Perianal fistula
Perianal fistula also commonly called fistula-in-ano, is an abnormal hollow tract or tunnel that is lined with granulation tissue that connects a primary opening inside the anal canal to a secondary opening in the perianal skin; secondary tracts may be multiple and can extend from the same primary opening 1 and have significant negative impact on their quality of life 2.
Underlying causes of perianal fistula include cryptoglandular infection, Crohn’s disease, radiotherapy, and secondary malignancy 3. Perianal fistulas are a major cause of morbidity among patients with Crohn’s disease, a type of inflammatory bowel disease (IBD). Fistulas due to Crohn’s disease most commonly develop in the perianal region, causing severe infections, fecal incontinence, perianal discharge, negative self-image and social isolation; they can lead to the need for numerous surgeries as well as infertility 4. Perianal fistulas often cause serious, debilitating complications that are difficult to treat, leading to increased costs 5.
Most perianal fistulas are thought to arise as a result of cryptoglandular infection with resultant perirectal abscess. The abscess represents the acute inflammatory event, whereas the perianal fistula is representative of the chronic process. Symptoms generally affect quality of life significantly, and they range from minor discomfort and drainage with resultant hygienic problems to sepsis.
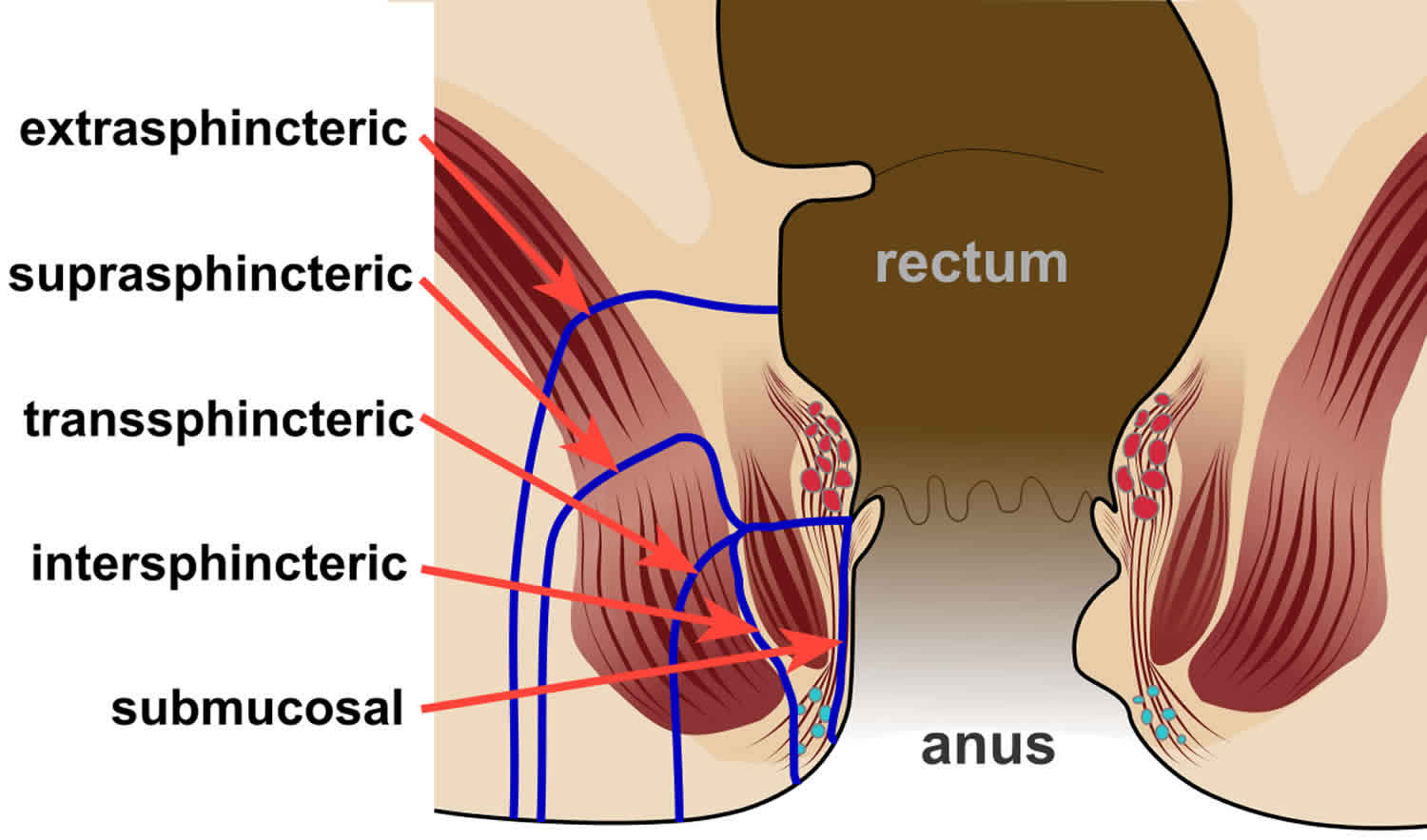
Perianal fistulas are traditionally described using the Parks classification based on their relationship to the external and internal anal sphincters (see Figure 3 below).
Treatment of perianal fistula remains challenging 6. Currently, there is no medical treatment available for perianal fistula and surgery is almost always necessary to cure an anal fistula, though long-term antibiotic prophylaxis and infliximab may have a role in recurrent fistulas in patients with Crohn disease. Traditional therapy for perianal fistulas in Crohn’s disease focuses on antibiotics such as metronidazole or ciprofloxacin. However, medical management has expanded over the years to include immunomodulators and most recently, biologic agents. Newer techniques such as intrafistulous biologic injections are also being explored as potentially effective treatments for patients with fistulizing disease 7. Surgery is the treatment of choice, with the goals of draining infection, eradicating the fistulous tract, and avoiding persistent or recurrent disease while preserving anal sphincter function 8.
If the perianal fistula is straightforward (involving minimal sphincter muscle), a fistulotomy may be performed. This procedure involves unroofing the tract, thereby connecting the internal opening within the anal canal to the external opening and creating a groove that will heal from the inside out.
The surgery may be performed at the same time as drainage of an abscess, although sometimes the fistula doesn’t appear until weeks or years after the initial drainage. Fistulotomy is a long-standing treatment with a high success rate (92-97%). This high success rate must be balanced, however, with the potential changes to a patient’s continence (ability to control stool), as the anal sphincter muscle is divided in a fistulotomy, the greater the risk of changes in continence. Therefore, the surgeon must assess whether a fistulotomy is appropriate for a given patient.
In addition to fistulotomy, there are a number of other surgical treatment options for anal fistula which do not involve division of the sphincter muscles. Fibrin glue injection is one such option, in which fibrin glue is injected into the fistula tract to obliterate the tract with the intention of becoming incorporated in the surrounding tissue. It has the advantage of avoiding dividing any sphincter muscle, thereby preserving continence. While there is a relatively high failure rate with this approach, it does not “burn any bridges” (risk affecting continence) and may be repeated.
An anal fistula plug is an elongated piece of material that is placed throughout the length of the fistula tract to fill the tract space and incorporate itself into the tissue around it. The plug also has the advantage of not requiring division of the sphincter muscle. However, like the fibrin glue, it has a relatively low success rate, with the majority of studies reporting success less than 50%.
An endoanal advancement flap is a procedure usually reserved for complex fistulas or for patients with an increased potential risk for suffering incontinence from a traditional fistulotomy. In this procedure, the internal opening of the fistula is covered over by healthy, native tissue in an attempt to close the point of origin of the fistula. Recurrence rates have been reported to be up to 50% of cases. Certain conditions, such as Crohn’s disease, malignancy, radiated tissue and previous attempts at repair, and smoking, increase the likelihood of failure. Although the sphincter muscle is not divided in this procedure, mild to moderate incontinence has still been reported.
Yet another non-sphincter dividing treatment for anal fistula is the LIFT (ligation of the intersphincteric fistula tract) procedure. This procedure involves division of the fistula tract in the space between the internal and external sphincter muscles. This procedure avoids division of the sphincter muscle, but has not been performed long enough to adequately assess its success or the most appropriate cases to attempt it on.
Most of the operations can be performed on an outpatient basis, but in selected cases, may require hospitalization. Consider identifying a specialist in colon and rectal surgery who will be familiar with a number of potential operations to treat the fistula.
What is the recovery like from perianal fistula surgery?
Pain after surgery is controlled with pain pills, fiber and bulk laxatives. Patients should plan for time at home using sitz baths and avoiding the constipation that can be associated with prescription pain medication. Discuss with your surgeon the specific care and time away from work prior to surgery to prepare yourself for post-operative care.
Can perianal fistula recur?
Up to 50% of abscesses may re-present as another abscess or as a frank fistula. Despite proper treatment and apparent complete healing, fistulas can potentially recur, with recurrence rates dependent upon the particular surgical technique utilized. Should similar symptoms arise, suggesting recurrence, it is recommended that you find a colon and rectal surgeon to manage your condition.
A large meta-analysis examined risk factors for recurrence of anal fistula after fistula surgery included a high transanal fistula, horseshoe extensions, and multiple fistula tracts as well as the patient having a history of anal procedures or not identifying the internal opening of the fistula intraoperatively 9. In a study of 251 patients who had high transphincteric fistulas and were treated with loose setons history of fistula surgery, horseshoe fistula, and anterior fistula were risk factors of recurrence 10.
Perianal fistula classification
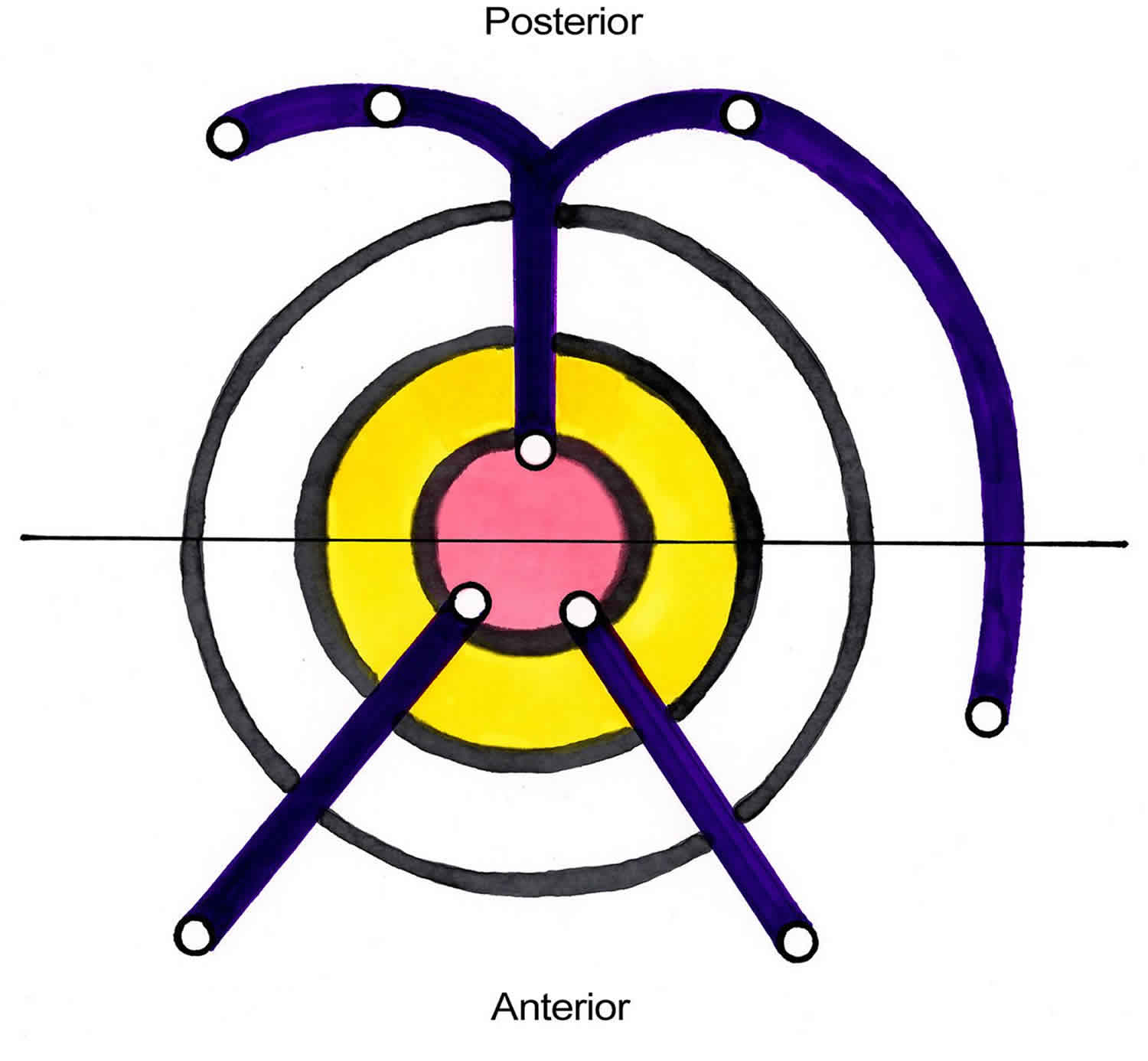
The Goodsall rule can help anticipate the anatomy of a perianal fistula. The Goodsall rule states that perianal fistulas with an external opening anterior to a plane passing transversely through the center of the anus will follow a straight radial course to the dentate line. Fistulas with their openings posterior to this line will follow a curved course to the posterior midline (see the image below). Exceptions to this rule are external openings lying more than 3 cm from the anal verge. These almost always originate as a primary or secondary tract from the posterior midline, consistent with a previous horseshoe abscess 11.
