
What is a mastectomy
A mastectomy is surgery to remove all breast tissue from a breast as a way to treat or prevent breast cancer in women and men. Mastectomy is often done when a woman cannot be treated with breast-conserving surgery (lumpectomy), which spares most of the breast. Mastectomy can also be done if a woman chooses mastectomy over breast-conserving surgery for personal reasons. Women at very high risk of getting a second cancer sometimes have a double mastectomy, the removal of both breasts. A mastectomy operation takes about 90 minutes, and most people go home the following day. It can take 4 to 6 weeks to recover from a mastectomy.
For those with early-stage breast cancer, a mastectomy may be one treatment option. Breast-conserving surgery (lumpectomy), in which only the tumor is removed from the breast, may be another option.
Deciding between a mastectomy and lumpectomy can be difficult. Both procedures are equally effective for preventing a recurrence of breast cancer. But a lumpectomy isn’t an option for everyone with breast cancer, and others prefer to undergo a mastectomy.
Newer mastectomy techniques can preserve breast skin and allow for a more natural breast appearance following the procedure. This is also known as skin-sparing mastectomy.
Breast reconstruction is surgery to make a new breast shape that looks like your other breast as much as possible — may be done at the same time as your mastectomy or during a second operation at a later date.
Breast reconstruction can be carried out at the same time as a mastectomy (immediate reconstruction), or it can be carried out later (delayed reconstruction).
Breast reconstruction can be done either by inserting a breast implant or by using tissue from another part of your body to create a new breast.
What you can expect
A mastectomy is an umbrella term used for several techniques to remove one or both breasts. In addition, the surgeon may also remove nearby lymph nodes to determine whether the cancer has spread.
During an axillary node dissection, the surgeon removes a number of lymph nodes from your armpit on the side of the tumor.
In a sentinel lymph node biopsy, your surgeon removes only the first few nodes into which a tumor drains (sentinel nodes).
Lymph nodes removed during a mastectomy are then tested for cancer. If no cancer is present, no further lymph nodes need be removed. If cancer is present, the surgeon will discuss options, such as radiation to your armpit. If this is what you decide to do, no further lymph nodes will need to be removed.
Removing all of the breast tissue and most of the lymph nodes is called a modified radical mastectomy. Newer mastectomy techniques remove less tissue and fewer lymph nodes.
Other types of mastectomy include:
- Total mastectomy. A total mastectomy, also known as a simple mastectomy, involves removal of the entire breast, including the breast tissue, areola and nipple. A sentinel lymph node biopsy may be done at the time of a total mastectomy.
- Skin-sparing mastectomy. A skin-sparing mastectomy involves removal of all the breast tissue, nipple and areola, but not the breast skin. A sentinel lymph node biopsy also may be done. Breast reconstruction can be performed immediately after the mastectomy. A skin-sparing mastectomy may not be suitable for larger tumors.
- Nipple-sparing mastectomy. A nipple- or areola-sparing mastectomy involves removal of only breast tissue, sparing the skin, nipple and areola. A sentinel lymph node biopsy also may be done. Breast reconstruction is performed immediately afterward.
What are lymph nodes?
Lymph nodes are small, oval-shaped balls that help remove bacteria and other waste from the body. If the cancer has spread to them, the lymph nodes under your arm will be removed during the operation.
If pre-surgery tests didn’t find cancer in your lymph nodes, a few may be removed during the operation for further testing. If these tests find cancer, you might need radiotherapy or another operation.
Some hospitals are able to test the lymph nodes while you’re being operated on, which reduces the need for a second operation.
What is lymph node surgery?
To find out if the cancer has spread, a procedure called a sentinel lymph node biopsy may be carried out.
The sentinel lymph nodes are the first lymph nodes that the cancer cells reach if they spread. They’re part of the lymph nodes under the arm (axillary lymph nodes).
The position of the sentinel lymph nodes varies, so they’re identified using a combination of a radioisotope and a blue dye.
The sentinel lymph nodes are examined in the laboratory to see if there are any cancer cells present. This provides a good indicator of whether the cancer has spread.
If there are cancer cells in the sentinel nodes, you may need further surgery to remove more lymph nodes from under the arm.
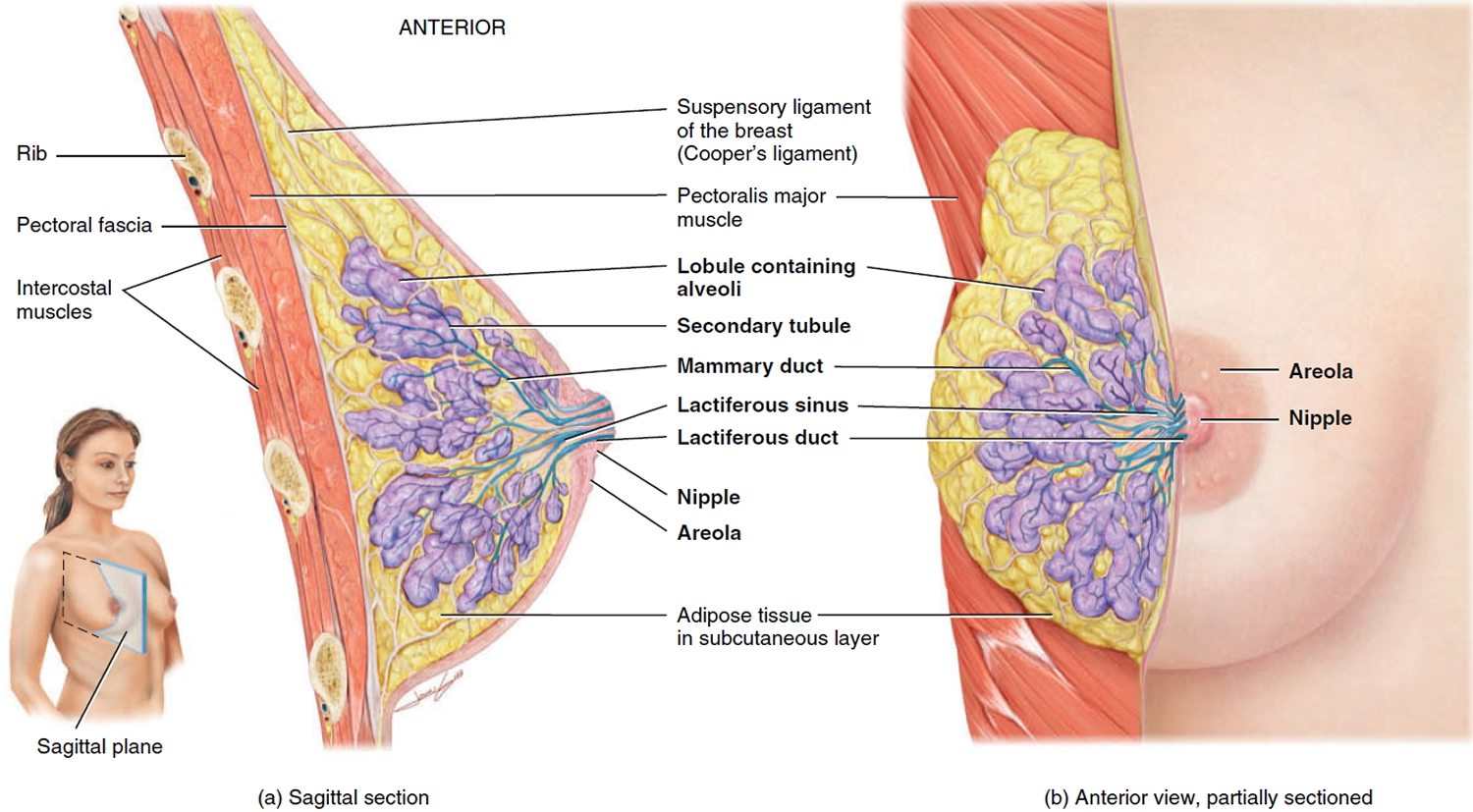
Figure 1. Normal breast (female)
What are reasons for having a mastectomy done?
A mastectomy is used to remove all breast tissue if you have breast cancer or are at very high risk of developing it. You may have a mastectomy to remove one breast (unilateral mastectomy) or both breasts (bilateral mastectomy).
Mastectomy for breast cancer treatment
A mastectomy may be a treatment option for many types of breast cancer, including:
- Ductal carcinoma in situ (DCIS), or noninvasive breast cancer
- Stages I and II (early-stage) breast cancer
- Stage III (locally advanced) breast cancer — after chemotherapy
- Inflammatory breast cancer — after chemotherapy
- Paget’s disease of the breast
- Locally recurrent breast cancer
Your doctor may recommend a mastectomy instead of a lumpectomy plus radiation if:
- You have two or more tumors in separate areas of the breast.
- You have widespread or malignant-appearing calcium deposits (microcalcifications) throughout the breast that have been determined to be cancer after a breast biopsy.
