
What is neuropathic pain
Neuropathic pain also called nerve pain, is caused by damage or injury to somatosensory nervous system including peripheral fibers (Aβ, Aδ and C fibers) and central neurons from conditions like shingles, diabetes, stroke and HIV 1. Neuropathic pain affects 7–10% of the general population. The International Association for the Study of Pain (IASP) Special Interest Group on Neuropathic Pain (NeuPSIG) in 2008 defined neuropathic pain as “pain arising as a direct consequence of a lesion or disease affecting the somatosensory system” 2. A slightly modified version of this definition was proposed by the International Association for the Study of Pain (IASP) Taxonomy Committee and accepted by the IASP: “pain caused by a lesion or disease of the somatosensory nervous system” 3. The restriction to the somatosensory nervous system is important because conditions such as musculoskeletal pain (e.g., due to spasticity) arising indirectly from disorders of the motor system should not be confused with neuropathic pain 4. Narrowing the definition also excludes nervous system changes, such as central sensitization, as well as conditions such as fibromyalgia, chronic regional pain syndrome type 1 or irritable bowel syndrome (IBS) where there is little to find in terms of nerve damage 5.
Neuropathic pain is different from other types of pain and simple pain medicines have little effect. Medications are only partially effective in managing neuropathic pain. Using a whole-person approach, including addressing lifestyle factors, can help address patient perception of pain, improve coping and restore daily function. Promoting pain acceptance, adopting realistic expectations for good pain management and integrating coping strategies as part of a management plan is important in helping patients live with their neuropathic pain.
Chronic neuropathic pain is more frequent in women (8% versus 5.7% in men) and in patients >50 years of age (8.9% versus 5.6% in those <49 years of age), and most commonly affects the lower back and lower limbs, neck and upper limbs 6. Lumbar and cervical painful radiculopathies are probably the most frequent cause of chronic neuropathic pain. Consistent with these data, a survey of >12,000 patients with chronic pain with both nociceptive and neuropathic pain types, referred to pain specialists in Germany, revealed that 40% of all patients experience at least some characteristics of neuropathic pain (such as burning sensations, numbness and tingling); patients with chronic back pain and radiculopathy were particularly affected 7.
Recognizing the challenges of determining the presence of neuropathic pain according to this new definition, International Association for the Study of Pain (IASP) Special Interest Group on Neuropathic Pain (NeuPSIG) also proposed a grading system 2 to guide decisions on the level of certainty with which neuropathic pain can be determined in an individual patient. Three levels of certainty—possible, probable, and definite neuropathic pain—were proposed. As an activity in the Global Year Against Neuropathic Pain 8, NeuPSIG established a committee to (1) critically evaluate the use of the grading system in the 7 years after its publication, (2) assess the usefulness and limitations of the grading system, and (3) update the grading system if required, for improved application in clinical and research settings. The committee consisted of an expert panel of neurologists, clinical neurophysiologists, neuroscientists, anesthesiologists, pain specialists, primary care physicians, and population health scientists 4.
The neuropathic pain grading system is intended for determining the level of certainty with which the pain in question is neuropathic pain 4. A finding of probable neuropathic pain in a given individual patient should prompt consideration of treatment according to the neuropathic pain treatment guidelines 9, but the grading system is not intended for medico-legal purposes or to classify diseases. The refinements in the present grading system (Figure 1) follow the classical clinical method of diagnosis in that history, clinical examination, and diagnostic tests stepwise add to level of certainty that the pain in question is neuropathic pain 4.
Commonly used pharmacological treatments include antidepressants (tricyclic antidepressants [TCAs], selective serotonin reuptake inhibitors [SSRIs] and serotonin–norepinephrine reuptake inhibitors [SNRIs]), antiepileptic (anticonvulsant) drugs, topical treatments and opioid analgesics. In addition to their potential benefits, all of these drug classes are associated with various adverse effects. Nonpharmacological approaches include cognitive-behavioral therapy, hypnosis, and neurostimulation therapies.
Figure 1. Neuropathic pain grading system
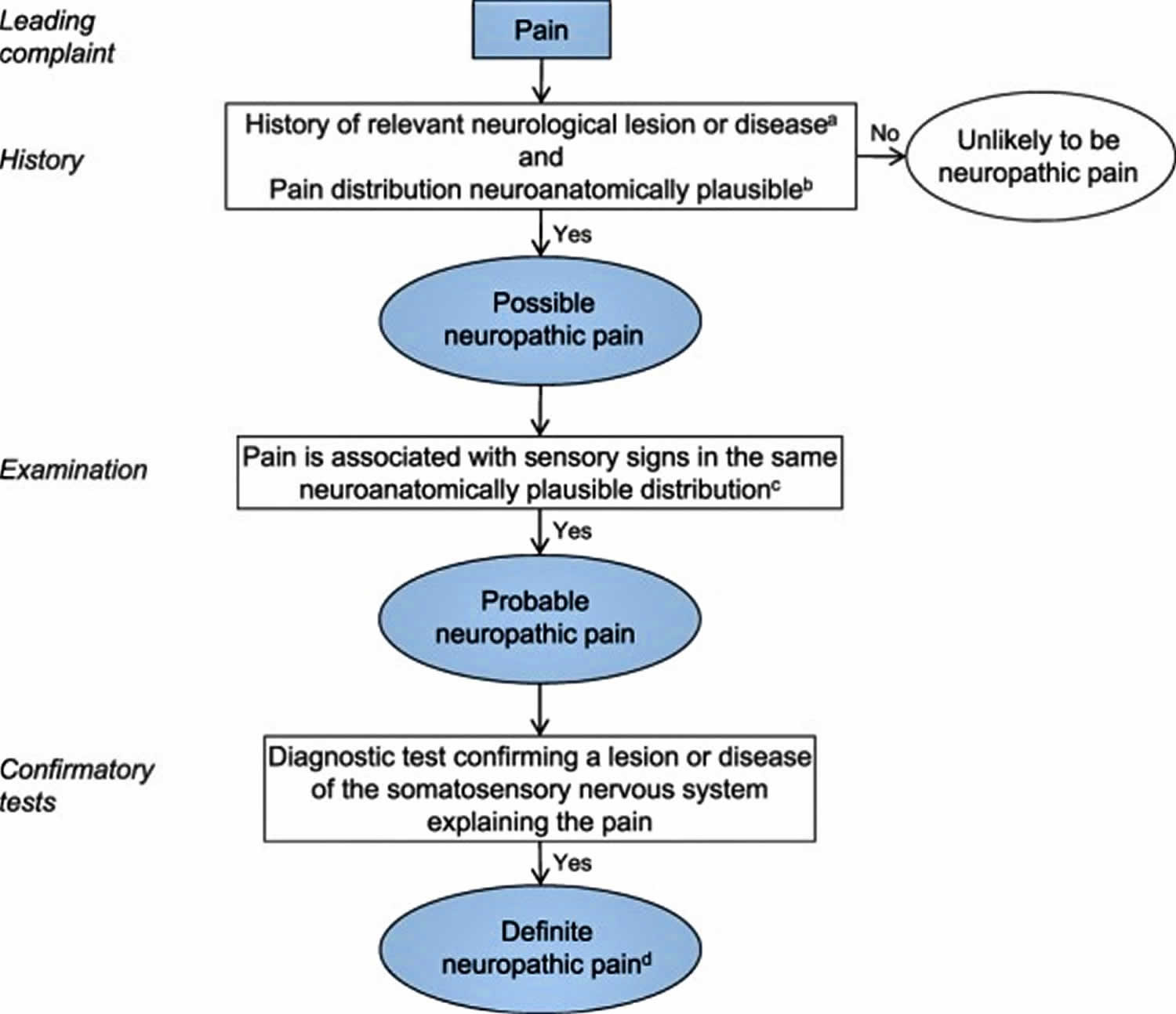
Footnote: Flow chart of updated grading system for neuropathic pain. (a) History, including pain descriptors, the presence of nonpainful sensory symptoms, and aggravating and alleviating factors, suggestive of pain being related to a neurological lesion and not other causes such as inflammation or non-neural tissue damage. The suspected lesion or disease is reported to be associated with neuropathic pain, including a temporal and spatial relationship representative of the condition; includes paroxysmal pain in trigeminal neuralgia. (b) The pain distribution reported by the patient is consistent with the suspected lesion or disease (Table 1). (c) The area of sensory changes may extend beyond, be within, or overlap with the area of pain. Sensory loss is generally required but touch-evoked or thermal allodynia may be the only finding at bedside examination. Trigger phenomena in trigeminal neuralgia may be counted as sensory signs. In some cases, sensory signs may be difficult to demonstrate although the nature of the lesion or disease is confirmed; for these cases the level “probable” continues to be appropriate, if a diagnostic test confirms the lesion or disease of the somatosensory nervous system. (d) The term “definite” in this context means “probable neuropathic pain with confirmatory tests” because the location and nature of the lesion or disease have been confirmed to be able to explain the pain. “Definite” neuropathic pain is a pain that is fully compatible with neuropathic pain, but it does not necessarily establish causality.