Figure 1. Rectal and anal canal anatomy
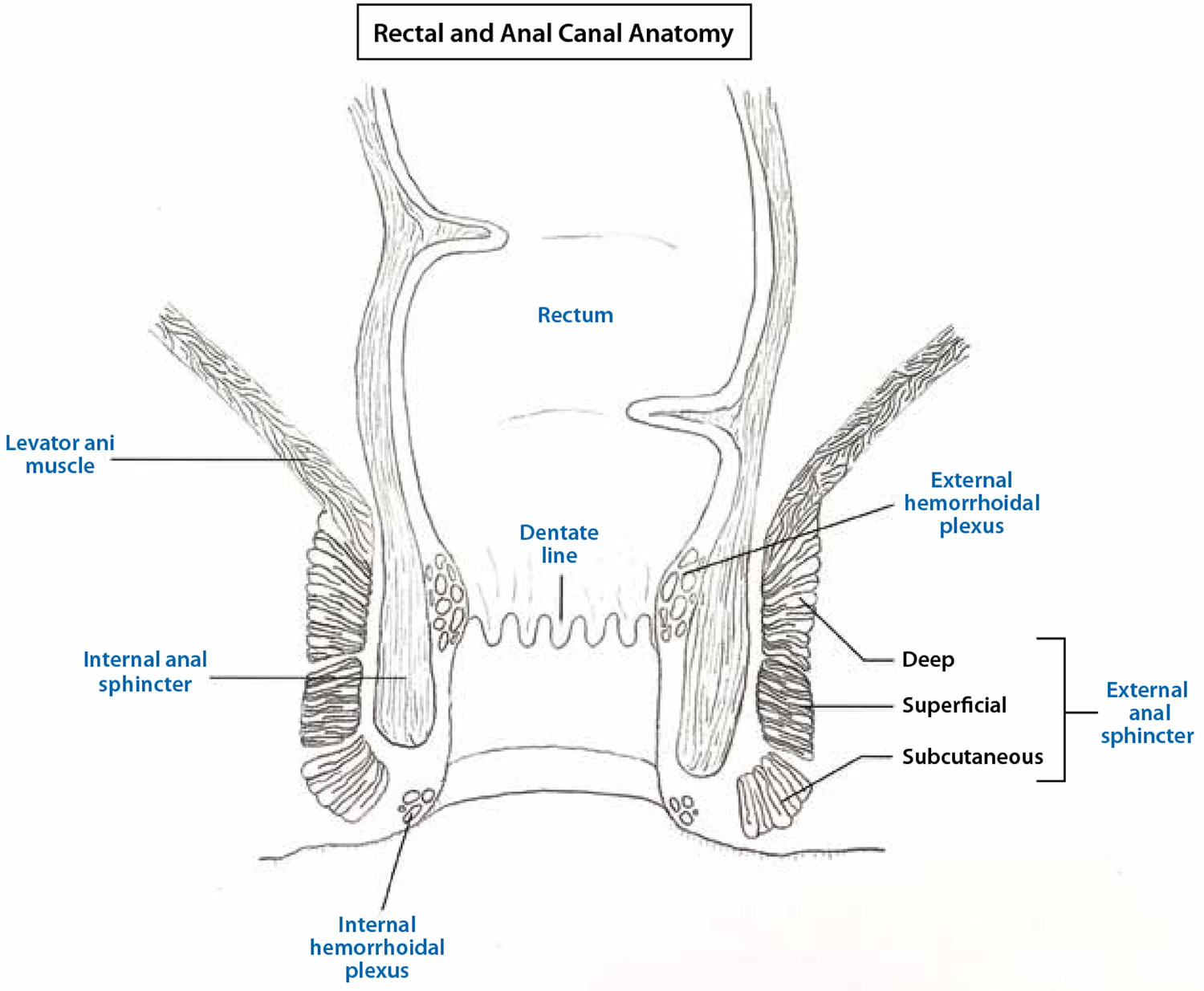
Figure 2. Perianal fistula Goodsall rule
Parks classification system
The classification system developed by Parks, Gordon, and Hardcastle (generally known as the Parks classification) is the one most commonly used for perianal fistula. The Parks classification categorizes perianal fistulas based on their relationship to the external and internal anal sphincters (Figures 1 and 3) 12. The Parks classification system (Figure 3 below) defines four types of perianal fistula or fistula-in-ano that result from cryptoglandular infections, as follows 13:
- Intersphincteric
- Transsphincteric
- Suprasphincteric
- Extrasphincteric
Figure 3. Parks classification of perianal fistula
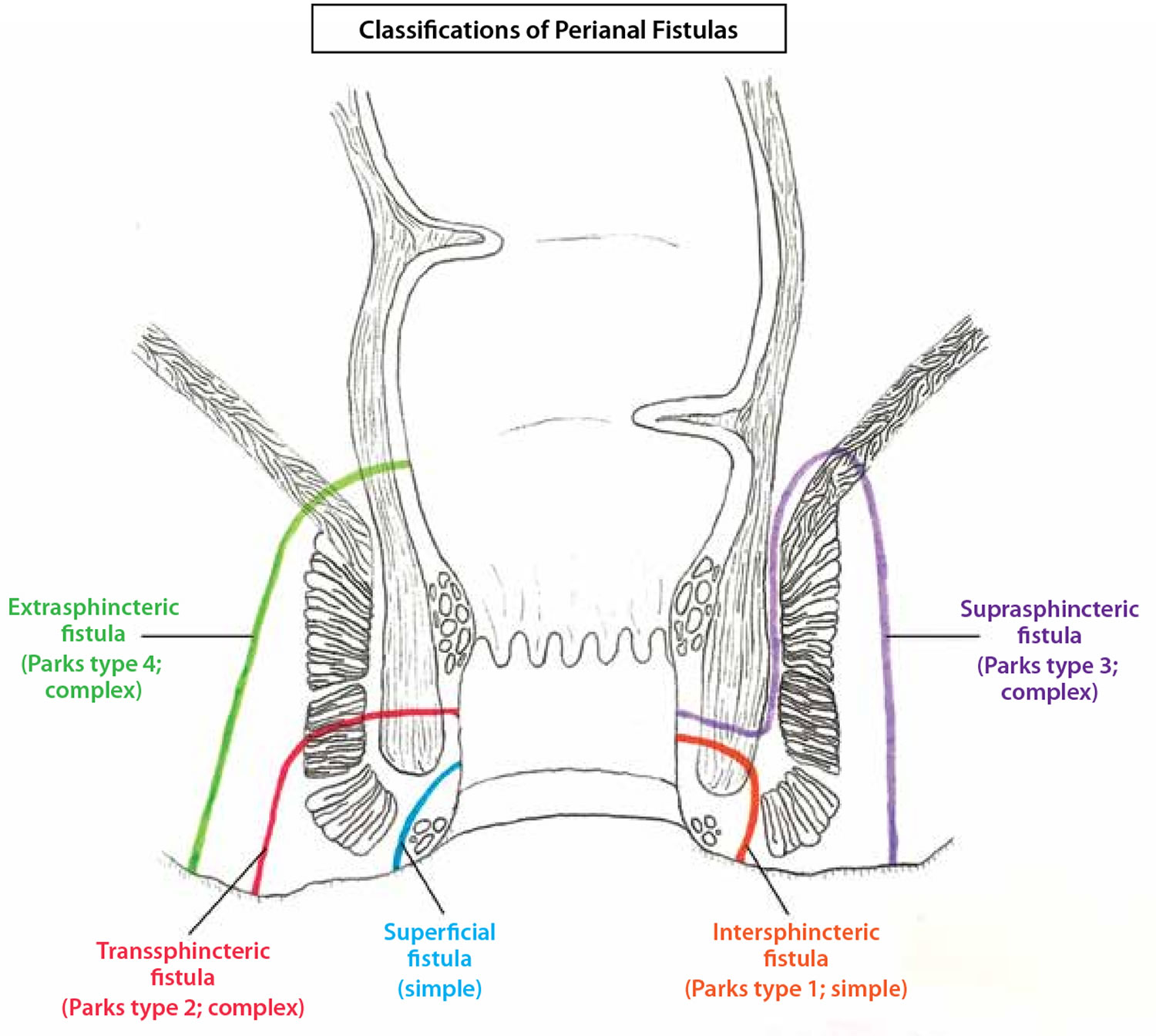
Footnote: The Parks classification of perianal fistulas illustrates a superficial fistula, intersphincteric fistula (type 1), transsphincteric fistula (type 2), suprasphincteric fistula (type 3), and extrasphincteric fistula (type 4) in relation to the internal and external anal sphincter muscles. A revised classification from the American Gastroenterological Association Technical Review Panel defines perianal fistulas as simple or complex.
[Source 7 ]Intersphincteric perianal fistula
Intersphincteric fistulas is one that crosses the internal sphincter and then has a tract to the outside of the anus. Intersphincteric fistulas are the most common type of fistula comprising 50-80% of all cryptoglandular fistulas.
An intersphincteric perianal fistula is characterized as follows:
- Intersphincteric perianal fistula is the result of a perianal abscess
- Common course – It begins at the dentate line, then tracks via the internal sphincter to the intersphincteric space between the internal and external anal sphincters, and finally terminates in the perianal skin or perineum
- Incidence – 70% of all anal fistulas
- Other possible tracts – No perineal opening; high blind tract; high tract to lower rectum or pelvis
Transsphincteric perianal fistula
Trans is a Latin word for “on the other side of.” So a trans-sphincteric fistula is one that crosses to the other side of the external sphincter before exiting in the perianal area and thus involving both the internal and external anal sphincters.
A transsphincteric perianal fistula is characterized as follows:
- In its usual variety, transsphincteric perianal fistula results from an ischiorectal fossa abscess
- Common course – It tracks from the internal opening at the dentate line via the internal and external anal sphincters into the ischiorectal fossa and then terminates in the perianal skin or perineum
- Incidence – 25% of all anal fistulas
- Other possible tracts – High tract with perineal opening; high blind tract
Suprasphincteric perianal fistula
Suprasphincteric fistula tracts travel superior to the external sphincter and cross the puborectal muscle before changing course caudal to their external opening. Accordingly, they pass the internal anal sphincter and the puborectal muscle but spare the external anal sphincter. When these patients typically present with a perirectal abscess, it may not be visible on inspection, but they will have tenderness on the digital rectal exam.
A suprasphincteric perianal fistula is characterized as follows:
- Suprasphincteric perianal fistul arises from a supralevator abscess
- Common course – It passes from the internal opening at the dentate line to the intersphincteric space, tracks superiorly to above the puborectalis, and then curves downward lateral to the external anal sphincter into the ischiorectal fossa and finally to the perianal skin or perineum
- Incidence – 5% percent of all anal fistulas
- Other possible tracts – High blind tract (ie, palpable through rectal wall above dentate line)
Extrasphincteric perianal fistula
Extrasphincteric fistulas often arise in the more proximal rectum rather than the anus and are often a complication of a procedure. Their external opening is in the perianal area and the tract courses superiorly to enter the anal canal above the dentate line.
An extrasphincteric perianal fistula is characterized as follows:
- Extrasphincteric perianal fistula may arise from foreign body penetration of the rectum with drainage through the levators, from penetrating injury to the perineum, from Crohn disease or carcinoma or its treatment, or from pelvic inflammatory disease
- Common course – It runs from the perianal skin via the ischiorectal fossa, tracking upward and through the levator ani muscles to the rectal wall, completely outside the sphincter mechanism, with or without a connection to the dentate line
- Incidence – 1% of all anal fistulas
Current procedural terminology codes classification
Current procedural terminology coding includes the following:
- Subcutaneous
- Submuscular (intersphincteric, low transsphincteric)
- Complex, recurrent (high transsphincteric, suprasphincteric and extrasphincteric, multiple tracts, recurrent)
- Second stage
Unlike the current procedural terminology coding, the Parks and colleagues classification system developed by Parks et al 13 does not include the subcutaneous fistula. These fistulas are not of cryptoglandular origin but are usually caused by unhealed anal fissures or anorectal procedures (eg, hemorrhoidectomy or sphincterotomy).
Perianal fistula causes
In the vast majority of cases, perianal fistula is caused by a previous anorectal abscess. Typically, there are eight to 10 anal crypt glands at the level of the dentate line in the anal canal, arranged circumferentially. These glands penetrate the internal sphincter and end in the intersphincteric plane. They provide a path by which infecting organisms can reach the intramuscular spaces. The cryptoglandular hypothesis states that an infection begins in the anal canal glands and progresses into the muscular wall of the anal sphincters to cause an anorectal abscess.
After surgical or spontaneous drainage in the perianal skin, a granulation tissue–lined tract is occasionally left behind, causing recurrent symptoms. Multiple series have shown that formation of a fistula tract after anorectal abscess occurs in 7-40% of cases 14.
Other fistulas develop secondary to trauma (eg, rectal foreign bodies), Crohn disease, anal fissures, carcinoma, radiation therapy, actinomycoses, tuberculosis, and lymphogranuloma venereum secondary to chlamydial infection.
The incidence of a perianal fistula developing from an anal abscess ranges from 26% to 38% 8. One study showed that the prevalence of perianal fistula is 8.6 cases per 100,000 population. In men, the prevalence is 12.3 cases per 100,000 population, and in women, it is 5.6 cases per 100,000 population. The male-to-female ratio is 1.8:1. The mean patient age is 38.3 years 15.
Perianal fistula symptoms
Patients with perianal fistula commonly have history of a previously drained anal abscess. Symptoms of perianal fistulas include severe anorectal pain, purulent drainage from the perianal skin, irritation of the perianal skin, fecal incontinence and sometimes rectal bleeding.
Signs and symptoms of perianal fistula, in order of prevalence, include the following:
- Perianal discharge
- Anorectal Pain
- Swelling
- Bleeding
- Diarrhea
- Skin excoriation
- External opening
Important points in the patient’s history that may suggest a complex perianal fistula include the following:
- Inflammatory bowel disease
- Diverticulitis
- Previous radiation therapy for prostate or rectal cancer
- Tuberculosis
- Steroid therapy
- HIV infection
A review of symptoms may reveal the following in patients with a perianal fistula:
- Abdominal pain
- Weight loss
- Change in bowel habits
Perianal fistula diagnosis
Most perianal fistulas are diagnosed and managed on the basis of clinical findings. Occasionally, additional studies can assist with the diagnosis or delineation of the fistula tunnel.
Your doctor should observe the entire perineum, looking for an external opening that appears as an open sinus or elevation of granulation tissue. Spontaneous discharge of pus or blood via the external opening may be apparent or expressible on digital rectal examination (DRE).
