What is a Rectum
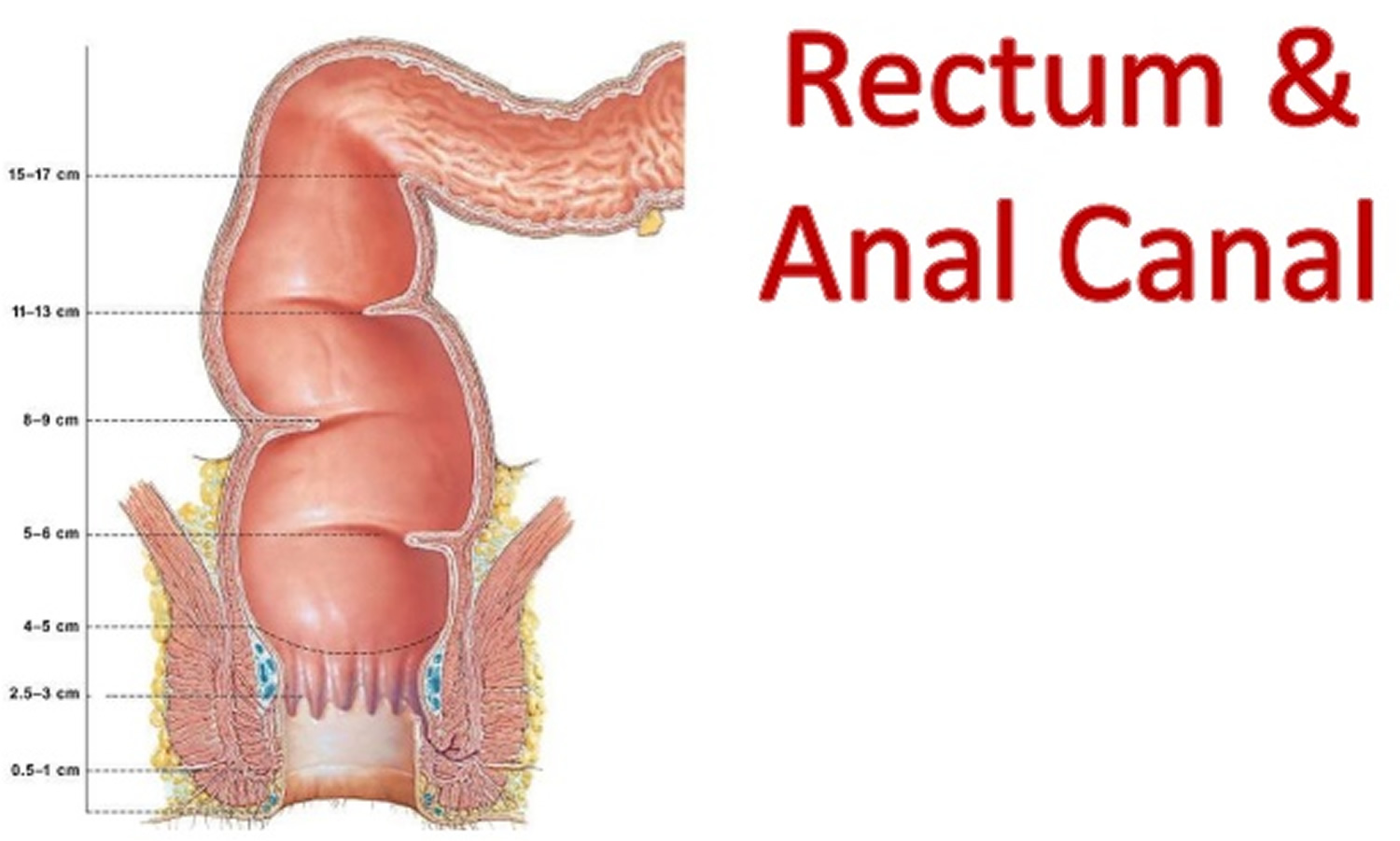
Extending from the sigmoid colon is the rectum. The rectum forms the last 15 cm (6 in.) of the large intestine. The rectum is an expandable organ for the temporary storage of feces. The rectum lies next to the sacrum and generally follows its curvature. The peritoneum firmly attaches the rectum to the sacrum. The rectum ends about 5 centimeters below the tip of the coccyx, where it becomes the anal canal.
