
What is olive oil
The Olive tree (Olea europaea L.), a native of the Mediterranean basin and parts of Asia. According to estimates, the cultivation of olive tree dates back more than 7000 years. The tree is typically distributed in the the coastal areas of the eastern Mediterranean Basin, the adjoining coastal areas of southeastern Europe, western Asia and northern Africa as well as northern Iran at the south end of the Caspian Sea. Although olive is now cultivated in several parts of the world, the Mediterranean region still serves as the major production area accounting for about 98% of the world’s olive cultivation 1. The tree, famous for its fruit, also called the olive, is commercially important in the Mediterranean region as a prime source of olive oil 2.
Olive oil is a liquid fat obtained from olives (the fruit of Olea europaea; family Oleaceae), a traditional tree crop of the Mediterranean Basin 3. The oil is produced by pressing whole olives. It is commonly used in cooking, whether for frying or as a salad dressing. It is also used in cosmetics, pharmaceuticals, and soaps, and as a fuel for traditional oil lamps. It is associated with the “Mediterranean diet” for its possible health benefits 4. The olive is one of three core food plants in Mediterranean cuisine; the other two are wheat and grapes.
Table 1. World wide major production and consumption of olive oil
| Country | Production in tons (2009)a | Production % (2009) | Consumption (2005)b | Consumption per person annually (liters/kg)c |
|---|---|---|---|---|
| World | 2,907,985 | 100% | 100% | 0.43 |
| Spain | 1,199,200 | 41.2% | 20% | 13.62 |
| Italy | 587,700 | 20.2% | 30% | 12.35 |
| Greece | 332,600 | 11.4% | 9% | 23.7 |
| Syria | 168,163 | 5.8% | 3% | 7.0 |
| Tunisia | 150,000 | 5.2% | 2% | 11.1 |
| Turkey | 143,600 | 4.9% | 2% | 1.2 |
| Morocco | 95,300 | 3.3% | 2% | 1.8 |
| Portugal | 53,300 | 1.8% | 2% | 7.1 |
| France | 6,300 | 0.2% | 4% | 1.34 |
| United States | 2,700 | 0.1% | 8% | 0.56 |
| Others | 169,122 | 5.8% | 18% | 1.18 |
The composition of olive oil varies with the cultivar, altitude, time of harvest and extraction process. It consists mainly of oleic acid (up to 83%), with smaller amounts of other fatty acids including linoleic acid (up to 21%) and palmitic acid (up to 20%). Extra-virgin olive oil is required to have no more than 0.8% free acidity and is considered to have favorable flavor characteristics; it forms as much as 80% of total production in Greece and 65% in Italy, but far less in other countries.
There are many different olive varieties or olives, each with a particular flavor, texture, and shelf life that make them more or less suitable for different applications such as direct human consumption on bread or in salads, indirect consumption in domestic cooking or catering, or industrial uses such as animal feed or engineering applications.
Olive varieties include Arbequina, Barnea, Coratina, Corregiola, Frantoio, Kalamata, Koroneiki, Leccino, Manzanillo, Pendolino and Picual. About 90 per cent of Australian olive oil is produced from 10 of these major varietals. Trained tasters can identify a variety by its trademark characteristics; oil from Picual olives (originally from Spain), for example, has peppery, bitter and slightly woody flavors.
Table 2. Some important properties of popular cultivars, their utilization and origin
| Cultivar | %Oil yield | Ratio flesh to pit | Olive size (Fruits/kg) | Purpose | Shape of the fruits | Origin |
|---|---|---|---|---|---|---|
| Hojiblanca | 23–29 | 4.9 and 6.6:1 | 230–700 | Oil extraction and table olives | Regular | Spain |
| Verdial | 22–30 | 6:1 | 220–800 | Oil extraction and table olives | Ellipsoidal | Spain |
| Picual | 23–27 | 3.8 and 6.1:1 | 270–470 | Oil extraction and table olives | Prominent tip at the button end | Spain |
| Domat | 22 | – | 180–190 | Green table olive | Regular | Turkey |
| Gemlik | 27 | 6:1 | 270–280 | Black table olives | Pronounced tip at the end | Turkey |
| Memecik | 22 | 6:1 | 205–215 | Oil extraction | Pronounced tip at the end | Turkey |
| Memeli | 25 | 7 : 1 | 200–210 | Green-type table olives | Small tip at the end | Turkey |
| Conservolea | 22–25 | 8:1 | 180–200 | Table olive | Round to oval | Greece |
| Nychati Kalamon | 25 | 8:1 | 220–240 | Black table olive | Cylindro-conical, Curved | Greece |
| Chalkidiki | 19 | – | 120–140 | Green table olive, oil extraction | Pronounced tip at the end | Greece |
| Sevillano | 14 | 7.3:1 | 70–80 | Table olive | – | Spain |
| Ascolano | 19 | 8.2:1 | 110–120 | Table olive | – | Italy |
| Ascolana | 17 | – | 100–180 | Table olive | Spherica | Italy |
| Barouni | 17 | 6.8:1 | 130–140 | Green & black – ripe olives | – | Tunisia |
| Picholine marocaine | 17 | 5:1 | 300–500 | Table olive | – | Morocco |
| Arauco | 22–24 | 7:1 | 125–300 | Table olive and oil extraction | Pronounced tip | Argentina |
| Galega vulga | – | 4:1 | 430 | Black table olive | – | Portugal |
| Oblitza | 22 | 6.5:1 | 200 | Table olive | Apple and heart shape | Yugoslavia |
| Ladoelia | 18–21 | 4.6:1 | 330 | Table olive | – | Cyprus |
An important issue often not realized in countries that do not produce olive oil is that the freshness makes a big difference. A very fresh oil, as available in an oil producing region, tastes noticeably different from the older oils available elsewhere 3. In time, olive oils deteriorate and become stale. One-year-old olive oil may be still pleasant to the taste, but it is less fragrant than fresh olive oil. After the first year, olive oil should be used for cooking, not for foods to be eaten cold, like salads.
The taste of the olive oil is influenced by the varietals used to produce the oil and by the moment when the olives are harvested and ground (less ripe olives give more bitter and spicy flavors – riper olives give a sweeter sensation in the oil).
Broadly speaking:
- “Early harvest” oils tend to be “robust” (bitter and pungent), with greener characters (such as grassy aromas, green apple aromas, green tomato, etc).
- “Late harvest” oils tend towards “mild and mellow” or “delicate and mild”, with sweeter characters (such as ripe banana aromas, tropical fruit, vanilla, etc.).
But other factors, such as variety and environment, can influence the character of the oils. Consequently, an early harvest Arbequina oil from a warm climate can be milder and mellower than a late harvest Coratina from a colder climate.
Here is a quick summary of olive oil grades
- “Virgin” oil is extracted from olives by a mechanical process cold pressed (or squeezed) from fresh olives without excessive heat, additives or solvents 7.
- Extra virgin olive oil, in addition to the above, has low acidity (0.8 per cent or less) and should comply with other technical specifications, as well as being free from taste defects.
- “Light”, “lite” or “pure” olive oils have been refined through a combination of physical (heat) and chemical processes they are subjected to, including gum extraction, neutralization, decolourisation, and heat treatments, resulting in an oil with no distinctive aroma, color or taste. A small percentage of virgin oil is then mixed with this oil to give it flavor. Refining removes antioxidants, so these oils aren’t as healthy as extra virgin. They don’t have less fat or fewer kilojoules than regular oils.
