What is priapism
Priapism is defined as painful, unwanted erection of the penis that is sustained for longer than 4 hours despite a lack of sexual desire or excitement and is not induced by physical or psychological stimulation. Priapism is painful and can have long term harmful effects, so is considered a medical emergency. If priapism is not treated within 24 hours your penis may be permanently damaged and you might have trouble getting an erection in future. If you have an erection that is painful and won’t go away or lasts more than four hours, you should go to the nearest emergency department for medical attention.
Priapism occurs because the blood in the penis becomes trapped and is unable to return to the circulation. Priapism results from abnormalities of blood vessels and nerves, usually in response to medication used to produce erections in males who otherwise cannot attain them. Other causes include a spinal cord disorder, leukemia, sickle-cell disease, or a pelvic tumor.
There are two main types of priapism:
- Low-flow priapism (also called ischemic priapism) – Most common form of disease, arising from the slow passage of blood through the vascular chambers of the penis. This is primarily caused by increased viscosity of blood in the penis. This type of priapism is a surgical emergency for the penis may be damaged with prolonged low-flow priapism.
- High-flow priapism (also called nonischemic priapism) – Less common, this form of disease occurs most commonly with trauma (penile, perineal or pelvic.) This form of priapism does not pose a threat to the future heath of the penis.
- Stuttering priapism – This type of priapism is similar to low-blood flow priapism except that it is episodic. The re-occurring, painful erections usually last between 2 and 3 hours before returning to a flaccid (soft or limp) state. If you have this type of priapism, it may occur during sleep, or before or after sexual stimulation. Over time, the episodes of priapism may become more frequent and last longer. Like low blood flow priapism, this type of priapism can cause permanent damage to the penis and affect your sexual function. It is important to seek medical treatment if this is happening to you.
Low flow priapism begins with the development of a painful persistent erection, with stimulation or sexual desire. The penis will remain erect and at significant risk of permanent damage, unless the patient seeks medical aid to restore normal blood flow to the penis. With adequate therapy, the patient will retain his erectile function. If therapy remains inadequate or is provided too late, the patient may suffer permanent damage and long-term impotence.
Priapism is exceedingly rare when the entire population is considered. The incidence in patient’s being treated for erectile dysfunction, however, varies between 0.5 and 6%. This is because the most common cause of priapism is the use of agents to treat erectile dysfunction.
The condition may occur in any age group, but most common occurs at 19-21 years of age in those with sickle cell disease induced priapism.
The most common cause of priapism are drugs used in the treatment of erectile dysfunction or impotence. Those drugs which are directly injected into the penis place the patient at most risk of this condition.
Priapism can be a side effect of medicines used to treat erectile dysfunction. You should take medicines for erection problems only if they are prescribed by an authorised health practitioner, such as your doctor or erectile specialist. Medicines bought on the internet may be of poor quality and may contain ingredients that are not safe when taken in combination with other medicines you are on. They may also be unsafe due to other health problems you have.
About 25% of priapism cases are associated with co-existing medical conditions such as:
- Advanced cancer,
- Leukemia and
- Sickle cell anemia and other hemoglobin disorders
- Treatment for erectile dysfunction (particularly penile injections)
- Use of anti-coagulant and some psychiatric medications
- Fabry’s disease
Other cases may be related to recent trauma, but the majority of patients have not predisposing factors, occurring spontaneously.
If you have had an erection that has lasted more than two hours, you should go to the nearest emergency department for medical attention.
The emergency room doctor will determine whether you have ischemic priapism or nonischemic priapism. This is necessary because the treatment for each is different, and treatment for ischemic priapism needs to be done as soon as possible.
If you experience recurrent, persistent, painful erections that resolve on their own, see your doctor. You might need treatment to prevent further episodes.
What is the penis?
