What is ovarian torsion
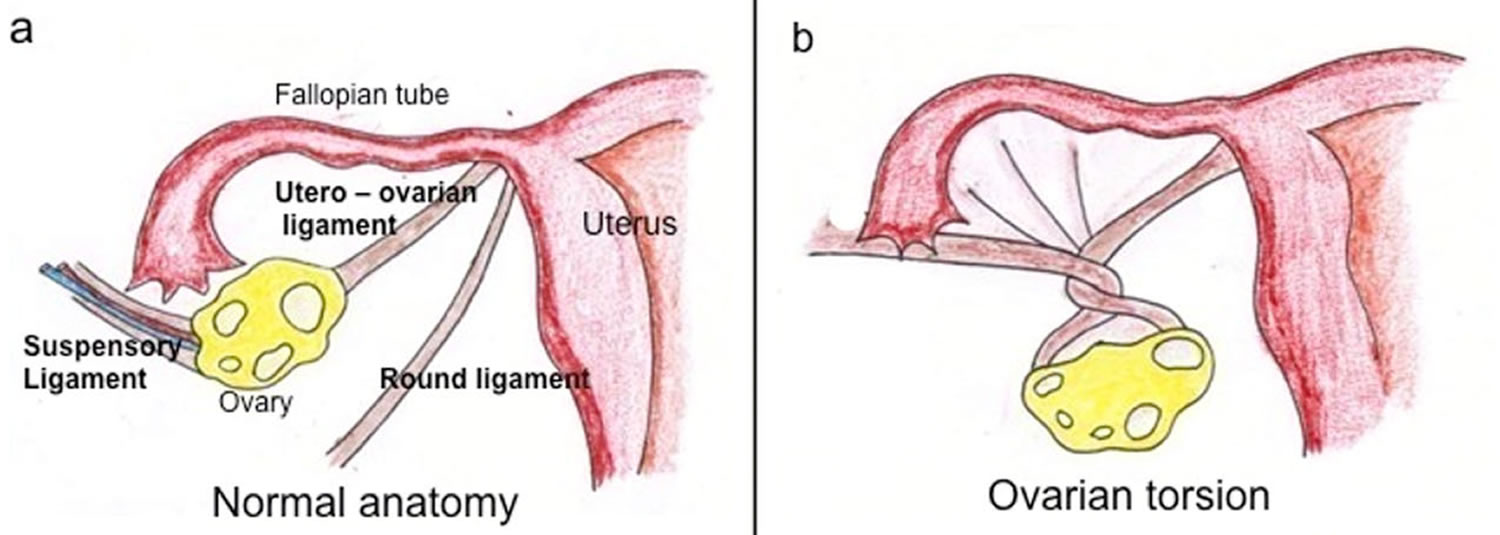
Ovarian torsion also sometimes termed adnexal torsion or tubo-ovarian torsion, refers to rotation of the ovary and portion of the fallopian tube on the supplying vascular pedicle leading to reduced venous return, stromal edema, internal hemorrhage, and infarction with the subsequent complications 1. The result of vascular compromise secondary to ovarian torsion is hemorrhagic infarction and necrosis, that can occur as rapidly as within hours of torsion onset. Ovarian torsion can be intermittent or sustained and results in venous, arterial and lymphatic stasis. It is a gynecological emergency and requires urgent surgical intervention to prevent ovarian necrosis. Ovarian torsion classically occurs unilaterally in a pathologically enlarged ovary. Torsion of a normal ovary is most common among young children 2.
Ovarian torsion has a bimodal age distribution occurring mainly in young women (15-30 years) and post-menopausal women. Approximately 20% of the cases occur during pregnancy 3. Studies reveal that ovarian torsion is the fifth most common gynecologic surgical emergency, accounting for 2.7% of cases of acute gynecologic complaints in 1 series. Ovarian torsion is encountered more often in women who have had ovarian stimulation, which likely accounts for a slightly increased incidence in developed countries.
The median age reported by a large review was 28 years. The percentage of patients younger than 30 years is approximately 70-75%. Two groups of women show a particular tendency to be affected by adnexal torsion (ovarian torsion): (1) women in their mid 20s and (2) women who are postmenopausal.
