
Scheuermann’s disease
Scheuermann’s disease also known as Scheuermann kyphosis, juvenile kyphosis or juvenile discogenic disease, is a condition of hyperkyphosis that involves the vertebral bodies and discs of the spine identified by anterior wedging of greater than or equal to 5 degrees in 3 or more adjacent vertebral bodies 1. Scheuermann’s disease makes the upper back rounded so it looks hunched over. The thoracic spine is most commonly involved, although involvement can include the thoracolumbar/lumbar region as well 2.
Scheuermann’s kyphosis is caused by a structural abnormality in the spine. In a patient with Scheuermann’s disease, an x-ray from the side will show that, rather than the normal rectangular shape, several consecutive vertebrae have a more triangular shape (see Figure 1). This irregular shape causes the vertebrae to wedge together toward the front of the spine, decreasing the normal disk space and creating an exaggerated forward curvature in the upper back.
The curve caused by Scheuermann’s kyphosis is usually sharp and angular. It is also stiff and rigid; unlike a patient with postural kyphosis, a patient with Scheuermann’s disease is not able to correct the curve by standing up straight.
Scheuermann’s disease can sometimes be painful. If pain is present, it is commonly felt at the highest part or “apex” of the curve. Pain may also be felt in the lower back. This results when the spine tries to compensate for the rounded upper back by increasing the natural inward curve of the lower back. Activity can make the pain worse, as can long periods of standing or sitting.
Most commonly, Scheuermann’s kyphosis diagnosis is made in adolescents aged 12 to 17 years who present after their parents notice a postural deformity or “hunchbacked” appearance. Pain in the affected hyperkyphotic region may also be the cause of initial evaluation 3.
There is a hereditary component associated with Scheuermann’s disease, although the exact mode of transmission is still unclear. This is supported by the fact that incidence is higher in monozygotic versus dizygotic twins 2.
It’s important for teens with Scheuermann’s kyphosis to get the right treatment before growth is finished. The spine usually won’t continue to curve after they’re done growing. If your child complains of back pain or has a rounded upper back, talk to your doctor.
Scheuermann’s disease key points
- Prevalence: 1% to 8% in the United States 4.
- Sex: Male to female ratio is at least 2:1
- Age: Most commonly diagnosed in adolescents 12-17 years
