
What is shingles
Shingles also called herpes zoster or zoster, is a painful blistering rash disease caused by the varicella zoster virus (VZV) the same virus that causes chickenpox, that reactivates (wakes up) causing a painful blistering rash. If you’ve ever had chickenpox, you can get shingles. Most cases of chickenpox occur in children under age 15, but older children and adults can get it too. Chickenpox (varicella-zoster virus infection) spreads very easily from one person to another. After the chickenpox clears, the varicella-zoster virus (VZV) stays inside your body inside the nerves within dorsal root ganglia and lie dormant for years. The varicella-zoster virus (VZV) may not cause problems for many years. Eventually, it may reactivates (wakes up) and travels along nerve pathways to your skin — producing shingles (herpes zoster) — a painful, blistering rash. But, not everyone who’s had chickenpox will develop shingles. Shingles tends to cause more pain and less itching than chickenpox. As you get older, the varicella-zoster virus (VZV) may reappear as shingles. Although shingles is most common in people over age 50, anyone who has had chickenpox is at risk. Shingles (herpes zoster) often affects people with weak immunity. People with various kinds of cancer have a 40% increased risk of developing shingles. People who have had shingles rarely get it again; the chance of getting a second episode is about 1%.
Almost 1 out of 3 people in the United States will develop shingles in their lifetime. There are an estimated 1 million cases of shingles each year in this country. Anyone who has recovered from chickenpox may develop shingles; even children can get shingles. However, the risk of shingles increases as you get older. About half of all cases occur in people 60 years old or older. Older adults also are more likely to have severe disease.
Shingles can lead to severe nerve pain called postherpetic neuralgia (PHN) that can last for months or years after the rash goes away.
Shingles generally lasts between two and six weeks. Most people get shingles only once, but it is possible to get it two or more times.
There is no cure for shingles. Early treatment with medicines that fight the virus may help. These medicines may also help prevent lingering pain.
- If you think you might have shingles, talk to your doctor as soon as possible. It’s important to see your doctor no later than 3 days after the rash starts. The doctor will confirm whether or not you have shingles and can make a treatment plan. Although there is no cure for shingles, early treatment with drugs that fight the virus can help the blisters dry up faster and limit severe pain. Shingles can often be treated at home. People with shingles rarely need to stay in a hospital.
The risk of getting shingles increases with age. A vaccine can reduce your risk of getting shingles or lessen its effects. Your doctor may recommend getting this vaccine after your 50th birthday or once you reach 60 years of age. There’s another — and maybe even more important — reason for getting the shingles vaccine. If you’ve had chickenpox, you can still get shingles after getting shingles vaccine. The vaccine also lessens your risk of developing serious complications from shingles, such as life-disrupting nerve pain.
The nerve pain can last long after the shingles rash goes away. Some people have this nerve pain, called post-herpetic neuralgia (PHN), for many years. The pain can be so bad that it interferes with your everyday life. The shingles vaccine reduces your risk of developing this nerve pain, even more than it reduces your risk of getting shingles.
An anti-viral medicine may also prevent long-lasting nerve pain if your get shingles. It’s most effective when started within 3 days of seeing the rash. The anti-viral medicine can also make shingles symptoms milder and shorter.
- Shingles and chickenpox are caused by the same virus called varicella zoster virus.
- An estimated 1 million people get shingles each year in the United States.
- Anyone who has had chickenpox can get shingles, and you can get shingles at any age.
- Your risk of getting shingles and having more severe pain increases as you get older.
- The Centers for Disease Control and Prevention (CDC) recommends people age 50 and older get two doses of the shingles vaccine Shingrix (recombinant zoster vaccine), separated by 2 to 6 months, to protect against shingles and its complications. Adults 19 years and older who have weakened immune systems because of disease or therapy should also get two doses of Shingrix (recombinant zoster vaccine), as they have a higher risk of getting shingles and related complications.
You can’t catch shingles from someone. However, if you have a shingles rash, you can pass the virus to someone who has not had chickenpox (or the chickenpox vaccine) can get this virus. This would usually be a child, when this happens, the person develops chickenpox, not shingles. The virus spreads through direct contact with the rash and cannot spread through the air. Chickenpox can be dangerous for some people. Until your shingles blisters scab over, you are contagious and should avoid physical contact with anyone who hasn’t yet had chickenpox or the chickenpox vaccine, especially people with weakened immune systems, pregnant women and newborns.
If you have shingles, what can you do to prevent spreading the virus?
When you have shingles, you’re only contagious while you have blisters. To prevent spreading the virus while you have blisters, the Centers for Disease Control and Prevention (CDC) recommends that you:
- Cover the rash
- Wash your hands often and try to avoid touching the rash
- Avoid being around people for whom catching the virus could be dangerous
The varicella-zoster virus is especially dangerous for these people
- Catching this virus and getting chickenpox can be dangerous for women who are pregnant and have not had chickenpox or gotten the chickenpox vaccine. In this situation, the virus can harm the woman’s unborn baby.