Digital rectal examination (DRE) may reveal a fibrous tract or cord beneath the skin. It also helps to delineate any further acute inflammation that is not yet drained. Lateral or posterior induration suggests deep postanal or ischiorectal extension.
Doctor should determine the relationship between the anorectal ring and the position of the tract before the patient is relaxed by anesthesia. The sphincter tone and voluntary squeeze pressures should be assessed before any surgical intervention to determine whether preoperative manometry is indicated. Anoscopy is usually required to identify the internal opening. Proctoscopy is also indicated in the presence of rectal disease (eg, Crohn disease or other associated conditions). Most patients cannot tolerate even gentle probing of the fistula tract in the office, and this should be avoided.
No specific laboratory studies are required in the diagnosis of perianal fistula (though the normal preoperative studies are performed, based on age and comorbidities). Instead, physical examination findings remain the mainstay of diagnosis.
Examination under anesthesia
Examination of the perineum, digital rectal examination (DRE), and anoscopy are performed after the anesthesia of choice is administered. This must be done before surgical intervention is initiated, especially if outpatient evaluation causes discomfort or has not helped to delineate the course of the fistulous process.
Several techniques have been described to help locate the course of the fistula and, more important, identify the internal opening. They include the following:
- Inject hydrogen peroxide, milk, or dilute methylene blue into the external opening and watch for egress at the dentate line; in the authors’ experience, methylene blue often obscures the field more than it helps identify the opening
- Traction (pulling or pushing) on the external opening may also cause a dimpling or protrusion of the involved crypt
- Insertion of a blunt-tip crypt probe via the external opening may help to outline the direction of the tract; if it approaches the dentate line within a few millimeters, a direct extension likely existed (care should be taken to not use excessive force and create false passages)
Proctosigmoidoscopy/colonoscopy
Rigid sigmoidoscopy can be performed at the initial evaluation to help rule out any associated disease process in the rectum. Further colonic evaluation is performed only as indicated.
Imaging studies
Radiologic studies are not performed for routine fistula evaluation, because in most cases, the anatomy of a perianal fistula can be determined in the operating room. However, such studies can be helpful when the primary opening is difficult to identify or when recurrent or persistent disease is present. In the case of recurrent or multiple fistulas, such studies can be used to identify secondary tracts or missed primary openings 16. Several imaging diagnostic modalities are available to evaluate perianal fistula. The efficacy of each modality is reviewed.
Fistulography
This technique involves injection of contrast via the internal opening, which is followed by anteroposterior, lateral, and oblique radiographic images to outline the course of the fistula tract.
Fistulography is relatively well tolerated but it can be painful when injecting the contrast material into the fistulous tract. It requires the ability to visualize the internal opening. Questions have been raised about its accuracy, which has been reported to range from 16% to 48% 17.
Because of these limitations, fistulography is generally reserved for cases in which there is a concern about a fistulous connection between the rectum and adjacent organs such as the bladder, where it may be slightly more useful than a careful examination under anesthesia.
Endoanal or endorectal ultrasonography
Endoanal or endorectal ultrasonography involves the passage of a 7- or 10-MHz ultrasound transducer into the anal canal to help define the muscular anatomy and thereby help differentiate intersphincteric from transsphincteric lesions. A standard water-filled balloon transducer can facilitate evaluation of the rectal wall for any suprasphincteric extension.
Investigations have shown that the addition of hydrogen peroxide via the external opening can aid in outlining the course of the fistula tract. This may be useful for helping to identify missed internal openings.
Endoanal/endorectal ultrasonography has been reported to be 50% better than physical examination alone in helping to detect an internal opening that is difficult to localize. This modality has not been used widely for routine clinical fistula evaluation 18.
Magnetic resonance imaging
Findings on magnetic resonance imaging (MRI) show 80-90% concordance with operative findings when a primary tract course and secondary extensions are observed. MRI is becoming the study of choice for the evaluation of complex fistulas and recurrent fistulas. It has been shown to reduce recurrence rates by providing information on otherwise unknown extensions 19.
Computed tomography
Computed tomography (CT) is more helpful in the setting of perirectal inflammatory disease than in the setting of small fistulas because it is better for delineating fluid pockets that require drainage than for delineating small fistulas. CT requires administration of oral and rectal contrast. Muscular anatomy is not well delineated.
Barium enema/small bowel series
These studies may be useful for patients with multiple fistulas or recurrent disease to help rule out inflammatory bowel disease.
Anal manometry
Anal manometry is rarely used in the evaluation of patients with fistula-in-ano. However, pressure evaluation of the sphincter mechanism is helpful in certain patients for operative planning, including the following:
- Patients in whom decreased tone is observed during preoperative evaluation
- Patients with a history of previous fistulotomy
- Patients with a history of obstetrical trauma
- Patients with a high transsphincteric or suprasphincteric fistula (if known)
- Very elderly patients
If a decrease in pressure is found, surgical division of any portion of the sphincter mechanism should be avoided.
Perianal fistula treatment
Therapeutic intervention is indicated for symptomatic patients. Symptoms usually involve recurrent episodes of anorectal sepsis. An abscess develops easily if the external opening on the perianal skin seals itself.
Crohn disease of the perineum with multiple and often complex fistulas requires careful surgical treatment. Acute perianal abscess requires incision and drainage. Definitive repair of fistulas in these patients requires that the intra-abdominal disease be under control with medical therapy. If the disease is controlled, routine therapy is warranted. Recurrent fistulous disease to the rectum and perineum with persistent anorectal sepsis is an indication for panproctocolectomy.
Studies have identified a role in Crohn disease for fistula therapy with infliximab, with 50-60% response rates for perianal fistulas 20. Adipose-derived stem-cell therapy is currently being studied for use in the treatment of Crohn fistula and other complex fistulas 21.
If patients are without symptoms and a fistula is found during a routine examination, no therapy is required.
Surgery for fistula-in-ano should not be performed for definitive repair of the fistula in the setting of anorectal abscess (unless the fistula is superficial and the tract is obvious). In the acute phase, simple incision and drainage of the abscess are sufficient 22. Only 7-40% of patients will develop a fistula. Recurrent anal sepsis and fistula formation are twofold higher after an abscess in patients younger than 40 years and are almost threefold higher in nondiabetics.
Preoperative considerations include the following:
- Rectal irrigation with enemas should be performed on the morning of the operation
- Anesthesia can be general, local with intravenous sedation, or a regional block
- Administer preoperative antibiotics
- The prone jackknife position with buttocks apart is the most advantageous position
Intraoperative considerations include the following:
- Examine the patient under anesthesia to confirm the extent of the fistula
- Identifying the internal opening to prevent recurrence is imperative
- A local anesthetic block at the end of the procedure provides postoperative analgesia
Medical management
Antibiotics
Traditionally, antibiotics such as metronidazole and ciprofloxacin have been used as first-line therapy for patients with fistulizing Crohn’s disease, although data supporting their efficacy are limited to small studies 23. In one of the initial studies evaluating metronidazole use, 56% of patients had fistula closure after 6 to 8 weeks of therapy 24. Although this study suggested that metronidazole is effective at inducing fistula closure, recurrence rates with antibiotic therapy are high. Brandt and colleagues 25 studied metronidazole use in patients with perianal fistulas and found that only 28% of patients who had fistula healing were able to successfully discontinue therapy without recurrence.
However, long-term use of antibiotics is associated with significant morbidity, making continued therapy less feasible 25. No clinical guidelines on antibiotic selection exist, but ciprofloxacin has been shown to have higher rates of clinical improvement and complete fistula closure when compared to metronidazole, although the difference did not reach significance 26. In addition to systemic therapy, the use of topical antibiotic ointments or creams for patients with perianal Crohn’s disease has been investigated. A randomized trial 27 assessing the use of metronidazole topical ointment reported an improvement in pain and drainage from the fistula tract.
Although the use of antibiotics as long-term monotherapy for perianal Crohn disease is not ideal, studies have evaluated the efficacy of metronidazole or ciprofloxacin as adjuvant therapy with immunomodulators or biologic agents. In a prospective, open-label study looking at fistula closure, combination therapy of metronidazole and/or ciprofloxacin with azathioprine (AZA) was significantly more effective at achieving a clinical response (48%) when compared to metronidazole and/or ciprofloxacin alone (15%) 28. Furthermore, a double-blind, placebo-controlled study demonstrated that patients treated with infliximab (Remicade) and ciprofloxacin tended to have a better clinical response than patients treated with infliximab and a placebo 28. Similarly, Dewint and colleagues evaluated the use of ciprofloxacin in combination with adalimumab (Humira) for patients with Crohn disease and found a clinical response in 71% of patients treated with adalimumab and ciprofloxacin compared with 47% of patients treated with adalimumab and placebo 29. These studies suggest that although antibiotics are not useful for long-term monotherapy, they can be effective as a bridge or as adjuvant therapy when combined with immunomodulators or biologic agents.
Plugs and adhesives
Advances in biotechnology have led to the development of many new tissue adhesives and biomaterials formed as fistula plugs. By their less-invasive nature, these therapies lead to decreased postoperative morbidity and risk of incontinence, but long-term data are lacking for eradication of disease, especially in complex fistulas, which carry high recurrence rates 30.
Reported series exist of fibrin glue treatment of fistula-in-ano, with 1-year follow-up showing recurrence rates approaching 40-80% 31. The Surgisis fistula plug has also had mixed long-term results in direct clinical trials 32.
Early success rates have been reported for newer materials, such as acellular dermal matrix and the bioabsorbable Gore Bio-A fistula plug, in low fistulas and good animal model data 33. Assessment of long-term success rates with plug techniques for complex disease will be based on further data from randomized trials.
In a randomized, controlled study designed to evaluate the efficacy and safety of the anal fistula plug in patients with fistulizing anoperineal Crohn disease, Senéjoux et al 34 did not find the plug to be superior to seton removal for achieving fistual closure, regardless of whether the fistula was simple or complex.
A combined sphincter-sparing repair that includes both an anal fistula plug and a rectal advancement flap has been proposed for the treatment of transsphincteric perianal fistula 35.
Perianal fistula surgery
Fistulotomy
The laying-open technique (fistulotomy) is useful for 85-95% of primary fistulas (ie, submucosal, intersphincteric, and low transsphincteric) 36.
A probe is passed into the tract through the external and internal openings. The overlying skin, subcutaneous tissue, and internal sphincter muscle are divided with a knife or electrocautery, and the entire fibrous tract is thereby opened.
At low levels in the anus, the internal sphincter and subcutaneous external sphincter can be divided at right angles to the underlying fibers without continence being affected. This is not the case if the fistulotomy is performed anteriorly in female patients. If the fistula tract courses higher into the sphincter mechanism, seton placement should be performed. Curettage is performed to remove granulation tissue in the tract base.
Opening the wound out on the perianal skin for 1-2 cm adjacent to the external opening with local excision of skin promotes internal healing before external closure. Some advocate marsupialization of the edges to improve healing times. Perform a biopsy on any firm, suggestive tissue.
Complete fistulectomy creates larger wounds that take longer to heal and offers no recurrence advantage over fistulotomy.
Figure 4. Fistulotomy
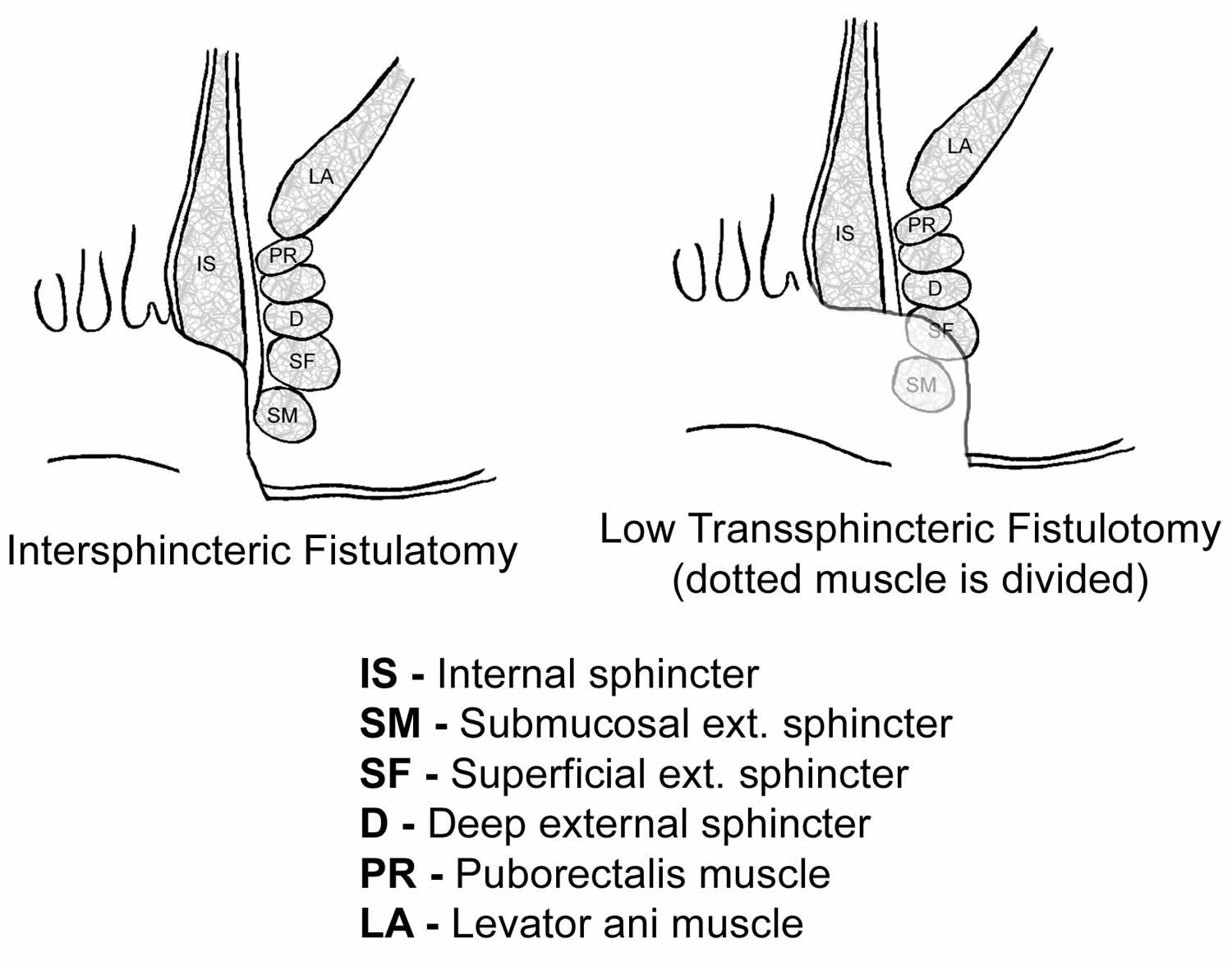 Footnote: Schematic of intersphincteric and low transsphincteric fistulotomy
Footnote: Schematic of intersphincteric and low transsphincteric fistulotomySeton placement
A seton can be placed alone, combined with fistulotomy, or in a staged fashion. This technique is useful in patients with the following conditions 37:
- Complex fistulas (ie, high transsphincteric, suprasphincteric, extrasphincteric) or multiple fistulas
- Recurrent fistulas after previous fistulotomy
- Anterior fistulas in female patients
- Poor preoperative sphincter pressures
- Patients with Crohn disease or patients who are immunosuppressed
Beyond giving a visual identification of the amount of sphincter muscle involved, the purposes of setons are to drain, to promote fibrosis, and to cut through the fistula. Setons can be made from large silk suture, silastic vessel markers, or rubber bands that are threaded through the fistula tract.