- “Cold pressed” and “first press” are outdated and unhelpful marketing terms. All virgin oils have to be “cold extracted” – extracted from the olive without the use of excessive heat (manufacturers can extract more oil from olives with heat but the quality suffers). Traditional hydraulic presses have been almost entirely replaced by centrifuges, and all virgin oil comes from a single extraction – there’s no second press.
Olive oils alone, are blends of mostly refined oil with a splash extra virgin olive oil. Refined oils are those that have been subject to chemical processing. Refined olive oils are often labeled “Pure”, “Extra Light” or “Light” which are simply marketing terms and not related to the quality or content of the oil.
Choosing the best olive oil
- An olive oil’s aromas and flavors are at their peak when it’s young. According to the Australian Olive Association, most extra virgin olive oils retain freshness for at least 12 months if stored properly in sealed bottles in a cool, dark place. Unlike wine, olive oil does not improve with age – so the closer to its production you use it, the better. Unfortunately, current labelling requirements don’t help in choosing the freshest oils. Most brands give only a general best-before date, if at all.
- The International Olive Council suggests a best-before date indicating the “minimum durability” of the oil, although how the date is calculated is at the discretion of the producer or importer.
- Date of bottling, harvest or production would be more helpful for consumers, but not necessarily feasible or precise, according to industry, as oil may be a blend from different years and held in a tank for an extended time before bottling.
In the meantime, we suggest you choose oils with a best-before date at least 12 months away, and avoid purchasing oils that are displayed under direct sunlight or in an overly warm environment.
Free fatty acids (FFA) and acidity
The “acidity” in olive oil is the result of the degree of breakdown of the triacylglycerols, due to a chemical reaction called hydrolysis or lipolysis, in which free fatty acids are formed 8. In exceptional circumstances, even oils made from fresh, healthy olives can have significant amounts of acidity, caused by anomalies during the actual biosynthesis of the oil in the olive fruit. Oil extracted carelessly and/or from poor quality fruit suffers from a very significant breakdown of the triacylglycerides into fatty acids. These “broken off” fatty acids are called Free Fatty Acids 8. Sometimes just one of the three fatty acids breaks off, leaving a diacylglycerol. If two fatty acids break off, we are left with a monoacylglycerol. If all three break off, were are left with glycerol.
Factors which lead to a high free fatty acidity in an oil include fruit fly infestation, delays between harvesting and extraction (especially if the fruit has been bruised or damaged during harvesting), fungal diseases in the fruit (gloesporium, macrophoma, etc.), prolonged contact between oil and vegetation water (after extraction), and careless extraction methods 8. Storing olives in heaps or silos to encourage enzymatic breakdown of cell structure, and thus facilitate oil release (as is the tradition in Portugal and other countries) is certainly not conducive to producing a high quality, low acidity oil 8.
The free fatty acidity is thus a direct measure of the quality of the oil, and reflects the care taken right from blossoming and fruit set to the eventual sale and consumption of the oil 8.
Measurement of free fatty acidity is a very simple procedure which can be done at a testing lab. The results are presented as grams of oleic acid per 100 grams oil, commonly known as the free fatty acidity of the oil in percent 8. Freshly pressed olive oil, made carefully, without the use of excessive heat, from sound, healthy, freshly picked olives, normally has a pretty low “acidity”, well under 0.5% FFA. Extra virgin olive oils have less than 0.8% FFA 8.
Olive oil nutrition
One tablespoon of olive oil (15 ml) contains the following nutritional information according to the USDA 9:
- Calories: 120
- Fat: 13.30 g (21% of the Daily Value, DV)
- Saturated fat: 2 g (9% of DV)
- Carbohydrates: 0
- Fibers: 0
- Protein: 0
- Vitamin E: 1.9 mg (10% of DV)
- Vitamin K: 8.1 µg (10% of DV)
Table 3. Olive oil nutrition facts
Nutrient | Unit | 15 ml | Value per 100 ml | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Approximates | |||||||||||||||||||
| Energy | kcal | 120 | 800 | ||||||||||||||||
| Protein | g | 0.00 | 0.00 | ||||||||||||||||
| Total lipid (fat) | g | 14.00 | 93.33 | ||||||||||||||||
| Carbohydrate, by difference | g | 0.00 | 0.00 | ||||||||||||||||
| Minerals | |||||||||||||||||||
| Sodium, Na | mg | 0 | 0 | ||||||||||||||||
| Lipids | |||||||||||||||||||
| Fatty acids, total saturated | g | 1.999 | 13.330 | ||||||||||||||||
| Fatty acids, total monounsaturated | g | 10.001 | 66.670 | ||||||||||||||||
| Fatty acids, total polyunsaturated | g | 1.500 | 10.000 | ||||||||||||||||
| Fatty acids, total trans | g | 0.000 | 0.000 | ||||||||||||||||
| Cholesterol | mg | 0 | 0 | ||||||||||||||||
Table 4. Extra-virgin olive oil nutrition facts
Nutrient | Unit | 15 ml | Value per 100 ml | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Approximates | |||||||||||||||||||
| Energy | kcal | 126 | 840 | ||||||||||||||||
| Protein | g | 0.00 | 0.00 | ||||||||||||||||
| Total lipid (fat) | g | 14.00 | 93.33 | ||||||||||||||||
| Carbohydrate, by difference | g | 0.00 | 0.00 | ||||||||||||||||
| Minerals | |||||||||||||||||||
| Sodium, Na | mg | 0 | 0 | ||||||||||||||||
| Lipids | |||||||||||||||||||
| Fatty acids, total saturated | g | 1.999 | 13.330 | ||||||||||||||||
| Fatty acids, total monounsaturated | g | 11.000 | 73.330 | ||||||||||||||||
| Fatty acids, total polyunsaturated | g | 1.000 | 6.670 | ||||||||||||||||
| Fatty acids, total trans | g | 0.000 | 0.000 | ||||||||||||||||
| Cholesterol | mg | 0 | 0 | ||||||||||||||||
Olive Oil Chemical Characteristics
Olive oil is composed mainly of triacylglycerols (triglycerides or fats) and contains small quantities of free fatty acids (FFA), glycerol, phosphatides, pigments, flavor compounds, sterols, and microscopic bits of olive 10. Triacylglycerols are the major energy reserve for plants and animals. Chemically speaking, these are molecules derived from the natural esterification of three fatty acid molecules with a glycerol molecule.
The fatty acid composition of olive oil varies widely depending on the cultivar, maturity of the fruit, altitude, climate, and several other factors.
The major fatty acids in olive oil triacylglycerols are:
- Oleic Acid (C18:1), a monounsaturated omega-9 fatty acid. It makes up 55 to 83% of olive oil.
- Linoleic Acid (C18:2), a polyunsaturated omega-6 fatty acid (an essential fatty acid) that makes up about 3.5 to 21% of olive oil.
- Palmitic Acid (C16:0), a saturated fatty acid that makes up 7.5 to 20% of olive oil.
- Stearic Acid (C18:0), a saturated fatty acid that makes up 0.5 to 5% of olive oil.
