
Minimal change disease
Minimal change disease also called “nil disease“, minimal change lesion or lipoid nephrosis (a description of lipid droplets in urine seen on light microscopy) is a kidney disorder that involves damage to the filtering units of the kidney (glomeruli) that can be seen only with an electron microscope and minimal change disease is the most common cause of idiopathic childhood nephrotic syndrome 1, 2, 3, 4. Minimal change disease accounts for 70% to 90% of children that present with nephrotic syndrome who are older than one year old as opposed to 10-15% of adults who present with nephrotic syndrome 5. Minimal change disease is the third most common cause of idiopathic nephrotic syndrome in adults after focal segmental glomerular sclerosis (FSGS) and membranous nephropathy (membranous glomerulopathy) 5. The reported incidence of minimal change disease in children varies between 2 to 7 new cases per 100,000 children 6, 7. The exact prevalence is unknown; however, it is estimated to be about 10 to 50 cases per 100,000 children 2. Minimal change disease is slightly more common in Asia and has a male predominance (approximately 2:1) in young children that disappears in adolescents and adults 6, 8. Minimal change disease is much less frequent in adults, but the exact incidence in this population is less well documented 3.
Nephrotic syndrome is a group of symptoms that include protein in the urine (proteinuria >40 mg/m2 per hour in children or urine protein-to-creatinine ratio >200 mg/mmol in children, >3.5 g/day in adults), low protein levels in the blood (hypoalbuminemia (<2.5 g/dl), high cholesterol levels, high triglyceride levels, an increased risk for blood clots, and swelling 9, 5. Other features of this disease include weight gain and a foamy appearance of the urine. Those with minimal change disease experience the signs and symptoms of nephrotic syndrome much quicker than they would with other glomerular diseases.
Minimal change disease gets its name because this damage is not visible under a regular microscope. It can only be seen under a very powerful microscope called an electron microscope.
On light microscopy of renal biopsy specimens from patients with minimal change disease, the kidney appears normal or nearly normal. Older pathologic terms for minimal change disease include nil disease (i.e, no abnormality) and lipoid nephrosis. Immunofluorescence microscopy may be normal or may show deposition of immunoglobulin M (IgM) antibody within the glomerulus. Electron microscopy shows podocyte foot process effacement, which is common to nearly all proteinuric diseases. Minimal change disease typically shows, prior to therapy, very extensive foot process effacement, often covering >90% of the glomerular capillary surface.
Each kidney is made of more than a million units called nephrons, which filter blood and produce urine.
In minimal change disease, there is damage to the glomeruli. These are the tiny blood vessels inside the nephron where blood is filtered to make urine and waste is removed.
Patients with minimal change typically present with the sudden onset of edema (swelling), either affecting the legs or, particularly in children, affecting the whole body, including facial edema (which may be the first manifestation). Other features of the nephrotic syndrome are often present, including hypercholesterolemia (high serum cholesterol) and low serum albumin. In children, the peak age of onset is age 2, with the disease being uncommon before age 1 and less common in during the teenage years. Minimal change disease also occurs in adulthood, even in the elderly, but is less common with advancing age.
The cause or causes of minimal change disease are largely unknown, but it may occur following an allergic reaction or infection 3, 2, 1, 10, 11, 12. Treatment may involve the use of steroids. The fluid retention and high blood pressure that often accompanies minimal change disease may be treated with the use of water pills (diuretics) in combination with a low sodium diet and blood pressure medications such as angiotensin-converting enzyme inhibitors (ACE inhibitors), angiotensin 2 receptor blocker (ARB) andcalcium channel antagonists.
There is an increased risk for the formation of blood clots (thromboembolic events) and infection in individuals with minimal change disease. It is recommended that individuals with minimal change disease stay active and should a blood clot occur, they may be treated with blood thinners. Infections, such as cellulitis, peritonitis, and pneumonia are common in individuals with minimal change disease and should be treated quickly 13.
Will minimal change disease cause kidney failure?
Kidney failure is rare if you have minimal change disease. Almost all children and adults recover from minimal change disease and avoid relapses over the long term. However, some may experience relapses of the protein in the urine, which can often be treated in the same way as the first episode. Progression to renal failure occurs in < 5 % of patients and is more common among those who do not initially respond to corticosteroids 14.
How your kidneys work
You have two kidneys, each about the size of an adult fist, located on either side of the spine just below the rib cage. Although they are small, your kidneys perform many complex and vital functions that keep the rest of the body in balance. Your kidneys remove waste and excess fluid from your blood through filtering units called nephrons. Each nephron contains a filter (glomerulus) that has a network of tiny blood vessels called capillaries. When blood flows into a glomerulus, tiny molecules — water, essential minerals and nutrients, and wastes — pass through the capillary walls. Large molecules, such as proteins and red blood cells, do not. The filtered solution then passes into another part of the nephron called the tubule. The water, nutrients and minerals your body needs are transferred back to the bloodstream. The excess water and waste become urine that flows to the bladder.