Single-stage seton (cutting)
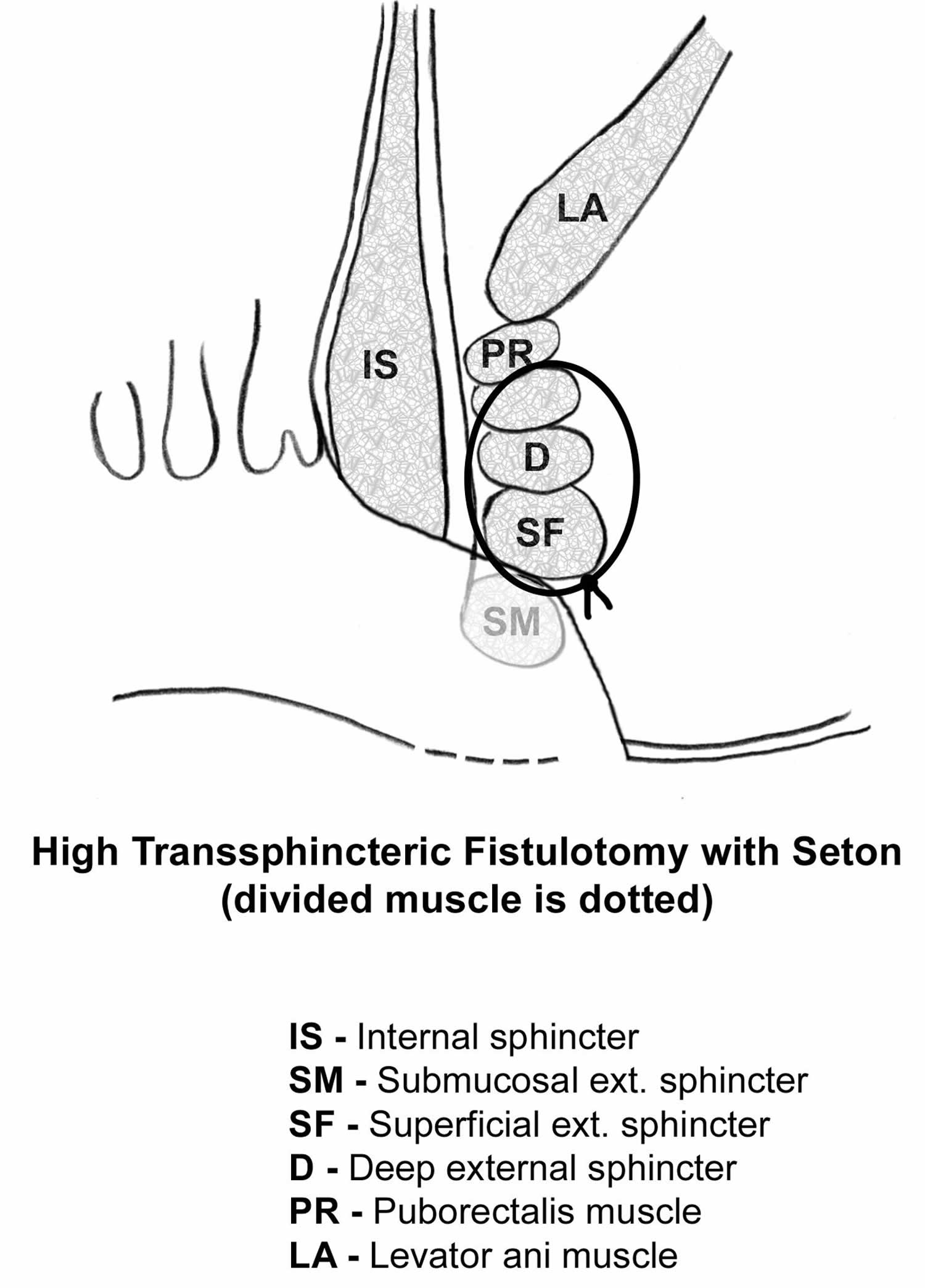
Pass the seton through the fistula tract around the deep external sphincter after opening the skin, subcutaneous tissue, internal sphincter muscle, and subcutaneous external sphincter muscle. The seton is tightened down and secured with a separate silk tie.
With time, fibrosis occurs above the seton as it gradually cuts through the sphincter muscles and essentially exteriorizes the tract. The seton is tightened on subsequent office visits until it is pulled through over 6-8 weeks. A cutting seton can also be used without associated fistulotomy.
Recurrence and incontinence are important factors to consider when this technique is employed. The success rates for cutting setons range from 82-100%; however, long-term incontinence rates can exceed 30% 38.
Figure 5. High transsphincteric fistulotomy with seton
Two-stage seton (draining/fibrosing)
Pass the seton around the deep portion of the external sphincter after opening the skin, subcutaneous tissue, internal sphincter muscle, and subcutaneous external sphincter muscle.
Unlike the cutting seton, the seton is left loose to drain the intersphincteric space and to promote fibrosis in the deep sphincter muscle. Once the superficial wound is healed completely (2-3 months later), the seton-bound sphincter muscle is divided.
Two studies (74 patients combined) supported the two-stage approach with a 0-nylon seton. Once wound healing is complete, the seton is removed without division of the remaining encircled deep external sphincter muscle. The researchers reported eradication of the fistula tract in 60-78% of cases.
Mucosal advancement flap
A mucosal advancement flap is reserved for use in patients with chronic high fistula but is indicated for the same disease process as seton use 39. Advantages include a one-stage procedure with no additional sphincter damage. A disadvantage is poor success in patients with Crohn disease or acute infection.
This procedure involves total fistulectomy, with removal of the primary and secondary tracts and complete excision of the internal opening.
A rectal mucomuscular flap with a wide proximal base (two times the apex width) is raised. The internal muscle defect is closed with an absorbable suture, and the flap is sewn down over the internal opening so that its suture line does not overlap the muscular repair.
LIFT Procedure
The ligation of the intersphincteric fistula tract (LIFT) procedure is a treatment for fistulas that pass through the anal sphincter muscles, where a fistulotomy would be too risky. During the treatment, a cut is made in the skin above the fistula and the sphincter muscles are moved apart. The fistula is then sealed at both ends and cut open so it lies flat.
This procedure has had some promising results so far, but it’s only been around since 2007 40, so more research is needed to determine how well it works in the short and long term.
Three randomized controlled trials have been reported ligation of the intersphincteric fistula tract (LIFT) procedure 41, 42, 43. One only compared LIFT with a modification of LIFT, rather than a standard treatment, whilst the other two compared LIFT with a mucosal advancement flap. In addition, 18 case series have been reviewed 44.
Madbouly et al. 43 randomized 70 patients to either LIFT or a mucosal advancement flap. Primary healing was achieved in 33 (94%) patients undergoing LIFT compared with 32 (91%) patients undergoing a flap repair. Median healing times were 22.6 and 32.1 days, respectively. After follow-up of 1 year, a successful outcome was achieved in 26 (74%) of the LIFT group compared with 20 (66%) in the advancement flap group, highlighting the importance of long-term follow up in fistula surgery research. There was no significant difference in continence scores in this study.
A similar, but smaller, study randomized 25 patients to LIFT and 14 to anorectal advancement flap 41. All patients had seton inserted prior to definitive surgery. Recurrences were seen in 2/25 and 1/14, respectively. The authors concluded that LIFT was simple and safe, took significantly less time than a flap and patients returned to work earlier.
Sileri et al. 45 reported 26 patients with complex fistulas, 19 of whom were healed at a minimum of 16 months following LIFT. The recurrences occurred between 4 and 8 weeks following surgery. They defined ‘complex’ as any track that was deeper than 30% of the external sphincter, anterior fistula in women, recurrent fistula or preexisting incontinence. Only two patients had previously had a loose seton inserted prior to the LIFT procedure. Another series of 40 patients with transsphincteric fistulas deemed to be inappropriate for fistulotomy underwent LIFT 46. Success rates of up to 74% were noted, although follow-up was short (a mean of 18 weeks).
Ooi et al. 47 reported 25 patients who had undergone LIFT. Ten of them had developed recurrence after previous fistula surgery. The primary and secondary end-points were cure rate and degree of incontinence, respectively. Primary healing was observed in 17 (68%) patients at a median of 6 weeks. Seven patients had recurrence of their fistula, which presented between 7 and 20 weeks’ postoperatively. There was no reported incontinence. Liu et al. 48 recruited 38 patients between 2008 and 2011. At a median follow-up of 26 months (26 patients had at least 12 months’ follow-up), healing was seen in 23/38 (61%). One failure occurred over 12 months after the index procedure, with 80% of failures occurring within the first 6 months following the procedure. No intra-operative complications or incontinence were noted. Increasing fistula length was associated with decreased likelihood of healing.
A recent large series (167 patients) reported a success rate (healing) of 94% at a median follow-up of 12 months 49. The majority of fistulas were transsphincteric 50 and a number were recurrent 51. Ten patients who developed a recurrent fistula were managed with a repeat LIFT procedure. Schulze et al. 52 performed LIFT on 75 patients between May 2008 and June 2013. All had undergone an initial procedure that involved drainage of sepsis, insertion of a loose seton and partial fistulotomy. There were nine recurrences, at a mean follow-up of 14.6 months, all of which were treated with repeat LIFT and biograft or anorectal advancement flap. There were no subsequent recurrences. Recurrences were related to fistulas with multiple tracks. Only one patient reported a change in continence.
An attempt has been made to determine whether LIFT is more effective in distinct fistula sub-types 53. LIFT was performed in simple transsphincteric (five), complex fistulae (six) and recurrent cases postfistulotomy (six). The overall success rate at a mean follow-up of 11 months was 53%. Healing rates in the three groups were four out of five, three out of six and two out of six, respectively. These numbers are too small to draw any conclusions, but intuitively LIFT should be more likely to succeed in less complicated fistulas (as is the case for all fistula treatments). There is general consensus that the presence of multiple tracks, diabetes mellitus, perianal collections and long tracks are all associated with a higher chance of failure of LIFT.
LIFT has been employed as an alternative to fistulotomy in patients with low transsphincteric fistulas 54. Healing was seen in 18/22 patients recruited at a median follow-up of 19.5 months. The four unsuccessful cases were treated with fistulotomy. Although there was no comparison with patients with similar fistulas undergoing fistulotomy as sole treatment, the authors reported a final healing rate of 100% and no alteration in continence, which was assessed prospectively.
A Chinese group recently reported on 43 patients with ‘complex’ fistulas treated by LIFT, all of whom were followed up for more than 1 year 55. Healing of the fistula was seen in 36 of 43 (84%) patients; failure, when seen, occurred a mean of 8.6 weeks after the original procedure. In this series, eight patients had dehiscence or infection at the site of the intersphincteric wound, with five patients requiring laying open. This complication is probably commoner than reported in many series.
Modifications to the LIFT procedure have been described. The Bio-LIFT procedure, for example, involves placing a biograft (usually a piece of collagen mesh) in the intersphincteric space following ligation of the intersphincteric fistula track. Success was reported in 11 of 16 (63%) fistulas treated, at a median follow-up of 26 weeks 56. A randomized trial comparing the two approaches in 235 patients reported healing rates at 6 months of 94% in the LIFT + biograft group, vs 84% in the LIFT group alone 42. The authors reported that the addition of the graft had the advantage of higher healing rates, decreased healing time and a lower early postoperative pain score. Another modification involves making a lateral incision from the external opening to the intersphincteric groove, ligating the fistula track within the intersphincteric space and complete excision of the external part of the fistula 57. In a series of 39 patients treated in this way and followed for a mean of 15 months, 34 (87%) achieved healing. There was no change in continence, as measured by the Cleveland Clinic score preoperatively and at 6 months postoperatively. An alternative approach is to de-roof the fistula from internal opening to intersphincteric groove and ligate the fistula track, while at the same time preserving the external sphincter. This modified LIFT was performed on a series 56 patients, with an overall cure rate of 71%. True recurrence (5%) was much less frequent than simple failure of the technique and persistence of an active fistula track after the operation 58.
LIFT has been used as treatment for recurrent fistulas 59. Fifteen patients with recurrent transsphincteric fistulas were followed up for 8–26 months (median 13.5 months). At the end of follow-up, six patients still had evidence of fistula, either persistence of the original fistula (four patients) or recurrence (two patients). LIFT has also been used in selected patients with Crohn’s disease, with 8 of 12 reported to be healed at 12 months 60.