Approximately 20% of cases of torsion occur during pregnancy 4. Postmenopausal women with an adnexal mass may also be affected. Adolescents are also at risk; this may be because of changes in the weight of their maturing adnexa 4. Approximately 17% of cases have been found to occur in premenarchal or postmenopausal women. Although ovarian torsion in very young children is rare, a case of ovarian cyst torsion was reported in a 2-year-old 5.
What causes ovarian torsion?
Ovarian torsion occurs due to two main reasons 6:
- Hypermobility of the ovary: <50%
- Adnexal mass: ~50-80%
- most lesions are dermoid cysts or para ovarian cysts
- large cystic ovaries undergoing ovarian hyperstimulation are at particular risk
- masses between 5-10 cm are at most risk 7
Torsion of a normal ovary more commonly occurs in young children when developmental abnormalities predispose the ovary to torsion, such as excessively long Fallopian tubes or an absent mesosalpinx.
In adulthood, causes include both benign and malignant ovarian tumors, polycystic ovaries and adhesions. In early pregnancy, a torsion can occur secondary to a corpus luteal cyst or laxity of the adjacent tissues.
Anatomic changes affecting the weight and the size of the ovary may alter the position of the fallopian tube and allow twisting to occur.
Pregnancy is associated with, and may be responsible for, torsion in approximately 20% of adnexal torsion cases 8, probably secondary to the ovarian enlargement that occurs during ovulation in combination with laxity of the supporting tissues of the ovary.
Congenitally malformed and elongated fallopian tubes may be seen, particularly in young, prepubertal patients.
Ovarian tumors, both benign and malignant, are implicated in 50-60% of cases of torsion. Involved masses are nearly all larger than 4-6 cm, although torsion is still possible with smaller masses. Dermoid tumors are most common. Malignant tumors are much less likely to result in torsion than benign tumors are. This is because of the presence of cancerous adhesions that fix the ovary to surrounding tissues.
Conversely, patients with a history of pelvic surgery (principally tubal ligation) are at increased risk for torsion, probably because of adhesions that provide a site around which the ovarian pedicle may twist.
Ovarian torsion signs and symptoms
Most patients present with severe non-specific lower abdominal and pelvic pain, either intermittent or sustained, nausea, and vomiting. There is adnexal tenderness. A raised white cell count is common.
Classically, patients present with the sudden onset (commonly during exercise or other agitating movement) of severe, unilateral lower abdominal pain that worsens intermittently over many hours. A minority of patients, however, complain of mild pain that follows a more prolonged time course. The pain usually is localized over the involved side, often radiating to the back, pelvis, or thigh. Approximately 25% of patients experience bilateral lower quadrant pain. It may be described as sharp and stabbing or, less frequently, crampy.
Nausea and vomiting occur in approximately 70% of patients, mimicking a gastrointestinal source of pain and further obscuring the diagnosis.
A history of previous episodes may be elicited, possibly attributable to partial, spontaneously resolving torsion. Fever may occur as a late finding as the ovary becomes necrotic.
Ovarian torsion in premenarchal girls is associated with a longer interval from onset of symptoms and an increased rate of fever and pelvic mass at presentation compared with postmenarchal patients, according to one study. Median duration of symptoms before presentation was 24 hours for premenarchal patients, versus 8 hours for postmenarchal patients 9. In another study, of 32 premenarchal patients with ovarian torsion, the main presenting symptoms were abdominal pain (92.3%) and nausea and vomiting (84.6%). Abdominal tenderness was present in 64.1%.On abdominal ultrasound, an enlarged ovary was identified in 28.9% 10.
In a retrospective study of ovarian torsion in premenarchal and postmenarchal patients in Israel, there was a higher frequency of nausea and vomiting in the premenarchal patients. Ovarian cysts were more commonly demonstrated in postmenarchal patients, and a normal adnexal appearance on ultrasound was more common in premenarchal patients. Because of a normal adnexa in 69% of cases in premenarchal patients, a high index of suspicion is necessary in any premenarchal patient with acute-onset abdominal pain 11.
Ovarian torsion in the third trimester of pregnancy is likely to present as nonspecific symptoms of lower abdominal pain, nausea, and vomiting and can often be misdiagnosed as appendicitis or preterm labor. Although conservative treatment has been proposed during pregnancy, surgical intervention may be necessary if ovarian torsion is highly suspected. Ultrasonography in early pregnancy should address the cervix and the adnexa for early diagnosis and management of ovarian masses, thus avoiding later emergency situations and the possibility of preterm deliveries 12.