- Linolenic Acid (C18:3) (specifically alpha-Linolenic Acid), a polyunsaturated omega-3 fatty acid (an essential fatty acid) that makes up 0 to 1.5% of olive oil.
The principal component of olive oil is always the oleic acid, contributing about 55–83% of the total fatty acids. Some parameters such as the area of production, the latitude, the climate, the variety, and the stage of maturity of the fruit greatly affect the fatty acid composition of olive oil. For example, varieties of olive oil from Greece, Italy, and Spain are low in linoleic and palmitic acids but they have a high percentage of oleic acid, while the Tunisian olive oil is high in linoleic and palmitic acids and low in oleic acid 11.
Olive oil contains more oleic acid and less linoleic and linolenic acids than other vegetable oils, that is, more monounsaturated than polyunsaturated fatty acids. This renders olive oil more resistant to oxidation because generally, the greater the number of double bonds in the fatty acid, the more unstable and easily broken down by heat, light, and other factors the oil is. It is generally accepted that cooler regions (e.g. Tuscany) will yield oil with higher oleic acid than warmer climates. That is, a cool region olive oil may be more monounsaturated in content than a warm region oil.
From a medical point of view essential fatty acid refers to all the omega-3 or omega-6 fatty acids. Essential fatty acids are the ones that the human body cannot make. There are only two, which are the building blocks from which many of the other omega-3 and omega-6 fatty acids are made in a healthy body: linoleic acid (LA) and alpha-linolenic acid (ALA).
Percentage of Linolenic Acid Allowed in Olive Oil
Regarding the polyunsaturated fatty acids (PUFAs), there is a wide range acceptable for extra virgin olive oil, however the linolenic acid has to be less than 0.9% per the International Olive Oil Council guidelines 12. Higher levels, e.g. 1.5%, do not present a nutritional problem, but the International Olive Oil Council uses the linolenic acid level to establish the authenticity of the olive oil. Seed oils like canola oil have higher levels of linolenic acid.
Table 5. Olive oil composition
| Fatty acid | Percentage | ref. |
|---|---|---|
| Oleic acid | 55 to 83% | 10, 13 |
| Linoleic acid | 3.5 to 21% | 10, 13 |
| Palmitic acid | 7.5 to 20% | 10 |
| Stearic acid | 0.5 to 5% | 10 |
| α-Linolenic acid | 0 to 1.5% | 10 |
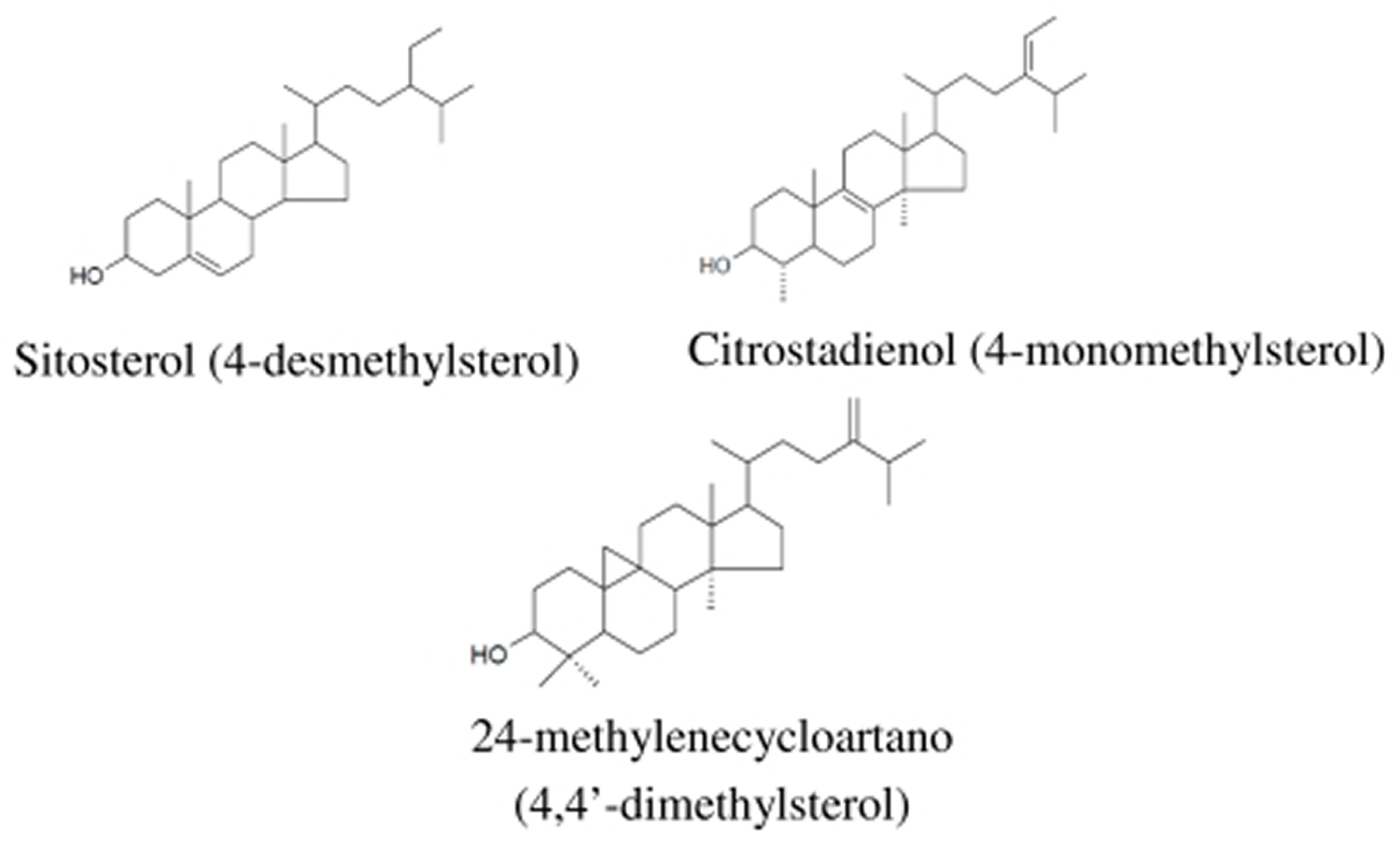
Note: Olive oil is composed mainly of the mixed triglyceride esters of oleic acid and palmitic acid and of other fatty acids, along with traces of squalene (up to 0.7%) and sterols (about 0.2% phytosterol and tocosterols). The composition varies by cultivar, region, altitude, time of harvest, and extraction process.
Figure 1. Chemical structure of important bioactives in olive/olive oil

Figure 2. Chemical structural of some important phytosterols in olive oil
What are Monounsaturated Fatty Acids
Monounsaturated fatty acids (MUFA) are chemically classified as fatty acids containing a single double bond (in contrast to polyunsaturated fatty acids (PUFA) containing two or more double bonds and saturated fatty acids (SFA) without double bonds) 15. In the cis-configuration, the hydrogen atoms are on the same side as the double bond, whereas in trans-configuration the hydrogen atoms and the double bond are present on opposite sides. The cis-isomers are the predominant form of MUFA in food sources. The most common cis-configured MUFA in daily nutrition is oleic acid (18:1 n-9), followed by palmitoleic acid (16:1 n-7), and vaccenic acid (18:1 n-7). Moreover, oleic acid represents the topmost MUFA provided in the diet (~90% of all MUFAs) 16.
