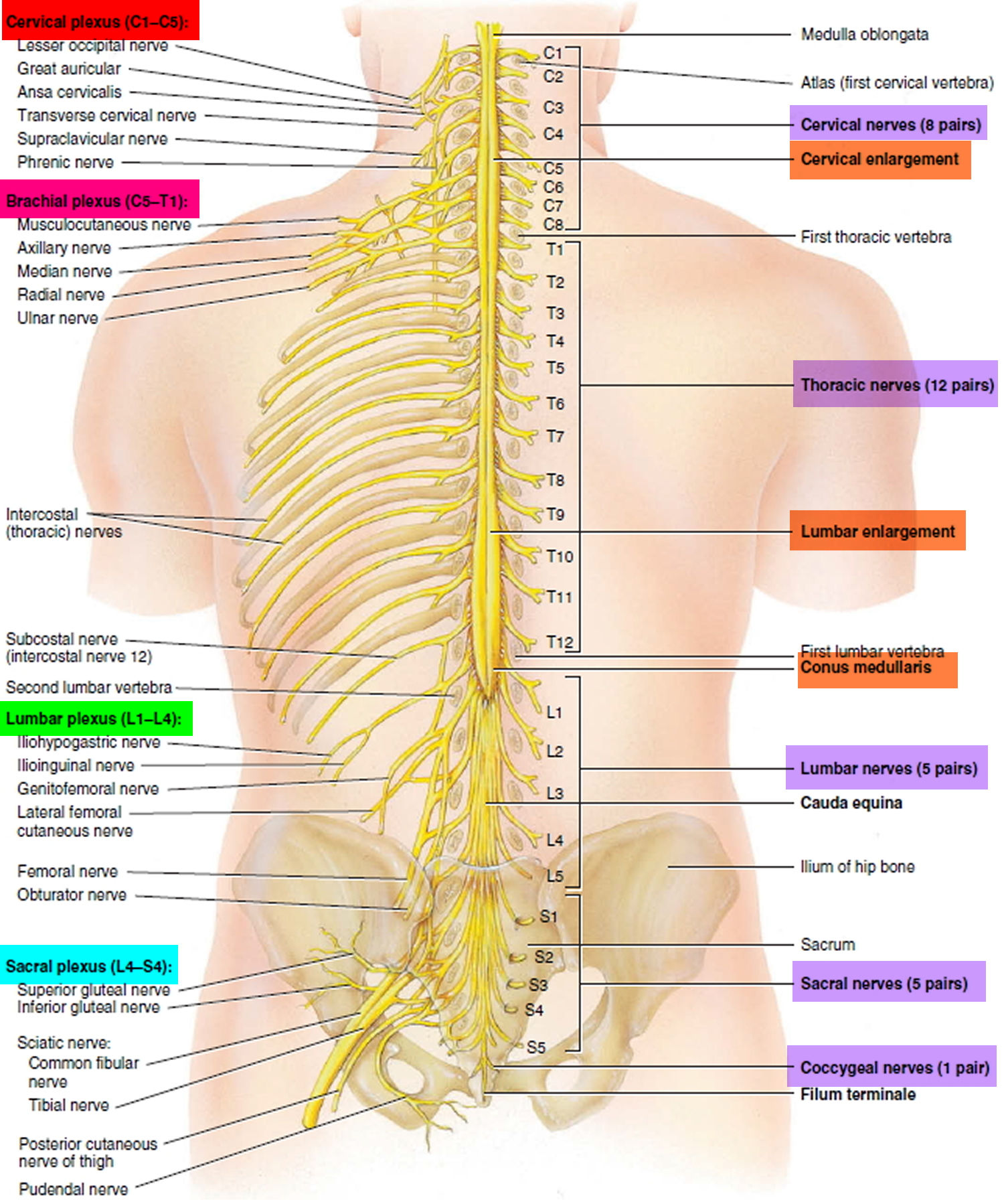
Figure 2. Herniated disc (the rubbery disks that lie between the vertebrae in your spine consist of a soft center (nucleus) surrounded by a tougher exterior (annulus). A herniated disk occurs when a portion of the nucleus pushes through a crack in the annulus. Symptoms may occur if the herniation compresses a nerve.)