To conclude, to date there are a few randomized studies as well as number of case series that attest to the potential efficacy of LIFT. LIFT appears to be associated with less functional compromise than some traditional treatments of transsphincteric fistulas, although recurrence/persistence rates are probably similar. One of the advantages of the LIFT procedure is that of secondary success. Where a genuine downstaging of the fistula from transsphincteric to intersphincteric takes place in a proportion of failures, allowing laying open of this intersphincteric fistula, preserving the external sphincter which would have been involved originally 61. Future work should focus on comparison with standard treatments, paying particular attention to comparing similar fistulas and focusing on deeper fistulas, where conventional treatments may be more problematic as regards functional outcome.
Diversion
In rare cases, the creation of a diverting stoma may be indicated to facilitate the treatment of a complex persistent fistula-in-ano. The most common indications include, but are not limited to, patients with perineal necrotizing fasciitis, severe anorectal Crohn disease, reoperative rectovaginal fistulas, and radiation-induced fistulas. Fecal diversion alone is effective in these select patients to control sepsis and symptoms; however, long-term success rates after reanastomosis are low because of recurrence from the underlying disease. Thus, this approach should be avoided unless the underlying fistula-in-ano disease process is repaired or has healed completely, which is unlikely.
Perianal fistula surgery complications
Early postoperative complications may include the following:
- Urinary retention
- Bleeding
- Fecal impaction
- Thrombosed hemorrhoids
Delayed postoperative complications may include the following:
- Recurrence
- Incontinence (stool)
- Anal stenosis – The healing process causes fibrosis of the anal canal; bulking agents for stool help to prevent narrowing
- Delayed wound healing – Complete healing occurs by 12 weeks unless an underlying disease process is present (ie, recurrence, Crohn disease)
Postoperative rates of recurrence and incontinence vary according to the procedure performed, as follows:
- Standard fistulotomy – The reported rate of recurrence is 0-18%, and the rate of any stool incontinence is 3-7%
- Seton use – The reported rate of recurrence is 0-17%, and the rate of any incontinence of stool is 0-17%
- Mucosal advancement flap – The reported rate of recurrence is 1-17%, and the rate of any incontinence of stool is 6-8% 62
Novel techniques
A number of novel surgical techniques for anal fistulas have been developed over the last 10 years. These include the LIFT procedure, lasers, clips, video-assisted anal fistula treatment (VAAFT) and autologous adipose-derived stem cells. Evidence of efficacy is scant and largely confined to personal series (Level III evidence) with a paucity of randomized controlled trials performed to date, and what is available is confined to the LIFT procedure. Whilst initial work on other techniques looks interesting, with minimal adverse events reported, long-term follow-up needs to be reported as many institutional series only document short/medium follow-up, functional outcome data are limited and few patient-reported outcome data are available. A degree of standardization is required in approaches using multiple concurrent treatments. Randomized evidence is needed before these new techniques will challenge conventional approaches.
Fibrin glue
Treatment with fibrin glue is currently the only non-surgical option for anal fistulas. It involves the surgeon injecting a glue into the fistula while you’re under a general anesthetic. The glue helps seal the fistula and encourages it to heal.
It remains uncertain as to which fistulas are suitable for fibrin glue treatment. Success (fistula healing) is low when the fistula track is short. Treatment with fibrin glue is generally less effective than fistulotomy for simple fistulas and the results may not be long-lasting, but it may be a useful option for fistulas that pass through the anal sphincter muscles because they do not need to be cut.
With variable and mostly low rates of healing, fibrin glue is not recommended for routine use in anal fistulas, but may be considered where other surgical options are not feasible 44.
Various autologous and commercial preparations of fibrin glue have been used to treat anal fistulas. Autologous glues are formed from the patient’s own blood, whilst commercially available glues are a mixture of clotting factors, aprotinin and calcium (Beriplast; CSL Behring, Pennsylvania, USA; Tisseel; Baxter Healthcare, Deerfield, Illinois, USA), or are synthetic glues, such as cyanoacrylate (Glubran; GEM SRL, Viareggio, Italy). The glues are applied to fill the fistula track and provide a bridge for fibroblasts and stromo-vascular cell in-growth to produce healing. Their ease of use, minimal risk to continence and repeatability make them an attractive option, especially in patients at high risk of sphincter dysfunction 50, 63.
A wide range of healing rates with fibrin glues have been reported, ranging from 14% to 94% 64, 65. Variability in disease complexity, fistula anatomy and surgical technique makes comparison of the results from randomized trials difficult to interpret 66. A meta-analysis has not shown any statistical difference with the use of fibrin glue, compared to other conventional surgical treatments, in terms of fistula recurrence or incontinence 67.
Some authors have reported better healing rates in longer tracks, suggesting that shorter tracks (< 3.5 cm) are less likely to retain the glue 68, but this has been contradicted in other reports 69, 70. Technical errors have been suggested for failure, including inadequate curettage and washout to remove all infected and epithelialized tissue 155, 161, 162, or incomplete filling of the track with the glue to ensure occlusion 68.
Like other fistula treatments, recurrence rates with fibrin glue increase with the length of follow-up. A long-term follow-up study showed that up to 26% of patients who were symptom free at 6 months went on to develop recurrence at an average of 4.1 years 71. However, on several occasions the recurrence was at a different site, suggesting that a new fistula had formed. The highest probability of failure appears to occur in the first 6 months following treatment, so 6 months should be the minimum follow up period 72.
A multicentre trial randomized patients to fibrin glue or seton treatment for transsphincteric fistulas and showed a 38% healing rate in the fibrin glue group, compared with 87% in the seton group 50. Patients who had a recurrence after fibrin glue were further randomized to repeat glue treatment or a loose seton. A further 50% healed with repeat glue treatment. Notably, there was a significant worsening in the Cleveland Clinic continence score in the seton group. Many studies have investigated the use of repeat glue application to increase healing rates, even up to four applications 73. A prospective study of fibrin glue for simple transsphincteric and intersphincteric fistulas showed that repeat glue treatment decreased the overall recurrence rate from 23% to 7.6% 74. Conversely, other authors have reported that repeated applications of fibrin glue are unlikely to succeed 75 and other studies have shown an adverse outcome when fibrin glue is combined with an endorectal advancement flap 76.
Various strategies have been suggested to improve the healing rates with glues. Local sepsis should be eradicated with the use of preoperative setons, the track should be thoroughly curetted and the track irrigated with either saline or hydrogen peroxide. Preoperative bowel preparation has not consistently shown a benefit. Suturing the internal or external openings shut has been advocated, but not shown to confer a significant benefit 64.
It has been suggested that high failure rates with the glue may be a consequence of the glue not being retained in the fistula track 77. To overcome this, some authors have recommended the use of stool softeners and avoiding straining and exercise in the postoperative period, although there are no data to support this. Other explanations for failure of fibrin glue include early resorption/degradation within 5–10 days of application, providing insufficient time for established healing 78, 79. A Phase 1 trial using Permacol® glue, which incorporates fibres suspended in fibrin glue to provide a physical scaffold for host cell proliferation after glue absorption, has shown promising results, but more, randomized, data are required 79. Newer autologous fibrin sealants have not shown any increased efficacy compared with conventional glues, with healing rates of up to 40% 80. Research continues into the use of stem cell autologous suspensions for fistula application and the ADMIRE CD study used fibrin glue as the scaffold for allogeneic mesenchymal stem cell treatment of Crohn’s anal fistulas 81. This may represent the main role for fibrin glue in the future.
Bioprosthetic plug
Another option is the insertion of a bioprosthetic plug. This is a cone-shaped plug made from animal tissue that’s used to block the internal opening of the fistula and preventing fecal material from entering. Anal fistula plugs procedure works well for blocking an anal fistula and there are no serious concerns about its safety. Anal fistula plugs provide a physical scaffold for in-growth of host regenerative and immune cells to promote healing and repair. The plugs degrade over a period of several weeks, by which time the repair process is established.
Accepting that rates of healing are variable, an anal fistula plug is an option for treating transsphincteric fistulas, especially where surgical options are considered to have a significant risk of jeopardizing continence. The additional cost of the plug should be taken into account when considering this surgical treatment. The initial reported high success rates of anal fistula plugs have not been maintained in later series, but, similar to fibrin glue, anal fistula plugs do not threaten continence. It remains uncertain as to which fistulas are best suited to fistula plug treatment.
Types of bioprosthetic plug
Several fistula plugs have been developed commercially, but the BioDesign Surgisis® Anal Fistula Plug (Cook Medical, Bloomington, Indiana, USA), composed of acellular, lyophilized porcine intestinal submucosa, is the most established 44. Other plugs include the GORE Bio A® Fistula Plug (Flagstaff, Arizona, USA), a composite of polyglycolic acid and trimethylenecarbonate synthetic polymers 174, which has now been withdrawn by the manufacturer, the Pressfit® plug (Deco Med s.r.l., Venice, Italy), which is made from acellular dermal matrix, and the Curaseal AF® device (CuraSeal, Inc., Santa Clara, California, USA), which incorporates a silicone disc to reinforce occlusion of the internal fistula opening. Secure anchoring of the plug at the internal opening is a critical feature in the design of all these plugs.
Reported success rates for fistula healing with anal fistula plugs vary, ranging from 24% to 88% 175, reflecting differences in patient selection, plugs used, surgical technique, definition of healing and length of follow-up. In 2007, a Consensus Conference was held to establish uniformity in the indications and techniques for insertion of the Cook Medical fistula plug 82. It concluded that all types of ano-cutaneous fistula were suitable for plug treatment, with transsphincteric fistulas being the ideal indication. Emphasis was placed on the prior control of associated sepsis and the use of seton drainage for 6–12 weeks preoperatively. Debridement or curettage of the track was discouraged, although gentle brushing to de-epithelialize the track was subsequently recommended, with saline or hydrogen peroxide irrigation being optional. Secure suturing of the plug to the internal opening/internal sphincter was considered important to prevent early extrusion of the plug, which had been reported as a cause for failure in some studies 83. There was no evidence to support the routine use of a rectal mucosal flap to cover the plug. Suturing of the plug has been facilitated by modification of the original plug design to incorporate an internal ‘button’.
Initial encouraging results from Johnson et al. 84 reporting closure rates of up to 87% have not been reproduced in later studies, which have presented mixed results. A randomized trial comparing the fistula plug with endorectal advancement flap (ERAF) was closed prematurely due to a high incidence of recurrence in the plug arm 85. In another randomized controlled trial, comparing an acellular dermal matrix (ADM) plug vs fistula plug with endorectal advancement flap (ERAF), a healing rate of 82% was reported in the ADM group, with lower rates of recurrence (ADM plug 4% vs ERAF 28%) 86. A subsequent meta-analysis comparing the plug with endorectal advancement flap (ERAF) failed to show any difference in recurrence rates or complications 87. However, a recent robust multicentre randomized controlled trial of 94 patients with a transsphincteric fistula demonstrated clinical healing at 12 months in only 38% (15 of 44 patients) treated by collagen plug, compared with 66% (27 of 41 patients) treated by endorectal advancement flap (ERAF) 88.
A potential disadvantage with the plug is the cost of the device, but this may be offset by a shorter hospital stay. In a study comparing fistula plug against endorectal advancement flap (ERAF), healing rates were similar, but the costs associated with endorectal advancement flap (ERAF) were higher due to a longer duration of hospital stay 89.
In a recent UK multicentre study (the NIHR FIAT trial) 152 patients were randomized to receive the Cook Biodesign fistula plug and compared with 152 patients receiving surgeon’s preference [cutting seton, ERAF, fistulotomy or ligation of intersphincteric fistula track (LIFT)] 90. Similar clinical fistula healing rates were observed at 12 months’ follow-up (plug 54% vs surgeon’s preference 57%) 90. Early plug extrusion remained a problem, despite the adoption of best surgical technique, occurring in 15% of cases. Rates of incontinence were low in both groups and there was no statistical difference in quality of life as measured by the Faecal Incontinence Quality of Life (FIQoL) and EQ-5D scoring systems. Complications rates were similar between the two groups, with the exception of increased early postoperative pain in the plug group, presumably associated with suturing to the internal anal sphincter.
The fistula plug has been successfully used in combination with other procedures, including the LIFT procedure. In a large, multicentre RCT, the LIFT–plug procedure was found to result in statistically significant higher healing rates compared with LIFT alone (LIFT–plug 94.0% vs LIFT 83.9%) 42.
Most studies have included variable follow-up after surgery, ranging from 3 to 12 months. A long-term follow-up study, using MRI to assess fistula healing at 12 months after plug insertion, showed radiological evidence of a persistent fistula in up to 21% of patients, suggesting that reports of fistula healing at 12 months are likely to be an overestimate 91.
Benefits in favor of the fistula plug include ease of use and lack of complications. No differences in complication rates have been reported between ERAF and AFP 87, with documented complications including sepsis/abscess, recurrence and constipation 42. Unlike some other techniques, no study has reported a detrimental effect to continence following use of a plug. Thus, the fistula plug is an option for treating a transsphincteric fistula. Uncertainty in healing efficacy is counterweighed by the lack of detrimental effect on continence. The cost of the device might be offset by shorter lengths of hospital stay.
Endoscopic ablation
In this procedure, an endoscope (a tube with a camera on the end) is put in the fistula. An electrode is then passed through the endoscope and used to seal the fistula.
Endoscopic ablation works well and there are no serious concerns about its safety.
Laser surgery
Radially emitting laser fiber treatment involves using a small laser beam to seal the fistula. There are uncertainties around how well it works, but there are no major safety concerns.
Laser therapy was described as a treatment option for anal fistula in the 1980s 92 and more recently with a radial emitting laser probe 93, the principle being to destroy epithelial cells lining the fistula track. It has been trialled in combination with fibrin glue 94, although more recent work, using the laser in isolation, demonstrated healing in 9 of 11 patients at a median of 7.4 months 93. In this study, the internal opening was closed using a flap in combination with laser ablation. A further larger study, recruiting 45 patients, found healing in 32 (71%) at a median of 30 months 215. All patients underwent placement of a loose seton prior to surgery, and 35 patients had a history of previous fistula surgery. A retrospective review of 50 patients treated by laser ablation showed ‘success’ in 41 (82%) at 12 months’ follow-up 216, which was mostly by phone, consequently these results need interpreting with caution. Wilhelm et al. 217 reported a series of 117 patients treated with the radial fibre fistula laser closing (FiLaC™) device. Patients in this series were followed for a median of 25 months (minimum 6 months) with primary healing in 64% of patients. A repeat procedure was performed in 31 patients who failed initial treatment, with overall healing achieved in 88% of patients. The treatment was associated with minimal alteration in anal control.