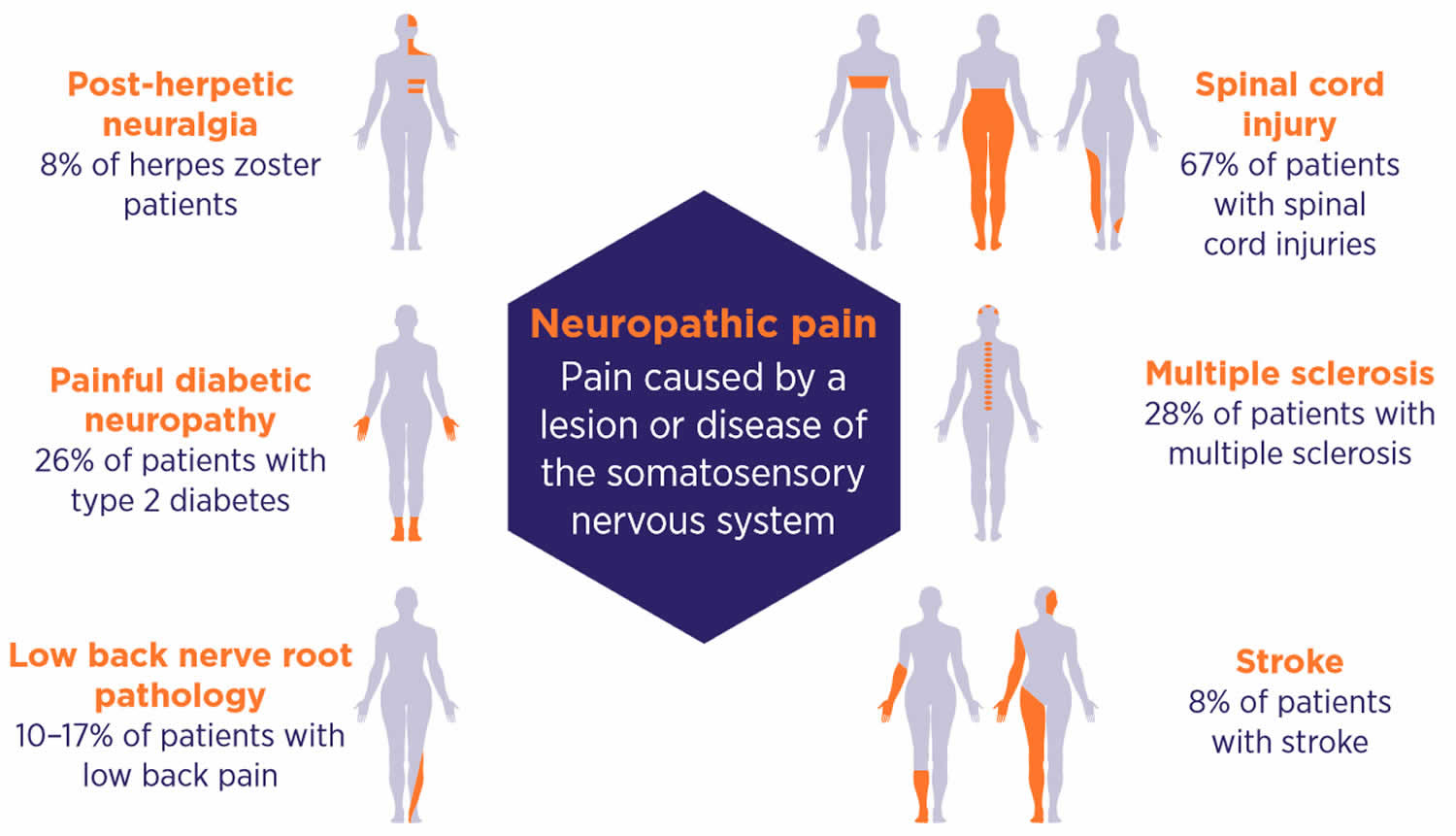
[Source 4 ]Figure 2. Types of neuropathic pain
Neuropathic pain key points
- The updated, narrower definition of neuropathic pain emphasizes its association with a lesion or disease of the somatosensory nervous system.
- Neuropathic and nociceptive pain have different treatments. A targeted history and a physical examination are important diagnostic prerequisites to medicine selection for effective pain management.
- Recognize that the differential diagnosis of neuropathic pain is crucial because it requires a different therapeutic approach from nociceptive pain.
- Use a targeted history and physical examination, and consider a validated screening tool (e.g., DN4 or Douleur Neuropathique en 4 questions) to make an accurate diagnosis of neuropathic pain.
- Low-dose amitriptyline remains a first-line contender in the treatment of neuropathic pain.
- Optimize the benefits of neuropathic pain medicines with the lowest possible starting dosages, up-titrating gradually and an adequate trial period.
- Recognize that medicines will often have limited efficacy for your patient and non-pharmacological strategies play a key role in coping.
Types of neuropathic pain
- Central poststroke pain
- Central neuropathic pain associated with multiple sclerosis
- Neuropathic pain associated with spinal cord injury
- Painful diabetic neuropathy. Painful chronic neuropathy in patients with diabetes mellitus ranges from 10% to 26% 10.
- Painful polyneuropathy
- Painful radiculopathy
- Peripheral nerve injury pain
- Postamputation pain
- Postherpetic neuralgia
- Trigeminal neuralgia
Causes of neuropathic pain
Neuropathic pain is a term used for a group of conditions with a wide range of causes and different pain distributions. However, all these conditions are characterized by a lesion or disease affecting the somatosensory nervous system peripherally or centrally.
Common causes for neural damage and subsequent neuropathic pain 11:
- Chemical irritation
- Chronic kidney disease
- Connective tissue disease
- Diabetes
- Entrapment or pressure on nerves by nearby bones, ligaments, blood vessels, or tumors
- Infections, such as herpes zoster (shingles), HIV/AIDS, Lyme disease, and syphilis
- Ischemia
- Malignancy
- Medicines such as cisplatin, paclitaxel, or vincristine
- Metabolic disease
- Porphyria (blood disorder)
- Toxins
- Trauma (including surgery)
In many cases, the cause is unknown. Neuropathic pain may develop without any identifiable cause (e.g., intercostal neuralgia,idiopathic polyneuropathy).
Postherpetic neuropathic pain and trigeminal neuropathic pain are the two most common forms of neuropathic pain. A related but less common neuropathic pain affects the glossopharyngeal nerve, which provides feeling to the throat.
Neuropathic pain is more common in older people, but it may occur at any age.
Neuropathic pain may be the first manifestation of a systemic disease.
Neuropathic pain pathogenesis:
- Central sensitization and ongoing discharges in central pain pathways contribute to the development of central pain.
- Spontaneous activity occurring in dorsal horn and other central neurons, disinhibited polysynaptic pathways, and sensitized spinothalamic tract pathways are possible substrates for central pain. In addition, changes occurring at supraspinal areas such as the thalamus, the anterior cingulate cortex, and prefrontal cortices may be involved in the generation, amplification, or modification of central neuropathic pain.
Central neuropathic pain is due to a lesion or disease of the spinal cord and/or brain 1. Cerebrovascular disease affecting the central somatosensory pathways (poststroke pain) and neurodegenerative diseases (notably Parkinson disease) are brain disorders that often cause central neuropathic pain 12. Spinal cord lesions or diseases that cause neuropathic pain include spinal cord injury, syringomyelia and demyelinating diseases, such as multiple sclerosis, transverse myelitis and neuromyelitis optica 13. By contrast, the pathology of the peripheral disorders that cause neuropathic pain predominantly involves the small unmyelinated C fibres and the myelinated A fibers, namely, the Aβ and Aδ fibers 4. Peripheral neuropathic pain will probably become more common because of the ageing global population, increased incidence of diabetes mellitus and the increasing rates of cancer and the consequence of chemotherapy, which affect all sensory fibres (Aβ, Aδ and C fibres). Peripheral neuropathic pain disorders can be subdivided into those that have a generalized (usually symmetrical) distribution and those that have a focal distribution (see Figure 3 below). The most clinically important painful generalized peripheral neuropathies include those associated with diabetes mellitus, pre-diabetes and other metabolic dysfunctions, infectious diseases mainly HIV infection 14 and leprosy 15, chemotherapy, immune (for example, Guillain-Barre syndrome) and inflammatory disorders, inherited neuropathies and channelopathies (such as inherited erythromelalgia, a disorder in which blood vessels are episodically blocked then become hyperaemic and inflamed).
Neuropathic pain symptoms
Burning, shooting and pins and needles descriptors can alert doctors to the possibility of neuropathic pain. Then the clinical history and examination helps to confirm that the location of the pain is anatomically consistent with a neurological lesion.
Neuropathic pain symptoms may include any of the following:
- Increased sensitivity of the skin along the path of the damaged nerve, so that any touch or pressure is felt as pain
- Pain along the path of the nerve that is sharp or stabbing, in the same location each episode, comes and goes (intermittent) or is constant and burning, and may get worse when the area is moved
- Weakness or complete paralysis of muscles supplied by the same nerve
Clinical features:
- Central pain can be spontaneous or stimulus-evoked and may involve dynamic mechanical allodynia and cold allodynia. Pain may be described in terms such as burning, pricking, shooting, squeezing, and painful cold. Central pain occurs in approximately 8% of patients with stroke, 25% of patients with multiple sclerosis, and 40–50% of patients with spinal cord injury. Early sensory hypersensitivity seems to predict the development of central pain. Little is known about other possible risk factors.
- Paresthesia and dysesthesia are common (e.g., tingling, pins and needles, cold, and pressing sensations).