Kidney functions:
- Help remove waste and excess fluid
- Filter the blood, keeping some compounds while removing others
- Control the production of red blood cells
- Make vitamins that control growth
- Release hormones that help regulate blood pressure
- Help regulate blood pressure, red blood cells, and the amount of certain nutrients in the body, such as calcium and potassium.
Here’s how kidneys perform their important work:
- Blood enters the kidneys through an artery from the heart
- Blood is cleaned by passing through millions of tiny blood filters
- Waste material passes through the ureter and is stored in the bladder as urine
- Newly cleaned blood returns to the bloodstream by way of veins
- Bladder becomes full and urine passes out of the body through the urethra.
The kidneys perform their life-sustaining job of filtering and returning to the bloodstream about 200 quarts of fluid every 24 hours. Approximately two quarts are eliminated from the body in the form of urine, while the remainder, about 198 quarts, is retained in the body. The urine we excrete has been stored in the bladder for approximately one to eight hours.
Figure 1. How kidneys work
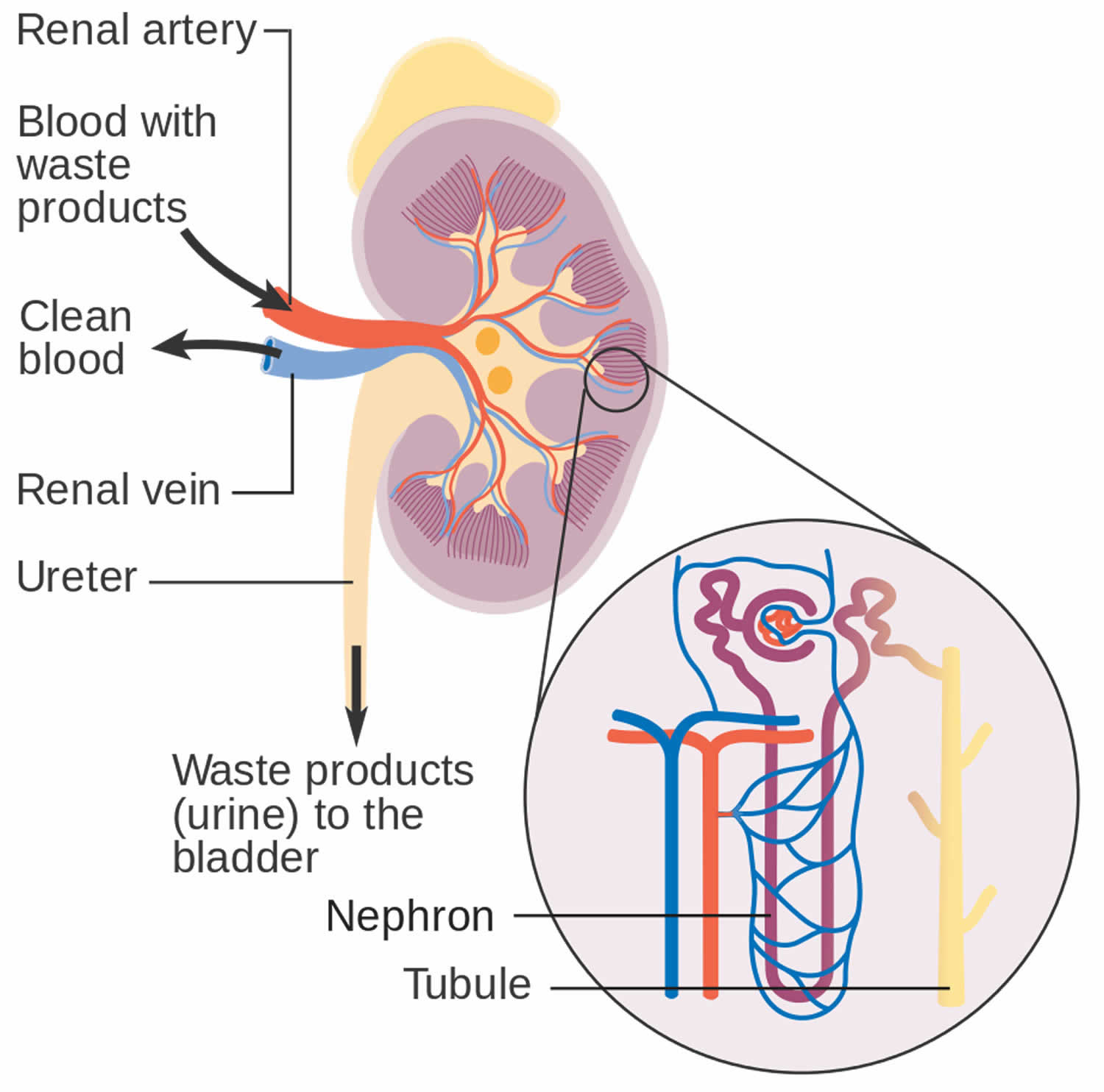
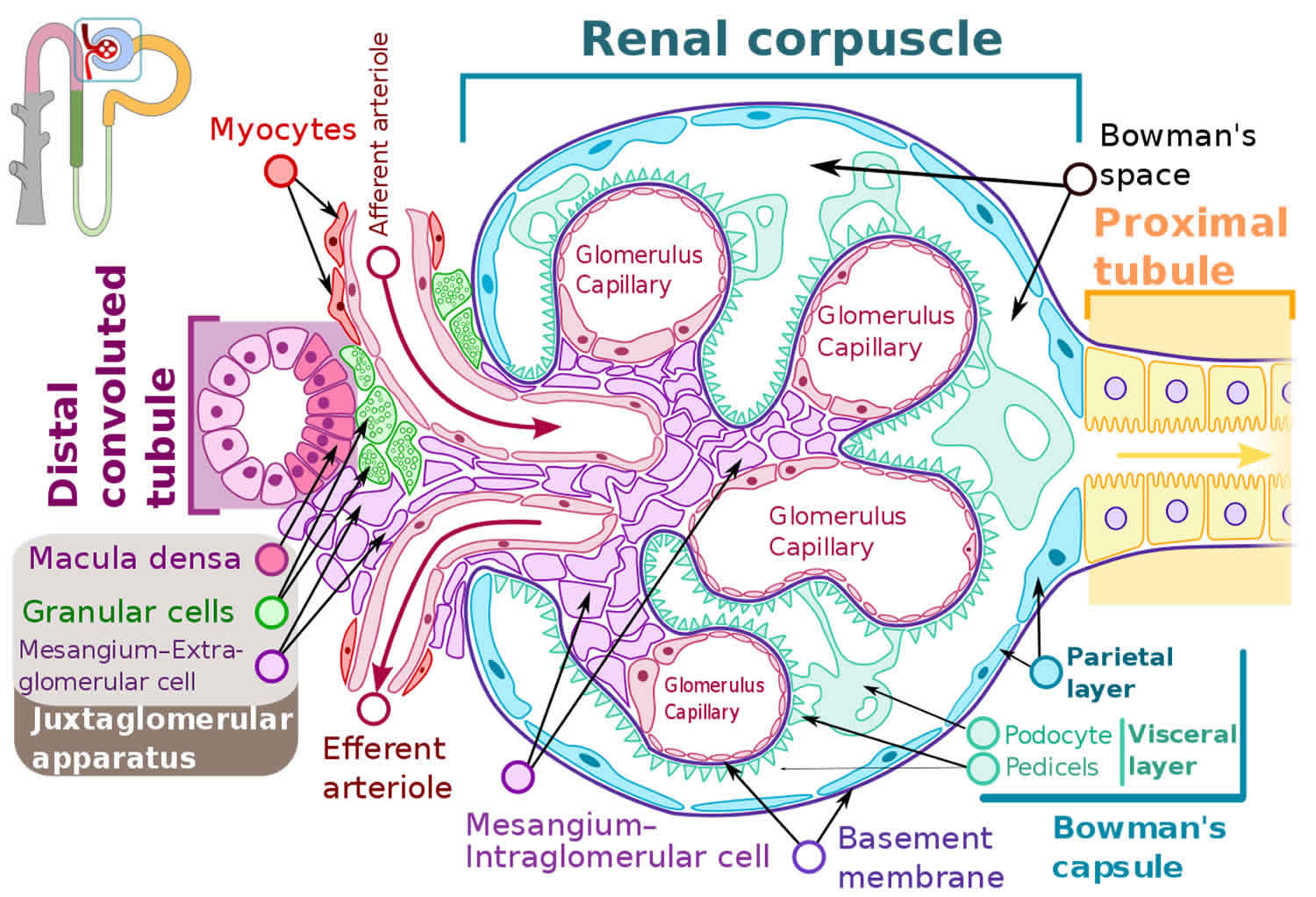
Figure 2. Glomerulus
How do glomerular diseases interfere with kidney function?
Glomerular diseases damage the glomeruli, letting protein and sometimes red blood cells leak into the urine. Sometimes a glomerular disease also interferes with the clearance of waste products by the kidney, so they begin to build up in the blood. Furthermore, loss of blood proteins like albumin in the urine can result in a fall in their level in the bloodstream. In normal blood, albumin acts like a sponge, drawing extra fluid from the body into the bloodstream, where it remains until the kidneys remove it. But when albumin leaks into the urine, the blood loses its capacity to absorb extra fluid from the body. Fluid can accumulate outside the circulatory system in the face, hands, feet, or ankles and cause swelling.
What are renal failure and end-stage renal disease?
