Schatzki ring
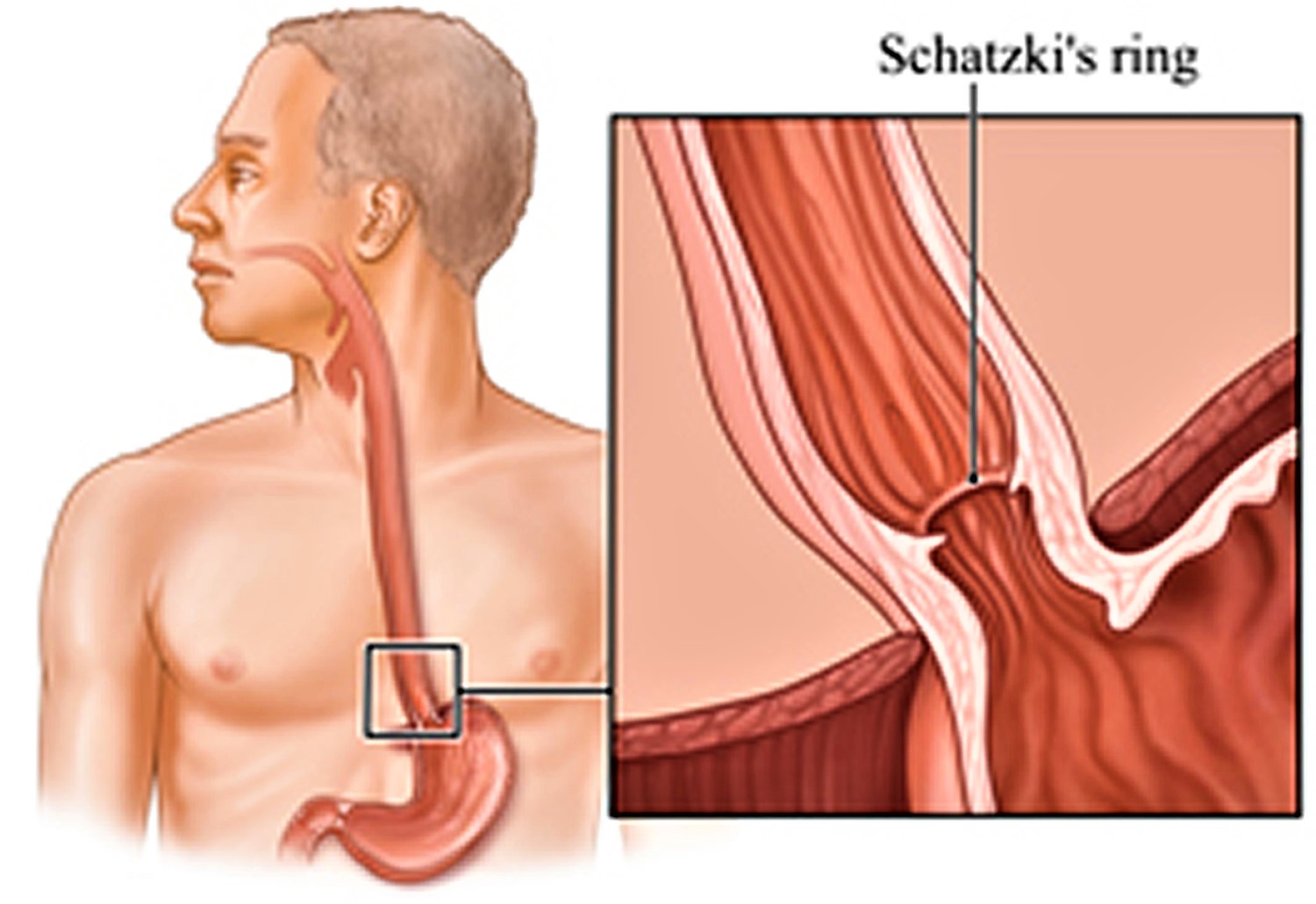
Schatzki ring also called Schatzki-Gary ring, is a ring of tissue that forms inside the distal esophagus, the tube that carries food and liquid to your stomach. Schatzki ring makes your esophagus narrow in one area, close to where it meets the stomach. Schatzki ring can make it hard for your to swallow solids. You may also feel like food gets stuck in your esophagus.