Signs of ovarian torsion
The whirlpool sign or whirl sign of ovarian torsion is characterized by the appearances of a twisted ovarian pedicle seen on ultrasound or even on CT scan. It appears as twisting of the thickened vascular pedicle of the enlarged ovary. It can be detected on ultrasound confirming the diagnosis along with the other suggestive imaging features and clinical presentation 13. On MRI, it is best demonstrated on axial T2 and T1 C+ fat sat sequences 14.
Figure 1. Whirl sign of ovarian torsion
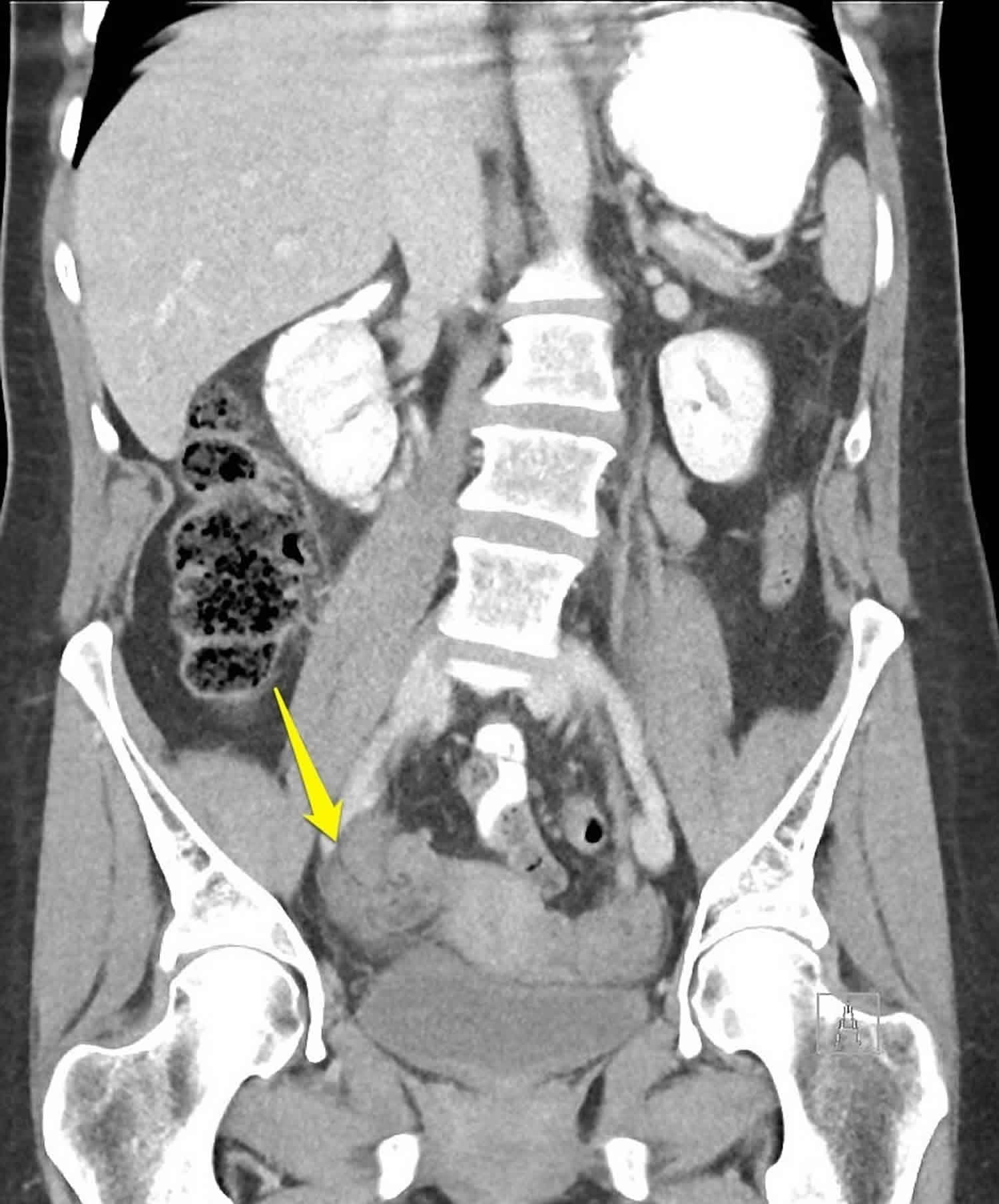
Footnote: 50 year old female with acute severe right iliac fossa pain. Yellow arrow indicates torted ovarian pedicle, note the “whirl” pattern.
