Paroxysmal nocturnal hemoglobinuria
Paroxysmal nocturnal hemoglobinuria (PNH) also called Marchiafava-Micheli Syndrome or paroxysmal hemoglobinuria, is a rare acquired blood disorder that causes red blood cells to break apart prematurely and impaired production of blood cells 1. Doctors call this breaking apart of red blood cells “hemolysis.” Paroxysmal nocturnal hemoglobinuria (PNH) happens because the surface of a person’s blood cells are missing a protein that protects them from the body’s immune system. Hemolysis happens when the complement system, a part of your body’s immune system, becomes more active and attacks your PNH red blood cells. The complement is made of small proteins that attack foreign objects, such as viruses and bacteria. Because PNH cells are abnormal, they are seen as foreign and attacked, causing them to burst.
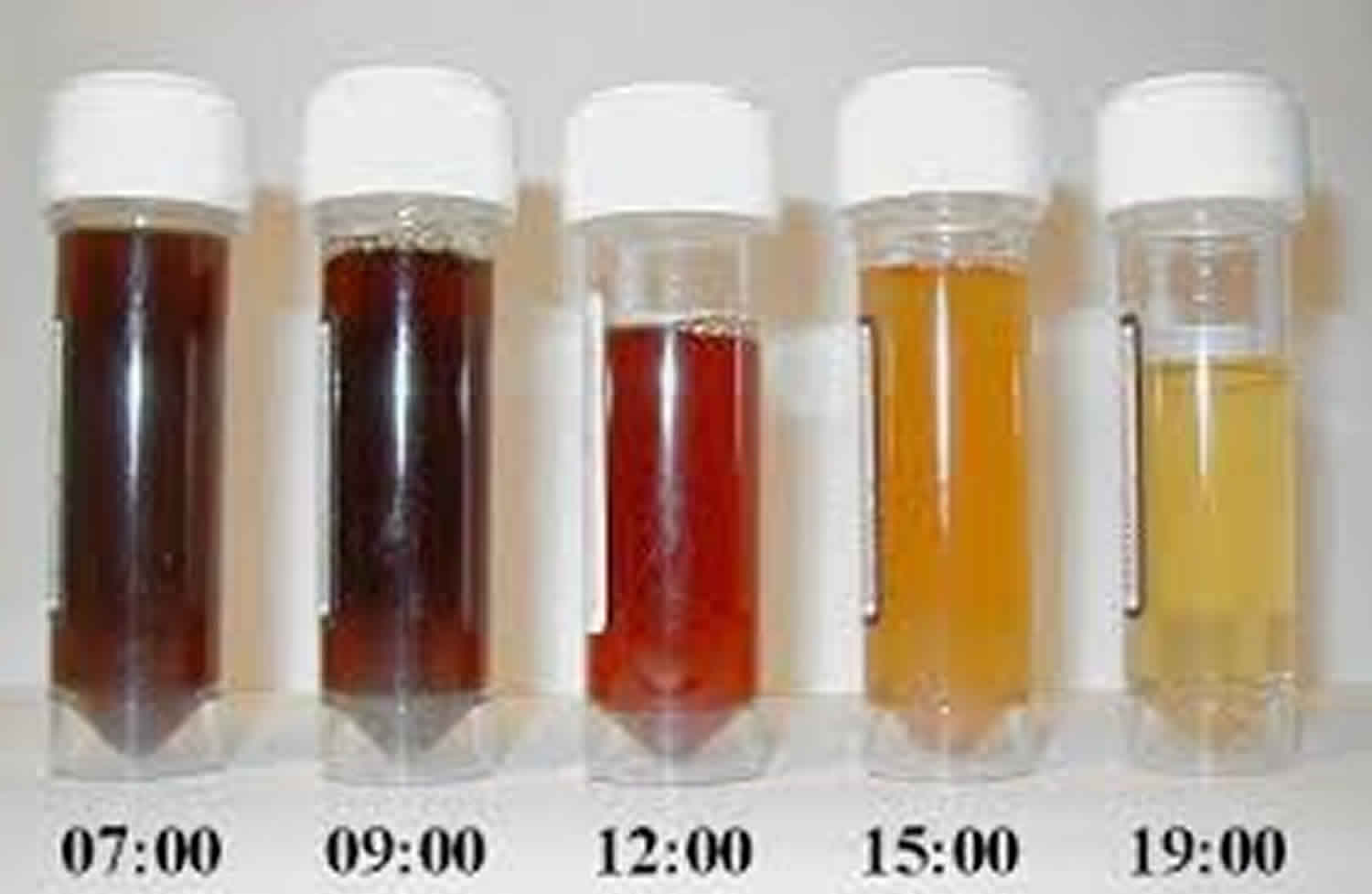
When red blood cells break apart, the hemoglobin inside is released. Hemoglobin is the red part of red blood cells that carries oxygen around the body. The release of hemoglobin causes many of the PNH symptoms. Paroxysmal means “sudden and irregular”. The term “nocturnal” refers to the belief that hemolysis is triggered by acidosis during sleep. However, this observation was later disproved. In individuals with paroxysmal nocturnal hemoglobinuria, hemolysis has been shown to occur throughout the day, but the urine concentrated overnight produces the dramatic change in color 2. Paroxysmal nocturnal hemoglobinuria (PNH) is most noticeable in the morning, upon passing urine that has accumulated in the bladder during the night 1. So, “paroxysmal nocturnal hemoglobinuria” means sudden, irregular episodes of passing dark colored urine, especially at night or in the early morning. It is important to note this can be a bit misleading, because many people with PNH do not have dark urine.
