What is prothrombin
Prothrombin is a clotting factor II (clotting factor 2), which is a modular protein composed of 579 amino acids 1. In plasma, prothrombin (clotting factor II) circulates in two forms at equilibrium, “closed” (~80%) and “open” (~20%), brokered by the flexibility of the linker regions 2. In response to vascular injury, prothrombin (coagulation factor II), is converted to its active form thrombin by prothrombinase complex, a macromolecular complex composed of factor Xa (fXa), factor Va (fVa), calcium ions, and phospholipids 3. Once in the circulation, thrombin converts fibrinogen into fibrin, activates platelets and increases endothelial permeability thereby halting the loss of blood at the site of injury 4 and facilitating vascular remodeling. Because of this critical role in biology, the prothrombin/thrombin axis remains an attractive target for anticoagulant therapy 5.
Prothrombin is synthesized by the hepatocytes in the liver as a single pre/pro-polypeptide composed of 622 amino acids 6, although elevated mRNA levels have also been detected in neurons and glia cells suggesting important yet unexplored roles of this protein in the central nervous system 7. Before secretion into the plasma, prothrombin undergoes extensive post-translational modifications including removal of the pre/pro peptide at the N-terminus (43 amino acids), addition of three N-glycosylations at positions 78, 100, and 373 and conversion of the first 10 residues of glutamic acid (Glu) to γ-carboxy glutamic acid (Gla) 6. The presence of glycans at position 373 increases the thermodynamic stability of the protein and confers protection to proteolysis without affecting the catalytic activity of thrombin 8. The role of the other two N-glycosylations at positions 78 and 100 remains unclear. The 10 Gla residues provide a calcium-dependent anchoring point to negatively charged phospholipid. Since prothrombin conversion to thrombin occurs on the membranes, pharmacological inhibition of the γ-carboxyl transfer reaction in the liver by vitamin K analogs, such as warfarin, represents an effective and widespread strategy to achieve profound anticoagulation in clinical practice 9. Likewise, mutations Glu7→ Lys in prothrombin Nijmegen and Glu29→ Gly in prothrombin Shanghai are associated with a severe bleeding disorders 10.
The mature form of prothrombin circulates in the plasma at a concentration of 0.1 mg/ml and has a half-life of about 60 hours 11. It contains four domains connected by three intervening linkers, Lnk1 (residues 47–64), Lnk2 (residues 144–169), and Lnk3 (residues 249–284) totaling 579 amino acids (Figure 1) 12. The N-terminal Gla-domain (residues 1–46), named after the posttranslational modifications, is followed by two kringles, kringle-1 (residues 65–143) and kringle-2 (residues 170–248), and a canonical protease domain (residues 285–579). The protease domain contains the A chain (residues 285–320) and the B chain (residues 321–579) which are connected by a conserved disulfide bond (Cys293–Cys439). The catalytic triad (His363, Asp419, and Ser525) is hosted in the B-chain and strategically located in a deep pocket surrounded by flexible loops that control access to and steer substrates toward the active site 13.
Figure 1. Prothrombin (closed structure)
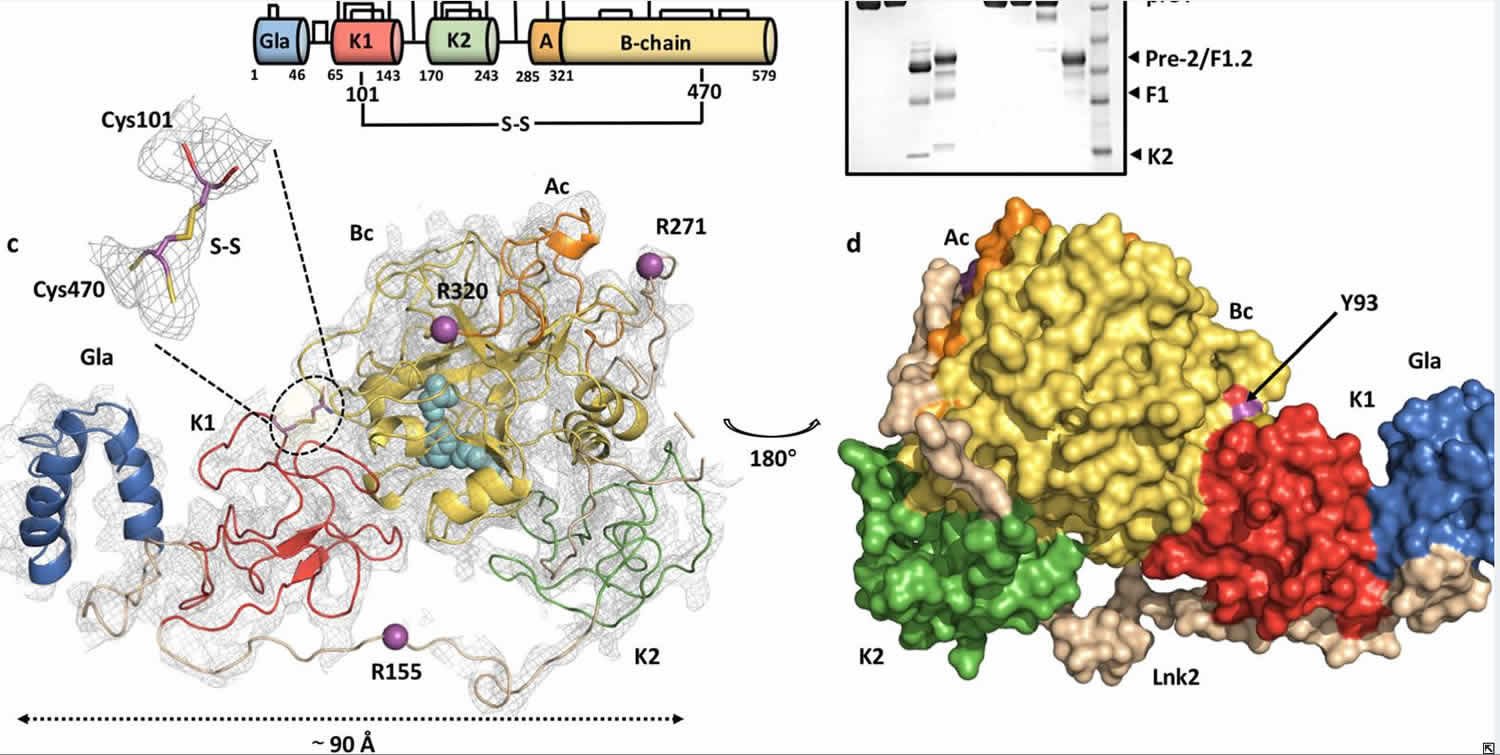
Footnote: (a) Color-coded domain architecture of prothrombin displaying the location of the engineered disulfide bond linking kringle-1 with the protease domain. Natural disulfide bonds are shown as black lines and positioning of the cleavage sites are indicated. (b) Limited proteolysis of protWT (lanes 0–4) and proTCC (lanes 5–8) by fXa (100 nM) in the absence (−) and presence (+) of reducing agent. Shown are times 0 (lanes 1–2 and 5–6, 6 μg) and 120 min (lanes 3–4 and 7–8, 2.5 μg). The MW marker is shown in lane 9 (62,49,38,28,17 kDa). The full-length gel is presented in Supplementary Fig. 5. (c) Overall structure of proTCC solved at 4.1 Å resolution colored as in a shown as cartoon (left) or surface (right) after 180° rotation. The key residue Tyr93 sits at the interface between kringle-1 and the protease domain. fXa cleavage sites Arg155, Arg271 and Arg320 are shown as spheres (magenta). The catalytic triad His363, Asp419 and Ser525 is shown as spheres (cyan). Zoom-in view of the artificial disulfide bond Cys101-Cys470. The electron density 2Fo-Fc map is countered at 1.5σ.