The Anus and Anal Canal
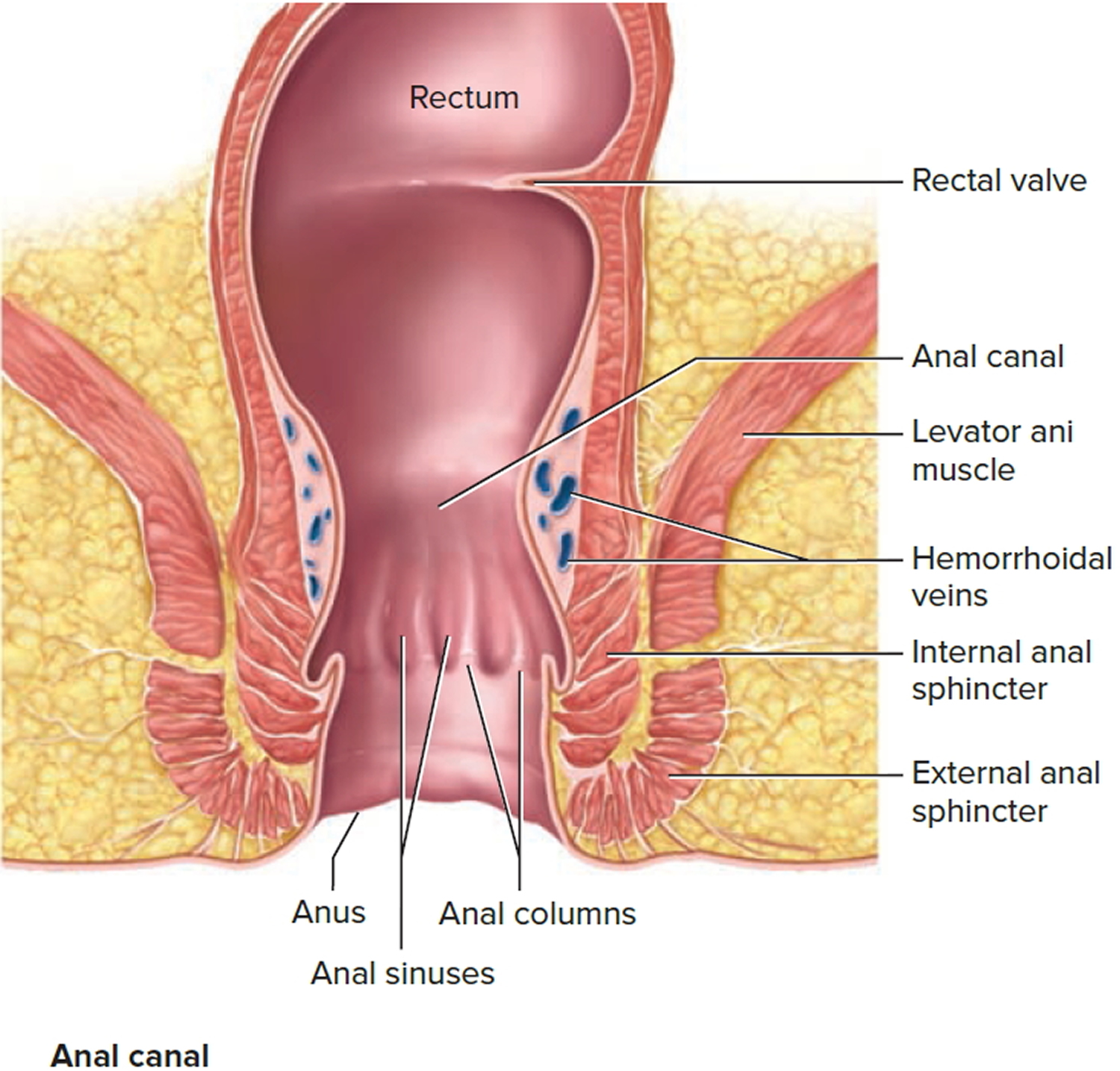
The anal canal is the continuation of the large intestine inferior to the rectum. The anal canal is about 3 cm long, it begins where the rectum passes through the levator ani, the muscle that forms the pelvic floor. At its distal end, the anal canal opens to the outside as the anus. Two sphincter muscles guard the anus—an internal anal sphincter muscle, composed of smooth muscle under involuntary control, and an external anal sphincter muscle, composed of skeletal muscle under voluntary control. A portion of the levator ani is responsible for maintaining the anorectal angle, an acute angle between the anus and the rectum that contributes to fecal continence. The anal canal lies entirely external to the abdominopelvic cavity in the perineum.
