
Paresthesia
Paresthesia refers to abnormal sensation of the skin such as burning, tingling, prickling, chilling, burning or numbness sensation that is usually felt in your hands, arms, legs, or feet, but can also occur in other parts of your body 1. The sensation, which happens without warning, is usually painless and described as tingling or numbness, skin crawling, or itching.
Paresthesia can result from many different causes. It is often caused by nerve, spinal cord, or brain damage. It can be temporary (reversible) or permanent.
Most people have experienced temporary paresthesia — a feeling of “pins and needles” — at some time in their lives when they have sat with legs crossed for too long, or fallen asleep with an arm crooked under their head. It happens when sustained pressure is placed on a nerve 2. The feeling quickly goes away once the pressure is relieved.
While the nerve is squeezed, so are the arteries that feed blood to the nerve. The nerve can’t work for long without a steady supply of oxygen and glucose. Anything that gets in the way of the nerve’s ability to send signals or with its blood supply causes a limb to “fall asleep.” For example, people in wheelchairs who sit for long periods of time are more likely to have nerve “traffic jams.”
When the blockage is removed, the nerve cells start waking up as they start getting impulses again. You may start to have an uncomfortable pins-and-needles feeling. The nervous system tends to become hyperactive as nerves regain normal function.
The nerve structures, as they recover, tend to be irritable for a period of time. That’s because the nerves are firing spontaneously. Most of the time, the pins and needles feeling is a good sign. It’s a short-term phase that means nerves are coming back to life.
Nerve entrapment syndromes, such as carpal tunnel syndrome, can cause paresthesia sometimes accompanied by pain but are usually very peripheral and obvious.
Paresthesia can be felt in people who have an implanted spinal cord or peripheral nerve stimulator.
Chronic paresthesia is often a symptom of an underlying neurological disease or traumatic nerve damage. Paresthesia can be caused by disorders affecting the central nervous system (brain and spinal cord), such as stroke and transient ischemic attacks (mini-strokes), multiple sclerosis, transverse myelitis, connective tissue diseases, sarcoidosis, some drugs (e.g., some local anesthetic agents can be neurotoxic), hypervitaminosis-D and encephalitis 2. A brain or spinal cord tumor or vascular lesion pressed up against the brain or spinal cord can also cause paresthesia. Diagnostic evaluation is based on determining the underlying condition causing the paresthetic sensations. An individual’s medical history, physical examination, and laboratory tests are essential for the diagnosis. Physicians may order additional tests depending on the suspected cause of the paresthesia.
Most often, pins and needles is just an odd but harmless feeling that we have from time to time. But it can also be more serious. In some cases, a nerve may be seriously injured, perhaps in an accident. Then the nerve may get stuck in a pins-and-needles stage. And you may have constant pain. A good example is carpal tunnel syndrome or diabetic neuropathy. In these instances, the pins and needles feeling can be a danger signal.
Paresthesia that happens with other symptoms may also mean there is an underlying condition. People who have this happen very often may have an underlying problem with their nerves. If these symptoms last for a long time, or are linked to weakness, talk with your healthcare provider. If paresthesia occurs suddenly and is linked to slurred speech, facial drooping, or weakness, get medical care right away.
Red flags
- Paresthesia onset after trauma, surgery or systemic infection
- Multiple areas involved or progressive symptoms
- Additional behavioral or memory changes
- Fever or other systemic upset
- Disturbances of autonomous nervous system or objective muscular weakness
- Patient is at high risk because of age, existing chronic conditions or lifestyle factors
The nervous system
The nervous system has two major anatomical subdivisions:
- The central nervous system (CNS) consists of the brain and spinal cord, which are enclosed and protected by the cranium and vertebral column. The central nervous system is discussed further in the other posts: Human brain and Spinal cord.
- The peripheral nervous system (PNS) consists of all the rest; it is composed of nerves and ganglia. The peripheral nervous system is the network of nerves that lie outside the central nervous system (the brain and spinal cord). A nerve is a bundle of nerve fibers (axons) wrapped in fibrous connective tissue. Nerves emerge from the central nervous system (CNS) through foramina of the skull and vertebral column and carry signals to and from other organs of the body. A ganglion (plural, ganglia) is a knotlike swelling in a nerve where the cell bodies of peripheral neurons are concentrated.
Figure 1. Nervous system and its parts
Peripheral nervous system
The peripheral nervous system includes different types of nerves with their own specific functions, including:
- sensory nerves – responsible for transmitting sensations, such as pain and touch
- motor nerves – responsible for controlling muscles
- autonomic nerves – responsible for regulating automatic functions of the body, such as blood pressure and bladder function
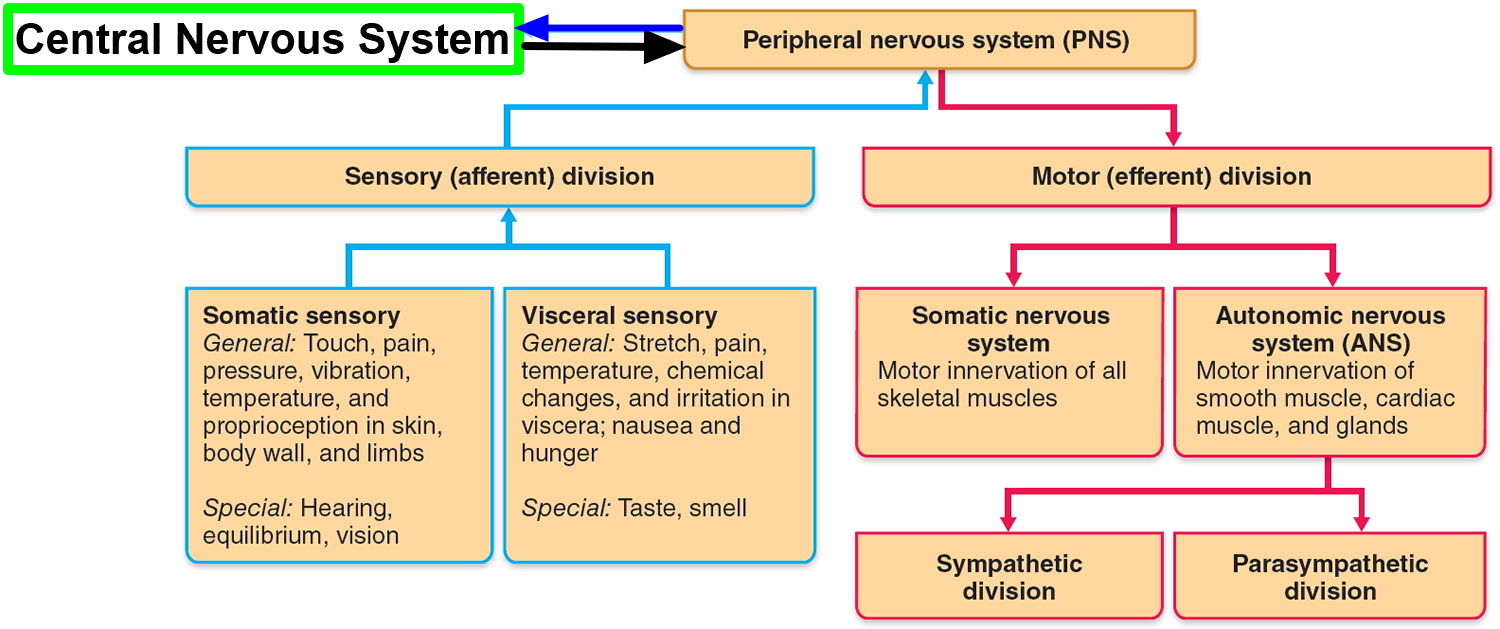
The peripheral nervous system is functionally divided into sensory and motor divisions, and each of these is further divided into somatic and visceral subdivisions.