- You’ve previously had radiation treatment to the breast region and the breast cancer has recurred in the breast.
- You’re pregnant and radiation creates an unacceptable risk to your unborn child.
- You’ve had a lumpectomy, but cancer is still present at the edges (margin) of the operated area and there is concern about cancer extending to elsewhere in the breast.
- You carry a BRCA gene (BRCA1 and BRCA2 genes) mutation that gives you a high risk of developing a second cancer in your breast.
- You have a large tumor relative to the overall size of your breast. You may not have enough healthy tissue left after a lumpectomy to achieve an acceptable cosmetic result.
- You have a connective tissue disease, such as scleroderma or lupus, and may not tolerate the side effects of radiation to the skin.
Mastectomy to prevent breast cancer
You might also consider a prophylactic mastectomy if you don’t have breast cancer, but have a very high risk of developing the disease.
A prophylactic (preventive) mastectomy or risk-reducing mastectomy involves removing both of your breasts and significantly reduces your risk of developing breast cancer in the future.
A prophylactic mastectomy is reserved for those with a very high risk of breast cancer, which is determined by a strong family history of breast cancer or the presence of certain genetic mutations that increase the risk of breast cancer.
Who should get a mastectomy?
Many women with early-stage cancers can choose between breast-conserving surgery (lumpectomy) and mastectomy. You may have an initial gut preference for mastectomy as a way to “take it all out as quickly as possible.” But the fact is that in most cases, mastectomy does not give you any better chance of long-term survival or a better outcome from treatment. Studies following thousands of women for more than 20 years show that when breast-conserving surgery can be done with radiation, doing a mastectomy instead does not provide any better chance of survival.
Although most women and their doctors prefer breast-conserving surgery (with radiation therapy) when it’s a reasonable option, there are cases where mastectomy is likely to be the best choice. For example, mastectomy might be recommended if you:
- Are unable to have radiation therapy
- Would prefer a more extensive surgery instead of having radiation therapy
- Have had the breast treated with radiation therapy in the past
- Have already had breast-conserving surgery along with re-excision(s) that did not completely remove the cancer
- Have two or more areas of cancer in the same breast that are not close enough to be removed together without changing the look of the breast too much
- Have a larger tumor (greater than 5 cm [2 inches] across), or a tumor that is large relative to your breast size
- Are pregnant and would need radiation therapy while still pregnant (risking harm to the fetus)
- Have a genetic factor such as a BRCA (BRCA1 and BRCA2 genes) mutation, which might increase your chance of a second cancer
- Have a serious connective tissue disease such as scleroderma or lupus, which may make you especially sensitive to the side effects of radiation therapy
- Have inflammatory breast cancer
For women who are worried about breast cancer recurrence, it is important to understand that having a mastectomy instead of breast-conserving surgery plus radiation only lowers your risk of developing a second breast cancer in the same breast. It does not lower the chance of the cancer coming back in other parts of the body.
Will more treatment be needed after mastectomy?
Some women might get other treatments after a mastectomy, such as radiation therapy, hormone therapy, chemotherapy, or targeted therapy. Talk to your doctor about what to expect.
What is breast-conserving surgery?
Breast-conserving surgery ranges from a lumpectomy or wide local excision, where just the tumor and a little surrounding breast tissue is removed, to a partial mastectomy or quadrantectomy, where up to a quarter of the breast is removed.
If you have breast-conserving surgery, the amount of breast tissue you have removed will depend on:
- the type of cancer you have
- the size of the tumor and where it is in your breast
- the amount of surrounding tissue that needs to be removed
- the size of your breasts
Your surgeon will always remove an area of healthy breast tissue around the cancer, which will be tested for traces of cancer.
If there’s no cancer present in the healthy tissue, there’s less chance that the cancer will return.
If cancer cells are found in the surrounding tissue, more tissue may need to be removed from your breast.
After having breast-conserving surgery, you’ll usually be offered radiotherapy to destroy any remaining cancer cells.
Types of mastectomy
There are several different types of mastectomies, based on how the surgery is done and how much tissue is removed.
Simple (or total) mastectomy
In this procedure, the surgeon removes the entire breast, including the nipple, areola, and skin. Some underarm lymph nodes may or may not be removed depending on the situation. Most women, if they are hospitalized, can go home the next day.
Skin-sparing mastectomy
In this procedure, most of the skin over the breast is left intact. Only the breast tissue, nipple and areola are removed. The amount of breast tissue removed is the same as with a simple mastectomy. Implants or tissue from other parts of the body are used at the time of surgery to reconstruct the breast.
Many women prefer skin-sparing mastectomy because it offers the advantage of less scar tissue and a reconstructed breast that seems more natural. But it may not be suitable for larger tumors or those that are close to the surface of the skin.
The risk of local cancer recurrence with this type of mastectomy is the same as with other types of mastectomies.
Nipple-sparing mastectomy
Nipple-sparing mastectomy also called subcutaneous mastectomy, is a variation of the skin-sparing mastectomy. In this procedure, the breast tissue is removed, but the breast skin and nipple are left in place. This can be followed by breast reconstruction. The surgeon often removes the breast tissue beneath the nipple (and areola) during the procedure to check for cancer cells. If cancer is found in this tissue, the nipple must be removed. Even if no cancer is found under the nipple, some doctors give the nipple tissue a dose of radiation during or after the surgery to try to reduce the risk of the cancer coming back.
It is more often an option for women who have a small, early-stage cancer near the outer part of the breast, with no signs of cancer in the skin or near the nipple. Cancer cells are more likely to be hidden in the nipple if the breast tumor is larger or close to the nipple. This means there is a higher risk the cancer will come back if the nipple is not removed.
There are still some issues with nipple-sparing surgeries. Afterward, the nipple may not have a good blood supply, causing the tissue to shrink or become deformed. Because the nerves are also cut, there often may be little or no feeling left in the nipple. For women with larger breasts, the nipple may look out of place after the breast is reconstructed. As a result, many doctors feel that this surgery is best done in women with small to medium sized breasts. This procedure leaves less visible scars, but if it isn’t done properly, it can leave behind more breast tissue than other forms of mastectomy. This could result in a higher risk of cancer developing than for a skin-sparing or simple mastectomy. This was more of a problem in the past, but improvements in technique have helped make this surgery safer. Still, many experts do not yet consider nipple-sparing mastectomy to be a standard treatment for breast cancer.
Radical mastectomy
In this extensive operation, the surgeon removes the entire breast, axillary (underarm) lymph nodes, and the pectoral (chest wall) muscles under the breast. This surgery was once very common, but less extensive surgery (such as the modified radical mastectomy) has been found to be just as effective and with fewer side effects, so this surgery is rarely done now. Radical mastectomy may still be done for large tumors that are growing into the pectoral muscles.
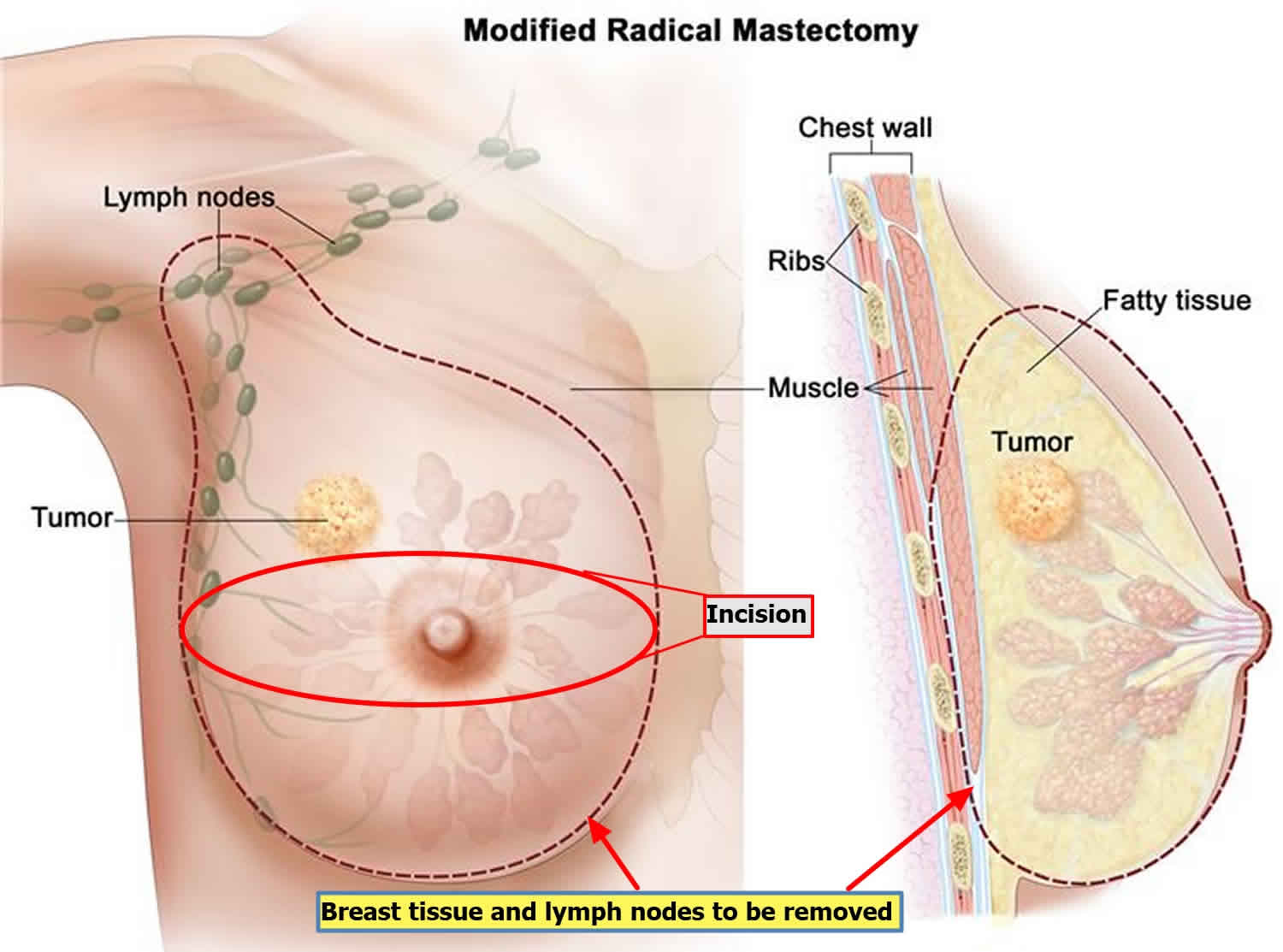
Modified radical mastectomy
A modified radical mastectomy combines a simple mastectomy with the removal of the lymph nodes under the arm (called an axillary lymph node dissection).