Babies less than 1 month old and people who have a weak immune system can also have complications if they catch the virus. People who have a weak immune system include those who are:
- HIV positive
- Taking medicine that weakens their immune system
- Receiving chemotherapy or radiation treatments
You’re not contagious before you develop blisters or after the blisters scab over. Be sure to take precautions while you have blisters.
A person must have had chickenpox to get shingles. Some people who have had chickenpox have a higher risk of getting shingles. But, not everyone who’s had chickenpox will develop shingles.
Most people who develop shingles have only one episode during their lifetime. However, a person can have a second or even a third episode.
- One out of every three people 60 years old or older will get shingles.
- One out of six people older than 60 years who get shingles will have severe pain. The pain can last for months or even years.
- The most common complication of shingles is severe pain where the shingles rash was. This pain can be debilitating. There is no treatment or cure from this pain. As people get older, they are more likely to develop long-term pain as a complication of shingles and the pain is likely to be more severe.
- Shingles may also lead to serious complications involving the eye.
- Very rarely, shingles can also lead to pneumonia, hearing problems, blindness, brain inflammation (encephalitis), or death.
Some illnesses and medical treatments can weaken a person’s immune system and increase the risk of getting shingles. These include:
- Are 50 years of age or older
- Have an illness or injury
- Are under great stress
- Have medical conditions that keep their immune systems from working properly:
- Cancers like leukemia and lymphoma
- Human immunodeficiency virus (HIV)/AIDS
- Some cancer treatments, such as chemotherapy or radiation
- Medicine taken to prevent rejection of a transplanted organ. Immunosuppressive drugs, such as steroids and drugs that are given after organ transplantation.
- Cortisone when taken for a long time
There is no cure for shingles. Early treatment with medicines that fight the virus may help. These medicines may also help prevent lingering pain.
- If you think you might have shingles, talk to your doctor as soon as possible. It’s important to see your doctor no later than 3 days after the rash starts. The doctor will confirm whether or not you have shingles and can make a treatment plan. Although there is no cure for shingles, early treatment with drugs that fight the virus can help the blisters dry up faster and limit severe pain. Shingles can often be treated at home. People with shingles rarely need to stay in a hospital.
The risk of getting shingles increases with age. A vaccine can reduce your risk of getting shingles or lessen its effects. Your doctor may recommend getting this vaccine after your 50th birthday or once you reach 60 years of age. There’s another — and maybe even more important — reason for getting the shingles vaccine. If you’ve had chickenpox, you can still get shingles after getting shingles vaccine. The vaccine also lessens your risk of developing serious complications from shingles, such as life-disrupting nerve pain.
The nerve pain can last long after the shingles rash goes away. Some people have this nerve pain, called post-herpetic neuralgia (PHN), for many years. The pain can be so bad that it interferes with your everyday life. The shingles vaccine reduces your risk of developing this nerve pain, even more than it reduces your risk of getting shingles.
An anti-viral medicine may also prevent long-lasting nerve pain if your get shingles. It’s most effective when started within 3 days of seeing the rash. The anti-viral medicine can also make shingles symptoms milder and shorter.
Protect Yourself Against Shingles
Adults 60 years old or older should talk to their healthcare professional about getting a one-time dose of the shingles vaccine.
- The shingles vaccine can reduce your risk of shingles and the long-term pain it can cause 3.
- Persons who have already had shingles or who have a chronic medical condition can receive the shingles vaccine.
- In a clinical trial involving thousands of adults 60 years old or older, the vaccine reduced the risk of shingles by about half. Even if the shingles vaccine doesn’t prevent you from getting shingles, it can still reduce the chance of having long-term pain or post-herpetic neuralgia.
Talk with your healthcare professional for more information and to find out if the shingles vaccine is right for you.
Adults can get vaccines at doctors’ offices, pharmacies, workplaces, community health clinics, and health departments. To find a place to get a vaccine near you, go to https://vaccinefinder.org/
Most private health insurance plans cover recommended vaccines. Check with your insurance provider for details and for a list of vaccine providers. Medicare Part D plans cover shingles vaccine, but there may be costs to you depending on your specific plan.
If you do not have health insurance, visit https://www.healthcare.gov/ to learn more about health insurance options.
Complications of shingles
The most common complication of shingles is a condition called post-herpetic neuralgia (PHN). People with post-herpetic neuralgia have severe pain in the areas where they had the shingles rash, even after the rash clears up. Post-herpetic neuralgia is diagnosed in people who have pain that persists after their rash has resolved. Some define post-herpetic neuralgia as any duration of pain after the rash resolves; others define it as duration of pain for more than 30 days, or for more than 90 days after rash onset.
The pain from post-herpetic neuralgia may be severe and debilitating, but it usually resolves in a few weeks or months. Some people can have pain from post-herpetic neuralgia for many years and can interfere with daily life.