Paroxysmal nocturnal hemoglobinuria affects red blood cells (erythrocytes), which carry oxygen; white blood cells (leukocytes), which protect the body from infection; and platelets (thrombocytes), which are involved in blood clotting. This results in a deficiency of various types of blood cells and can cause signs and symptoms such as fatigue, weakness, abnormally pale skin (pallor), shortness of breath, and an increased heart rate. People with PNH may also be prone to infections and abnormal blood clotting (thrombosis) or hemorrhage, and are at increased risk of developing leukemia.
Paroxysmal nocturnal hemoglobinuria is a rare disorder, estimated to affect between 1 and 5 per million people. Experts estimate between 400 and 500 PNH cases are diagnosed in the U.S. each year 3. Paroxysmal nocturnal hemoglobinuria affects both sexes equally, and can occur at any age, although it is most often diagnosed in young adulthood. Paroxysmal nocturnal hemoglobinuria can occur at any age, but is usually diagnosed in young adulthood in people in their 30s and 40s. People with PNH have recurring episodes of symptoms due to hemolysis, which may be triggered by stresses on the body such as infections or physical exertion.
Paroxysmal nocturnal hemoglobinuria is caused by acquired, rather than inherited, mutations in the PIGA gene (located on Xp22.1); the condition is not passed down to children of affected individuals 4. Sometimes, people who have been treated for aplastic anemia may develop PNH 1. The treatment of paroxysmal nocturnal hemoglobinuria is largely based on symptoms; stem cell transplantation is typically reserved for severe cases of PNH with aplastic anemia or those whose develop leukemia 2.
What is bone marrow failure?
Bone marrow failure happens when the marrow does not produce enough red cells, white cells or platelets, or the blood cells that are produced are damaged or defective. This means the body can not supply itself with the blood it needs. PNH, along with aplastic anemia and myelodysplastic syndromes (MDS), are bone marrow failure diseases.
What happens to my blood with PNH?
Blood consists of blood cells floating in plasma. Plasma is mostly made of water. It also includes salts, proteins, hormones, minerals, vitamins and other nutrients and chemicals your body needs.
The 3 basic types of blood cells:
- Red blood cells (RBCs) are also called erythrocytes. They make up almost half of blood. Red blood cells are filled with the protein hemoglobin that picks up oxygen in the lungs and brings it to cells all around the body.
- White blood cells (WBCs) are also called leukocytes. They fight disease and infection by attacking and killing germs that get into the body. There are several kinds of white blood cells, each of which fights a different kind of germ.
- Platelets are also called thrombocytes. They are small pieces of cells that help blood clot and stop bleeding.
Blood cells formation
The process of making blood cells is called hematopoiesis. Blood cells are made in the bone marrow, a spongy tissue located inside certain bones. Marrow contains blood-forming stem cells that make copies of themselves to create all 3 types of blood cells. When blood cells are fully mature and functional, they leave the bone marrow and enter the bloodstream. Healthy people have enough stem cells to make all the blood cells they need.
What is the complement system in PNH?
The complement system is a group of proteins in the blood. They help support (complement) the work of white blood cells by fighting infections.
These proteins are always active at a very low level. But when bacteria, viruses and other foreign or abnormal cells get into your body, these proteins become more active. They work together to attack and destroy these abnormal cells.
Normal red blood cells have a shield of proteins. This shield protects the cells from being attacked by the complement system. The gene in charge of making this protective shield is called PIGA (phosphatidylinositol glycan class A).
Why are blood clots so common for people with PNH?
Scientists are not sure exactly why people with PNH are more likely to get blood clots. But some believe that PNH patients have abnormal platelets that are too “sticky.” This means the platelets make clots too easily.
Many people with PNH have a shortage of nitric oxide. Nitric oxide helps prevent blood clots by making it harder for platelets to stick together. Hemolysis – another symptom of PNH – can cause a shortage of nitric oxide.
How do I find out if I have a blood clot?
To diagnose a blood clot, your doctor may take pictures of your insides using:
- CT scan (Cat Scan)
- MRI (Magnetic Resonance Imaging)
- Doppler scan
- V-Q Scan (Ventilation-Perfusion Scan)
Your doctor may also order a lab test called D-dimer. It is also called Fragment D-Dimer, or Fibrin degradation fragment.
What immunizations should a PNH patient get?
Patients with PNH should receive vaccinations against certain types of bacteria to prevent infection. Ask your doctor which ones are right for you.
Seasonal flu vaccines protect against the three influenza viruses (trivalent) that research indicates will be most common during the upcoming season. Talk with your hematologist about whether you should get a flu shot. He will help you weigh the risks and benefits of getting a flu shot. Don’t forget to ask whether your family members and others in close contact with you should get a flu vaccine. This may reduce your chance of getting the flu. To read more about flu shots, read our article.
There have been a few case reports of PNH patients getting flares of hemolysis (when red blood cells are destroyed) after receiving a flu shot. Although case reports are not the same as randomized clinical trials, one case of hemolysis was severe enough to put the patient in the hospital. That is why some PNH experts recommend against having a flu shot, but each case is different. PNH patients who are receiving eculizumab may be less likely to have hemolysis after receiving a flu shot.
Can PNH patients get pregnant and have a healthy delivery?
Pregnancy is possible with PNH, but it is not a good idea. It carries serious risks for both mother and child.
A woman with PNH faces a number of risks during pregnancy:
- Her blood may have fewer healthy cells.
- Her bone marrow may make fewer healthy cells.
- She is more likely to get blood clots. Most doctors place pregnant women with PNH on blood thinners to prevent clots. But warfarin (Coumadin®) cannot be used during the first trimester, since it may affect fetus development.
- She is more likely to get preeclampsia, a dangerous condition that causes very high blood pressure and can put both mother and baby at risk.
- She may need red blood cell transfusions more often.