At present, laser ablation of a fistula track is in its infancy, with evidence supporting its use confined to a few case series. The best technique has not been established: for instance, is surgical closure of the internal opening necessary prior to laser ablation? Further larger studies, especially randomized trails against other sphincter-preserving techniques, are required to establish its role in treatment of anal fistulas.
Stem cell therapy
Autologous adipose-derived stem cells may represent a novel treatment option for complex fistulas, although as yet there is insufficient evidence to attest to its efficacy. As a technique it may be used in isolation or in combination with fibrin glue or advancement flaps. It has been used in patients with Crohn’s disease. Allogeneic, expanded, adipose-derived stem cells have been used in a randomized, multicentre, double-blind placebo-controlled study involving 212 patients 81. The primary end-point was remission at 24 weeks. In the intention-to-treat analysis 53/107 (50%) receiving stem cells achieved this, compared with 36/105 (34%) in the placebo arm 81. A separate multicentre, single-blind trial randomized 200 patients to stem cells alone, stem cells in combination with fibrin glue or fibrin glue alone, following closure of the internal opening 95. There was no significant difference in healing rates between any of the groups, which were 40–50% at 12 months’ follow-up: no serious adverse events were reported. A further small case series of seven patients reported healing rates of five out of seven at 6 months and four out of seven at a median of 46 months Borowski DW, Gill TS, Agarwal AK, Tabaqchali MA, Garg DK, Bhaskar P. Adipose Tissue-Derived Regenerative Cell-Enhanced Lipofilling for Treatment of Cryptoglandular Fistulae-in-Ano: The ALFA Technique. Surg Innov. 2015 Dec;22(6):593-600. doi: 10.1177/1553350615572656. Long-term results of a Phase 2 trial in patients with Crohn’s disease reported healing rates of 75% at 24 months’ follow-up 96. Recently reported work looked at whether autologous mesenchymal stem cells could heal fistulas in Crohn’s disease if applied in a bioabsorbable matrix 97. At 6 months 10/12 patients had complete clinical healing. It is too soon to comment on the role of this complex treatment in the routine management of anal fistulas.
Fistula clips
The principle of fistula clips technique is to debride the primary track and close the internal opening with a tightly applied metal clip. The most extensively investigated apparatus is the OTSC® Proctology (Ovesco Endoscopy AG, Tu72074 Tübingen, Germany), which employs a nitinol clip. A recent case-series has demonstrated healing in 18 of 20 (90%) fistulas at 6 months 98. This group consisted of 14 patients with a transsphincteric fistula and 6 with suprasphincteric fistulas, although details of the complexity of the tracks was not given. Two patients required removal of the clip as a result of delayed wound healing and discomfort. Another case-series of consecutive patients from a single institution used the OTSC® in refractory cases of anal fistula following previous surgery 99. Six of the 10 patients recruited had Crohn’s disease. Seven patients’ fistulas were healed at a median follow-up of approximately 8 months. The FISCLOSE trial is aimed at evaluating the efficacy and safety of a clip vs rectal mucosal advancement flap 100. The aim is to recruit 46 patients to two centers. The primary outcome is healing at 3 months. Secondary outcomes include healing at 6 and 12 months, anal pain, fecal incontinence and quality of life.
In a similar way to laser ablation, clipping the internal opening of a fistula is at an early stage of evolution, with a few encouraging case series having been published. Migration and pain, requiring removal of the clip at the request of patient, are significant risks that have been reported in the few studies which have been reported. Further larger studies, especially randomized trails against other sphincter-preserving techniques, are required to establish whether it has role in treatment of anal fistulas.
Video-assisted anal fistula treatment (VAAFT)
Video-assisted anal fistula treatment (VAAFT) consists of a diagnostic and a therapeutic phase. In the former, a fistuloscope and obturator are used to identify the internal opening as well as any secondary tracks and/or abscesses. The scope is inserted through the external opening and a glycine-mannitol solution infused to enable opening of the primary track and advancement under direct vision. The therapeutic phase involves destruction and cleaning of the track using cautery and further irrigation. One of the principles is closure of the internal opening using a circular/linear stapler, OTSC® nitinol clip or advancement/mucosal flap. Cyanoacrylate may be used to reinforce the closure of the internal opening, though the track must be left open to allow secretions to drain.
Work from Italy reported on 136 patients undergoing video-assisted anal fistula treatment (VAAFT) over a 5-year period 101. Ninety-eight patients were followed up for a minimum of 6 months. Primary healing occurred in 72 (73%) patients within 2–3 months of surgery, with no major complications seen. Sixty-two patients were followed up for over a year, with healing noted in 52 (84%). A further study from Singapore reported on 41 patients treated with VAAFT 102: all were cryptoglandular in etiology, though low intersphincteric fistulas and patients with abscesses were excluded. A number of approaches were used to obliterate the internal opening – stapling, advancement flap and OTSC® nitinol clip. Eleven patients had undergone previous fistula surgery. Overall primary healing was seen in 29 (71%) patients at a median follow-up of 34 months, with the best results seen with VAAFT in combination with the OTSC® nitinol clip. This approach has also been used in patients with Crohn’s disease in combination with an advancement flap 103. Success in the 13 patients recruited was defined as closure of both internal and external openings, absence of drainage without requirement for intervention and no abscess formation. All patients had complex fistulae, five were on biological agents and four had a proximal stoma. At a mean follow-up of 9 months 9 of 11 patients, where video-assisted anal fistula treatment (VAAFT) was technically possible, were deemed a success, and no deterioration in continence was observed. VAAFT has also been reported in a paediatric population 104. Thirteen procedures were performed on nine children (mean age 9.6 years). One was associated with Crohn’s disease, though only five were described as idiopathic. All patients who underwent a complete VAAFT (n = 8) were healed at 10 months.
Vvideo-assisted anal fistula treatment (VAAFT) is another novel treatment that shows some promise, although it is far from clear which part of the treatment is important and whether the video element is vital to its success or whether thorough cleaning of the track and secure closure of the internal opening is equally successful, saving the investment in the video technology. Proponents argue that the diagnostic phase finds tracks that MRI has missed, although evidence to support this assertion is lacking. More detailed studies are required before this dilemma can be resolved and the role of VAAFT be defined.
Perianal fistula in Crohn disease
Perianal fistula in Crohn disease patients is a severe disease to treat, but early recognition and diagnosis are critical to effective therapy. These patients should be referred to a gastroenterologist and receive anti-TNF alpha therapy as their primary treatment for fistula disease. After medical treatment, if the fistula persists, setons are the most commonly used primary surgical option in these patients with reasonable healing rates after anti-TNF alpha therapy 105. Crohn disease patients often are misdiagnosed and have delays in care and also may experience prolonged waiting periods to obtain their medications; thus, a comprehensive care team may be more effective in the management of these patients 105. Infliximab is the primary treatment for these patients. In patients receiving infliximab therapy, higher blood levels of the drug have been associated with improved healing rates 106. Patients with Chron disease are likely to have concomitant proctitis, which is revealed by preoperative imaging. A study of 126 patients with anal fistulas who underwent preoperative MRI found that MRI findings of concomitant rectal inflammation were more closely associated with Crohn disease 107.
The International Organisation for Inflammatory Bowel Diseases (IOIBD) global consensus guidelines emphasize the importance of evaluation of the rectum in these patients as their disease may often affect the rectal mucosa and anorectal area simultaneously. In a study of 36 pediatric and adult patients with fistulizing Crohn disease, a cutoff of 2.5 cm seen on MRI predicted patients who responded to infliximab therapy and those with the persistence of illness 108. A few studies have shown effective healing rates around 67-90% of combined seton and anti-TNF alpha therapy in Crohn disease patients that were retrospective in nature 109. A large meta-analysis comparing healing of primary seton versus infliximab failed to determine which was superior as the studies varied in outcomes 110.
Perianal fistula prognosis
Prognosis of the anorectal fistula is variable depending on the cause. In anal fistulas of cryptoglandular origin healing rates for simple fistulas approach 80%, and that of complex fistulas are around 60% for sphincter preserving operation 111. Recurrence of anal fistula is higher in obese patients, smokers, and those with a history of anal surgery. Anatomical factors including multiple fistula tracts, high transphincteric fistula, inability to determine an internal opening, seton placement, and horseshoe abscesses were also associated with a higher rate of recurrence 9. Recurrence of the fistula often occurs within the first year of treatment 112.
Setons have been used with much success up to 80 to 90% healing rates, but these are healing rates measured after six months. In general, a fistula that is treated with a fistulotomy or fistulectomy, depending on the wound size, should be entirely healed by 12 weeks. If drainage is increased or persistent up the twelfth week that the fistula recurred or did not close completely. Causes for failure of surgical therapy include incomplete division of the fistula in a fistulotomy or incomplete resection or obliteration of tract in a fistulectomy. In the LIFT procedure, leaving a long fistula tract behind and incomplete ligation of the fistula tract are possible causes of failure. In anal-cutaneous or rectal mucosal advancement flap techniques, if the flap fails, the fistula will either not heal or will recur. Smoking is a risk factor for failure of treatment with flap, as well as Crohn disease 113. This is often secondary to the inadequate blood supply of the flap, as evidenced by improved healing rates when the muscular layer is used in the flap.
Failure of anal fistula plugs to allow fistulas to heal can be attributed to multiple reasons including, not completely covering the plug internally, incomplete debridement of the fistula tract, and premature dislodgement of the fistula plug. Setons that are removed too early may lead to the fistula not healing if the tract has not migrated sufficiently to allow the fistula to heal. Some setons may lead to a lower fistula that then requires a fistulotomy for complete healing to occur.
Depending on the initial procedure performed, additional procedures are used to treat recurrence fistula. When a fistula recurs, an MRI is helpful to determine its course, and an exam under anesthesia should be performed to characterize the fistula tract. Treatment is based on the type of fistula present, which may be different on recurrence than on complex fistula. Because the risk of incontinence is increased with repeated anorectal surgeries, a sphincter preserving approach is best utilized in the treatment of recurrent fistula, mainly if a fistulotomy or fistulectomy was the primary treatment. LIFT procedure is an option for recurrent fistulas. A failed LIFT procedure may be followed by a repeat LIFT procedure or an advancement flap procedure or seton. One study which evaluated outcomes of 53 patients who failed LIFT procedure and went on to undergo an endorectal advancement flap or fistulotomy staged with seton showed a 50% healing rate 114. Of patients with a high transphincteric fistula, those with a horseshoe extension of the fistula may have improved success with anal advancement flap repair 115.
Setons used as the primary treatment should be considered a staged procedure and followed by a fistulotomy. Anal fistula plug procedure that has failed may be followed by a seton, advancement flap, LIFT, or even fistulotomy depending on the location of the fistula. A failed flap may be repeated using tissue from a different site. VAAFT is a safe treatment option when repeated for failed initial VAAFT with increased healing rates on the repeat procedure 116.
References- Fistula-in-Ano. https://emedicine.medscape.com/article/190234-overview
- Lam TJ, van Bodegraven AA, Felt-Bersma RJ. Anorectal complications and function in patients suffering from inflammatory bowel disease: a series of patients with long-term follow-up. International journal of colorectal disease. 2014;29(8):923–9. 10.1007/s00384-014-1926-7
- Sainio P. Fistula-in-ano in a defined population. Incidence and epidemiological aspects. Ann Chir Gynaecol. 1984;73(4):219–24.
- Norton C, Dibley LB, Bassett P. Faecal incontinence in inflammatory bowel disease: associations and effect on quality of life. Journal of Crohn’s & colitis. 2013;7(8):e302–11. 10.1016/j.crohns.2012.11.004
- Zwintscher NP, Shah PM, Argawal A, Chesley PM, Johnson EK, Newton CR, et al. The impact of perianal disease in young patients with inflammatory bowel disease. International journal of colorectal disease. 2015;30(9):1275–9. 10.1007/s00384-015-2251-5
- Phillips J, Lees N, Arnall F. Current management of fistula-in-ano. Br J Hosp Med (Lond). 2015 Mar. 76 (3):142, 144-7.
- Gold, S.L., Cohen-Mekelburg, S., Schneider, Y., & Steinlauf, A.F. (2018). Perianal Fistulas in Patients With Crohn’s Disease, Part 1: Current Medical Management. Gastroenterology & hepatology, 14 8, 470-481
- Davis BR, Kasten KR. Anorectal abscess and fistula. Steele SR, Hull TL, Read TE, Saclarides TJ, Senagore AJ, Whitlow CB, eds. The ASCRS Textbook of Colon and Rectal Surgery. 3rd ed. New York: Springer; 2016. Vol 1: 215-44.
- Mei Z, Wang Q, Zhang Y, Liu P, Ge M, Du P, Yang W, He Y. Risk Factors for Recurrence after anal fistula surgery: A meta-analysis. Int J Surg. 2019 Sep;69:153-164. doi: 10.1016/j.ijsu.2019.08.003
- Emile SH, Elfeki H, Thabet W, Sakr A, Magdy A, El-Hamed TMA, Omar W, Khafagy W. Predictive factors for recurrence of high transsphincteric anal fistula after placement of seton. J Surg Res. 2017 Jun 1;213:261-268. doi: 10.1016/j.jss.2017.02.053
- Rosen L. Anorectal abscess-fistulae. Surg Clin North Am. 1994 Dec. 74(6):1293-308.
- Parks AG, Gordon PH, Hardcastle JD. A classification of fistula-in-ano. Br J Surg. 1976;63(1):1-12
- Parks AG, Gordon PH, Hardcastle JD. A classification of fistula-in-ano. Br J Surg. 1976 Jan. 63(1):1-12.
- Hamalainen KP, Sainio AP. Incidence of fistulas after drainage of acute anorectal abscesses. Dis Colon Rectum. 1998 Nov. 41(11):1357-61; discussion 1361-2.