Men’s penis is used for urination and sexual intercourse. The penis is made up of two erectile or spongelike cylinders called corpora cavernosa, that enlarge with blood during erection. During sexual arousal, nerve impulses increase blood flow to both of these cylinders (corpora cavernosa). This sudden influx of blood causes an erection by expanding, straightening and stiffening the penis. A tough fibrous, partially elastic outer casing surrounds the cavernosa. The corpus spongiosum surrounds the urethra (urinary tube), a tube that runs from the bladder to the end of the penis. The urethra carries urine and semen out of the body.
Figure 1. Male reproductive system
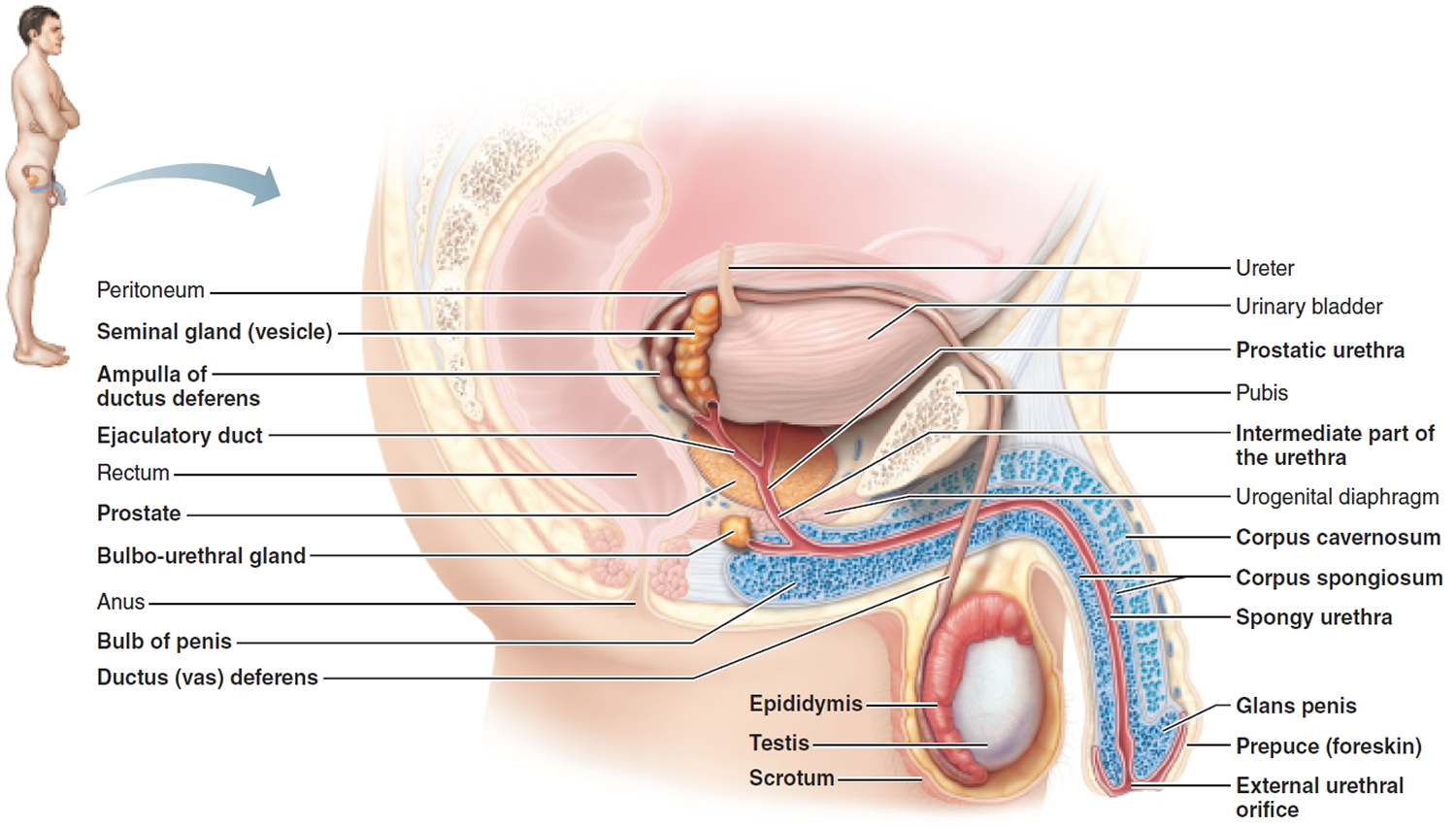
Figure 2. Flaccid and erect penis
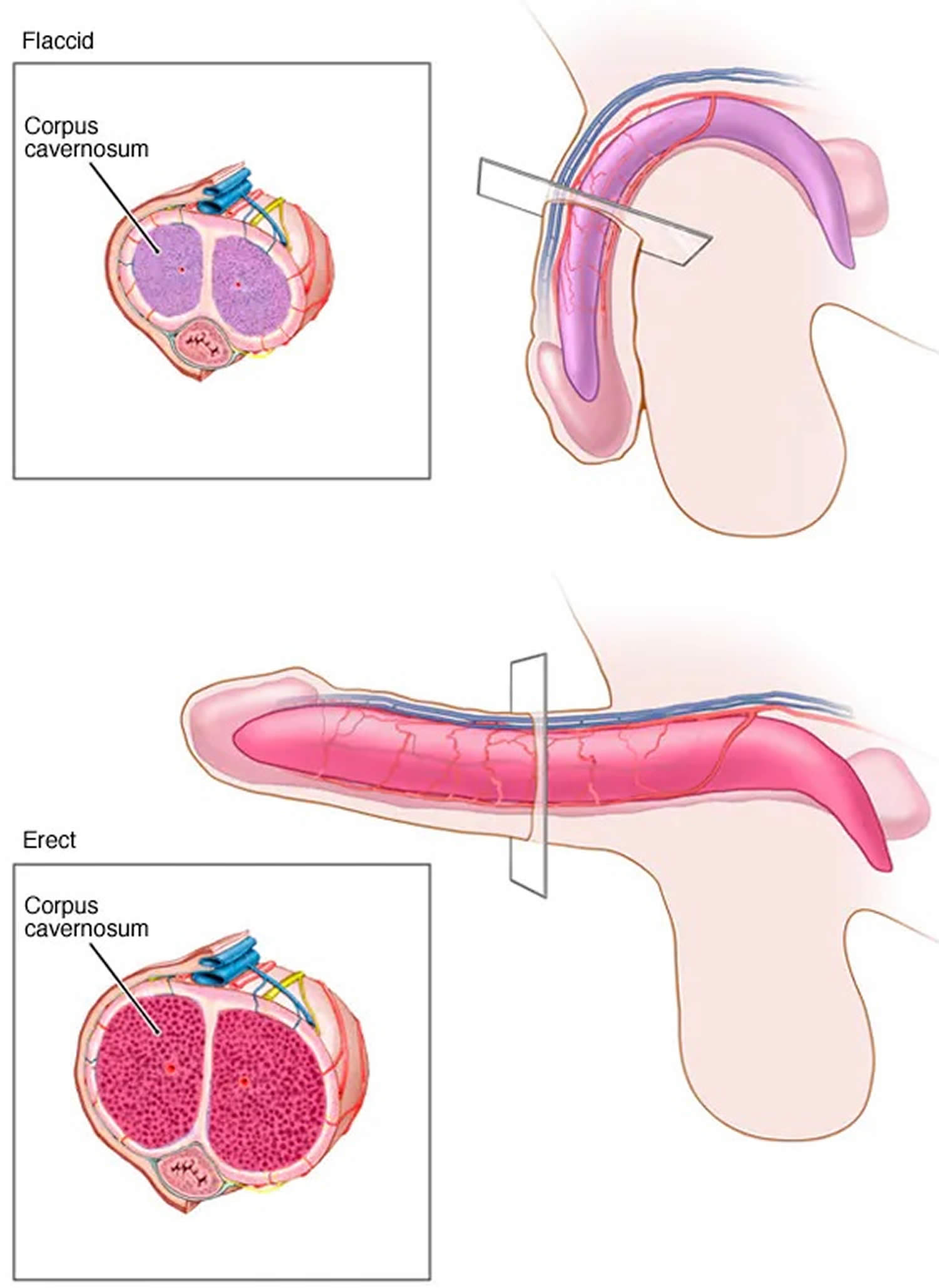
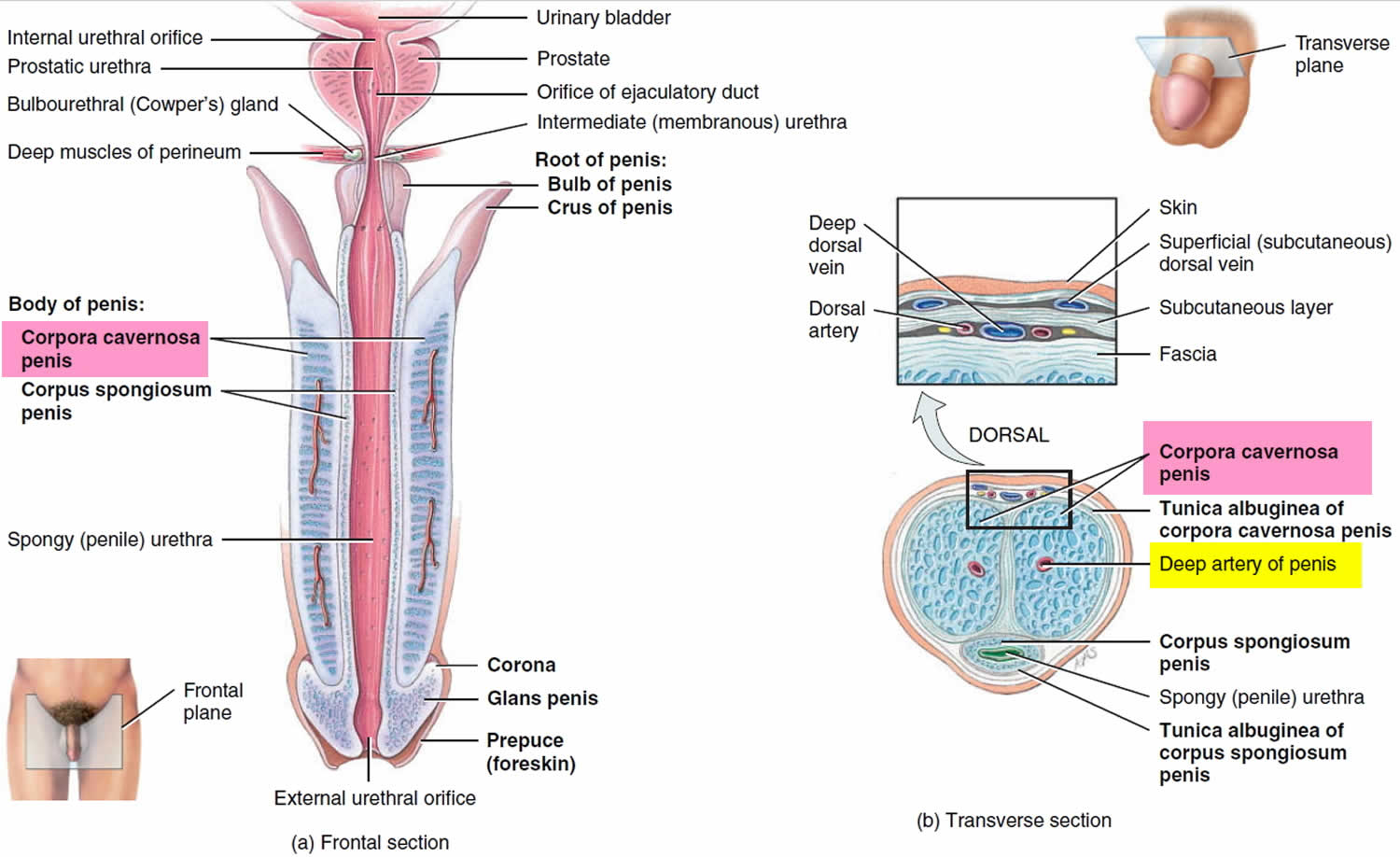
Figure 3. Penis (cross section)
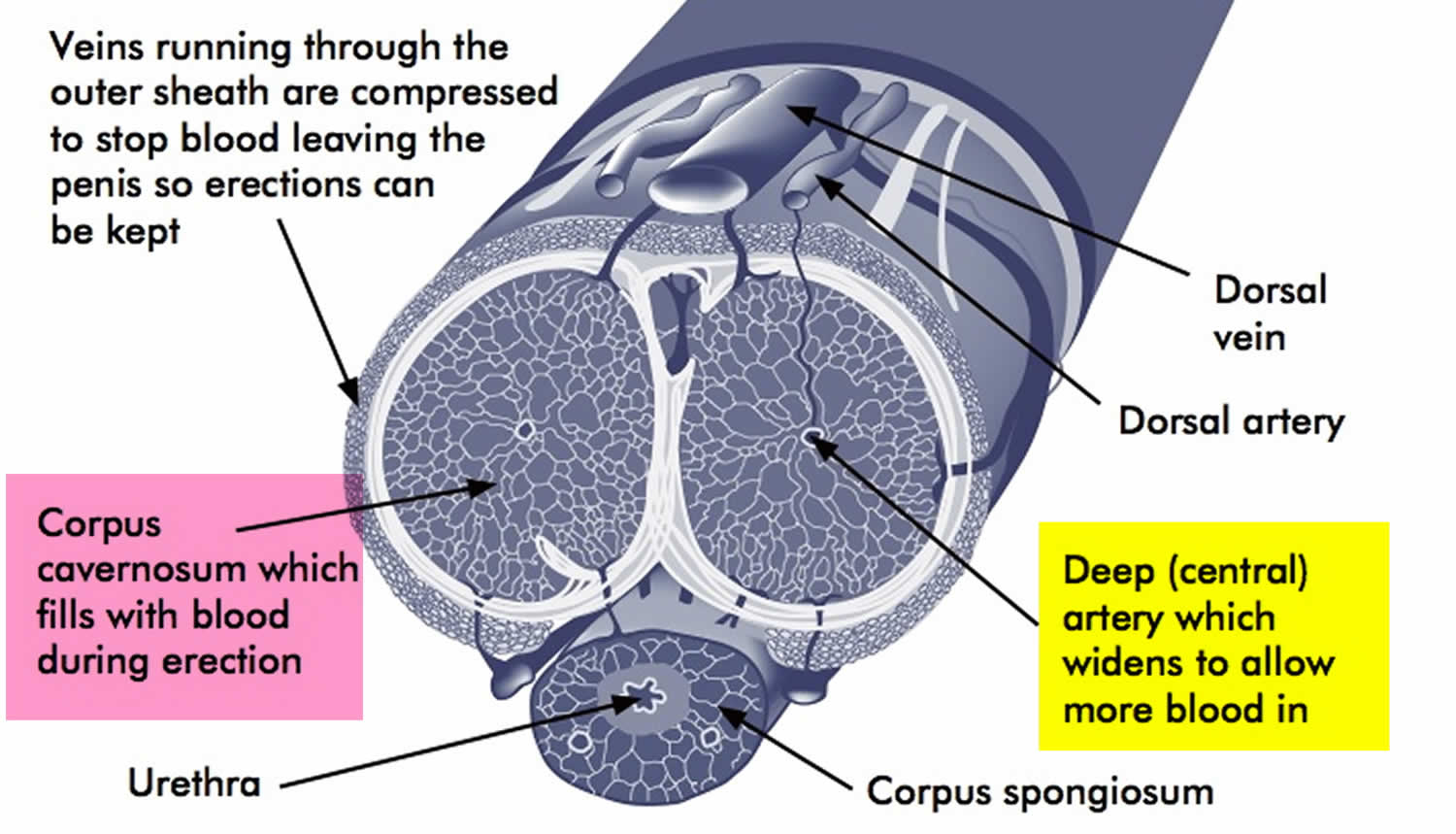
Footnote: The penis contains two cylindrical, spongelike structures (corpora cavernosa). During sexual arousal, nerve impulses increase blood flow to both of these cylinders. This sudden influx of blood causes an erection by expanding, straightening and stiffening the penis.