A baby whose mother has PNH has a greater risk of:
- Premature birth
- Dying in the womb
- Having a low birth weight
- Having delayed growth and development
Still, about 1 out of 3 babies whose mothers have PNH do not have any of these problems.
If you do get pregnant, look for a PNH specialist and an obstetrician who specializes in high-risk births.
Is surgery safe for PNH patients?
Surgery can also be risky for people with PNH because it:
- Makes the complement system more active, which can cause hemolysis
- Increases the risk of getting blood clots
- Can cause serious bleeding in people with a low platelet count
- May require platelet transfusions before surgery.
If you do have surgery, it is a good idea to:
- Make sure your PNH specialist talks with your surgeon
- Take the blood thinner Heparin (Calciparine or Liquaemin) as soon as possible after surgery, as long as your platelet count is good and your doctor advises it.
Special precautions for PNH patients
Airplane travel and high altitudes
The farther you move away from sea level, the less oxygen there is. If you have anemia, flying in an airplane or visiting places at higher elevations than you’re used to may cause a shortage of oxygen. It may also cause chest pain. Before you do either of these things, it’s a good idea to:
- Check with your doctor
- Get a red blood cell count
- Get treatment for your anemia (blood transfusions or growth factors)
- If you do fly, remember to:
- Drink plenty of water
- Get up and walk around every hour or two if it is safe to do so
Paroxysmal nocturnal hemoglobinuria causes
Paroxysmal nocturnal hemoglobinuria or PNH is caused by a genetic change (mutation) in the PIGA gene (phosphatidylinositol glycan class A gene) of a single stem cell in your bone marrow 5. The PIGA gene provides instructions for making a protein called phosphatidylinositol glycan class A. This protein takes part in a series of steps that produce a molecule called glycosyl-phosphatidylinositol anchor or GPI anchor. GPI anchor attaches many different proteins to the cell membrane, including the complement inhibitory proteins CD55 (decay accelerating factor [DAF]) and CD59 (membrane inhibitor of reactive lysis [MIRL]), thereby ensuring that these proteins are available when needed at the surface of the cell 6, 7. GPI deficiency results in complement-mediated intravascular hemolysis and thrombophilia, the main cause of morbidity and mortality in PNH 8, 9, 10, 11.
Here are the steps that lead to PNH:
- The abnormal stem cell makes copies of or “clones” itself. This leads to a whole population of bone marrow stem cells that have mutant PIGA.
- The abnormal cells mature into red blood cells that have mutant PIGA. These are called PNH red blood cells. Doctors also call them your PNH clone.
- The PNH red blood cells lack the shield of proteins that protect normal red blood cells from the complement system, leaving them open to attack and destruction by the complement system proteins.
Many healthy people have a small number of PNH stem cells. In people with PNH, however, these stem cells grow fast and make lots of mature PNH red blood cells.
Some doctors believe this growth happens because people with PNH have bone marrow that is weaker than normal. This weakening may be caused by aplastic anemia or another mild and/or undiagnosed bone marrow failure disease.
If you have had aplastic anemia, you are more likely to get PNH. There are no other known factors that increase your chances of getting PNH.
Some gene mutations are acquired during a person’s lifetime and are present only in certain cells. These changes, which are called somatic mutations, are not inherited. In people with paroxysmal nocturnal hemoglobinuria, somatic mutations of the PIGA gene occur in blood-forming cells called hematopoietic stem cells, which are found mainly in the bone marrow. These mutations result in the production of abnormal blood cells. As the abnormal hematopoietic stem cells multiply, increasing numbers of abnormal blood cells are formed, alongside normal blood cells produced by normal hematopoietic stem cells.
The premature destruction of red blood cells seen in paroxysmal nocturnal hemoglobinuria is caused by a component of the immune system called complement. Complement consists of a group of proteins that work together to destroy foreign invaders such as bacteria and viruses. To protect the individual’s own cells from being destroyed, this process is tightly controlled by complement-regulating proteins. Complement-regulating proteins normally protect red blood cells from destruction by complement. In people with paroxysmal nocturnal hemoglobinuria, however, abnormal red blood cells are missing two important complement-regulating proteins that need the GPI anchor protein to attach them to the cell membrane. These red blood cells are prematurely destroyed, leading to hemolytic anemia.
Research suggests that certain abnormal white blood cells that are also part of the immune system may mistakenly attack normal blood-forming cells, in a malfunction called an autoimmune process. In addition, abnormal hematopoietic stem cells in people with paroxysmal nocturnal hemoglobinuria may be less susceptible than normal cells to a process called apoptosis, which causes cells to self-destruct when they are damaged or unneeded. These features of the disorder may increase the proportion of abnormal blood cells in the body. The proportion of abnormal blood cells affects the severity of the signs and symptoms of paroxysmal nocturnal hemoglobinuria, including the risk of hemoglobinuria and thrombosis.
Paroxysmal nocturnal hemoglobinuria inheritance pattern
Paroxysmal nocturnal hemoglobinuria is acquired, rather than inherited. Paroxysmal nocturnal hemoglobinuria results from new mutations in the PIGA gene, and generally occurs in people with no previous history of the disorder in their family. Paroxysmal nocturnal hemoglobinuria is not passed down to children of affected individuals.
Risk factors of having PNH
Having aplastic anemia is the only known risk factor for developing PNH. More than 10 out of every 100 people with aplastic anemia will develop PNH. In addition, some people with PNH will develop aplastic anemia. People with PNH can share symptoms with aplastic anemia patients, such as low blood cell counts.
On average, 2 out of 100 people with PNH go on to develop myelodysplastic syndrome (MDS).