Renal failure is any acute or chronic loss of kidney function and is the term used when some kidney function remains. Total kidney failure, sometimes called end-stage renal disease (ESRD), indicates permanent loss of kidney function. Depending on the form of glomerular disease, kidney function may be lost in a matter of days or weeks or may deteriorate slowly and gradually over
the course of decades.
Acute renal failure (acute kidney failure)
A few forms of glomerular disease cause very rapid deterioration of kidney function. For example, post-streptococcal glomerulonephritis (PSGN) can cause severe symptoms (hematuria, proteinuria, edema) within 2 to 3 weeks after a sore throat or skin infection develops. The patient may temporarily require dialysis to replace kidney function. This rapid loss of kidney function is called acute renal failure (acute kidney failure). Although acute renal failure (acute kidney failure) can be life-threatening while it lasts, kidney function usually returns after the cause of the kidney failure has been treated. In many patients, acute kidney failure is not associated with any permanent damage. However, some patients may recover from acute renal failure and subsequently develop chronic kidney disease (CKD).
Chronic kidney disease (CKD)
Most forms of glomerular disease develop gradually, often causing no symptoms for many years. Chronic kidney disease (CKD) is the slow, gradual loss of kidney function. Some forms of chronic kidney disease (CKD) can be controlled or slowed down. For example, diabetic nephropathy can be delayed by tightly controlling blood glucose levels and using angiotensin-converting enzyme inhibitors (ACE inhibitors) and angiotensin 2 receptor blockers (ARBs) to reduce proteinuria and control blood pressure. But chronic kidney disease (CKD) cannot be cured. Partial loss of kidney function means that some portion of the patient’s nephrons have been scarred, and scarred nephrons cannot be repaired. In many cases, CKD leads to total kidney failure.
Total kidney failure
To stay alive, a patient with total kidney failure must go on dialysis, either hemodialysis or peritoneal dialysis or receive a new kidney through kidney transplantation. Patients with chronic kidney disease (CKD) who are approaching total kidney failure should learn as much about their treatment options as possible so they can make an informed decision when the time comes. With the help of dialysis or kidney transplantation, many people continue to lead full, productive lives after reaching total kidney failure.
Minimal change disease causes
Scientists do not know the exact cause of minimal change disease 3, 2, 1, 10, 11, 12. In adults, minimal change disease is usually secondary (it is caused by another disease) to medication use (nonsteroidal anti-inflammatory drugs [NSAIDS], gold injection, interferon-alpha, lithium, pamidronate) or may follow insect stings. In children, minimal change disease is usually primary or idiopathic, which means the exact cause is not known. Minimal change disease is the most common cause of nephrotic syndrome in children. It is also seen in adults with nephrotic syndrome, but is less common.
The cause of minimal change disease is unknown, but if you have secondary causes for minimal change disease, the disease may occur or be related to 15, 16, 2:
- Allergic reactions (e.g., bee and medusa stings, cat fur, fungi, poison ivy, ragweed pollen, house dust, food allergens such as cow’s milk & egg)
- Drugs: nonsteroidal anti-inflammatory drugs (NSAIDs), lithium, antibiotics (ampicillin, cephalosporins), salazopyrin, D-penicillamine, mercury, gold, tiopronin, tyrosine-kinase inhibitors, immunizations, and gamma interferon
- Neoplasms: blood cancers, including leukemia, Hodgkin and non-Hodgkin lymphoma, multiple myeloma, thymoma, bronchogenic cancer, colon cancer, eosinophilic lymphoid granuloma (Kimura disease)
- Vaccinations (flu and pneumococcal, though rare)
- Infections: tuberculosis, syphilis, mycoplasma, ehrlichiosis, hepatitis C virus, HIV
- Autoimmune disorders: SLE, type 1 diabetes mellitus, myasthenia gravis, autoimmune pancreatitis, celiac disease, allogeneic stem cell transplantation
- Other glomerular diseases associated with IgA nephropathy
Minimal change disease pathophysiology
Minimal change disease presents with a nephrotic syndrome characterized by an increased renal membrane permeability and loss of protein (primarily albumin) due to damage to the glomerular filtration barrier 2. The glomerular filtration barrier is composed of fenestrated endothelium (inner layer), the glomerular basement membrane (middle layer), and an outer epithelial layer composed of podocytes 2. Podocytes are epithelial cells with large cell bodies and long foot processes that run parallel along the outside of glomerular capillaries. The space between foot processes is interspersed by cell-to-cell junctions called slit diaphragms 17.
Glomerular filtration is both size-specific and charge-specific. The actin cytoskeleton of podocytes provides support to the glomerular basement membrane (GBM) and regulates flow across the basement membrane depending on hydrostatic pressures, molecular size, and molecular charge 17. The apical and luminal membrane of the slit diaphragms and podocytes are coated with a sialoglycoprotein (podocalyxin) which contributes to repels negatively charged molecules such as albumin. The two outer layers of the glomerular basement membrane are composed of heparin sulfate proteoglycans that are also negatively charged and contribute to the charge selectivity of the barrier 18. Disruption of this barrier leads to the proteinuria seen in nephrotic syndrome.