Figure 3. Monounsaturated Fatty Acids Structure (MUFA)
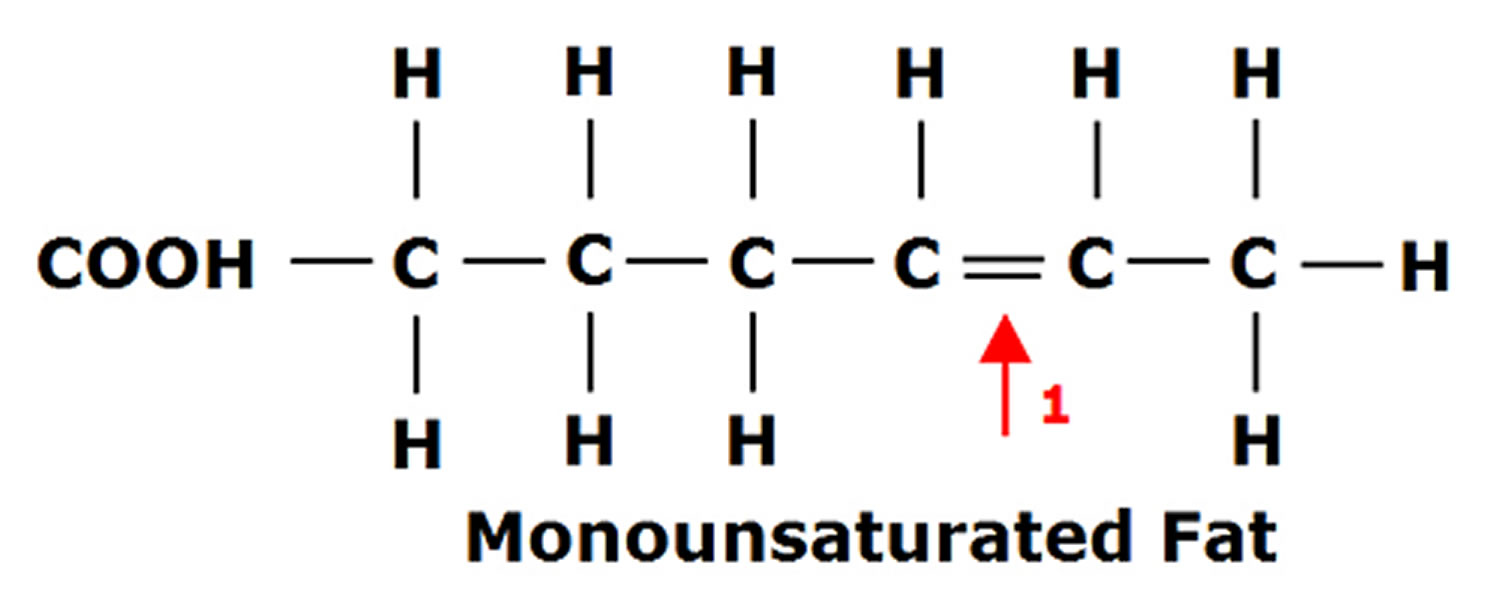
Figure 4. Polyunsaturated Fatty Acids Structure
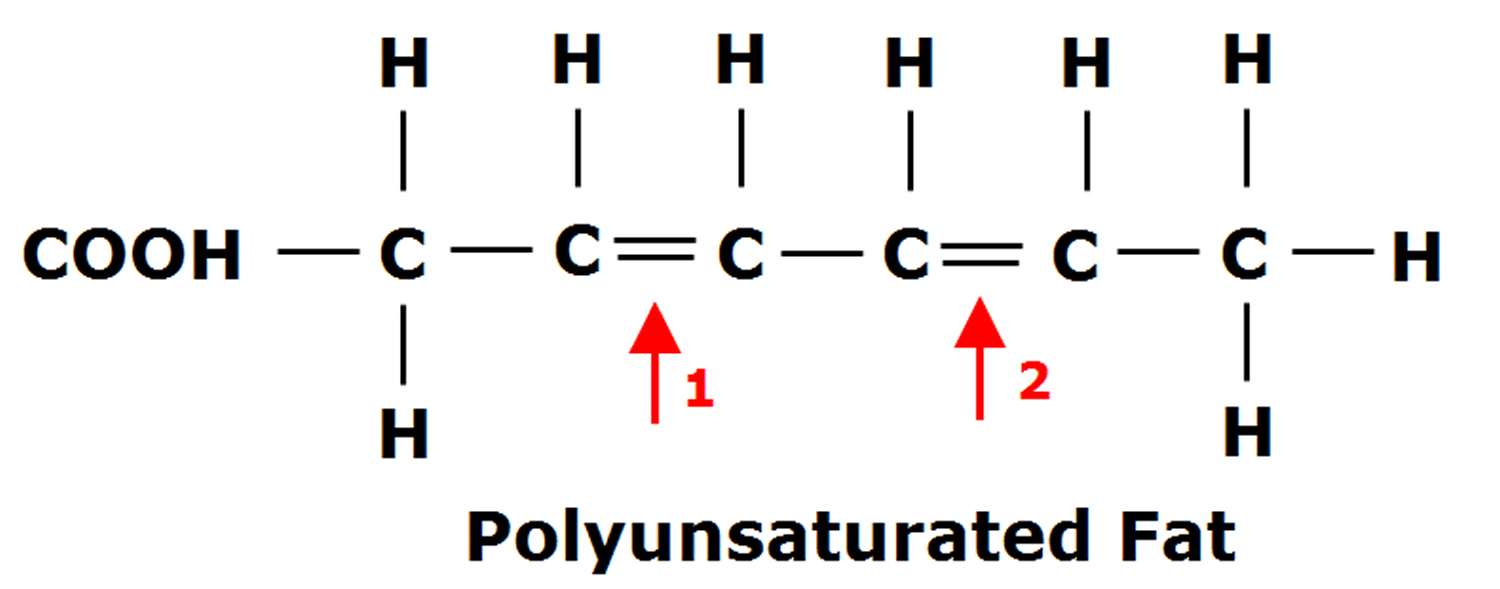
Figure 5. Saturated Fatty Acids Structure
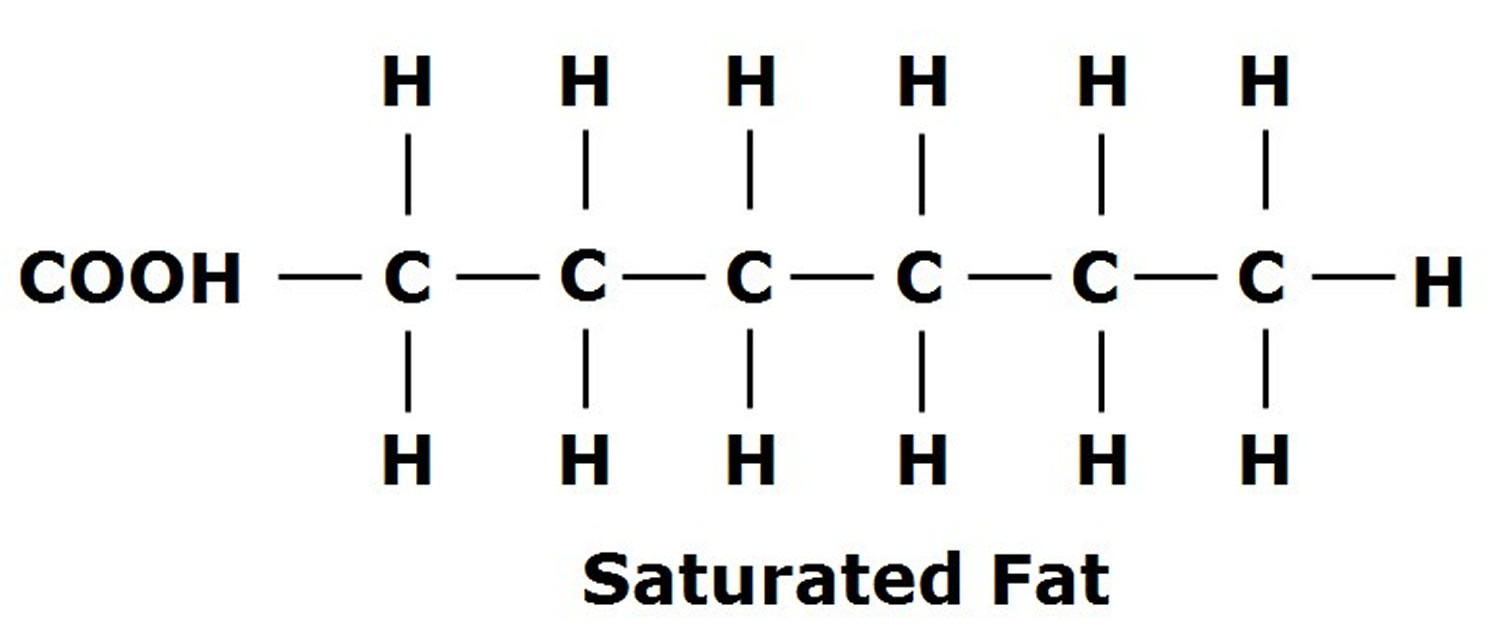
Note: Saturated fatty acids (SFA) without double bonds
Table 6. Selected monounsaturated fatty acids
| C-Atoms: Double Bonds | Scientific Name of Acid | Molecular Formula | Chemical Name |
|---|---|---|---|
| 11:1 | Undecylenic | C10H19COOH | cis-10-undecenoic acid |
| 14:1 | Myristoleic | C13H25COOH | cis-9-tetradecenoic acid |
| 16:1 | Palmitoleic | C15H29COOH | cis-9-hexadecenoic acid |
| 16:1 | Palmitelaidic | C15H29COOH | trans-9-hexadecenoic acid |
| 16:1 | / | C15H29COOH | cis-7-hexadecenoic |
| 18:1 | Petroselinic | C17H33COOH | cis-6-octadecenoic acid |
| 18:1 | Oleic | C17H33COOH | cis-9-octadecenoic acid |
| 18:1 | Elaidic | C17H33COOH | trans-9-octadecenoic acid |
| 18:1 | Vaccenic | C17H33COOH | cis-11-octadecenoic acid |
| 20:1 | Gondoleic | C19H37COOH | cis-9-eicosenoic acid |
| 20:1 | Gondolic | C19H37COOH | cis-11-eicosenoic acid |
| 22:1 | Cetoleic | C21H41COOH | cis-11-docosenoic acid |
| 22:1 | Erucic | C21H41COOH | cis-13-docosenoic acid |
| 24:1 | Nervonic | C23H45COOH | cis-15-tetracosaenoic acid |
General Nutrition Guidelines on Monounsaturated Fatty Acids (MUFA)
Based upon 13 peer-reviewed background papers dealing with fats and fatty acids in human nutrition, the Joint FAO/WHO Expert Consultation Committee concluded that replacement of carbohydrates by MUFA beneficially increases HDL-cholesterol, while the substitution of SFA with MUFA exerts favorable effects on LDL-cholesterol and the ratio of total cholesterol to HDL-cholesterol 17. In their position on dietary fatty acids of 2007, the American and Canadian Dietetic Association suggested a high maximum quota of MUFA, i.e., <25% of total energy content 18. Less than 20% of total energy content should be consumed in the form of MUFA as recommended by the American Heart Association in 2006, which is interesting with respect to the fact that the corresponding value was only <15% in the year 2000-statement 19 of the American Heart Association 20. The National Cholesterol Education Program III suggested that <20% of total energy content should be consumed in the form of MUFA 21. In their Dietary Guidelines for Americans, edition 2015-2020, the United States Department of Agriculture (USDA) gives no specific recommendations for MUFA 22. In addition, the National Institute of Medicine did not mention any specific recommendations for MUFA 23. In their statement, they concluded that “n-9 cis Monounsaturated fatty acids are synthesized by the body and have no known independent beneficial role in human health and are not required in the diet.” Therefore, neither an Adequate Intake nor a Recommended Daily Allowance was set. Since there is insufficient evidence for an Upper Level as well, the Dietary Reference Intakes did not consider MUFA at all 23. In accordance with these proceedings and with a similar rationale, the European Food and Safety Authority (EFSA) skipped MUFA