[Source 14 ]Blood coagulation process
Blood is a necessary component of the human body, and the loss of this fluid may be life-threatening. The human body protects against loss of blood through the clotting mechanism. Vascular mechanisms, platelets, coagulation factors, prostaglandins, enzymes, and proteins are the contributors to the clotting mechanism which act together to form clots and stop a loss of blood 15. Through vasoconstriction, adhesion, activation, and aggregation, the contributors form a transient plug to act as the cork to the leaking blood flow. Soon after, fibrin, the functioning form of fibrinogen, stabilizes this weak platelet plug.
The cellular components of the clotting mechanism include platelets, endothelial cells, and a series of proteins, enzymes, and ions.
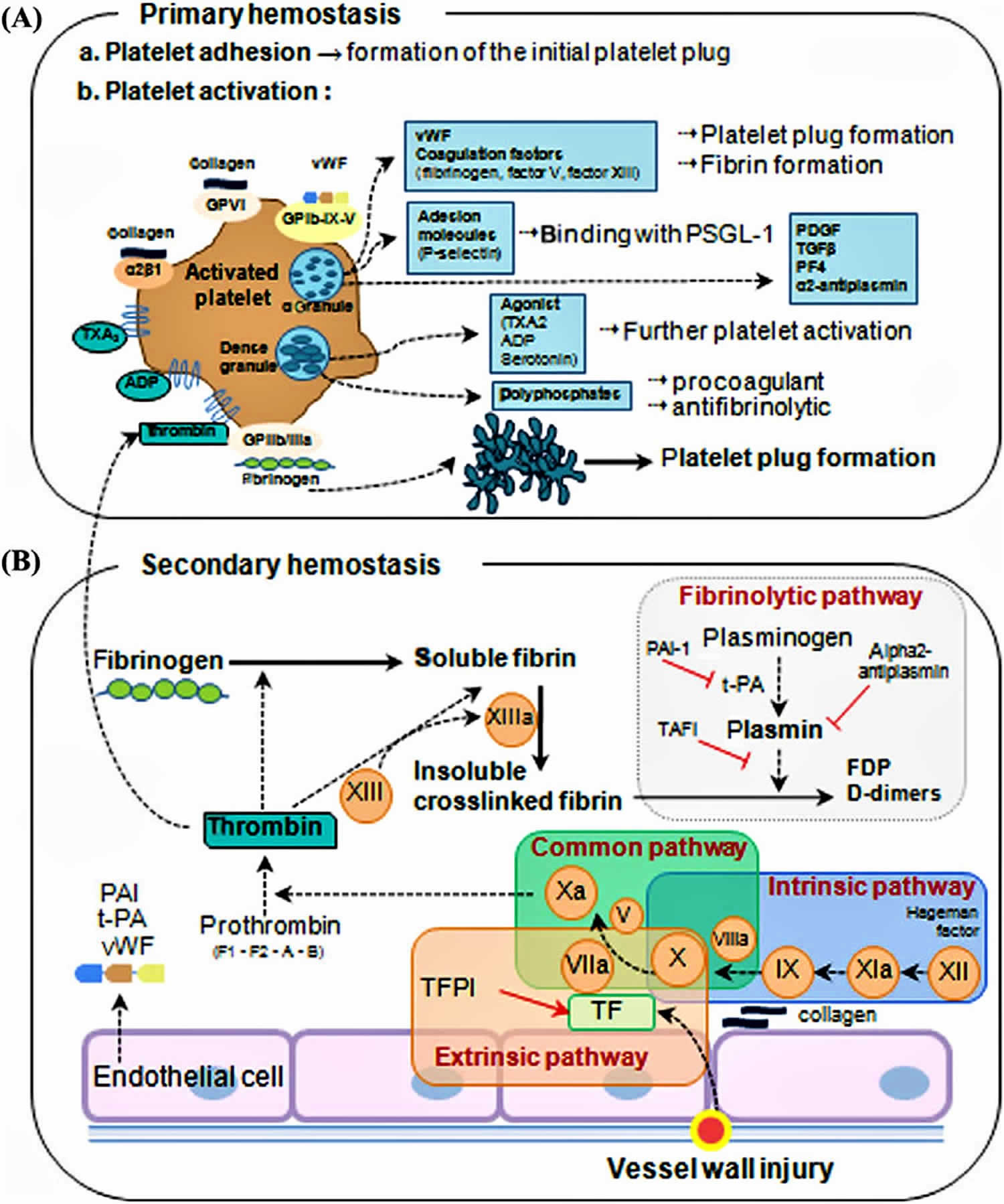
The clotting mechanism is broken into 2 stages:
- Primary hemostasis: Formation of a weak platelet plug
- Secondary hemostasis: Stabilizing the weak platelet plug into a clot by the fibrin network
Figure 2. Overview of blood coagulation
Secondary hemostasis
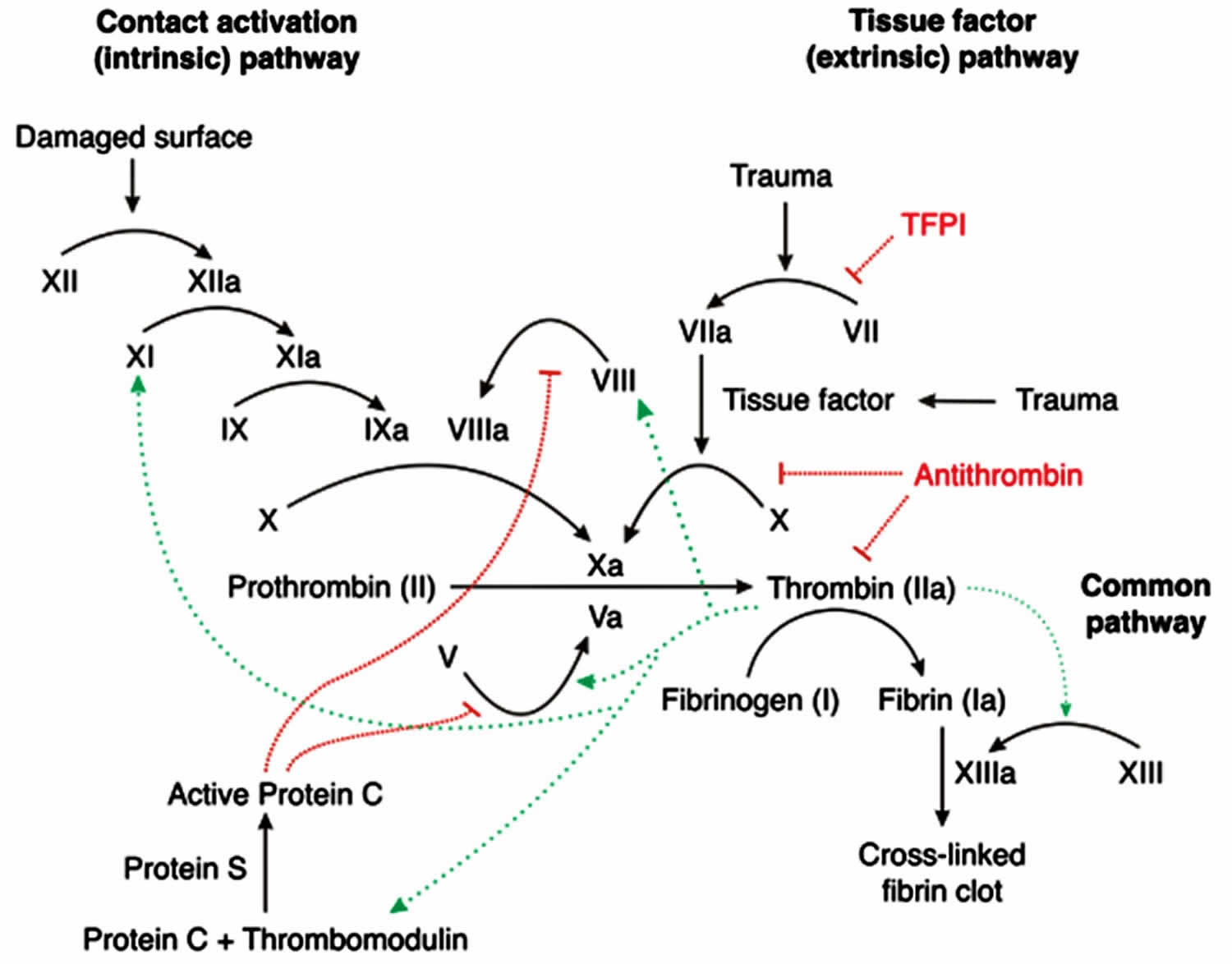
Secondary hemostasis involves the clotting factors acting in a cascade to ultimately stabilize the weak platelet plug. This is accomplished by completing three tasks: (1) triggering activation of clotting factors, (2) conversion of prothrombin to thrombin, and (3) conversion of fibrinogen to fibrin. These tasks are accomplished initially by 1 of 2 pathways; the extrinsic and intrinsic pathway, which converge at the activation of factor X and then complete their tasks via the common pathway. Please note that calcium ions are required for the entire process of secondary hemostasis.