- Rarely diagnosed in children less than 10 years.
- Classification:
- Type I (Classic) – Thoracic spine involvement only, with the apex of curve T7-T9
- Type II – Thoracic and lumbar involvement, with the apex of curve T10-T12
Figure 1. Scheuermann’s kyphosis
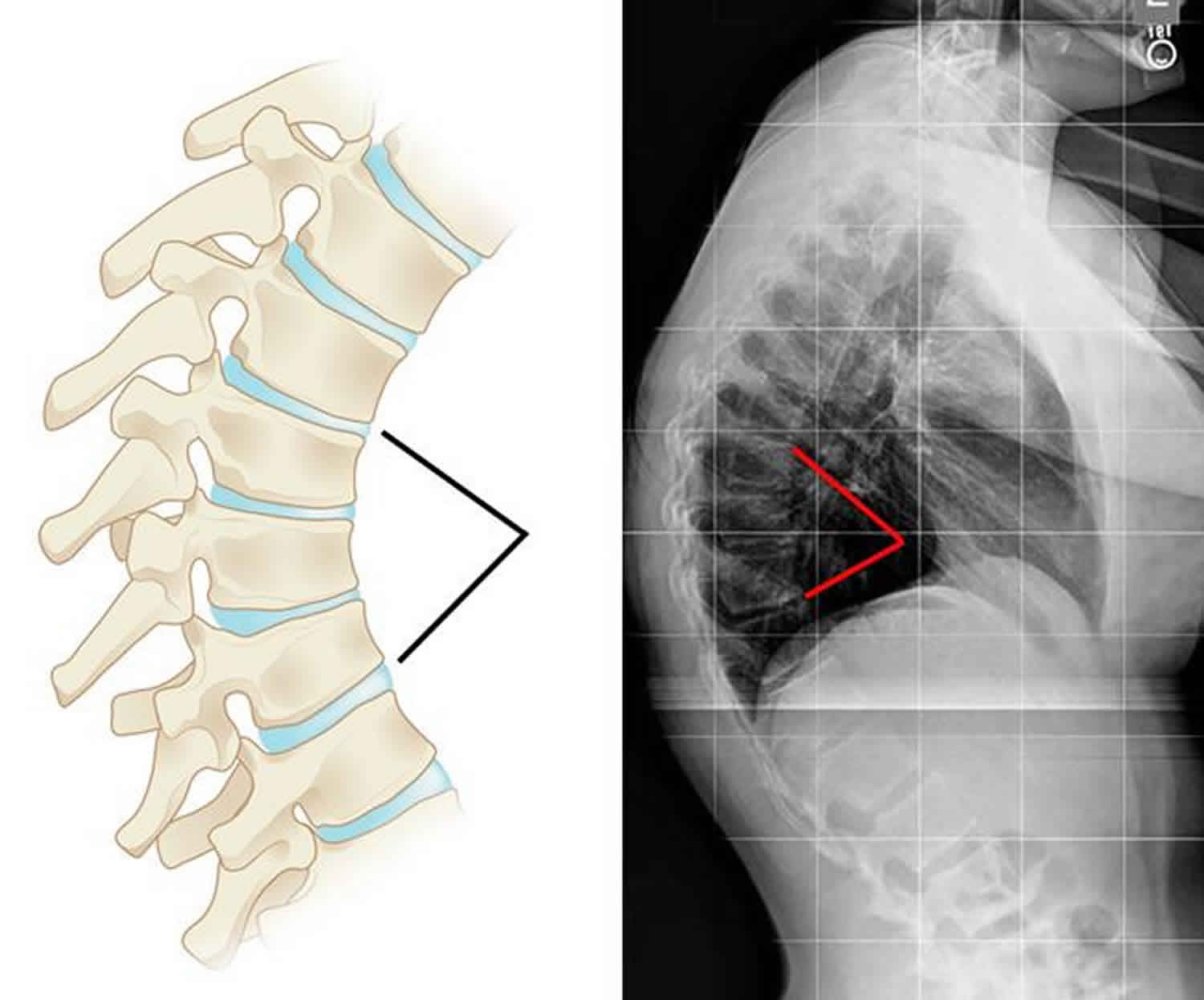
Footnote: Illustration and x-ray show the vertebral wedging that occurs in patients with Scheuermann’s kyphosis.
Scheuermann’s disease cause
The small bones (called vertebrae) that make up the spine are usually rectangular. They stack like bricks with flexible cartilage in between. When a child has Scheuermann’s disease, the front edge of some of the vertebrae in the upper back grow slower than the back edge. These vertebrae become wedge shaped, so when the vertebrae stack up, the spine curves, making the back round out.
The signs of Scheuermann’s kyphosis usually are first seen during or after the puberty growth spurt. Most kids are between 12 and 15 years old when they’re diagnosed. Definitive and universally accepted cause of Scheuermann kyphosis remains undetermined. As previously mentioned, a hereditary component is understood to contribute to Scheuermann’s disease development, although the mode of transmission is still unclear 5.
One growing theory, supported by histologic findings, suggests discordant vertebral endplate mineralization and ossification during growth which causes disproportional vertebral body growth and resultant classic wedge-shaped vertebral bodies that lead to kyphosis 6.
Suggested components that might explain or partially explain Scheuermann kyphosis, among many others, include abnormal collagen to proteoglycan ratios, dural cysts, childhood osteoporosis, biomechanical stressors such as tight hamstrings, and growth hormone hypersecretion.
The most common findings associated with Scheuermann’s disease include thoracic spine hyperkyphosis as defined by the diagnostic criteria commonly associated with irregular vertebral endplates, Schmorl nodes, and loss of disc space height noted on sagittal imaging studies 6.
Scheuermann’s disease symptoms
The main signs of Scheuermann’s disease or Scheuermann’s kyphosis are:
- A rounded, hunched back. Sometimes the rounding is hard to see. Other times it can be more noticeable. Children can’t straighten their curve by standing up.
- Back pain. About half of children with Scheuermann’s kyphosis have back pain.
The signs of kyphosis often become obvious during the growth spurt that happens around puberty.