The pathogenesis of minimal change disease is not exactly known, but it is thought to be multifactorial. Several studies have focused on the integrity and biology of podocytes. Because the actin cytoskeleton of podocytes maintains the integrity of the podocytes by supporting the cell body and foot processes, regulation of flow across the basement membrane is controlled by a series of interactions. As a result, multiple theories have been proposed to explain the cause of proteinuria in minimal change disease. Some of the proposed theories published include T cell dysfunction/dysregulation that leads to cytokine release and upregulation of proteins, such as CD80 and C-mip that affects the integrity of podocytes, systemic circulating factors that disrupt podocyte function, and B- cell activation (suspected due to the efficacy of anti- CD-20 monoclonal antibodies, such as rituximab) 19, 20, 21.
Minimal change disease symptoms
Minimal change disease causes nephrotic syndrome, usually without hypertension or azotemia (a condition in which you have too much nitrogen, creatinine and other waste products in your blood) 22. Microscopic blood in urine (hematuria) occurs in about 10% to 30% of patients, mainly adults 23, 22. Albumin is lost in the urine of patients with minimal change disease more so than larger serum proteins, probably because the disease causes changes in the charge barrier that affect albumin selectively.
There may be symptoms of nephrotic syndrome, including:
- Foamy appearance of the urine due to large amounts of protein leaking into your urine, called proteinuria
- Poor appetite
- Swelling called edema (especially around the eyes, feet, legs and ankles, and in the abdomen), due to fluid building up in your body
- Weight gain (from fluid retention), due to the fluid your body is not able to get rid of
Always speak with your doctor if you experience any of these signs and symptoms.
Minimal change disease does not reduce the amount of urine produced. It rarely progresses to kidney failure. Progression to renal failure occurs in < 5 % of patients and is more common among those who do not initially respond to corticosteroids 14.
Minimal change disease diagnosis
Your health care provider may not be able to see any signs of minimal change disease, other than swelling. Blood and urine tests reveal signs of nephrotic syndrome, including:
- High cholesterol
- High levels of protein in the urine (proteinuria)
- Low levels of albumin in the blood (hypoalbuminemia)
Tests and procedures used to diagnose nephrotic syndrome include:
- Urine tests. A urinalysis can reveal abnormalities in your urine, such as large amounts of protein, if you have nephrotic syndrome. You may be asked to collect urine samples over 24 hours for an accurate measure of the protein in your urine.
- Blood tests. If you have nephrotic syndrome, a blood test may show low levels of the protein albumin (hypoalbuminemia) specifically and often decreased levels of blood protein overall. Albumin is lost in the urine of patients with minimal change disease more so than larger serum proteins. Loss of albumin is often associated with an increase in blood cholesterol and blood triglycerides. Serum creatinine, blood urea and glomerular filtration rate (GFR) also may be measured to assess your overall kidney function and to know how well your kidneys are filtering the wastes from your body.
- Complete metabolic panel (CMP): Complete metabolic panel (CMP) demonstrates a low total protein, low albumin (frequently <2.5 g/dl), and low total calcium (ionized calcium binds to albumin, and albumin is low).
- Complete blood count (CBC): Complete blood count (CBC) will show hemoconcentration and thrombocytosis. This is seen due to the intravascular volume contraction from fluid sequestration into the interstitial space.
- Total cholesterol and triglyceride levels: Total cholesterol and triglyceride are increased due to an increase in hepatic lipoprotein synthesis as a result of low oncotic pressures 17.
- A kidney biopsy and examination of the tissue with an electron microscope can show signs of minimal change disease. During a kidney biopsy, a special needle is inserted through your skin and into your kidney.
If a kidney biopsy shows little or no damage under a regular microscope, then a diagnosis of minimal change disease may be made if other symptoms, such as protein in the urine and swelling, are noticed. Because minimal change disease is the most common cause of nephrotic syndrome in children, they first get treated for minimal change disease before getting a kidney biopsy. Most people will have a response in fewer than 8 weeks. If the protein in the urine disappears, the doctors may call the disease steroid-sensitive nephrotic syndrome instead of minimal change disease. If treatment does not improve their symptoms over the course of several months a kidney biopsy is done to see if there is another cause for their symptoms.
In children, minimal change disease is primarily a clinical diagnosis, and biopsy is only required in the presence of atypical clinical features 2, 3:
- Age of onset before 1 or after 12 years old
- Gross hematuria
- Low serum C3
- Marked Hypertension
- Elevated creatinine
- Renal failure without hypovolemia
- Positive history or serology for secondary causes
- Steroid resistance
Minimal change disease treatment
Medicines called corticosteroids can cure minimal change disease in most children. Some children may need to stay on steroids to keep the disease from returning. It is very important to not stop treatment suddenly. By sticking to the full treatment plan, your child will be less likely to relapse (experience the signs and symptoms again).