in their scientific opinions on dietary reference values for fat 24. On a national level, the recommendations given in European countries are far from being conclusive. The Italian Society of Human Nutrition did not list any specific references for MUFA 25. The Joint Committees of Germany, Austria, and Switzerland stated that MUFA consumption should be 10% of TEC, albeit with higher intakes being acceptable 26. The Nordic Nutrition Recommendations agreed on 10%–15% of total energy content in the form of MUFA 27. The particulars of the Dutch Dietary Guidelines proposed a limit of 38% of total energy content in the form of MUFA and PUFA for people with optimal body weight, whereas overweight and obese people should be more restrictive and limit their daily energy uptake in the form of MUFA/PUFA to 28% 28. The UK COMA Committee advocated that MUFA (in the form of oleic acid) should provide an average of 12% of total energy content 29. The Nutritional Recommendations for the French Population promoted an intake of MUFA up to 20% of total energy content for adults including pregnant and lactating women. It was emphasized that the neutrality of oleic acid represents a benefit and that its consumption was justified 30.
Table 7. National and international MUFA recommendations for healthy adults and patients with diabetes
| Authority/Society | MUFA (% of TEC) | Target Group/Remarks |
|---|---|---|
| American Heart Association | <20 | Healthy adults |
| Academy of Nutrition and Dietetics/Canadian Dietetic Association | <25 | Healthy adults |
| Dutch Dietary Guidelines | 8–38 | Healthy adults Upper limit for obese: 25% of TEC |
| European Food Safety Authority | No specific recommendations | Healthy adults |
| Italian Society of Human Nutrition | No specific recommendations | Healthy adults |
| Joint Committees of Germany, Austria, and Switzerland | 10 | Healthy adults |
| National Cholesterol Educational Program III | <20 | Healthy adults |
| National Institute of Medicine | No specific recommendations | Healthy adults |
| Nordic Nutrition Dietary Guidelines | 10–15 | Healthy adults |
| Nutritional Recommendations for the French Population | 20 | Healthy adults Including pregnant and lactating women |
| UK COMA Committee | 12 | Healthy adults |
| US Department of Agriculture | No specific recommendations | Healthy adults |
| World Health Organization/Food Agriculture Organization | 15–20 | Healthy adults Adjusted to total fat intake |
| American Association of Clinical Endocrinologists | No specific recommendations | Diabetic patients |
| American Diabetes Association | No specific recommendations | Diabetic patients Initial recommendation: 10%–20% of TEC |
| British Diabetes Association | 10–15 | Diabetic patients |
| Canadian Diabetes Association | No specific recommendations | Diabetic patients Replacement of SFA by MUFA |
| European Association for the Study of Diabetes | 10–20 | Diabetic patients Limitation of total fat to 35% of TEC |
| International College of Nutrition of India | 7 | Diabetic patients |
Note: MUFA = monounsaturated fatty acids; SFA = saturated fatty acids; TEC = total energy content.
