
What is a heart attack?
A heart attack is sometimes called myocardial infarction or acute coronary syndrome, is a serious medical emergency in which the flow of oxygen-rich blood to a section of your heart muscle suddenly becomes blocked (usually by a blood clot) and your heart can’t get oxygen. If blood flow isn’t restored quickly, the section of your heart muscle begins to die 1. The blockage is most often a buildup of fat, cholesterol and other substances, which form a plaque in the coronary arteries that feed your heart. The blood in your coronary arteries carries oxygen to your heart muscle. Most heart attacks occur when a blockage slows or stops blood flow. Every 40 seconds, someone in the United States has a heart attack 2. It’s important to call your local emergency services number or get emergency medical help if you think you might be having a heart attack. Women are less likely to survive heart attacks than men. No one knows why. It may be that women don’t seek or receive treatment as soon as men. Their symptoms can be different from what men experience. Their symptoms may be subtler and more often overlooked. Or it may be because women’s smaller hearts and blood vessels are more easily damaged. Doctors are working on finding answers to these questions.
Other Names for a Heart Attack
- Myocardial infarction (MI)
- Acute myocardial infarction (AMI)
- Acute coronary syndrome
- Coronary thrombosis
- Coronary occlusion
A heart attack is life threatening. If you’re experiencing any of the symptoms described below, it’s vital you dial your local emergency services number immediately for an ambulance.
Heart attack symptoms can vary but the most common signs and symptoms of heart attack in both men and women of a heart attack are:
- Chest pain or discomfort (also called angina) that suddenly occurs and doesn’t go away. It may feel like pressure, tightness, squeezing or heaviness in your chest. It can feel like indigestion or a burning sensation like heartburn
- Pain that may spread to your left or right arm or may spread to your neck, jaw, back or stomach
- Pain or discomfort in the neck, shoulders, lower jaw, arms, upper back, or abdomen
- Feeling sick, sweaty, light-headed or shortness of breath that lasts more than a few seconds.
Other less common symptoms include:
- A sudden feeling of anxiety that can feel similar to a panic attack
- Excessive coughing or wheezing due to a build up of fluid in the lungs
- Feeling lightheaded, dizzy, or faint.
- Nausea and/or vomiting.
- Unusual sweating.
- Overwhelming fatigue.
- Feeling anxious.
- Heart palpitations (feeling like your heart is beating really fast, or out of rhythm).
- Feeling unusually tired for no reason (sometimes for multiple days).
Not all people who have heart attacks have the same symptoms or have the same severity of symptoms. Pain levels can also vary from person to person. For some people the pain or tightness in their chest is severe, while other people just feel uncomfortable, or pain similar to indigestion. And some people have no symptoms. For others, the first sign may be sudden cardiac arrest. However, the more signs and symptoms you have, the greater the chance you’re having a heart attack.
Heart attack symptoms can persist over days, or they can come on suddenly and unexpectedly. Some heart attacks strike suddenly, but many people have warning signs and symptoms hours, days or weeks in advance. The earliest warning might be recurrent chest pain or pressure (angina) that’s triggered by activity and relieved by rest. Angina is caused by a temporary decrease in blood flow to the heart.
If you think you may be having a heart attack, get treatment right away! Some people wait too long because they don’t recognize the important signs and symptoms. Follow these steps:
- Call for emergency medical help. If you suspect you’re having a heart attack, don’t hesitate. Immediately call your local emergency number. Do not have someone else drive you to the hospital. Do not try to drive yourself. Emergency Medical Technicians (EMTs) can give you life-saving treatment in the ambulance on the way to the hospital.
- If you don’t have access to emergency medical services, have someone drive you to the nearest hospital. Drive yourself only if there are no other options. Because your condition can worsen, driving yourself puts you and others at risk.
- Take nitroglycerin, if prescribed to you by a doctor. Take it as instructed while awaiting emergency help.
- Take aspirin [1 uncoated adult aspirin (325 mg) or 4 uncoated baby aspirins (81 mg each)], if recommended. Taking aspirin during a heart attack could reduce heart damage by helping to keep your blood from clotting. Aspirin can interact with other medications, however, so don’t take an aspirin unless your doctor or emergency medical personnel recommend it. Also don’t take this if you’re allergic to aspirin. But don’t delay calling your local emergency services number to take an aspirin. Call for emergency help first.
- If you are alone and are able, unlock your door to let emergency personnel enter your home.
- Sit in a comfortable chair and wait for help.
- Keep a phone near you.
If you see someone who’s unconscious and you believe is having a heart attack, first call for emergency medical help. Then check if the person is breathing and has a pulse. If the person isn’t breathing or you don’t find a pulse, only then should you begin cardiopulmonary resuscitation (CPR).
Push hard and fast on the person’s chest in a fairly rapid rhythm — about 100 to 120 compressions a minute. If you have been trained in CPR, you can go on to opening the airway and rescue breathing.
If you’re afraid to do cardiopulmonary resuscitation (CPR) or unsure how to perform CPR correctly, know that it’s always better to try than to do nothing at all. The difference between doing something and doing nothing could be someone’s life.
If you haven’t been trained in cardiopulmonary resuscitation (CPR), doctors recommend.
Here’s advice from the American Heart Association:
- Untrained. If you’re not trained in CPR or worried about giving rescue breaths, then provide hands-only CPR (performing only chest compressions). That means uninterrupted chest compressions of 100 to 120 a minute until paramedics arrive. You don’t need to try rescue breathing.
- Trained and ready to go. If you’re well-trained and confident in your ability, check to see if there is a pulse and breathing. If there is no pulse or breathing within 10 seconds, begin chest compressions. Start CPR with 30 chest compressions before giving two rescue breaths.
- Trained but rusty. If you’ve previously received CPR training but you’re not confident in your abilities, then just do chest compressions at a rate of 100 to 120 a minute.
The above advice applies to situations in which adults, children and infants need CPR, but not newborns (infants up to 4 weeks old).
CPR can keep oxygen-rich blood flowing to the brain and other organs until emergency medical treatment can restore a normal heart rhythm. When the heart stops, your body no longer gets oxygen-rich blood. The lack of oxygen-rich blood can cause brain damage in only a few minutes.
If you are untrained and have immediate access to a phone, call your local emergency number before beginning CPR. The dispatcher can instruct you in the proper procedures until help arrives. To learn CPR properly, take an accredited first-aid training course, including CPR and how to use an automated external defibrillator (AED).
Chest Discomfort
- Most heart attacks involve discomfort in the center of the chest that lasts more than a few minutes, or that goes away and comes back. It can feel like uncomfortable pressure, squeezing, fullness or pain.
Discomfort in Other Areas of the Upper Body
- Symptoms can include pain or discomfort in one or both arms, the back, neck, jaw or stomach.
Shortness of Breath with or without chest discomfort.
Other signs may include breaking out in a cold sweat, nausea or lightheadedness.
- Don’t Wait–Get Help Quickly
- Quick Action Can Save Your Life
- If you think you or someone else is having a heart attack, even if you’re not sure, don’t feel embarrassed to call your local emergency number right away !
- Do not drive to the hospital or let someone else drive you. Call an ambulance so that medical personnel can begin life-saving treatment on the way to the emergency room. Take a nitroglycerin pill if your doctor has prescribed this type of treatment.
Heart attack treatment works best when it’s given right after symptoms occur.
- Don’t Wait–Get Help Quickly
- Quick Action Can Save Your Life
- If you think you or someone else is having a heart attack, even if you’re not sure, don’t feel embarrassed to call your local emergency number right away !
- Do not drive to the hospital or let someone else drive you. Call an ambulance so that medical personnel can begin life-saving treatment on the way to the emergency room. Take a nitroglycerin pill if your doctor has prescribed this type of treatment.
Every year, about 790,000 Americans have a heart attack. Of these cases:
- 580,000 are a first heart attack.
- 210,000 happen to people who have already had a first heart attack 2.
- About 15% of people who have a heart attack will die from it 2.
- Almost half of sudden cardiac deaths happen outside a hospital 3.
- One of 5 heart attacks is silent—the damage is done, but the person is not aware of it 2.
Heart attacks most often occur as a result of coronary heart disease (CHD), also called coronary artery disease. Coronary heart disease is a condition in which a waxy substance called plaque (cholesterol plaque) builds up inside the coronary arteries. These arteries supply oxygen-rich blood to your heart.
When plaque builds up in the arteries, the condition is called atherosclerosis. The buildup of plaque occurs over many years.