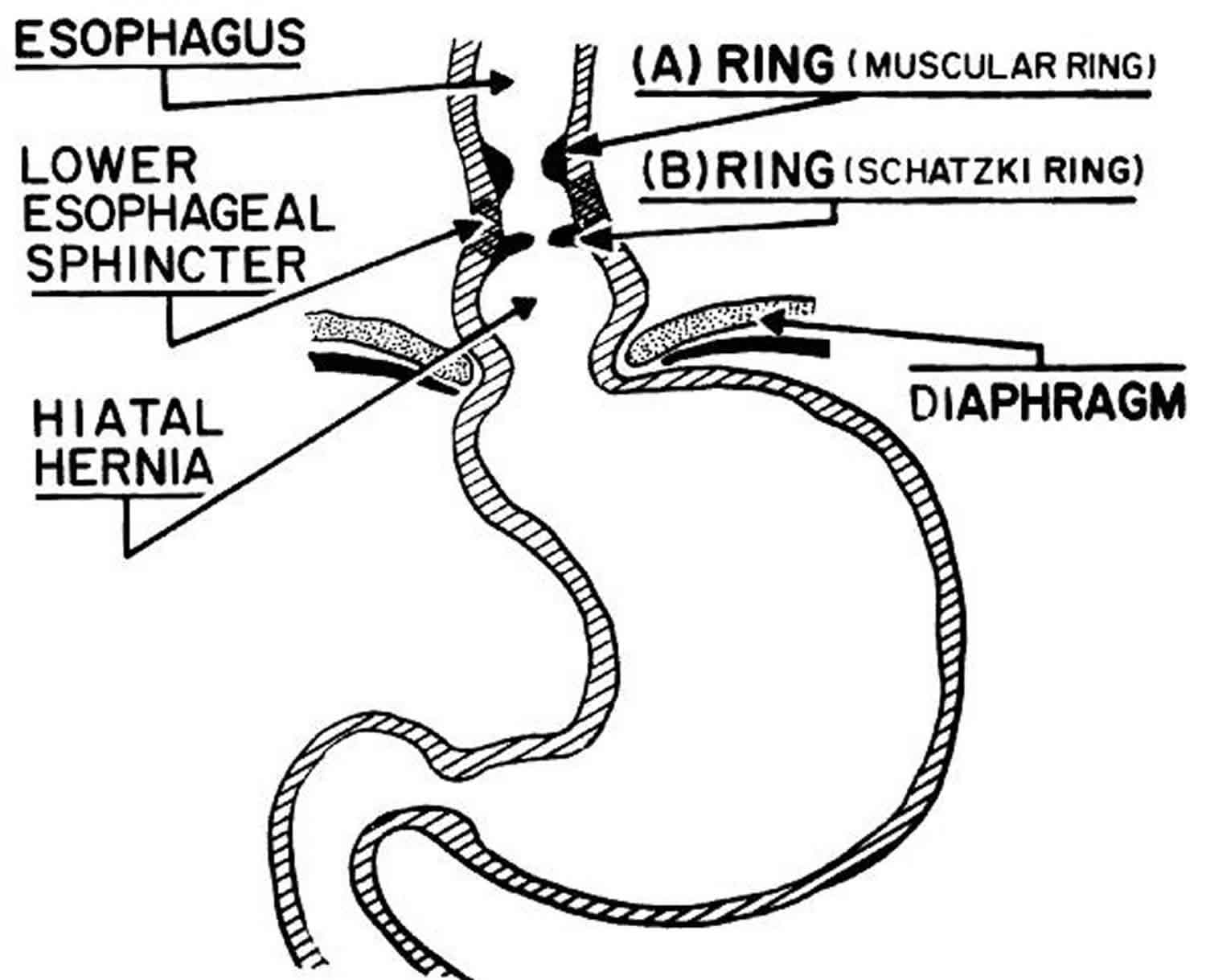
Schatzki ring also referred to as a narrow esophageal B-ring occurring in the distal esophagus and usually associated with a hiatus hernia. Two rings have been identified in the distal esophagus. The muscular ring, or A ring, is a thickened symmetric band of muscle that forms the upper border of the esophageal vestibule and is located approximately 2 cm above the gastroesophageal junction. The A ring is rare; furthermore, it is even more rarely associated with dysphagia. On the other hand, the mucosal ring, or B ring, is quite common and is the subject of discussion in this article. The B ring is a diaphragmlike thin mucosal ring usually located at the squamocolumnar junction; it may be symptomatic or asymptomatic, depending on the luminal diameter.