Benefits of olive oil
The main type of fat found in all kinds of olive oil is monounsaturated fatty acids (MUFAs). Monounsaturated fatty acids are considered a healthy dietary fat 31. Olive oil consumption is thought to affect cardiovascular health 32. If you replace saturated and trans fats with unsaturated fats, such as monounsaturated fatty acids (MUFAs) and polyunsaturated fats (PUFAs), you may gain certain health benefits. In this meta-analysis 32, comparison of the top versus the bottom third of combined MUFA subgroups (MUFA, olive oil, oleic acid, and MUFA:Saturated Fatty Acid) was associated with reduced risk of all-cause mortality (11%), cardiovascular mortality (12%), combined cardiovascular events (9%), and stroke (17%). Monounsaturated fatty acids (MUFAs) and polyunsaturated fats (PUFAs) may help lower your risk of heart disease by improving related risk factors. For instance, monounsaturated fatty acids (MUFAs) have been found to lower total cholesterol and low-density lipoprotein (LDL) cholesterol levels. Even healthier fats like olive oil are high in calories, so use them in moderation.
Epidemiological studies indicate that a higher proportion of monounsaturated fats in the diet may be linked with a reduction in the risk of coronary heart disease 33. There is preliminary evidence that regular consumption of olive oil may lower risk of all-cause mortality and several chronic diseases 32, 34.
In addition, some research shows that MUFAs may benefit insulin levels and blood sugar control, which can be helpful if you have or are at risk of type 2 diabetes 35, 36, 37, 38.
In a comprehensive scientific review by the European Food Safety Authority (EFSA) in 2011, health claims on olive oil were approved for protection by its polyphenols against oxidation of blood lipids 39 and for the contribution to the maintenance of normal blood LDL-cholesterol levels by replacing saturated fats in the diet with oleic acid 40 (Commission Regulation (EU) 432/2012 of 16 May 2012) 41. A cause-and-effect relationship has not been adequately established for consumption of olive oil and maintaining normal (fasting) blood concentrations of triglycerides, normal blood HDL-cholesterol concentrations, and normal blood glucose concentrations 42.
A 2011 meta-analysis concluded that olive oil consumption may play a protective role against the development of any type of cancer, but could not clarify whether the beneficial effect is due to olive oil monounsaturated fatty acid content or its polyphenol components 43.
A 2014 meta-analysis concluded that an elevated consumption of olive oil is associated with reduced risk of all-cause mortality, cardiovascular events and stroke, while monounsaturated fatty acids of mixed animal and plant origin showed no significant effects 32.
In the United States, producers of olive oil may place the following restricted health claim on product labels:
“Limited and not conclusive scientific evidence suggests that eating about 2 tablespoons (23 grams) of olive oil daily may reduce the risk of coronary heart disease due to the monounsaturated fat in olive oil. To achieve this possible benefit, olive oil is to replace a similar amount of saturated fat and not increase the total number of calories you eat in a day. One serving of this product contains [x] grams of olive oil” 44.
Similar labels are permitted for canola oil: “Limited and not conclusive scientific evidence suggests that eating about 1 ½ tablespoons (19 grams) of canola oil daily may reduce the risk of coronary heart disease due to the unsaturated fat content in canola oil. To achieve this possible benefit, canola oil is to replace a similar amount of saturated fat and not increase the total number of calories you eat in a day. One serving of this product contains [x] grams of canola oil” 45 and foods rich in omega-3 fatty acids: “Supportive but not conclusive research shows that consumption of EPA and DHA omega-3 fatty acids may reduce the risk of coronary heart disease. One serving of [Name of the food] provides [ ] gram of EPA and DHA omega-3 fatty acids. [See nutrition information for total fat, saturated fat, and cholesterol content.]” 46 and hemp seed oil 47.
Olive oil for skin care
Olive oil has a long history of being used as a home remedy for skincare. Egyptians used it alongside beeswax as a cleanser, moisturizer, and antibacterial agent since pharaonic times 48. In ancient Greece, olive oil was used during massage, to prevent sports injuries, relieve muscle fatigue, and eliminate lactic acid buildup. In 2000, Japan was the top importer of olive oil in Asia (13,000 tons annually) because consumers there believe both the ingestion and topical application of olive oil to be good for skin and health 49.
Olive oil is popular for use in massaging infants and toddlers, but scientific evidence of its efficacy is mixed. One analysis of olive oil versus mineral oil found that, when used for infant massage, olive oil can be considered a safe alternative to sunflower, grapeseed and fractionated coconut oils. This stands true particularly when it is mixed with a lighter oil like sunflower, which “would have the further effect of reducing the already low levels of free fatty acids present in olive oil” 50. Another trial stated that olive oil lowered the risk of dermatitis for infants in all gestational stages when compared with emollient cream 51. However, another study 52 involving one-hundred and fifteen healthy, full-term neonates with a family history of atopic eczema (atopic dermatitis) were randomly assigned to olive oil, sunflower oil or no oil, twice daily for 4 weeks. Some research has suggested that there is a potential for development of atopic eczema (atopic dermatitis) if topical products with adverse effects on skin barrier function are used for the prevention or treatment of baby dry skin 53, 54. The results of that study showed there were no significant differences in trans-epidermal water loss, pH or erythema/skin scores 52. The sunflower oil was found to have a similar effect on skin barrier function to olive oil. Moreover, the findings of that study 52 suggest that using olive oil or sunflower oil may have the potential to damage the skin barrier function of neonatal skin. This could consequently increase the development of atopic eczema (atopic dermatitis). Another study on adults found that topical treatment with olive oil “significantly damages the skin barrier” when compared to sunflower oil, and that it may make existing atopic dermatitis worse. The researchers concluded that due to the negative outcome in adults, they do not recommend the use of olive oil for the treatment of dry skin and infant massage 55.
Applying olive oil to the skin does not help prevent or reduce stretch marks 56.
This double-blind randomized clinical trial study on the effect of topical olive oil on the healing of foot ulcer in patients with type 2 diabetes 57 indicated that olive oil in combination with routine cares is more effective than routine cares alone. Olive oil significantly decreased ulcer area and depth compared with control group who just received routine cares. Complete ulcer healing in the intervention group was significantly greater than control group at the end of follow up. Also, there were no adverse effects to report during the study in intervention group.
References- Ryan D., Robards K. Phenolic compounds in olives. Analyst. 1998;123:31R–44R.
- Boskou D. History and characteristics of the olive tree. In: Boskou D., editor. Olive Oil Chemistry and Technology. Am. Oil Chem. Soc. Press; Champaign, IL, USA: 1996.