A person’s risk of having post-herpetic neuralgia after herpes zoster increases with age. As people get older, they are more likely to develop post-herpetic neuralgia, and the pain is more likely to be severe. Post-herpetic neuralgia occurs rarely among people under 40 years of age but can occur in approximately 13% (and possibly more) of untreated people who are 60 years of age and older with herpes zoster. Older adults are more likely to have post-herpetic neuralgia and to have longer lasting and more severe pain. Other predictors of post-herpetic neuralgia include the level of pain a person has when they have the rash and the size of their rash.
Other complications of herpes zoster include:
- Shingles may also lead to serious complications involving the eye (herpes zoster ophthalmicus, when the ophthalmic division of the fifth cranial nerve is involved) may result in vision loss.
- Bacterial superinfection of the lesions, usually due to Staphylococcus aureus and, less commonly, due to group A beta hemolytic streptococcus.
- Cranial and peripheral nerve palsies. Depending on which nerves are affected, shingles can cause an inflammation of the brain (encephalitis), facial paralysis, or hearing or balance problems. Muscle weakness in about one in 20 patients. Facial nerve palsy is the most common result (Ramsay Hunt syndrome). There is a 50% chance of complete recovery, but some improvement can be expected in nearly all cases
- Deep blisters that take weeks to heal followed by scarring.
- Very rarely, shingles can also lead to pneumonia, hearing problems, blindness, brain inflammation (meningoencephalitis), hepatitis, acute retinal necrosis or death.
People with compromised or suppressed immune systems are more likely to have complications from herpes zoster. They are more likely to have severe rash that lasts longer. Also, they are at increased risk of developing disseminated herpes zoster.
Shingles (herpes zoster) in the early months of pregnancy can harm the fetus, but luckily this is rare. Shingles in late pregnancy can cause chickenpox in the fetus or newborn. Herpes zoster may then develop as an infant.
What does shingles look like?
Shingles or Herpes zoster is a localized, blistering and painful rash caused by reactivation of varicella zoster virus (VZV). It is characterized by dermatomal distribution (Dermatome see Figure 6 below), that is the blisters are confined to the cutaneous distribution of one or two adjacent sensory nerves.
The distribution of shingles refers to how the skin lesions are scattered or spread out. The localization of multiple lesions in certain regions helps diagnosis, as shingles tend to have characteristic distributions.
Figure 1. Shingles rash (blisters) – the typical early onset of herpes zoster (shingles) includes blisters in groups. The blisters often have a central depression.

Figure 2. Shingles rash body – typical of zoster (shingles), these images display grouped blisters with central depressions in a red, band-like distribution.

Figure 3. Shingles rash


Figure 4. Shingles on face

Note: If blisters appear on the tip of your nose, it may be a warning of possible eye problems. Shingles that involve the eye are called ocular shingles or herpes zoster ophthalmicus. Signs and symptoms of shingles in the eye are blisters around the eye or on the eyelid, swelling and redness of the eye or eyelid, and eye pain. Some people become sensitive to light. After a bout with shingles that involves the eye, a person can have blurred vision or feel that something is in the eye.
Anyone who gets blisters on the nose should see a doctor immediately. Without treatment, permanent eye damage can result. Glaucoma, scarring, and even blindness are possible. People who have shingles in the eye also may have a higher risk for having a stroke.
Figure 5. Shingles in the eye

Note: Shingles rash along the face or brow area may involve the eye. The varicella-zoster virus can travel through the nerve fibers and emerge in the cornea. Eye pain, redness, tearing, and blurring are common symptoms of ocular shingles. If this happens, your eye care professional may prescribe oral anti-viral treatment to reduce the risk of inflammation and scarring in the cornea. Shingles can also cause decreased sensitivity in the cornea. Corneal problems may arise months after the shingles are gone from the rest of the body. If you experience shingles in your eye, or nose, or on your face, it’s important to have your eyes examined several months after the shingles have cleared. If left untreated, this infection can lead to permanent eye damage.