Eventually, an area of plaque can rupture (break open) inside of an artery. This causes a blood clot to form on the plaque’s surface. If the clot becomes large enough, it can mostly or completely block blood flow through a coronary artery.
If the blockage isn’t treated quickly, the portion of heart muscle fed by the artery begins to die. Healthy heart tissue is replaced with scar tissue. This heart damage may not be obvious, or it may cause severe or long-lasting problems.
A less common cause of heart attack is a severe spasm (tightening) of a coronary artery. The spasm cuts off blood flow through the artery. Spasms can occur in coronary arteries that aren’t affected by atherosclerosis.
Heart attacks can be associated with or lead to severe health problems, such as heart failure and life-threatening arrhythmias.
Heart failure is a condition in which the heart can’t pump enough blood to meet the body’s needs. Arrhythmias are irregular heartbeats. Ventricular fibrillation is a life-threatening arrhythmia that can cause death if not treated right away.
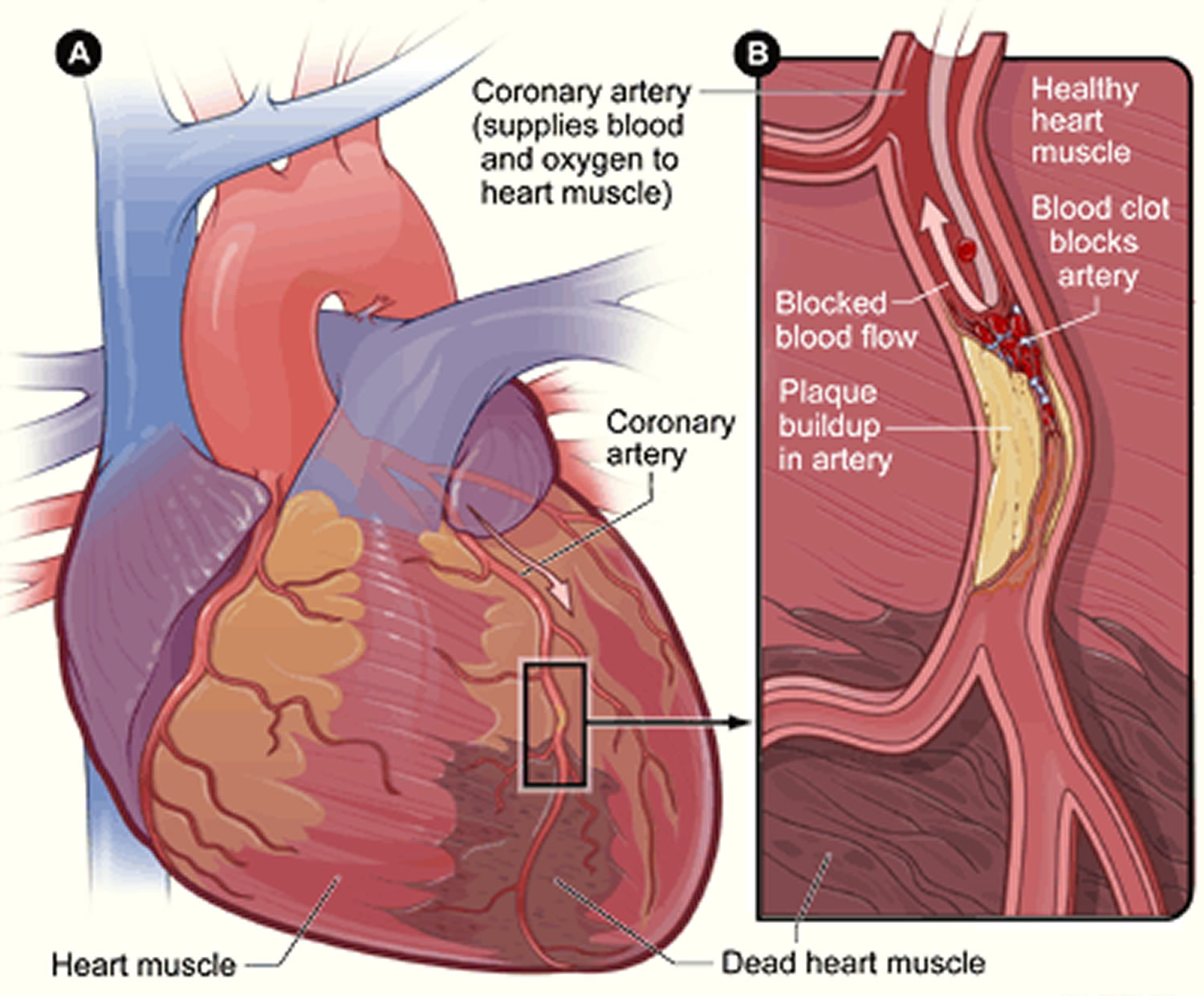
Figure 1. Heart With Muscle Damage and a Blocked Coronary Artery
What’s the difference between a cardiac arrest and a heart attack?
The phrases cardiac arrest and heart attack are often confused, however are different.
- If you’re having a cardiac arrest you will be unconscious, not breathing or not breathing normally. Your heart has stopped pumping blood around your body and you’ll need CPR and medical attention immediately.
- During a heart attack you’ll be conscious and breathing, but experiencing chest pain or discomfort.
A heart attack is a medical emergency and can lead to cardiac arrest so it’s important to seek medical attention straight away.
What’s the difference between angina and a heart attack?
Angina is pain felt in your chest often caused by coronary heart disease. As the symptoms of angina are similar to a heart attack, it’s important to know how to distinguish between the two.
If you haven’t been diagnosed with angina and you start experiencing chest pain that feels similar to the symptoms of a heart attack, phone your local emergency services number immediately.
If you have angina and you start experiencing chest pain symptoms similar to a heart attack:
- sit down and rest
- use your glyceryl trinitrate (nitroglycerin) spray that you’ve been prescribed
- if the pain still persists after a few minutes, take another dose of your spray
- if the pain doesn’t go away a few minutes after your second dose, dial your local emergency services number immediately.
What’s the difference between indigestion and a heart attack?
Indigestion or heartburn, is a feeling that usually comes on after eating. It causes a burning and uncomfortable sensation in your chest and abdomen, and often a sour taste in your mouth.
If you haven’t experienced heartburn or indigestion before and you’re experiencing persistent burning chest pain or chest pain combined with other heart attack symptoms, phone your local emergency services number immediately.
If you’re prone to heartburn or indigestion and you’re experiencing the same symptoms as usual, take the steps you usually would to ease your discomfort, such as taking some medicine and/or drinking water.
If the burning feeling in your chests persists, or it begins to spread to your arms, neck or jaw, phone your local emergency services number immediately as you may be having a heart attack.
How to perform a Cardiopulmonary Resuscitation (CPR)
If the person’s breathing or heart stops, cardiopulmonary resuscitation (CPR) should be performed immediately.
Hands-only CPR
- Ensure the area is safe
- Check for hazards, such as electrical equipment or traffic.
To carry out a chest compression:
- Place the heel of your hand on the breastbone at the center of the person’s chest. Place your other hand on top of your first hand and interlock your fingers.
- Position yourself with your shoulders above your hands.
- Using your body weight (not just your arms), press straight down by 5-6cm (2-2.5 inches) on their chest.
- Keeping your hands on their chest, release the compression and allow the chest to return to its original position.
- Repeat these compressions at a rate of 100 to 120 times per minute until an ambulance arrives or you become exhausted.
When you call for an ambulance, telephone systems now exist that can give basic life-saving instructions, including advice about CPR. These are now common and are easily accessible with mobile phones.
Cardiopulmonary Resuscitation (CPR) with rescue breaths
If you’ve been trained in CPR, including rescue breaths, and feel confident using your skills, you should give chest compressions with rescue breaths. If you’re not completely confident, attempt hands-only CPR instead (see above).
Adults
- Place the heel of your hand on the center of the person’s chest, then place the other hand on top and press down by 5-6cm (2-2.5 inches) at a steady rate of 100 to 120 compressions per minute.
- After every 30 chest compressions, give two rescue breaths.
- Tilt the casualty’s head gently and lift the chin up with two fingers. Pinch the person’s nose. Seal your mouth over their mouth and blow steadily and firmly into their mouth for about one second. Check that their chest rises. Give two rescue breaths.
- Continue with cycles of 30 chest compressions and two rescue breaths until they begin to recover or emergency help arrives.