- Sainio P. Fistula-in-ano in a defined population. Incidence and epidemiological aspects. Ann Chir Gynaecol. 1984. 73(4):219-24.
- Sun MR, Smith MP, Kane RA. Current techniques in imaging of fistula in ano: three-dimensional endoanal ultrasound and magnetic resonance imaging. Semin Ultrasound CT MR. 2008 Dec. 29(6):454-71.
- Weisman RI, Orsay CP, Pearl RK, Abcarian H. The role of fistulography in fistula-in-ano. Report of five cases. Dis Colon Rectum. 1991 Feb. 34(2):181-4.
- Nevler A, Beer-Gabel M, Lebedyev A, Soffer A, Gutman M, Carter D, et al. Transperineal ultrasonography in perianal Crohn’s disease and recurrent cryptogenic fistula-in-ano. Colorectal Dis. 2013 Aug. 15 (8):1011-8.
- Buchanan GN, Halligan S, Williams AB, Cohen CR, Tarroni D, Phillips RK, et al. Magnetic resonance imaging for primary fistula in ano. Br J Surg. 2003 Jul. 90(7):877-81.
- Present DH, Rutgeerts P, Targan S, Hanauer SB, Mayer L, van Hogezand RA, et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. N Engl J Med. 1999 May 6. 340(18):1398-405
- Cho YB, Park KJ, Yoon SN, Song KH, Kim do S, Jung SH, et al. Long-term results of adipose-derived stem cell therapy for the treatment of Crohn’s fistula. Stem Cells Transl Med. 2015 May. 4 (5):532-7.
- Afsarlar CE, Karaman A, Tanir G, Karaman I, Yilmaz E, Erdogan D, et al. Perianal abscess and fistula-in-ano in children: clinical characteristic, management and outcome. Pediatr Surg Int. 2011 Oct. 27(10):1063-8.
- Kotze PG, Shen B, Lightner A, et al. Modern management of perianal fistulas in Crohn’s disease: future directions. Gut. 2018;67(6):1181-1194.
- Bernstein LH, Frank MS, Brandt LJ, Boley SJ. Healing of perineal Crohn’s disease with metronidazole. Gastroenterology. 1980;79(3):599
- Brandt LJ, Bernstein LH, Boley SJ, Frank MS. Metronidazole therapy for perineal Crohn’s disease: a follow-up study. Gastroenterology. 1982;83(2):383-387.
- Marzo M, Felice C, Pugliese D, et al. Management of perianal fistulas in Crohn’s disease: an up-to-date review. World J Gastroenterol. 2015;21(5):1394-1403.
- Maeda Y, Ng SC, Durdey P, et al; Topical Metronidazole in Perianal Crohn’s Study Group. Randomized clinical trial of metronidazole ointment versus placebo in perianal Crohn’s disease. Br J Surg. 2010;97(9):1340-1347.
- Vavricka SR, Rogler G. Fistula treatment: the unresolved challenge. Dig Dis. 2010;28(3):556-564.
- Dewint P, Hansen BE, Verhey E, et al. Adalimumab combined with cipro-floxacin is superior to adalimumab monotherapy in perianal fistula closure in Crohn’s disease: a randomised, double-blind, placebo controlled trial (ADAFI). Gut. 2014;63(2):292-299.
- O’Riordan JM, Datta I, Johnston C, Baxter NN. A systematic review of the anal fistula plug for patients with Crohn’s and non-Crohn’s related fistula-in-ano. Dis Colon Rectum. 2012 Mar. 55(3):351-8.
- Johnson EK, Gaw JU, Armstrong DN. Efficacy of anal fistula plug vs. fibrin glue in closure of anorectal fistulas. Dis Colon Rectum. 2006 Mar. 49(3):371-6.
- Abbas MA, Jackson CH, Haigh PI. Predictors of outcome for anal fistula surgery. Arch Surg. 2011 Sep. 146(9):1011-6.
- Han JG, Xu HM, Song WL, Jin ML, Gao JS, Wang ZJ, et al. Histologic analysis of acellular dermal matrix in the treatment of anal fistula in an animal model. J Am Coll Surg. 2009 Jun. 208(6):1099-106.
- Senéjoux A, Siproudhis L, Abramowitz L, et al, Groupe d’Etude Thérapeutique des Affections Inflammatoires du tube Digestif [GETAID]. Fistula Plug in Fistulising Ano-Perineal Crohn’s Disease: a Randomised Controlled Trial. J Crohns Colitis. 2016 Feb. 10 (2):141-8.
- Borreman P, de Gheldere C, Fierens J, Vanclooster P. Can a flap help the plug ? Or vice versa ? Proposing a combined sphincter-sparing anal fistula repair. Acta Chir Belg. 2014 Nov-Dec. 114 (6):376-80.
- Blumetti J, Abcarian A, Quinteros F, Chaudhry V, Prasad L, Abcarian H. Evolution of treatment of fistula in ano. World J Surg. 2012 May. 36(5):1162-7.
- Memon AA, Murtaza G, Azami R, Zafar H, Chawla T, Laghari AA. Treatment of complex fistula in ano with cable-tie seton: a prospective case series. ISRN Surg. 2011. 2011:636952.
- Hammond TM, Knowles CH, Porrett T, Lunniss PJ. The Snug Seton: short and medium term results of slow fistulotomy for idiopathic anal fistulae. Colorectal Dis. 2006 May. 8(4):328-37.
- Leng Q, Jin HY. Anal fistula plug vs mucosa advancement flap in complex fistula-in-ano: A meta-analysis. World J Gastrointest Surg. 2012 Nov 27. 4(11):256-61.
- Rojanasakul A, Pattanaarun J, Sahakitrungruang C, Tantiphlachiva K. Total anal sphincter saving technique for fistula-in-ano; the ligation of intersphincteric fistula tract. J Med Assoc Thai. 2007 Mar;90(3):581-6.
- Mushaya C, Bartlett L, Schulze B, Ho YH. Ligation of intersphincteric fistula tract compared with advancement flap for complex anorectal fistulas requiring initial seton drainage. Am J Surg. 2012 Sep;204(3):283-9. doi: 10.1016/j.amjsurg.2011.10.025
- Han JG, Wang ZJ, Zheng Y, Chen CW, Wang XQ, Che XM, Song WL, Cui JJ. Ligation of Intersphincteric Fistula Tract vs Ligation of the Intersphincteric Fistula Tract Plus a Bioprosthetic Anal Fistula Plug Procedure in Patients With Transsphincteric Anal Fistula: Early Results of a Multicenter Prospective Randomized Trial. Ann Surg. 2016 Dec;264(6):917-922. doi: 10.1097/SLA.0000000000001562
- Madbouly KM, El Shazly W, Abbas KS, Hussein AM. Ligation of intersphincteric fistula tract versus mucosal advancement flap in patients with high transsphincteric fistula-in-ano: a prospective randomized trial. Dis Colon Rectum. 2014 Oct;57(10):1202-8. doi: 10.1097/DCR.0000000000000194
- Williams, G., Williams, A., Tozer, P., Phillips, R., Ahmad, A., Jayne, D. and Maxwell-Armstrong, C. (2018), The treatment of anal fistula: second ACPGBI Position Statement – 2018. Colorectal Dis, 20: 5-31. https://doi.org/10.1111/codi.14054
- Sileri P, Giarratano G, Franceschilli L, Limura E, Perrone F, Stazi A, Toscana C, Gaspari AL. Ligation of the intersphincteric fistula tract (LIFT): a minimally invasive procedure for complex anal fistula: two-year results of a prospective multicentric study. Surg Innov. 2014 Oct;21(5):476-80. doi: 10.1177/1553350613508018
- Abcarian AM, Estrada JJ, Park J, Corning C, Chaudhry V, Cintron J, Prasad L, Abcarian H. Ligation of intersphincteric fistula tract: early results of a pilot study. Dis Colon Rectum. 2012 Jul;55(7):778-82. doi: 10.1097/DCR.0b013e318255ae8a
- Ooi K, Skinner I, Croxford M, Faragher I, McLaughlin S. Managing fistula-in-ano with ligation of the intersphincteric fistula tract procedure: the Western Hospital experience. Colorectal Dis. 2012 May;14(5):599-603. doi: 10.1111/j.1463-1318.2011.02723.x
- Liu WY, Aboulian A, Kaji AH, Kumar RR. Long-term results of ligation of intersphincteric fistula tract (LIFT) for fistula-in-ano. Dis Colon Rectum. 2013 Mar;56(3):343-7. doi: 10.1097/DCR.0b013e318278164c
- Parthasarathi R, Gomes RM, Rajapandian S, Sathiamurthy R, Praveenraj P, Senthilnathan P, Palanivelu C. Ligation of the intersphincteric fistula tract for the treatment of fistula-in-ano: experience of a tertiary care centre in South India. Colorectal Dis. 2016 May;18(5):496-502. doi: 10.1111/codi.13162
- Altomare DF, Greco VJ, Tricomi N, Arcanà F, Mancini S, Rinaldi M, Pulvirenti d’Urso A, La Torre F. Seton or glue for trans-sphincteric anal fistulae: a prospective randomized crossover clinical trial. Colorectal Dis. 2011 Jan;13(1):82-6. doi: 10.1111/j.1463-1318.2009.02056.x
- Cho DY. Endosonographic criteria for an internal opening of fistula-in-ano. Dis Colon Rectum. 1999 Apr;42(4):515-8. doi: 10.1007/BF02234179
- Schulze B, Ho YH. Management of complex anorectal fistulas with seton drainage plus partial fistulotomy and subsequent ligation of intersphincteric fistula tract (LIFT). Tech Coloproctol. 2015 Feb;19(2):89-95. doi: 10.1007/s10151-014-1245-6
- Romaniszyn M, Walega PJ, Nowak W. Efficacy of lift (ligation of intersphincteric fistula tract) for complex and recurrent anal fistulas–a single-center experience and a review of the literature. Pol Przegl Chir. 2015 Feb 3;86(11):532-6. doi: 10.2478/pjs-2014-0094
- van Onkelen RS, Gosselink MP, Schouten WR. Ligation of the intersphincteric fistula tract in low transsphincteric fistulae: a new technique to avoid fistulotomy. Colorectal Dis. 2013 May;15(5):587-91. doi: 10.1111/codi.12030
- Chen HJ, Sun GD, Zhu P, Zhou ZL, Chen YG, Yang BL. Effective and long-term outcome following ligation of the intersphincteric fistula tract (LIFT) for transsphincteric fistula. Int J Colorectal Dis. 2017 Apr;32(4):583-585. doi: 10.1007/s00384-016-2723-2
- Tan KK, Lee PJ. Early experience of reinforcing the ligation of the intersphincteric fistula tract procedure with a bioprosthetic graft (BioLIFT) for anal fistula. ANZ J Surg. 2014 Apr;84(4):280-3. doi: 10.1111/ans.12242
- Ye F, Tang C, Wang D, Zheng S. Early experience with the modificated approach of ligation of the intersphincteric fistula tract for high transsphincteric fistula. World J Surg. 2015 Apr;39(4):1059-65. doi: 10.1007/s00268-014-2888-1
- Bastawrous A, Hawkins M, Kratz R, Menon R, Pollock D, Charbel J, Long K. Results from a novel modification to the ligation intersphincteric fistula tract. Am J Surg. 2015 May;209(5):793-8; discussion 798. doi: 10.1016/j.amjsurg.2015.01.002
- Lehmann JP, Graf W. Efficacy of LIFT for recurrent anal fistula. Colorectal Dis. 2013 May;15(5):592-5. doi: 10.1111/codi.12104
- Gingold DS, Murrell ZA, Fleshner PR. A prospective evaluation of the ligation of the intersphincteric tract procedure for complex anal fistula in patients with Crohn’s disease. Ann Surg. 2014 Dec;260(6):1057-61. doi: 10.1097/SLA.0000000000000479
- Tan KK, Tan IJ, Lim FS, Koh DC, Tsang CB. The anatomy of failures following the ligation of intersphincteric tract technique for anal fistula: a review of 93 patients over 4 years. Dis Colon Rectum. 2011 Nov;54(11):1368-72. doi: 10.1097/DCR.0b013e31822bb55e
- Abbas MA, Lemus-Rangel R, Hamadani A. Long-term outcome of endorectal advancement flap for complex anorectal fistulae. Am Surg. 2008 Oct. 74(10):921-4.
- Jacob TJ, Perakath B, Keighley MR. Surgical intervention for anorectal fistula. Cochrane Database Syst Rev. 2010 May 12;(5):CD006319. doi: 10.1002/14651858.CD006319.pub2
- Adams T, Yang J, Kondylis LA, Kondylis PD. Long-term outlook after successful fibrin glue ablation of cryptoglandular transsphincteric fistula-in-ano. Dis Colon Rectum. 2008 Oct;51(10):1488-90. doi: 10.1007/s10350-008-9405-2
- Buchanan GN, Bartram CI, Phillips RK, Gould SW, Halligan S, Rockall TA, Sibbons P, Cohen RG. Efficacy of fibrin sealant in the management of complex anal fistula: a prospective trial. Dis Colon Rectum. 2003 Sep;46(9):1167-74. doi: 10.1007/s10350-004-6708-9
- Ellis CN, Clark S. Fibrin glue as an adjunct to flap repair of anal fistulas: a randomized, controlled study. Dis Colon Rectum. 2006 Nov;49(11):1736-40. doi: 10.1007/s10350-006-0718-8
- Cirocchi R, Santoro A, Trastulli S, Farinella E, Di Rocco G, Vendettuali D, Giannotti D, Redler A, Coccetta M, Gullà N, Boselli C, Avenia N, Sciannameo F, Basoli A. Meta-analysis of fibrin glue versus surgery for treatment of fistula-in-ano. Ann Ital Chir. 2010 Sep-Oct;81(5):349-56.