The extrinsic pathway includes tissue factor (TF) and factor VII (FVII). It is initiated when tissue factor (TF) binds to factor VII (FVII), activating FVII to factor VIIa (FVIIa), forming a TF-FVIIa complex. This complex, in turn, activates factor X (FX). Note, the TF-FVIIa complex can also activate factor IX of the intrinsic pathway, which is called the alternate pathway. Once Factor X is activated to FXa by TF-FVIIa complex, the cascade continues down the common pathway (see below).
The intrinsic pathway includes Hageman factor (FXII), factor I (FXI), factor IX (FIX), and factor VIII (FVIII). The process is initiated when FXII comes into contact with exposed subendothelial collagen and becomes activated to FXIIa. Subsequently, FXIIa activates FXI to FXIa, and FXIa activates FIX to FIXa. FIXa works in combination with activated factor VIII (FVIIIa) to activate factor X. Once Factor X is activated by FIXa-FVIIIa complex, the cascade continues down the common pathway (see below).
The common pathway is initiated via activation of Factor Xa. Factor Xa combines with Factor Va and calcium on phospholipid surfaces to create a prothrombinase complex ultimately activating prothrombin (coagulation factor II) into thrombin. This activation of thrombin occurs via serine protease cleaving of prothrombin. Now, thrombin activates factor XIIIa (FXIIIa). FXIIIa crosslinks with fibrin forming the stabilized clot.