- Wikipedia. Olive oil. https://en.wikipedia.org/wiki/Olive_oil
- Bergouignan A, Momken I, Schoeller DA, Simon C, Blanc S. Metabolic fate of saturated and monounsaturated dietary fats: the Mediterranean diet revisited from epidemiological evidence to cellular mechanisms. Prog Lipid Res. 2009 May-Jul;48(3-4):128-47. doi: 10.1016/j.plipres.2009.02.004. Epub 2009 Mar 9. https://www.ncbi.nlm.nih.gov/pubmed/19275915
- FAOSTAT Crops Processed Data for Olive Oil. FAO; Rome, Italy: 2009. http://www.fao.org/faostat/en/#data/QD
- Fernández A.G., Díez M.J.F., Adams M.R. Table Olives: Production and Processing. Chapman & Hall; London, UK: 1997. p. 478.
- Australian Extra Virgin Olive Oil. http://australianextravirgin.com.au/the-best-olive-oil-in-the-world/
- The Olive Oil Source. https://www.oliveoilsource.com/page/chemical-characteristics
- United States Department of Agriculture Agricultural Research Service. USDA Branded Food Products Database. https://ndb.nal.usda.gov/ndb/search/list
- “Olive Oil : Chemical Characteristics”. https://www.oliveoilsource.com/page/chemical-characteristics
- Boskou D. Polar phenolic compounds. In: Boskou D., editor. Olive Oil: Chemistry and Technology. Am. Oil Chem. Soc. Press; Champaign, IL, USA: 2006. pp. 73–92.
- International Olive Council. http://www.internationaloliveoil.org/
- Beltran; et al. (2004). “Influence of Harvest Date and Crop Yield on the Fatty Acid Composition of Virgin Olive Oils from Cv. Picual” http://hera.ugr.es/doi/15058025.pdf
- Ghanbari R, Anwar F, Alkharfy KM, Gilani A-H, Saari N. Valuable Nutrients and Functional Bioactives in Different Parts of Olive (Olea europaea L.)—A Review. International Journal of Molecular Sciences. 2012;13(3):3291-3340. doi:10.3390/ijms13033291. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3317714/
- Schwingshackl L, Hoffmann G. Monounsaturated Fatty Acids and Risk of Cardiovascular Disease: Synopsis of the Evidence Available from Systematic Reviews and Meta-Analyses . Nutrients. 2012;4(12):1989-2007. doi:10.3390/nu4121989. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3546618/
- AHA Science Advisory. Monounsaturated fatty acids and risk of cardiovascular disease. American Heart Association. Nutrition Committee. Kris-Etherton PM. Circulation. 1999 Sep 14; 100(11):1253-8. http://circ.ahajournals.org/content/100/11/1253.long
- Fats and Fatty Acids in Human Nutrition. Report of an Expert Consultation. http://www.fao.org/docrep/013/i1953e/i1953e00.pdf
- Kris-Etherton P.M., Innis S. Ammerican Dietetic Assocition; Dietitians of Canada. Position of the American Dietetic Association and the Dietitians of Canada: Dietary fatty acids. J. Am. Diet. Assoc. 2007;107:1599–1611. https://www.ncbi.nlm.nih.gov/pubmed/17936958
- Krauss R.M., Eckel R.H., Howard B.V., Appel L.J., Daniels S.R., Deckelbaum R.J., Erdman J.W., Jr., Kris-Etherton P., Goldberg I.J., Kotchen T.A., et al. AHA Dietary Guidelines: Revision 2000: A statement for healthcare professionals from the Nutrition Committee of the American Heart Association. Stroke. 2000;31:2751–2766. http://stroke.ahajournals.org/content/31/11/2751.long
- Lichtenstein A.H., Appel L.J., Brands M., Carnethon M., Daniels S., Franch H.A., Franklin B., Kris-Etherton P., Harris W.S., Howard B., et al. Diet and lifestyle recommendations revision 2006: A scientific statement from the American Heart Association Nutrition Committee. Circulation. 2006;114:82–96. doi: 10.1161/CIRCULATIONAHA.106.176158. http://circ.ahajournals.org/content/114/1/82.long
- Expert Panel on Detection, Valuation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) JAMA. 2001;285:2486–2497. doi: 10.1001/jama.285.19.2486. https://www.ncbi.nlm.nih.gov/pubmed/11368702
- Office of Disease Prevention and Health Promotion. https://health.gov/dietaryguidelines/
- Institute of Medicine of the National Academies. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients) The National Academy Press; Washington, DC, USA: 2002. Dietary Fats: Total Fat and Fatty Acids; pp. 335–342. https://www.ncbi.nlm.nih.gov/pubmed/12449285
- European Food Safety Authority (EFSA) Scientific Opinion on Dietary Reference Values for fats, including saturated fatty acids, polyunsaturated fatty acids, monounsaturated fatty acids, trans fatty acids, and cholesterol. EFSA J. 2010;8:1461.
- Lipidi. http://www.sinu.it/html/cnt/home.asp
- German Nutrition Society; Austrian Nutrition Society; Swiss Society for Nutrition Research; Swiss Nutrition Association. Reference Values for Nutrient Intake. Umschau Braus Publishers; Frankfurt, Germany: 2008.
- Nordic Nutrition Recommendations (NNR) Integrating Nutrition and Physical Activity. Nordic Council of Ministers; Copenhagen, Denmark: 2004. p. 436.
- Spaaij C.J.K., Pijls L.T.J. New dietary reference intakes in the Netherlands for energy, proteins, fats and digestible carbohydrates. Eur. J. Clin. Nutr. 2004;58:191–194. doi: 10.1038/sj.ejcn.1601788. https://www.ncbi.nlm.nih.gov/pubmed/14679385
- Great Britain Department of Health. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom: Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy. Stationery Office; London, UK: 1991. https://www.ncbi.nlm.nih.gov/pubmed/1961974
- Agence Francaise de Sécurité Sanitaire des Aliments (AFSSA) Apports Nutritionnels Conseillés pour la Population Francaise. Editions Tec & Doc; Paris, France: 2001. p. 605.