Depending on its luminal diameter, an esophageal B-ring may be symptomatic or asymptomatic 1:
- <13 mm: almost always symptomatic
- 13-20 mm: sometimes symptomatic
- >20 mm: rarely symptomatic
When it is symptomatic, it is termed a “Schatzki ring”.
Schatzki rings are located at the gastro-esophageal junction, illustrated by the fact that there is squamous epithelium above and columnar epithelial below the ring. They should not be confused with:
- A-rings, which are found a few centimeters proximal to the B-ring
- esophageal webs, which are lined on both sides by esophageal mucosa 2
Relatively common, Schatzki rings (lower esophageal rings) are found in 10% to 15% of barium swallow studies or oesophagrams; however, few of these patients exhibit any symptoms of difficulty swallowing (dysphagia). Patients typically present with intermittent non-progressive dysphagia (difficulty swallowing) for solids. Most episodes of dysphagia are short lived, and intervening periods between episodes may vary from weeks to months or even to years. Although no known predilection for a specific age group exists, most patients are older than 40 years at presentation. Schatzki ring is relatively rare in children 3.
More than half of Schatzki ring patients will have an associated esophageal condition such as 4:
- hiatus hernia
- reflux esophagitis
- esophageal web
- esophageal diverticulum
Fortunately, most patients respond well to initial and repeat dilatation therapy. A small number of patients may have stubborn Schatzki rings that require more aggressive endoscopic or surgical intervention.
Figure 1. Schatzki ring
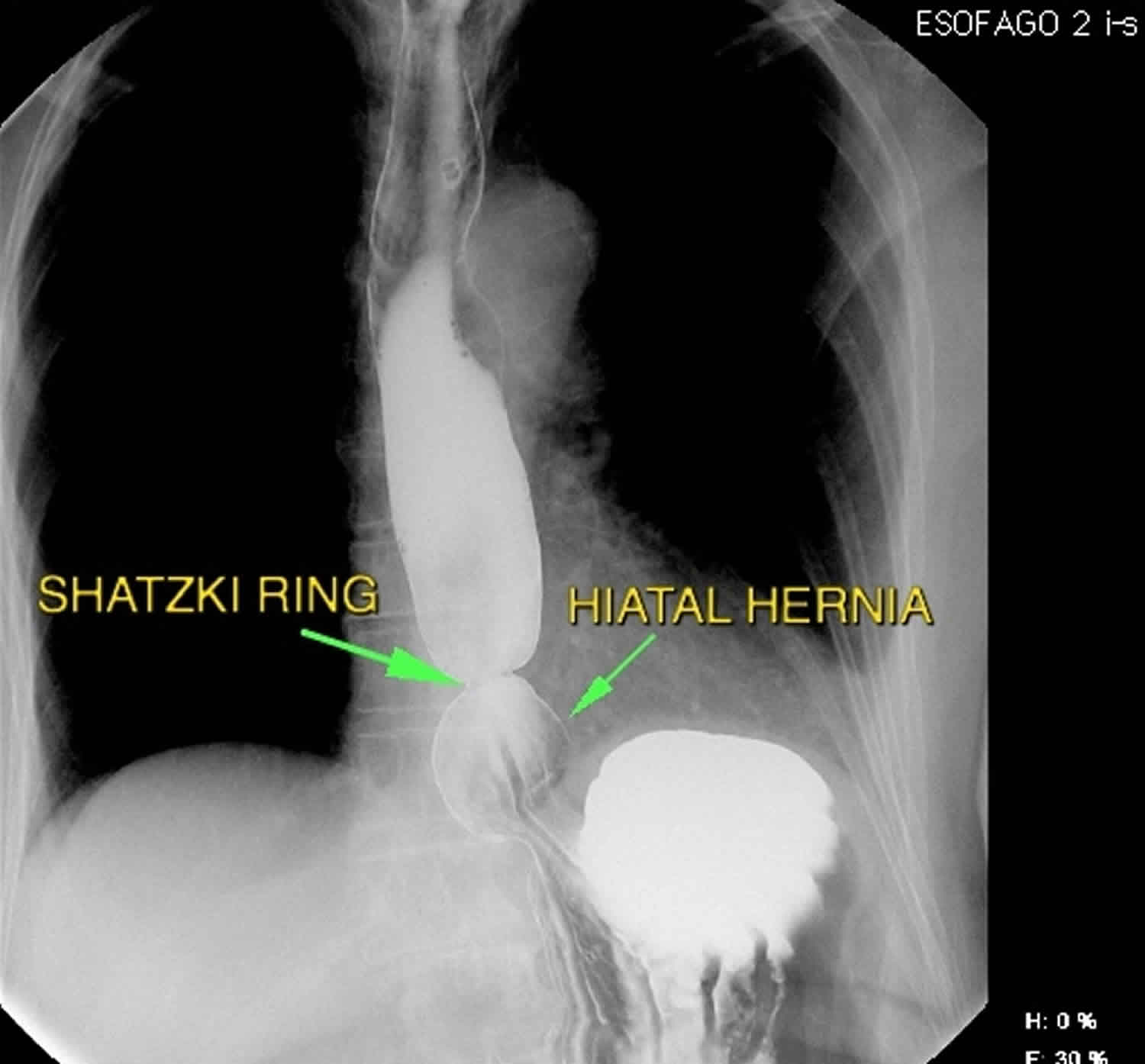
Figure 2. Schatzki ring barium swallow studies
Schatzki ring causes
The cause of Schatzki ring is not clear. In 1953, Ingelfinger and Kramer believed that Schatzki rings occurred as a result of a contraction by an overactive band of esophageal muscle 5; however, Schatzki and Gary believed that these rings were fixed and not contractile 6. Some of this controversy may be related to the confusion of categorizing muscular and mucosal rings under the same entity, as concluded by Goyal et al 7.
There are at least 4 hypotheses have been proposed for the formation of Schatzki ring. These hypotheses may not be mutually exclusive. Proposed hypotheses are as follows:
- Schatzki ring is a pleat of redundant mucosa that forms when the esophagus shortens transiently or permanently for unknown reasons.
- Schatzki ring is congenital in origin.
- Schatzki ring is actually a short peptic stricture occurring as a consequence of gastroesophageal reflux disease.
- Schatzki ring is a consequence of pill-induced esophagitis.
Data supporting or refuting the first 2 hypotheses are few.
Data about the association of gastroesophageal reflux disease and rings are inconclusive or contradictory. It has been hypothesized that the ring acts as a protective barrier against further reflux. However, in one recent study involving 20 patients, no significant differences were noted in any of the reflux parameters measured before and after dilation. In fact, it was interesting to note that thick rings may actually decrease esophageal acid clearance, especially in the supine position, thereby increasing esophageal acid exposure.
The last hypothesis was based on a chance observation in one study showing that 62% of patients with rings had ingested medications known to cause pill-induced esophagitis.
In some studies, the severity of symptoms has clearly been demonstrated to correlate with the luminal diameter. Dysphagia predictably occurs in patients with a luminal diameter less than 13 mm and may vary between 13-20 mm, depending on the size and type of bolus.
Schatzki ring symptoms
Most commonly Schatzki ring presents with intermittent, episodic, nonprogressive dysphagia to solids. Dysphagia to liquids is usually not present.
A history of food impaction is also very common. Dysphagia is more common in patients with an associated motility disorder.
- The episode of dysphagia appears to be short lived.
- Typically, the patient ate a meal in a hurried fashion.
- The bolus of food may occasionally be forced down by drinking liquids, or may be regurgitated to relieve the obstruction.
- After forcing the bolus through or regurgitating it, the patient can usually finish his or her meal without difficulty.
- Dysphagia may not recur for months or years in these patients. Daily dysphagia is unlikely to be caused by a Schatzki ring.
- The patient may salivate and drool if the offending food bolus continues to completely obstruct the lower esophagus for a longer duration, but this scenario is excessively rare.