The sensory (afferent) division carries signals from various receptors (sense organs and simple sensory nerve endings) to the central nervous system (CNS). This pathway informs the central nervous system (CNS) of stimuli within and around the body.
- The somatic sensory division carries signals from receptors in the skin, muscles, bones, and joints.
- The visceral sensory division carries signals mainly from the viscera of the thoracic and abdominal cavities, such as the heart, lungs, stomach, and urinary bladder.
The motor (efferent) division carries signals from the CNS (the brain and the spinal cord) mainly to gland and muscle cells that carry out the body’s responses. Cells and organs that respond to these signals are called effectors.
- The somatic motor division carries signals to the skeletal muscles. This produces voluntary muscle contractions as well as involuntary somatic reflexes.
- The visceral motor division (autonomic nervous system) carries signals to glands, cardiac muscle, and smooth muscle. We usually have no voluntary control over these effectors, and the autonomic nervous system operates at an unconscious level. The responses of the autonomic nervous system and its effectors are visceral reflexes. The autonomic nervous system has two further divisions:
- The sympathetic division tends to arouse the body for action—for example, by accelerating the heartbeat and increasing respiratory airflow—but it inhibits digestion.
- The parasympathetic division tends to have a calming effect—slowing the heartbeat, for example—but it stimulates digestion.
Figure 2. Functional classes of neurons
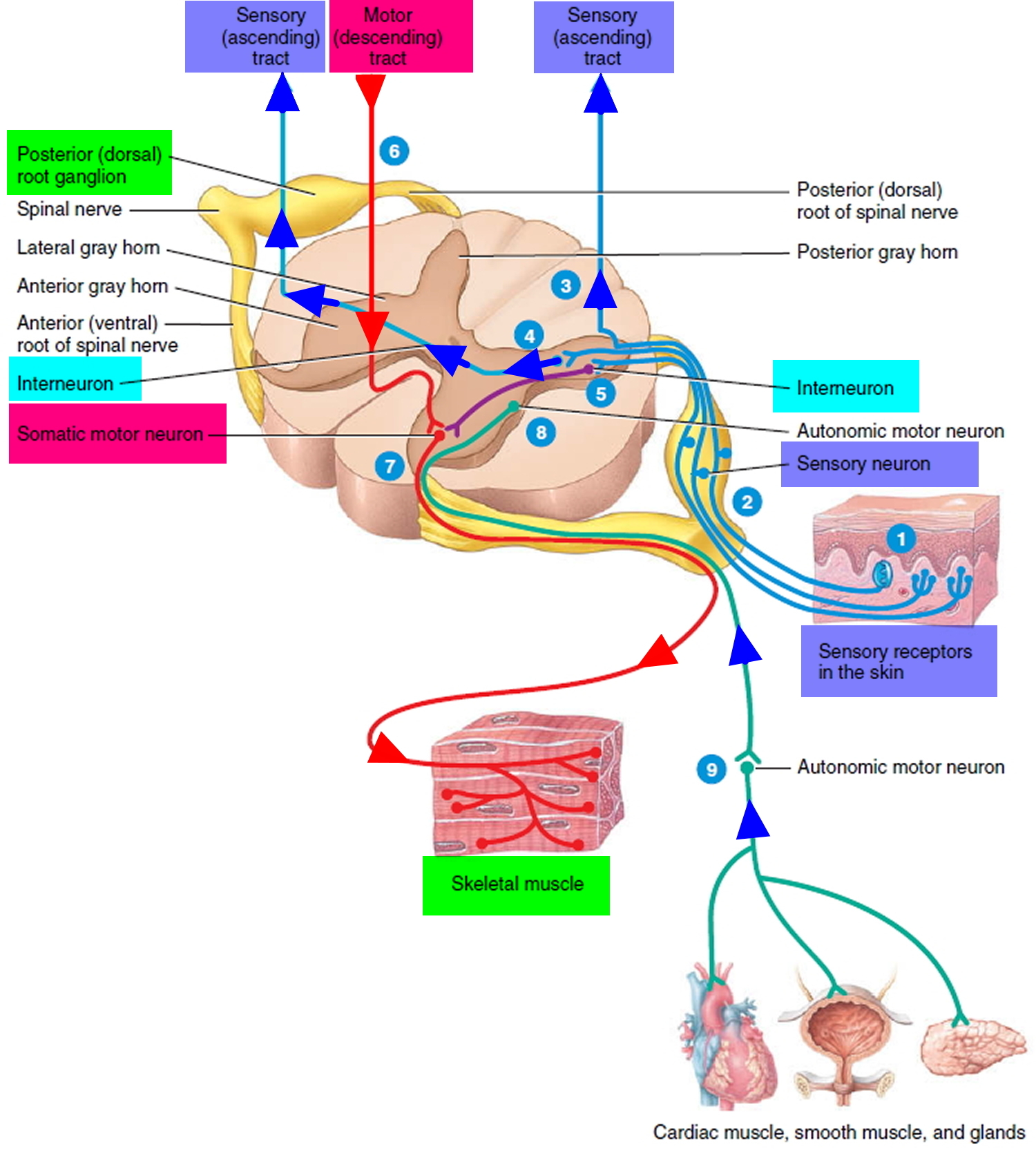
Figure 3. General structure of a neuron
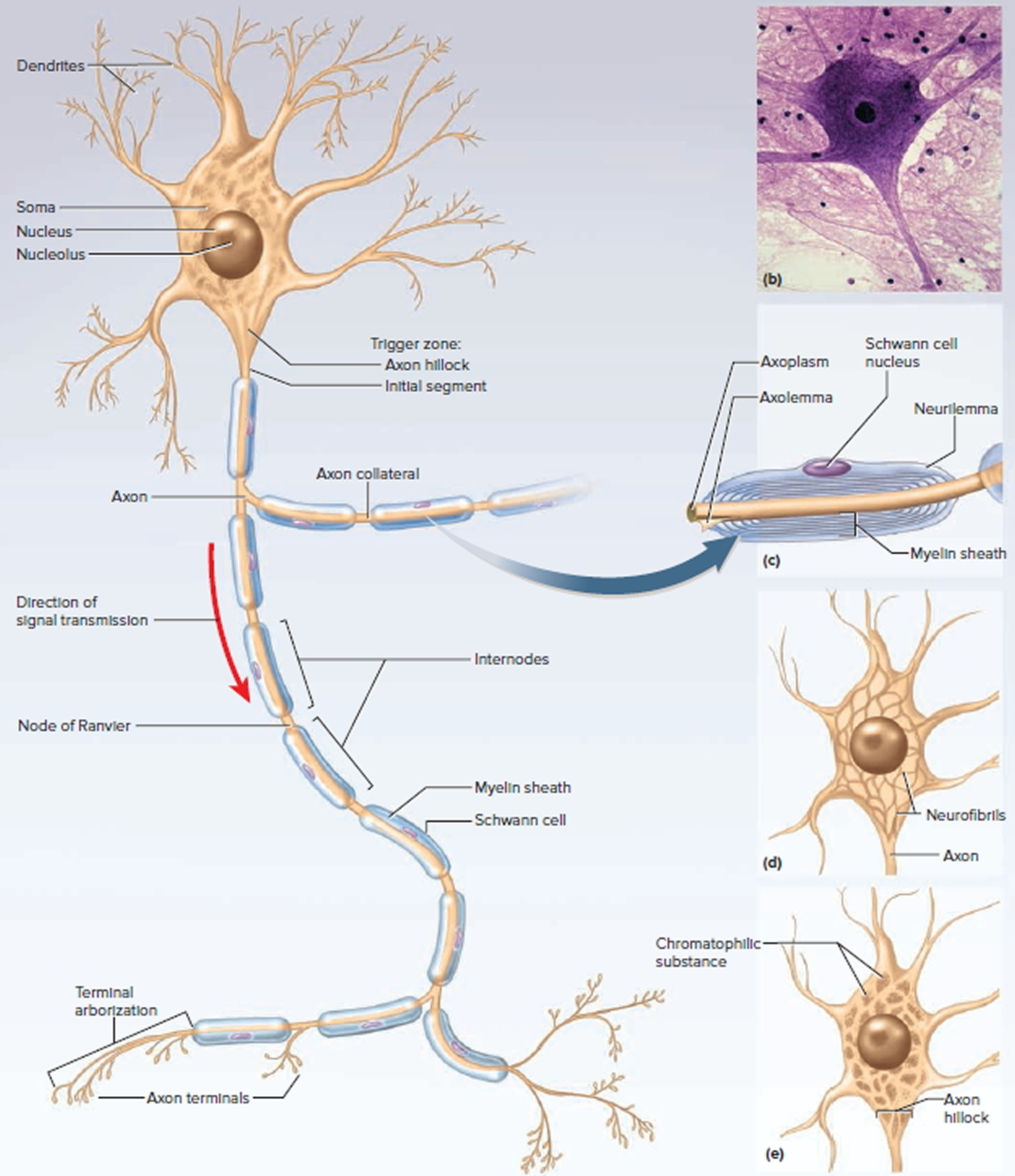
Figure 4. Peripheral nervous system
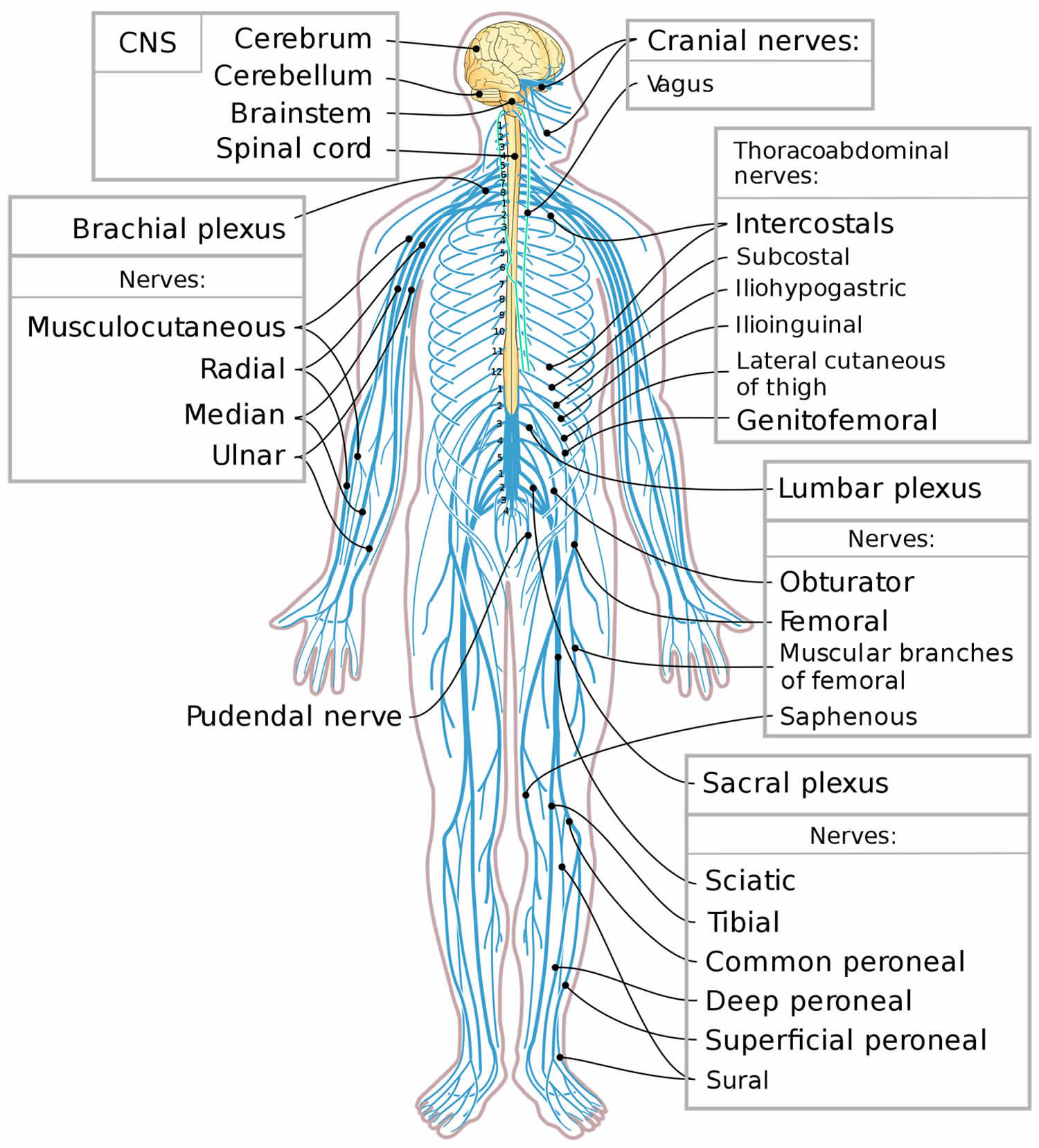
Figure 5. Dermatome levels
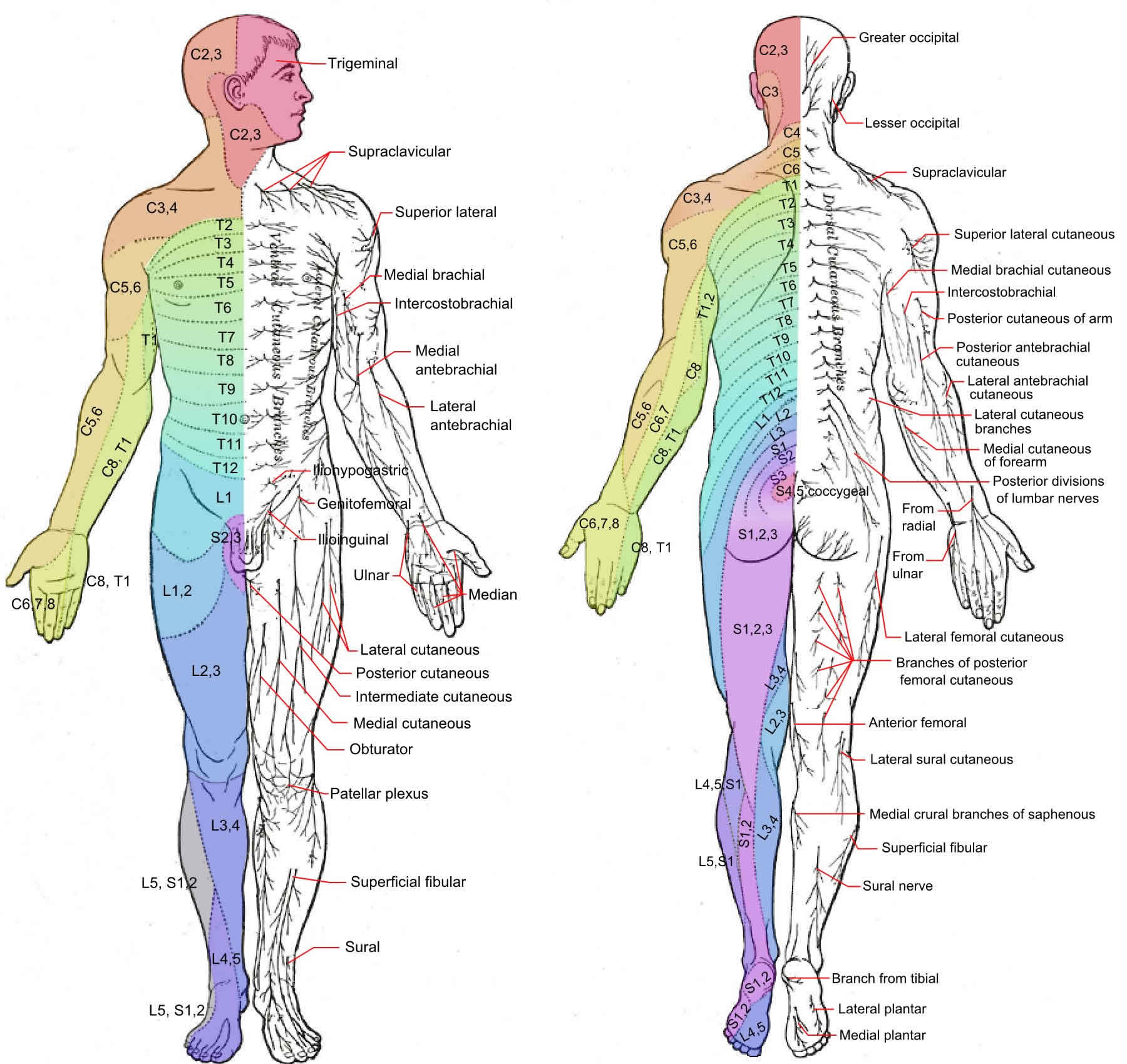
Footnote: The letter-number combinations show the relationship between each area and its corresponding sensory nerve. The vertebrae are classified as C for cervical, T for thoracic, L for lumbar, and S for sacral. The trigeminal nerve is the fifth cranial nerve, represented by V.