Figure 2. Modified radical mastectomy
Double mastectomy
If a mastectomy is done on both breasts, it is called a double (or bilateral) mastectomy. When this is done, it is often a risk-reducing surgery for women at very high risk for getting breast cancer, such as those with a BRCA gene (BRCA1 and BRCA2 genes) mutation. Most of these mastectomies are simple mastectomies, but some may be nipple-sparing.
Prophylactic mastectomy
Prophylactic mastectomy also known as preventive mastectomy, may reduce your risk of breast cancer.
Finding out you’re at high risk of breast cancer leads to difficult questions and decisions.
One such question is whether to have preventive mastectomy (prophylactic mastectomy) — surgery to remove one or both breasts in hopes of preventing or reducing your risk of breast cancer.
Keep in mind that being identified as high risk doesn’t mean you’re certain to get breast cancer. All it means is that your likelihood of developing the disease is several times higher than that of an average-risk woman.
Understanding your individual level of risk can help you weigh your options for risk-reducing strategies, including prophylactic mastectomy.
Who may consider prophylactic mastectomy to reduce breast cancer risk?
All women are at risk of breast cancer just by being female and advancing in age. But some factors increase your risk significantly.
You may consider prophylactic mastectomy if you have:
- Already had cancer in one breast. If you need to have one breast removed because of a new cancer diagnosis, and you have a very high risk of cancer in the other breast, based on a strong family history or a genetic test, you may decide to have the other, unaffected breast removed at the same time. This prophylactic mastectomy reduces the possibility of another breast cancer in your lifetime, but doesn’t completely eliminate the risk.
- A family history of breast cancer. If your mother, sister or daughter has had breast cancer, especially if she was diagnosed before age 50, you may be at increased risk. If you have multiple family members — on your mother’s or father’s side — with breast or ovarian cancer, your risk of breast cancer may be greater.
- Positive results from gene testing. Genetic testing can identify mutations in genes, such as BRCA1 and BRCA2, that substantially increase your risk of breast or other cancers. If you have a strong family history of breast cancer, consider meeting with a genetic counselor to discuss genetic testing. Women who are of Ashkenazi Jewish descent have a higher incidence of the BRCA1 and BRCA2 mutations.
- Breast changes that significantly increase your risk of cancer. Your doctor may have discovered abnormal cells in the milk-producing glands of your breast, a condition known as lobular carcinoma in situ (LCIS). Lobular carcinoma in situ isn’t cancer, but it’s a marker of an increased risk of developing cancer in both breasts. If you have a strong family history of breast cancer and a personal history of lobular carcinoma in situ (LCIS), chemoprevention or prophylactic mastectomy may be options to manage your risk.
- Radiation therapy. If you had radiation therapy to your chest between the ages of 10 and 30, you have an increased risk of developing breast cancer.
- Dense breasts. Dense breast tissue is associated with breast cancer. Dense breast tissue also makes it harder for doctors to diagnose breast cancer. A woman with dense breasts may consider a prophylactic mastectomy, especially if she has other risk factors, such as a strong family history of breast cancer or precancerous conditions.
Your doctor determines whether you’re at high risk of breast cancer based on your risk factors.
With whom should high-risk women discuss their options?
Deciding what to do with the knowledge that you are at high risk of breast cancer is a complex and time-consuming process. It’s best if you can work with a team of health professionals to get a complete evaluation of your risk and take the time to understand all of your options.
Many breast centers are staffed with breast-health specialists, genetic counselors, breast surgeons and reconstructive surgeons who can collaborate with you. Second opinions are strongly recommended for women considering prophylactic mastectomy.
Making the decision whether to have prophylactic mastectomy is not urgent. Give yourself time to weigh all the pros and cons. You may want to discuss your concerns and feelings with a breast-health specialist and psychologist.
How much does prophylactic mastectomy reduce the risk of breast cancer?
Prophylactic mastectomy can reduce the chances of developing breast cancer in women at high risk of the disease:
- For women with the BRCA1 or BRCA2 mutation, prophylactic mastectomy reduces the risk of developing breast cancer by up to 90 percent.
- For women who have already had breast cancer and also have a family history of the disease, prophylactic mastectomy can reduce the risk of developing cancer in the other breast by 90 to 95 percent.
However, studies indicate that prophylactic mastectomy has little or no effect on survival for women who have had breast cancer in one breast but who don’t have a strong family history of cancer or a genetic mutation. For these women with an average risk, prophylactic mastectomy may increase the risks of surgical complications without offering additional benefits, such as longer overall survival.
Having a prophylactic mastectomy doesn’t guarantee that you’ll never develop breast cancer because all of your breast tissue can’t be removed during the surgery. Sometimes breast tissue can be found in your chest, armpit or skin, above your collarbone, or on the upper part of your abdominal wall.
It is impossible for a surgeon to remove all of this breast tissue. Although the chances are slim, breast tissue remaining in your body can still develop breast cancer.
What are the risks of having prophylactic mastectomy?
As with any surgery, prophylactic mastectomy has potential complications, including:
- Bleeding
- Infection
- Pain
- Anxiety or disappointment about changes to your appearance
- Complications arising from breast reconstruction
- The need for multiple operations
Are there other options for reducing the risk of breast cancer?
If you’re at high risk of breast cancer and you decide against prophylactic mastectomy, you have other options for early detection and risk reduction.
Medications
Estrogens are hormones produced in your body that can promote breast cancer development and growth. Medications that block the effects of estrogen or reduce estrogen production in your body can reduce your risk of breast cancer. The options include:
- Tamoxifen, for premenopausal or postmenopausal women
- Raloxifene (Evista), for postmenopausal women
- Exemestane (Aromasin), for postmenopausal women
- Anastrozole (Arimidex), for postmenopausal women
Although these medications can reduce the risk of invasive breast cancer by about 50 percent, they carry a risk of side effects. Discuss the risks and benefits of these medications with your doctor and together you can decide whether medication is right for you.
Other options
Other options for early detection and risk reduction include:
- Breast cancer screening. Your doctor may suggest mammogram and magnetic resonance imaging (MRI) every year. Screening should also involve an annual clinical breast exam by your doctor and breast-awareness education to familiarize you with normal consistency of your breast tissue.
- Surgery to remove the ovaries (prophylactic oophorectomy). This procedure can reduce the risk of both breast and ovarian cancers. In women at high risk of breast cancer, prophylactic oophorectomy may reduce that risk by up to 50 percent if the procedure is done before age 50, when women are premenopausal.
- Healthy lifestyle. Maintaining a healthy weight, exercising most days of the week, limiting alcohol use and avoiding hormone therapy during menopause may reduce the risk of breast cancer. However, there aren’t yet any conclusive studies showing that specific dietary changes reduce the risk of breast cancer.
Mastectomy recovery
In general, women having a mastectomy stay in the hospital for 1 or 2 nights and then go home. However, some women may be placed in a 23-hour, short-stay observation unit before going home.