- Children. Initial prednisone therapy is 60 mg/m²(or 2 mg/kg) administered daily for 4-6 weeks (maximum dose, 60 mg/day), or 40 mg/m²/(or 1.5 mg/kg) on alternate days for 2-5 months taper. Reduce the dose by 5 mg/m² to 10 mg/m² each week for another four weeks, then stop, with a minimum duration of 12 weeks 24.
- Adults. Initial prednisone treatment is 1 mg/kg per day or 2 mg/kg/kg every other day (max 80mg/day or 120 mg every other day) for 4-16 weeks. Taper slowly over a course of 6 months after remission 23.
Most children (>90%) and adults (>70%) enter a complete remission with a course of steroids. Adults may have more frequent relapses and become dependent on steroids.
Patients who relapse demonstrate the following 2:
- Steroid resistance is noted as the persistence of proteinuria in children after 4 weeks of prednisone and after 16 weeks for adults.
- Frequent relapses occur, which are defined as two or more relapses in the first six months of presentation or four or more relapses within any 12 months
- Steroid dependency is defined as relapses that occur during the tapering phase of steroid therapy or less than two weeks after discontinuing steroids
- Relapse nephrosis – > 2+ proteinuria on 3 consecutive days
- Prednisolone should be restarted if there is a relapse: 2 mg/kg daily (maximum 60 mg) until in remission for 3 days, then 1.5 mg/kg alternate days for 4 weeks, then stop or taper the dose over 4-8 weeks.
Mortality at present is very low. Many steroid regimens have been used. The most common regimens involve the use prednisone daily or every other day. Unfortunately, relapses are common. When patients respond to steroids but experience frequent relapses, therapeutic options include cyclophosphamide, chlorambucil, and cyclosporine.
If steroids are not effective (you do not enter complete remission with steroid therapy), your doctor will likely suggest other medicines that include cyclosporine. For children who do not respond to traditional treatment they have what is called steroid-resistant nephrotic syndrome or SRNS. Treatment for steroid-resistant nephrotic syndrome includes other combinations of drugs. It is recommended that children with steroid-resistant nephrotic syndrome take a blood pressure medication (ACE inhibitor or angiotensin 2 receptor blocker [ARB]). These two drugs control high blood pressure and reduce the amount of protein in the urine.
For frequent relapses/ steroid-dependent (steroid-sparing agents) 2:
- Cyclophosphamide: the dose of 2 mg/kg/ day for 8 to 12 weeks (should be started after reaching remission with the steroid)- potential gonadal toxicity, alopecia, bone marrow suppression.
- Cyclosporine: At a dose of 4 to 5 mg/kg/day, usually for 1-2 years. Levels should be monitored after 1 to 2 weeks. Aim for a trough of 70 to 150. Can cause nephrotoxicity, hirsutism, hypertension, and gingival hyperplasia.
If intolerant to the above-mentioned drugs, can give 2:
- Mycophenolate mofetil (MMF): Doses of 500 to 1000 mg two times a day for 1 to 2 years. Should be monitored for leukopenia 24.
- Rituximab (chimeric monoclonal antibody): 375 mg/weekly for 1 to 4 doses 25. Side effects such as fulminant myocarditis, pulmonary fibrosis, fatal Pneumocystis jirovecii infections, ulcerative colitis, and allergic reactions 3.
Edema is managed by dietary salt restriction and diuretics, either administered orally or intravenously.
- Cholesterol-reducing medications. Medications called statins can help lower cholesterol levels. However, it’s currently unclear whether or not cholesterol-lowering medications can specifically improve the outcomes of people with nephrotic syndrome, such as avoiding heart attacks or decreasing the risk of early death. Statins include atorvastatin (Lipitor), fluvastatin (Lescol), lovastatin (Altoprev), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor).
- Blood thinners. Medications called anticoagulants help decrease your blood’s ability to clot and may be prescribed if you’ve had a blood clot to reduce your risk of future blood clots. Anticoagulants include heparin, warfarin (Coumadin, Jantoven), dabigatran (Pradaxa), apixaban (Eliquis) and rivaroxaban (Xarelto).
Swelling may be treated with:
- Angiotensin-converting-enzyme inhibitor (ACE inhibitor) medicines. Medications in this category include benazepril (Lotensin), captopril and enalapril (Vasotec). Another group of drugs that works in a similar way is called angiotensin 2 receptor blockers (ARBs) and includes losartan (Cozaar) and valsartan (Diovan). Other medications, such as renin inhibitors, also may be used, though ACE inhibitors and angiotensin 2 receptor blockers are generally used first.
- Dietary salt restriction. Limit sodium (salt) in your diet
- Blood pressure control
- Diuretics (water pills). Water pills (diuretics) help control swelling by increasing your kidneys’ fluid output. Diuretic medications typically include furosemide (Lasix). Others may include spironolactone (Aldactone) and thiazides, such as hydrochlorothiazide.