Figure 3. Coagulation cascade
Prothrombin gene mutation
In humans, prothrombin is encoded by the F2 gene, which is located on the short arm of chromosome 11, at position 11.2 5. The F2 gene contains 14 exons spanning 21 kb, and its structural integrity is critical for life. Single-nucleotide polymorphisms (SNPs) found in patients are often associated with moderate to severe bleeding phenotypes and the mutation G20210A in the 3′ untranslated region of the F2 gene is a well-established risk factor for prothrombin thrombophilia 10.
Prothrombin thrombophilia
Prothrombin thrombophilia is an inherited disorder of blood clotting. Prothrombin thrombophilia is caused by a particular mutation (written G20210A or 20210G>A) in the F2 gene. People can inherit one or two copies of the gene mutation from their parents 16. The treatment for prothrombin thrombophilia is dependent on whether a blood clot has occurred and if there are additional risk factors. In individuals with a history of one or more blood clots, blood thinning medications may be used 17.
Thrombophilia is an increased tendency to form abnormal blood clots in blood vessels 16. People who have prothrombin thrombophilia are at somewhat higher than average risk for a type of clot called a deep venous thrombosis, which typically occurs in the deep veins of the legs. Affected people also have an increased risk of developing a pulmonary embolism, which is a clot that travels through the bloodstream and lodges in the lungs. Most people with prothrombin thrombophilia never develop abnormal blood clots, however.
Prothrombin thrombophilia is the second most common inherited form of thrombophilia after factor V Leiden thrombophilia 16. Approximately 1 in 50 people in the white population in the United States and Europe has prothrombin thrombophilia. This condition is less common in other ethnic groups, occurring in less than one percent of African American, Native American, or Asian populations.
Some research suggests that prothrombin thrombophilia is associated with a somewhat increased risk of pregnancy loss (miscarriage) and may also increase the risk of other complications during pregnancy. These complications may include pregnancy-induced high blood pressure (preeclampsia), slow fetal growth, and early separation of the placenta from the uterine wall (placental abruption). It is important to note, however, that most women with prothrombin thrombophilia have normal pregnancies.
How is prothrombin thrombophilia inherited?
Prothrombin thrombophilia is inherited in an autosomal dominant manner 18. This means that having one mutated copy of the disease-causing gene (F2) in each cell may be sufficient to cause signs or symptoms of the condition. The mutation in the F2 gene that causes prothrombin thrombophilia is called 20210G>A (also called the 20210G>A allele). An individual can be heterozygous (having the mutation in only one copy of the F2 gene) or homozygous (having a mutation in both copies of the F2 gene). Heterozygosity results in an increased risk for thrombosis; homozygosity results in more severe thrombophilia and/or increased risk for thrombosis 17.
The risk of developing an abnormal clot in a blood vessel depends on whether a person inherits one or two copies of the F2 gene mutation that causes prothrombin thrombophilia. In the general population, the risk of developing an abnormal blood clot is about 1 in 1,000 people per year 16. Inheriting one copy of the F2 gene mutation increases that risk to 2 to 3 in 1,000 16. People who inherit two copies of the mutation, one from each parent, may have a risk as high as 20 in 1,000 16.
All individuals reported to date with prothrombin thrombophilia who are heterozygous for the 20210G>A allele have had an affected parent. Because of the relatively high prevalence of this allele in the general population, occasionally one parent is homozygous or both parents are heterozygous for this allele 17.
When an individual who is heterozygous for the 20210G>A allele has children, each child has a 50% (1 in 2) risk to inherit that allele and also be heterozygous. An individual who is homozygous will always pass one of the 20210G>A alleles to each of his/her children. If two heterozygotes have children together, each child has a 25% (1 in 4) risk to be homozygous (having 2 mutated copies), a 50% risk to be heterozygous like each parent, and a 25% risk to inherit 2 normal copies of the F2 gene.
Prothrombin thrombophilia diagnosis
No clinical signs or symptoms are specific for prothrombin thrombophilia. A confirmed diagnosis of this condition requires specific genetic testing via DNA analysis of the F2 gene, which provides instructions for making the protein prothrombin. The test identifies the presence of a common change (mutation) called 20210G>A 17. An individual can be a heterozygote (having one mutated copy of the F2 gene) or a homozygote (having two mutated copies).
Most heterozygotes have a mildly elevated plasma concentration of prothrombin (which can be measured in a blood test) that is approximately 30% higher than normal. However, these values can vary greatly, and the range of prothrombin concentrations in heterozygotes overlaps significantly with the normal range. Therefore, plasma concentration of prothrombin is not reliable for diagnosis of this condition 17.
Individuals interested in learning more about testing for prothrombin thrombophilia should speak with a genetics professional or other healthcare provider.
Prothrombin deficiency
Prothrombin deficiency is a very rare bleeding disorder that slows the blood clotting process 19. Prothrombin deficiency is estimated to affect 1 in 2 million people in the general population 19. People with prothrombin deficiency often experience prolonged bleeding following an injury, surgery, or having a tooth pulled. In severe cases of prothrombin deficiency, heavy bleeding occurs after minor trauma or even in the absence of injury (spontaneous bleeding). Women with prothrombin deficiency can have prolonged and sometimes abnormally heavy menstrual bleeding. Serious complications can result from bleeding into the joints, muscles, brain, or other internal organs. Milder forms of prothrombin deficiency do not involve spontaneous bleeding, and the condition may only become apparent following surgery or a serious injury.
Prothrombin deficiency is caused by changes (mutations) in the F2 gene 19. There are two types of inherited prothrombin deficiency. Type I or hypoprothrombinemia and type II or dysprothrombinemia. Inheritance of both types is autosomal recessive 20. Type I or hypoprothrombinemia is more severe, and it is characterized by a decreased level of normally functioning protein, and therefore, by a decrease in proteinactivity. Type II or dysprothrombinemia is characterized by normal or low-normal levels of an abnormal (dysfunctional) protein. Bleeding symptoms vary depending on the amount of residual functional activity 20.
In other cases, prothrombin deficiency is acquired. This means that prothrombin deficiency develops later in life and is not caused by a genetic change. Potential causes of acquired prothrombin deficiency include severe liver disease, vitamin K deficiency, or an autoimmune response that prevents the prothrombin protein from working properly 21.