Most people who have a mastectomy recover well. You may wake up with:
- a drip in your arm so you can be given fluids
- one or more drainage tubes coming from the wound
- a dressing to help keep your wound clean
You will probably feel sore for a few days and should be given painkillers in hospital. If they don’t work, tell the nursing staff before you leave so you can try something else.
Most people find their wounds take around 2 to 3 weeks to heal, but it may be several months before your chest and arm area fully recover.
The area will be bruised, swollen and stiff at first. You may also have:
- painless swelling around your stitches (seroma) – this usually disappears without treatment after several weeks
- numbness where your lymph nodes were removed – this should improve with time
Mastectomy recovery time
How long it takes to recover from surgery depends on what procedures were done, and some women may need help at home. It can take 4 to 6 weeks to recover from a mastectomy. Most women should be fairly functional after going home and can often return to their regular activities within about 4 weeks. Recovery time is longer if breast reconstruction was done as well, and it can take months to return to full activity after some procedures.
Scar
The scar from a mastectomy will extend across the skin of the chest and into the armpit, usually hidden by the bra cup. It will fade over time but never completely disappear. It will also feel permanently numb.
If you don’t like the look of your scar, you may be able to have some corrective surgery.
A number of treatments are available if you have a scar that’s painful, itchy or unsightly, or if it restricts your movement.
Scars can’t be removed completely, but they can often be made less visible.
Some scar treatments are:
Skin camouflage (make-up)
You can buy make-up that’s specially designed for covering scars from pharmacies. Fully trained skin camouflage practitioners will be able to find a good color match for your skin tone and teach you how to apply the make-up. It’s waterproof and can stay in place for two or three days.
Silicone gels or sheets
Silicone gels or sheets can be used on healing skin (not open wounds) to help soften and flatten a scar. They can also relieve itching and discomfort.
To be effective, silicone gels or sheets should be placed over the scar for 12 hours a day for at least three months. They can be washed and reused.
Ask your doctor, dermatologist or pharmacist if they can recommend a suitable silicone-based scar treatment for you.
Steroids
Steroids can’t remove scars completely, but they can improve their appearance. Corticosteroid injections can be used to treat some keloid and hypertrophic scars.
The scar is injected a number of times to reduce any swelling and flatten it. Depending on the type of scar, the injections may need to be repeated.
Injections are usually given on three occasions, four to six weeks apart, to assess your body’s response. Treatment may continue for several months if the scar is improving.
Steroid-impregnated tape can also be used to try to flatten keloid scars. It can be prescribed by a doctor or dermatologist and is applied for 12 hours a day.
Laser therapy
Laser or light therapy (pulses of light) can reduce the redness in a scar by targeting the blood vessels in the excess scar tissue.
For some pitted scars, laser surgery (laser resurfacing) is used to try to make the scar flatter. This involves using a laser to remove the top layers of skin, which stimulates collagen production in the deeper layers.
But there aren’t many long-term studies to prove the effectiveness and safety of laser therapy. If you have laser therapy, make sure the person doing it is a fully trained medical practitioner with experience in improving scars.
Cryotherapy
Liquid nitrogen can be used to freeze keloid scars. If cryotherapy is used in the early stages, it may flatten keloid scars and stop them growing. A side effect of treatment is that it can lighten the colour of the skin in the area being treated.
Dermal fillers
Dermal fillers are injections (often of a man-made acid) used to “plump up” pitted scars. Treatments can be costly and the results are usually temporary. Repeat treatments are needed to maintain the effect.
Skin needling
Skin needling, which involves rolling a small device covered in hundreds of tiny needles across the skin, can also help improve the appearance of scars. But repeat treatments are often needed to achieve an effect, and results vary considerably.
Surgery
Surgery can sometimes be used to improve a scar by:
- making it appear more natural
- making it less noticeable (by using a skin graft)
- releasing a tight scar that’s close to a joint to improve movement
Scar reduction surgery is an invasive treatment that may not be suitable for everyone.
You should carefully consider the pros and cons before deciding to have surgery. As well as the normal risks of surgery, there’s also a chance of making the scar worse.
If you’re considering scar reduction surgery, make sure the plastic surgeon is fully trained and experienced in this type of surgery. You should fully discuss the procedure with your surgeon so you’re aware of the risks and expected results.
If surgery is used to treat a keloid scar, you may also need other treatments immediately after surgery, such as steroid injections or radiotherapy, to stop the scar growing back larger.
Pressure dressings
Pressure dressings are usually used under specialist supervision for treating large burn scars or after skin grafts. The aim is to flatten and soften the scars.
Pressure dressings are usually made from a stretchy, elastic material. They’re worn over the scar 24 hours a day for around 6 to 12 months. They can also be used with silicone gel sheeting to improve the appearance of scars over a long period of time.
Scars and skin creams
Vitamin E cream is sometimes recommended for managing scars, but there’s no medical evidence to suggest it has an effect.
But massaging a moisturizer like E45 into the scar will stop it becoming dry and help make it supple.
You should also apply sunscreen to your scar as it may be particularly sensitive to the sun.
Going home
Most people go home the day after their operation, although some feel well enough to go home on the same day.
If you’ve had breast reconstruction, you may need to stay in hospital for up to a week depending on how you’re recovering.
Before you leave hospital, your doctor or nurse will talk to you about what to do when you get home. You’ll probably feel more tired than usual for several weeks and will need a lot of rest, so try not to do too much.
The results of the operation and any further treatment will be discussed at a follow-up appointment around 2 weeks after the operation.
Arm exercises
Arm exercises are recommended to encourage the full range of movement back to your arm and shoulder. You can do gentle exercise as soon as you feel comfortable, usually around 3 to 4 weeks after surgery. Avoid more strenuous exercise, including housework and heavy lifting, until you get the all-clear from your doctor or nurse.
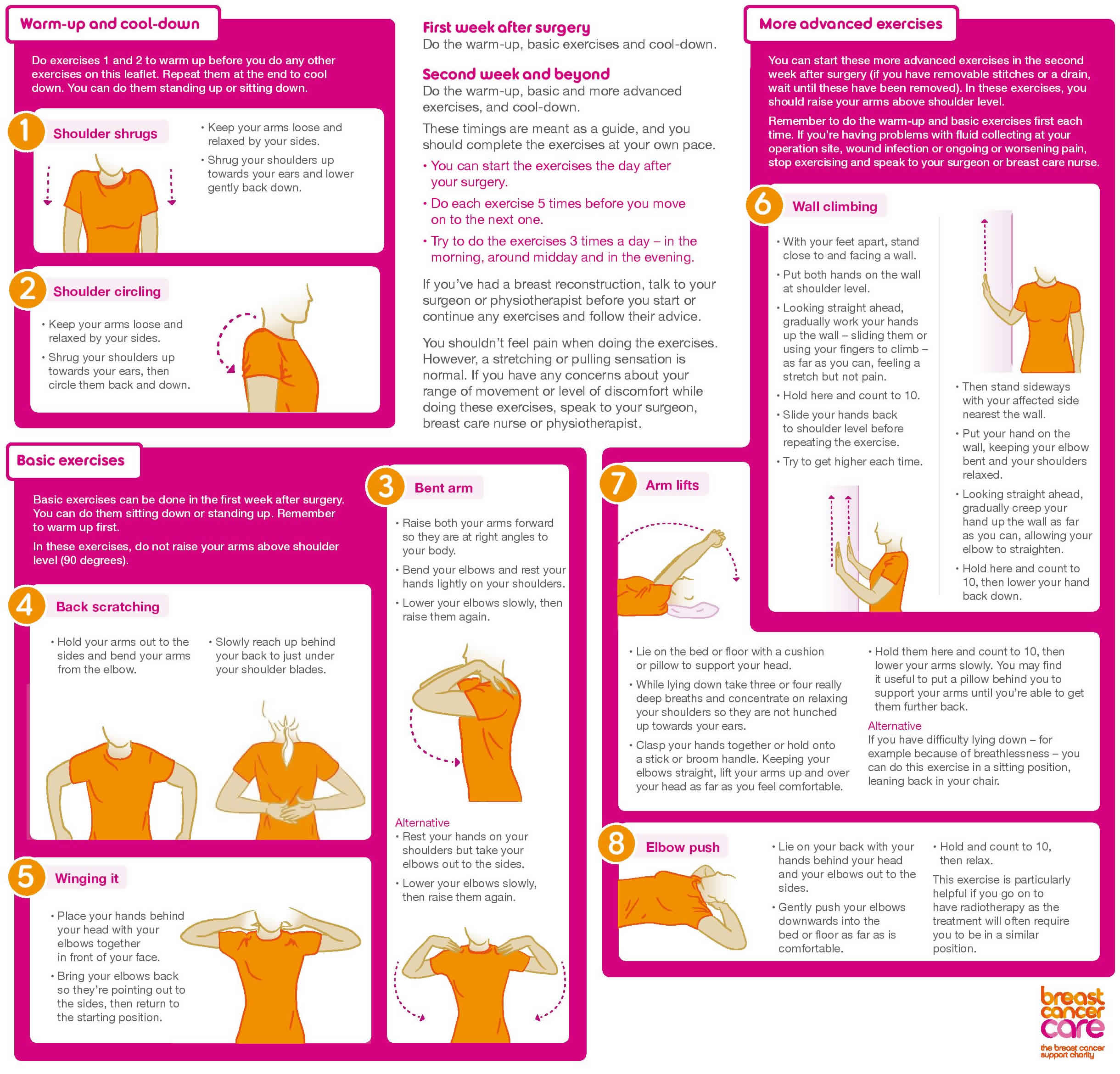
Figure 3. Post mastectomy arm exercises
Why do the arm exercises?