- The distribution of pain can range from a small area to large areas, covering half of sethe body in stroke or the lower body in spinal cord injury. In patients with lateral medullary infarction, the pain can involve one side of the face and the contralateral side of the body or limbs, and periorbital pain is common. In spinal cord injury, neuropathic pain is classified as “at-level” pain, which is pain perceived in a segmental pattern at the level of injury, and “below-level” pain, which is pain felt below the injury level. The pain in multiple sclerosis has a distribution compatible with a brain or a spinal lesion.
- Central pain is located in areas with sensory abnormalities compatible with the central nervous system lesion.
- Central pain can occur immediately at disease onset or can be delayed for several months.
- Bedside clinical examination typically reveals altered pinprick sensation, decreased or increased sensation to touch and cold, and increased deep-tendon reflexes.
Guidelines 4 recommend a structured approach, with patient history and clinical examination being the most important parts of the diagnosis. Neuropathic pain can be graded as possible, probable or definite based on the built-up evidence (see Figure 1 above). Treatment can be commenced once probable neuropathic pain has been diagnosed 4, with further investigations only considered if these tests would inform treatment.
History is needed to reach a ‘possible’ level of certainty 4.
A history suggestive of a relevant neurological lesion (like herpes zoster or a traumatic nerve injury), pain descriptors (burning, shooting, pricking and pins and needles) or the presence of non-painful sensations like numbness or tingling are suggestive of neuropathic pain 4. Furthermore, the pain distribution should be explainable by a lesion or disease in the somatosensory system, or be typical of an underlying neuropathic disorder (see Figure 1) 4. Validated assessment tools 4 have been created to help in this assessment, but should not be used alone 4.
A clinical examination is needed to reach a ‘probable’ level of certainty 4.
Once the history suggests a possible diagnosis of neuropathic pain, tools such as toothpicks, brushes or cotton wool can be used in a clinical examination to detect clinically consistent sensory changes that help further differentiate neuropathic from non-neuropathic pain.2,13-5 Hypoalgesia to pinprick, hypoesthesia to tactile stimuli and allodynia to brush and cold are particularly discriminant.13,31 Sensory changes should also lie within a plausible neurological distribution (see Figure 2).
Confirmatory tests can be considered in order to reach a ‘definite’ level of certainty 4 if these tests would inform treatment. A ‘definite’ level of certainty is commonly not required in primary care.
Tests must confirm that a lesion or disease of the somatosensory system can explain the pain 4. These include magnetic resonance imaging (MRI) to confirm a stroke, multiple sclerosis or spinal cord injury and a skin biopsy showing reduced nerve fibre density 4.
Neuropathic pain diagnosis
Your health care provider will perform a physical exam, and ask about the symptoms.
The exam may show:
- Abnormal sensation in the skin
- Reflex problems
- Loss of muscle mass
- Lack of sweating (sweating is controlled by nerves)
- Tenderness along a nerve
- Trigger points (areas where even a slight touch triggers pain)
You may also need to see a dentist if the pain is in your face or jaw. A dental exam can rule out dental disorders that may cause facial pain (such as a tooth abscess).
Other symptoms (such as redness or swelling) may help rule out conditions such as infections, bone fractures, or rheumatoid arthritis.
There are no specific tests for neuropathic pain. But, the following tests may be done to find the cause of the pain:
- Blood tests to check blood sugar, kidney function, and other possible causes of neuropathic pain
- Magnetic resonance imaging (MRI)
- Nerve conduction study with electromyography
- Ultrasound
- Spinal tap (lumbar puncture)
Possible neuropathic pain
Evaluation of the patient according to the grading system should be undertaken if the patient’s history suggests that pain could be related to a neurological lesion or disease and not other causes such as inflammation or non-neural tissue damage. At this stage, pain descriptors, the presence of nonpainful sensory symptoms, and any aggravating and alleviating factors can be taken into account. Pain descriptions such as burning or hot, electric shocks or shooting, pricking or pins and needles, pain evoked by light touching or cold, and nonpainful sensations such as numbness and tingling are suggestive, but not pathognomonic for neuropathic pain, and other descriptors may apply as well 16. The combination of several descriptors, however, has a highly discriminant value and several screening tools (questionnaires) have been developed to identify patients who may have neuropathic pain to alert the clinician to undertake further assessment (though they cannot be used alone to identify neuropathic pain) 17. These include, but are not limited to the Leeds assessment of neuropathic symptoms and signs (LANSS) Pain Scale 18, the neuropathic pain questionnaire 19, the Douleur Neuropathique en 4 questions 20, the painDETECT 21 and ID-Pain 22.
Validated screening tools for neuropathic pain
Symptom and clinical examination items can be assessed using distinct validated screening tools. The most common tools are listed below.
Leeds Assessment of Neuropathic Symptoms and Signs (LANSS Pain Scale) 18:
- Four symptom items (pricking, tingling, pins and needles; electric shocks; hot or burning sensations; and pain evoked by light touching)
- One item related to skin appearance (mottled or red)
- Two clinical examination items (touch-evoked allodynia and altered pinprick sensation)
Douleur Neuropathique 4 questions 20:
- Seven symptom items (burning, painful cold, electric shocks, tingling, pins and needles, numbness and itching)
- Three clinical examination items (touch hypoaesthesia (reduced sense), pinprick hypoaesthesia and brush-evoked allodynia)
Neuropathic Pain Questionnaire 23:
- Seven sensory descriptors (burning pain, shooting pain, numbness, electrical-like sensations, tingling pain, squeezing pain and freezing pain)
- Three items related to provoking factors (overly sensitive to touch, touch-evoked pain and increased pain due to weather change)
- Two items describing affect (unpleasantness and overwhelming)
painDETECT 21:
- Seven weighted symptom items (burning, tingling or prickling, touch-evoked pain, electric shocks, temperature-evoked pain, numbness and pressure-evoked pain)
- Two items related to spatial (radiating pain) and temporal characteristics
ID Pain 22:
- Five symptom items (pins and needles, hot or burning, numbness, electrical shocks and touch-evoked pain)
- One item related to location (joints)
Neuropathic Pain Symptom Inventory 24:
- Ten descriptors (burning, pressure, squeezing, electrical shocks, stubbing, pain evoked by brushing, pain evoked by pressure, pain evoked by cold stimuli, pins and needles, and tingling)
- Two temporal items (the temporal sequence of spontaneous ongoing pain and paroxysmal pain)
- Five clinically relevant dimensions (evoked pain, paroxysmal pain, abnormal sensations, superficial and deep components of spontaneous ongoing pain)
The following two criteria need to be fulfilled to reach the first level of certainty-“possible” neuropathic pain.
When both requirements 1 and 2 of the pain history are fulfilled, the pain complaint may be termed possible neuropathic pain 4.
1) A history of relevant neurological lesion or disease
There should be a clinical suspicion of a relevant lesion or disease of the somatosensory nervous system (eg, an episode of acute herpes zoster or a traumatic nerve injury). The temporal relationship between the lesion or disease and the pain may vary, but a close temporal relationship helps strengthen the clinical suspicion. The onset of pain is usually immediate or within a few weeks of the lesion or disease but may be delayed for up to several months after injury (eg, after stroke) or for many years in conditions with an insidious onset such as diabetic neuropathy. In some cases, the history of pain or sensory disturbances by themselves suggest a disease, eg, in polyneuropathy (peripheral neuropathy), where the insidious onset of distal pain or numbness may be the only history indicating the disease. Characteristic sudden short-lasting (usually a few seconds) paroxysmal pain in the face, which may recur several times and may be separated by a refractory period (usually some minutes), suggests trigeminal neuralgia, where the pain is the only symptom indicating a relevant neurological disease.