Bread (especially freshly baked) and meat appear to be common foods that frequently precipitate symptoms. Patients often present after rapidly eating meat and drinking alcohol at a restaurant; hence, some authorities equate Schatzki ring to the “steakhouse syndrome.”
Associated symptoms of heartburn and regurgitation characteristic of gastroesophageal reflux disease may occur in some patients.
Schatzki ring diagnosis
Your doctor may check your esophagus if you are having trouble swallowing or if you feel like food is getting stuck. The doctor will use a tool called an endoscope, or scope. It’s a thin, flexible, lighted viewing tool. It goes into the mouth and down the throat. Your doctor can use it to check for any problems. The scope can also be used to take a sample of tissue to test (biopsy).
You might need an X-ray. For the X-ray, you may need to swallow a substance, such as barium, that makes it easier to see what happens in your esophagus.
Barium esophagram
Single-contrast solid barium swallows (especially in the right anterior oblique prone position) are more sensitive than endoscopy in detecting Schatzki rings 8. On barium swallow the following features may be seen 9:
- full-column barium swallow will reveal a circumferential narrowing at the gastro-esophageal junction, often a few centimeters above the diaphragmatic hiatus
- thin smooth ring, 1-3 mm
- double contrast studies are less sensitive
- performing a Valsalva maneuver may improve sensitivity
- barium-tablet or barium-coated marshmallow may also improve sensitivity.
Esophagogastroduodenoscopy
Although barium studies are performed initially, esophagogastroduodenoscopy is performed subsequently to confirm the diagnosis and to exclude any other diagnosis.
Endoscopic examination evaluates the mucosa of the distal esophagus, confirming the diagnosis of concomitant gastroesophageal reflux disease or a short peptic stricture instead of a ring.
Schatzki ring treatment
A Schatzki’s ring is usually treated with a procedure called esophageal dilation. Using a large French mercury bougie, polyvinyl bougie, or a balloon, esophageal dilatation is used with the intention of fracturing the ring—not merely stretching it. Dilation can open up narrow areas of the esophagus.
Before the procedure, you will get medicines through a needle in your vein (IV) in your arm or hand. These medicines reduce pain and will make you feel relaxed and drowsy. Your throat will also be numbed. You may not remember much about the treatment.
The doctor will guide a balloon or a plastic tool for widening (dilator) down your throat and into your esophagus. The dilator is used to widen any narrow area.
To guide the dilator, the doctor may use a scope. Or he or she may use a thin wire as a guide.
After the procedure, you will be observed for 1 to 2 hours until the medicines wear off. If your throat was numbed before the test, you should not eat or drink until your throat is no longer numb. When you are fully recovered, you can go home.
You will not be able to drive or operate machinery for 12 hours after the test. Your doctor will tell you when you can go back to your usual diet and activities. Do not drink alcohol for 12 to 24 hours after the test.
You may still need to treat some symptoms of gastroesophageal reflux disease (GERD). Your doctor may give you information about that. In one prospective, randomized, placebo-controlled study involving 44 consecutive patients, acid suppressive maintenance therapy with omeprazole after bougienage was shown to prevent relapse of the Schatzki ring as compared to the placebo group. The duration of follow-up was about 60 months, and the mean duration of relapse was 19.9 months.
If your dysphagia persists or recurs shortly after dilatation, your doctor may do an esophageal manometry study to look for any treatable motility disorder.
If the manometry does not reveal any treatable motility disorder, your doctor may repeat an upper endoscopy to assure healing of esophagitis or to confirm persistence of the Schatzki ring.
Successful endoscopic electrocautery incision using a needle-knife papillotome has been reported and may be considered. A recent randomized, controlled trial compared 52-Fr Maloney dilator versus 4 quadrant biopsy of the ring and found that both modalities were equally effective in relieving dysphagia at 3 months and at 12 months in 26 patients. However, 100% of the biopsy group described the procedure as easy as opposed to 55% of the dilation group.
Surgery
On very rare occasions, your doctor may have to resort to surgical excision if medical therapy fails. Antireflux surgery may also be considered at the same time for concomitant gastroesophageal reflux disease (GERD) 10.