These exercises aim to help you regain arm and shoulder movement after surgery for breast cancer. They have been devised with the help of breast surgeons, breast care nurses and physiotherapists.
The arm exercises are suitable for people who have had:
- breast surgery
- lymph node removal
- radiotherapy.
The arm exercises can help you:
- get back the range of movement and function you had before surgery
- improve symptoms of tight scars and cording – when you feel as if you have a tight cord running from the armpit to your elbow in your affected arm, or sometimes down the whole length of the arm
- prevent long-term problems with arm and shoulder movement, posture and stiffness
- reduce the risk of lymphedema – swelling caused by a build-up of lymph fluid.
If you’re worried about any of these, or have symptoms of cording, speak to your breast care nurse.
When should I start the arm exercises?
Start the arm exercises as soon as you can, ideally the day after your surgery.
- In the first week after your surgery, you can start the warm-up and basic exercises.
- In the second week, you can do the more advanced exercises as well (if you have removable stitches or a drain, wait until these have been removed).
These timings are meant as a guideline only. Complete the exercises at your own pace.
How much exercise should I do?
- You should do the exercises every day.
- Do each exercise 5 times before you move on to the next one.
- Try to do the exercises 3 times a day – in the morning, around midday and in the evening.
- Don’t worry if you can’t manage to do all the exercises every time. For example, during radiotherapy you may find the exercises more difficult.
- Do as much as you feel able to at a pace you’re comfortable with.
How long should I do the exercises for?
Muscles seize up very quickly if they’re not used, so it’s important to do these exercises as part of your daily routine.
Arm stiffness or weakness can occur long after surgery and following radiotherapy. If you’ve just had surgery, keep doing the exercises until you have got back the range of movement you had before your operation. Continue doing the exercises if you’re going on to have radiotherapy as they will help your shoulder flexibility.
If you’ve had radiotherapy, it’s a good idea to do the exercises for as long as you’re still experiencing tightness and stiffness, and you may want to continue doing them after this.
Talk to your breast care nurse or physiotherapist if you’re not sure how long to keep up the exercise programme or if you have any concerns about your recovery after surgery.
Bra inserts
Before leaving hospital, you’ll have the opportunity to be fitted with a lightweight breast shape (prosthesis) to wear inside your bra.
You’ll usually be fitted with a longer-term prosthesis and given advice on bra fitting 6 to 8 weeks after the operation.
Driving
Get advice from your doctor or nurse about when to start driving. Generally, you should be OK to drive if you can make an emergency stop without discomfort in the wound.
Some people are able to drive about 3 weeks after the operation, but it may be sooner or later than this depending on how you feel.
Some insurance companies will not insure drivers for a number of weeks after surgery, so you may want to check your policy.
Returning to work
You can return to work when you feel up to it. Taking 4 to 8 weeks off is fairly typical, but it varies from person to person.
The hospital staff or your doctor can supply you with a medical note for your employer if needed.
Emotional support
Recovering from a mastectomy can be emotionally difficult. You may find it helpful, before and after your mastectomy, to talk to others who have had the operation.
You can get information on contacting others who have had a mastectomy from your doctor or nurse, or from organizations such as:
- The National Cancer Institute (https://www.cancer.gov/)
- The American Cancer Society (https://www.cancer.org/)
Mastectomy procedure
Preparing for a mastectomy
Meet with your surgeon to discuss your options
Before your surgery, you’ll meet with a surgeon and an anesthesiologist to discuss your operation, review your medical history and determine the plan for your anesthesia.
This is a good time to ask questions and to make sure you understand the procedure, including the reasons for and risks of the surgery.
Your surgeon will discuss the type of mastectomy you’ll have, the possible complications and the option of breast reconstruction. You may need to have chemotherapy or hormone therapy before the operation to reduce the size of any tumors.
The other issue to discuss is whether you’ll have breast reconstruction and when. One option may be to have the reconstruction done immediately after your mastectomy, while you’re still anesthetized.
You’ll also get practical advice about bras and bra inserts, if you need them.
Preparing for your surgery
You’ll be given instructions about any restrictions before surgery and other things you need to know, including:
- Tell your doctor about any medications, vitamins or supplements you’re taking. Some substances could interfere with the surgery.
- Stop taking aspirin or other blood-thinning medication. A week or longer before your surgery, talk to your provider about which medications to avoid because they can increase your risk of excessive bleeding. These include aspirin, ibuprofen (Advil, Motrin IB, others) and other pain relievers, and blood-thinning medications (anticoagulants), such as warfarin (Coumadin, Jantoven).
- Don’t eat or drink 8 to 12 hours before surgery. You’ll receive specific instructions from your health care team.
- Prepare for a hospital stay. Ask your doctor how long to expect to stay in the hospital. Bring a robe and slippers to help make you more comfortable in the hospital. Pack a bag with your toothbrush and something to help you pass the time, such as a book.
Before the mastectomy procedure
Your doctor or nurse will tell you when to arrive at the hospital. A mastectomy without reconstruction usually takes one to three hours. The surgery is often done as an outpatient procedure, and most people go home on the same day of the operation.
If you’re having both breasts removed (a double mastectomy), expect to spend more time in surgery and possibly an additional day in the hospital. If you’re having breast reconstruction following a mastectomy, the procedure also takes longer and you may stay in the hospital for a few additional days.
If you’re having a sentinel node biopsy, before your surgery a radioactive tracer and a blue dye are injected into the area around the tumor or the skin above the tumor. The tracer and the dye travel to the sentinel node or nodes, allowing your doctor to see where they are and remove them during surgery.
During the mastectomy procedure
A mastectomy is usually performed under general anesthesia, so you’ll be asleep while it happens and you’re not aware during the surgery. Your surgeon starts by making an elliptical incision around your breast. The breast tissue is removed and, depending on your procedure, other parts of the breast also may be removed.
Regardless of the type of mastectomy you have, the breast tissue and lymph nodes that are removed will be sent to a laboratory for analysis.
If you’re having breast reconstruction at the same time as a mastectomy, the plastic surgeon will coordinate with the breast surgeon to be available at the time of surgery.
One option for breast reconstruction involves placing temporary tissue expanders in the chest. These temporary expanders will form the new breast mound.
For women who will have radiation therapy after surgery, one option is to place temporary tissue expanders in the chest to hold the breast skin in place. This allows you to delay final breast reconstruction until after radiation therapy.
If you’re planning to have radiation therapy after surgery, meet with a radiation oncologist before surgery to discuss benefits and risks, as well as how radiation will impact your breast reconstruction options.
As the surgery is completed, the incision is closed with stitches (sutures), which either dissolve or are removed later. You might also have one or two small plastic tubes placed where your breast was removed. The tubes will drain any fluids that accumulate after surgery. The tubes are sewn into place, and the ends are attached to a small drainage bag. These may be left in for a few days.
After the mastectomy procedure
After your surgery, you can expect to:
- Be taken to a recovery room where your blood pressure, pulse and breathing are monitored
- Have a dressing (bandage) over the surgery site
- Feel some pain, numbness and a pinching sensation in your underarm area
- Receive instructions on how to care for yourself at home, including taking care of your incision and drains, recognizing signs of infection, and understanding activity restrictions
- Talk with your health care team about when to resume wearing a bra or wearing a breast prosthesis
- Be given prescriptions for pain medication and possibly an antibiotic
Results
The results of your pathology report should be available within a week or two after your mastectomy. At your follow-up visit, your doctor can explain the report.
If you need more treatment, your doctor may refer you to:
- A radiation oncologist to discuss radiation treatments, which may be recommended if you had a large tumor, many lymph nodes that tested positive for cancer, cancer that had spread into the skin or nipple, or cancer remaining after the mastectomy
- A medical oncologist to discuss other forms of treatment after the operation, such as hormone therapy if your cancer is sensitive to hormones or chemotherapy or both
- A plastic surgeon, if you’re considering breast reconstruction
- A counselor or support group to help you cope with having breast cancer.