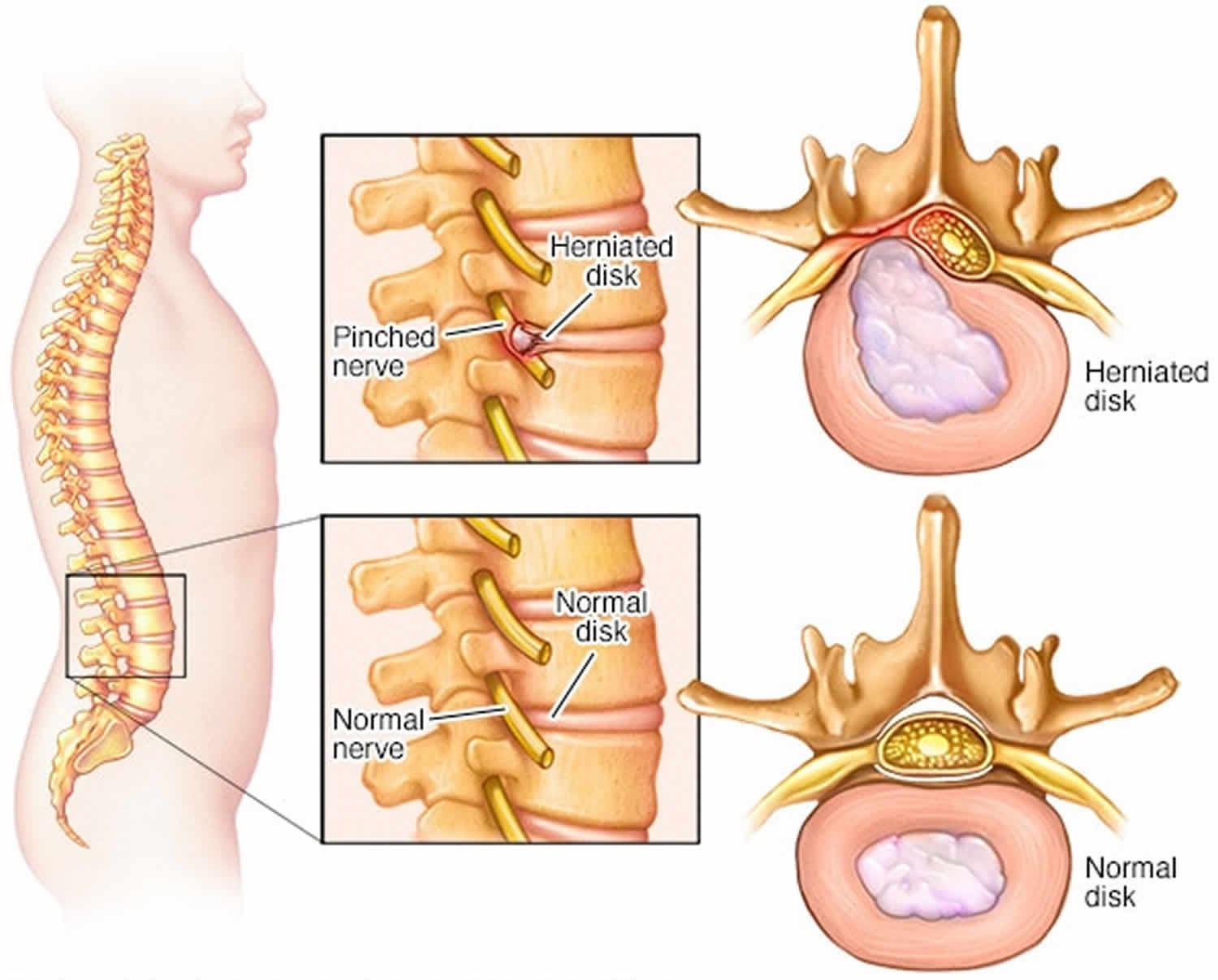
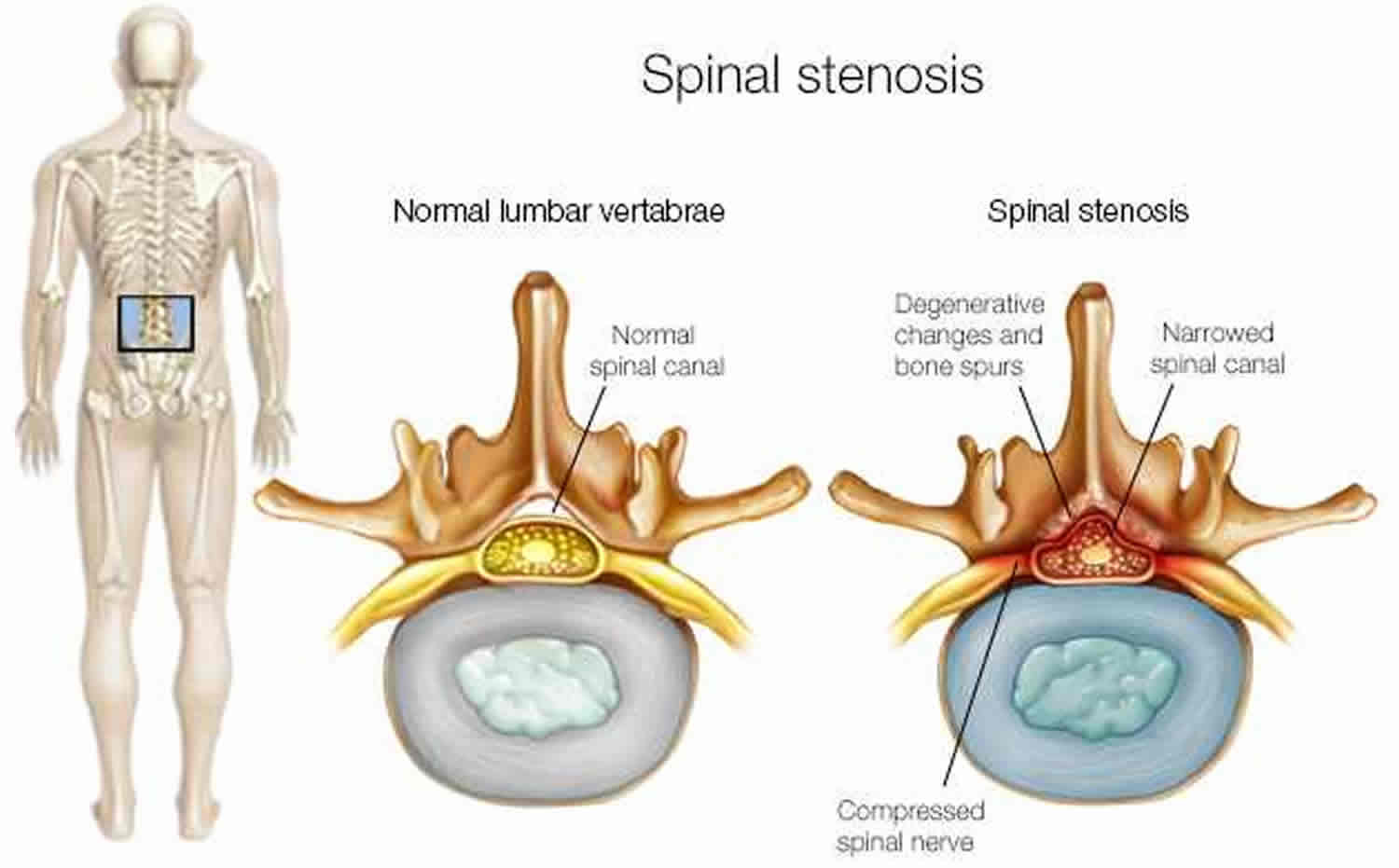
Figure 3. Spinal stenosis (spinal stenosis occurs when the space within the spinal canal or around the nerve roots becomes narrowed)
Lumbar radiculopathy causes
The noxious stimulus of a spinal nerve creates ectopic nerve signals that are perceived as pain, numbness, and tingling along the nerve distribution. Lesions of the intervertebral discs and degenerative disease of the spine are the most common causes of lumbosacral radiculopathy. However, any process that causes irritation of the spinal nerves can cause radicular symptoms. The differential diagnosis for lumbosacral radiculopathy should include (but is not limited to) the following:
Degenerative conditions of the spine (most common causes)
- Spondylolisthesis: in the degenerative setting, this occurs as a result of a pathologic cascade including intervertebral disc degeneration, ensuing intersegmental instability, and facet joint arthropathy
- Spinal stenosis
- Adult isthmic spondylolisthesis is typically caused by an acquired defect in the par interarticularis
- Pars defects (i.e. spondylolisis) in adults are most often secondary to repetitive microtrauma
Trauma (e.g. burst fractures with bony fragment retropulsion)
- Clinicians should recognize spinal fractures can occur in younger, healthy patient populations secondary to high-energy injuries (e.g. motor vehicle accident, fall from height) or secondary low energy injuries and spontaneous fractures in the elderly populations, including any patient with osteoporosis
