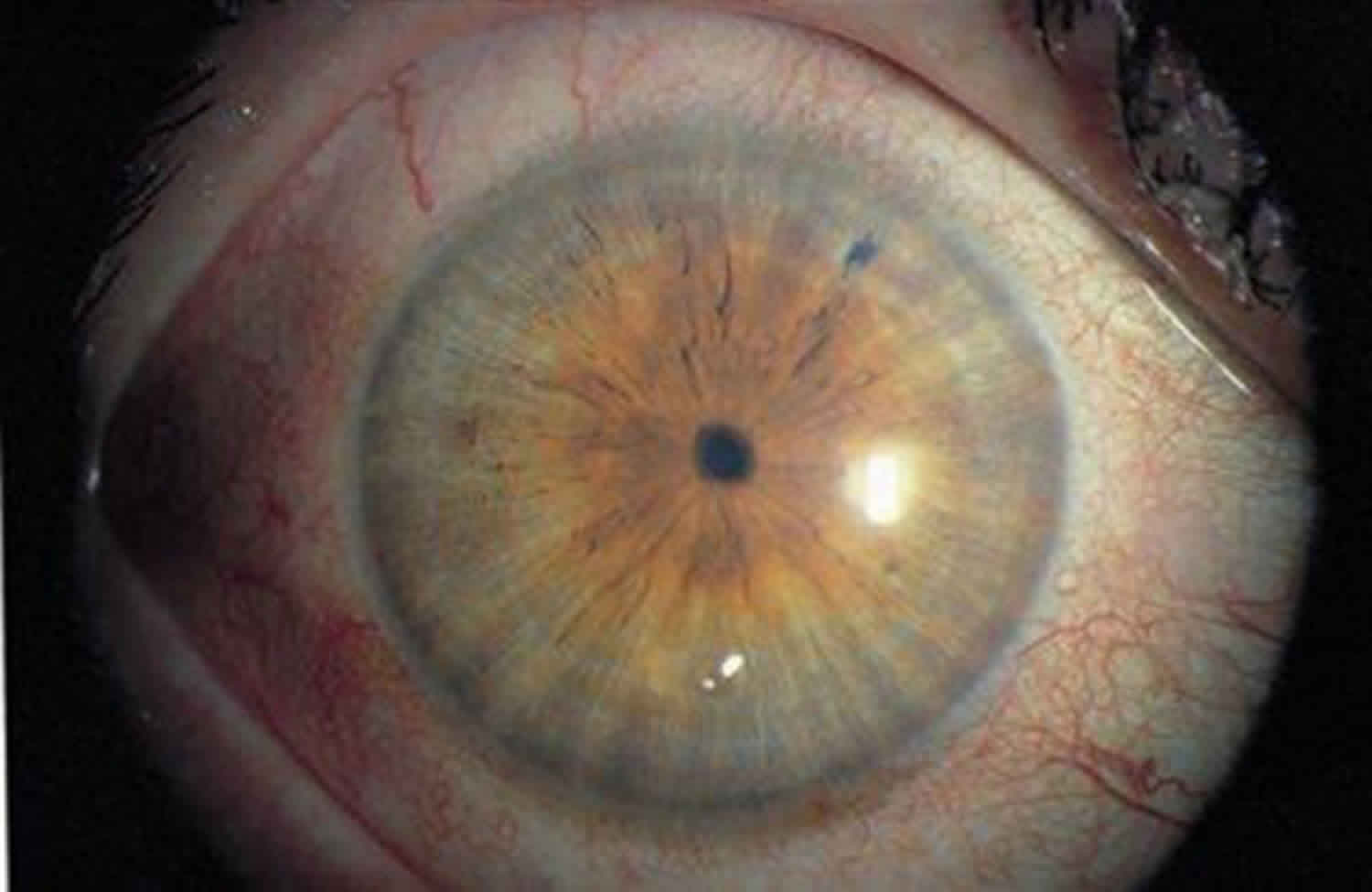
Miosis
Miosis is a medical term for constriction of the pupil. It is the opposite of mydriasis. It is seen in a variety of medical conditions, and can also be caused by certain drugs and chemicals. Eye drops used to intentionally cause miosis are known as “miotics”. Extreme miosis is commonly called “pinpoint pupils”, a situation that can be caused by use of opiates.