Mastectomy side effect
To some extent, the side effects of mastectomy can depend on the type of mastectomy you have (with more extensive surgeries tending to have more side effects). Side effects can include:
- Pain or tenderness
- Swelling at the surgery site
- Buildup of blood in the wound (hematoma)
- Buildup of clear fluid in the wound (seroma)
- Limited arm or shoulder movement
- Numbness in the chest or upper arm
- Nerve (neuropathic) pain (sometimes described as burning or shooting pain) in the chest wall, armpit, and/or arm that doesn’t go away over time. It is also called post-mastectomy pain syndrome (PMPS).
As with all operations, bleeding and infection at the surgery site are also possible. If axillary lymph nodes are also removed, other side effects such as lymphedema may occur.
Mastectomy risks
Risks of a mastectomy include:
- Bleeding
- Infection
- Pain
- Swelling (lymphedema) in your arm if you have an axillary node dissection
- Formation of hard scar tissue at the surgical site
- Shoulder pain and stiffness
- Numbness, particularly under your arm, from lymph node removal
- Buildup of blood in the surgical site (hematoma)
Get urgent medical advice if:
- your wound becomes infected – it may be red, painful or swollen, or ooze liquid
- your arm and hand become swollen and sore because of a build-up of fluid (lymphedema)
- your wound is bleeding
What is post-mastectomy pain syndrome?
After having breast cancer surgery, some women have problems with nerve (neuropathic) pain in the chest wall, armpit, and/or arm that doesn’t go away over time. This is called post-mastectomy pain syndrome because it was first described in women who had mastectomies, but it can also happen after breast-conserving surgery (such as a lumpectomy).
Post-mastectomy pain syndrome symptoms
The classic symptoms of post-mastectomy pain syndrome are pain and tingling in the chest wall, armpit, and/or arm. Pain may also be felt in the shoulder or surgical scar. Other common complaints include: numbness, shooting or pricking pain, or unbearable itching. Most women with post-mastectomy pain syndrome say their symptoms are not severe.
How common is post-mastectomy pain syndrome?
Studies have shown that between 20% and 30% of women develop symptoms of post-mastectomy pain syndrome after surgery.
Post-mastectomy pain syndrome is thought to be linked to damage done to the nerves in the armpit and chest during surgery. But the causes are not known for sure. Women who are younger, who have had a full axillary lymph node dissection and not just a sentinel lymph node biopsy, or who were treated with radiation after surgery are more likely to have problems with post-mastectomy pain syndrome. Because axillary lymph node dissection is done less often now, post-mastectomy pain syndrome is less common than it once was.
Post-mastectomy pain syndrome treatment
It is important to talk to your doctor about any pain you are having. post-mastectomy pain syndrome can cause you to not use your arm the way you should, and over time you could lose the ability to use it normally.
Post-mastectomy pain syndrome can be treated. Some pain medicines such as opioids (narcotics) don’t always work well for nerve pain, but there are medicines and treatments that do work for this kind of pain. Talk to your doctor to get the pain control you need.
Mastectomy reconstruction
After having a mastectomy a woman might want to consider having the breast mound rebuilt to restore the breast’s appearance. This is called breast reconstruction. Although each case is different, most mastectomy patients can have breast reconstruction. Breast reconstruction can be done at the same time as the mastectomy or sometime later. Surgery to reconstruct the breasts can be done (or started) at the time of the mastectomy (which is called immediate reconstruction) or it can be done after the mastectomy incisions have healed and breast cancer therapy has been completed (which is called delayed reconstruction). Delayed reconstruction can happen months or even years after the mastectomy.
In a final stage of breast reconstruction, a nipple and areola may be re-created on the reconstructed breast, if these were not preserved during the mastectomy.
Sometimes breast reconstruction surgery includes surgery on the other, or contralateral, breast so that the two breasts will match in size and shape.
If you are thinking about having reconstructive surgery, it’s a good idea to discuss it with your surgeon and a plastic surgeon before your mastectomy. This allows the surgical teams to plan the treatment that’s best for you, even if you wait and have the reconstructive surgery later. Insurance companies typically cover breast reconstruction, but you should check with your insurance company so you know what is covered.
Some women choose not to have reconstructive surgery. Wearing a breast prosthesis (breast form) is an option for women who want to have the contour of a breast under their clothes without having surgery. Some women are also comfortable with just ‘going flat,’ especially if both breasts were removed.
For other women, breast reconstruction might be difficult, or even not possible, because of other health issues they have. For example, you might not be able to have reconstruction if you are obese, too thin, or have blood circulation problems.
Breast reconstruction may involve:
- Using breast expanders with saline or silicone implants
- Using your body’s own tissue (autologous tissue reconstruction)
- Using a combination of tissue reconstruction and implants
Breast reconstruction is a complex procedure performed by a plastic surgeon, also called a reconstructive surgeon. If you’re planning breast reconstruction at the same time as a mastectomy, you’ll meet with the plastic surgeon before the surgery.
What are some new developments in breast reconstruction after mastectomy?
Oncoplastic surgery
In general, women who have lumpectomy or partial mastectomy for early-stage breast cancer do not have reconstruction. However, for some of these women the surgeon may use plastic surgery techniques to reshape the breast at the time of cancer surgery. This type of breast-conserving surgery, called oncoplastic surgery, may use local tissue rearrangement, reconstruction through breast reduction surgery, or transfer of tissue flaps. Long-term outcomes of this type of surgery are comparable to those for standard breast-conserving surgery 1.
Autologous fat grafting
A newer type of breast reconstruction technique involves the transfer of fat tissue from one part of the body (usually the thighs, abdomen, or buttocks) to the reconstructed breast. The fat tissue is harvested by liposuction, washed, and liquified so that it can be injected into the area of interest. Fat grafting is mainly used to correct deformities and asymmetries that may appear after breast reconstruction. It is also sometimes used to reconstruct an entire breast. Although concern has been raised about the lack of long-term outcome studies, this technique is considered safe 2.
How do surgeons use implants to reconstruct a woman’s breast?
Breast implants are inserted underneath the skin or chest muscle following the mastectomy. Most mastectomies are performed using a technique called skin-sparing mastectomy, in which much of the breast skin is saved for use in reconstructing the breast.
Breast implants are usually placed as part of a two-stage procedure.
- In the first stage, the surgeon places a device, called a tissue expander, under the skin that is left after the mastectomy or under the chest muscle 3. The expander is slowly filled with saline during periodic visits to the doctor after surgery.
- In the second stage, after the chest tissue has relaxed and healed enough, the expander is removed and replaced with an implant. The chest tissue is usually ready for the implant 2 to 6 months after mastectomy.
In some cases, the implant can be placed in the breast during the same surgery as the mastectomy—that is, a tissue expander is not used to prepare for the implant 4.
Surgeons are increasingly using material called acellular dermal matrix as a kind of scaffold or “sling” to support tissue expanders and implants. Acellular dermal matrix is a kind of mesh that is made from donated human or pig skin that has been sterilized and processed to remove all cells to eliminate the risks of rejection and infection.
How do surgeons use tissue from a woman’s own body to reconstruct the breast?
In autologous tissue reconstruction, a piece of tissue containing skin, fat, blood vessels, and sometimes muscle is taken from elsewhere in a woman’s body and used to rebuild the breast. This piece of tissue is called a flap.
Different sites in the body can provide flaps for breast reconstruction. Flaps used for breast reconstruction most often come from the abdomen or back. However, they can also be taken from the thigh or buttocks.
Depending on their source, flaps can be pedicled or free:
- With a pedicled flap, the tissue and attached blood vessels are moved together through the body to the breast area. Because the blood supply to the tissue used for reconstruction is left intact, blood vessels do not need to be reconnected once the tissue is moved.
- With free flaps, the tissue is cut free from its blood supply. It must be attached to new blood vessels in the breast area, using a technique called microsurgery. This gives the reconstructed breast a blood supply.
Abdominal and back flaps include:
- Deep inferior epigastric artery perforator flap (DIEP or DIEAP flap): Tissue comes from the abdomen and contains only skin, blood vessels, and fat, without the underlying muscle. This type of flap is a free flap.
- Latissimus dorsi flap: Tissue comes from the middle and side of the back. This type of flap is pedicled when used for breast reconstruction. Latissimus dorsi flaps can be used for other types of reconstruction as well.
- SIEA flap (also called SIEP flap): Tissue comes from the abdomen as in a deep inferior epigastric artery perforator flap (DIEP flap) but includes a different set of blood vessels. It also does not involve cutting of the abdominal muscle and is a free flap. This type of flap is not an option for many women because the necessary blood vessels are not adequate or do not exist.
- Transverse rectus abdominus myocutaneous flap (TRAM flap): Tissue comes from the lower abdomen as in a DIEP flap but includes muscle. It can be either pedicled or free.
Flaps taken from the thigh or buttocks are used for women who have had previous major abdominal surgery or who don’t have enough abdominal tissue to reconstruct a breast. These types of flaps are free flaps. With these flaps an implant is often used as well to provide sufficient breast volume.