Paresthesia causes
There are many potential causes of paresthesia. These can basically be divided into central and peripheral. Paresthesias can be caused by a dysfunction or abnormality affecting any level of the somatosensory pathway. However, the most common causes affect peripheral sensory nerves. The peripheral nervous system includes nerves in your face, arms, legs, torso, and some cranial nerves. All of your nerves not located in your central nervous system (brain and spinal cord) are peripheral nerves. Peripheral neuropathy is a general term indicating disturbances in the peripheral nerves. It can affect one side of the body (unilateral) or both (bilateral).
Paresthesia can be caused by disorders affecting the central nervous system (encephalitis, multiple sclerosis, stroke, transverse myelitis, tumors on the brain or spinal cord) or any of the peripheral nerves (carpel tunnel syndrome, atherosclerosis, diabetic neuropathy).
Possible causes of paresthesia:
- Simple, temporary local mechanical pressure (especially in elbows, shoulders, lower legs, cervical spine)
- Chronic nerve compression syndromes such as carpal tunnel syndrome
- Progressing arthritis, fibromyalgia, vertebral collapse or disc herniation, cervical rib, carcinomatosis, complex regional pain syndrome
- Electrolyte disturbance (hyperventilation, dehydration, hyper- or hypoglycaemia)
- Side-effects of medication such as benzodiazepines, selective serotonin reuptake inhibitor (SSRI) withdrawal
- Chemotherapy
- Metal poisoning
- MS or motor neurone disease
- Brain or spinal compression processes, including abscesses, trauma, tumours or metastases
- Sensory epilepsy or psychiatric conditions, such as somatoform disorders
- Polyneuropathy of diabetes
- Hypothyroidism or other metabolic conditions
- Barotrauma
- Frostbite
- Autoimmune conditions
- Malnutrition or vitamin deficiency
- Infections, for example, herpes simplex, HIV, varicella zoster, Lyme disease, Guillain-Barré syndrome or Bell’s palsy
- Acute limb ischemia, thrombosis, chronic peripheral vascular disease
- Transient ischemic attack (TIA, Mini-Stroke)
- Migraines
Short-term paresthesia is most often caused by temporary pressure or other mechanical impact on nerves, but chronic paresthesia is more likely to indicate a problem with the functioning of the anatomical neurons because of inflammation or poor circulation.
This may result directly from a problem of blood flow in the area (for example, constrictions or obstructions, impact of heat or cold, infection-induced or autoimmune conditions) or from metabolic disturbances, such as electrolytes or blood glucose.
Peripheral causes
Disorders affecting the peripheral elements of the nervous system are the more common causes of numbness and tingling. They also tend to be associated with more localized symptoms and sharper borders between normal and abnormal sensation.
Generalized polyneuropathy as well as more focal entrapment neuropathies are quite common in neurologic practice. The polyneuropathies tend to produce distal and symmetrical sensory loss starting in the feet. Only much later does it tend to affect the fingers. Differential diagnosis for polyneuropathy is discussed in a later chapter though a table of possible causes is provided here.
The peripheral entrapment neuropathies are also quite common. The distribution of symptoms is the principal mode of recognition of the specific nerve injury, and the specific positions and activities that exacerbate symptoms are important clues to mechanism. Pain is variable and is not particularly helpful in diagnosis. Tinel sign may give strong evidence of the precise location of the nerve damage though provocative measures (such as Phalen maneuver for carpal tunnel syndrome) may be more specific.
Tinel sign is the generation of paresthesias in the distribution of a nerve following a light tap with a reflex hammer. This suggests an excessive excitability of nerve due to some focal damage. It is quite sensitive, but not very specific for conditions such as entrapment neuropathy. It is very useful for localizing a lesion.
Radiculopathies tend to produce relatively localized numbness or tingling in the distal extremities. This is because each dermatome is completely overlapped by adjacent dermatomes. There are only relatively small “autonomous zones” where only a single nerve root supplies the region. Therefore, “numbness” tends to be found only in small areas of the distal limbs. Of course there may be associated signs of damage to motor nerve fibers as well.
Brachial plexus lesions affect broader areas of the limb, overlapping the distributions of individual nerves or roots. With rare exception, they have motor signs and symptoms in addition to the sensory loss.
Risk factors for peripheral neuropathies
Peripheral neuropathy may be either inherited or acquired.
Peripheral neuropathy risk factors include:
- Diabetes mellitus, especially if your sugar levels are poorly controlled
- Alcohol
- Nutritional deficiencies (vitamin B1, B3, B6, B12 and vitamin E)
- Toxins (carbon disulfide, acrylamide)
- Endocrine causes (diabetes, thyroid disease)
- Metabolic causes (renal failure)
- Liver or thyroid disorders
- Infections (HIV, Lyme disease, Leprosy, Epstein-Barr virus, hepatitis C and shingles)
- Connective tissue disease (scleroderma, SLE, sarcoidosis)
- Immune disorders (Guillain-Barre syndrome, chronic inflammatory demyelinating neuropathy)
- Cancer
- Medications/Drugs
- Repetitive motion, such as those performed for certain jobs
- Family history of neuropathy
- Inherited conditions (Charcot-Marie-Tooth disease)
Central causes
There are many conditions affecting the central nervous system that can produce “numbness.” Spinal cord disease often produces bilateral symptoms with a sensory level, below which the sensation is lost (due to tract damage). The causes of spinal cord damage generally are either extrinsic compressions (extramedullary) or conditions that intrinsically damage the spinal cord (intramedullary). The general differential diagnosis of myelopathy is shown in this table.