2) Pain distribution neuroanatomically plausible
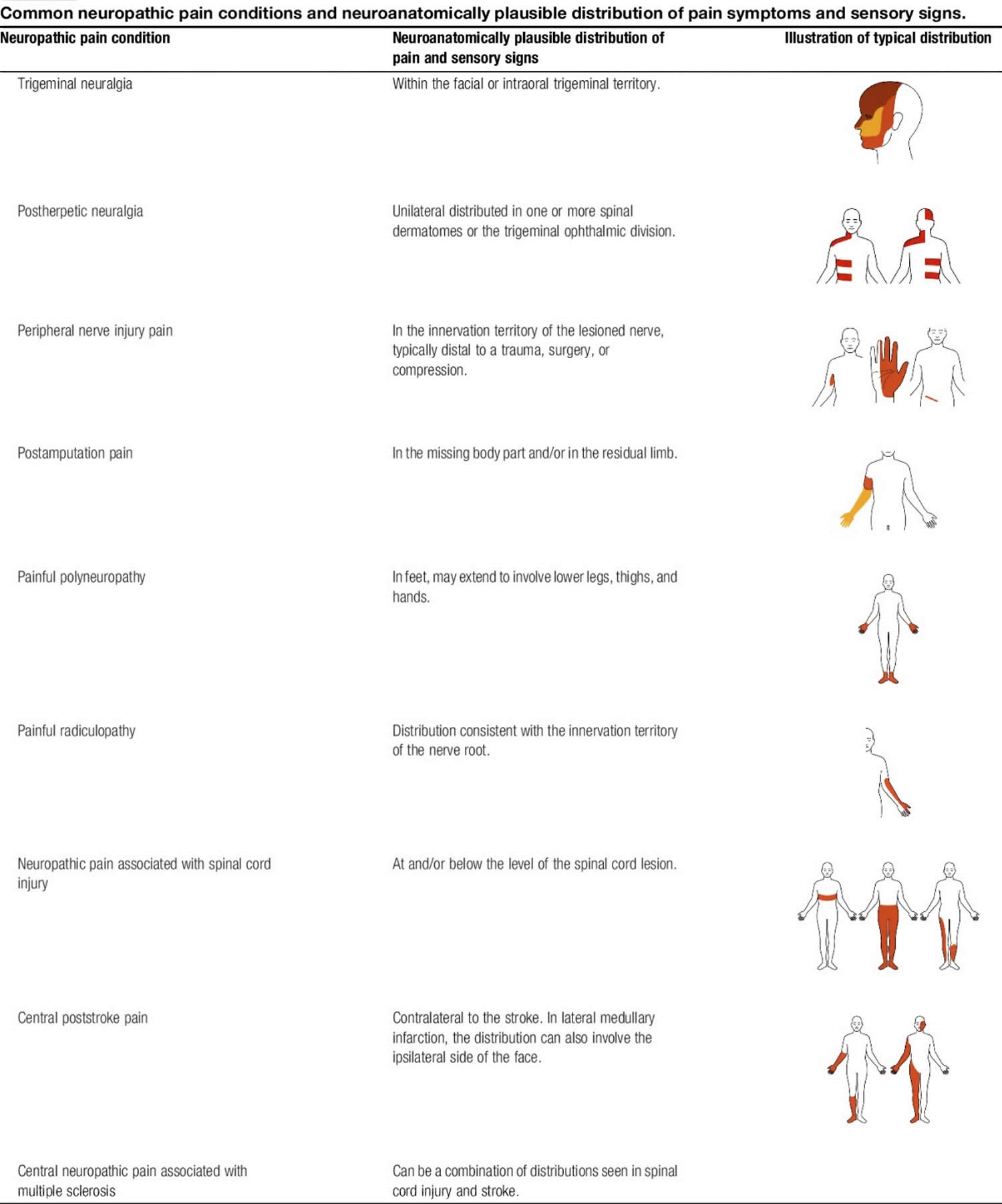
The pain distribution should be anatomically consistent with the suspected location of the lesion or disease in the peripheral or central somatosensory nervous system (as derived from the patient’s history). This can be difficult to decipher in the single patient, as the distribution of pain can occupy a smaller area or extend somewhat outside the innervation territory of a peripheral nerve or root or the somatotopic representation of the body within the central nervous system, but it should be in a distribution that is typical for the underlying disorder (see examples in Figure 3). In painful channelopathies, the pain distribution may be unusual but should be consistent with the disorder, eg, familial episodic pain syndrome, in which pain is mainly localized to the chest and upper arms, or inherited erythromelalgia, in which pain is localized to the extremities (feet and hands and in some cases ears).
Figure 3. Neuropathic pain distribution (common neuropathic pain conditions and neuroanatomically plausible distribution of pain symptoms and sensory signs)
Probable neuropathic pain
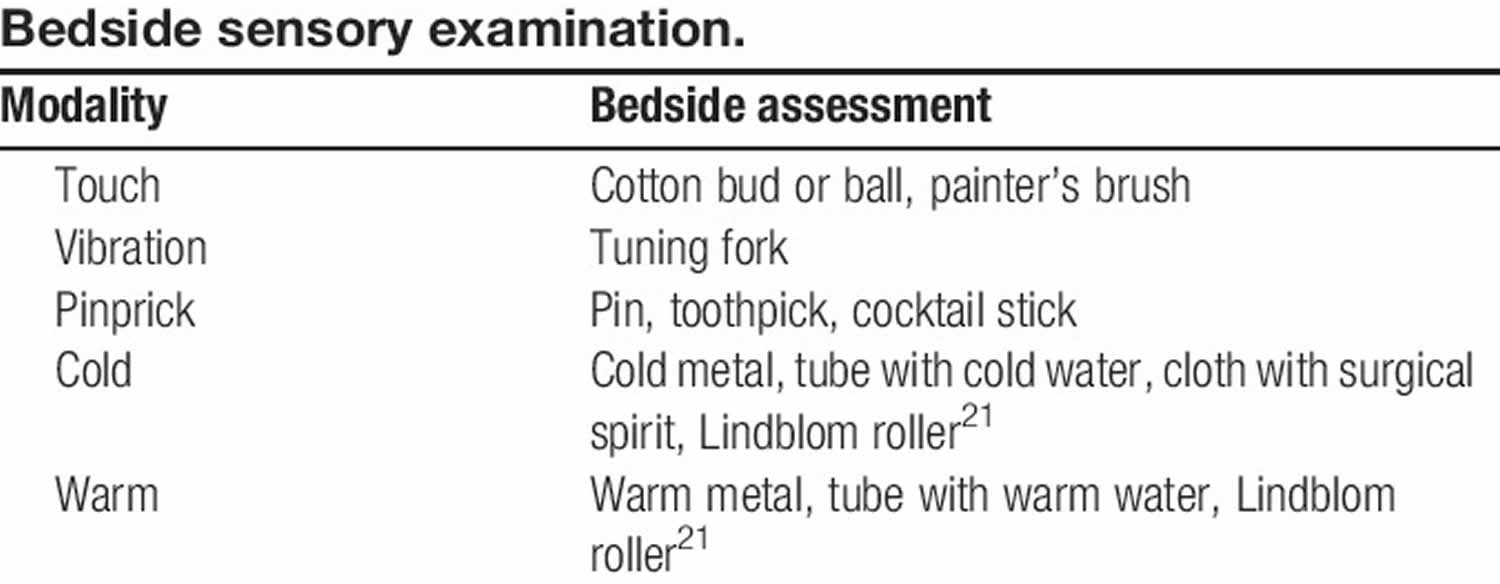
The next level of certainty requires supporting evidence obtained by a clinical examination. The examination should optimally confirm the presence of negative sensory signs, ie, partial or complete loss to one or several sensory modalities concordant with the lesion or disease of the somatosensory nervous system (eg, light touch, cold temperature) see Figures 3 and 4.
Demonstrating sensory loss to one or more of these modalities and delineation of the area affected by the negative sensory phenomena are central to the determination as to whether a nervous system lesion is the cause of the sensory disturbance (ie, whether it is compatible with neuropathy). Negative sensory signs may also be seen in nociceptive pain, but in these cases they lack neuroanatomically distinct borders and are not reproducible 25. The sensory signs may or may not be accompanied by motor or autonomic signs.
Positive sensory signs alone (eg, pressure-evoked hyperalgesia) carry less weight towards neuropathic pain probability, in particular, if their distribution does not follow relevant neuroanatomical delineation. Positive sensory symptoms and signs may be seen in patients with other conditions such as inflammatory pain, pain of unknown origin, anxiety, and sleep deprivation, and can be affected by stress and negative emotions 26. It is important to emphasize that there are conditions where sensory loss is not a prerequisite for a neuropathic pain condition. In certain neuropathic pain conditions such as hereditary channelopathies 27 and in subgroups of patients with, eg, peripheral nerve injury 28, touch-evoked allodynia or thermal hyperalgesia may be present without detectable sensory loss. The presence of such positive signs may mask sensory loss in some of these patients.
Idiopathic or classical trigeminal neuralgia is a special case. In trigeminal neuralgia, sensory deficits may not be found on clinical examination, although quantitative sensory testing may show sensory abnormality 28. In these cases, a history of characteristic triggering maneuvers may be counted as positive sensory signs. They can sometimes be repeated by the examiner, who may thus evoke and see the characteristic tic. Another special case is painful channelopathies as they are often paroxysmal and sensory examination can be normal between attacks. A history of characteristic symptoms may be considered a surrogate for positive sensory signs. In phantom pain, a sensory examination is not possible in the pain area. In these cases, the loss of the body part where pain is perceived is counted as a surrogate for sensory signs within the pain distribution.
Often, sensory changes to light touch, vibration, pinprick, cold, or warmth can be confirmed by a clinical examination (Figure 4), but more detailed analysis using quantitative sensory testing may be needed 29. Prolonged pain after herpes zoster is associated with sensory abnormalities in a neuroanatomically plausible distribution in most, but not all cases 28. In rare cases where sensory abnormalities are doubtful or lacking, documentation of a herpes zoster rash in the form of a photograph or clinical record will add to the evidence of somatosensory pathway involvement, allowing a subsequent designation of the condition as probable neuropathic pain. Sensory function is difficult to evaluate in deep tissue and viscera. For that reason, a level of certainty beyond possible neuropathic pain can rarely be obtained for visceral or deep somatic types of pain. Innervation territories of nerves and roots vary between individuals, they are not always clearly demarcated, and there is often overlap between them. Because of central sensitization phenomena, the areas of allodynia and hyperalgesia may extend beyond the innervation territory 30.