Diagnosis is based on laboratory test results that are consistent with the prothrombin deficiency.
The treatment of prothrombin deficiency depends on the exact cause and severity of the disease. When a person with prothrombin (factor II) deficiency has bleeding episodes, fresh frozen plasma, the part of the blood that contains the blood clotting factors, can be used to treat the bleeding. If a person with prothrombin deficiency requires surgery, plasma exchange therapy may be used to increase factor II (prothrombin) levels prior to surgery. People who have acquired prothrombin deficiency may benefit from taking vitamin K. Some people with prothrombin deficiency may be recommended to avoid activities that can result in physical contact or injuries 21. In some cases, prothrombin complex concentrates can be used to increase factor II levels. However, because these concentrates contain clotting factors other than factor II, they can result in an increased risk for blood to clot too quickly within the blood vessels (thromboembolic event) 21
A form of the disease that is not inherited (acquired) can be caused by vitamin K deficiency, liver disease, or an autoimmune response. The underlying cause of acquired prothrombin deficiency should be treated in order to relieve symptoms of the disease 21.
How is prothrombin deficiency inherited?
Prothrombin deficiency is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.
What is prothrombin time
Prothrombin time (PT) is a blood test that measures the time it takes for the liquid portion (plasma) of your blood to clot. The prothrombin time is a test that helps evaluate a person’s ability to appropriately form blood clots. The international normalized ratio (INR) is a calculation based on results of a prothrombin time that is used to monitor individuals who are being treated with the blood-thinning medication (anticoagulant) warfarin (Coumadin®). A related blood test is partial thromboplastin time (PTT).
A prothrombin time measures the number of seconds it takes for a clot to form in a person’s sample of blood after substances (reagents) are added. The prothrombin time is often performed with a partial thromboplastin time (PTT) and together they assess the amount and function of proteins called coagulation factors that are an important part of proper blood clot formation.
In your body, when there is an injury and bleeding occurs, the clotting process called hemostasis begins. This process involves in part a series of sequential chemical reactions called the coagulation cascade, in which coagulation or “clotting” factors are activated one after another and result in the formation of a clot. There must be a sufficient quantity of each coagulation factor, and each must function properly, in order for normal clotting to occur. Too little can lead to excessive bleeding; too much may lead to excessive clotting.
In a test tube during a laboratory test, there are two “pathways” that can initiate clotting, the so-called extrinsic and intrinsic pathways. Both of these then merge into a common pathway to complete the clotting process. The prothrombin time test evaluates how well all of the coagulation factors in the extrinsic and common pathways of the coagulation cascade work together. Included are: factors I (Fibrinogen), II (Prothrombin), V, VII and X. The PTT test evaluates those protein factors that are part of the intrinsic and common pathways: XII, XI, IX, VIII, X, V, II (prothrombin), and I (fibrinogen) as well as prekallikrein (PK) and high molecular weight kininogen (HK). The prothrombin time and PTT evaluate the overall ability to produce a clot in a reasonable amount of time and, if any of these factors are deficient in quantity or not functioning properly, the test results will be prolonged.
The prothrombin time test is usually measured in seconds and is compared to a normal range that reflects prothrombin time values in healthy individuals. Because the reagents used to perform the prothrombin time test vary from one laboratory to another and even within the same laboratory over time, the normal ranges also will fluctuate. To standardize results across different laboratories in the U.S. and the world, a World Health Organization (WHO) committee developed and recommended the use of the Internationalized Normalized Ratio (INR), calculated based on the prothrombin time test result, for people who are receiving the anticoagulant warfarin (Coumadin®).
The INR (Internationalized Normalized Ratio) is a calculation that adjusts for changes in the prothrombin time reagents and allows for results from different laboratories to be compared. Most laboratories report both prothrombin time and INR values whenever a prothrombin time test is performed. The INR should be only applicable, however, for those taking the blood-thinning medication warfarin.
Can I do prothrombin time test at home?
Yes, if you will be taking warfarin for an extended period of time. The Food and Drug Administration has approved several home prothrombin time and international normalized ratio (INR) testing systems. However, home testing is usually done in the context of a home-based coagulation management program that involves patient training and defined response and management protocols.
Should I have prothrombin time test done at the same time of day?
It is not generally necessary to have your prothrombin time and international normalized ratio (INR) measured at a particular time of day. It is, however, important that you take your warfarin medication at the same time each day to maintain a continuous level. If your healthcare provider increases or decreases your dosage, he or she may want you to have your blood rechecked in a couple of days or so to judge the effect of the dosage change on your prothrombin time/INR (it is not an immediate effect).
My prothrombin time results vary sometimes, yet my doctor doesn’t change my prescription. Why?
Illness, change in diet, and some medications (as mentioned above) can alter prothrombin time results. Certain foods, such as beef and pork liver, green tea, broccoli, chickpeas, kale, turnip greens, and soybean products contain large amounts of vitamin K and can alter prothrombin time results. The blood collection technique and the difficulty in obtaining the blood sample can also affect test results. If your healthcare provider has concerns about the stability of your prothrombin time/INR, he or she may test your blood more frequently.
Why is my prothrombin time high?
Prothrombin time (PT) may be prolonged due to deficiencies of factors X, VII, V, and II of the extrinsic pathway, presence of inhibitors, or oral anticoagulation therapy.
Prothrombin time (PT) is not useful for detecting deficiencies of coagulation factors that have no influence on the prothrombin time test (eg, factors VIII, IX, XI, XII, XIII).
How is prothrombin time test used?
The prothrombin time (PT) is used, often along with a partial thromboplastin time (partial thromboplastin time), to help diagnose the cause of unexplained bleeding or inappropriate blood clots. The international normalized ratio (INR) is a calculation based on results of a prothrombin time and is used to monitor individuals who are being treated with the blood-thinning medication (anticoagulant) warfarin (Coumadin®).
Several proteins called coagulation factors are involved in the process that the body uses to form blood clots to help stop bleeding (hemostasis). When an injury occurs and bleeding begins, some coagulation factors are activated in a sequence of steps (coagulation cascade) that eventually help to form a clot. There must be a sufficient quantity of each coagulation factor, and each must function properly, in order for normal clotting to occur. Too little can lead to excessive bleeding; too much may lead to excessive clotting.