Paroxysmal nocturnal hemoglobinuria symptoms
When your PNH red blood cells break apart, their hemoglobin is released into your plasma. Hemoglobin is the red part of red blood cells. Its carries oxygen around your body. The release of hemoglobin can cause a number of symptoms, including:
- Dark or tea colored urine, but it does not darken in all cases
- Low red blood cell count (anemia) which can cause you to:
- Feel tired
- Have headaches
- Have trouble breathing when you exercise
- Have an irregular heartbeat
- Muscle spasms in certain parts of your body. This happens when the released hemoglobin binds with nitric oxide and removes it from your blood. Nitric oxide helps your muscles stay smooth and relaxed. When you have a shortage of nitric oxide, you may experience the following:
- Mild to severe pain in your abdomen or belly area.
- Spasms in your esophagus which is a “tube” in your throat that goes from your mouth to your stomach; the spasms can make it hard to swallow.
- Men may have trouble getting or keeping an erection (become impotent).
- Thrombosis is a blood clot in a vein. It is often simply called a blood clot. At least 1 out of 3 people with PNH get blood clots. The symptoms of blood clots depend on where the blood clots occur. People who are otherwise healthy and do not have PNH sometimes get blood clots in the veins of the leg. People with PNH tend to get blood clots in other parts of the body, such as in the brain or abdomen (belly area).
- Blood clot in abdomen (belly area): You may get a blood clot in your abdomen, or belly area. That’s the area below your chest and above your hips. Some places in the abdomen where you may get a blood clot include:
- Your spleen
- The major vein that leaves your liver; this is called Budd-Chiari syndrome
- Your intestine (bowel) may not get enough blood; this is called ischemia
- Symptoms of getting a blood clot in your abdomen may include:
- Having fluid and swelling in the belly area; this is called ascites.
- The area where the clot is may feel warm to the touch.
- The area where the clot is may be painful.
- If the blood clot in your abdomen is not treated:
- Part of your intestine may die (dead bowel)
- Your liver may be damaged and stop working
- Blood clot in brain: You may get a blood clot in the veins covering your brain. If this happens, symptoms may include:
- A very bad headache.
- Trouble speaking, seeing, or moving parts of your body.
- Blood clot in skin: You may get a blood clot in the veins of your skin. If this happens, your skin in that area may get red, puffy, warm or painful
- Blood clot in arm or leg: You may get a blood clot in the veins of your arm or leg. If this happens that limb may get warm, puffy or painful
- Blood clot in lung: Sometimes, a blood clot breaks off and travels to your lung. This is called a pulmonary embolism. If you have a pulmonary embolism, symptoms may include:
- A sharp pain in your chest; it may get worse when you breathe deeply
- Trouble breathing (shortness of breath), or you may start breathing fast
- Suddenly feeling anxious
- Coughing up some blood
- Feeling dizzy; you may even faint
- Sweating a lot
- Blood clot in abdomen (belly area): You may get a blood clot in your abdomen, or belly area. That’s the area below your chest and above your hips. Some places in the abdomen where you may get a blood clot include:
People with paroxysmal nocturnal hemoglobinuria have sudden, recurring episodes of symptoms (paroxysmal symptoms), which may be triggered by stresses on the body, such as infections or physical exertion. During these episodes, red blood cells are prematurely destroyed (hemolysis). Affected individuals may pass dark-colored urine due to the presence of hemoglobin, the oxygen-carrying protein in blood. The abnormal presence of hemoglobin in the urine is called hemoglobinuria. In many, but not all cases, hemoglobinuria is most noticeable in the morning, upon passing urine that has accumulated in the bladder during the night (nocturnal).
The premature destruction of red blood cells results in a deficiency of these cells in the blood (hemolytic anemia), which can cause signs and symptoms such as fatigue, weakness, abnormally pale skin (pallor), shortness of breath, and an increased heart rate. People with paroxysmal nocturnal hemoglobinuria may also be prone to infections due to a deficiency of white blood cells.
Abnormal platelets associated with paroxysmal nocturnal hemoglobinuria can cause problems in the blood clotting process. As a result, people with this disorder may experience abnormal blood clotting (thrombosis), especially in large abdominal veins; or, less often, episodes of severe bleeding (hemorrhage).
Individuals with paroxysmal nocturnal hemoglobinuria are at increased risk of developing cancer in blood-forming cells (leukemia).
In some cases, people who have been treated for another blood disease called aplastic anemia may develop paroxysmal nocturnal hemoglobinuria.
Low red blood cell count
PNH will mostly cause low red blood cell counts and anemia. A low red blood cell count is called anemia. If you have a low red blood cell count, you may:
- Feel a little tired or very tired
- Feel less alert or have trouble concentrating
- Have a loss of appetite or lose weight
- Have paler-than-normal skin
- Have trouble breathing – shortness of breath
- Have rapid heartbeat
- Have difficulty exercising or climbing stairs
Low white blood cell counts
A low white blood cell count is called neutropenia. In general, a low white cell count lowers an aplastic anemia patient’s ability to fight bacterial infections. If you have a low white blood cell count, you may:
- Have repeated fevers and infections
- Get bladder infections that make it painful to urinate or make you urinate more often
- Get lung infections that cause coughing and difficulty breathing
- Get mouth sores
- Get sinus infections and a stuffy nose
- Get skin infections
A fever in an aplastic anemia patient is potentially serious. A doctor should be notified if a fever occurs.
Low platelet counts
A low platelet count is called thrombocytopenia. If you have a low platelet count, you may:
- Bruise or bleed more easily, even from minor scrapes and bumps
- Get heavier than normal menstrual periods
- Get nose bleeds
- Get tiny, flat red spots under your skin (petechiae) caused by bleeding
- Have bleeding gums, especially after dental work or from brushing your teeth.
If platelet counts are not too low, there may be no obvious symptoms. In rare cases, the number of platelets can get so low that dangerous internal bleeding occurs.