Above the foramen magnum, conditions that can cause “numbness” range from cerebral vascular disease through tumors, demyelinating lesions (such as multiple sclerosis) and infectious lesions. Typically, the symptoms are unilateral, specifically affecting the contralateral side of the body. Transient phenomena, such as migraine (where symptoms spread over the body over a period of minutes) and transient ischemic attacks should be considered. To a large extent, the tempo and timing of onset of symptoms, as well as their distribution are critical factors in guiding the investigation.
Paresthesia diagnosis
Medical History
The experience of paresthesia is subjective and can be difficult to describe. Patients may use terms such as ‘trickling’, ‘pins and needles’, ‘like an electrical current’ or descriptions such as pressure, tightness, heaviness or numbness. If the patient reports pain, neuralgia would be readily considered.
Details about the onset, timeline and any variability of the symptoms are essential to help understand progression or regression, any patterns (or lack of) as well as the emotional and functional impact.
An occupational history and details of physical activities may reveal a musculoskeletal strain. A recent travel history is useful (long-haul flights or long car journeys, possible infection risks). The patient should also be asked about lifestyle factors that could indicate cancers, acute or chronic infections, metabolic diseases or alcoholism, for example.
Do not forget to check if the patient is taking medications, if these have been recently started or changed, and if they have attempted to self-treat the paresthesia.
Physical examination
The examination should be focused on detecting any areas of pins and needles or paresthesia and the borders of this distribution. The main interest here is an attempt to define a pattern suggestive of a particular location of damage to the nervous system. It is good to have a reference available showing the approximate sensory distribution of peripheral nerves as well as nerve roots while examining patients. Broad or vague, sensory complaints with inconsistent distribution and borders are more likely to result from distorted sensory perceptions that often occur in patients with psychological distress or diffuse, chronic pain. In many such cases, you may be able to confirm of the nature of the paresthesia by magnifying or provoking the distal symptoms with maneuvers that do not directly impact the nervous system. For example, the patient complaining of paresthesias resulting from a chronic pain problem (such as fibromyalgia), will usually have “numbness” or paresthesias that are magnified by compression of painful sites in muscles, even when these maneuvers completely avoid pressing on nerves or stretching them. This finding requires evaluation of the chronic pain problem and not the “numbness.”
Sensory changes that follow artificial boundaries such as the hairline or jawline are also suggestive of hysterical sensory loss. Other findings, on examination that are suggestive of hysterical sensory loss include vibratory sensation loss across the midline of the skull, pelvis or sternum. This is because vibration of these midline osseous structures is transmitted bilaterally.
The examination may be useful in demonstrating whether the sensory loss is to all modalities, or whether there is some selectivity. For example, temperature and pin sensation are transmitted along small-diameter nerve fibers and then up the spinothalamic tract. The ability to detect vibration is transmitted via large-diameter, heavily myelinated nerve fibers and then the dorsal column-medial lemniscus tracts. Selective loss of sensation can aid in localization of damage and in understanding its mechanism.
On occasion, reflexes and other responses to simulation can be used to objectify what is fundamentally a subjective exam. The corneal reflex is a good test of trigeminal (ophthalmic) sensory loss. The reaction of the patient to unexpected stimulation with a sharp object can often confirm whether sensations are lost.
Certain laboratory studies may be helpful. Peripheral conduction along sensory pathways can be quantified with nerve conduction studies. This is particularly helpful for the evaluation of trauma or compressive neuropathies. Somatosensory evoked potentials can examine the entire sensory pathway for large diameter sensory fiber input all the way from the periphery to the cerebral cortex and often shows abnormalities in patients with disease of the dorsal column-medial lemniscus tracts of the central nervous system (such as with multiple sclerosis). However, despite these laboratory aids, the evaluation of the sensory system largely depends on patient cooperation and is fundamentally subjective.
Once the history and exam are completed, and once you are convinced that some sensory component of the nervous system is damaged, various factors need to be weighed to reach a conclusion about the cause.
Distribution
The pattern of numbness may help define its origin. Numbness confined to a specific nerve or nerve root distribution (see the maps of dermatomes and peripheral nerve sensory innervation) lead to consideration of peripheral nerve or nerve root damage. Loss of sensation on one side of the body is more likely to result from central nervous system damage and if the sensory loss also involves the same side of the face, you can be sure that the cause is located above the level of the pons.
When there is a clear sensory level (a line on the body, below which sensations are lost), a spinal cord lesion must be suspected. Loss of sensation over the upper limbs or upper part of the trunk bilaterally, with preservation over the lower limbs and buttocks, suggests an expanding intraspinal mass. This so-called “sacral sparing” is seen with intraspinal tumors or syrinxes. Numbness over one side of the face, while being a relatively common presentation of psychiatric disease, can also be caused by damage to the lateral part of the brain stem, or upper spinal cord (spinal tract of the trigeminal). Lateral brain stem damage can also produce a picture of sensory decrease on one side of the head and on the opposite side of the body.
Numbness over the face is a relatively common hysterical presentation, reflecting psychiatric disease. This is especially true with perioral paresthesias. Often, the symptoms in these cases do not follow known anatomical nerve distributions and may appear at times of particular stress.
The distribution of symptoms may be helpful in another way. A progression of sensory complaints, particularly tingling, from one region of the body to adjacent regions (which has been described as a “march” of symptoms – paresthesias that progress from one area of the body to adjacent regions over time measured in minutes) is common in migraine and may be seen with focal seizures affecting the sensory cortex. Such a march of symptoms may be very helpful and distinguishing transient sensory changes due to these conditions from transient sensory loss due to stroke or transient ischemic attack.