Internally, the superior half of the anal canal contains longitudinal folds of mucosa, the anal columns. These columns contain the terminal portions of the superior rectal artery and vein (the hemorrhoidal vessels). Neighboring anal columns join each other inferiorly at crescent-shaped transverse folds called anal valves. The pockets just superior to these valves are anal sinuses, which release mucus when they are compressed by feces, providing lubrication that eases fecal passage during defecation. The horizontal line along which the anal valves lie is called the pectinate (“comb-shaped”) line. Because the mucosa superior to this line is innervated by visceral sensory fibers, it is relatively insensitive to pain. Inferior to the pectinate line, however, the mucosa is sensitive to pain because it is innervated by somatic nerves.
The wall of the anal canal contains two sphincter muscles: an internal anal sphincter of smooth muscle and an external anal sphincter of skeletal muscle. The former is a thickening of the circular layer of the muscularis, whereas the latter is a distinct muscle. The external sphincter contracts voluntarily to inhibit defecation, whereas the internal sphincter contracts involuntarily, both to prevent feces from leaking from the anus between defecations and to inhibit defecation during emotional stress. During toilet training, children learn to control the external anal sphincter.
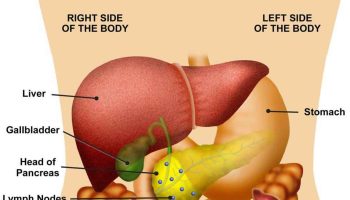
Figure 1. Rectum