Children over one year old
- Open the child’s airway by placing one hand on the child’s forehead and gently tilting their head back and lifting the chin. Remove any visible obstructions from the mouth and nose.
- Pinch their nose. Seal your mouth over their mouth and blow steadily and firmly into their mouth, checking that their chest rises. Give five initial rescue breaths.
- Place the heel of one hand on the center of their chest and push down by 5cm (about two inches), which is approximately one-third of the chest diameter.
- The quality (depth) of chest compressions is very important. Use two hands if you can’t achieve a depth of 5cm using one hand.
- After every 30 chest compressions at a rate of 100 to 120 per minute, give two breaths.
- Continue with cycles of 30 chest compressions and two rescue breaths until they begin to recover or emergency help arrives.
Infants under one year old
- Open the infant’s airway by placing one hand on their forehead and gently tilting the head back and lifting the chin. Remove any visible obstructions from the mouth and nose.
- Place your mouth over the mouth and nose of the infant and blow steadily and firmly into their mouth, checking that their chest rises. Give five initial rescue breaths.
- Place two fingers in the middle of the chest and push down by 4cm (about 1.5 inches), which is approximately one-third of the chest diameter. The quality (depth) of chest compressions is very important. Use the heel of one hand if you can’t achieve a depth of 4cm using the tips of two fingers.
- After 30 chest compressions at a rate of 100 to 120 per minute, give two rescue breaths.
- Continue with cycles of 30 chest compressions and two rescue breaths until they begin to recover or emergency help arrives.
Causes of heart attack
A heart attack occurs when one or more of your coronary arteries becomes blocked (see Figure 1). Over time, a buildup of fatty deposits, including cholesterol, form substances called plaques, which can narrow the coronary arteries (atherosclerosis). It takes years for the plaque to build up. This condition, called coronary artery disease, causes most heart attacks. When a blockage occurs in your coronary arteries, blood and oxygen don’t get to the heart. This can lead to a heart attack if it isn’t treated quickly.
During a heart attack, a plaque can rupture and spill cholesterol and other substances into the bloodstream. A blood clot forms at the site of the rupture. If the clot is large, it can block blood flow through the coronary artery, starving the heart of oxygen and nutrients (ischemia). A heart attack occurs when part of the heart muscle is damaged or dies from lack of oxygen.
You might have a complete or partial blockage of the coronary artery.
- A complete blockage of the coronary artery means you’ve had an ST elevation myocardial infarction (STEMI).
- A partial blockage of the coronary artery means you’ve had a non-ST elevation myocardial infarction (NSTEMI).
Diagnosis and treatment might be different depending on which type you’ve had.
Another cause of a heart attack is a spasm of a coronary artery that shuts down blood flow to part of the heart muscle. Using tobacco and illicit drugs, such as cocaine, can cause a life-threatening spasm.
Coronary Heart Disease
A heart attack happens if the flow of oxygen-rich blood to a section of heart muscle suddenly becomes blocked and the heart can’t get oxygen. Most heart attacks occur as a result of coronary heart disease (CHD) 4.
Coronary heart disease is a condition in which a waxy substance called plaque builds up inside of the coronary arteries. These arteries supply oxygen-rich blood to your heart.
When plaque builds up in the arteries, the condition is called atherosclerosis. The buildup of plaque occurs over many years.
Eventually, an area of plaque can rupture (break open) inside of an artery. This causes a blood clot to form on the plaque’s surface. If the clot becomes large enough, it can mostly or completely block blood flow through a coronary artery.
If the blockage isn’t treated quickly, the portion of heart muscle fed by the artery begins to die. Healthy heart tissue is replaced with scar tissue. This heart damage may not be obvious, or it may cause severe or long-lasting problems.
Coronary Artery Spasm
A less common cause of heart attack is a severe spasm (tightening) of a coronary artery 4. The spasm cuts off blood flow through the artery. Spasms can occur in coronary arteries that aren’t affected by atherosclerosis.
What causes a coronary artery to spasm isn’t always clear. A spasm may be related to:
- Taking certain drugs, such as cocaine
- Emotional stress or pain
- Exposure to extreme cold
- Cigarette smoking.
Who is at Risk for a Heart Attack?
Certain risk factors make it more likely that you’ll develop coronary heart disease and have a heart attack 5. You can control many of these risk factors.
Risk Factors You Can Control
The major risk factors for a heart attack that you can control include:
- High blood cholesterol (hypercholesterolemia). High levels of cholesterol in your blood can increase the risk of plaque formation and atherosclerosis.
- High blood pressure (hypertension). Uncontrolled high blood pressure can result in hardening and thickening of your arteries, narrowing the vessels through which blood flows. Blood pressure is considered high if it stays at or above 140/90 mmHg over time. If you have diabetes or chronic kidney disease, high blood pressure is defined as 130/80 mmHg or higher. (The mmHg is millimeters of mercury—the units used to measure blood pressure.)
- Diabetes. Diabetes increases your risk of heart disease. Both conditions share similar risk factors, such as obesity and high blood pressure.
- Insulin resistance. This condition occurs if the body can’t use its own insulin properly. Insulin is a hormone that helps move blood sugar into cells where it’s used for energy. Insulin resistance may lead to diabetes.
- Obesity or being overweight. Excess weight typically worsens other heart disease risk factors.
- Metabolic syndrome. Metabolic syndrome occurs when you have obesity, high blood pressure and high blood sugar. Having metabolic syndrome makes you twice as likely to develop heart disease than if you don’t have it.
- Smoking. Nicotine tightens your blood vessels, and carbon monoxide can damage their inner lining, making them more susceptible to atherosclerosis. Heart attacks are more common in smokers than in nonsmokers.
- Poor diet. A diet that’s high in fat, salt, sugar and cholesterol can contribute to the development of heart disease. A healthy diet can help reduce your risk of developing coronary heart disease and stop you gaining weight, reducing your risk of diabetes and high blood pressure.
- Physical inactivity. Lack of exercise also is associated with many forms of heart disease and some of its other risk factors as well.
- Air pollution. Air pollution is harmful to your heart and circulation. Research shows that air pollution can affect your heart and circulation by:
- damaging the inside walls of your blood vessels, causing them to become narrower and harder
- restricting the movement of your blood vessels, which can increase your blood pressure and add to the strain on your heart
- making your blood more likely to clot
- affecting the normal electrical functioning of your heart which could cause abnormal heart rhythms
- causing small changes to the structure of your heart like those that are seen in the early stages of heart failure.
- This damage can contribute to the development of new health problems, or put people with existing heart and circulatory conditions at increased risk of events like a heart attack or stroke.
- Poor dental health. It’s important to brush and floss your teeth and gums often, and have regular dental checkups. If your teeth and gums aren’t healthy, germs can enter your bloodstream and travel to your heart, causing endocarditis.
- Stress. Unrelieved stress may damage your arteries and worsen other risk factors for heart disease. Research suggests that an emotionally upsetting event, particularly one involving anger, can serve as a trigger for a heart attack or angina in some people. Stress can contribute to high blood pressure and other heart disease risk factors. Some of the ways people cope with stress—drinking alcohol, using other substances, smoking, or overeating—are not healthy ways to manage stress.
- Drug abuse. Using stimulant drugs, such as cocaine or amphetamines, can trigger a spasm of your coronary arteries that can cause a heart attack.
- Excessive use of alcohol or caffeine. Heavy drinking can damage the heart muscle and worsen other coronary heart disease risk factors. Men should have no more than two drinks containing alcohol a day. Women should have no more than one drink containing alcohol a day. If you do not drink, you should not start. You should not drink if you are pregnant, are under the age of 21, taking certain medicines, or if you have certain medical conditions, including heart failure.
- Alcohol can:
- Add calories to your daily diet and possibly cause you to gain weight.
- Raise your blood pressure and levels of triglyceride fats in your blood.
- Contribute to or worsen heart failure in some people, such as some people who have cardiomyopathy.
- Raise your risk of other diseases such as cancer.
- Alcohol can:
- Sleep apnea. Sleep apnea is a common disorder in which you have one or more pauses in breathing or shallow breaths while you sleep. Untreated sleep apnea can increase your risk for high blood pressure, diabetes, and even a heart attack or stroke.
- An autoimmune condition. Having a condition such as rheumatoid arthritis or lupus can increase your risk of a heart attack.