Figure 6. Dermatome (spinal nerves sensory innvervation)
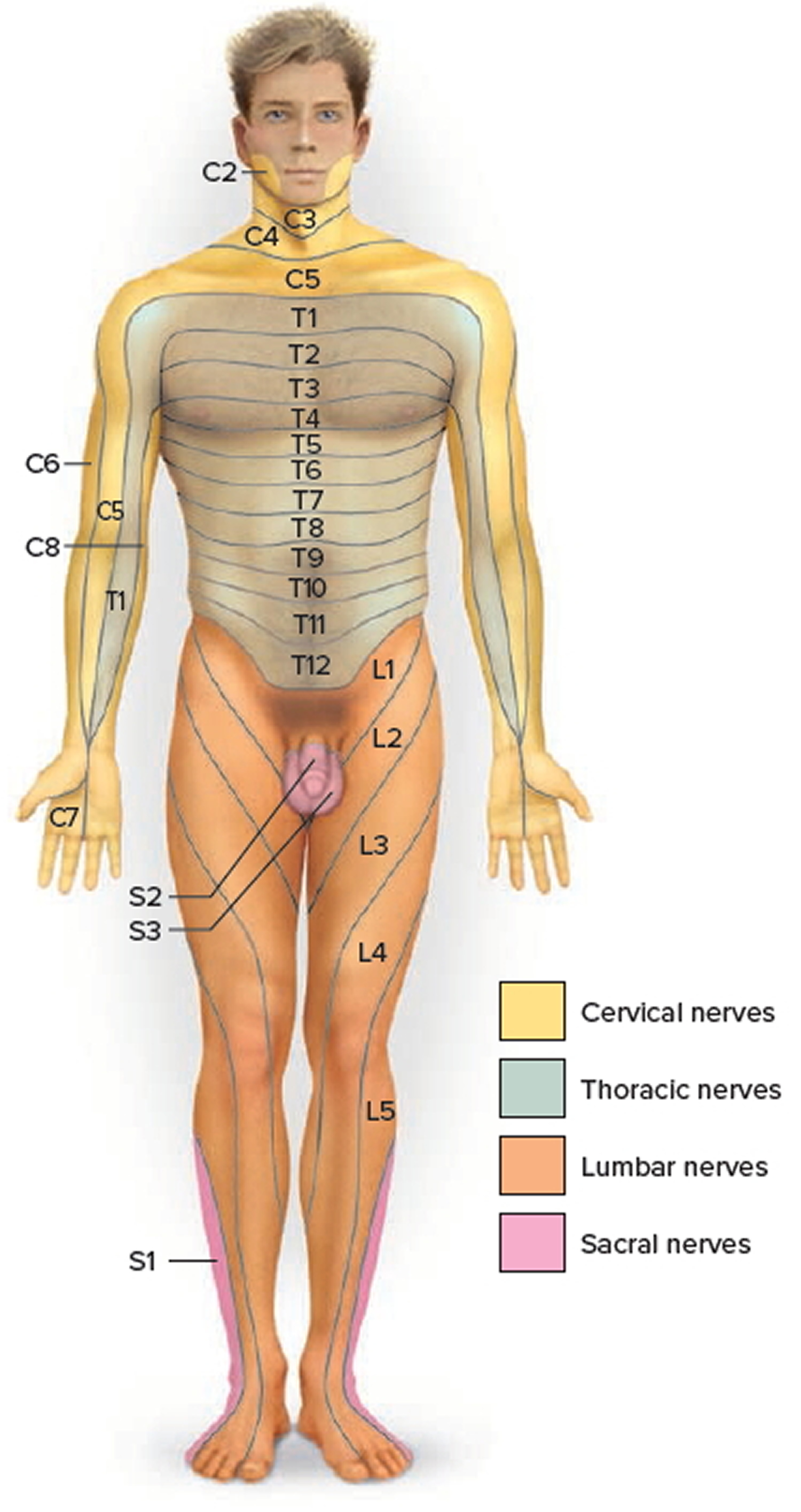
Footnote: A dermatome is an area of skin that is primarily supplied by a single nerve root – communicating sensation from this skin region to the brain. The skin over the entire body is supplied by somatic sensory neurons that carry nerve impulses from the skin into the spinal cord and brain. Each spinal nerve contains sensory neurons that serve a specific, predictable segment of the body. One of the cranial nerves, the Trigeminal (V) nerve, serves most of the skin of the face and scalp. The area of the skin that provides sensory input to the central nervous system (CNS) via one pair of spinal nerves or the Trigeminal (V) nerve is called a dermatome. The varicella zoster virus lie dormant inside these nerves and only to be reactivated and travel along the nerve pathways to your skin — producing shingles — a painful, blistering rash.
What causes shingles
Shingles is caused by the varicella zoster virus (VZV), the same virus that causes chickenpox. After a person recovers from chickenpox, the virus stays dormant (inactive) in the body (in the nervous system). Shingles appears when the virus wakes up. Scientists aren’t sure why the virus can reactivates or “wakes up” years later, causing shingles. A short-term weakness in immunity may cause this. Shingles is more common in older adults and in people who have weakened immune systems.
Shingles cannot be passed from one person to another. However, the virus that causes shingles, the varicella zoster virus, can spread from a person with active shingles to cause chickenpox in someone who had never had chickenpox or received chickenpox vaccine.
The virus is spread through direct contact with fluid from the rash blisters caused by shingles.
A person with active shingles can spread the virus when the rash is in the blister-phase. A person is not infectious before the blisters appear. Once the rash has developed crusts, the person is no longer infectious.
Shingles is less contagious than chickenpox and the risk of a person with shingles spreading the virus is low if the rash is covered.
If you have shingles, you should:
- Cover the rash.
- Avoid touching or scratching the rash.
- Wash your hands often to prevent the spread of varicella zoster virus.