Figure 4. Neuropathic pain bedside sensory examination
Definite neuropathic pain
The final level of certainty requires that an objective diagnostic test confirms the lesion or disease of the somatosensory nervous system. This may not always be possible in the nonspecialist environment. Examples of such diagnostic tests include computed tomography, magnetic resonance imaging, or other imaging techniques to confirm the presence of stroke, multiple sclerosis, spinal cord injury, or nerve lesion; skin biopsy showing reduced intraepidermal nerve fiber density, neurophysiological tests such as nerve conduction velocity, heat and laser evoked potentials, nerve excitability tests, R1 blink reflex demonstrating neural function compromise, microneurography with evidence of aberrant nociceptor activity; and genetic tests confirming a hereditary neuropathic pain disorder such as inherited erythromelalgia 29. In cases of amputation or a surgeon’s clear verification of an intraoperative nerve lesion, further diagnostic tests are not necessary to arrive at the grading of “definite” neuropathic pain, because direct anatomical or surgical evidence counts as a confirmatory test.
This final level is reached by using only positive criteria for the location and nature of the neurological lesion or disease, without excluding other potential causes of the pain. Patients can have nociceptive pain in an area within the territory affected by an injury or disease involving the nervous system. Examples include spasticity-related pain below the level of injury in a patient with incomplete spinal cord injury, shoulder pain because of a lesion of the rotator cuff tendons in the area with sensory abnormalities after a stroke, inflammatory pain in the innervation territory of the lesioned nerves after thoracotomy or herniotomy, and plantar fasciitis in a patient with polyneuropathy. In these cases, despite fulfilling all 4 criteria of the grading system, the pain may still not be neuropathic. Thus, it is important to note that the final level does not completely rule out the possibility that other conditions such as tissue inflammation may fully or partially explain the pain. This remaining uncertainty about causality between the identified lesion or disease and the clinical presentation of the patient is a common situation in neurological diagnostics. In this context, the term definite neuropathic pain means that the clinician, by using history, clinical examination and auxiliary testing, is able to reach the level of confirming clinically that a patient has a neurological lesion that can explain the pain. Because the grading system only determines the level of certainty with which the presence or absence of a lesion or disease of the somatosensory nervous system can explain the pain, it is always important to consider if other causes for the patient’s pain conditions may be present.
Neuropathic pain treatment
The treatment of neuropathic pain remains challenging and medicines are just one aspect to managing this condition. Partial pain relief is usually considered a good result 31. Other strategies involve social, psychological and physical support. The benefit of these coping strategies cannot be underestimated. They can have lasting effects on emotional and physical wellbeing.
Pharmaceutical pain relief is part of a total plan for living with pain, which focuses on improving the patient’s quality of life and ability to function 32.
Non-pharmacological treatment such as physical exercise, cognitive behavioural therapy (CBT) and meditation can help in accepting and coping with the pain 33.
You may need to try a few different strategies to find which work best to lessen the effect pain has on your daily activities, mood or sleep.Work with your health professional to set realistic goals for managing your pain, and review these regularly. Your goals can be short-term or long-term and will probably change over time.
Psychology and psychological approaches to neuropathic pain (nerve pain) are an important and accepted part of the holistic pain management model. Research has shown that psychological approaches such as cognitive behavior therapy (CBT), mindfulness and hypnotherapy can be important components in improving pain management and indeed for warding off or being of benefit if anxiety or depression develop.
There are a variety of psychological approaches needed to deal with chronic pain because not all treatments work the same way for everyone, hence the therapist will work with you to try alternative approaches to lessening the stress that neuropathic pain (nerve pain) causes on brain function and emotional responses.
Cognitive behavior therapy
Cognitive behavior therapy (CBT) has been researched intensely and shown to be effective in reducing the psychological distress that is associated with long-term pain. Through the use of learning adaptive coping skills such as: relaxation, distraction, planning and routine, and problem solving, people are able to reduce the pain experience, improve positive social function and generally cope better with chronic pain. All of these techniques are used in order to replace the negative and catastrophic thoughts common to unmanaged chronic pain with more positive and calming thought processes.
MoodGYM (https://moodgym.com.au), is a web based CBT program designed to prevent and manage anxiety and depression. MoodGYM (https://moodgym.com.au) has been shown to reduce depression and anxiety in research studies.
Mindfulness
Jon Kabat-Zinn (https://www.mindfulnesscds.com) has been the leading figure in bringing mindfulness to the fore in recent decades. His approach to mindfulness involves: deliberately paying attention to everything, using all the senses, to be in the present moment, and to let each experience happen moment by moment without judgement.
The mindfulness technique is about recognizing that the person with pain’s mood, thoughts and emotions can play a huge role in an individual’s quality of life. Therefore, this approach is about separating the person’s emotions, thoughts and mood from the pain sensation itself.
The thoughts, emotions and mood associated with the chronic pain experience may seem attached to the pain experience. However, a mindful approach involves noticing when an individual is preoccupied with thoughts about the future or the past, recognizing whether these are helpful or not, and developing the ability to free yourself from them.
A growing awareness of mindfulness allows an individual to differentiate between the unpleasant experience that is pain, from thoughts about it, for example “I’m going to become disabled by it” or the emotions sparked by it, such as fear.
The ‘acceptance’ element of mindfulness is about modifying the unnecessary distress caused in fighting (or ignoring) the fact that something unwanted has happened. It is not about “giving into the pain” but rather it is about finding that an individual doesn’t have to pin an unpleasant value to it – it can just exist or to ‘be there’. It is not surprising that people with pain are often relieved to find that they can gradually let go of their unpleasant reactions to pain and in turn, can learn that the pain itself becomes more tolerable as the mindfulness begins to retrain the brain’s response to pain.
Biofeedback therapy
Antidepressants are often effective in treating anxiety and depression, and neuropathic pain in some people. However, if people with chronic pain can lessen the amount of medication used or boost the drug’s effectiveness by employing psychological techniques as well, then this is likely to benefit long term health as well as pain management.
Biofeedback is the process of gaining a greater understanding of how to notice and control body processes e.g. tension. This can be gained using an instrument to measure the tension or be taught without mechanical support.
Biofeedback has been found to be effective in the treatment of adult migraines and headaches. Pediatric studies have also found that chronic migraines and episodic headaches can be improved by using biofeedback therapy.
Biofeedback therapy comprises learning and performing relaxation and visualizing exercises with the aim of lessening muscle tension and gaining some influence over autonomic nervous system functions such as heart rate and skin temperature. These techniques are then used to stimulate relaxation, lessen muscle tension, prevent worsening of headaches, and reduce the frequency of headaches and pain.
Trials have found that biofeedback has produced similar effectiveness to that of meditation and relaxation in treating anxiety.
Biofeedback is also gaining legitimacy in the rehabilitation for stroke victims after being subjected to scientific scrutiny.
Another quick note is on relaxation. This technique may be recommended for anyone dealing with chronic pain which could lead to ways to control and cope with chronic pain on a daily basis. Some activities linked to relaxation include meditation or yoga or simply just activities that you find relaxing and that reduce your stress levels overall.
Interventional therapies
Other treatments may include:
- Shots with pain-relieving (anesthetic) drugs
- Nerve blocks
- Physical therapy (for some types of neuropathic pain, especially postherpetic neuropathic pain)
- Procedures to reduce feeling in the nerve (such as nerve ablation using radiofrequency, heat, balloon compression, or injection of chemicals)
- Surgery to take pressure off a nerve
- Alternative therapy, such as acupuncture or biofeedback
Procedures may not improve symptoms and can cause loss of feeling or abnormal sensations. Interventional treatments, such as nerve blocks or surgical procedures that deliver drugs to targeted areas, or modulation of specific neural structures, provide alternative treatment strategies in selected patients with refractory neuropathic pain 34. Although generally safe, spinal cord stimulation and peripheral nerve stimulation have been associated with hardware-related, biological complications, such as infections and programming-related or treatment-related adverse effects (including painful paraesthesias) 35.
In rare cases, a procedure called motor cortex stimulation is tried. An electrode is placed over part of nerve, spinal cord, or brain and is hooked to a pulse generator under the skin. This changes how your nerves signal and it may reduce pain.
Neural blockade and steroid injections
A perineural injection of steroids provides transient relief (1–3 months) for trauma-related and compression-related peripheral neuropathic pain 36. Systematic reviews and meta-analysis of epidural steroid injections for the treatment of cervical and lumbar radiculopathies indicate an immediate modest reduction in pain and function of <3 months duration, but had no effects on reducing the risk for subsequent surgery 37. Epidural local anaesthetic and steroid nerve blocks were given a weak recommendation for the treatment of lumbar radiculopathy and acute zoster-associated neuropathic pain119. Although sympathetic ganglion blocks have been used to treat pain in some patients with complex regional pain syndromes (also known as causalgia and reflex sympathetic dystrophy), the evidence for long-term benefit is weak 34.
Spinal cord stimulation
Low-intensity electrical stimulation of large myelinated Aβ fibers was introduced based on the gate control theory 38 as a strategy to modulate the pain signals transmitted by the unmyelinated C fibers. The most commonly used and the best-studied neuromodulation strategy has been spinal cord stimulation, in which a monophasic square-wave pulse (frequency ranging 30–100 Hz) is applied, resulting in paraesthesia in the painful region 39. Newer stimulation parameters, such as burst (40 Hz burst with five spikes at 500 Hz per burst) and high-frequency (10 kHz with sinusoidal waveforms) spinal cord stimulation, provide paraesthesia-free stimulation and equivalent or better pain relief compared with the monophasic square-wave pulse 40.