- Associated hemorrhage from the injury can result in a deteriorating clinical and neurologic exam
Benign or malignant tumors
- Metastatic tumors (most common)
- Primary tumors
- Ependymoma
- Schwannoma
- Neurofibroma
- Lymphoma
- Lipomas
- Paraganglioma
- Ganglioneuroma
- Osteoblastoma
Infection
- Osteodiscitis
- Osteomyelitis
- Epidural abscess
- Fungal infections (e.g. Tuberculosis)
- Other infections: lyme disease, HIV/AIDS-defining ilnesses, Herpes zoster
Vascular conditions
- Hemangioblastoma, aterior-venous malformations (AVM) 3
Lumbar radiculopathy symptoms
Lumbosacral radiculopathy patients can present with radiating pain, numbness, weakness, tingling along the distribution supplied by the respective nerve root(s) and gait abnormalities across a spectrum of severity. Depending on the nerve root(s) affected, patients can present with these symptoms in predictable patterns affecting the corresponding dermatome or myotome 4.
Radicular pain is typically characterized by patients as “electrical shocks” or “shooting pains” that radiate from the buttock to the foot. While gathering the history, it is important to screen for any red-flag symptoms, which could indicate an urgent/emergent clinical condition. Evaluating clinicians must first rule out associated “red flag” symptoms including 1:
- Thoracic pain
- Fever/unexplained weight loss
- Night sweats
- Bowel or bladder dysfunction