Precipitants
The identification of clear precipitants for symptoms may be the best indicator of cause and often suggests a particular location of injury as well as a mechanism. This may be very clear, such as with trauma, or may be more subtle, due to the effect of activities or intercurrent illness. When symptoms are intermittent, the specific conditions under which symptoms are present may be the most important factor in diagnosis. For example, the production of distal paresthesias by neck movement or by particular neck positions suggests compressive lesions in the cervical region (nerve roots or spinal cord). Being awakened from sleep by symptoms, usually with the limb in an unusual position, suggests either local compression of a nerve or compression of the circulation to the limb. Common examples include median nerve compressive neuropathy at the wrist or ulnar nerve compression at the elbow. Also, the axillary artery can be occluded in the “thoracic outlet” by certain limb positions, resulting in ischemia of the entire limb.
Associated symptoms
The presence of associated symptoms may be also quite helpful in evaluation. For example, if the symptoms precede or accompany a migraine headache, they are likely to be part of an aura. On the other hand, if they are associated with the situation that provokes extreme anxiety, and particularly if the symptoms are perioral or in the fingers, they are quite likely to be associated with a panic attack and hyperventilation. Of course, if there are other signs or symptoms that would lead to consideration of such conditions as stroke or multiple sclerosis exacerbation, diagnosis may be facilitated.
Clinical setting
Of course, diagnosis of the cause of numbness must take place in the context of the complete presentation. For example, other associated neurologic symptoms may lead to diagnosis. Additionally, a predilection of a particular patient to certain neurologic conditions based on their age, sex or other factors, must be considered. For example, recent localized, but persistent tingling in an elderly patient should raise the suspicion of early zoster. Any tingling in one limb should be intensively investigated for peripheral entrapment or thoracic outlet syndrome. The presence of vascular risk factors, such as age, hypertension, diabetes mellitus and dyslipidemia, increase the likelihood of stroke as a cause.
Investigations
Consider baseline bloods to check for signs of inflammation, calcium and ESR, deficiencies in anaemia, vitamin B12, thiamin or ferritin, or metabolic dysfunction (liver, renal, glucose, thyroid). Nerve conduction studies may be indicated and useful, depending on your local facilities. In potential at-risk groups, such as smokers, consider a chest X-ray, even in the absence of other symptoms and normal chest auscultation. Other investigations, including spinal MRI or CT head, may be indicated, but discuss with a radiologist or neurologist first, if possible.
Confirming if you have a peripheral neuropathy
Some people may need to see a neurologist (a specialist in conditions affecting the nervous system) in hospital for further tests such as:
- a nerve conduction test – where small metal wires called electrodes are placed on your skin which release tiny electric shocks that stimulate your nerves; the speed and strength of the nerve signal is measured
- electromyography (EMG) – where a small needle is inserted through your skin into your muscle and used to measure the electrical activity of your muscles
Nerve conduction test and electromyography are usually carried out at the same time.
Occasionally, a nerve biopsy may be carried out as part of your diagnosis. This is a minor surgical procedure where a small sample of a peripheral nerve is removed from near your ankle so it can be examined under a microscope.
It’s then checked for changes that could be a sign of certain types of peripheral neuropathy. However, nerve biopsies are rarely needed.
You may also need a scan and blood tests to look for any underlying cause of your peripheral neuropathy, such as:
- Chest x-ray
- Computerised tomography (CT) scan
- Magnetic resonance imaging (MRI) scan
- Genetic testing is available for the evaluation of specific types of hereditary sensorimotor neuropathies.
- Blood tests measuring haemoglobin, inflammatory markers, vitamin levels, blood sugar and thyroid function, infection markers and antibody levels
Urinalysis
Paresthesia treatment
The appropriate treatment for paresthesia depends on accurate diagnosis of the underlying cause and treating the underlying cause, followed by symptomatic treatment.
In general, adopting healthy habits, such as maintaining optimal weight, avoiding exposure to toxins, following a physiotherapist supervised exercise program, eating a balanced diet, correcting vitamin deficiencies, and limiting or avoiding alcohol consumption can reduce the physical and emotional effects of peripheral neuropathy.
Quitting smoking is particularly important because smoking constricts the blood vessels that supply nutrients to the peripheral nerves and can worsen neuropathic symptoms.
Treatment may be more successful for certain underlying causes. For example, ensuring diabetes is well controlled may help improve neuropathy or at least stop it getting worse. Strict control of blood glucose levels has been shown to reduce neuropathic symptoms and help people with diabetic neuropathy avoid further nerve damage. Inflammatory and autoimmune conditions leading to neuropathy can be controlled with steroids or immunosupressive medications.
If you have neuropathies caused by pressure on nerves, such as pressure from tumors, you might need surgery to reduce the pressure.
There are many different possible causes of peripheral neuropathy, some of which can be treated in different ways. For example:
- diabetes can sometimes be controlled by lifestyle changes, such as stopping smoking, cutting down on alcohol, maintaining a healthy weight and exercising regularly
- vitamin B12 deficiency can be treated with B12 injections or tablets
- peripheral neuropathy caused by a medication you’re taking may improve if the medication is stopped
Some less common types of peripheral neuropathy may be treated with medication, such as:
- Corticosteroids – powerful anti-inflammatory medication
- Immunosuppressants – medications that reduce the activity of the immune system
- Plasma exchange and intravenous immune globulin. These procedures, which help suppress immune system activity, might benefit people with certain inflammatory conditions. Plasma exchange involves removing your blood, then removing antibodies and other proteins from the blood and returning the blood to your body. In immune globulin therapy, you receive high levels of proteins that work as antibodies (immunoglobulins).
However, the underlying cause may not always be treatable.
Relieving nerve pain
You may also require medication to treat any nerve pain (neuropathic pain) you’re experiencing.
Unlike most other types of pain, neuropathic pain doesn’t usually get better with common painkillers, such as paracetamol and ibuprofen.
For more-severe symptoms, your doctor might prescribe painkillers. Medications containing opioids, such as tramadol (Conzip, Ultram) or oxycodone (Oxycontin, Roxicodone, others), can lead to dependence and addiction, so these drugs generally are prescribed only when other treatments fail.