How is minimal change disease treated in adults?
The treatment for nephrotic syndrome in adults with minimal change disease is usually with a type of drug called a corticosteroid, often called steroids. You may notice that you start getting better within weeks, or less, although it may take an adult longer to respond than a child. It is important to stick with your treatment plan until all medications are finished; even if your symptoms go away sooner
If you are a woman and want to have children, you should speak with your healthcare provider to see how the medicines you are given affect this process.
For symptoms of swelling (edema), your healthcare provider may give you:
- ACE inhibitor or angiotensin 2 receptor blocker (ARB) medicines
- Diuretics (water pills)
- Limit sodium (salt) in your diet
Minimal change disease diet
Changes to your diet may help you cope with nephrotic syndrome. Your doctor may refer you to a dietitian to discuss how what you eat can help you cope with the complications of nephrotic syndrome. A dietitian may recommend that you:
- Choose lean sources of protein
- Reduce the amount of fat and cholesterol in your diet to help control your blood cholesterol levels
- Eat a low-salt diet to help control the swelling (edema) you experience
- Limit foods that increase blood sugar levels when taking medications that can lead to weight gain, such as steroids
Some people with nephrotic syndrome may also be deficient in the mineral zinc. A recent study showed treatment with zinc supplements in children under 18 improved nephrotic syndrome. But always check with your doctor before giving your child a supplement or taking one yourself to avoid any potential adverse interactions.
Minimal change disease relapse
Other medications that may be used in instances of minimal change disease recurrence include those that are used to treat certain types of cancer (cyclophosphamide, chlorambucil, rituximab) and those that suppress the immune system (cyclosporine, tacrolimus, azathioprine, mycophenolate mofetil) 13.
Minimal change disease prognosis
Before the use of steroids became standard in the 1960’s, there was a high mortality in children with minimal change disease due to infection, as antibodies are lost in urine and this produces immunodeficiency. As discussed below, most patients respond to steroids and have an excellent long-term prognosis. In those who are steroid-resistant, a renal biopsy may subsequently show focal segmental glomerulosclerosis, which has a worse prognosis (more likely to progress to end-stage kidney disease). Spontaneous remissions (occurring without specific therapy) also occur.
Children usually respond better to corticosteroids than adults. Children often respond within the first month 3.
A relapse can occur. The condition may improve after long-term treatment with corticosteroids and medicines that suppress the immune system (immunosuppressive medicines).
In individuals who are not treated, there is an increased risk for infection and blood clotting events. About 5-10% of untreated adults may have spontaneous remission (resolution) of disease within a few months.
One major indication of the long-term outcome of minimal change disease is the initial response to corticosteroid treatment. About 80-95% of adults with minimal change disease who receive treatment via corticosteroids experience complete remission of symptoms. About half of all adults treated for minimal change disease have remission within four weeks, while 10-25% require longer treatment. minimal change disease may recur or relapse in about half of all adults. This usually occurs within one year of treatment 26.
Despite the potential for minimal change disease to recur, the occurrence of kidney failure and end stage renal disease is rare 13. Progression to renal failure occurs in < 5 % of patients and is more common among those who do not initially respond to corticosteroids 14.
References- Teh YM, Lim SK, Jusoh N, Osman K, Mualif SA. CD80 Insights as Therapeutic Target in the Current and Future Treatment Options of Frequent-Relapse Minimal Change Disease. Biomed Res Int. 2021 Jan 6;2021:6671552. doi: 10.1155/2021/6671552
- Zamora G, Pearson-Shaver AL. Minimal Change Disease. [Updated 2023 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560639
- Vivarelli M, Massella L, Ruggiero B, Emma F. Minimal Change Disease. Clin J Am Soc Nephrol. 2017 Feb 7;12(2):332-345. doi: 10.2215/CJN.05000516
- Nephrotic Syndrome. https://www.merckmanuals.com/home/kidney-and-urinary-tract-disorders/kidney-filtering-disorders/nephrotic-syndrome
- Waldman M, Crew RJ, Valeri A, Busch J, Stokes B, Markowitz G, D’Agati V, Appel G. Adult minimal-change disease: clinical characteristics, treatment, and outcomes. Clin J Am Soc Nephrol. 2007 May;2(3):445-53. doi: 10.2215/CJN.03531006
- Eddy AA, Symons JM. Nephrotic syndrome in childhood. Lancet. 2003 Aug 23;362(9384):629-39. doi: 10.1016/S0140-6736(03)14184-0
- Hogg RJ, Portman RJ, Milliner D, Lemley KV, Eddy A, Ingelfinger J. Evaluation and management of proteinuria and nephrotic syndrome in children: recommendations from a pediatric nephrology panel established at the National Kidney Foundation conference on proteinuria, albuminuria, risk, assessment, detection, and elimination (PARADE). Pediatrics. 2000 Jun;105(6):1242-9. doi: 10.1542/peds.105.6.1242
- Gdadegesin R, Smoyer WE: Nephrotic syndrome. In: Comprehensive Pediatric Nephrology, edited by Geary DF, Scaefer F, Philadelphia, Mosby Elsevier, 2008, pp 205–218.