In a randomized, prospective trial, Wills et al 11 compared the efficacy of bougie dilation (n = 25) with electrosurgical incision (n = 25) of symptomatic Schatzki rings at 1-year follow-up in the presence of acid suppression with rabeprazole treatment. The investigators found electrosurgical incision of Schatzki rings to be a safe procedure that provided a longer duration of symptom improvement (7.99 months) relative to bougie dilation (5.86 months). Gastroesophageal reflux disease scores in both groups were significantly improved with the addition of rabeprazole therapy 11.
Successful complete excision of symptomatic Schatzki ring with the use of jumbo cold biopsy forceps has been reported 12. Gonzalez et al 12 revealed that all 10 patients with dysphagia as a result of a Schatzki ring in their observational study (mean follow-up, 376 days) achieved complete endoscopic obliteration of their Schatzki rings with cold jumbo biopsy forceps. Six of 10 patients had been previously treated with bougienage or balloon dilation, 5 patients were on proton pump inhibitor maintenance therapy, and 1 patient was on H2 blocker maintenance therapy. No serious complications were noted 12.
Schatzki ring diet
No major dietary restrictions are applicable. The patient may be advised to avoid eating quickly and to chew his or her food well, especially meat and bread; however, whether this advice is truly beneficial is unclear.
Schatzki ring prognosis
Although results of dilatation are excellent, some series report that patients frequently have recurrence of dysphagia. In one study of 33 patients, 32% had recurrence at 1 year, and 89% had recurrence at 5 years.
No known prognostic indicators for recurrence of dysphagia exist, except for associated gastroesophageal reflux disease as reported in some studies. Other studies have refuted this contention.
Reassure patients that the ring is a benign entity; however, prepare them for repeat dilatation in the event of recurrence of dysphagia.
References- Gore RM, Levine MS. Textbook of Gastrointestinal Radiology. Saunders. (2008) ISBN:1416023321
- Richard Schatzki: A Familiar Ring. Birju Patel, Eugene Han, and Kenneth Swan. American Journal of Roentgenology 2013 201:5, W678-W682 https://www.ajronline.org/doi/full/10.2214/AJR.13.10748
- Towbin AJ, Diniz LO. Schatzki ring in pediatric and young adult patients. Pediatr Radiol. 2012 Aug 11.
- Müller M, Gockel I, Hedwig P, et al. Is the Schatzki ring a unique esophageal entity?. World J Gastroenterol. 2011;17(23):2838–2843. doi:10.3748/wjg.v17.i23.2838 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3120943
- Ingelfinger FJ, Kramer P. Dysphagia produced by a contractile ring in the lower esophagus. Gastroenterology. 1953. 23:419-430.
- Schatzki R, Gary JE. Dysphagia due to a diaphragm-like localized narrowing in the lower esophagus (“lower esophageal ring”). Am J Roentgenol. 1953. 70:911-922.
- Goyal RK, Bauer JL, Spiro HM. The nature and location of lower esophageal ring. N Engl J Med. 1971 May 27. 284(21):1175-80.
- Schatzki Ring, Statistically Reexamined. John C. Pezzullo and Ann M. Lewicki. Radiology 2003 228:3, 609-613. https://doi.org/10.1148/radiol.2283021162
- Eponyms in Radiology of the Digestive Tract: Historical Perspectives and Imaging Appearances. Jeffrey P. Kanne, Charles A. Rohrmann, Jr, and Joel E. Lichtenstein. RadioGraphics 2006 26:1, 129-142 https://doi.org/10.1148/rg.261055084
- Schatzki Ring Treatment & Management. https://emedicine.medscape.com/article/182647-treatment
- Wills JC, Hilden K, Disario JA, Fang JC. A randomized, prospective trial of electrosurgical incision followed by rabeprazole versus bougie dilation followed by rabeprazole of symptomatic esophageal (Schatzki’s) rings. Gastrointest Endosc. 2008 May. 67(6):808-13.
- Gonzalez A, Sullivan MF, Bonder A, Allison HV, Bonis PA, Guelrud M. Obliteration of symptomatic Schatzki rings with jumbo biopsy forceps (with video). Dis Esophagus. 2014 Sep-Oct. 27(7):607-10.





{kind=link}