- Malignancy (document/record any previous surgeries, chemo/radiation, recent scans and bloodwork, and history of metastatic disease)
- Can be seen in association with pain at night, pain at rest, unexplained weight loss, or night sweats
- Significant medical comorbidities
- Neurologic deficit or serial exam deterioration
- Gait ataxia
- Saddle anesthesia
- Age of onset (bimodal — Age < 20 years or Age > 55 years)
A full neurologic exam shoulder is performed, including an assessment for upper motor neuron findings (Babinski sign, clonus, spasticity). On physical exam, several maneuvers can assist the clinician in making a diagnosis. Lasègue test, or straight leg test, is performed by passively raising one leg into the air. This creates increased tension on the sciatic nerve between 30 degrees to 60 degrees from the exam table. A reproduction of the patient’s symptoms during passive movement between 30 degrees to 60 degrees is considered a positive sign and is suggestive of lower lumbar nerve root involvement (L4 to S1). Of note, a similar stretch can be created on the femoral nerve using a reverse straight leg, or Ely test. With this test, the patient’s symptoms are reproduced by extending the hip and flexing the knee with the patient in the prone position. This will stretch the femoral nerve and the L2 to L4 nerve roots. Reproduction of radicular symptoms can also be produced by placing the patient in a seated position with the neck in full flexion and knees in full extension (slump test) 5.