- Avoid contact with the people below until your rash has developed crusts
- pregnant women who have never had chickenpox or the chickenpox vaccine;
- premature or low birth weight infants; and
- people with weakened immune systems, such as people receiving immunosuppressive medications or undergoing chemotherapy, organ transplant recipients, and people with human immunodeficiency virus (HIV) infection.
Risk factors for shingles
Anyone who has ever had chickenpox can develop shingles. Most adults in the United States had chickenpox when they were children, before the advent of the routine childhood vaccination that now protects against chickenpox.
Factors that may increase your risk of developing shingles include:
- Being older than 50. Shingles is most common in people older than 50. The risk increases with age. Some experts estimate that half the people age 80 and older will have shingles.
- Having certain diseases. Diseases that weaken your immune system, such as HIV/AIDS and cancer, can increase your risk of shingles.
- Undergoing cancer treatments. Radiation or chemotherapy can lower your resistance to diseases and may trigger shingles.
- Taking certain medications. Drugs designed to prevent rejection of transplanted organs can increase your risk of shingles — as can prolonged use of steroids, such as prednisone.
Triggering factors for shingles
Shingles triggering factors are sometimes recognized, such as:
- Pressure on the nerve roots
- Radiotherapy at the level of the affected nerve root
- Spinal surgery
- An infection
- An injury (not necessarily to the spine)
- Contact with someone with varicella (chickenpox) or herpes zoster (shingles)
Shingles symptoms
Early signs of shingles include burning or shooting pain and tingling or itching, usually on one side of the body or face. The most common place for shingles is a band that goes around one side of your waistline. The pain can be mild to severe. Rashes or blisters appear anywhere from one to 14 days later. The rash consists of blisters that typically scab over in 7 to 10 days. The rash usually clears up within 2 to 4 weeks. If shingles appears on your face, it may affect your vision or hearing. The pain of shingles may last for weeks, months, or even years after the blisters have healed.
- The warning: Before the rash develops, people often have pain, itching, burning or tingling in the area where the rash will develop. And area of skin may feel very sensitive. This usually occurs in a small area on 1 side of the body. These symptoms can come and go or be constant. The lymph nodes draining the affected area are often enlarged and tender. Most people experience this for 1 to 5 days before the rash appears. It can last longer.
- Rash: A rash then appears in the same area. Most commonly, the rash occurs in a single stripe around either the left or the right side of the body. In other cases, the rash occurs on one side of the face. In rare cases (usually among people with weakened immune systems), the rash may be more widespread and look similar to a chickenpox rash. Shingles can affect the eye and cause loss of vision.
- Blisters: The rash soon turns into groups of clear blisters. The blisters turn yellow or bloody before they crust over (scab) and heal. The blisters tend to last 2 to 3 weeks.
- Pain: It is uncommon to have blisters without pain. Once the blisters heal, the pain tends to lessen. The pain can last for months after the blisters clear.
- Flu-like symptoms: The person may get a fever, headache, chills or upset stomach with the rash.
The chest (thoracic), neck (cervical), forehead (ophthalmic) and lumbar or sacral sensory nerve supply regions are most commonly affected at all ages. The frequency of ophthalmic herpes zoster or herpes zoster ophthalmicus (shingles affecting the eye) increases with age. Herpes zoster occasionally causes blisters inside the mouth or ears, and can also affect the genital area. Sometimes there is pain without rash—herpes zoster “sine eruptione”—or rash without pain, most often in children.
Pain and general symptoms subside gradually as the eruption disappears. In uncomplicated cases, recovery is complete within 2–3 weeks in children and young adults, and within 3–4 weeks in older patients.
How Long Does Shingles Last?
Most cases of shingles last 3 to 5 weeks. Shingles follows a pattern:
- The first sign is often burning or tingling pain; sometimes, it includes numbness or itching on one side of the body.
- Somewhere between 1 and 5 days after the tingling or burning feeling on the skin, a red rash will appear.
- A few days later, the rash will turn into fluid-filled blisters.
- About a week to 10 days after that, the blisters dry up and crust over.
- A couple of weeks later, the scabs clear up.
Most people get shingles only one time. But, it is possible to have it more than once.
Longterm pain and other lasting problems
After the shingles rash goes away, some people may be left with ongoing pain called post-herpetic neuralgia or PHN. The pain is felt in the area where the rash had been. For some people, post-herpetic neuralgia is the longest lasting and worst part of shingles. The older you are when you get shingles, the greater your chance of developing post-herpetic neuralgia.
The post-herpetic neuralgia pain can cause depression, anxiety, sleeplessness, and weight loss. Some people with post-herpetic neuralgia find it hard to go about their daily activities, like dressing, cooking, and eating. Talk with your doctor if you have any of these problems.
There are medicines that may help with post-herpetic neuralgia. Steroids may lessen the pain and shorten the time you’re sick. Analgesics, antidepressants, and anticonvulsants may also reduce the pain. Usually, post-herpetic neuralgia will get better over time.