- Mental health problems. Some common mental health conditions include:
- Depression, which is a long-lasting low mood disorder
- Anxiety disorders such as social anxiety disorder, phobias and post-traumatic stress disorder (PTSD)
- Personality disorders such as paranoia, borderline personality disorder and obsessive-compulsive disorder (OCD)
- Bipolar disorder (BPD), previously called manic depression, which causes extreme and unpredictable mood changes
- Psychosis and schizophrenia, which is when a person experiences an altered state of reality
Some of these risk factors—such as obesity, high blood pressure, and high blood sugar—tend to occur together. When they do, it’s called metabolic syndrome.
In general, a person who has metabolic syndrome is twice as likely to develop heart disease and five times as likely to develop diabetes as someone who doesn’t have metabolic syndrome.
For more information about the risk factors that are part of metabolic syndrome, go to the The Metabolic Syndrome article.
Risk Factors You Can’t Control
Risk factors that you can’t control include:
- Age. Growing older increases your risk of damaged and narrowed arteries and a weakened or thickened heart muscle. Genetic or lifestyle factors cause plaque to build up in your arteries as you age. In men, the risk for coronary heart disease increases starting at age 45. In women, the risk for coronary heart disease increases starting at age 55. About 83% of people who die from heart disease are 65 or older.
- Sex. Men are generally at greater risk of heart disease. The risk for women increases after menopause.
- Ethnicity. African Americans, Mexican Americans, Native Americans, and native Hawaiians are at greater risk.
- Family history. A family history of heart disease increases your risk of coronary artery disease, especially if a parent developed it at an early age (before age 55 for a male relative, such as your brother or father, and 65 for a female relative, such as your mother or sister).
- Preeclampsia. Preeclampsia (high blood pressure during pregnancy) can occur during pregnancy. The two main signs of preeclampsia are a rise in blood pressure and excess protein in the urine. Preeclampsia is linked to an increased lifetime risk of heart disease, including coronary heart disease, heart attack, heart failure, and high blood pressure. Preeclampsia (high blood pressure during pregnancy) is a risk factor that you can’t control. However, if you’ve had the condition, you should take extra care to monitor your blood pressure and try to lower other heart disease risk factors.
How to prevent getting a heart attack
When heart experts talk about prevention, they usually refer to one of three types: secondary, primary and primordial prevention 6. All three have similar elements, but different starting times and different effects.
You can help reduce your risk of heart disease by taking steps to control factors that put you at greater risk:
- Control your blood pressure. Ask your doctor for a blood pressure measurement at least every two years. He or she may recommend more frequent measurements if your blood pressure is higher than normal or you have a history of heart disease. Optimal blood pressure is less than 120 systolic and 80 diastolic, as measured in millimeters of mercury (mm Hg).
- Lower your cholesterol. Ask your doctor for a baseline cholesterol test when you’re in your 20s and then at least every five years. You may need to start testing earlier if high cholesterol is in your family. If your test results aren’t within desirable ranges, your doctor may recommend more-frequent measurements. Most people should aim for a low-density lipoprotein (LDL or “bad” cholesterol) level below 130 milligrams per deciliter (mg/dL), or 3.4 millimoles per liter (mmol/L). If you have other risk factors for heart disease, you should aim for an LDL level below 100 mg/dL (2.6 mmol/L). If you’re at very high risk of heart disease — if you’ve already had a heart attack or have diabetes, for example — aim for an LDL level below 70 mg/dL (1.8 mmol/L).
- Keep diabetes under control. If you have diabetes, tight blood sugar control can help reduce the risk of heart disease.
- Don’t smoke. Smoking is a major risk factor for heart disease, especially atherosclerosis. One of the best things you can do for your heart is to stop smoking or using smokeless tobacco. Quitting is the best way to reduce your risk of heart disease and its complications. Even if you’re not a smoker, be sure to avoid secondhand smoke. Chemicals in tobacco can damage your heart and blood vessels. Cigarette smoke reduces the oxygen in your blood, which increases your blood pressure and heart rate because your heart has to work harder to supply enough oxygen to your body and brain. There’s good news though. Your risk of heart disease starts to drop in as little as a day after quitting. After a year without cigarettes, your risk of heart disease drops to about half that of a smoker. No matter how long or how much you smoked, you’ll start reaping rewards as soon as you quit.
- Don’t drink or limit your alcohol intake. Alcohol can cause abnormal heart rhythms, high blood pressure, damage to your heart muscle and other diseases such as stroke, liver problems and some cancers. Alcohol is also high in calories so it can lead to weight gain. It also lowers your inhibitions which might mean you find it harder to stick to your healthy eating plans when you have been drinking. If you are trying to lose weight, cut down on alcohol. Drinking more than the recommended amount of alcohol can have a harmful effect on your heart and general health.
- Get enough exercise. Regular, daily physical activity can lower your risk of heart disease. Physical activity helps you achieve and maintain a healthy weight and control diabetes, high cholesterol and high blood pressure — all risk factors for heart disease. If you have a heart arrhythmia or heart defect, there may be some restrictions on the activities you can do, so talk to your doctor. Exercise at least 30 to 60 minutes most days of the week. If you haven’t been active for a while, you may need to slowly work your way up to these goals, but in general, you should aim for at least:
- 150 minutes a week of moderate aerobic exercise, such as walking at a brisk pace
- 75 minutes a week of vigorous aerobic activity, such as running
- Two or more strength training sessions a week
- Even shorter bouts of activity offer heart benefits, so if you can’t meet those guidelines, don’t give up. Just five minutes of moving can help, and activities such as gardening, housekeeping, taking the stairs and walking the dog all count toward your total. You don’t have to exercise strenuously to achieve benefits, but you can see bigger benefits by increasing the intensity, duration and frequency of your workouts.
- Get enough good-quality sleep. Quality sleep is good for your heart. It can be a challenge to make time for good sleep, but it’s important. For two weeks try to get 8 hours of good, quality sleep each night. Yes, each person’s sleep needs vary slightly, but eight is a good number to shoot for.
- Eat healthy foods. A heart-healthy diet based on fruits, vegetables and whole grains — and low in saturated fat, salt (sodium), cholesterol and added sugar — can help you control your weight, blood pressure and cholesterol.
- Maintain a healthy weight. Being overweight increases your risk of heart disease. A body mass index (BMI) of less than 25 and a waist circumference of 35 inches (88.9 centimeters) or less is the goal for preventing and treating heart disease.
- Reduce and manage stress. Reduce stress as much as possible. Practice techniques for managing stress, such as muscle relaxation and deep breathing.
- Get treatment for depression. Being depressed can increase your risk of heart disease significantly. Talk to your doctor if you feel hopeless or uninterested in your life.
- Practice good hygiene. Regularly wash your hands and brush and floss your teeth to keep yourself well.
- Get regular medical checkups. Early detection and treatment can set the stage for a lifetime of better heart health.
Primordial prevention
The word “primordial” means existing from the beginning. Primordial prevention involves working to prevent inflammation, atherosclerosis, and endothelial dysfunction from taking hold, and thus prevent risk factors such as high blood pressure, high cholesterol, excess weight, and ultimately cardiovascular events. Once rarely discussed, primordial prevention is now the cornerstone of the American Heart Association’s definition of ideal heart health and efforts to help people achieve it 6. As its name implies, the sooner you can start practicing primordial prevention—ideally from childhood on—the more likely you are to achieve it and protect yourself from heart disease.
Primary prevention
Primary prevention aims to keep an individual at risk of heart disease from having a first heart attack or stroke, needing angioplasty or surgery, or developing some other form of heart disease 6. Primary prevention is usually aimed at people who already have developed cardiovascular risk factors, such as high blood pressure or high cholesterol. As with secondary prevention, primary prevention focuses on controlling these risk factors by making healthy lifestyle changes and, if needed, taking medications. That said, the appearance of worrisome cardiovascular risk factors means that inflammation, atherosclerosis, and/or endothelial dysfunction are already at work and, in most cases, aren’t reversible.
Secondary prevention
These efforts are started after someone has a heart attack or stroke, undergoes angioplasty or bypass surgery, or develops some other form of heart disease 6. It involves taking medications like aspirin and/or a cholesterol-lowering statin, quitting smoking and losing weight if needed, exercising more, and following a healthy diet. Although secondary prevention may sound like “closing the barn door after the horse has gone,” it isn’t. These steps can prevent a second heart attack or stroke, halt the progression of heart disease, and prevent early death. It may be obvious, but the number one killer of individuals who survive a first heart attack is a second heart attack.