Lumbar radiculopathy diagnosis
As with any disease process, a thorough history and physical exam are crucial in diagnosing lumbosacral radiculopathy. Given the favorable outcome, and often spontaneous resolution of the vast majority of low back pain symptoms, extensive imaging is usually not necessary in patients with low back pain of less than four to six weeks duration. As stated above, work-up begins with a thorough physical exam. Neurologic deficits in a focal distribution warrant further workup. In cases of low back pain that fails to resolve within one to two months, MRI is considered the gold standard in evaluating radicular low back pain. Of note, MRI with contrast is recommended in patients with previous spinal surgeries. For patients unable to undergo MRI, CT scan is an alternative option. However, CT is not as sensitive in visualizing soft tissue or tumors and is not recommended for routine use. X-rays are simple, readily available in most developed countries, and can reveal gross bony abnormalities such as fractures, disc space narrowing, and other osteodegenerative changes. Often, it is not clinically possible to distinguish lumbosacral radiculopathy from peripheral neuropathy or plexopathy. In these instances, electromyography and nerve conduction study can be utilized to localize a lesion with relatively high diagnostic specificity 6.
Lumbar radiculopathy treatment
Lumbosacral radiculopathy treatment is varied depending on the cause and severity of symptoms 1. However, conservative management of symptoms is generally considered first line. Medications are used to manage pain symptoms including nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and in severe cases, opiates. Radicular symptoms are often treated with neuroleptic agents. Systemic steroids are often prescribed for acute low back pain, although there is limited evidence to support its use. Nonpharmacologic interventions are often utilized as well. Physical therapy, acupuncture, chiropractic manipulation, and traction are all commonly used in the treatment of lumbosacral radiculopathy. Of note, the data supporting the use of these treatment modalities is equivocal. Interventional techniques are also commonly used and include epidural steroid injections and percutaneous disc decompression. In refractory cases, surgical decompression and spinal fusion can be performed 7.
Physical therapy
A method that is commonly referred to as “back school” involves teaching the patient back-protection techniques (eg, proper lifting, posture awareness). A lumbar stabilization program is another useful method that physical therapists may incorporate for patients with low back pain 8. The patient is instructed in various techniques to control his or her back pain, and he or she also works on strengthening the stabilizing muscles of the lumbar spine. This is actually a combination of different techniques and may involve the McKenzie exercise program (a series of repetitive lumbar spine exercises for the management of low back pain).
Core strengthening is advocated by many rehabilitation specialists as a means of improving muscular control around the lumbar spine to maintain functional stability 9. The core muscles include the abdominals anteriorly, the paraspinals and gluteals posteriorly, the diaphragm as the roof, and the pelvic floor and hip girdle musculature as the floor. A typical program consists of a series of graded exercises that promote movement awareness and motor relearning in addition to strengthening.
Soft-tissue modalities are also usually incorporated into a back pain program. These modalities involve specific manual techniques, myofascial release, or massage to improve the soft-tissue component of a patient’s pain.
The use of lumbar traction has long been a preferred method of treating lumbar disc problems. Lumbar traction requires approximately 1.5 times the person’s body weight to develop distraction of the vertebral bodies. However, this method can be cumbersome and time consuming; furthermore, most individuals find lumbar traction difficult to tolerate.
Vertebral axial decompression is a relatively newer method that causes distraction of the vertebral bodies and probably represents a more technical version of traction. Currently, there is no evidence in the peer-reviewed literature to support this form of treatment. No significant difference in outcome has been demonstrated with traction relative to sham traction; however, greater morbidity has been demonstrated in the traction group. A limited amount of evidence supports its use. Given the effectiveness of more active treatments, traction is generally not recommended in the treatment of acute low back pain.
The above techniques may also be used during the recovery phase, with a lifelong home exercise program forming part of the maintenance phase.
Surgical intervention
Most sources agree on the urgent and definitive indications for surgical intervention in patients with lumbosacral radiculopathy (eg, significant/severe and progressive motor deficits, cauda equina syndrome with bowel and bladder dysfunction). The 5 surgical treatment options are as follows:
- Simple discectomy
- Discectomy plus fusion
- Chemonucleolysis
- Percutaneous discectomy
- Microdiscectomy
Ninety percent of patients who have surgery for lumbar disc herniation undergo discectomy alone, although the number of spinal fusion procedures has greatly increased 10. Additionally, the complication rate of simple discectomy is reported at less than 1%.