[Source 15 ]Ovarian torsion complications
Complications of ovarian torsion include the following:
- Infection
- Peritonitis
- Sepsis
- Adhesions
- Chronic pain
- Infertility (rare)
Ovarian torsion diagnosis
The physical examination, like the history, is typically nonspecific and is highly variable. A unilateral, tender adnexal mass has been reported in between 50 and 90% of patients. However, the absence of such a finding does not exclude the diagnosis. Tenderness to palpation is common; however, it is mild in approximately 30% and absent in another 30% of patients. Therefore, the absence of tenderness cannot be used to rule out torsion.
Peritoneal findings are infrequent and indicate advanced disease if present.
Radiographic features
The main feature of torsion is ovarian enlargement due to venous/lymphatic engorgement, edema and hemorrhage. Secondary signs include free pelvic fluid, an underlying ovarian lesion, reduced or absent vascularity and a twisted dilated tubular structure corresponding to the vascular pedicle. Adnexal torsion is commonly unilateral, with a slight (3:2) right-sided predilection (presumably due to the protective effects of the sigmoid colon on the left) 16.
Diagnostic ultrasonography should be the first examination performed; typically, the affected ovary is enlarged, with multiple immature or small follicles along its periphery.
Ultrasonography with color Doppler analysis is the method of choice for the evaluation of adnexal torsion because it can show morphologic and physiologic changes in the ovary and can help in determining whether blood flow is impaired 17. Gray-scale and spectral findings are correlated with the age of the torsion (ie, acute torsion or chronic torsion) and the degree of the twist or torsion. Normal Doppler imaging must not, however, be used as a basis for excluding the diagnosis.
Rarely, computed tomography (CT) or magnetic resonance imaging (MRI) is needed to make a definitive diagnosis. CT or MRI can serve as a secondary modality when ultrasonographic findings are nondiagnostic 18.
Culdocentesis is a nonspecific test that is unlikely to confirm or exclude torsion and therefore is not recommended in the diagnostic workup.
Ovarian torsion treatment
In a patient with a history and physical examination findings suggestive of ovarian torsion, gynecologic consultation and subsequent laparoscopy are critical, regardless of whether laboratory and radiologic studies yield normal results.
Approximately 1 in 1800 pregnancies is complicated by adnexal torsion, typically between the sixth and fourteenth weeks of gestation. This increased frequency in pregnant women is likely due to greater laxity of the tissues adjoining the ovaries and oviducts during pregnancy, as well as to enlargement of the ovary in early pregnancy secondary to the corpus luteum cyst.
Detorsion of the adnexa during pregnancy has not been found to compromise fetal well-being. However, if the corpus luteum cyst is removed during salpingo-oophorectomy, supplemental progesterone is indicated.
Outpatient care has no role in the treatment of ovarian torsion. Patients with either a suspected or confirmed diagnosis of ovarian torsion should be admitted and either operated on or observed by a gynecologist. Laparoscopy can be used for both confirmation of the diagnosis and treatment.
Ovarian torsion prognosis
With early diagnosis and appropriate treatment, the prognosis of ovarian torsion is excellent. However, most patients with ovarian torsion have a delayed diagnosis, often resulting in infarction and necrosis of the ovary. The ovarian salvage rate has been reported below 10% in adults but as high as 27% in a study among pediatric patients 19.
Although the loss of a single ovary is unlikely to result in significantly reduced fertility and no cases of death due to ovarian torsion have been reported, early diagnosis allows conservative laparoscopic treatment and reduction in complications. In a retrospective large study comparing pregnant patients with adnexal torsion to nonpregnant patients with adnexal torsion, the recurrence rate of torsion was 19.5% in pregnant women and 9.1% in nonpregnant women 20.