There are two types of muscle that control the size of the iris: circular muscle and radial muscle (Figures 1 and 2). The circular muscle is innervated by the parasympathetic nervous system, the radial muscle by the sympathetic nervous system. Parasympathetic stimulation cause contraction of the circular muscle and constriction of the iris known as miosis. Conversely, sympathetic stimulation of α1 adrenergic receptors causes the contraction of the radial muscle, and subsequent dilation of the pupil (mydriasis).
Visual stimuli enters the eye and through the retinal photoceptors is converted into an electric impulse, carried through the optic nerve (cranial nerve II) to the brain, where it connects to the pretectal nucleus of the high midbrain. It bypasses the lateral geniculate nucleus and the primary visual cortex. From the pretectal nucleus neurons send axons to neurons of the Edinger-Westphal nucleus whose visceromotor axons run along both the left and right oculomotor nerves. Visceromotor nerve axons (which constitute a portion of the III cranial nerve, along with the somatomotor portion derived from the Edinger-Westphal nucleus) synapse on ciliary ganglion neurons, whose parasympathetic axons innervate the constrictor muscle of the iris, producing miosis.
Relevant anatomy
The pupil is innervated by sympathetic and parasympathetic fibers. Pupillary dilation is mediated by a three- neuron sympathetic pathway that originates in the hypothalamus.
First order (central) neuron
The first order (central) neuron descends caudally from the hypothalamus to the first synapse in the cervical spinal cord (C8-T2 level-also called the ciliospinal center of Budge). The descending sympathetic tract is in close proximity to other tracts and nuclei in the brainstem.
Second order (preganglionic) neuron