The prothrombin time and INR (Internationalized Normalized Ratio) are used to monitor the effectiveness of the anticoagulant warfarin. This drug affects the function of the coagulation cascade and helps inhibit the formation of blood clots. It is prescribed on a long-term basis to people who have experienced recurrent inappropriate blood clotting. The goal of warfarin therapy is to maintain a balance between preventing clots and causing excessive bleeding. This balance requires careful monitoring. The INR (Internationalized Normalized Ratio) can be used to adjust a person’s drug dosage to get the PT into the desired range that is right for the person and his or her condition.
Warfarin may be prescribed for conditions such as:
- Irregular heartbeat (atrial fibrillation)
- The presence of artificial heart valves
- Deep vein thrombosis (DVT), pulmonary embolism (PE)
- Antiphospholipid syndrome
- Occasionally, in heart attacks with certain risk factors
The prothrombin time test may be used along with a partial thromboplastin time (PTT) as the starting points for investigating excessive bleeding or clotting disorders. The prothrombin time evaluates the coagulation factors VII, X, V, II and I (fibrinogen). The partial thromboplastin time (PTT) test evaluates coagulation factors XII, XI, IX, VIII, X, V, II (prothrombin), and I (fibrinogen) as well as prekallikrein (PK) and high molecular weight kininogen (HK). By evaluating the results of the prothrombin time and partial thromboplastin time together, a health practitioner can gain clues as to what bleeding or clotting disorder may be present. These tests are not diagnostic by themselves but usually provide information on whether further tests may be needed.
Examples of other testing that may be done along with a prothrombin time and partial thromboplastin time or in follow up to abnormal results include:
- Platelet count – to determine if platelets are decreased, which can cause excessive bleeding
- Thrombin time testing – sometimes ordered to help rule out a fibrinogen abnormality
- Fibrinogen testing – may be done to rule out a low level or dysfunction of fibrinogen as a cause of a prolonged PT
- Coagulation factor tests – these measure the activity (function) of coagulation factors. They can detect reduced levels of the protein or proteins that don’t work properly (have reduced function). Rarely, the antigen level (quantity) of a coagulation factor may also be measured.
- von Willebrand factor – sometimes ordered to help determine if von Willebrand disease is the cause of a prolonged partial thromboplastin time
Based on carefully obtained patient histories, the partial thromboplastin time and prothrombin time tests are sometimes selectively performed as pre-surgical or before other invasive procedures to screen for potential bleeding tendencies.
When is prothrombin time test ordered?
A prothrombin time and INR are ordered on a regular basis when a person is taking the anticoagulant drug warfarin to ensure that the prescription is working properly and that the prothrombin time/INR is appropriately prolonged. There is no set frequency for doing the test. A health practitioner will order them often enough to make sure that the drug is producing the desired effect – that it is increasing the person’s clotting time to a therapeutic level without significant risk of excessive bleeding or bruising.
The prothrombin time may be ordered when a person who is not taking anticoagulant drugs has signs or symptoms of excessive bleeding or clotting, such as:
- Unexplained bleeding or easy bruising
- Nosebleeds
- Bleeding gums
- A blood clot in a vein or artery
- An acute condition such as disseminated intravascular coagulation (DIC) that may cause both bleeding and clotting as coagulation factors are used up at a rapid rate
- A chronic condition such as severe liver disease that may affect hemostasis
Prothrombin time, along with partial thromboplastin time (PTT), may be ordered prior to surgery when the surgery carries an increased risk of blood loss and/or when the person has a clinical history of bleeding, such as frequent or excessive nosebleeds and easy bruising, which may indicate the presence of a bleeding disorder.
Normal prothrombin time
Prothrombin time is measured in seconds. Most of the time, results are given as what is called INR (international normalized ratio).
If you are not taking blood thinning medicines, such as warfarin, the normal range for your prothrombin time results is:
- 11 to 13.5 seconds
- INR of 0.8 to 1.1
If you are taking warfarin to prevent blood clots, your provider will most likely choose to keep your INR between 2.0 and 3.0.
Ask your doctor what result is right for you.
Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your doctor about the meaning of your specific test results.
Some consumed substances, such as alcohol, can affect the prothrombin time and INR tests. Some antibiotics can increase the prothrombin time and INR. Barbiturates, oral contraceptives and hormone-replacement therapy (HRT), and vitamin K (either in a multivitamin or liquid nutrition supplement) may decrease prothrombin time. Certain foods, such as beef and pork liver, green tea, broccoli, chickpeas, kale, turnip greens, and soybean products, contain large amounts of vitamin K and can alter prothrombin time results. It is important that a healthcare provider know about all of the drugs, supplements, and foods that a person has ingested recently so that the prothrombin time and INR results are interpreted and used correctly.
Some laboratories will report a prothrombin time as a percentage of normal, although this is not a common practice.
What does the prothrombin time test result mean?
For people taking warfarin, most laboratories report prothrombin time results that have been adjusted to the INR. These people should have an INR of 2.0 to 3.0 for basic “blood-thinning” needs. For some who have a high risk of a blood clot, the INR needs to be higher – about 2.5 to 3.5.
The test result for a prothrombin time depends on the method used, with results measured in seconds and compared to the normal range established and maintained by the laboratory that performs the test. This normal range represents an average value of healthy people who live in that area and will vary somewhat from lab to lab. Someone who is not taking warfarin would compare their prothrombin time test result to the normal range provided with the test result by the laboratory performing the test.
A prolonged prothrombin time means that the blood is taking too long to form a clot. This may be caused by conditions such as liver disease, vitamin K deficiency, or a coagulation factor deficiency. The prothrombin time result is often interpreted with that of the partial thromboplastin time (PTT) in determining what condition may be present.
If you are not taking blood thinning medicines, such as warfarin, an INR result above 1.1 means your blood is clotting more slowly than normal. This may be due to:
- Bleeding disorders, a group of conditions in which there is a problem with the body’s blood clotting process.
- Disorder in which the proteins that control blood clotting become over active (disseminated intravascular coagulation).
- Liver disease.
- Low level of vitamin K.