Some people have other problems that last after shingles has cleared up. For example, the blisters caused by shingles can become infected. They may also leave a scar. It is important to keep the area clean and try not to scratch the blisters. Your doctor can prescribe an antibiotic treatment if needed.
See your doctor right away if you notice blisters on your face—this is an urgent problem. Blisters near or in the eye can cause lasting eye damage or blindness. Hearing loss, a brief paralysis of the face, or, very rarely, swelling of the brain (encephalitis) can also occur.
Prevention of shingles
Herpes zoster is infectious to people who have not previously had chickenpox. A shingles vaccine may help prevent shingles. Two vaccines may help prevent shingles — the chickenpox (varicella) vaccine and the shingles (varicella-zoster) vaccine. Because the risk of serious complications from herpes zoster is more likely in older people, those aged over 60 years might consider the varicella-zoster vaccine, which can reduce the incidence of herpes zoster by half. In people who do get herpes zoster despite being vaccinated, the symptoms are usually less severe, and post-herpetic neuralgia is less likely to develop.
Herpes zoster vaccination is contraindicated in immunosuppressed patients due to the risk of it causing disseminated herpes zoster infection.
In the United States, Shingrix (varicella-zoster vaccine) was approved by the Food and Drug Administration (FDA) in 2017. Studies suggest that Shingrix offers protection against shingles for more than five years. Shingrix is a nonliving vaccine made of a virus component. It is given in two doses, with 2-6 months between doses.
Shingrix is approved and recommended for people age 50 and older, including those who’ve previously received the Zostavax vaccine or had shingles.
The Zostavax vaccine is no longer sold in the U.S., but other countries may still use it.
The most common side effects of either shingles vaccine are redness, pain, tenderness, swelling and itching at the injection site, and headaches.
The shingles vaccine doesn’t guarantee that you won’t get shingles. But this vaccine will likely reduce the course and severity of the disease and reduce your risk of postherpetic neuralgia.
The shingles vaccine is used only as a prevention strategy. It’s not intended to treat people who currently have the disease. Talk to your doctor about which option is right for you.
Chickenpox vaccine
The varicella vaccine (Varivax) has become a routine childhood immunization to prevent chickenpox. The vaccine is also recommended for adults who’ve never had chickenpox. Though the vaccine doesn’t guarantee you won’t get chickenpox or shingles, it can reduce your chances of complications and reduce the severity of the disease.
Shingles vaccine
The Centers for Disease Control and Prevention (CDC) recommends people age 50 and older get two doses of the shingles vaccine Shingrix (recombinant zoster vaccine), separated by 2 to 6 months, to protect against shingles and its complications. Adults 19 years and older who have weakened immune systems because of disease or therapy should also get two doses of Shingrix (recombinant zoster vaccine), as they have a higher risk of getting shingles and related complications.
Routine vaccination of people 50 years old and older 4:
- Whether or not they report a prior episode of herpes zoster.
- Whether or not they report a prior dose of Zostavax, a shingles vaccine that is no longer available for use in the United States.
- It is not necessary to screen, either verbally or by laboratory serology, for evidence of prior varicella.
In the United States, Shingrix (recombinant zoster vaccine) was approved by the Food and Drug Administration (FDA) in 2017. Studies suggest that Shingrix offers protection against shingles for more than five years. Shingrix is a nonliving vaccine made of a virus component. It is given in two doses, with 2-6 months between doses.
The shingles vaccine is used only as a prevention strategy. It’s not intended to treat people who currently have the disease. Talk to your doctor about which option is right for you.
Shingrix is approved and recommended for people age 50 and older, including those who’ve previously received the Zostavax vaccine or had shingles.
- The Zostavax vaccine is no longer sold in the U.S., but other countries may still use it.
The most common side effects of either shingles vaccine are redness, pain, tenderness, swelling and itching at the injection site, and headaches.
The shingles vaccine doesn’t guarantee that you won’t get shingles. But this vaccine will likely reduce the course and severity of the disease and reduce your risk of postherpetic neuralgia.
Adults 50 years old or older should talk to their healthcare professional about getting two doses of the shingles vaccine Shingrix (recombinant zoster vaccine), separated by 2 to 6 months, to protect against shingles and its complications.
- The shingles vaccine can reduce your risk of shingles and the long-term pain it can cause 3.
- Persons who have already had shingles or who have a chronic medical condition can receive the shingles vaccine.
- In a clinical trial involving thousands of adults 60 years old or older, the vaccine reduced the risk of shingles by about half. Even if the shingles vaccine doesn’t prevent you from getting shingles, it can still reduce the chance of having long-term pain or post-herpetic neuralgia (PHN).
Talk with your healthcare professional for more information and to find out if the shingles vaccine is right for you.