The second order (preganglionic) neuron destined for the head and neck exits the spinal cord and travels in the cervical sympathetic chain through the brachial plexus, over the pulmonary apex and synapses in the superior cervical ganglion. The superior cervical ganglion is located near the angle of the mandible and bifurcation of the common carotid artery.
Third order (postganglionic) neuron
The third order (postganglionic) neuron for the orbit enters the cranium within the adventitia of the internal carotid artery into the cavernous sinus. Here the oculosympathetic fibers exit the internal carotid artery in close proximity to the trigeminal ganglion and the sixth cranial nerve and join the 1st division of the trigeminal nerve to enter the orbit.
- The fibers (long ciliary nerve) innervate the dilator muscles of the iris and the smooth muscle (Müller’s muscle) in the upper and lower eyelid (inferior retractors).
- The vasomotor and sudomotor fibers to the face exit the superior cervical ganglion and ascend in the external carotid artery.
- Pupillary constriction is produced by parasympathetic (cholinergic) fibers that travel with the third cranial (oculomotor) nerve.
Figure 1. Ciliary muscles
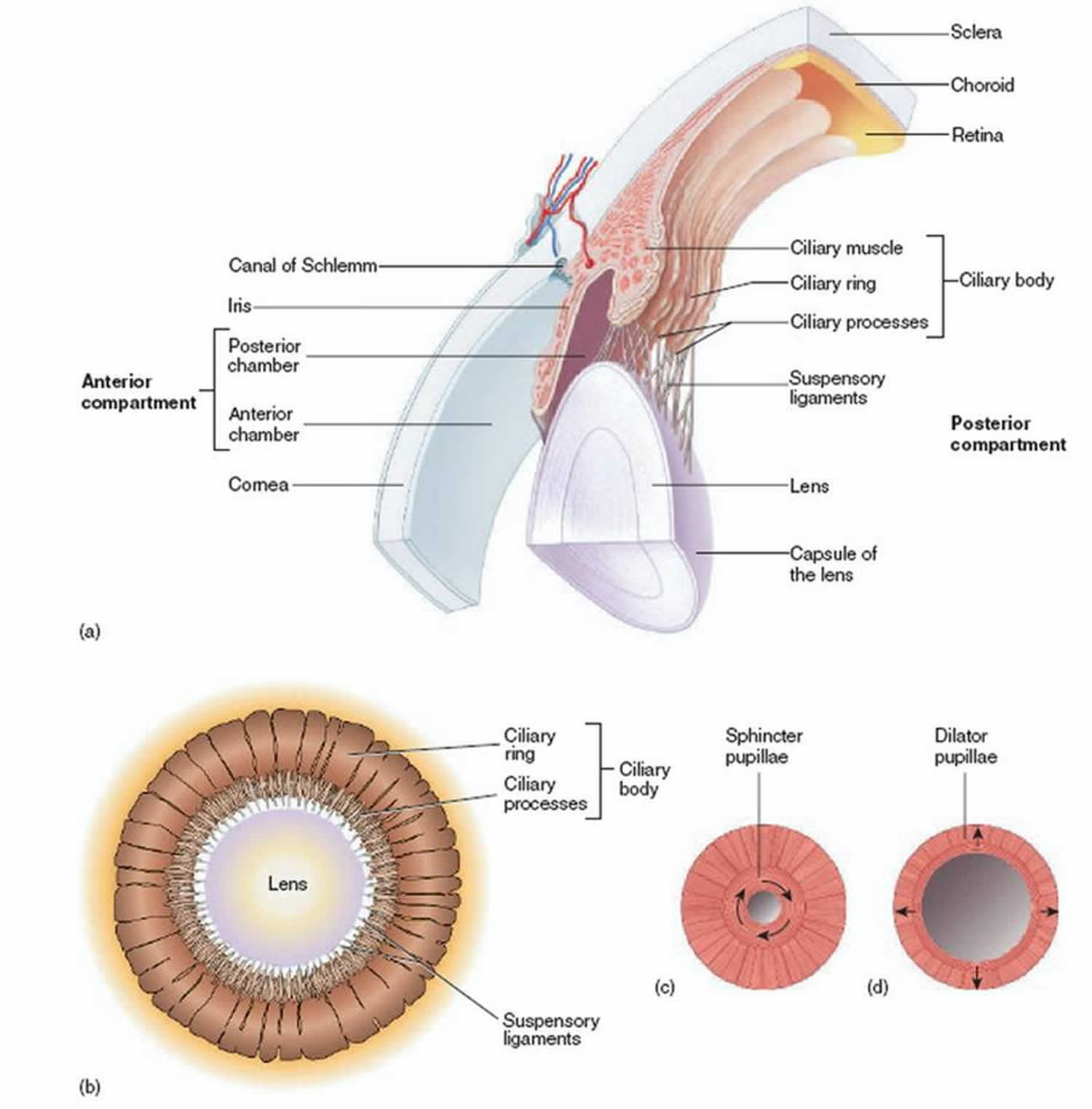
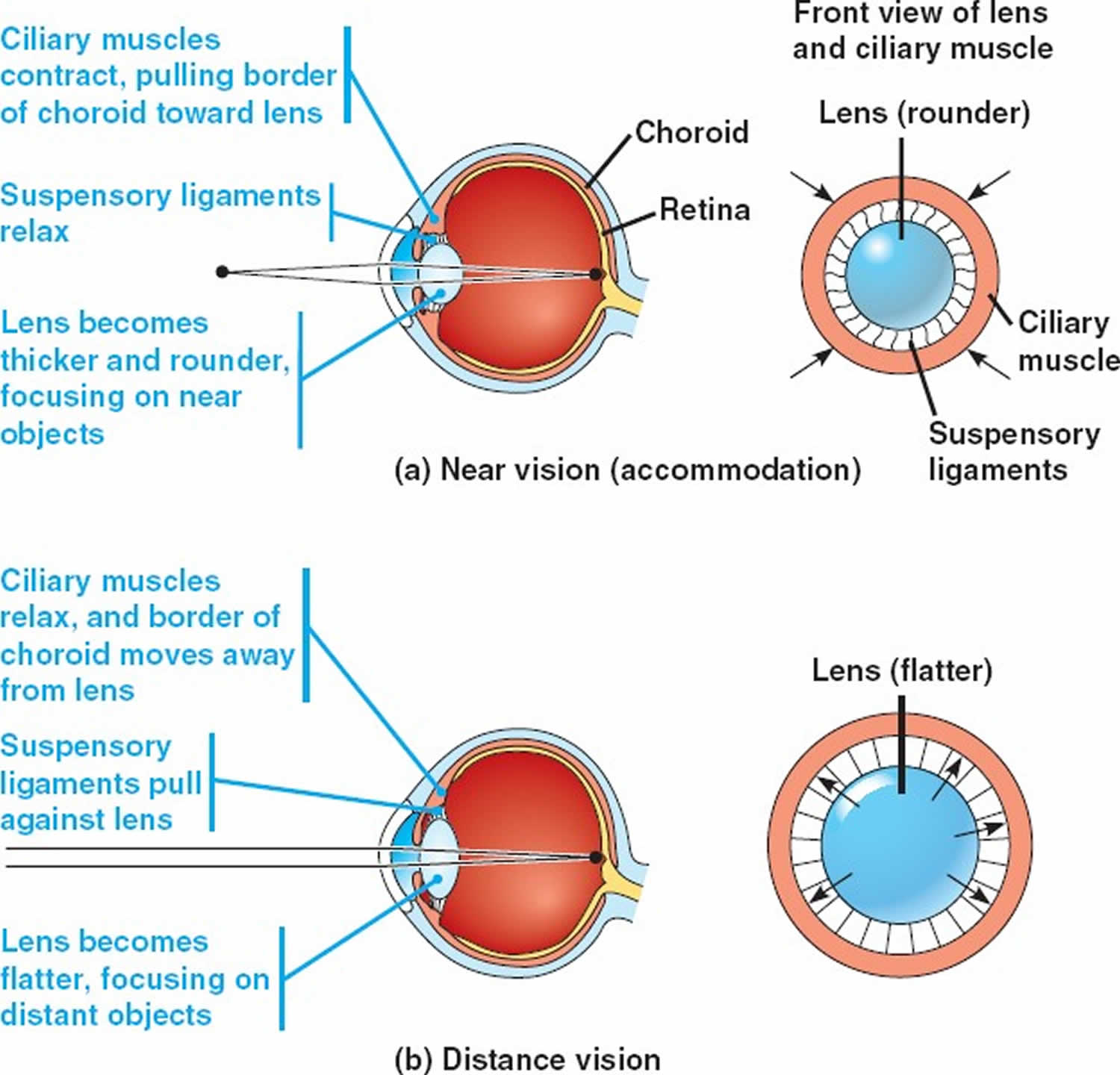
Figure 2. Ciliary muscles function
Miosis causes
Miosis is usually caused as a side effect from drugs intending to treat pain, as well as chemotherapy agents. Other common causes include various neurologic and ophthalmologic conditions.
Common causes of miosis:
- Acetaminophen
- Acetylcholine
- Acute iritis
- Adie’s pupil
- Ambenonium
- Anisocoria
- Argyll Robertson pupils
- Camptothecin derivatives
- Carbachol
- Carbamates
- Cerebrovascular arteriosclerosis
- Cluster headache
- Coma
- Corneal foreign body