Bleeding that will not stop is a medical emergency. A PNH patient needs to seek immediate medical help if they have bleeding that can’t be stopped by usual methods, such as applying pressure to the area.
Paroxysmal nocturnal hemoglobinuria complications
Common complications of PNH include thrombosis (reported in as many as 40% of patients) including hepatic, cerebral, and abdominal and both venous and arterial thrombosis 12. Thrombosis mainly affects the venous blood vessels and may also occur in atypical sites, including the cerebral, mesenteric, and renal vessels. Hepatic veins may also be involved in the so-called Budd–Chiari syndrome 13, 14. Some studies have suggested that larger PNH clones correlate with increased thrombotic risk, however, many adjunctive congenital (eg, factor V Leiden or factor II mutations, protein C and S deficiencies, etc.) or acquired risk factors (eg, cigarette smoke, diabetes, obesity, estro-progestin compounds, pregnancy, surgery, prolonged immobilization, etc.) may contribute to thrombosis in this setting and deserve consideration 15. PNH can also be complicated by infectious events, either related to the coexistence of bone marrow failure and immunosuppression, or to complement inhibition. Anti-Neisseria meningitidis vaccinations are mandatory before eculizumab, and the addition of anti-Streptococcus pneumoniae and anti-Hemophilus influenzae vaccines have been required with novel agents in clinical trials. However, not all vaccinated subjects will get proper immunization and antibody titers are not routinely evaluated. Therefore, patient education remains pivotal for prompt recognition and treatment of infectious episodes. Additionally, infections may trigger breakthrough hemolysis, further complicating the clinical picture.
Other complications associated with PNH include acute or chronic kidney disease, pulmonary hypertension, erectile dysfunction, and dysphagia.
Paroxysmal nocturnal hemoglobinuria diagnosis
When you have anemia caused by the destruction of red blood cells, doctors call this hemolytic anemia. In addition to a complete blood cell count (CBC), the principal studies used to establish the diagnosis of paroxysmal nocturnal hemoglobinuria (PNH) are flow cytometry of peripheral blood and bone marrow analysis. Flow cytometry measures the percentage of cells that are deficient in the glycosyl phosphatidylinositol–anchored proteins (GPI-APs) and identifies discrete populations with different degrees of deficiency. Because of the missing GPI-APs, red blood cells (RBCs) and other cells in patients with PNH lack DAF (CD55) and MIRL (CD59), which regulate complement.
Hemosiderin is nearly always present in the urine sediment and can accumulate in the kidneys; this is visible on magnetic resonance images (MRI) or computed tomography (CT) scans. An elevated reticulocyte count and serum lactate dehydrogenase (LDH) level with a low serum haptoglobin level in the absence of hepatosplenomegaly are the hallmarks of intravascular hemolysis.
Bone marrow examination will differentiate classic PNH from PNH that develops in the setting of other bone marrow disorders 16. In addition, bone marrow examination will identify an erythroid and hyperplastic bone marrow during the hemolytic phase or a hypoplastic bone marrow in the aplastic phase.
Imaging studies are indicated in patients with venous thrombosis.
PNH test
There are several blood tests used to help confirm a diagnosis of PNH by looking for signs of hemolytic anemia. Specific tests include:
- A complete blood count (CBC) to look for signs of low hemoglobin. This test uses a number of methods to measure how many of each blood cell type are in your blood sample.
- An LDH test looks at the level of an enzyme called lactate dehydrogenase. High levels of LDH in the blood can mean that red blood cells are breaking apart (hemolysis) or that there is tissue damage in the body. It is important for patients with PNH to have LDH monitored regularly.
- A bilirubin test measures the total amount of this substance in your blood. High levels may indicate destruction of red blood cells.
- A reticulocyte count measures the number of young red blood cells in your blood. People who have PNH may have elevated reticulocyte counts because their bone marrow is making lots of new red blood cells.
Flow Cytometry
The gold standard for confirming the presence of PNH is a flow cytometry test. This test tells your doctor if any proteins are missing from the surface of blood cells. PNH cells are missing some or all of two proteins on their surface. These proteins are called CD55 and CD59. FLAER is a new type of flow cytometry test that is also used.
Using flow cytometry, your doctor can usually divide your blood cells into 3 types:
- PNH 1 cells, or Type 1 cells: These cells are normal. They respond in a healthy way to the complement system.
- PNH 2 cells, or Type 2 cells: These cells are partially sensitive to the complement system. They are missing some of the CD55 and CD59 proteins that protect them from attack.
- PNH 3 cells, or Type 3 cells: These cells are extremely sensitive to the complement system. Of the 3 groups of cells, these break apart most easily. They are missing all the proteins that protect normal cells from attack. Most people with PNH have Type 1 and Type 3 cells, but the amount of each type of cell can vary greatly.
Other blood tests
Doctors may ask you do to several types of blood tests to help them understand your case of PNH and create a treatment plan. These include:
- EPO level, also called erythropoietin, measures how much of this protein is being made by your kidneys. EPO is created in response to low oxygen levels in the body, typically caused by low red cell counts and anemia. EPO causes your bone marrow to make more red blood cells. A low EPO level may indicate a problem other than PNH, or it may make anemia worse in people who have PNH.
- Iron level test, also called a ferritin test, checks the level of iron in your blood. If a shortage of iron is causing anemia, it can be easily treated with iron supplements. If you have too much iron in your body this is called iron overload. It can be caused from getting lots of red blood cell transfusions or by genetic conditions. A number of treatments exist to remove iron from your body.
- Vitamin B12 and a folate level may be done to rule out other causes of low red cell counts. If your red blood cells have an abnormal shape, size or look, this can be caused by low levels of vitamin B12 and folate (folic acid). These abnormal looking cells don’t work right, and this can lead to anemia.