These should usually be started at the minimum dose, with the dose gradually increased until you notice an effect, because the ideal dose for each person is unpredictable. Higher doses may be better at managing the pain, but are also more likely to cause side effects.
The most common side effects are tiredness, dizziness or feeling “drunk”. If you get these, it may be necessary to reduce your dose. Don’t drive or operate machinery if you experience drowsiness or blurred vision. You also may become more sensitive to the effects of alcohol.
The side effects should improve after a week or two as your body gets used to the medication. However, if your side effects continue, tell your GP as it may be possible to change to a different medication that suits you better.
Even if the first medication tried doesn’t help, others may.
Peripheral neuropathy medications
Many of these medications may also be used for treating other conditions, such as depression, epilepsy, anxiety or headaches. If you’re given an antidepressant, this may treat pain even if you’re not depressed. This doesn’t mean your doctor suspects you’re depressed.
Medications used to relieve peripheral neuropathy pain include:
- Duloxetine – also used for treatment of bladder problems and depression
- Pregabalin and gabapentin – also used to treat epilepsy, headaches or anxiety. Side effects can include drowsiness and dizziness.
- Antidepressants. Certain tricyclic antidepressants, such as amitriptyline, doxepin and nortriptyline (Pamelor), have been found to help relieve pain by interfering with chemical processes in your brain and spinal cord that cause you to feel pain. Amitriptyline – also used for treatment of headaches and depression. The serotonin and norepinephrine reuptake inhibitor duloxetine (Cymbalta) and the extended-release antidepressant venlafaxine (Effexor XR) also might ease the pain of peripheral neuropathy caused by diabetes. Side effects may include dry mouth, nausea, drowsiness, dizziness, decreased appetite and constipation.
There are also some additional medications that can be used to relieve pain in a specific area of the body or to relieve particularly severe pain for short periods. These are described below.
Capsaicin cream
If your pain is confined to a particular area of your body and you can’t, or would prefer not to, take the medications above, you may benefit from using capsaicin cream.
Capsaicin is the substance that makes chilli peppers hot and is thought to work in neuropathic pain by stopping the nerves sending pain messages to the brain.
A pea-sized amount of capsaicin cream is rubbed on the painful area of skin three or four times a day.
Side effects of capsaicin cream can include skin irritation and a burning sensation in the treated area when you first start treatment.
Don’t use capsaicin cream on broken or inflamed skin and always wash your hands after applying it.
Tramadol
Tramadol is a powerful painkiller related to morphine that can be used to treat neuropathic pain that doesn’t respond to other treatments your GP can prescribe.
Like all opioids, tramadol can be addictive if it’s taken for a long time. It will usually only be prescribed for a short time. Tramadol can be useful to take at times when your pain is worse.
Common side effects of tramadol include:
- feeling sick or vomiting
- dizziness
- constipation
Treating other symptoms
In addition to treating pain, you may also require treatment to help you manage other symptoms you’re experiencing as a result of peripheral neuropathy.
For example, if you have muscle weakness, you may need physiotherapy to learn exercises to improve your muscle strength. You may also need to wear splints to support weak ankles or use walking aids to help you get around.
Other problems associated with peripheral neuropathy may be treatable with medication, such as:
- erectile dysfunction
- constipation
- the slow movement of food through your stomach (gastroparesis)
In some cases, you may need more invasive treatment, such as botulinum toxin injections for hyperhidrosis or urinary catheterisation if you have problems emptying your bladder.
Peripheral neuropathy natural treatment
As peripheral neuropathy can be a very painful and troublesome condition that may only partly be relieved by medication, some people may be tempted to try other treatments, such as:
- Acupuncture. Inserting thin needles into various points on your body might reduce peripheral neuropathy symptoms. You might need multiple sessions before you notice improvement. Acupuncture is generally considered safe when performed by a certified practitioner using sterile needles.
- Transcutaneous electrical nerve stimulation (TENS). Electrodes placed on the skin deliver a gentle electric current at varying frequencies. TENS should be applied for 30 minutes daily for about a month.
- Herbal medicine. Certain herbs, such as evening primrose oil, might help reduce neuropathy pain in people with diabetes. Some herbs interact with medications, so discuss herbs you’re considering with your doctor.
- Physical therapy. If you have muscle weakness, physical therapy can help improve your movements. You may also need hand or foot braces, a cane, a walker, or a wheelchair.
- Benfotiamine (a form of vitamin B1) supplements
- Alpha-lipoic acid (an antioxidant) supplements. This has been used as a treatment for peripheral neuropathy in Europe for years. Discuss using alpha-lipoic acid with your doctor because it can affect blood sugar levels. Other side effects can include stomach upset and skin rash.
- Amino acids. Amino acids, such as acetyl-L-carnitine, might benefit people who have undergone chemotherapy and people with diabetes. Side effects might include nausea and vomiting.
However, while some people may find these helpful, the evidence for them isn’t always clear. It’s advisable to speak to your doctor before trying these treatments in case they could interfere with your ongoing treatment.
Home remedies
To help you manage peripheral neuropathy:
- Take care of your feet, especially if you have diabetes. Check daily for blisters, cuts or calluses. Wear soft, loose cotton socks and padded shoes. You can use a semicircular hoop, which is available in medical supply stores, to keep bedcovers off hot or sensitive feet.
- Exercise. Regular exercise, such as walking three times a week, can reduce neuropathy pain, improve muscle strength and help control blood sugar levels. Gentle routines such as yoga and tai chi might also help.
- Quit smoking. Cigarette smoking can affect circulation, increasing the risk of foot problems and other neuropathy complications.
- Eat healthy meals. Good nutrition is especially important to ensure that you get essential vitamins and minerals. Include fruits, vegetables, whole grains and lean protein in your diet.
- Avoid excessive alcohol. Alcohol can worsen peripheral neuropathy.
- Monitor your blood glucose levels. If you have diabetes, this will help keep your blood glucose under control and might help improve your neuropathy.
Paresthesia prognosis
The prognosis for those with paresthesia depends on the severity of the sensations and the associated disorders.
References




{kind=link}