Other treatment
Epidural steroid injections are a modality that appears promising, despite a paucity of well-designed trials of their efficacy 11. A study by Abrams 12 reported that only 13 controlled, randomized trials had been published on the use of epidural steroid injections for back pain. Although some controversy exists in the literature, caudal epidural steroid or saline injections may be another treatment option for chronic lumbar radiculopathy. A multicenter, blinded, randomized controlled trial conducted in Norway assessed the efficacy of caudal epidural steroid or saline injections in chronic lumbar radiculopathy at 6 weeks, 12 weeks, and 52 weeks. All patients studied improved after treatment, but no statistical or clinical differences were noted over time 13.
Lutz et al 14 demonstrated an outcome success rate of 75.4% with the use of selective nerve blocks in conjunction with oral medications and physical therapy in patients who had a herniated lumbar nucleus pulposus and radiculopathy in whom conservative therapy had not yielded positive results. Other investigators also found similar benefits from the procedure. Although epidural steroid injections may be performed within months to years of symptom onset, with comparable symptomatic relief, the optimal time period is 6-9 months from onset. However, the growing consensus is that this treatment is most effective in acute cases (3-6 months post onset) 15.
In a review study, DePalma et al 16 found level 3 (moderate) evidence supporting the use of transforaminal epidural steroid injections in the treatment of lumbosacral radiculopathy. Six trials were analyzed in the review, and no significant complications were reported.
Chang-Chien et al 17 assessed studies that compared transforaminal epidural steroid injections and interlaminar epidural steroid injections for pain relief and functional improvement from lumbosacral radicular pain. The findings show that both transforaminal epidural steroid injections and interlaminar epidural steroid injections are effective in the short term (average 3 months) reducing pain and improving functional scores in unilateral lumbosacral radicular pain.
Moreover, a literature review by Liu et al 18 found no significant difference in the efficacy of transforaminal versus caudal epidural steroid injections for lumbosacral radicular pain.
In addition, in patients with chronic lumbosacral radicular pain who received transforaminal epidural steroid injections, a retrospective cohort study by McCormick et al 19 found no significant difference between particulate and nonparticulate steroids with regard to pain reduction at short- and intermediate-term follow-up or in the mean number of repeat injections given by intermediate-term follow-up.
In another report, Friedly et al 11 investigated trends of increasing lumbosacral injections (eg, epidural steroid injections, facet joint injections, sacroiliac joint injections, and related fluoroscopy) for low back pain from 1994-2000 in the Medicare population. The authors reviewed Medicare Part B claims data with use of Current Procedural Technology billing codes from the relevant period and found a 271% increase in lumbar epidural steroid injections, an increase from $24 million to $175 million of the total inflation-adjusted reimbursed costs for professionals, and almost a doubling of the costs per injection, from $115 to $227.
Most clinicians agree that image-guided transforaminal epidural injections are preferred to an interlaminar or caudal approach. This technique routinely delivers medication to the anterior epidural space.
Although most clinicians utilize a supraneural technique for transforaminal injections, the Kambin triangle approach offers a reasonable alternative which may provide similar outcomes 20. The Kambin triangle technique places the tip of the needle below the spinal nerve, as opposed to the traditional supraneural approach in which the needle is positioned above the nerve.
Saeidian et al 21 conducted a study to evaluate trigger point therapy on the outcome of pain in patients with lumbosacral radiculopathy. Results show that trigger point injection therapy in patients suffering from chronic lumbosacral radiculopathy with trigger points can significantly improve their pain for the short term (10 days).
References- Alexander CE, Varacallo M. Lumbosacral Radiculopathy. [Updated 2019 Mar 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430837
- Hoy D, Brooks P, Blyth F, Buchbinder R. The Epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010 Dec;24(6):769-81.
- Urits I, Burshtein A, Sharma M, Testa L, Gold PA, Orhurhu V, Viswanath O, Jones MR, Sidransky MA, Spektor B, Kaye AD. Low Back Pain, a Comprehensive Review: Pathophysiology, Diagnosis, and Treatment. Curr Pain Headache Rep. 2019 Mar 11;23(3):23.