- IGAP flap: Tissue comes from the buttocks and contains only skin, blood vessels, and fat.
- PAP flap: Tissue, without muscle, that comes from the upper inner thigh.
- SGAP flap: Tissue comes from the buttocks as in an IGAP flap, but includes a different set of blood vessels and contains only skin, blood vessels, and fat.
- Transverse upper gracilis flap (TUG flap): Tissue, including muscle, that comes from the upper inner thigh.
In some cases, an implant and autologous tissue are used together. For example, autologous tissue may be used to cover an implant when there isn’t enough skin and muscle left after mastectomy to allow for expansion and use of an implant 5.
For any of these procedures, you will have general anesthesia. This is medicine that keeps you asleep and pain-free.
For TRAM surgery:
- The surgeon makes a cut (incision) across your lower belly, from one hip to the other. Your scar will be hidden later by most clothing and bathing suits.
- The surgeon loosens skin, fat, and muscle in this area. This tissue is then tunneled under the skin of your abdomen up to the breast area to create your new breast. Blood vessels remain connected to the area from where the tissue is taken.
- In another method called the free flap procedure, skin, fat, and muscle tissue are removed from your lower belly. This tissue is placed in your breast area to create your new breast. The arteries and veins are cut and reattached to blood vessels under your arm or behind your breastbone.
- This tissue is then shaped into a new breast. The surgeon matches the size and shape of your remaining natural breast as closely as possible.
- The incisions on your belly are closed with stitches.
- If you would like a new nipple and areola created, you will need a second, much smaller surgery later. Or, the nipple and areola can be created with a tattoo.
For latissimus dorsi muscle flap with a breast implant:
- The surgeon makes a cut in your upper back, on the side of your breast that was removed.
- The surgeon loosens skin, fat, and muscle from this area. This tissue is then tunneled under your skin to the breast area to create your new breast. Blood vessels remain connected to the area from where the tissue was taken.
- This tissue is then shaped into a new breast. The surgeon matches the size and shape of your remaining natural breast as closely as possible.
- An implant may be placed underneath the chest wall muscles to help match the size of your other breast.
- The incisions are closed with stitches.
- If you would like a new nipple and areola created, you will need a second, much smaller surgery later. Or, the nipple and areola can be created with a tattoo.
For a DIEP or DIEAP flap:
- The surgeon makes a cut across your lower belly. Skin and fat from this area is loosened. This tissue is then placed in your breast area to create your new breast. The arteries and veins are cut and then reattached to the blood vessels under your arm or behind your breastbone.
- The tissue is then shaped into a new breast. The surgeon matches the size and shape of your remaining natural breast as closely as possible.
- The incisions are closed with stitches.
- If you would like a new nipple and areola created, you will need a second, much smaller surgery later. Or, the nipple and areola can be created with a tattoo.
For a gluteal flap:
- The surgeon makes a cut in your buttocks. Skin, fat, and possibly muscle from this area are loosened. This tissue is placed in your breast area to create your new breast. The arteries and veins are cut and then reattached to the blood vessels under your arm or behind your breastbone.
- The tissue is then shaped into a new breast. The surgeon matches the size and shape of your remaining natural breast as closely as possible.
- The incisions are closed with stitches.
- If you would like a new nipple and areola created, you will need a second, much smaller surgery later. Or, the nipple and areola can be created with a tattoo.
For a TUG flap:
- The surgeon makes a cut in your thigh. Skin, fat, and muscle from this area are loosened. This tissue is placed in your breast area to create your new breast.
- The arteries and veins are cut and then reattached to the blood vessels under your arm or behind your breastbone.
- The tissue is then shaped into a new breast. The surgeon matches the size and shape of your remaining natural breast as closely as possible.
- The incisions are closed with stitches.
- If you would like a new nipple and areola created, you will need a second, much smaller surgery later. Or, the nipple and areola can be created with a tattoo.
When breast reconstruction is done at the same time as a mastectomy, the entire surgery may last 8 to 10 hours. When it is done as a second surgery, it may take up to 12 hours.
How do surgeons reconstruct the nipple and areola?
After the chest heals from reconstruction surgery and the position of the breast mound on the chest wall has had time to stabilize, a surgeon can reconstruct the nipple and areola. Usually, the new nipple is created by cutting and moving small pieces of skin from the reconstructed breast to the nipple site and shaping them into a new nipple. A few months after nipple reconstruction, the surgeon can re-create the areola. This is usually done using tattoo ink. However, in some cases, skin grafts may be taken from the groin or abdomen and attached to the breast to create an areola at the time of the nipple reconstruction 3.
Some women who do not have surgical nipple reconstruction may consider getting a realistic picture of a nipple created on the reconstructed breast from a tattoo artist who specializes in 3-D nipple tattooing.
A mastectomy that preserves a woman’s own nipple and areola, called nipple-sparing mastectomy, may be an option for some women, depending on the size and location of the breast cancer and the shape and size of the breasts 6.
What factors can affect the timing of breast reconstruction?
One factor that can affect the timing of breast reconstruction is whether a woman will need radiation therapy. Radiation therapy can sometimes cause wound healing problems or infections in reconstructed breasts, so some women may prefer to delay reconstruction until after radiation therapy is completed. However, because of improvements in surgical and radiation techniques, immediate reconstruction with an implant is usually still an option for women who will need radiation therapy. Autologous tissue breast reconstruction is usually reserved for after radiation therapy, so that the breast and chest wall tissue damaged by radiation can be replaced with healthy tissue from elsewhere in the body.
Another factor is the type of breast cancer. Women with inflammatory breast cancer usually require more extensive skin removal. This can make immediate reconstruction more challenging, so it may be recommended that reconstruction be delayed until after completion of adjuvant therapy.
Even if a woman is a candidate for immediate reconstruction, she may choose delayed reconstruction. For instance, some women prefer not to consider what type of reconstruction to have until after they have recovered from their mastectomy and subsequent adjuvant treatment. Women who delay reconstruction (or choose not to undergo the procedure at all) can use external breast prostheses, or breast forms, to give the appearance of breasts.
What factors can affect the choice of breast reconstruction method?
Several factors can influence the type of reconstructive surgery a woman chooses. These include the size and shape of the breast that is being rebuilt, the woman’s age and health, her history of past surgeries, surgical risk factors (for example, smoking history and obesity), the availability of autologous tissue, and the location of the tumor in the breast 2. Women who have had past abdominal surgery may not be candidates for an abdominally based flap reconstruction.
Each type of reconstruction has factors that a woman should think about before making a decision. Some of the more common considerations are listed below.
Reconstruction with implants
Surgery and recovery:
- Enough skin and muscle must remain after mastectomy to cover the implant
- Shorter surgical procedure than for reconstruction with autologous tissue; little blood loss
- Recovery period may be shorter than with autologous reconstruction
- Many follow-up visits may be needed to inflate the expander and insert the implant
Possible complications:
- Infection
- Accumulation of clear fluid causing a mass or lump (seroma) within the reconstructed breast 7
- Pooling of blood (hematoma) within the reconstructed breast
- Blood clots
- Extrusion of the implant (the implant breaks through the skin)
- Implant rupture (the implant breaks open and saline or silicone leaks into the surrounding tissue)
- Formation of hard scar tissue around the implant (known as a contracture)
- Obesity, diabetes, and smoking may increase the rate of complications
- Possible increased risk of developing a very rare form of immune system cancer called anaplastic large cell lymphoma 8
Other considerations:
- May not be an option for patients who have previously undergone radiation therapy to the chest
- May not be adequate for women with very large breasts
- Will not last a lifetime; the longer a woman has implants, the more likely she is to have complications and to need to have her implants removed or replaced
- Silicone implants may feel more natural than saline implants to the touch
- The Food and Drug Administration (FDA) recommends that women with silicone implants undergo periodic MRI screenings to detect possible “silent” rupture of the implants 9.
Reconstruction with autologous tissue
Surgery and recovery:
- Longer surgical procedure than for implants
- The initial recovery period may be longer than for implants
- Pedicled flap reconstruction is usually a shorter operation than free flap reconstruction and usually requires a shorter hospitalization
- Free flap reconstruction is a longer, highly technical operation compared with pedicled flap reconstruction that requires a surgeon who has experience with microsurgery to re-attach blood vessels
Possible complications:
- Necrosis (death) of the transferred tissue
- Blood clots may be more frequent with some flap sources
- Pain and weakness at the site from which the donor tissue was taken
- Obesity, diabetes, and smoking may increase the rate of complications
Other considerations:
- May provide a more natural breast shape than implants
- May feel softer and more natural to the touch than implants
- Leaves a scar at the site from which the donor tissue was taken
- Can be used to replace tissue that has been damaged by radiation therapy
All women who undergo mastectomy for breast cancer experience varying degrees of breast numbness and loss of sensation (feeling) because nerves that provide sensation to the breast are cut when breast tissue is removed during surgery. However, a woman may regain some sensation as the severed nerves grow and regenerate, and breast surgeons continue to make technical advances that can spare or repair damage to nerves.