Steps for the prevention of heart disease (before you have a heart attack)
Four key choices can dramatically reduce your chances of developing cardiovascular risk factors and ultimately heart disease. All four are important. Below, each choice is listed in order of significance to heart health, along with ways to put each into practice.
1. Not smoking
One of the best things you can do for your health is to not use tobacco in any form. Tobacco use is a hard-to-break habit that can slow you down, make you sick, and shorten your life. One way it does this is by contributing to heart disease.
In fact, researchers examining the relationship between cigarette smoking and smoking cessation on mortality during a decades-long perspective study of over 100,000 women found that approximately 64% of deaths among current smokers and 28% of deaths among former smokers were attributable to cigarette smoking 7.
This study 7 also reported that much of the excess risk due to smoking may be drastically lowered after quitting. Additionally, the excess risk for all-cause mortality—that is, death from any cause—decreases to the level of a “never-smoker” 20 years after quitting.
The nicotine that tobacco products deliver is one of the most addictive substances around. That makes tobacco use one of the toughest unhealthy habits to break. But don’t get discouraged; many smokers do quit! In fact, in the United States today there are more ex-smokers than smokers 8. Learn more about the hazards of smoking, the benefits of quitting, and tips for quitting from the Centers for Disease Control and Prevention 9.
2. Maintaining a healthy weight
Excess weight and an extra-large waist size both contribute to heart disease, as well as a host of other health problems 10, 11, 12.
In a study of over one million women, body-mass index (BMI) was a strong risk factor for coronary heart disease. The incidence of coronary heart disease increases progressively with BMI 13.
In the Nurses’ Health Study and the Health Professionals Follow-Up Study, middle-aged women and men who gained 11 to 22 pounds after age 20 were up to three times more likely to develop heart disease, high blood pressure, type 2 diabetes, and gallstones than those who gained five pounds or fewer.
Those who gained more than 22 pounds had an even greater risk of developing these diseases 10, 14, 15.
Weight and height go hand-in-hand. The taller you are, the more you weigh. That’s why researchers have devised several measures that account for both weight and height. The one most commonly used is BMI.
You can calculate your BMI by dividing your weight in kilograms by your height in meters squared (kg/m2). You can also use an online BMI calculator or BMI table.
To find out about your body mass index (BMI), you can use a FREE online BMI calculators from the Centers for Disease Control and Prevention (CDC) :
- Adults (https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html)
For children and adolescents (younger than 20 years of age), overweight and obesity are based on the Centers for Disease Control and Prevention’s (CDC’s) BMI-for-age growth charts, which are available at 16.
The CDC has a BMI percentile calculator for children and teens at 17.
Body Mass Index for Men and Women Adults
The body mass index is an attempt to quantify the amount of tissue mass (muscle, fat, and bone) in an individual, and then categorize that person as underweight, normal weight, overweight, or obese based on that value. Commonly accepted body mass index ranges are:
- A) Underweight: under 18.5 kg/m2,
- B) Normal (Healthy BMI) weight: 18.5 to 25 kg/m2,
- C) Overweight: 25 to 30 kg/m2,
- D) Obese: over 30 to 39.9 kg/m2.
- E) Severely Obese: over 40 kg/m2.
Waist size matters, too. In people who are not overweight, waist size may be an even more telling warning sign of increased health risks than BMI 18. An expert panel convened by the National Institutes of Health identified these useful benchmarks: Men should aim for a waist size below 40 inches (102 cm) and women should aim for a waist size below 35 inches (88 cm) 19.
3. Exercising
Exercise and physical activity are excellent ways to prevent heart disease and many other diseases and conditions 20, 21, 22, but many of us get less activity as we get older.
Getting regular physical activity is one of the best things you can do for your health. It lowers the risk of heart disease, diabetes, stroke, high blood pressure, osteoporosis, and certain cancers, and it can also help control stress, improve sleep, boost mood, keep weight in check, and reduce the risk of falling and improve cognitive function in older adults.
It doesn’t take marathon training to see real health gains. A 30-minute brisk walk five days of the week will provide important benefits for most people. Getting any amount of exercise is better than none.
Exercise and physical activity benefit the body, while a sedentary lifestyle does the opposite—increasing the chances of becoming overweight and developing a number of chronic diseases.
Research shows that people who spend more time each day watching television, sitting, or riding in cars have a greater chance of dying early than people who are more active 23, 24, 25. A 2013 study showed that, among women ages 50-79 with no cardiovascular disease at the start of study, prolonged sitting time was associated with increased heart disease risk regardless of the amount of time spent in leisure-time physical activity 22.
4. Following a healthy diet
For years, research into connections between diet and heart disease focused on individual nutrients like cholesterol (and foods high in dietary cholesterol, like eggs), types of fats, and specific vitamins and minerals. This work has been revealing, but it has also generated some dead ends, along with myths and confusion about what constitutes a heart-healthy diet. That’s because people eat food, not nutrients.
- The best diet for preventing heart disease is one that is full of fruits and vegetables, whole grains, nuts, fish, poultry, and vegetable oils; includes alcohol in moderation, if at all; and goes easy on red and processed meats, refined carbohydrates, foods and beverages with added sugar, sodium, and foods with trans fat.
- People with diets consistent with this dietary pattern had a 31% lower risk of heart disease, a 33% lower risk of diabetes, and a 20% lower risk of stroke 26.
- A randomized controlled trial found that a Mediterranean diet supplemented with extra-virgin olive oil or nuts, both rich sources of unsaturated fat, reduced the incidence of major cardiovascular events amongst patients with cardiovascular disease over a 4.8-year follow-up period. This study highlighted that low-fat diets are not beneficial to heart health, and that incorporating healthy fats – such as those included in the
- Mediterranean diet – can improve heart health and weight loss.
There isn’t one exact Mediterranean diet, as this eating style takes into account the different foods, eating patterns, and lifestyles in multiple countries that border the Mediterranean Sea. However, there are similarities that define a Mediterranean eating pattern, and as described by this study the traditional
Mediterranean diet includes:
- High intake of olive oil, nuts, vegetables, fruits, and cereals
- Moderate intake of fish and poultry
- Low intake of dairy products, red meat, processed meats, and sweets
- Wine in moderation, consumed with meals 27.
Prevention of Heart Attack Summary
You can help prevent heart disease by doing four key things and making them into habits:
- Don’t smoke (or quit if you do)
- Maintain a healthy weight
- Exercise; be active
- Follow a healthy diet
Table 1. Lifestyle factors for heart attack prevention
| Goal/Metric | Ideal Cardiovascular Health Definition |
| Current smoking | |
| Adults >20 years of age | Never or quit >12 months ago |
| Children 12–19 years of age | Never tried; never smoked whole cigarette |
| Body mass index | |
| Adults >20 years of age | <25 kg/m² |
| Children 2–19 years of age | <85th Percentile |
| Physical activity | |
| Adults >20 years of age | ≥150 minutes/week moderate intensity or ≥75 minutes/week vigorous intensity or combination |
| Children 12–19 years of age | ≥60 minutes of moderate- or vigorous-intensity activity every day |
| Healthy diet score* | |
| Adults >20 years of age | 4–5 Components* |
| Children 5–19 years of age | 4–5 Components* |
| Total cholesterol | |
| Adults >20 years of age | <200 mg/dL† |
| Children 6–19 years of age | <170 mg/dL† |
| Blood pressure | |
| Adults >20 years of age | <120/<80 mm Hg† |
| Children 8–19 years of age | <90th Percentile† |
| Fasting plasma glucose | |
| Adults >20 years of age | <100 mg/dL† |
| Children 12–19 years of age | <100 mg/dL† |
Footnotes: *The committee selected 5 aspects of diet to define a healthy dietary score. The score is not intended to be comprehensive. Rather, it is a practical approach that provides individuals with a set of potential concrete actions. A comprehensive rationale is set forth in the text of this document, and a comprehensive set of nutrition recommendations is provided in the 2006 Nutrition Guidelines 28, 29, 30.
†Untreated values.
[Source 6 ]Strong studies make it possible to link reductions in risk to these habits. Following a healthy lifestyle may prevent over 80% of cases of coronary artery disease 31, 32, 50% of ischemic strokes 33, 80% of sudden cardiac deaths 34 and 72% of premature deaths related to heart disease 35. In other words, a healthy lifestyle is a good investment in a longer, healthier life.