The relative safety and reversibility of spinal cord stimulation, as well as its cost-effectiveness over the long term have made it an attractive strategy for managing patients with refractory chronic neuropathic pain 41. Systematic reviews, randomized controlled trials and several case series provide evidence for the long-term efficacy of spinal cord stimulation when combined with medical treatment compared with medical management in various pain neuropathies 42, and has been shown to offer sustained results at 24 months of treatment 43. Two randomized trials in individuals with painful diabetic neuropathy reported greater reduction in pain and improvements in measures of quality of life compared with controls 44. Current European guidelines provide a weak recommendation for spinal cord stimulation (combined with medical treatment) in, for example, diabetic neuropathic pain 45. The success of spinal cord stimulation for neuropathic pain may depend on the appropriate selection of patients based on psychological traits, sensory phenotype, enhanced central sensitization and reduced conditioned pain modulation 46.
Dorsal root ganglion, peripheral nerve and peripheral nerve field stimulation
Neurostimulation of afferent fibres outside the spinal cord (for example, the dorsal root ganglion, which contains the cell bodies of sensory neurons, and peripheral nerves) and subcutaneous peripheral nerve field stimulation have been reported to provide pain relief in various chronic neuropathic pain states, including occipital neuralgia and postherpetic neuralgia 47. A multicentre prospective cohort study in patients with chronic neuropathic pain reported that dorsal root ganglion stimulation provided 56% pain reduction with a 60% responder rate (>50% reduction in pain) 48. These preliminary observations are being examined with controlled trials.
Epidural and transcranial cortical neurostimulation
Epidural motor cortex stimulation (ECMS), repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) of the pre-central motor cortex at levels below the motor threshold have been proposed as treatment options for patients with refractory chronic neuropathic pain 49. Cortical neurostimulation may reduce pain-related thalamic hyperactivity or activate descending inhibitory pathways. Meta-analysis reports suggest that 60–65% of patients respond (>40% pain reduction) to epidural motor cortex stimulation 49. Epidural motor cortex stimulation is a neurosurgical procedure that requires precise intra-operative placement of the stimulating electrode over the motor cortex region corresponding to the painful body part for optimal outcome.
Repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) are non-invasive therapies that involve neurostimulation of brain areas of interest via magnetic coils or electrodes on the scalp. Repetitive sessions (5–10 sessions over 1–2 weeks) with high-frequency repetitive transcranial magnetic stimulation (rTMS) (5–20 Hz) have shown benefits in a mixture of central, peripheral and facial neuropathic pain states, with effects lasting >2 weeks after the stimulation. tDCS has been reported to be beneficial in reducing several peripheral neuropathic conditions 50. Current European guidelines include a weak recommendation for the use of epidural motor cortex stimulation and rTMS in refractory chronic neuropathic pain and tDCS for peripheral neuropathic pain 51. Contraindications of rTMS include a history of epilepsy and the presence of aneurysm clips, deep brain electrodes, cardiac pacemakers and cochlear implants.
Deep brain stimulation
The use of long-term intracranial stimulation for neuropathic pain remains controversial. Multiple sites for deep brain stimulation, including the internal capsule, various nuclei in the sensory thalamus, periaqueductal and periventricular grey, motor cortex, septum, nucleus accumbens, posterior hypothalamus and anterior cingulate cortex, have been examined as potential brain targets for pain control 52. The UK National Institute for Health and Care Excellence (NICE) guidelines recognize that the procedure can be efficacious in some patients who are refractory to other forms of pain control, but current evidence on the safety of deep brain stimulation shows significant potential risks, such as intra-operative seizure, lead fractures and wound infections 53. Contrary to the NICE guidelines, the current European guidelines give inconclusive recommendations 54.
Intrathecal therapies
Intrathecal therapies have been developed to deliver drugs to targeted nerves through an implanted and refillable pump in patients with severe and chronic pain that is refractory to conservative treatments, including psychological, physical, pharmacological and neuromodulation therapies 55. The report from the 2012 Polyanalgesic Consensus Conference highlighted that this therapy is associated with risks of serious morbidity and mortality and made recommendations to reduce the incidence of these serious adverse effects 56. The only US FDA-approved drugs for use with such devices are morphine and ziconotide (an N-type calcium channel antagonist) 57. The most frequently reported adverse reactions associated with intrathecal ziconotide are dizziness, nausea, confusion, memory impairment, nystagmus (uncontrolled movement of the eyes) and an increase in the levels of serum creatine kinase. Ziconotide is contraindicated in patients with a history of psychosis, and patients should be monitored for evidence of cognitive impairment, hallucinations or changes in mood and consciousness. No high-quality randomized trials have been conducted to assess the efficacy of ziconotide and morphine; hence, the recommendations are a consensus of experts based on clinical experience or case series.
Physical therapies
Physical therapy, exercise and movement representation techniques (that is, treatments such as mirror therapy and motor imagery that use the observation and/or imagination of normal pain-free movements) have been suggested to be beneficial in neuropathic pain management 58. For example, mirror therapy and motor imagery are effective in the treatment of pain and disability associated with complex regional pain syndrome type I and type II 59. The quality of evidence supporting these interventions for neuropathic pain is weak and needs further investigation 60.
Neuropathic pain medication
International guidelines 61 recommend four first-line medicines for the treatment of neuropathic pain (except trigeminal neuralgia) 62:
- Amitriptyline,
- Duloxetine,
- Gabapentin,
- Pregabalin.
Medicine selection should be done on a case-by-case basis, taking into account the patient’s profile, contraindications and comorbidities. Some guidelines recommend the tricyclic antidepressant (TCA) drug class first-line, of which amitriptyline has the most evidence, as well as the serotonin and norepinephrine reuptake inhibitor (SNRI) drug class, of which duloxetine is uniformly recommended.
Amitriptyline has been effectively used (in low doses) for many years, is still one of the most efficacious medicines for neuropathic pain and remains relevant today.
If the initial treatment is not effective or is not tolerated, offer one of the remaining 3 drugs, and consider switching again if the second and third drugs tried are also not effective or not tolerated. Consider tramadol only if acute rescue therapy is needed 62. Consider capsaicin cream for people with localized neuropathic pain who wish to avoid, or who cannot tolerate, oral treatments.
Other medicines recommended as second- or third-line options include tramadol, lignocaine, capsaicin and botulinum toxin A 61.
There is a limited role for strong opioids in the treatment of neuropathic pain because of safety concerns and poor evidence of long-term efficacy 61. There is little evidence that paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs) are effective 63.
Evidence suggests that not all patients are receiving effective doses of recommended neuropathic pain medicines 64. Studies have also demonstrated that low doses at initiation, followed by a gradual increase until maximum benefit is obtained, helps with tolerability 32.
Some clinicians try to hurry the process by giving higher and higher doses, and the patients stop taking the medication due to adverse effects. Start low, go slow is my motto. Starting the patients on a very small dose and gradually increasing it is the best way to find the balance between the analgesic benefit and the side effect burden. It may help to work with the patient to develop a plan for trialling the agreed medicine. Such a plan should include a careful up-titration, and a treatment response review after a 3–8 week treatment trial 62. If the initial medicine is not effective or not tolerated, one or more of the other agents could be tried 62. It may be necessary to use more than one medicine concurrently, although the evidence for benefit of combination therapy is limited 31.
A recent systematic review confirmed the tolerability of low-dose amitriptyline (and other antidepressants) for the treatment of chronic pain. It reveals specific profiles of adverse effects that differ from those caused by higher doses of the same drugs prescribed for depression 65.
There have been a number of small head-to-head studies comparing the different neuropathic pain medicines, but as they have small sample sizes, their findings need to be treated cautiously. Overall, no significant differences in efficacy or safety were found between the first-line treatments 61.
Studies have examined the use of different neuropathic pain medicines for different conditions with neuropathic pain. Overall, all of the four first-line options can be considered, regardless of the cause or underlying disorder 61.
Unfortunately, only partial relief is possible in many cases, and people will need support and strategies to help them understand, accept, and live with their pain. A clear and targeted diagnosis, tackling the source of the pain where possible, and a considered treatment plan, including both pharmacological and non-pharmacological components, remain the best approaches to help people living with neuropathic pain.
Trigeminal neuralgia
Offer carbamazepine as initial treatment for trigeminal neuralgia 62. If initial treatment with carbamazepine is not effective, is not tolerated or is contraindicated, consider seeking expert advice from a specialist and consider early referral to a specialist pain service or a condition-specific service.
Treatments that should NOT be used:
Do not start the following to treat neuropathic pain in non-specialist settings, unless advised by a specialist to do so 62:
- cannabis sativa extract
- capsaicin patch
- lacosamide
- lamotrigine
- levetiracetam
- morphine
- oxcarbazepine
- topiramate
- tramadol (this is referring to long-term use)
- venlafaxine
- sodium valproate
Strong opioids (particularly oxycodone and morphine) and botulinum toxin type A (specialist use for peripheral neuropathic pain and presumed local pain generator) have weak Grading of Recommendations Assessment, Development, and Evaluation (GRADE) recommendations for use and are recommended as third-line 61. Prescription of opioids should be strictly monitored particularly for patients requiring high dosages (including tracking the dose in morphine equivalence, use of risk assessment tools and treatment agreements) 66.
Tapentadol, other antiepileptics, capsaicin cream, topical clonidine, SSRI antidepressants, NMDA antagonists and combination therapy 67 have inconclusive GRADE recommendations. Combination of pregabalin/gabapentin and duloxetine/tricyclic antidepressants (TCAs) may be considered as an alternative to increasing dosages in monotherapy for patients unresponsive to monotherapy with moderate dosages.