- Corneal ulcer
- Chemotherapy
- Cholinergic agents
- Clonidine poisoning
- Codeine
- Dapiprazole
- Demerol
- Diamorphine
- Distigmine
- Donepezil toxicity
- Fatal familial insomnia
- Fentanyl
- Haloperidol
- Hereditary disorders
- Hereditary sensorimotor neuropathy type 3
- Heroin
- Horner’s syndrome
- Hyphema
- Intracranial hemorrhage
- Iridocyclitis
- Iritis
- Lateral medullary syndrome
- MAO inhibitors
- Methadone
- Migraine
- Miostat
- Miotics
- Mirtazapine
- Morphine
- Muscarine
- Mustard gas
- Naphazoline
- Neostigmine
- Neuropathy
- Nicotine
- Olanzapine
- Ondansetron
- Opioid poisoning
- Organophosphates
- Oxycodone
- Oxymetazoline
- Pancoast tumor
- Parasympathomimetics
- Pethidine
- Phencyclidine poisoning
- Phenoxybenzamine
- Physostigmine
- Pilocarpine
- Pontine hemorrhage
- Posterior iris synechiae
- Pyridostigmine
- Quetiapine
- Raeder paratrigeminal syndrome
- Stormorken syndrome
- Tacrine toxicity
- Tertiary syphillis
- Tetrahydazoline
- Thorazine
- Tramadol
- Trazodone
- Uveitis
- Wallenberg’s syndrome
Horner’s syndrome
Horner’s syndrome also called oculosympathetic paresis, or Horner syndrome, comprises a constellation of clinical signs including the classic triad of ptosis, miosis and anhidrosis. Horner’s syndrome results from a lesion to the sympathetic pathways that supply the head and neck region, including the oculosympathetic fibers. The causes of Horner’s syndrome varies with the age of the patient and site of the lesion. Prompt evaluation is necessary to detect and treat life-threatening conditions.
In a population based study of Horner’s syndrome in the pediatric age group, the incidence of Horner’s syndrome was estimated to be 1.42 per 100 000 patients younger than 19 years, with a birth prevalence of 1 in 6,250 for those with a congenital onset 1.