Steps for the primary and secondary prevention of a heart attack
Lowering your risk factors for coronary heart disease can help you prevent a heart attack. Even if you already have coronary heart disease, you still can take steps to lower your risk for a heart attack. These steps involve making heart-healthy lifestyle changes and getting ongoing medical care for related conditions that make heart attack more likely. Talk to your doctor about whether you may benefit from aspirin primary prevention, or using aspirin to help prevent your first heart attack.
Heart-Healthy Lifestyle Changes
A heart-healthy lifestyle can help prevent a heart attack and includes heart-healthy eating, being physically active, quitting smoking, managing stress, and managing your weight.
Ongoing Care – Treat Related Conditions
Treating conditions that make a heart attack more likely also can help lower your risk for a heart attack. These conditions may include:
- Diabetes (high blood sugar). If you have diabetes, try to control your blood sugar level through diet and physical activity (as your doctor recommends). If needed, take medicine as prescribed.
- High blood cholesterol. Your doctor may prescribe a statin medicine to lower your cholesterol if diet and exercise aren’t enough.
- High blood pressure. Your doctor may prescribe medicine to keep your blood pressure under control.
- Chronic kidney disease. Your doctor may prescribe medicines to control your high blood pressure or high blood sugar levels.
- Peripheral artery disease. Your doctor may recommend surgery or procedures to unblock the affected arteries.
Have an Emergency Action Plan
Make sure that you have an emergency action plan in case you or someone in your family has a heart attack. This is very important if you’re at high risk for, or have already had, a heart attack.
Write down a list of medicines you are taking, medicines you are allergic to, your health care provider’s phone numbers (both during and after office hours), and contact information for a friend or relative. Keep the list in a handy place (for example, fill out this wallet card) to share in a medical emergency.
Talk with your doctor about the signs and symptoms of a heart attack, when you should call your local emergency number, and steps you can take while waiting for medical help to arrive.
Symptoms of a heart attack
Remember acting fast at the first sign of heart attack symptoms can save your life and limit damage to your heart 1. Treatment works best when it’s given right after symptoms occur.
Not all heart attacks begin with the sudden, crushing chest pain that often is shown on TV or in the movies. In one study, for example, one-third of the patients who had heart attacks had no chest pain 36. These patients were more likely to be older, female, or diabetic.
The symptoms of a heart attack can vary from person to person. Some people can have few symptoms and are surprised to learn they’ve had a heart attack. If you’ve already had a heart attack, your symptoms may not be the same for another one. It is important for you to know the most common symptoms of a heart attack and also remember these facts:
- Heart attacks can start slowly and cause only mild pain or discomfort. Symptoms can be mild or more intense and sudden. Symptoms also may come and go over several hours.
- People who have high blood sugar (diabetes) may have no symptoms or very mild ones.
- The most common symptom, in both men and women, is chest pain or discomfort.
- Women are somewhat more likely to have shortness of breath, nausea and vomiting, unusual tiredness (sometimes for days), and pain in the back, shoulders, and jaw.
Some people don’t have symptoms at all. Heart attacks that occur without any symptoms or with very mild symptoms are called silent heart attacks.
Many people aren’t sure what’s wrong when they are having symptoms of a heart attack.
Most Common Symptoms of a heart attack
The most common warning symptoms of a heart attack for both men and women are:
- Chest pain or discomfort. Most heart attacks involve discomfort in the center or left side of the chest. The discomfort usually lasts for more than a few minutes or goes away and comes back. It can feel like pressure, squeezing, fullness, or pain. It also can feel like heartburn or indigestion. The feeling can be mild or severe.
- Upper body discomfort. You may feel pain or discomfort in one or both arms, the back, shoulders, neck, jaw, or upper part of the stomach (above the belly button).
- Shortness of breath. This may be your only symptom, or it may occur before or along with chest pain or discomfort. It can occur when you are resting or doing a little bit of physical activity.
Not everyone having a heart attack has typical symptoms. If you’ve already had a heart attack, your symptoms may not be the same for another one. However, some people may have a pattern of symptoms that recur.
The more signs and symptoms you have, the more likely it is that you’re having a heart attack.
Other Common Signs and Symptoms include:
- Breaking out in a cold sweat
- Feeling unusually tired for no reason, sometimes for days (especially if you are a woman)
- Nausea (feeling sick to the stomach) and vomiting
- Light-headedness or sudden dizziness
- Any sudden, new symptom or a change in the pattern of symptoms you already have (for example, if your symptoms become stronger or last longer than usual)
The symptoms of angina can be similar to the symptoms of a heart attack. Angina is chest pain that occurs in people who have coronary heart disease, usually when they’re active. Angina pain usually lasts for only a few minutes and goes away with rest.
Chest pain or discomfort that doesn’t go away or changes from its usual pattern (for example, occurs more often or while you’re resting) can be a sign of a heart attack.
- All chest pain should be checked by a doctor.
The signs and symptoms of a heart attack can develop suddenly. However, they also can develop slowly—sometimes within hours, days, or weeks of a heart attack.
Any time you think you might be having heart attack symptoms or a heart attack, don’t ignore it or feel embarrassed to call for help. Call your local emergency number for emergency medical care, even if you are not sure whether you’re having a heart attack. Here’s why:
- Acting fast can save your life.
- An ambulance is the best and safest way to get to the hospital. Emergency medical services personnel can check how you are doing and start life-saving medicines and other treatments right away. People who arrive by ambulance often receive faster treatment at the hospital.
- The emergency phone operator or EMS technician can give you advice. You might be told to crush or chew an aspirin if you’re not allergic, unless there is a medical reason for you not to take one. Aspirin taken during a heart attack can limit the damage to your heart and save your life.
Every minute matters. Never delay calling your local emergency number in order to take aspirin or do anything else you think might help.
Heart attack symptoms in women
It’s a common misconception that men and women experience different symptoms when having a heart attack. While symptoms vary from person to person, there are no symptoms that women experience more or less often than men. It may be that women are more likely to dismiss the idea that they may be having a heart attack and delay seeking medical attention. It’s important to recognize the symptoms of a heart attack, take them seriously and act quickly to prevent damaging the heart muscle.
The most common heart attack symptom for women is pain or discomfort in the chest. Women are more likely to have a heart attack without having any chest pain. Therefore, women should pay close attention to other symptoms of heart attack. These include shortness of breath, sweating, fatigue, and dizziness.
Heart attack symptoms can vary from person to person but the most common signs of a heart attack are:
- chest pain or discomfort in your chest that suddenly occurs and doesn’t go away. It may feel like pressure, tightness or squeezing
- the pain may spread to your left or right arm or may spread to your neck, jaw, back or stomach
- you may also feel sick, sweaty, light-headed or short of breath.
Other less common symptoms include:
- a sudden feeling of anxiety that can feel similar to a panic attack
- excessive coughing or wheezing
If you think you’re having a heart attack, call your local emergency services number for an ambulance immediately.
Women may be less likely to seek medical attention and treatment quickly, despite the warning signs. This can dramatically reduce your chance of survival.
Rapid treatment is essential, and the aim is to restore blood flow to the affected part of the heart muscle as soon as possible. This helps to limit the amount of damage to the heart.
How is a Heart Attack Diagnosed?
Your doctor will diagnose a heart attack based on your signs and symptoms, your medical and family histories, and test results 37.
Diagnostic Tests
- EKG or ECG (Electrocardiogram)
An EKG (ECG) is a simple, painless test that detects and records the electrical activity of your heart. The ECG shows how fast your heart is beating and its rhythm (steady or irregular). An EKG also records the strength and timing of electrical signals as they pass through each part of the heart.
An EKG can show signs of heart damage due to coronary heart disease and signs of a previous or current heart attack. It can also find damage from a decrease in blood flow.
- Blood Tests
During a heart attack, heart muscle cells die and release proteins into the bloodstream. Blood tests can measure the amount of these proteins in the bloodstream. Higher than normal levels of these proteins suggest a heart attack.
Commonly used blood tests include troponin tests, CK or CK–MB tests, and serum myoglobin tests. Your doctor will want to test your blood several times during the first 24 to 48 hours after yours symptoms start to check for changes over time.
- Coronary Angiography (coronary catheterization)
Coronary angiography also known as coronary catheterization, is a test that uses dye and special x-rays to show the insides of your coronary arteries. This test often is done during a heart attack to help find blockages in the coronary arteries. A liquid dye is injected into the arteries of your heart through a long, thin tube (catheter) that’s fed through an artery, usually in your leg or groin, to the arteries in your heart. The dye makes the arteries visible on X-ray, revealing areas of blockage.