Adults can get vaccines at doctors’ offices, pharmacies, workplaces, community health clinics, and health departments. To find a place to get a vaccine near you, go to https://vaccinefinder.org/
Most private health insurance plans cover recommended vaccines. Check with your insurance provider for details and for a list of vaccine providers. Medicare Part D plans cover shingles vaccine, but there may be costs to you depending on your specific plan.
If you do not have health insurance, visit https://www.healthcare.gov/ to learn more about health insurance options.
Who Should Get Shingles Vaccine?
The Centers for Disease Control and Prevention (CDC) recommends people age 50 and older get two doses of the shingles vaccine Shingrix (recombinant zoster vaccine), separated by 2 to 6 months, to protect against shingles and its complications. Adults 19 years and older who have weakened immune systems because of disease or therapy should also get two doses of Shingrix (recombinant zoster vaccine), as they have a higher risk of getting shingles and related complications.
What Are the Possible Side Effects of Shingles Vaccine?
A vaccine, like any medicine, could possibly cause serious problems, such as severe allergic reactions. However, the risk of a vaccine causing serious harm, or death, is extremely small.
No serious problems have been identified with shingles vaccine.
Mild side effects of shingles vaccine:
- Redness, soreness, swelling, or itching at the site of the injection (about 1 person in 3).
- Headache (about 1 person in 70).
It is safe to be around infants and young children, pregnant women, or people with weakened immune systems after you get the shingles vaccine. There is no documentation of a person getting chickenpox from someone who has received the shingles vaccine (which contains varicella zoster virus).
Some people who get the shingles vaccine will develop a chickenpox-like rash near the place where they were vaccinated. As a precaution, this rash should be covered until it disappears.
Like all vaccines, shingles vaccine is being closely monitored for unusual or severe problems by CDC and FDA.
Signs of a severe allergic reaction can include hives, swelling of the face and throat, difficulty breathing, a fast heartbeat, dizziness, and weakness. These would start a few minutes to a few hours after the vaccination. If you have a severe allergic reaction or other emergency that can’t wait, call your local emergency number or get the person to the nearest hospital. Otherwise, see your doctor.
Who Should Not Get Shingles Vaccine?
Shingrix (recombinant zoster vaccine) should NOT be administered to 4, 5:
- A person with a history of severe allergic reaction, such as anaphylaxis, to any component of this vaccine.
- A person experiencing an acute episode of herpes zoster. Shingrix is not a treatment for herpes zoster or postherpetic neuralgia (PHN). The general guidance for any vaccine is to wait until the acute stage of the illness is over and symptoms abate.
There is currently no CDC recommendation for Shingrix use in pregnancy; therefore, providers should consider delaying vaccination until after pregnancy. There is no recommendation for pregnancy testing before vaccination with Shingrix. Recombinant vaccines such as Shingrix pose no known risk to people who are breastfeeding or to their infants. Providers may consider vaccination without regard to breastfeeding status if Shingrix is otherwise indicated.
Adults with a minor acute illness, such as a cold, can receive Shingrix. Adults with a moderate or severe acute illness should usually wait until they recover before getting the vaccine.
Diagnosis of shingles
Shingles is usually diagnosed based on the history of pain on one side of your body, along with the telltale rash and blisters. Your doctor may also take a tissue scraping or culture of the blisters for examination in the laboratory.
Shingles treatment
There’s no cure for shingles, but prompt treatment with prescription antiviral drugs can speed healing and reduce your risk of complications. These medications include:
- Acyclovir (Zovirax)
- Valacyclovir (Valtrex)
- Famciclovir
Antiviral treatment can reduce pain and the duration of symptoms if started within one to three days after the onset of herpes zoster. Aciclovir 800 mg 5 times daily for seven days is most often prescribed. Valaciclovir and famciclovir are also useful.
In healthy children shingles is often relatively mild and may not require treatment, however, children who take courses of systemic steroids, e.g., for asthma, are rendered vulnerable for up to three months after treatment is complete – if the child develops chickenpox in this period parents should seek urgent competent advice as treatment with oral antiviral therapy will be required.
Immunocompromised patients
- Should continue on with oral antiviral therapy for two days after crusting of the lesions
- If the patient is unwell / develops widespread (disseminated) zoster, hospital admission will be needed
Management of acute herpes zoster may include:
- Rest and pain relief
- Protective ointment applied to the rash, such as petroleum jelly.
- Oral antibiotics for secondary infection
Shingles can cause severe pain, so your doctor also may prescribe:
- Capsaicin topical patch (Qutenza)
- Anticonvulsants, such as gabapentin (Neurontin)
- Tricyclic antidepressants, such as amitriptyline
- Numbing agents, such as lidocaine, delivered via a cream, gel, spray or skin patch
- Medications that contain narcotics, such as codeine
- An injection including corticosteroids and local anesthetics
Shingles generally lasts between two and six weeks. Most people get shingles only once, but it is possible to get it two or more times.