Scheuermann’s disease diagnosis
To diagnose Scheuermann’s disease, a doctor will:
- examine the spine: the child will stand, bend from the waist, and lie down
- get X-rays: to see the curve
- do an MRI: if something else might be causing the problem (such as an infection or tumor)
- order breathing tests: if the kyphosis might affect breathing, the doctor may ask for pulmonary (lung) function tests
History and physical along with AP/lateral radiographs comprise the essential components for evaluating Scheuermann kyphosis. Lateral radiographs are required for diagnosis, and diagnostic criteria including the following 4:
- Rigid hyperkyphosis, greater than 40 degrees
- Anterior wedging, greater than or equal to 5 degrees in three or more adjacent vertebral bodies
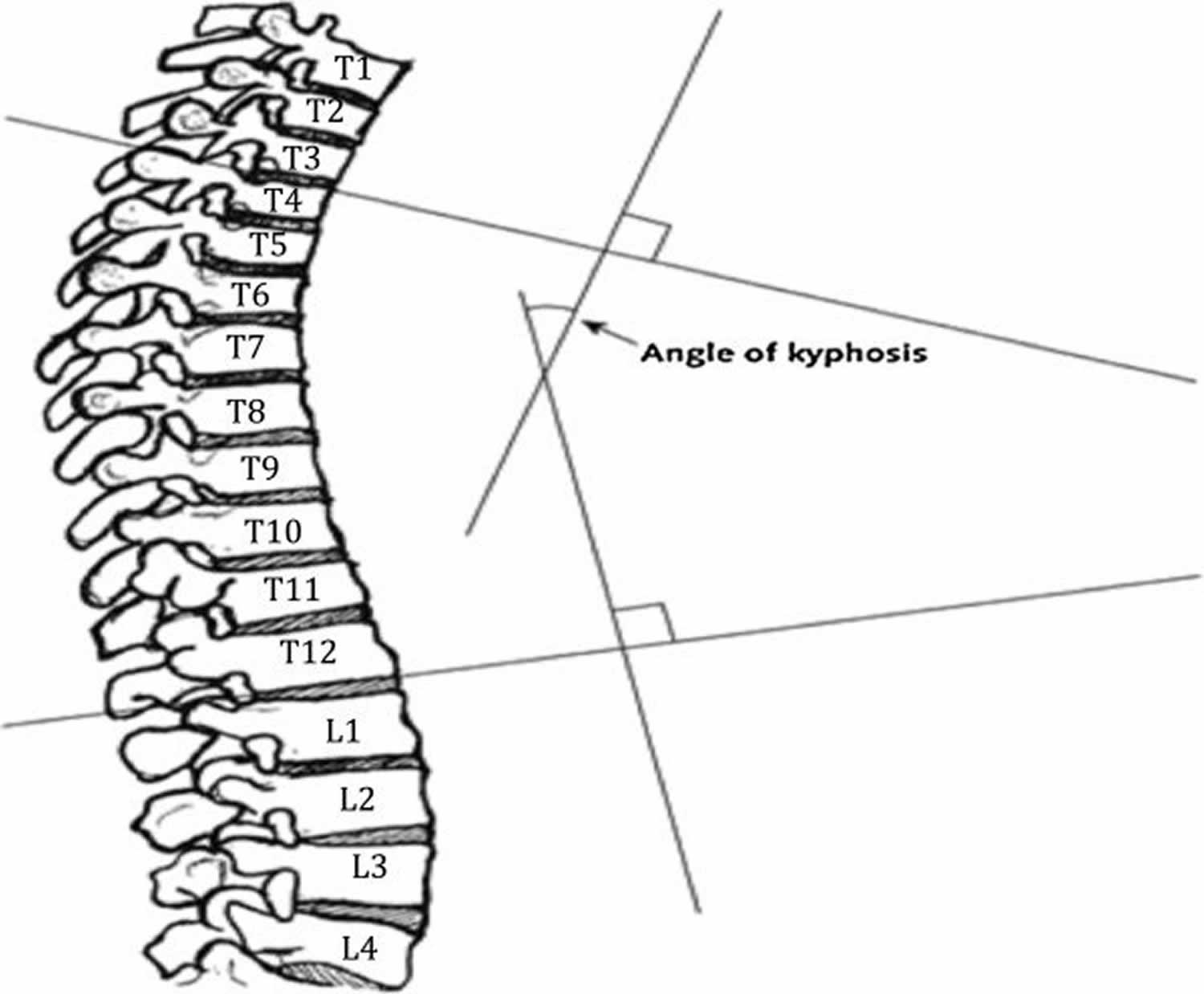
Technique for Determining Degree of Kyphosis on Lateral Imaging 4:
- Line is drawn along the superior endplate of the most tilted vertebrae on the cephalad portion of the kyphotic curve
- Line is drawn along the inferior endplate of the most tilted vertebrae on the caudal portion of the kyphotic curve
- The angle formed by the intersection of lines perpendicular to the above-described lines is the measured Cobb angle
- Hyperkyphosis is described as, measured Cobb angle greater than 40 degrees
Technique for Determining Degree of Anterior Wedging on Lateral Imaging 4:
- Line is drawn from posterior to anterior along the superior endplate
- Line is drawn from posterior to anterior along the inferior endplate
- The angle formed by the intersection of these lines anteriorly is the measured Wedge angle
- Anterior wedging of greater than or equal to 5 degrees in three or more adjacent vertebral bodies, with an associated rigid hyperkyphosis greater than 40 degrees, is diagnostic for Scheuermann’s disease
Other Associated Findings Noted on AP/Lateral Radiographs 4:
- Irregular vertebral endplates
- Schmorl nodes
- Loss of disc space height
- Scoliosis
- Spondylolysis/spondylolisthesis
- Disc herniation
Although typically not a necessity, MRI can be helpful to further evaluate anatomic changes or for pre-operative planning. CT imaging is usually not needed. There are also no specific laboratory tests or histologic findings necessary for the diagnosis of Scheuermann kyphosis.