- Lindsey I, Smilgin-Humphreys MM, Cunningham C, Mortensen NJ, George BD. A randomized, controlled trial of fibrin glue vs. conventional treatment for anal fistula. Dis Colon Rectum. 2002 Dec;45(12):1608-15. doi: 10.1007/s10350-004-7247-0
- Maralcan G, Başkonuş I, Aybasti N, Gökalp A. The use of fibrin glue in the treatment of fistula-in-ano: a prospective study. Surg Today. 2006;36(2):166-70. doi: 10.1007/s00595-005-3121-5
- Sentovich SM. Fibrin glue for anal fistulas: long-term results. Dis Colon Rectum. 2003 Apr;46(4):498-502. doi: 10.1007/s10350-004-6589-y
- Haim N, Neufeld D, Ziv Y, Tulchinsky H, Koller M, Khaikin M, Zmora O. Long-term results of fibrin glue treatment for cryptogenic perianal fistulas: a multicenter study. Dis Colon Rectum. 2011 Oct;54(10):1279-83. doi: 10.1097/DCR.0b013e318223c894
- de Oca J, Millán M, Jiménez A, Golda T, Biondo S. Long-term results of surgery plus fibrin sealant for anal fistula. Colorectal Dis. 2012 Jan;14(1):e12-5. doi: 10.1111/j.1463-1318.2011.02747.x
- Witte ME, Klaase JM, Gerritsen JJ, Kummer EW. Fibrin glue treatment for simple and complex anal fistulas. Hepatogastroenterology. 2007 Jun;54(76):1071-3.
- Cestaro G, De Rosa M, Gentile M. Treatment of fistula in ano with fibrin glue: preliminary results from a prospective study. Minerva Chir. 2014 Aug;69(4):225-8.
- Yeung JM, Simpson JA, Tang SW, Armitage NC, Maxwell-Armstrong C. Fibrin glue for the treatment of fistulae in ano–a method worth sticking to? Colorectal Dis. 2010 Apr;12(4):363-6. doi: 10.1111/j.1463-1318.2009.01801.x
- van Koperen PJ, Wind J, Bemelman WA, Slors JF. Fibrin glue and transanal rectal advancement flap for high transsphincteric perianal fistulas; is there any advantage? Int J Colorectal Dis. 2008 Jul;23(7):697-701. doi: 10.1007/s00384-008-0460-x
- Chung W, Kazemi P, Ko D, Sun C, Brown CJ, Raval M, Phang T. Anal fistula plug and fibrin glue versus conventional treatment in repair of complex anal fistulas. Am J Surg. 2009 May;197(5):604-8. doi: 10.1016/j.amjsurg.2008.12.013
- Currie LJ, Sharpe JR, Martin R. The use of fibrin glue in skin grafts and tissue-engineered skin replacements: a review. Plast Reconstr Surg. 2001 Nov;108(6):1713-26. doi: 10.1097/00006534-200111000-00045
- Hammond TM, Grahn MF, Lunniss PJ. Fibrin glue in the management of anal fistulae. Colorectal Dis. 2004 Sep;6(5):308-19. doi: 10.1111/j.1463-1318.2004.00676.x
- Lara FJ, Serrano AM, Moreno JU, Carmona JH, Marquez MF, Pérez LR, del Rey Moreno A, Muñoz HO. Platelet-rich fibrin sealant as a treatment for complex perianal fistulas: a multicentre study. J Gastrointest Surg. 2015 Feb;19(2):360-8. doi: 10.1007/s11605-014-2698-7
- Panés J, García-Olmo D, Van Assche G, Colombel JF, Reinisch W, Baumgart DC, Dignass A, Nachury M, Ferrante M, Kazemi-Shirazi L, Grimaud JC, de la Portilla F, Goldin E, Richard MP, Leselbaum A, Danese S; ADMIRE CD Study Group Collaborators. Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn’s disease: a phase 3 randomised, double-blind controlled trial. Lancet. 2016 Sep 24;388(10051):1281-90. doi: 10.1016/S0140-6736(16)31203-X
- The Surgisis AFP anal fistula plug: report of a consensus conference. Colorectal Dis. 2008 Jan;10(1):17-20. doi: 10.1111/j.1463-1318.2007.01423.x
- Amrani S, Zimmern A, O’Hara K, Corman ML. The Surgisis AFP anal fistula plug: a new and reasonable alternative for the treatment of anal fistula. Gastroenterol Clin Biol. 2008 Nov;32(11):946-8. doi: 10.1016/j.gcb.2008.09.003
- Johnson EK, Gaw JU, Armstrong DN. Efficacy of anal fistula plug vs. fibrin glue in closure of anorectal fistulas. Dis Colon Rectum. 2006 Mar;49(3):371-6. doi: 10.1007/s10350-005-0288-1
- Ortiz H, Marzo J, Ciga MA, Oteiza F, Armendáriz P, de Miguel M. Randomized clinical trial of anal fistula plug versus endorectal advancement flap for the treatment of high cryptoglandular fistula in ano. Br J Surg. 2009 Jun;96(6):608-12. doi: 10.1002/bjs.6613
- A ba-bai-ke-re MM, Wen H, Huang HG, Chu H, Lu M, Chang ZS, Ai EH, Fan K. Randomized controlled trial of minimally invasive surgery using acellular dermal matrix for complex anorectal fistula. World J Gastroenterol. 2010 Jul 14;16(26):3279-86. doi: 10.3748/wjg.v16.i26.3279
- Göttgens KW, Smeets RR, Stassen LP, Beets G, Breukink SO. Systematic review and meta-analysis of surgical interventions for high cryptoglandular perianal fistula. Int J Colorectal Dis. 2015 May;30(5):583-93. doi: 10.1007/s00384-014-2091-8
- Bondi J, Avdagic J, Karlbom U, Hallböök O, Kalman D, Šaltytė Benth J, Naimy N, Øresland T. Randomized clinical trial comparing collagen plug and advancement flap for trans-sphincteric anal fistula. Br J Surg. 2017 Aug;104(9):1160-1166. doi: 10.1002/bjs.10549
- Fisher OM, Raptis DA, Vetter D, Novak A, Dindo D, Hahnloser D, Clavien PA, Nocito A. An outcome and cost analysis of anal fistula plug insertion vs endorectal advancement flap for complex anal fistulae. Colorectal Dis. 2015 Jul;17(7):619-26. doi: 10.1111/codi.12888
- Jayne DG, Scholefield J, Tolan D, Gray R, Edlin R, Hulme CT, Sutton AJ, Handley K, Hewitt CA, Kaur M, Magill L. Anal fistula plug versus surgeon’s preference for surgery for trans-sphincteric anal fistula: the FIAT RCT. Health Technol Assess. 2019 May;23(21):1-76. doi: 10.3310/hta23210
- Zubaidi A, Al-Rowais M, Teraiki T, Alobeed O, Alkhayal K, Alkubair M. Anal fistula plug for treatment of high anal fistula: MRI evidence (Abstract). Dis Colon Rectum 2015; 58: e89.
- Slutzki S, Abramsohn R, Bogokowsky H. Carbon dioxide laser in the treatment of high anal fistula. Am J Surg. 1981 Mar;141(3):395-6. doi: 10.1016/0002-9610(81)90207-5
- Wilhelm A. A new technique for sphincter-preserving anal fistula repair using a novel radial emitting laser probe. Tech Coloproctol. 2011 Dec;15(4):445-9. doi: 10.1007/s10151-011-0726-0
- Salim AS, Ahmed TM. KTP-Laser and fibrin glue for treatment of fistulae in ano. Saudi Med J. 2001 Nov;22(11):1022-4
- Herreros MD, Garcia-Arranz M, Guadalajara H, De-La-Quintana P, Garcia-Olmo D; FATT Collaborative Group. Autologous expanded adipose-derived stem cells for the treatment of complex cryptoglandular perianal fistulas: a phase III randomized clinical trial (FATT 1: fistula Advanced Therapy Trial 1) and long-term evaluation. Dis Colon Rectum. 2012 Jul;55(7):762-72. doi: 10.1097/DCR.0b013e318255364a
- Cho YB, Park KJ, Yoon SN, Song KH, Kim DS, Jung SH, Kim M, Jeong HY, Yu CS. Long-term results of adipose-derived stem cell therapy for the treatment of Crohn’s fistula. Stem Cells Transl Med. 2015 May;4(5):532-7. doi: 10.5966/sctm.2014-0199
- Dietz AB, Dozois EJ, Fletcher JG, Butler GW, Radel D, Lightner AL, Dave M, Friton J, Nair A, Camilleri ET, Dudakovic A, van Wijnen AJ, Faubion WA. Autologous Mesenchymal Stem Cells, Applied in a Bioabsorbable Matrix, for Treatment of Perianal Fistulas in Patients With Crohn’s Disease. Gastroenterology. 2017 Jul;153(1):59-62.e2. doi: 10.1053/j.gastro.2017.04.001
- Prosst RL, Joos AK, Ehni W, Bussen D, Herold A. Prospective pilot study of anorectal fistula closure with the OTSC Proctology. Colorectal Dis. 2015 Jan;17(1):81-6. doi: 10.1111/codi.12762
- Mennigen R, Laukötter M, Senninger N, Rijcken E. The OTSC(®) proctology clip system for the closure of refractory anal fistulas. Tech Coloproctol. 2015 Apr;19(4):241-6. doi: 10.1007/s10151-015-1284-7
- Dubois A, Carrier G, Pereira B, Gillet B, Faucheron JL, Pezet D, Balayssac D. Therapeutic management of complex anal fistulas by installing a nitinol closure clip: study protocol of a multicentric randomised controlled trial–FISCLOSE. BMJ Open. 2015 Dec 16;5(12):e009884. doi: 10.1136/bmjopen-2015-009884
- Meinero P, Mori L. Video-assisted anal fistula treatment (VAAFT): a novel sphincter-saving procedure for treating complex anal fistulas. Tech Coloproctol. 2011 Dec;15(4):417-22. doi: 10.1007/s10151-011-0769-2
- Seow-En I, Seow-Choen F, Koh PK. An experience with video-assisted anal fistula treatment (VAAFT) with new insights into the treatment of anal fistulae. Tech Coloproctol. 2016 Jun;20(6):389-393. doi: 10.1007/s10151-016-1450-6
- Schwandner O. Video-assisted anal fistula treatment (VAAFT) combined with advancement flap repair in Crohn’s disease. Tech Coloproctol. 2013 Apr;17(2):221-5. doi: 10.1007/s10151-012-0921-7
- Pini Prato A, Zanaboni C, Mosconi M, Mazzola C, Muller L, Meinero PC, Faticato MG, Leonelli L, Montobbio G, Disma N, Mattioli G. Preliminary results of video-assisted anal fistula treatment (VAAFT) in children. Tech Coloproctol. 2016 May;20(5):279-285. doi: 10.1007/s10151-016-1447-1
- Lee MJ, Freer C, Adegbola S, Elkady S, Parkes M, Hart A, Fearnhead NS, Lobo AJ, Brown SR. Patients with perianal Crohn’s fistulas experience delays in accessing anti-TNF therapy due to slow recognition, diagnosis and integration of specialist services: lessons learned from three referral centres. Colorectal Dis. 2018 Sep;20(9):797-803. doi: 10.1111/codi.14102
- Strik AS, Löwenberg M, Buskens CJ, B Gecse K, I Ponsioen C, Bemelman WA, D’Haens GR. Higher anti-TNF serum levels are associated with perianal fistula closure in Crohn’s disease patients. Scand J Gastroenterol. 2019 Apr;54(4):453-458. doi: 10.1080/00365521.2019.1600014
- Oliveira IS, Kilcoyne A, Price MC, Harisinghani M. MRI features of perianal fistulas: is there a difference between Crohn’s and non-Crohn’s patients? Abdom Radiol (NY). 2017 Apr;42(4):1162-1168. doi: 10.1007/s00261-016-0989-z
- Shenoy-Bhangle A, Nimkin K, Goldner D, Bradley WF, Israel EJ, Gee MS. MRI predictors of treatment response for perianal fistulizing Crohn disease in children and young adults. Pediatr Radiol. 2014 Jan;44(1):23-9. doi: 10.1007/s00247-013-2771-5
- Hukkinen M, Pakarinen MP, Piekkala M, Koivusalo A, Rintala R, Kolho KL. Treatment of complex perianal fistulas with seton and infliximab in adolescents with Crohn’s disease. J Crohns Colitis. 2014 Aug;8(8):756-62. doi: 10.1016/j.crohns.2014.01.001
- de Groof EJ, Sahami S, Lucas C, Ponsioen CY, Bemelman WA, Buskens CJ. Treatment of perianal fistula in Crohn’s disease: a systematic review and meta-analysis comparing seton drainage and anti-tumour necrosis factor treatment. Colorectal Dis. 2016 Jul;18(7):667-75. doi: 10.1111/codi.13311
- Jimenez M, Mandava N. Anorectal Fistula. [Updated 2021 Sep 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560657
- Ortiz H, Marzo M, de Miguel M, Ciga MA, Oteiza F, Armendariz P. Length of follow-up after fistulotomy and fistulectomy associated with endorectal advancement flap repair for fistula in ano. Br J Surg. 2008 Apr;95(4):484-7. doi: 10.1002/bjs.6023
- Mizrahi N, Wexner SD, Zmora O, Da Silva G, Efron J, Weiss EG, Vernava AM 3rd, Nogueras JJ. Endorectal advancement flap: are there predictors of failure? Dis Colon Rectum. 2002 Dec;45(12):1616-21. doi: 10.1097/01.DCR.0000037654.01119.CD
- Wright M, Thorson A, Blatchford G, Shashidharan M, Beaty J, Bertelson N, Aggrawal P, Taylor L, Ternent CA. What happens after a failed LIFT for anal fistula? Am J Surg. 2017 Dec;214(6):1210-1213. doi: 10.1016/j.amjsurg.2017.08.042
- van Onkelen RS, Gosselink MP, Thijsse S, Schouten WR. Predictors of outcome after transanal advancement flap repair for high transsphincteric fistulas. Dis Colon Rectum. 2014 Aug;57(8):1007-11. doi: 10.1097/DCR.0000000000000154
- Giarratano G, Shalaby M, Toscana C, Sileri P. Video-assisted anal fistula treatment for complex anal fistula: a long-term follow-up study. Colorectal Dis. 2020 Aug;22(8):939-944. doi: 10.1111/codi.15005





{kind=link}