Bone marrow tests
An examination of your bone marrow is important for the diagnosis of PNH. It is usually a simple 30-minute procedure. First, the doctor uses a hollow needle to remove some bone marrow aspirate (liquid bone marrow), typically from the pelvic or breast bone. A solid piece of bone marrow is also removed for a bone marrow biopsy.
The doctor will look at your liquid bone marrow under a microscope and send a sample of your bone marrow to a lab.
A bone marrow test is done for two main reasons:
- To help confirm a diagnosis of PNH
- To understand how well or poorly your bone marrow is making blood cell
The bone marrow test shows:
- The quantity (cellularity) of your bone marrow occupied by different cells
- Exactly what types and amounts of cells your bone marrow is making
- Increased, decreased, or normal levels of iron in your bone marrow
- Chromosomal (DNA) abnormalities
Paroxysmal nocturnal hemoglobinuria treatment
According to current understanding of paroxysmal nocturnal hemoglobinuria (PNH), the ideal treatment is to replace the defective hematopoietic stem cell with a normal equivalent by stem cell transplantation; however, this is not realistic for many patients, because stem cell transplantation requires a histocompatible donor and is associated with significant morbidity and mortality 17. This form of treatment is reserved for severe cases of PNH with aplastic anemia or transformation to leukemia, both of which are life-threatening complications.
Androgens
Androgens are natural male hormones that can cause your bone marrow to make more red blood cells. This can improve anemia. Androgens are sometimes used to treat aplastic anemia and PNH.
Blood transfusions
A blood transfusion is a safe and common procedure. Most people who have a bone marrow failure disease like aplastic anemia, MDS or PNH will receive at least one blood transfusion. When you receive a blood transfusion, parts of blood from a donor are put into your bloodstream. This can help some patients with low blood counts.
Eculizumab
In 2007, eculizumab (Soliris), an anti-complement antibody targeting the CD5 complement component, was approved by the US Food and Drug Administration (FDA) and the European Medicines Evaluation Agency (EMEA) to treat PNH 18. It works by making your complement system less active by preventing its activation to C5b by the C5 convertase thus inhibiting the formation of the membrane attack complex and reduces hemolysis. Treatment with eculizumab reduced transfusions, improved anemia and fatigue, and reduce PNH symptoms. Furthermore, it reduced thrombosis occurrence and improved survival 19, 20, 21, 22. Additionally, eculizumab appeared safe during pregnancy, and reduce fetal-maternal outcomes, although formal toxicology studies in pregnancy are lacking 23. The recommended maintenance dose of eculizumab is fixed (900 mg every 2 weeks ± 2 days) intravenously 8.
Eculizumab is approved for the treatment of patients with PNH in nearly 50 countries worldwide.
Eculizumab alleviates the hemolysis associated with PNH and its complications, dramatically improving symptoms, improving quality of life, and eliminating complications of PNH 24. However, eculizumab does not alter the underlying defect of the disease, thus, treatment needs to continue life-long or until spontaneous remission, which occurred only in a minority of patients (12 of 80 patients in one study) before the advent of eculizumab 25.
Ravulizumab
In 2018, the FDA approved ravulizumab (Ultomiris) for treatment of the hemolysis of PNH. Ravulizumab (Ultomiris) is a long-acting C5 inhibitor that works by inhibiting the C5 protein in the terminal complement cascade. Ravulizumab has 3 to 4 times longer half-life and requires dosing every eight weeks. It is shown to be more cost-effective compared to eculizumab. It has fewer breakthrough hemolysis episodes, and it is non-inferior to eculizumab in terms of efficacy and safety profile.
Pegcetacoplan
In 2021, the FDA approved pegcetacoplan (Empaveli) to treat adults with PNH. Compared to eculizumab and ravulizumab that block the C5 component of complemen, pegcetacoplan blocks the C3 component of complement. Consequently, pegcetacoplan blocks both extravascular hemolysis and intravascular hemolysis, whereas eculizumab and ravulizumab block intravascular hemolysis but not extravascular hemolysis. Patients who remain anemic (particularly if transfusions are required) due to extravascular hemolysis despite treatment with eculizumab or ravulizumab may benefit from treatment with pegcetacoplan. Pegcetacoplan is given as a self-administered subcutaneous infusion two or in some cases, three times per week.
Folic acid
Folic acid, also called folate or vitamin B9, is found in fresh or lightly cooked green vegetables. It helps your bone marrow make normal blood cells. When your bone marrow has to make more cells, it needs a larger supply of folic acid.
Most people get enough folate in their diet. But if you have PNH, it’s a good idea to take 1 mg each day of a man-made form of folate called folic acid.
Some individuals with PNH receive folic acid (folate) supplements to ensure that the supply of folate is adequate as demand increases when the bone marrow attempts to compensate for the hemolytic anemia of PNH by augmenting red blood cell production (erythropoiesis) in the bone marrow.
Growth factors
Growth factors are naturally occurring hormones in your body that signal your bone marrow to make more of certain types of blood cells. Man-made growth factors may be given to some people with bone marrow failure diseases to help increase red blood cell, white blood cell or platelet counts.
Iron supplement
Supplemental iron should be given to individuals with iron deficiency, which can occur because of red blood cell destruction and the consequent loss of iron in the urine.
Iron chelation
Iron chelation therapy is the main treatment used when you have a condition called iron overload. Iron overload means you have too much iron in your body. This can be a problem for people who get lots of red blood cell transfusions.