Shingles medication
It is best to get treatment immediately. Treatment can include:
Pain relievers to help ease the pain: The pain can be very bad, and prescription painkillers may be necessary. Your doctor also may prescribe:
- Capsaicin topical patch (Qutenza)
- Anticonvulsants, such as gabapentin (Neurontin)
- Tricyclic antidepressants, such as amitriptyline
- Numbing agents, such as lidocaine, delivered via a cream, gel, spray or skin patch
- Medications that contain narcotics, such as codeine
- An injection including corticosteroids and local anesthetics
Post-herpetic neuralgia may be difficult to treat successfully. It may respond to any of the following.
- Local anesthetic applications
- Topical capsaicin
- Tricyclic antidepressant medications such as amitriptyline
- Anti-epileptic medications gabapentin and pregabalin
- Transcutaneous electrical nerve stimulation or acupuncture
- Botulinum toxin into the affected area
- Early use of antiviral medication
Nonsteroidal anti-inflammatories (NSAIDs) and opioids are generally unhelpful.
Anti-viral medicine: This medicine may be prescribed when a doctor diagnoses shingles within 72 hours of the rash first appearing. The earlier anti-viral treatment is started, the better it works. Anti-viral medicines include famciclovir, valacyclovir, and acyclovir. These can lessen the pain and the amount of time the pain lasts.
Nerve blocks: Given for intense pain, these injections (shots) contain a numbing anesthetic and sometimes a corticosteroid.
Corticosteroids: To lower swelling and pain, some patients may get corticosteroid pills with their anti-viral medicine. This treatment is not common because it can make the rash spread.
Treatments for pain after the rash clears: Certain anti-depressants, pain relievers, anesthetic creams and patches, and anti-seizure medicines can help.
Ophthalmic zoster
- All patients with ophthalmic zoster, irrespective of age or severity of symptoms, should be prescribed oral antiviral drugs at the first sign of disease
- Patients with a red eye or visual complaints must be referred to an ophthalmologist on an urgent basis
- Those not needing referral must be reviewed after at most one week
Ramsay-Hunt syndrome
- Oral antiviral therapy must be started immediately and contact the on-call ENT (ear nose and throat) specialist
- Some advocate the use of systemic steroids – refer to local guidelines for management
Home remedies for shingles
- Get plenty of rest and eat well-balanced meals.
- Try simple exercises like stretching or walking. Check with your doctor before starting a new exercise routine.
- Apply a cool washcloth to your blisters to ease the pain and help dry the blisters.
- Cool compresses, baths or ice packs may help with the discomfort. Do not apply ice packs directly to the skin. Wrap the ice pack in a light towel and place it gently over the dressing. Wash the towel in hot water after use.
- Apply calamine lotion to the blisters.
- Cover the rash with loose, non-stick, sterile bandages.
- Wear loose cotton clothes around the body parts that hurt.
- Do things that take your mind off your pain. For example, watch TV, read, talk with friends, listen to relaxing music, or work on a hobby you like.
- Avoid stress. It can make the pain worse.
- Try not to scratch the rash. Scratching may cause scarring and infection of the blisters.
- If the blisters are open, applying creams or gels is not recommended because they might increase the risk of a secondary bacterial infection.
- After a bath or shower, gently pat yourself dry with a clean towel. Do not rub or use the towel to scratch yourself and do not share towels.
- Do not use antibiotic creams or sticking plasters on the blisters since they may slow down the healing process.
- Take an oatmeal bath or use calamine lotion to see if it soothes your skin.
- Avoid contact with people who may be more at risk, such as pregnant women who are not immune to chickenpox, people who have a weak immune system and babies less than 1 month old.
- Do not share towels, play contact sports, or go swimming.
- Share your feelings about your pain with family and friends. Ask for their understanding.
Also, you can limit spreading the virus by:
- Keeping the rash covered
- Not touching or scratching the rash
- Washing your hands often
Shingles prognosis
Most cases of shingles last 3 to 5 weeks. Shingles follows a pattern:
- The first sign is often burning or tingling pain; sometimes, it includes numbness or itching on one side of the body.
- Somewhere between 1 and 5 days after the tingling or burning feeling on the skin, a red rash will appear.
- A few days later, the rash will turn into fluid-filled blisters.
- About a week to 10 days after that, the blisters dry up and crust over.
- A couple of weeks later, the scabs clear up.
Most people get shingles only one time. But, it is possible to have it more than once.
References- Shingles. https://www.cdc.gov/dotw/shingles
- Shingles Vaccination. https://www.cdc.gov/vaccines/vpd/shingles/public/shingrix/index.html
- What You Need to Know About Shingles and the Shingles Vaccine. https://www.cdc.gov/vaccines/hcp/adults/downloads/fs-shingles.pdf
- Shingrix Recommendations. https://www.cdc.gov/vaccines/vpd/shingles/hcp/shingrix/recommendations.html
- Harpaz R, Ortega-Sanchez IR, Seward JF. Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2008;57(RR-5):1-30; quiz CE32-34.





{kind=link}