To get the dye into your coronary arteries, your doctor will use a procedure called cardiac catheterization. A thin, flexible tube called a catheter is put into a blood vessel in your arm, groin (upper thigh), or neck. The tube is threaded into your coronary arteries, and the dye is released into your bloodstream. Special x-rays are taken while the dye is flowing through the coronary arteries. The dye lets your doctor study the flow of blood through the heart and blood vessels.
If your doctor finds a blockage, he or she may recommend a procedure called percutaneous coronary intervention (PCI), sometimes referred to as coronary angioplasty. This procedure can help restore blood flow through a blocked artery. Sometimes a small mesh tube called a stent is placed in the artery to help prevent blockages after the procedure.
Other tests your doctor may want you to have include:
- Echocardiogram. This test uses sound waves (ultrasound) to create pictures of your heart. An echocardiogram can help identify whether an area of your heart has been damaged. The pictures show how well your heart is pumping. It can show if there are problems with your heart valves and heart chambers.
- Chest X-ray. An X-ray image of your chest allows your doctor to check the size of your heart and its blood vessels. It can show if there is any fluid in your lungs.
- Nuclear imaging. This test injects a tiny radioactive substance into your blood. This substance travels to your heart to create pictures of it. It shows how well your heart is pumping. The radioactive substance is safe and leaves your body after the test is finished.
- Cardiac CT or MRI. These tests create images of your heart and chest. Cardiac CT scans use X-rays. Cardiac MRI uses a magnetic field and radio waves to create images of your heart. For both tests, you lie on a table that slides inside a long tubelike machine. Each can be used to diagnose heart problems, including the extent of damage from heart attacks.
Treatment of a heart attack
Early treatment for a heart attack can prevent or limit damage to your heart muscle 38. Acting fast, by calling your local emergency number at the first symptoms of a heart attack, can save your life. Medical personnel can begin diagnosis and treatment even before you get to the hospital.
Immediate Treatment
Certain treatments usually are started right away if a heart attack is suspected, even before the diagnosis is confirmed. These include:
- Aspirin to prevent further blood clotting
- Nitroglycerin to reduce your heart’s workload and improve blood flow through the coronary arteries
- Oxygen therapy
- Treatment for chest pain
Once the diagnosis of a heart attack is confirmed or strongly suspected, doctors start treatments promptly to try to restore blood flow through the blood vessels supplying the heart. The two main treatments are clot-busting medicines and percutaneous coronary intervention (PCI), also known as coronary angioplasty, a procedure used to open blocked coronary arteries.
Clot-Busting Medicines
Thrombolytic medicines also called clot busters, are used to dissolve blood clots that are blocking the coronary arteries. To work best, these medicines must be given within several hours of the start of heart attack symptoms. Ideally, the medicine should be given as soon as possible.
Percutaneous Coronary Intervention
Percutaneous coronary intervention is a nonsurgical procedure that opens blocked or narrowed coronary arteries. A thin, flexible tube (catheter) with a balloon or other device on the end is threaded through a blood vessel, usually in the groin (upper thigh), to the narrowed or blocked coronary artery. Once in place, the balloon located at the tip of the catheter is inflated to compress the plaque and related clot against the wall of the artery. This restores blood flow through the artery. During the procedure, the doctor may put a small mesh tube called a stent in the artery. The stent helps to keep the blood vessel open to prevent blockages in the artery in the months or years after the procedure.
Other Treatments for a Heart Attack
Other treatments for heart attack include:
- Medicines
- Medical procedures
- Heart-healthy lifestyle changes
- Cardiac rehabilitation
Medicines
Your doctor may prescribe one or more of the following medicines.
- ACE inhibitors. ACE inhibitors lower blood pressure and reduce strain on your heart. They also help slow down further weakening of the heart muscle.
- Anticlotting medicines. Anticlotting medicines stop platelets from clumping together and forming unwanted blood clots. Examples of anticlotting medicines include aspirin and clopidogrel.
- Anticoagulants. Anticoagulants, or blood thinners, prevent blood clots from forming in your arteries. These medicines also keep existing clots from getting larger.
- Beta blockers. Beta blockers decrease your heart’s workload. These medicines also are used to relieve chest pain and discomfort and to help prevent another heart attack. Beta blockers also are used to treat arrhythmias (irregular heartbeats).
- Statin medicines. Statins control or lower your blood cholesterol. By lowering your blood cholesterol level, you can decrease your chance of having another heart attack or stroke.
You also may be given medicines to relieve pain and anxiety, and treat arrhythmias. Take all medicines regularly, as your doctor prescribes. Don’t change the amount of your medicine or skip a dose unless your doctor tells you to.
Coronary artery bypass surgery (CABG)
Coronary artery bypass grafting also may be used to treat a heart attack. During coronary artery bypass grafting, a surgeon removes a healthy artery or vein from your body. The artery or vein is then connected, or grafted, to bypass the blocked section of the coronary artery. The grafted artery or vein bypasses (that is, goes around) the blocked portion of the coronary artery. This provides a new route for blood to flow to the heart muscle.
Heart-Healthy Lifestyle Changes
Treatment for a heart attack usually includes making heart-healthy lifestyle changes. Your doctor also may recommend:
- Heart-healthy eating
- Aiming for healthy weight
- Managing stress
- Physical activity
- Quitting smoking
Taking these steps can lower your chances of having another heart attack.
Cardiac Rehabilitation
Your doctor may recommend cardiac rehabilitation (cardiac rehab) to help you recover from a heart attack and to help prevent another heart attack. Nearly everyone who has had a heart attack can benefit from rehab. Cardiac rehab is a medically supervised program that may help improve the health and well-being of people who have heart problems.
The cardiac rehab team may include doctors, nurses, exercise specialists, physical and occupational therapists, dietitians or nutritionists, and psychologists or other mental health specialists.
Rehab has two parts:
- Education, counseling, and training. This part of rehab helps you understand your heart condition and find ways to reduce your risk for future heart problems. The rehab team will help you learn how to cope with the stress of adjusting to a new lifestyle and how to deal with your fears about the future.
- Exercise training. This part helps you learn how to exercise safely, strengthen your muscles, and improve your stamina. Your exercise plan will be based on your personal abilities, needs, and interests.
Most cardiac rehabilitation programs last 3 to 6 months. It’s extremely important to participate in cardiac rehabilitation. People who attend cardiac rehab after a heart attack generally live longer and are less likely to have another heart attack or complications from the heart attack. If cardiac rehab is not recommended during your hospitalization, ask your doctor about it.
Life After a Heart Attack
Many people survive heart attacks and live active, full lives 39. If you get help quickly, treatment can limit damage to your heart muscle. Less heart damage improves your chances for a better quality of life after a heart attack.
After you’ve had a heart attack, you are at higher risk of having another one. Your doctor will likely recommend heart-healthy lifestyle changes to help reduce your risk. They include:
- Maintaining a heart-healthy diet.
- Working toward a healthy weight.
- Managing your stress.
- Being physically active.
- Quitting smoking.
Symptoms during a second heart attack may be different than the first one. If you have any new symptoms of heart attack or are in any doubt, call your local emergency services number. Early treatment is the key to surviving a heart attack.
Medical Followup
After a heart attack, you’ll need treatment for coronary heart disease. This will help prevent another heart attack. Your doctor may recommend:
- Lifestyle changes, such as following a healthy diet, being physically active, maintaining a healthy weight, and quitting smoking.
- Medicines to control chest pain or discomfort, high blood cholesterol, high blood pressure, and your heart’s workload. Some of these medicines can help you prevent another heart attack.
- Anticlotting medicines, such as aspirin, that your doctor may prescribe to help you prevent another heart attack.
- A cardiac rehabilitation program
If you find it hard to get your medicines or or complete your cardiac rehabilitation program, talk with your doctor. Don’t stop the medicines or program because it can help you prevent another heart attack.
Returning to Normal Activities
After a heart attack, most people who don’t have chest pain or discomfort or other problems can safely return to most of their normal activities within a few weeks. Most can begin walking right away.
Sexual activity also can begin within a few weeks for most patients. Talk with your doctor about a safe schedule for returning to your normal routine.
If allowed by State law, driving usually can begin within a week for most patients who don’t have chest pain or discomfort or other disabling problems. Each State has rules about driving a motor vehicle following a serious illness. People who have complications shouldn’t drive until their symptoms have been stable for a few weeks.