Treatment of bone marrow hypoplasia with bone marrow transplant
Bone marrow hypoplasia is a serious cause of morbidity and mortality. Bone marrow hypoplasia is treated most effectively with bone marrow transplantation also called a stem cell transplant (SCT) or hematopoietic stem cell transplant (HSCT). The specific form of bone marrow transplantation used most often in treating PNH is an allogeneic bone marrow transplant. During an allogeneic bone marrow transplant, an affected individual’s bone marrow is destroyed usually by chemotherapy, immunotherapy, radiation or some combination and replaced with healthy marrow obtained from a donor. The donor marrow is transplanted intravenously into the body where it travels to the bone marrow and eventually begins producing new blood cells. The best match for a bone marrow transplant is a sibling with an identical HLA type. However, in some individuals, a search for an unrelated, matched donor is necessary. Bone marrow transplantation can cure underlying bone marrow dysfunction and can eliminate the defective PNH stem cells. Moroover, if there is no suitable donor available, antithymocyte globulin has been used in the treatment of aplastic anemia with considerable success.
Thromboembolism
Patients with PNH who develop acute thrombosis should immediately be started on eculizumab, if they are not already taking it, as this reduces the risk of thrombosis extension or recurrence 26. Otherwise, management of thrombotic complications follows standard principles, including using heparin emergently, then maintenance therapy with the use of an oral anticoagulant (drug that blocks the formation of blood clots), such as warfarin. Sometimes, heparin can exacerbate the thrombotic problem, possibly by activating complement. This can be prevented using inhibitors of the cyclooxygenase system, such as aspirin, ibuprofen, and sulfinpyrazone.
Primary prophylaxis of thromboembolism for patients with PNH has been advocated. Whether this approach is safe and effective in all patients with PNH remains controversial, however.
Corticosteroids
Some physicians suggest that individuals exhibiting symptoms of hemolysis should receive treatment with steroids such as prednisone because it is believed that such treatment slows the rate of destruction of red blood cells. The usual adult dose of prednisone is 20-40 mg/d (0.3-0.6 mg/kg/day) given daily during hemolysis and changed to alternate days during remission. On this regimen, about 70% of adult patients experience improvement in hemoglobin levels, but long-term therapy is fraught with complications. Furthermore, treatment with steroids such as prednisone is controversial because steroid therapy is not beneficial to everyone and carries the potential for serious side effects, especially if the therapy is continued for a long duration.
Investigational agents
A variety of agents that inhibit complement are under development for treatment of PNH. Novel anti-C5 agents include monoclonal antibodies and an anti-C5 small interfering RNA 27. Because clinically relevant C3-mediated extravascular hemolysis can occur in PNH 28, the anti-C3 small peptide compstatin and its derivatives are being investigated, along with inhibitors of complement Factor D or B 27.
Yuan et al 29 reported that two novel small-molecule inhibitors of Factor D, which is a component of the alternative complement pathway, show potential as oral agents for treating PNH. In the Ham test, using cells from PNH patients, the Factor D inhibitors significantly reduced complement-mediated hemolysis at concentrations as low as 0.01 μM. In an animal model, the compound ACH-4471 blocked alternative pathway activity.
PNH prognosis
The prognosis in patients with paroxysmal nocturnal hemoglobinuria (PNH) may vary from person to person, depending on the severity of symptoms and the presence of complications. If not treated, PNH could lead to death in approximately 35% of affected people within five years of diagnosis and 50% within 10 years of diagnosis 30. You may have only mild symptoms, or you may have severe symptoms and need medicines or blood transfusions. An aplastic phase is a serious prognostic factor, because the resulting pancytopenia and thrombosis of hepatic, abdominal, and cerebral veins can have life-threatening consequences. Prophylactic anticoagulation has not been shown to be of benefit because of a lack of data from a clinical trial setting.
In many patients with paroxysmal nocturnal hemoglobinuria (PNH), the abnormal clone may eventually disappear. This usually takes at least 5 years, and often as long as 15-20 years. Reactivation of PNH in these patients has been observed with acute infections. Patients with chronic anemia alone, without thrombotic complications, can live relatively normal lives for many years.
Many people with PNH live for decades. People who develop blood clots in key parts of the body, or also have MDS (myelodysplastic syndromes) or AML (acute myeloid leukemia), may have a shorter lifespan.
The good news is that good treatments are available, and new treatments are being developed that help people with PNH live longer. You may have seen older research saying that patients with PNH live an average of 15 to 20 years, but more recent research shows that life expectancy has been steadily climbing over the past 20 years. It is even possible that PNH patients will soon live just as long as the average person of the same age 31.
References- Paroxysmal nocturnal hemoglobinuria. https://ghr.nlm.nih.gov/condition/paroxysmal-nocturnal-hemoglobinuria
- Paroxysmal Nocturnal Hemoglobinuria. https://emedicine.medscape.com/article/207468-overview
- Paroxysmal Nocturnal Hemoglobinuria (PNH). https://www.aamds.org/diseases/pnh
- Parker CJ. The pathophysiology of paroxysmal nocturnal hemoglobinuria. Exp Hematol. 2007;35:523-33. https://doi.org/10.1016/j.exphem.2007.01.046
- Luzzatto L. Paroxysmal nocturnal hemoglobinuria: An acquired X-linked genetic disease with somatic-cell mosaicism. Curr. Opin. Genet. Dev. 2006;16:317–322. doi: 10.1016/j.gde.2006.04.015
- Parker CJ. Update on the diagnosis and management of paroxysmal nocturnal hemoglobinuria. Hematol Am Soc Hematol Educ Program. 2016;2016(1):208–216. doi: 10.1182/asheducation-2016.1.208
- Kinoshita T, Inoue N, Takeda J. Defective glycosyl phosphatidylinositol anchor synthesis and paroxysmal nocturnal hemoglobinuria. Adv Immunol. 1995;60:57-103. doi: 10.1016/s0065-2776(08)60584-2
- Fattizzo B, Cavallaro F, Oliva EN, Barcellini W. Managing Fatigue in Patients with Paroxysmal Nocturnal Hemoglobinuria: A Patient-Focused Perspective. J Blood Med. 2022 Jun 17;13:327-335. doi: 10.2147/JBM.S339660
- Parker CJ. Hemolysis in PNH. In: Young NS, Moss J, editors. Paroxysmal Nocturnal Hemoglobinuria and the Glycosylphosphatidylinositol-Linked Proteins. San Diego: Academic Press; 2000:49–100.