Horner syndrome causes
The cause of Horner’s syndrome varies with the patient age and site of lesion. The etiology remains unknown in 35-40% of cases.
Central (first order neuron) Horner’s syndrome
Central (first order neuron) Horner’s syndrome include lesions of the hypothalamus, brainstem and spinal cord such as stroke (classically the lateral medullary syndrome), demyelination (such as multiple sclerosis), neoplasms (such as glioma) or other processes such as a syrinx (syringomyelia or syringobulbia).
Preganglionic (second order neuron) Horner’s syndrome
Preganglionic (second order neuron) Horner’s syndrome include lesions of the thoracic outlet (cervical rib, subclavian artery aneurysm), mediastinum (mediastinal tumors), pulmonary apex (Pancoast’s tumor), neck (thyroid malignancies) or the thoracic spinal cord (trauma) or surgical procedures in this region including radical neck dissection, jugular vein cannulation, thoracoscopy or mediastinoscopy, chest tube placement and other thoracic surgical procedures.
Third order neuron or postganglionic lesion syndrome
Third order neuron or postganglionic lesion: These include lesions of the superior cervical ganglion (trauma, radical neck dissection or jugular vein ectasia), lesions of the internal carotid artery (ICA) in the neck and skull base (dissection, thrombosis, invasion by tumors or iatrogenic from endarterectomy or stenting, base of skull malignancies), lesions of internal carotid artery in the cavernous sinus (thrombosis, aneurysm, inflammation or invasive tumors) and lesions of the sellar and parasellar regions (invasive pituitary tumors, metastatic tumors, paratrigeminal tumors). Other causes include cluster headaches.
Children
In children, trauma (birth trauma or neck trauma) is the most common cause of Horner’s syndrome.
Other causes
Other causes include surgical trauma, neuroblastoma, brainstem lesions (such as vascular malformations, glioma and demyelination) and carotid artery thrombosis.
Horner’s syndrome symptoms
Isolated Horner’s syndrome
Isolated Horner’s: The patient, an acquaintance, or a health care provider may notice a difference in the palpebral aperture or pupillary size. Patients may also complain of ocular redness, nasal stuffiness and headache. Children with isolated Horner’s syndrome may present when parents notice a difference in eye color or impaired facial flushing.
Non-isolated Horner’s syndrome
Non-isolated Horner’s: Horner’s syndrome may accompany other neurologic or systemic deficits from disease processes listed above.
Horner’s syndrome diagnosis
Horner’s syndrome is diagnosed clinically by observing ptosis (of upper and lower lids), miosis of the ptotic eye and demonstration of dilation lag in the affected eye. Pharmacological confirmation tests can be performed in subtle cases.
Examination
Horner’s syndrome can be established clinically by an ocular examination. A targeted physical and neurological examination is a must to identify signs that may help localize the lesion and guide appropriate investigations.
Ocular signs
- Eyelids: patients have a mild (less than 2 mm) ptosis of upper lid and inverse ptosis of the lower lid (lower lid rests at a higher level than normal) which produces a decreased palpebral aperture compared to the fellow eye.
- Pupils: Patients have anisocoria (difference in the pupillary size) with the ptotic eye having the smaller pupil (miosis). The anisocoria is more prominent in the dark indicating pathology of the pupillary dilator. The smaller pupil takes a longer time to dilate when a bright source of light is moved away from the eye. This phenomenon is called dilation lag.
- Iris heterochromia (different colored irides) may be seen in children with congenital Horner’s syndrome.
- Extraocular movements may be affected in lesions of the brainstem or the cavernous sinus.
- Other signs of sympathetic denervation include ipsilateral conjunctival injection, changes in accommodation and lower intraocular pressure.
Neurologic signs
Neurologic signs may be present depending on the site of lesion
- Brainstem (bulbar) signs: ataxia, diplopia, nystagmus, lateralized weakness or numbness, hoarseness and dysphagia.
- Spinal cord (myelopathic) signs: sensory or motor abnomalities with a level, dysfunction of bowel or bladder movements, erectile dysfunction in men and spasticity.
- Brachial plexopathy: pain and weakness in the arm, or hand; abnormalities can be confirmed by nerve conduction studies and electromyography of the involved extremity.
- Cranial neuropathy (single or multiple cranial nerves) can be produced by lesions in the cavernous sinus or base of skull
Other signs
- Anhidrosis: Variable degree of loss of sweating can be seen depending on the site of lesion. Central or preganglionic lesions tend to produce more noticeable anhidrosis. The sudomotor and vasomotor fibers to most of the face separate out at the superior cervical ganglion and anhidrosis is often not noticeable in postganglionic lesions.