If you are taking warfarin to prevent clots, your provider will most likely choose to keep your INR between 2.0 and 3.0:
- Depending on why you are taking the blood thinner, the desired level may be different.
- Even when your INR stays between 2.0 and 3.0, you are more likely to have bleeding problems.
- INR results higher than 3.0 may put you at even higher risk for bleeding.
- INR results lower than 2.0 may put you at risk for developing a blood clot.
INR therapeutic ranges for orally administered drugs:
- Standard-intensity warfarin therapeutic range: 2.0 to 3.0
- High-intensity warfarin therapeutic range: 2.5 to 3.5
Note: The INR should only be used for patients on stable oral anticoagulant therapy, though it is reported for all patients despite whether they are receiving oral anticoagulants.
A prothrombin time result that is too high or too low in someone who is taking warfarin (Coumadin) may be due to:
- The wrong dose of medicine
- Drinking alcohol
- Taking certain over-the-counter (OTC) medicines, vitamins, supplements, cold medicines, antibiotics, or other medicines
- Eating food that changes the way the blood-thinning medicine works in your body
Your provider will teach you about taking warfarin (Coumadin) the proper way.
Table 1. Interpretation of prothrombin time (PT) and partial thromboplastin time (PTT) in patients with a bleeding or clotting syndrome
| Prothrombin time (PT) result | Partial Thromboplastin Time (PTT) result | Examples of conditions that may be present |
|---|---|---|
| Prolonged | Normal | Liver disease, decreased vitamin K, decreased or defective factor VII, chronic low-grade disseminated intravascular coagulation (DIC), anticoagulation drug (warfarin) therapy |
| Normal | Prolonged | Decreased or defective factor VIII, IX, XI, or XII, von Willebrand disease (severe type), presence of lupus anticoagulant, autoantibody against a specific factor (e.g., factor VIII) |
| Prolonged | Prolonged | Decreased or defective factor I, II, V or X, severe liver disease, acute DIC, warfarin overdose |
| Normal | Normal or slightly prolonged | May indicate normal hemostasis; however, PT and PTT can be normal in conditions such as mild deficiencies in coagulation factor(s) and mild form of von Willebrand disease. Further testing may be required to diagnose these conditions. |
Partial thromboplastin time
The partial thromboplastin time (PTT) is a screening test that helps evaluate a person’s ability to appropriately form blood clots. It measures the number of seconds it takes for a clot to form in a person’s sample of blood after substances (reagents) are added. The partial thromboplastin time assesses the amount and the function of certain proteins called coagulation factors that are an important part of blood clot formation.
The partial thromboplastin time is used to evaluate the coagulation factors XII, XI, IX, VIII, X, V, II (prothrombin), and I (fibrinogen) as well as prekallikrein (PK) and high molecular weight kininogen (HK). A PT test evaluates the coagulation factors VII, X, V, II, and I (fibrinogen). By evaluating the results of the two tests together, a health practitioner can gain clues as to what bleeding or clotting disorder may be present. The partial thromboplastin time and PT are not diagnostic but usually provide information on whether further tests may be needed.
Some examples of uses of a partial thromboplastin time (PTT) include:
- To identify coagulation factor deficiency; if the partial thromboplastin time is prolonged, further studies can then be performed to identify what coagulation factors may be deficient or dysfunctional, or to determine if an antibody to a coagulation factor (a specific inhibitor) is present in the blood.
- To detect nonspecific autoantibodies, such as lupus anticoagulant; these are associated with clotting episodes and with recurrent miscarriages. For this reason, partial thromboplastin time testing may be performed as part of a clotting disorder panel to help investigate recurrent miscarriages or diagnose antiphospholipid syndrome (APS). A variation of the partial thromboplastin time called the LA-sensitive partial thromboplastin time may be used for this purpose.
- To monitor standard (unfractionated, UF) heparin anticoagulant therapy; heparin is an anticoagulation drug that is given intravenously (IV) or by injection to prevent and to treat blood clots (embolism and thromboembolism). It prolongs partial thromboplastin time. When heparin is administered for therapeutic purposes, it must be closely monitored. If too much is given, the treated person may bleed excessively; with too little, the treated person may continue to clot.
- Based on carefully obtained patient histories, the partial thromboplastin time (PTT) and prothrombin time (PT) tests are sometimes selectively performed as pre-surgical or before other invasive procedures to screen for potential bleeding tendencies.
Examples of other testing that may be done along with a partial thromboplastin time (PTT) or in follow up to abnormal results include:
- Platelet count – should always be monitored during heparin therapy to promptly detect any heparin-induced thrombocytopenia
- Thrombin time testing – sometimes ordered to help rule out heparin contamination
- Fibrinogen testing – may be done to rule out a low level of fibrinogen as a cause of a prolonged partial thromboplastin time
- When an initial partial thromboplastin time is prolonged, a second partial thromboplastin time test is performed by mixing the person’s plasma with pooled normal plasma (a collection of plasma from a number of normal donors). If the partial thromboplastin time time returns to normal (“corrects”), it suggests a deficiency of one or more of the coagulation factors in the person’s plasma. If the time remains prolonged, then the problem may be due to the presence of an abnormal specific factor inhibitor (autoantibody) or nonspecific lupus anticoagulant.
- Coagulation factor tests – these measure the activity (function) of coagulation factors. They can detect reduced levels of the protein or proteins that don’t work properly (have reduced function). Rarely, the antigen level (quantity) of a coagulation factor may also be measured.
- Dilute Russell viper venom test (DRVVT) – a test that may be done if the presence of lupus anticoagulant is suspected.
- von Willebrand factor – sometimes ordered to help determine if von Willebrand disease is the cause of a prolonged partial thromboplastin time
When body tissue(s) or blood vessel walls are injured, bleeding occurs and a process called hemostasis begins. Small cell fragments called platelets adhere to and then clump (aggregate) at the injury site. At the same time, a process called the coagulation cascade begins and coagulation factors are activated. Through the cascading reactions, threads called fibrin form and crosslink into a net that adheres to the injury site and stabilizes it. Along with the platelets adhering, this forms a stable blood clot to seal off injuries to blood vessels, prevents additional blood loss, and gives the damaged areas time to heal.