- Tarulli AW, Raynor EM. Lumbosacral radiculopathy. Neurol Clin. 2007 May;25(2):387-405.
- Al Nezari NH, Schneiders AG, Hendrick PA. Neurological examination of the peripheral nervous system to diagnose lumbar spinal disc herniation with suspected radiculopathy: a systematic review and meta-analysis. Spine J. 2013 Jun;13(6):657-74.
- Nguyen HS, Doan N, Shabani S, Baisden J, Wolfla C, Paskoff G, Shender B, Stemper B. Upright magnetic resonance imaging of the lumbar spine: Back pain and radiculopathy. J Craniovertebr Junction Spine. 2016 Jan-Mar;7(1):31-7.
- Tang S, Mo Z, Zhang R. Acupuncture for lumbar disc herniation: a systematic review and meta-analysis. Acupunct Med. 2018 Apr;36(2):62-70.
- Barr KP, Griggs M, Cadby T. Lumbar stabilization: a review of core concepts and current literature, part 2. Am J Phys Med Rehabil. 2007 Jan. 86(1):72-80.
- Willardson JM. Core stability training: applications to sports conditioning programs. J Strength Cond Res. 2007 Aug. 21(3):979-85.
- Memmo PA, Nadler SF, Malanga GA. Lumbar disc herniation: a review of surgical and non-surgical indications and outcomes. J Back Musculoskelet Rehabil. 2000. 14(3):79-88.
- Friedly J, Chan L, Deyo R. Increases in lumbosacral injections in the Medicare population: 1994 to 2001. Spine. 2007 Jul 15. 32(16):1754-60.
- Abram SE. Treatment of lumbosacral radiculopathy with epidural steroids. Anesthesiology. 1999 Dec. 91(6):1937-41.
- Iversen T, Solberg TK, Romner B, et al. Effect of caudal epidural steroid or saline injection in chronic lumbar radiculopathy: multicentre, blinded, randomised controlled trial. BMJ. 2011 Sep 13. 343:d5278.
- Lutz GE, Vad VB, Wisneski RJ. Fluoroscopic transforaminal lumbar epidural steroids: an outcome study. Arch Phys Med Rehabil. 1998 Nov. 79(11):1362-6.
- Cyteval C, Fescquet N, Thomas E, et al. Predictive factors of efficacy of periradicular corticosteroid injections for lumbar radiculopathy. AJNR Am J Neuroradiol. 2006 May. 27(5):978-82.
- DePalma MJ, Bhargava A, Slipman CW. A critical appraisal of the evidence for selective nerve root injection in the treatment of lumbosacral radiculopathy. Arch Phys Med Rehabil. 2005 Jul. 86(7):1477-83.
- Chang-Chien GC, Knezevic NN, McCormick Z, Chu SK, Trescot AM, Candido KD. Transforaminal versus interlaminar approaches to epidural steroid injections: a systematic review of comparative studies for lumbosacral radicular pain. Pain Physician. 2014 Jul-Aug. 17(4):E509-24.
- Liu J, Zhou H, Lu L, et al. The Effectiveness of Transforaminal Versus Caudal Routes for Epidural Steroid Injections in Managing Lumbosacral Radicular Pain: A Systematic Review and Meta-Analysis. Medicine (Baltimore). 2016 May. 95 (18):e3373.
- McCormick ZL, Cushman D, Marshall B, et al. Pain Reduction and Repeat Injections After Transforaminal Epidural Injection With Particulate Versus Nonparticulate Steroid for the Treatment of Chronic Painful Lumbosacral Radiculopathy. PM R. 2016 Apr 6.
- Park KD, Lee J, Jee H, Park Y. Kambin Triangle Versus the Supraneural Approach for the Treatment of Lumbar Radicular Pain. Am J Phys Med Rehabil. 2012 Jul 30.
- Saeidian SR, Pipelzadeh MR, Rasras S, Zeinali M. Effect of trigger point injection on lumbosacral radiculopathy source. Anesth Pain Med. 2014 Oct. 4(4):e15500.





{kind=link}