Priapism prognosis
The prognosis of low-flow priapism depends largely on the time taken to restore normal blood flow to the penis. If treatment is initiated early and is successful, the patient will retain normal erectile function and appearance. If treatment is delayed or unsuccessful, the patient may suffer irreversible penile damage and loss of erectile function.
The prognosis of high-flow priapism is generally good, for the blood supply to the penis is not compromised, only deranged. The penis is not at risk of major damage, and thus many physicians prefer to treat this condition is a “wait-and-see” manner, with the condition settling by itself in many cases.
Priapism causes
An erection normally occurs in response to physical or psychological stimulation. This stimulation causes certain blood vessels and smooth muscles to relax and/or expand, increasing blood flow to spongy tissues in the penis. Consequently, the blood-filled penis becomes erect. After stimulation ends, the blood flows out and the penis returns to its nonrigid (flaccid) state.
Priapism occurs when some part of this system — the blood, blood vessels, smooth muscles or nerves — changes normal blood flow. Subsequently, the erection persists. While the underlying cause of priapism often can’t be determined, several conditions are believed to play a role.
Blood disorders
Blood-related diseases might contribute to priapism — usually ischemic priapism, when blood isn’t able to flow out of the penis.
These disorders include:
- Sickle cell anemia
- Leukemia
- Other hematologic dyscrasias, such as thalassemia, multiple myeloma and others
Priapism most commonly affects children is sickle cell anemia.
Less common causes include:
- blood-thinning medicines, like warfarin and heparin
- some antidepressants
- recreational drugs, like cannabis, methamphetamine (crystal meth) and cocaine
- some medicines for high blood pressure
- other blood disorders, like thalassemia and leukemia
- some treatments for erection problems
- conditions that affect the nervous system and so indirectly affect blood flow to the penis, such as brain or spinal cord tumors or injury.
- tumors of the prostate, bladder or kidney, which can upset blood flow to the penis
- infections in the genitals, such as prostatitis or urethritis.
Prescription medications
Priapism, usually ischemic priapism, is a possible side effect of a number of drugs, including:
- Medications injected directly into the penis to treat erectile dysfunction, such as alprostadil, papaverine, phentolamine and others
- Antidepressants, such as fluoxetine (Prozac), bupropion (Wellbutrin), and sertraline
- Alpha blockers including prazosin, terazosin, doxazosin and tamsulosin
- Medications used to treat anxiety or psychotic disorders, such as hydroxyzine, risperidone (Risperdal), olanzapine (Zyprexa), lithium, clozapine, chlorpromazine and thioridazine
- Blood thinners, such as warfarin (Coumadin) and heparin
- Hormones such as testosterone, tamoxifen or gonadotropin-releasing hormone
- Medications used to treat attention-deficit/hyperactivity disorder (ADHD), such as atomoxetine (Strattera) and methylphenidate (Ritalin, Concerta)
Alcohol and drug use
Alcohol, marijuana, cocaine and other illicit drug abuse can cause priapism, particularly ischemic priapism.
Injury
A common cause of nonischemic priapism — a persistent erection caused by excessive blood flow into the penis — is trauma or injury to your penis, pelvis or perineum, the region between the base of the penis and the anus.
Other factors
Other causes of priapism include:
- A spider bite, scorpion sting or other toxic infections
- Metabolic disorders including gout or amyloidosis
- Neurogenic disorders, such as a spinal cord injury or syphilis
- Cancers involving the penis.
Priapism prevention
If you have recurrent or stuttering priapism, to prevent future episodes your doctor might recommend:
- Treatment for an underlying condition, such as sickle cell anemia, that might have caused priapism
- Use of oral or injectable phenylephrine
- Hormone-blocking medications — only for adult men
- Use of oral medications used to manage erectile dysfunction
Priapism symptoms
Priapism symptoms vary depending on the type of priapism. The two main types of priapism are ischemic and nonischemic priapism.