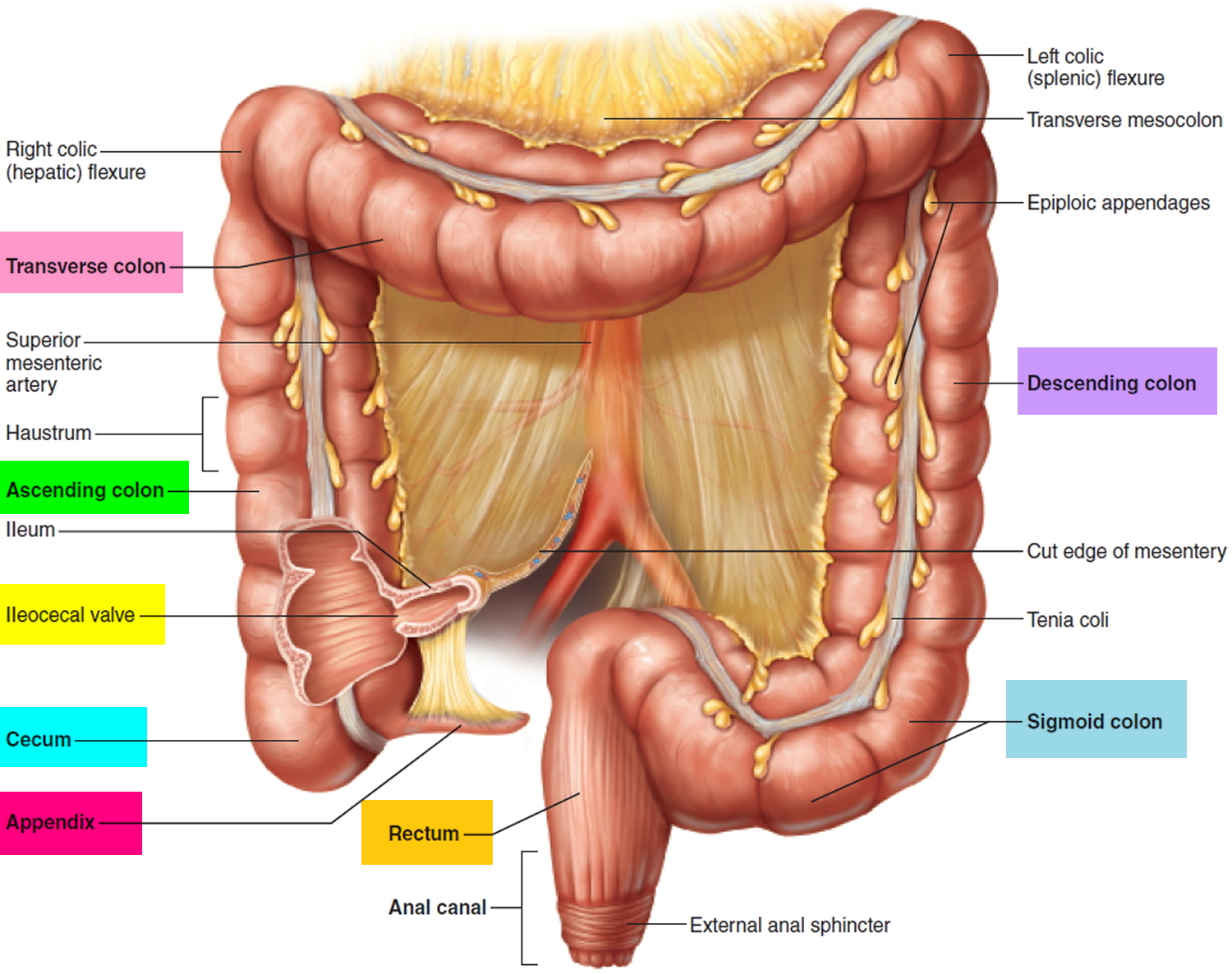
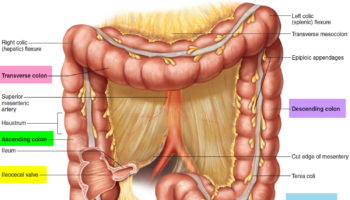
Figure 2. Rectum anatomy and Anus (anal canal)
Rectum function
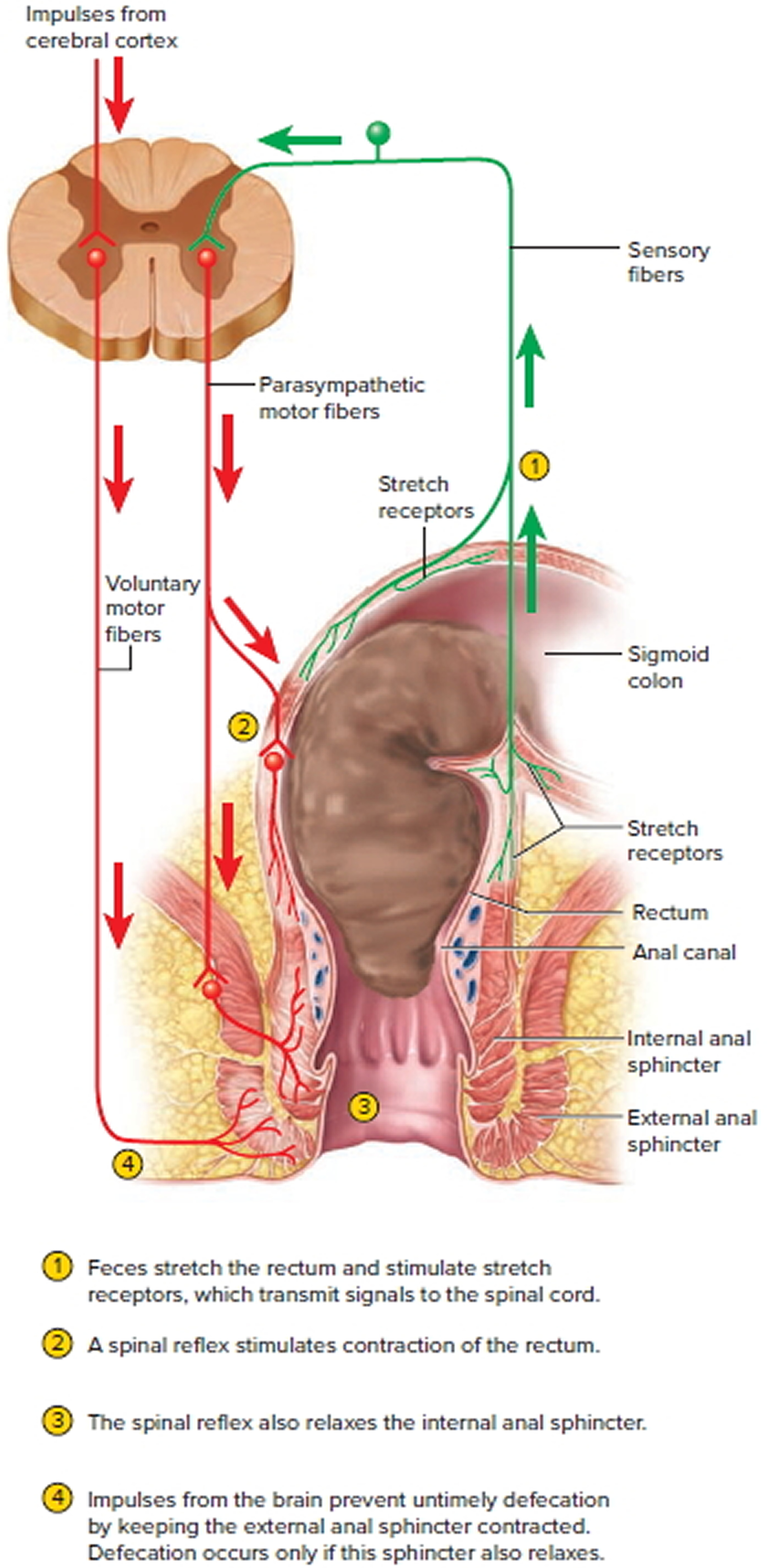
The rectum is usually empty and the anal sphincters contracted. When feces are squeezed into the rectum by mass peristaltic movements, the stretching of the rectal wall initiates the defecation reflex, which account for the urge to defecate that is often felt soon after a meal (Figure 3).
Figure 3. Rectum function and neural control of defecation
The defecation reflexes involve two reflexes:
- The intrinsic defecation reflex. This reflex is mediated entirely by the myenteric plexus. Stretch signals travel through the plexus to the muscularis of the descending and sigmoid colon and the rectum. This activates a peristaltic wave that drives feces downward, and it relaxes the internal anal sphincter. This reflex is relatively weak, however, and usually requires the cooperative action of the following reflex.
- The parasympathetic defecation reflex. This is a spinal reflex. Its principal events are that stretch signals are transmitted to the spinal cord; motor signals return by way of the pelvic nerves; and these signals intensify peristalsis in the descending and sigmoid colon and rectum while they relax the internal anal sphincter. These reflexes are involuntary and are the sole means of controlling defecation in infants and some people with transecting spinal cord injuries. However, the external anal sphincter is under voluntary control, enabling one to limit defecation to appropriate circumstances.
Voluntary retention of feces is also aided by the puborectalis muscle, which loops around the rectum like a sling and creates a sharp anorectal angle that blocks the passage of feces. Defecation normally occurs only when the external anal sphincter and puborectalis muscle are voluntarily relaxed. The kink in the rectum then straightens out and the sphincter opens to allow the feces to fall away. Defecation is also aided by the voluntary Valsalva maneuver, in which a breath hold and contraction of the abdominal muscles increase abdominal pressure, compress the rectum, and squeeze the feces from it. This maneuver can also initiate the defecation reflex by forcing feces from the descending colon into the rectum. The external anal sphincter and external urethral sphincter are controlled together by inhibitory signals from the brainstem, so as this inhibition is released, defecation is usually accompanied by urination.
Some spinal cord injuries and diseases abolish the voluntary control of the external anal sphincter. The resulting inability to voluntarily retain the feces is called fecal incontinence. If the defecation urge is suppressed, contractions cease in a few minutes and the rectum relaxes. The defecation reflexes reoccur a few hours later or when another mass movement propels more feces into the rectum.



{kind=link}