Figure 2. Cobb angle for determining degree of kyphosis
Scheuermann’s disease treatment
Children with Scheuermann’s kyphosis will see an orthopedist (a doctor who treats conditions involving the bones). The orthopedist will examine the spine, look at the X-rays, and recommend treatment.
Nonoperative management 7:
Observation
If the rounding of the back isn’t likely to cause any problems, kyphosis may not need any treatment. Children will have routine checkups to make sure the rounding doesn’t start causing problems. Most cases will stop progressing when kids are done growing.
Stretching, lifestyle modification, nonsteroidal anti-inflammatory drugs (NSAIDs), plus/minus physical therapy
- Indication: Kyphosis less than 60 degrees and asymptomatic
- Course:
- Majority of patients fall into this category
- Patients typically do well without significant longterm complications
Extension bracing plus “A”
- Indication: Kyphosis 60 to 80 degrees plus/minus symptomatic
- Course:
- Bracing typically required for 12 to 24 months
- Most effective in skeletally immature patients
- Typically, does not improve curve but rather impedes progression
- Back braces 8. This brace is like a jacket that can be worn under clothes. It won’t straighten the curve, but will keep it from getting worse. Some kids wear the brace only at night, and others wear it for 18–20 hours a day. The brace is usually worn until a child stops growing.
- Milwaukee brace
- Kyphologic brace
- Thoracolumbosacral orthosis-style Boston brace
Surgery
Surgery isn’t usually needed. But doctors might recommend a procedure called a spinal fusion for a severe case that causes pain or breathing trouble.
Scheuermann’s disease surgery
Scheuermann’s kyphosis surgical management 2:
Spinal fusion, typically combination of anterior release + fusion as well as posterior instrumentation + fusion
Indications
- Kyphosis greater than 75 degrees causing unacceptable deformity
- Kyphosis greater than 75 degrees with associated pain
- Neurologic deficit/spinal cord compression
- Severe refractory pain
Course
- Majority of patients experience symptomatic improvement as well as improved curve deformity towards normal
- Operative/postoperative complications must be considered.
Scheuermann’s disease prognosis
The majority of patients are successfully treated with conservative measures 3. Pain in the affected region typically improves after skeletal maturity is reached, although patients with Scheuermann kyphosis are at increased risk of chronic back pain as compared to the general population.
Patients with a kyphotic curve less than 60 degrees at skeletal maturity typically have no long-term complications.
Complications
Potential complications
- Progressive cosmetic deformity
- Chronic back pain
- Neurologic deficits/spinal cord compression
Postoperative complications
- Pseudoarthrosis (most common complication)
- Persistent pain.
- Mansfield JT, Bennett M. Scheuermann Disease. [Updated 2019 Nov 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499966
- Palazzo C, Sailhan F, Revel M. Scheuermann’s disease: an update. Joint Bone Spine. 2014 May;81(3):209-14.
- Tomé-Bermejo F, Tsirikos AI. [Current concepts on Scheuermann kyphosis: clinical presentation, diagnosis and controversies around treatment]. Rev Esp Cir Ortop Traumatol. 2012 Nov-Dec;56(6):491-505.
- Makurthou AA, Oei L, El Saddy S, Breda SJ, Castaño-Betancourt MC, Hofman A, van Meurs JB, Uitterlinden AG, Rivadeneira F, Oei EH. Scheuermann disease: evaluation of radiological criteria and population prevalence. Spine. 2013 Sep 01;38(19):1690-4.
- Zaidman AM, Zaidman MN, Strokova EL, Korel AV, Kalashnikova EV, Rusova TV, Mikhailovsky MV. The mode of inheritance of Scheuermann’s disease. Biomed Res Int. 2013;2013:973716.
- Aufdermaur M. Juvenile kyphosis (Scheuermann’s disease): radiography, histology, and pathogenesis. Clin. Orthop. Relat. Res. 1981 Jan-Feb;(154):166-74.
- Patel DR, Kinsella E. Evaluation and management of lower back pain in young athletes. Transl Pediatr. 2017 Jul;6(3):225-235.
- Weiss HR, Turnbull D, Bohr S. Brace treatment for patients with Scheuermann’s disease – a review of the literature and first experiences with a new brace design. Scoliosis. 2009 Sep 29;4:22.





{kind=link}