Low-flow priapism (ischemic priapism)
Ischemic priapism, also called low-flow priapism, is the result of blood not being able to leave the penis. It’s the more common type of priapism. Signs and symptoms include:
- Erection lasting more than four hours or unrelated to sexual interest or stimulation
- Rigid penile shaft, but the tip of penis (glans) is soft
- Progressive penile pain
Recurrent or stuttering priapism, a form of ischemic priapism, is an uncommon condition. It’s more common in males who have an inherited disorder characterized by abnormally shaped red blood cells (sickle cell anemia). Sickle cells can block the blood vessels in the penis. Recurrent priapism describes repetitive episodes of prolonged erections and often includes episodes of ischemic priapism. In some cases, the condition starts off with unwanted and painful erections of short duration and might progress over time to more frequent and more prolonged erections.
High-flow priapism (nonischemic priapism)
Nonischemic priapism, also known as high-flow priapism, occurs when penile blood flow isn’t regulated appropriately. Nonischemic priapism is usually painless. Signs and symptoms include:
- Erection lasting more than four hours or unrelated to sexual interest or stimulation
- Erect but not fully rigid penile shaft
Priapism complications
Ischemic priapism can cause serious complications. The blood trapped in the penis is deprived of oxygen. When an erection lasts for too long, this oxygen-poor blood can begin to damage or destroy tissues in the penis. As a result, untreated priapism can cause erectile dysfunction.
Priapism diagnosis
If you have an erection lasting more than four hours, you need emergency care. The emergency room doctor will determine whether you have ischemic priapism or nonischemic priapism. This is necessary because the treatment for each is different, and treatment for ischemic priapism needs to be done as soon as possible.
Medical history and exam
To determine what type of priapism you have, your doctor will ask questions and examine your genitals, abdomen, groin and perineum. He or she might be able to determine what type of priapism you have based on whether you’re experiencing pain and the rigidity of the penis. This exam might also reveal the presence of a tumor or signs of trauma.
Diagnosis tests
Diagnostic tests might be needed to determine what type of priapism you have. Additional tests might identify the cause of priapism. In an emergency room setting, your treatment will likely begin before all test results are received. Diagnostic tests can include:
- Blood gas measurement. In this test, a tiny needle is inserted into your penis to remove a sample of blood – this helps determine whether your priapism is low or high-blood flow priapism. If the blood is black — deprived of oxygen — the condition is most likely ischemic priapism (low-flow priapism). If it’s bright red, the priapism is more likely nonischemic (high-flow priapism). A lab test measuring the amounts of certain gases in the blood can confirm the type of priapism.
- Blood tests. Your blood can be tested to measure the number of red blood cells and platelets present. Results might show evidence of diseases, such as sickle cell anemia, other blood disorders or certain cancers.
- Ultrasound. You might have Doppler ultrasonography, a noninvasive test that can be used to estimate your blood flow through blood vessels by bouncing high-frequency sound waves (ultrasound) off circulating red blood cells. This test can be used to measure blood flow within your penis that would suggest ischemic or nonischemic priapism. The exam might also reveal an injury or abnormality that might be an underlying cause.
- Toxicology test. Your doctor might order a urine test to screen for drugs that might be the cause of priapism.
Priapism treatment
Hospital treatment for priapism
Treatments to help reduce your erection include:
- tablets or injections directly into your penis
- using a needle to drain blood from your penis, done while the area is numbed under local anesthetic
- surgery to drain the blood through a tiny cut, done while you’re asleep under general anesthetic
- If you have stuttering priapism, you may be given medicines to prevent further episodes. This could be short-term self-injection with a medicine called phenylephrine to control blood flow to the penis when priapism occurs. Another option is a course of hormone treatment that helps reduce your testosterone levels. This therapy is only recommended for adults.