- Inoue N, Izui-Sarumaru T, Murakami Y, et al. Molecular basis of clonal expansion of hematopoiesis in 2 patients with paroxysmal nocturnal hemoglobinuria (PNH). Blood. 2006;108(13):4232–4236. doi: 10.1182/blood-2006-05-025148
- Endo M, Ware RE, Vreeke TM, et al. Molecular basis of the heterogeneity of expression of glycosyl phosphatidylinositol anchored proteins in paroxysmal nocturnal hemoglobinuria. Blood. 1996;87(6):2546–2557. doi: 10.1182/blood.V87.6.2546.bloodjournal8762546
- Hill A, Kelly RJ, Hillmen P. Thrombosis in paroxysmal nocturnal hemoglobinuria. Blood. 2013 Jun 20;121(25):4985-96; quiz 5105. doi: 10.1182/blood-2012-09-311381
- Gurnari C, Colak C, Zawit M, Maciejewski JP. Chronic Budd-Chiari syndrome in paroxysmal nocturnal haemoglobinuria. Lancet. 2021;398 (10304):e14. doi: 10.1016/S0140-6736(21)01542-7
- Plessier A, Esposito-Farèse M, Baiges A, et al. Paroxysmal nocturnal hemoglobinuria and vascular liver disease: eculizumab therapy decreases mortality and thrombotic complications. Am J Hematol. 2022;97(4):431–439. doi: 10.1002/ajh.26474
- Fattizzo B, Dunlop A, Ireland RM, et al. Prognostic and predictive impact of small PNH clones in a large cohort of patients with myelodysplastic syndromes and aplastic anemia: a single-center experience. Blood. 2018;132:3870. doi: 10.1182/blood-2018-99-116772
- Dulau-Florea A, Maric I, Calvo KR, Braylan RC. Detection of paroxysmal nocturnal hemoglobinuria (PNH) in bone marrow aspirates☆. Semin Hematol. 2019 Jan. 56 (1):65-68.
- Paroxysmal Nocturnal Hemoglobinuria Treatment & Management. https://emedicine.medscape.com/article/207468-treatment
- Parker C. Eculizumab for paroxysmal nocturnal haemoglobinuria. Lancet. 2009;373(9665):759–767. doi: 10.1016/S0140-6736(09)60001-5
- Brodsky RA, Young NS, Antonioli E, et al. Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria. Blood. 2008;111(4):1840–1847. doi: 10.1182/blood-2007-06-094136
- Hillmen P, Hall C, Marsh JC, et al. Effect of eculizumab on hemolysis and transfusion requirements in patients with paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2004;350(6):552–559. doi: 10.1056/NEJMoa031688
- Hillmen P, Young NS, Schubert J, et al. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2006;355(12):1233–1243. doi: 10.1056/NEJMoa061648
- Kelly RJ, Hill A, Arnold LM, et al. Long-term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria: sustained©efficacy and improved survival. Blood. 2011;117(25):6786–6792. doi: 10.1182/blood-2011-02-333997
- Kelly RJ, Hochsmann B, Szer J, et al. Eculizumab in pregnant patients with paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2015;373 (11):1032–1039. doi: 10.1056/NEJMoa1502950
- Sicre de Fontbrune F, Peffault de Latour R. Ten Years of Clinical Experience With Eculizumab in Patients With Paroxysmal Nocturnal Hemoglobinuria. Semin Hematol. 2018 Jul. 55 (3):124-129.
- Hillmen P, Lewis SM, Bessler M, Luzzatto L, Dacie JV. Natural history of paroxysmal nocturnal hemoglobinuria. N Engl J Med. 1995 Nov 9. 333(19):1253-8.
- Griffin M, Munir T. Management of thrombosis in paroxysmal nocturnal hemoglobinuria: a clinician’s guide. Ther Adv Hematol. 2017 Mar. 8 (3):119-126.
- Risitano AM, Marotta S. Toward complement inhibition 2.0: Next generation anticomplement agents for paroxysmal nocturnal hemoglobinuria. Am J Hematol. 2018 Aug. 93 (4):564-577.
- Notaro R, Sica M. C3-mediated extravascular hemolysis in PNH on eculizumab: Mechanism and clinical implications. Semin Hematol. 2018 Jul. 55 (3):130-135.
- Yuan X, Gavriilaki E, Thanassi JA, Yang G, Baines AC, Podos SD, et al. Small-molecule factor D inhibitors selectively block the alternative pathway of complement in paroxysmal nocturnal hemoglobinuria and atypical hemolytic uremic syndrome. Haematologica. 2017 Mar. 102 (3):466-475.
- Hillmen P., Lewis S.M., Bessler M., Luzzatto L., Dacie J.V. Natural history of paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 1995;333:1253–1258. doi: 10.1056/NEJM199511093331904
- Gembillo G, Siligato R, Cernaro V, Santoro D. Complement Inhibition Therapy and Dialytic Strategies in Paroxysmal Nocturnal Hemoglobinuria: The Nephrologist’s Opinion. J Clin Med. 2020 Apr 26;9(5):1261. doi: 10.3390/jcm9051261





{kind=link}