Any type of breast reconstruction can fail if healing does not occur properly. In these cases, the implant or flap will have to be removed. If an implant reconstruction fails, a woman can usually have a second reconstruction using an alternative approach.
Will health insurance pay for breast reconstruction?
The Women’s Health and Cancer Rights Act of 1998 (WHCRA) is a federal law that requires group health plans and health insurance companies that offer mastectomy coverage to also pay for reconstructive surgery after mastectomy. This coverage must include all stages of reconstruction and surgery to achieve symmetry between the breasts, breast prostheses, and treatment of complications that result from the mastectomy, including lymphedema. More information about WHCRA is available from the Department of Labor (https://www.dol.gov/) and the Centers for Medicare & Medicaid Services (https://www.cms.gov/CCIIO/Programs-and-Initiatives/Other-Insurance-Protections/whcra_factsheet.html).
Some health plans sponsored by religious organizations and some government health plans may be exempt from WHCRA. Also, WHCRA does not apply to Medicare and Medicaid. However, Medicare may cover breast reconstruction surgery as well as external breast prostheses (including a post-surgical bra) after a medically necessary mastectomy.
Medicaid benefits vary by state; a woman should contact her state Medicaid office for information on whether, and to what extent, breast reconstruction is covered.
A woman considering breast reconstruction may want to discuss costs and health insurance coverage with her doctor and insurance company before choosing to have the surgery. Some insurance companies require a second opinion before they will agree to pay for a surgery.
What type of follow-up care and rehabilitation is needed after breast reconstruction?
Any type of reconstruction increases the number of side effects a woman may experience compared with those after a mastectomy alone. A woman’s medical team will watch her closely for complications, some of which can occur months or even years after surgery 3.
Women who have either autologous tissue or implant-based reconstruction may benefit from physical therapy to improve or maintain shoulder range of motion or help them recover from weakness experienced at the site from which the donor tissue was taken, such as abdominal weakness 10. A physical therapist can help a woman use exercises to regain strength, adjust to new physical limitations, and figure out the safest ways to perform everyday activities.
Does breast reconstruction affect the ability to check for breast cancer recurrence?
Studies have shown that breast reconstruction does not increase the chances of breast cancer coming back or make it harder to check for recurrence with mammography 11.
Women who have one breast removed by mastectomy will still have mammograms of the other breast. Women who have had a skin-sparing mastectomy or who are at high risk of breast cancer recurrence may have mammograms of the reconstructed breast if it was reconstructed using autologous tissue. However, mammograms are generally not performed on breasts that are reconstructed with an implant after mastectomy.
A woman with a breast implant should tell the radiology technician about her implant before she has a mammogram. Special procedures may be necessary to improve the accuracy of the mammogram and to avoid damaging the implant.
Using a breast form or prosthesis
A breast form is a prosthesis (artificial body part) worn either inside a bra or attached to the body to simulate the appearance and feel of a natural breast. Wearing a breast form is an option for women who have decided not to get reconstructive surgery but want to keep the same look under their clothes. If you haven’t decided about reconstruction, or are having reconstruction later, you might decide to use a breast form temporarily.
Most breast forms are made from materials that mimic the movement, feel, and weight of natural breast tissue. A properly weighted form provides the balance your body needs for correct posture and anchors your bra, keeping it from riding up. At first, these forms may feel too heavy, but in time they should feel natural.
If you are planning to use a breast form, your doctor will tell you when you have healed enough to be fitted for a permanent breast form or prosthesis.
Choosing the right bra for your breast form
The right bra for you may very well be the one you have always worn. It may or may not need adjustments. If there is tenderness during healing, a bra extender can help by increasing the circumference of the bra so that it does not bind the chest too tightly. Heavy-breasted women can relieve pressure on shoulder straps by slipping a bra shoulder pad under one or both straps.
If you decide to wear your breast form in a pocket in your bra, you can have your regular bra adapted. There are also special mastectomy bras with the pockets already sewn in. If the breast form causes any kind of skin irritation, use a bra with a pocket. If your bra has underwires, you may be able to wear it, but be sure to clear this with your doctor.
If you want to wear your prosthesis under sleepwear but would like something more comfortable than a regular bra, look for a soft bra, sometimes called a leisure or night bra. These are in most department stores.
Finding and paying for breast prostheses
Prices for breast forms vary considerably. High price doesn’t necessarily mean that the product is the best for you. Take time to shop for a good fit, comfort, and an attractive, natural appearance in the bra and under clothing. Your clothes should fit the way they did before surgery.
Insurance coverage of breast prostheses can vary. Be sure to contact your health insurance provider to find out what will be covered and how you must submit claims. Also, ask your doctor to write prescriptions for your prosthesis and for any special mastectomy bras. When purchasing bras or breast forms, mark the bills and any checks you write “surgical.” Medicare and Medicaid can be used to pay for some of these expenses if you are eligible. The cost of breast forms and bras with pockets might be tax deductible, and also the cost if you have a bra altered. Keep careful records of all related expenses.
Some insurance companies will not cover both a breast prosthesis and reconstructive surgery. That can mean that if you submit a claim for a prosthesis or bra to your insurance company, in some cases the company will not cover reconstruction, should you choose this procedure in the future. Make sure you get all the facts before submitting any insurance claims.
Going flat
Some women, who do not have reconstruction surgery, decide not to wear a breast form, either.
For most women, there aren’t likely to be any added health issues from going flat, especially if both breasts were removed. But if you’ve only had one breast removed, you might notice issues with balance, posture, or back pain, especially if you’ve always had large breasts. This is one reason some women prefer to wear a breast form – to balance out the weight on their chest. Talk to your doctor about your options if you think this might be an issue for you.
Some women might use a breast form when out but not when at home. This might be because they find breast forms uncomfortable or too expensive, or just because they’re comfortable with how they look and feel without a breast form and don’t feel the need to wear one.
If the idea of going flat appeals to you but you’re worried about what others might think, try going without a breast form in different situations, such as at home, out with friends, or while out running errands. You might find that most people won’t notice a difference. If you find you still feel self-conscious, you can always go back to wearing a breast form.
If you decide to go flat, you might want to consider wearing clothing that might help you feel more comfortable with your appearance. Try wearing tops that are not tight fitting and that have busy patterns, or layer sweaters or jackets over close-fitting tops. Scarves and shawls can also cover all or part of your chest.
Some women might like the idea of going flat but are uncomfortable about not having nipples. Some companies now make nipple prosthetics, which are made of silicone or other materials and look and feel like real nipples. They can be attached to the chest and then taken off when you choose.
References- De La Cruz L, Blankenship SA, Chatterjee A, et al. Outcomes after oncoplastic breast-conserving surgery in breast cancer patients: A systematic literature review. Annals of Surgical Oncology 2016; 23(10):3247-3258.
- Schmauss D, Machens HG, Harder Y. Breast reconstruction after mastectomy. Frontiers in Surgery 2016; 2:71-80.
- Mehrara BJ, Ho AY. Breast Reconstruction. In: Harris JR, Lippman ME, Morrow M, Osborne CK, eds. Diseases of the Breast. 5th ed. Philadelphia: Wolters Kluwer Health; 2014.
- Roostaeian J, Pavone L, Da Lio A, et al. Immediate placement of implants in breast reconstruction: patient selection and outcomes. Plastic and Reconstructive Surgery 2011; 127(4):1407-1416
- Cordeiro PG. Breast reconstruction after surgery for breast cancer. New England Journal of Medicine 2008; 359(15):1590–1601. DOI: 10.1056/NEJMct0802899
- Petit JY, Veronesi U, Lohsiriwat V, et al. Nipple-sparing mastectomy—is it worth the risk? Nature Reviews Clinical Oncology 2011; 8(12):742–747
- Jordan SW, Khavanin N, Kim JY. Seroma in prosthetic breast reconstruction. Plastic and Reconstructive Surgery 2016; 137(4):1104-1116.
- Gidengil CA, Predmore Z, Mattke S, van Busum K, Kim B. Breast implant-associated anaplastic large cell lymphoma: a systematic review. Plastic and Reconstructive Surgery 2015; 135(3):713-720.
- Breast Implants. https://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ImplantsandProsthetics/BreastImplants/default.htm
- McAnaw MB, Harris KW. The role of physical therapy in the rehabilitation of patients with mastectomy and breast reconstruction. Breast Disease 2002; 16:163–174.
- Agarwal T, Hultman CS. Impact of radiotherapy and chemotherapy on planning and outcome of breast reconstruction. Breast Disease. 2002;16:37–42. DOI: 10.3233/BD-2002-16107





{kind=link}