Low-flow priapism (Ischemic priapism)
Ischemic priapism — the result of blood not being able to exit the penis — is an emergency situation that requires immediate treatment. This treatment usually begins with a combination of draining blood from the penis and using medications.
Excess blood is drained from your penis using a small needle and syringe (aspiration). As part of this procedure, the penis might also be flushed with a saline solution. This treatment often relieves pain, removes oxygen-poor blood and might stop the erection. This treatment might be repeated until the erection ends.
They may also inject a vasoconstrictor agent (a medicine used to narrow blood vessels). If this approach doesn’t work, you may need to have urgent surgery.
Medications
A sympathomimetic medication, such as phenylephrine, might be injected into the penis. This drug constricts blood vessels that carry blood into the penis. This action allows blood vessels that carry blood out of the penis to open up and allow increased blood flow out. This treatment might be repeated several times if needed. You will be monitored for side effects, such as a headache, dizziness and high blood pressure, particularly if you have high blood pressure or heart disease.
- Supportive measures – Analgesia such as morphine and anxiolytics such as diazepam to reduce patient anxiety.
- Conservative measures – Exercise, ice and ejaculation have proven effective in some cases of this condition and should be tried before surgery.
- Medical techniques – Antiandrogens, digoxin and alpha-blockers have been advocated in the treatment of priapism.
Surgical or other procedures
If other treatments aren’t successful, a surgeon might perform surgery to reroute blood flow so that blood can move through your penis normally.
If you have a blood clot in the penis, you will need to have surgery to remove it so that blood can flow normally through the penis again.
If you have sickle cell anemia, you might receive additional treatments that are used to treat disease-related episodes.
- Surgical techniques – The surgical procedures used for this condition all aim to create an anastomosis between the corpus cavernosum and another vascular chamber of the penis. Initially, a connection is attempted between the glans and the cavernsum in the Winter and Ebbehoj procedures. If this fails (which occurs in 1/3) a more permanent connection between the corpus cavernosum and corpus spongiosum is fashioned. This is technique is more effective than the former, but the occurrence of iatrogenic impotence is far greater.
- Sickle cell patients – This group of patients may require a specific regime of therapy to treatment their sickle cell disease, including oxygenation, hydration, alkalinization, analgesia and exchange transfusion.
High-flow priapism (Nonischemic priapism)
Nonischemic priapism often goes away with no treatment. Because there isn’t a risk of damage to the penis, your doctor might suggest a watch-and-wait approach. Putting ice packs and pressure on the perineum — the region between the base of the penis and the anus — might help end the erection.
- Expectant approach – As the condition poses little threat to erectile function or appearance, the patient may only be observed, as the condition may resolve on its own accord.
- Interventional radiology – The use of specialized techniques may hasten the resolution of this condition, which does not pose significant threat to erectile function or appearance. These procedures aim to dissolve any clot that induces anomalous blood flow through the penis, causing high-flow priapism.
Surgical or other procedures
Surgery might be necessary in some cases to insert material, such as an absorbable gel, that temporarily blocks blood flow to your penis. Your body eventually absorbs the material. Surgery might also be necessary to repair arteries or tissue damage resulting from an injury.
- Surgical intervention – If the condition does not resolve with conventional therapy, surgery is the only other option available. Those blood vessels responsible for the condition are located by ultrasound and removed in surgery.
Priapism home treatment
Priapism may get better on its own within 2 hours. If an erection is painful, you can use an ice-pack to relieve the swelling. But it should not be placed directly against the skin – try wrapping a bag of frozen peas in a cloth (such as a tea towel) and mould this around the swollen area and the perineum (the area between the base of the penis and the anus).
Other things you can try to reduce your erection:
- Try to go for a pee
- Have a warm bath or shower
- Drink lots of water
- Go for a gentle walk
- Try vigorous exercise such as climbing stairs or running on the spot
- Take painkillers like paracetamol if you need to
DON’T
- apply ice packs or cold water to your penis – this can make things worse
- have sex or masturbate – it won’t make your erection go away
- drink alcohol
- smoke





{kind=link}