Cannabinoids and valproate have weak recommendations against their use in neuropathic pain and levetiracetam and mexiletine have strong recommendations against their use 61.
Table 1. Recommendations for individual drugs or drug classes based on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) classification and for first-, second-, and third-line drugs for neuropathic pain. Drugs pertaining to the same drug class are presented in alphabetical order.
| GRADE classification | Drugs | Daily dosages and dose regime | Recommendations |
|---|---|---|---|
| STRONG FOR | Gapabentin Gabapentin ER/enacarbil Pregabalin SNRIs duloxetine/venlafaxine Tricyclic antidepressants (TCAs) | 1200–3600 mg TID 1200–3600 mg BID 300–600 mg BID 60–120 mg QD (duloxetine);150–225 mg QD (venlafaxine ER) 25–150 mg qd or BID | First-line First-line First-line First-line First-line 1 |
| WEAK FOR | Capsaicin 8% patches Lidocaine patches Tramadol BTX- A (SC) Strong opioids | 1–4 patches to the painful area for 30–60 min every 3 months 1–3 patches to the painful area for up to 12 hours 200–400 mg BID (tramadol ER) or TID 50–200 units to the painful area every 3 months Individual titration | Second-line (PNP) 2 Second-line (PNP) Second-line Third-line ; specialist use (PNP) Third line3 |
| INCONCLUSIVE | Combination therapy Capsaicin cream Carbamazepine Clonidine topical Lacosamide Lamotrigine NMDA antagonists Oxcarbazepine SSRI antidepressants Tapentadol Topiramate Zonisamide | ||
| WEAK AGAINST | Cannabinoids Valproate | ||
| STRONG AGAINST | Levetiracetam Mexiletine |
Abbreviations: SNRIs = serotonin noradrenaline reuptake inhibitors; TCAs = tricyclic antidepressants; ER = extended realease; BID = twice daily; QD = once daily; PNP = peripheral neuropathic pain.
1) TCAs generally have similar efficacy. Tertiary amine TCAs (amitriptyline, imipramine, clomipramine) are not recommended at dosages > 75 mg/day in older adults because of their major anticholinergic and sedative side effects and potential risk of falls 68. An increased risk of sudden cardiac death has been reported for doses > 100 mg daily 69.
2) The long-term safety of repeated applications of high concentration capsaicin patches in patients has not been clearly established particularly with respect to degeneration of epidermal nerve fibres, which may be a concern in progressive neuropathy.
3) Sustained release oxycodone and morphine have been the most studied with maximal daily dosages of 120 mg and 240 mg respectively in clinical trials. Long-term opioid use may be associated with abuse particularly at high doses, cognitive impairment and endocrine and immunologic changes 70.
Table 2. Summary of Grading of Recommendations Assessment, Development, and Evaluation (GRADE) recommendations. Drug classes with recommendation for use.
| FIRST LINE DRUGS | SECOND LINE DRUGS | THIRD LINE DRUGS | ||||||
|---|---|---|---|---|---|---|---|---|
| SNRIs duloxetine venlafaxine | TCAs | Pregabalin Gabapentin Gabapentin ER/enacarbil | Tramadol | Capsaicin 8% patches | Lidocaine patches* | Strong opioids | Botulinum toxin type A | |
| Quality of evidence | ||||||||
| High | Moderate | High | Moderate | High | Low* | Moderate | Low | |
| Balance between desirable and undesirable effects | ||||||||
| Effect size | Moderate | Moderate | Moderate | Moderate | Low | Unknown | Moderate | Moderate |
| Tolerability and safety** | Moderate | Low -Moderate | Moderate-high | Low-moderate | Moderate-high | High | Low-moderate | High |
| Values and preferences | ||||||||
| Low-moderate | Low-moderate | Low-moderate | Low-moderate | High | High | Low-moderate | High | |
| Cost and resource allocation | ||||||||
| Low-moderate | Low | Low-moderate | Low | Moderate-high | Moderate-high | Low-moderate | Moderate-high | |
| Strength of recommendation | ||||||||
| Strong | Strong | Strong | Weak | Weak | Weak | Weak | Weak | |
| Neuropathic pain conditions | All | All | All | All | Peripheral | Peripheral | All | Peripheral |
Abbreviations: SNRIs = serotonin noradrenaline reuptake inhibitors; TCAs = tricyclic antidepressants; BTX-A = botulinum toxin type A ; ER = extended realease.
Footnote:
*FDA and EMEA approval for the treatment of postherpetic neuralgia
**Common side effects:
- antidepressants: somnolence, constipation, dry mouth (particularly TCAs), nausea (particularly duloxetine);
- pregabalin/gabapentin: somnolence, dizziness, weight gain;
- opioids (including tramadol): constipation, nausea, vomiting, tiredness, somnolence, dizziness, dry mouth, itch;
- lidocaine patches: local irritation;
- capsaicin patches: local pain, edema, erythema;
- botulinum toxin A: local pain.
- Colloca L, Ludman T, Bouhassira D, et al. Neuropathic pain. Nat Rev Dis Primers. 2017;3:17002. Published 2017 Feb 16. doi:10.1038/nrdp.2017.2 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5371025
- Neuropathic pain: redefinition and a grading system for clinical and research purposes. Treede RD, Jensen TS, Campbell JN, Cruccu G, Dostrovsky JO, Griffin JW, Hansson P, Hughes R, Nurmikko T, Serra J. Neurology. 2008 Apr 29; 70(18):1630-5.
- A new definition of neuropathic pain. Jensen TS, Baron R, Haanpää M, Kalso E, Loeser JD, Rice AS, Treede RD. Pain. 2011 Oct; 152(10):2204-5.
- Finnerup NB, Haroutounian S, Kamerman P, et al. Neuropathic pain: an updated grading system for research and clinical practice. Pain. 2016;157(8):1599–1606. doi:10.1097/j.pain.0000000000000492 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4949003
- Magrinelli F, Zanette G, Tamburin S. Neuropathic pain: diagnosis and treatment. Practical Neurology 2013;13:292-307. https://pn.bmj.com/content/13/5/292
- Prevalence of chronic pain with neuropathic characteristics in the general population. Bouhassira D, Lantéri-Minet M, Attal N, Laurent B, Touboul C. Pain. 2008 Jun; 136(3):380-7.
- Freynhagen R, et al. Screening of neuropathic pain components in patients with chronic back pain associated with nerve root compression: a prospective observational pilot study (MIPORT) Curr Med Res Opin. 2006;22:529–537
- IASP. Global year against neuropathic pain. 2015. https://www.iasp-pain.org/GlobalYear/NeuropathicPain?navItemNumber=580
- Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Finnerup NB, Attal N, Haroutounian S, McNicol E, Baron R, Dworkin RH, Gilron I, Haanpää M, Hansson P, Jensen TS, Kamerman PR, Lund K, Moore A, Raja SN, Rice AS, Rowbotham M, Sena E, Siddall P, Smith BH, Wallace M. Lancet Neurol. 2015 Feb; 14(2):162-73.
- Tesfaye S, Boulton AJ, Dickenson AH. Mechanisms and management of diabetic painful distal symmetrical polyneuropathy. Diabetes Care. 2013;36:2456–2465
- Sommer C. Painful neuropathies. Curr Opin Neurol 2003;16:623–628
- Borsook D. Neurological diseases and pain. Brain. 2012;135:320–344
- Watson JC, Sandroni P. Central neuropathic pain syndromes. Mayo Clin Proc. 2016;91:372–385.
- Stavros K, Simpson DM. Understanding the etiology and management of HIV-associated peripheral neuropathy. Curr HIV/AIDS Rep. 2014;11:195–201
- Thakur S, Dworkin RH, Haroun OM, Lockwood DN, Rice AS. Acute and chronic pain associated with leprosy. Pain. 2015;156:998–1002
- Using screening tools to identify neuropathic pain. Bennett MI, Attal N, Backonja MM, Baron R, Bouhassira D, Freynhagen R, Scholz J, Tölle TR, Wittchen HU, Jensen TS. Pain. 2007 Feb; 127(3):199-203.
- Prevalence of neuropathic pain according to the IASP grading system in patients with chronic non-malignant pain. Vaegter HB, Andersen PG, Madsen MF, Handberg G, Enggaard TP. Pain Med. 2014 Jan; 15(1):120-7.
- The LANSS Pain Scale: the Leeds assessment of neuropathic symptoms and signs. Bennett M. Pain. 2001 May; 92(1-2):147-57. https://www.ncbi.nlm.nih.gov/pubmed/11323136
- Development of a neuropathic pain questionnaire. Krause SJ, Backonja MM. Clin J Pain. 2003 Sep-Oct; 19(5):306-14.
- Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Bouhassira D, Attal N, Alchaar H, Boureau F, Brochet B, Bruxelle J, Cunin G, Fermanian J, Ginies P, Grun-Overdyking A, Jafari-Schluep H, Lantéri-Minet M, Laurent B, Mick G, Serrie A, Valade D, Vicaut E. Pain. 2005 Mar; 114(1-2):29-36.
- painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Freynhagen R, Baron R, Gockel U, Tölle TR. Curr Med Res Opin. 2006 Oct; 22(10):1911-20. https://www.ncbi.nlm.nih.gov/pubmed/17022849
- Development and testing of a neuropathic pain screening questionnaire: ID Pain. Portenoy R. Curr Med Res Opin. 2006 Aug; 22(8):1555-65. https://www.ncbi.nlm.nih.gov/pubmed/16870080
- Krause SJ, Backonja MM. Development of a neuropathic pain questionnaire. Clin J Pain. 2003;19:306–314
- Bouhassira D, et al. Development and validation of the Neuropathic Pain Symptom Inventory. Pain. 2004;108:248–257
- Numbness in clinical and experimental pain–a cross-sectional study exploring the mechanisms of reduced tactile function. Geber C, Magerl W, Fondel R, Fechir M, Rolke R, Vogt T, Treede RD, Birklein F. Pain. 2008 Sep 30; 139(1):73-81.
- One night of total sleep deprivation promotes a state of generalized hyperalgesia: a surrogate pain model to study the relationship of insomnia and pain. Schuh-Hofer S, Wodarski R, Pfau DB, Caspani O, Magerl W, Kennedy JD, Treede RD. Pain. 2013 Sep; 154(9):1613-21.
- Painful and painless channelopathies. Bennett DL, Woods CG. Lancet Neurol. 2014 Jun; 13(6):587-99.
- Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): somatosensory abnormalities in 1236 patients with different neuropathic pain syndromes. Maier C, Baron R, Tölle TR, Binder A, Birbaumer N, Birklein F, Gierthmühlen J, Flor H, Geber C, Huge V, Krumova EK, Landwehrmeyer GB, Magerl W, Maihöfner C, Richter H, Rolke R, Scherens A, Schwarz A, Sommer C, Tronnier V, Uçeyler N, Valet M, Wasner G, Treede RD. Pain. 2010 Sep; 150(3):439-50.
- NeuPSIG guidelines on neuropathic pain assessment. Haanpää M, Attal N, Backonja M, Baron R, Bennett M, Bouhassira D, Cruccu G, Hansson P, Haythornthwaite JA, Iannetti GD, Jensen TS, Kauppila T, Nurmikko TJ, Rice AS, Rowbotham M, Serra J, Sommer C, Smith BH, Treede RD. Pain. 2011 Jan; 152(1):14-27.
- Central sensitization: implications for the diagnosis and treatment of pain. Woolf CJ. Pain. 2011 Mar; 152(3 Suppl):S2-15.
- Neurology Expert Group. Therapeutic guidelines: Neuropathic pain: version 4. West Melbourne: Therapeutic Guidelines Ltd, 2011
- Dworkin RH, O’Connor AB, Backonja M, et al. Pharmacologic management of neuropathic pain: evidence-based recommendations. Pain 2007;132:237-51
- Dimitrova A, Murchison C, Oken B. Acupuncture for the treatment of peripheral neuropathy: A systematic review and meta-analysis. J Altern Complement Med 2017;23:164-79
- Dworkin RH, et al. Interventional management of neuropathic pain: NeuPSIG recommendations. Pain. 2013;154:2249–2261
- Eldabe S, Buchser E, Duarte R. V Complications of spinal cord stimulation and peripheral nerve stimulation techniques: a review of the literature. Pain Med. 2016;17:325–336
- Bhatia A, Flamer D, Shah PS. Perineural steroids for trauma and compression-related peripheral neuropathic pain: a systematic review and meta-analysis. Can J Anaesth. 2015;62:650–662
- Chou R, et al. Epidural corticosteroid injections for radiculopathy and spinal stenosis: a systematic review and meta-analysis. Ann Intern Med. 2015;163:373–381
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150:971–979
- Yearwood TL, Hershey B, Bradley K, Lee D. Pulse width programming in spinal cord stimulation: a clinical study. Pain Physician. 2010;13:321–335
- Russo M, Van Buyten JP. 10-kHz high-frequency SCS therapy: a clinical summary. Pain Med. 2015;16:934–942
- Deer TR, et al. The appropriate use of neurostimulation: new and evolving neurostimulation therapies and applicable treatment for chronic pain and selected disease states. Neuromodulation Appropriateness Consensus Committee. Neuromodulation. 2014;17:599–615
- North RB, et al. Spinal cord stimulation versus re-operation in patients with failed back surgery syndrome: an international multicenter randomized controlled trial (EVIDENCE study) Neuromodulation. 2011;14:330–335
- Kumar K, et al. The effects of spinal cord stimulation in neuropathic pain are sustained: a 24-month follow-up of the prospective randomized controlled multicenter trial of the effectiveness of spinal cord stimulation. Neurosurgery. 2008;63:762–770
- de Vos CC, et al. Spinal cord stimulation in patients with painful diabetic neuropathy: a multicentre randomized clinical trial. Pain. 2014;155:2426–2431
- Cruccu G, et al. EAN guidelines on central neurostimulation therapy in chronic pain conditions. Eur J Neurol. 2016;23:1489–1499.
- Campbell CM, et al. Dynamic pain phenotypes are associated with spinal cord stimulation-induced reduction in pain: a repeated measures observational pilot study. Pain Med. 2015;16:1349–1360.
- Krames ES. The role of the dorsal root ganglion in the development of neuropathic pain. Pain Med. 2014;15:1669–1685
- Liem L, et al. One-year outcomes of spinal cord stimulation of the dorsal root ganglion in the treatment of chronic neuropathic pain. Neuromodulation. 2015;18:41–48
- Lefaucheur JP. Cortical neurostimulation for neuropathic pain: state of the art and perspectives. Pain. 2016;157:S81–S89.
- Lefaucheur JP, et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS) Clin Neurophysiol. 2016;128:56–92
- Kumar K, et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007;132:179–188
- Keifer OP, Jr, Riley JP, Boulis NM. Deep brain stimulation for chronic pain: intracranial targets, clinical outcomes, and trial design considerations. Neurosurg Clin N Am. 2014;25:671–692
- Tan T, Barry P, Reken S, Baker M, Guideline Development Group Pharmacological management of neuropathic pain in non-specialist settings: summary of NICE guidance. BMJ. 2010;340:c1079
- Cruccu G, et al. EAN guidelines on central neurostimulation therapy in chronic pain conditions. Eur J Neurol. 2016;23:1489–1499
- Prager J, et al. Best practices for intrathecal drug delivery for pain. Neuromodulation. 2014;17:354–372
- Deer TR, et al. Polyanalgesic Consensus Conference — 2012: recommendations to reduce morbidity and mortality in intrathecal drug delivery in the treatment of chronic pain. Neuromodulation. 2012;15:467–482
- Pope JE, Deer TR, Bruel BM, Falowski S. Clinical uses of intrathecal therapy and its placement in the pain care algorithm. Pain Pract. 2016;16:1092–1106
- Dobson JL, McMillan J, Li L. Benefits of exercise intervention in reducing neuropathic pain. Front Cell Neurosci. 2014;8:102
- Smart KM, Wand BM, O’Connell NE. Physiotherapy for pain and disability in adults with complex regional pain syndrome (CRPS) types I and II. Cochrane Database Syst Rev. 2016;2:CD010853
- Thieme H, Morkisch N, Rietz C, Dohle C, Borgetto B. The efficacy of movement representation techniques for treatment of limb pain — a systematic review and meta-analysis. J Pain. 2016;17:167–180
- Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/S1474-4422(14)70251-0 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4493167
- Neuropathic pain in adults: pharmacological management in non-specialist settings. https://www.nice.org.uk/guidance/CG173
- Wiffen PJ, Knaggs R, Derry S, Cole P, Phillips T, Moore RA. Paracetamol (acetaminophen) with or without codeine or dihydrocodeine for neuropathic pain in adults. Cochrane Database Syst Rev. 2016;12(12):CD012227. Published 2016 Dec 27. doi:10.1002/14651858.CD012227.pub2 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6463878
- O’Connor AB. Neuropathic pain: quality-of-life impact, costs and cost effectiveness of therapy. Pharmacoeconomics 2009;27:95-112
- Riediger C, Schuster T, Barlinn K, et al. Adverse effects of antidepressants for chronic pain: A systematic review and meta-analysis. Front Neurol 2017;8:307
- Opioid prescribing: a systematic review and critical appraisal of guidelines for chronic pain. Nuckols TK, Anderson L, Popescu I, Diamant AL, Doyle B, Di Capua P, Chou R. Ann Intern Med. 2014 Jan 7; 160(1):38-47.
- Duloxetine and pregabalin: high-dose monotherapy or their combination? The “COMBO-DN study”–a multinational, randomized, double-blind, parallel-group study in patients with diabetic peripheral neuropathic pain. Tesfaye S, Wilhelm S, Lledo A, Schacht A, Tölle T, Bouhassira D, Cruccu G, Skljarevski V, Freynhagen R. Pain. 2013 Dec; 154(12):2616-25.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60:616–31
- Ray WA, Meredith S, Thapa PB, Hall K, Murray KT. Cyclic antidepressants and the risk of sudden cardiac death. Clin Pharmacol Ther. 2004;75:234–41
- Edlund MJ, Martin BC, Russo JE, DeVries A, Braden JB, Sullivan MD. The role of opioid prescription in incident opioid abuse and dependence among individuals with chronic noncancer pain: the role of opioid prescription. Clin J Pain. 2014;30:557–64





{kind=link}