Each component of this hemostatic process must function properly and be present in sufficient quantity for normal blood clot formation. If there is a deficiency in one or more of these factors, or if the factors function abnormally, then a stable clot may not form and bleeding continues.
With a partial thromboplastin time, a person’s sample is compared to a normal reference interval for clotting time. When a person’s partial thromboplastin time takes longer than normal to clot, the partial thromboplastin time is considered “prolonged.” A prolonged partial thromboplastin time may be due to a condition that decreases or creates a dysfunction in one or more coagulation factors. Less often, it may be due to a condition in which the body produces certain antibodies directed against one or more coagulation factors, affecting their function.
Sometimes a partial thromboplastin time may be prolonged because the person tested produces an autoantibody called an antiphospholipid antibody that interferes with the test. This type of antibody affects the results of the test because it targets substances called phospholipids that are used in the partial thromboplastin time. Though antiphospholipid antibodies can prolong the partial thromboplastin time test result, in the body they are associated with excessive clotting. A person who produces these antibodies may be at an increased risk for a blood clot. A partial thromboplastin time maybe used as part of an evaluation of a person with signs and symptoms of excessive clotting or antiphospholipid syndrome. (See the article on Antiphospholipid Antibodies for additional details.)
When a partial thromboplastin time is used to investigate bleeding or clotting episodes, it is often ordered along with a prothrombin time (PT). A health practitioner will evaluate the results of both tests to help determine the cause of bleeding or clotting episode(s).
It is now understood that coagulation tests such as the prothrombin time and partial thromboplastin time are based on what happens artificially in the test setting (in vitro) and thus do not necessarily reflect what actually happens in the body (in vivo). Nevertheless, they can be used to evaluate certain components of the hemostasis system. The partial thromboplastin time and prothrombin time tests each evaluate coagulation factors that are part of different groups of chemical reaction pathways in the cascade, called the intrinsic, extrinsic, and common pathways.
References- Chinnaraj M, Chen Z, Pelc LA, et al. Structure of prothrombin in the closed form reveals new details on the mechanism of activation. Sci Rep. 2018;8(1):2945. Published 2018 Feb 13. doi:10.1038/s41598-018-21304-1 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5811608
- Chinnaraj M, Planer W, Pozzi N. Structure of Coagulation Factor II: Molecular Mechanism of Thrombin Generation and Development of Next-Generation Anticoagulants. Front Med (Lausanne). 2018;5:281. Published 2018 Oct 2. doi:10.3389/fmed.2018.00281 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6176116/
- The transition of prothrombin to thrombin. Krishnaswamy S. J Thromb Haemost. 2013 Jun; 11 Suppl 1():265-76.
- Ariens RA. Fibrin(ogen) and thrombotic disease. J Thromb Haemost. (2013) 11 (Suppl 1):294–305. 10.1111/jth.12229
- Degen SJ, Davie EW. Nucleotide sequence of the gene for human prothrombin. Biochemistry (1987) 26:6165–77.
- Mann KG, Elion J, Butkowski RJ, Downing M, Nesheim ME. Prothrombin. Methods Enzymol. (1981) 80 (Pt C):286–302.
- Arai T, Miklossy J, Klegeris A, Guo JP, McGeer PL. Thrombin and prothrombin are expressed by neurons and glial cells and accumulate in neurofibrillary tangles in Alzheimer disease brain. J Neuropathol Exp Neurol. (2006) 65:19–25.
- Frasson R, Pozzi N, Johnson DJD, Huntington JA, De Fillips V. Effect of glycosylation on thrombin structure, stability and function. J Thromb Haemost. (2009) 7:230.
- Shen G, Cui W, Zhang H, Zhou F, Huang W, Liu Q, et al. . Warfarin traps human vitamin K epoxide reductase in an intermediate state during electron transfer. Nat Struct Mol Biol. (2017) 24:69–76. 10.1038/nsmb.3333
- Lancellotti S, Basso M, De Cristofaro R. Congenital prothrombin deficiency: an update. Semin Thromb Hemost. (2013) 39:596–606. 10.1055/s-0033-1348948
- Kaushansky K, Lichtman MA, Prchal JT, Levi MM, Press OW, Burns LJ, et al. Williams Hematology. 9th ed McGraw-Hill Education; (2016).
- Chinnaraj M, Chen Z, Pelc LA, Grese Z, Bystranowska D, Di Cera E, et al. . Structure of prothrombin in the closed form reveals new details on the mechanism of activation. Sci Rep. (2018) 8:2945. 10.1038/s41598-018-21304-1
- Pozzi N, Zerbetto M, Acquasaliente L, Tescari S, Frezzato D, Polimeno A, et al. . Loop electrostatics asymmetry modulates the preexisting conformational equilibrium in thrombin. Biochemistry (2016) 55:3984–94. 10.1021/acs.biochem.6b00385
- Chinnaraj M, Chen Z, Pelc LA, et al. Structure of prothrombin in the closed form reveals new details on the mechanism of activation. Sci Rep. 2018;8(1):2945. Published 2018 Feb 13. doi:10.1038/s41598-018-21304-1 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5811608/
- Garmo C, Burns B. Physiology, Clotting Mechanism. [Updated 2018 Jun 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507795
- Prothrombin thrombophilia. https://ghr.nlm.nih.gov/condition/prothrombin-thrombophilia
- Kujovich JL. Prothrombin-Related Thrombophilia. 2006 Jul 25 [Updated 2014 Aug 14]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1148
- Prothrombin thrombophilia. https://rarediseases.info.nih.gov/diseases/10815/prothrombin-related-thrombophilia
- Prothrombin deficiency. https://ghr.nlm.nih.gov/condition/prothrombin-deficiency
- Meeks SL & Abshire TC. Prothrombin (Factor II) Deficiency Disease Overview. Rare Bleeding Disorders. 2014; http://www.rarecoagulationdisorders.org/diseases/prothrombin-factor-ii-deficiency/disease-overview
- Schwartz RA, Steen CJ, and Gascon P. Factor II Deficiency. Medscape Reference. March 1, 2017; https://emedicine.medscape.com/article/209742-overview





{kind=link}