- Avner ED, Harmon WE, Niaudet P, Yoshikawa N, Emma F, Goldstein SL: Idiopathic Nephrotic Syndrome in Children: Clinical Aspects. Pediatric Nephrology, 7th Ed., Berlin, Springer, 2016, pp 2730
- Mathieson PW. Immune dysregulation in minimal change nephropathy. Nephrol Dial Transplant. 2003 Aug;18 Suppl 6:vi26-9. doi: 10.1093/ndt/gfg1066
- Elie V, Fakhoury M, Deschênes G, Jacqz-Aigrain E. Physiopathology of idiopathic nephrotic syndrome: lessons from glucocorticoids and epigenetic perspectives. Pediatr Nephrol. 2012 Aug;27(8):1249-56. doi: 10.1007/s00467-011-1947-1
- Shalhoub RJ. Pathogenesis of lipoid nephrosis: a disorder of T-cell function. Lancet. 1974 Sep 7;2(7880):556-60. doi: 10.1016/s0140-6736(74)91880-7
- Minimal-Change Disease. https://emedicine.medscape.com/article/243348-overview
- Tarshish P, Tobin JN, Bernstein J, Edelmann CM Jr. Prognostic significance of the early course of minimal change nephrotic syndrome: report of the International Study of Kidney Disease in Children. J Am Soc Nephrol. 1997 May;8(5):769-76. doi: 10.1681/ASN.V85769
- Nachman PH, Jennette JC, Falk RJ: Primary glomerular disease. In: The Kidney, 8th Ed., edited by Brenner BM, Philadelphia, Saunders Elsevier, 2008, pp 987–1066.
- Avner ED, Harmon WE, Niaudet P, Yoshikawa N, Emma F, Goldstein SL: Idiopathic Nephrotic Syndrome in Children: Clinical Aspects. Pediatric Nephrology, 7th Ed., Berlin, Springer, 2016, pp 2730.
- Downie ML, Gallibois C, Parekh RS, Noone DG. Nephrotic syndrome in infants and children: pathophysiology and management. Paediatr Int Child Health. 2017 Nov;37(4):248-258. doi: 10.1080/20469047.2017.1374003
- Bertelli R, Bonanni A, Caridi G, Canepa A, Ghiggeri GM. Molecular and Cellular Mechanisms for Proteinuria in Minimal Change Disease. Front Med (Lausanne). 2018 Jun 11;5:170. doi: 10.3389/fmed.2018.00170
- Frank C, Herrmann M, Fernandez S, Dirnecker D, Böswald M, Kolowos W, Ruder H, Haas JP. Dominant T cells in idiopathic nephrotic syndrome of childhood. Kidney Int. 2000 Feb;57(2):510-7. doi: 10.1046/j.1523-1755.2000.00870.x
- Fiser RT, Arnold WC, Charlton RK, Steele RW, Childress SH, Shirkey B. T-lymphocyte subsets in nephrotic syndrome. Kidney Int. 1991 Nov;40(5):913-6. doi: 10.1038/ki.1991.293
- Cara-Fuentes G, Clapp WL, Johnson RJ, Garin EH. Pathogenesis of proteinuria in idiopathic minimal change disease: molecular mechanisms. Pediatr Nephrol. 2016 Dec;31(12):2179-2189. doi: 10.1007/s00467-016-3379-4
- Minimal Change Disease. https://www.msdmanuals.com/professional/genitourinary-disorders/glomerular-disorders/minimal-change-disease
- Hogan J, Radhakrishnan J. The treatment of minimal change disease in adults. J Am Soc Nephrol. 2013 Apr;24(5):702-11. doi: 10.1681/ASN.2012070734
- Lombel RM, Gipson DS, Hodson EM; Kidney Disease: Improving Global Outcomes. Treatment of steroid-sensitive nephrotic syndrome: new guidelines from KDIGO. Pediatr Nephrol. 2013 Mar;28(3):415-26. doi: 10.1007/s00467-012-2310-x
- Munyentwali H, Bouachi K, Audard V, Remy P, Lang P, Mojaat R, Deschênes G, Ronco PM, Plaisier EM, Dahan KY. Rituximab is an efficient and safe treatment in adults with steroid-dependent minimal change disease. Kidney Int. 2013 Mar;83(3):511-6. doi: 10.1038/ki.2012.444
- Treatment of minimal change disease in adults. https://www.uptodate.com/contents/treatment-of-minimal-change-disease-in-adults





{kind=link}