References- Ovarian Torsion. https://emedicine.medscape.com/article/2026938-overview
- Naffaa L, Deshmukh T, Tumu S, Johnson C, Boyd KP, Meyers AB. Imaging of Acute Pelvic Pain in Girls: Ovarian Torsion and Beyond☆. Curr Probl Diagn Radiol. 2017 Jul – Aug. 46 (4):317-329.
- Bider D, Mashiach S, Dulitzky M et-al. Clinical, surgical and pathologic findings of adnexal torsion in pregnant and nonpregnant women. Surg Gynecol Obstet. 1991;173 (5): 363-6
- Griffin D, Shiver SA. Unusual presentation of acute ovarian torsion in an adolescent. Am J Emerg Med. 2008 May. 26(4):520.e1-3.
- Huang TY, Lau BH, Lin LW, Wang TL, Chong CF, Chen CC. Ovarian cyst torsion in a toddler. Am J Emerg Med. 2009 Jun. 27(5):632.e1-3.
- Dähnert W. Radiology Review Manual. Hubsta Ltd. (2007) ISBN:0781766206
- Amirbekian S, Hooley RJ. Ultrasound Evaluation of Pelvic Pain. Radiol. Clin. North Am. 2014;52 (6): 1215-1235. doi:10.1016/j.rcl.2014.07.008
- Asfour V, Varma R, Menon P. Clinical risk factors for ovarian torsion. J Obstet Gynaecol. 2015. 35 (7):721-5
- Ashwal E, Hiersch L, Krissi H, Eitan R, Less S, Wiznitzer A, et al. Characteristics and Management of Ovarian Torsion in Premenarchal Compared With Postmenarchal Patients. Obstet Gynecol. 2015 Sep. 126 (3):514-20
- Ashwal E, Krissi H, Hiersch L, Less S, Eitan R, Peled Y. Presentation, Diagnosis, and Treatment of Ovarian Torsion in Premenarchal Girls. J Pediatr Adolesc Gynecol. 2015 Mar 28.
- Ganer Herman H, Shalev A, Ginat S, Kerner R, Keidar R, Bar J, et al. Clinical characteristics of adnexal torsion in premenarchal patients. Arch Gynecol Obstet. 2016 Mar. 293 (3):603-8.
- Koumoutsea EV, Gupta M, Hollingworth A, Gorry A. Ovarian Torsion in the Third Trimester of Pregnancy Leading to Iatrogenic Preterm Delivery. Case Rep Obstet Gynecol. 2016. 2016:8426270.
- Sonographic whirlpool sign in ovarian torsion. J Ultrasound Med. 2004 Dec;23(12):1643-9; quiz 1650-1. https://doi.org/10.7863/jum.2004.23.12.1643
- Duigenan S, Oliva E, Lee SI. Ovarian torsion: diagnostic features on CT and MRI with pathologic correlation. AJR Am J Roentgenol. 2012;198 (2): W122-31. doi:10.2214/AJR.10.7293
- Ovarian torsion. https://radiopaedia.org/cases/ovarian-torsion-6
- Chiou SY, Lev-toaff AS, Masuda E et-al. Adnexal torsion: new clinical and imaging observations by sonography, computed tomography, and magnetic resonance imaging. J Ultrasound Med. 2007;26 (10): 1289-301.
- Mashiach R, Melamed N, Gilad N, Ben-Shitrit G, Meizner I. Sonographic diagnosis of ovarian torsion: accuracy and predictive factors. J Ultrasound Med. 2011 Sep. 30(9):1205-10.
- Van Kerkhove F, Cannie M, Op de Beeck K, Timmerman D, Pienaar A, Smet MH, et al. Ovarian torsion in a premenarcheal girl: MRI findings. Abdom Imaging. 2007 May-Jun. 32(3):424-7
- Anders JF, Powell EC. Urgency of evaluation and outcome of acute ovarian torsion in pediatric patients. Arch Pediatr Adolesc Med. 2005 Jun. 159(6):532-5.
- Hasson J, Tsafrir Z, Azem F, Bar-On S, Almog B, Mashiach R, et al. Comparison of adnexal torsion between pregnant and nonpregnant women. Am J Obstet Gynecol. 2010 Jun. 202(6):536.e1-6.





{kind=link}