- Mayo Foundation for Medical Education and Research. If olive oil is high in fat, why is it considered healthy? http://www.mayoclinic.org/healthy-lifestyle/nutrition-and-healthy-eating/expert-answers/food-and-nutrition/faq-20058439
- Schwingshackl L, Hoffmann G. Monounsaturated fatty acids, olive oil and health status: a systematic review and meta-analysis of cohort studies. Lipids in Health and Disease. 2014;13:154. doi:10.1186/1476-511X-13-154. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4198773/
- Keys A, Menotti A, Karvonen MJ, et al. (December 1986). “The diet and 15-year death rate in the seven countries study”. Am. J. Epidemiol. 124 (6): 903–15. https://www.ncbi.nlm.nih.gov/pubmed/3776973
- Buckland G, González CA (Apr 2015). “The role of olive oil in disease prevention: a focus on the recent epidemiological evidence from cohort studies and dietary intervention trials” (PDF). Br J Nutr (Review). 113 Suppl 2: S94–101. https://www.cambridge.org/core/journals/british-journal-of-nutrition/article/role-of-olive-oil-in-disease-prevention-a-focus-on-the-recent-epidemiological-evidence-from-cohort-studies-and-dietary-intervention-trials/067113B01A4A7254066C542D640BC1AE/core-reader
- Schwingshackl L, Strasser B, High-MUFA Diets Reduce Fasting Glucose in Patients with Type 2 Diabetes. Ann Nutr Metab 2012;60:33-34. https://www.ncbi.nlm.nih.gov/pubmed/22212514
- Garg A. High-monounsaturated-fat diets for patients with diabetes mellitus: a meta-analysis. Am J Clin Nutr. 1998 Mar;67(3 Suppl):577S-582S. http://ajcn.nutrition.org/content/67/3/577S.long
- Kotake J, Tanaka Y, Umehara N, Miyashita A, Tsuru T, Hikida S, Mizote H. Effects of a high-monounsaturated fat diet on glucose and lipid metabolisms in normal and diabetic mice. J Nutr Sci Vitaminol (Tokyo). 2004 Apr;50(2):106-13. https://www.ncbi.nlm.nih.gov/pubmed/15242014
- Monounsaturated Fatty Acid–Enriched High-Fat Diets Impede Adipose NLRP3 Inflammasome–Mediated IL-1β Secretion and Insulin Resistance Despite Obesity. Diabetes 2015 Jun; 64(6): 2116-2128. https://doi.org/10.2337/db14-1098. http://diabetes.diabetesjournals.org/content/64/6/2116.long
- European Food Safety Authority (2011). “Scientific Opinion on the substantiation of health claims related to polyphenols in olive”. EFSA Journal. 9 (4): 2033. http://onlinelibrary.wiley.com/doi/10.2903/j.efsa.2011.2033/pdf
- European Food Safety Authority (2011). “Scientific Opinion on the substantiation of health claims related to oleic acid intended to replace saturated fatty acids (SFAs) in foods or diets”. EFSA Journal. 9 (4): 2043. http://onlinelibrary.wiley.com/doi/10.2903/j.efsa.2011.2043/pdf
- “COMMISSION REGULATION (EU) No 432/2012 of 16 May 2012 establishing a list of permitted health claims made on foods, other than those referring to the reduction of disease risk and to children’s development and health. Text with EEA relevance” http://eur-lex.europa.eu/eli/reg/2012/432/oj
- Scientific Committee/Scientific Panel of the European Food Safety Authority (2011). “Scientific Opinion on the substantiation of health claims related to olive oil and maintenance of normal blood LDL-cholesterol concentrations (ID 1316, 1332), maintenance of normal (fasting) blood concentrations of triglycerides (ID 1316, 1332), maintenance of normal blood HDL cholesterol concentrations (ID 1316, 1332) and maintenance of normal blood glucose concentrations (ID 4244) pursuant to Article 13(1) of Regulation (EC) No 1924/2006” (PDF). EFSA Journal. European Commission. 9 (4): 2044 [19 pp]. http://onlinelibrary.wiley.com/doi/10.2903/j.efsa.2011.2044/pdf
- Psaltopoulou T, Kosti RI, Haidopoulos D, Dimopoulos M, Panagiotakos DB. Olive oil intake is inversely related to cancer prevalence: a systematic review and a meta-analysis of 13800 patients and 23340 controls in 19 observational studies. Lipids in Health and Disease. 2011;10:127. doi:10.1186/1476-511X-10-127. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3199852/
- U.S. Food and Drug Administration. Letter Responding to Health Claim Petition dated August 28, 2003: Monounsaturated Fatty Acids from Olive Oil and Coronary Heart Disease (Docket No 2003Q-0559). https://www.fda.gov/food/ingredientspackaginglabeling/labelingnutrition/ucm072963.htm
- U.S. Food and Drug Administration. Qualified Health Claims: Letter of Enforcement Discretion – Unsaturated Fatty Acids from Canola Oil and Reduced Risk of Coronary Heart Disease (Docket No. 2006Q-0091). https://www.fda.gov/food/ingredientspackaginglabeling/labelingnutrition/ucm072958.htm
- U.S. Food and Drug Administration. Letter Responding to Health Claim Petition dated November 3, 2003 (Martek Petition): Omega-3 Fatty Acids and Reduced Risk of Coronary Heart Disease (Docket No. 2003Q-0401). https://www.fda.gov/food/ingredientspackaginglabeling/labelingnutrition/ucm072932.htm
- U.S. Food and Drug Administration. GRAS Notice 000035: Hempseed oil. https://www.fda.gov/downloads/food/ingredientspackaginglabeling/gras/noticeinventory/ucm265977.pdf
- Grossman, A. J. (September 27, 2007). “Behind a Mysterious Balm, a Self-Made Pharaoh”. The New York Times. http://www.nytimes.com/2007/09/27/fashion/27SKIN.html
- Shoji, K. (February 26, 2013). “The Japanese woman’s perpetual quest for perfect skin”. The New York Times. http://www.nytimes.com/2004/02/26/news/the-japanese-womans-perpetual-quest-for-perfect-skin.html
- Carpenter, P.; Richards, K. (2011). “Olive versus mineral oil”. Community practitioner : the journal of the Community Practitioners’ & Health Visitors’ Association. 84 (2): 40–42. https://www.ncbi.nlm.nih.gov/pubmed/21388045
- Kiechl-Kohlendorfer, U.; Berger, C.; Inzinger, R. (2008). “The Effect of Daily Treatment with an Olive Oil/Lanolin Emollient on Skin Integrity in Preterm Infants: A Randomized Controlled Trial”. Pediatric Dermatology. 25 (2): 174–178. https://www.ncbi.nlm.nih.gov/pubmed/18429773
- Cooke A, Cork MJ, Victor S, Campbell M, Danby S, Chittock J, Lavender T. Olive Oil, Sunflower Oil or no Oil for Baby Dry Skin or Massage: A Pilot, Assessor-blinded, Randomized Controlled Trial (the Oil in Baby SkincaRE [OBSeRvE] Study). Acta Derm Venereol. 2016 Mar;96(3):323-30. https://www.medicaljournals.se/acta/content/html/10.2340/00015555-2279
- Danby S, Al Enezi T, Sultan A, Lavender T, Chittock J, Brown K, et al. Effect of olive and sunflower seed oil on the adult skin barrier: implications for neonatal skin care. Pediatr Dermatol 2013; 30: 42–50.
- Silverberg J, Lee-Wong M, Silverberg N. Complementary and alternative medicines and childhood eczema: a US population-based study. Dermatitis 2014; 25: 246–254.
- Danby, S. G.; Alenezi, T.; Sultan, A.; Lavender, T.; Chittock, J.; Brown, K.; Cork, M. J. (2013). “Effect of Olive and Sunflower Seed Oil on the Adult Skin Barrier: Implications for Neonatal Skin Care”. Pediatric Dermatology. 30 (1): 42–50. https://www.ncbi.nlm.nih.gov/pubmed/22995032
- Moore J, Kelsberg G, Safranek S (December 2012). “Clinical Inquiry: Do any topical agents help prevent or reduce stretch marks?”. J Fam Pract. 61 (12): 757–8.
- Nasiri M, Fayazi S, Jahani S, Yazdanpanah L, Haghighizadeh MH. The effect of topical olive oil on the healing of foot ulcer in patients with type 2 diabetes: a double-blind randomized clinical trial study in Iran. Journal of Diabetes and Metabolic Disorders. 2015;14:38. doi:10.1186/s40200-015-0167-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4428202/





{kind=link}