- Harlequin sign: Impaired hemi-facial (or hemi-body) flushing seen in children with sympathetic denervation to the face.
- Cervical or abdominal mass may be seen in children with neuroblastoma.
Pharmacologic tests
- Topical Cocaine may be used to confirm Horner’s syndrome in subtle cases. Cocaine blocks reuptake of the neurotransmitter norepinephrine from the synaptic cleft and will cause dilation of the pupil with intact sympathetic innervation. One hour after instillation of two drops of 10% cocaine, the normal pupil dilates more than the Horner’s pupil, thus increasing the degree of anisocoria. It is becoming increasingly difficult to obtain cocaine eye drops due to increased regulations.
- Topical Apraclonidine is an alternative to topical cocaine to confirm Horner’s syndrome. Apraclonidine is an alpha adrenergic agonist. It causes pupillary dilation in the Horner’s pupil due to denervation supersensitivity while producing a mild pupillary constriction in the normal pupil presumably by down-regulating the norepinephrine release at the synaptic cleft. A reversal of anisocoria after instilling two drops of 0.5% apraclonidine is suggestive of Horner’s syndrome.
- Topical Hydroxyamphetamine is used to differentiate pre and postganglioninc Horner’s. Hydroxyamphetamine causes a release of norepinephrine from intact adrenergic nerve endings causing pupillary dilation. One hour after instillation of 1% hydroxyamphetamine eye drops dilation of both pupils indicate a lesion of the 1st or 2nd order neuron. If the smaller pupil fails to dilate it indicates a lesion of the 3rd order or postganglionic neuron.
Horner’s syndrome treatment
Acute onset of painful Horner’s syndrome should be considered a neurological emergency and subject should be evaluated for dissection of the internal carotid artery as described below. These patients are at increased risk for cerebral infarction.
The first step in the management of a patient with Horner’s syndrome is to perform appropriate studies to identify the cause. Imaging is often indicated in new onset Horner’s syndrome unless it occurs in the setting of trauma or surgical manipulation. High-yield sites of imaging can be identified based on accompanying signs and symptoms. These may include amongst others radiologic evaluation of brain, cervical spinal cord, cerebral vasculature, head, neck and thorax. Treatment depends on the etiology of Horner’s syndrome.
- Carotid artery dissection: Appropriate imaging modalities should be obtained emergently and may include MRI and MR angiography or CT angiography of the neck. Conventional angiogram remains the gold standard. Patients should be treated promptly by anticoagulation under the supervision of a neurologist.
- Neuroblastoma: Children with new Horner’s syndrome without obvious cause such as trauma should be evaluated for systemic malignancy particularly neuroblastoma with the help of the pediatrician. They should be evaluated for neck and abdominal masses and tested for urinary catecholamine metabolites. Appropriate radiological evaluation of head, neck and chest should be obtained in consultation with the pediatrician.
- Brainstem or myelopathic lesions: Patients with brainstem or myelopathic signs require imaging of the brain and the spinal cord typically by MR imaging. Appropriate sequences should be ordered based on the suspected etiology. Cavernous sinus and sellar region should be evaluated in patients with Horner’s syndrome with ophthalmoparesis especially isolated sixth cranial nerve palsy. These patients should be under the care of a neurologist or neurosurgeon for treatment of the underlying causes.
- Thoracic malignancy: Isolated spontaneous onset Horner without additional neurologic signs should prompt imaging of the neck and thorax for lesions of the pulmonary apex or the paravertebral area. Contrasted CT or MR scans should be obtained based on the suspected etiology.
- Blepharoptosis: Once life-threatening conditions have been ruled out and the patient is stable, visually symptomatic ptosis can be managed surgically. The surgical approach varies on surgeon preference. Since characteristically the levator palpebrae function is normal in Horner’s syndrome, surgery typically involves strengthening the action of the levator muscle. The approach may include either aponeurotic advancement or Müller’s muscle- conjunctival resection.
Follow up
Follow up of Horner’s syndrome depends on the etiology of Horner’s syndrome
Horner’s syndrome prognosis
Prognosis depends on the etiology of Horner’s syndrome
Miosis treatment
Miosis treatment involves treating the underlying cause.
References




{kind=link}