Anxiety and Depression After a Heart Attack
After a heart attack, many people worry or have anxiety about having another heart attack. Sometimes they feel depressed and have trouble adjusting to new lifestyle changes. As many as 1 out of every 3 people who have had a heart attack report feelings of depression. People with a higher risk of depression after a heart attack include:
- Women.
- People who have had depression before.
- People who feel alone and without social or emotional support.
Many people who have depression don’t recognize it. They don’t seek help or get treatment. Being depressed can make it harder for you to recover physically. Depression can be treated.
Talk about how you feel with your health care team. Talking to a professional counselor also can help. If you’re very depressed, your doctor may recommend medicines or other treatments that can improve your quality of life.
Joining a patient support group may help you adjust to life after a heart attack. You can see how other people who have the same symptoms have coped with them. Talk with your doctor about local support groups or check with an area medical center.
Support from family and friends also can help relieve stress and anxiety. Let your loved ones know how you feel and what they can do to help you.
Risk of a Repeat Heart Attack
Once you’ve had a heart attack, you’re at higher risk for another one 39. Knowing the difference between angina and a heart attack is important. Angina is chest pain that occurs in people who have coronary heart disease.
The pain from angina usually occurs after physical exertion and goes away in a few minutes when you rest or take medicine as directed.
The pain from a heart attack usually is more severe than the pain from angina. Heart attack pain doesn’t go away when you rest or take medicine.
If you don’t know whether your chest pain is angina or a heart attack, call your local emergency number.
The symptoms of a second heart attack may not be the same as those of a first heart attack. Don’t take a chance if you’re in doubt. Always call your local emergency number right away if you or someone else has heart attack symptoms.
Unfortunately, most heart attack victims wait 2 hours or more after their symptoms start before they seek medical help. This delay can result in lasting heart damage or death 39.
Sex after a heart attack
Some people worry about having sex after a heart attack, but most people can safely return to sexual activity after recovery. When you can resume sexual activity will depend on your physical comfort, emotional readiness and previous sexual activity. Ask your doctor when it’s safe to have sex.
Some heart medications can affect sexual function. If you’re having problems with sexual dysfunction, talk to your doctor.
Will I have to take medicine for the rest of my life?
If you have had a heart attack, your doctor will probably want you to take certain medicines for a long time. This can help reduce your risk of more heart problems. Your doctor can answer your questions about these medicines. He or she can tell you the benefits and risks of taking them.
- Aspirin can reduce the risk of a heart attack. A low dose of aspirin each day can keep your blood from forming clots that can eventually block the arteries. Talk to your doctor about the risks and benefits of aspirin therapy.
- Antiplatelet medicines also help stop blood clots from forming. These drugs are especially important to take for at least a year if you have had a stent placed in your heart.
- Beta blockers are a group of drugs that lower the heart rate and blood pressure. They help improve blood flow to the heart.
- ACE inhibitors are a group of drugs that can help if your heart is not pumping blood well. This medicine helps open your arteries and lower your blood pressure. This improves blood flow.
- Statins are a group of drugs that are used to control cholesterol. They lower “bad” cholesterol (LDL) levels and may help increase “good” cholesterol (HDL).
What is coronary heart disease?
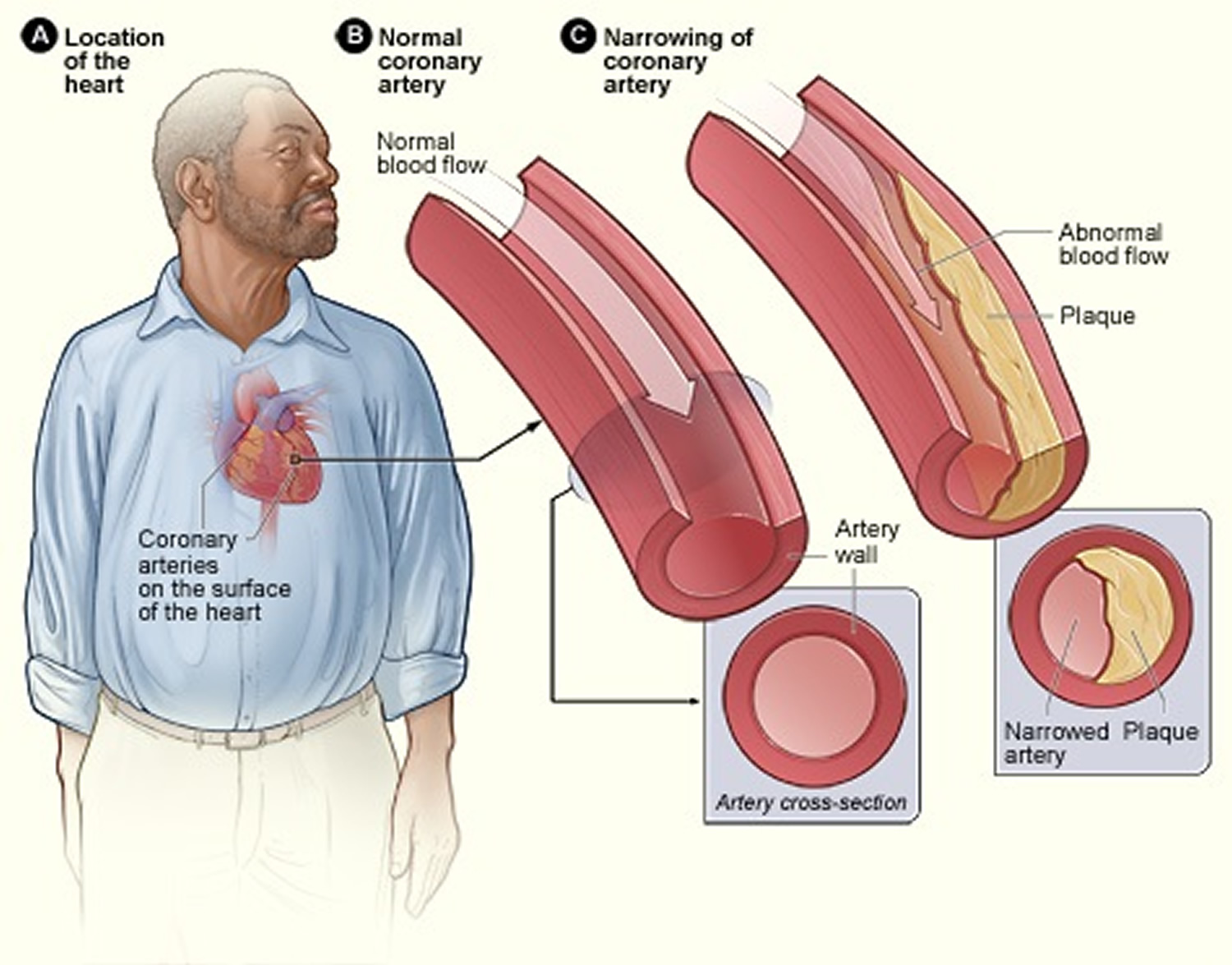
Coronary heart disease (CHD) is a disease in which a waxy substance called plaque builds up inside the coronary arteries. Arteries are blood vessels that carry oxygen-rich blood to your heart and other parts of your body. These arteries supply oxygen-rich blood to your heart muscle. Plaque is made up of fat, cholesterol, calcium, and other substances found in the blood. Over time, plaque hardens and narrows your arteries. This limits the flow of oxygen-rich blood to your organs and other parts of your body.
When plaque builds up in the arteries, the condition is called atherosclerosis.
Atherosclerosis is a disease in which plaque builds up inside your arteries. The buildup of plaque occurs over many years.
Atherosclerosis plaque narrows the coronary arteries and reduces blood flow to your heart muscle. Plaque narrows and stiffens the coronary arteries. This reduces the flow of oxygen-rich blood to the heart muscle, causing chest pain.
Plaque buildup also makes it more likely that blood clots will form in your arteries. Blood clots can partially or completely block blood flow, which can cause a heart attack.
- If blood flow to your heart muscle is reduced or blocked, you may have angina (chest pain or discomfort) or a heart attack.
Plaque also can form in the heart’s smallest arteries. This disease is called coronary microvascular disease (MVD). In coronary MVD, plaque doesn’t cause blockages in the arteries as it does in coronary heart disease.
Atherosclerosis can lead to serious problems, including heart attack, stroke, or even death.
Figure 2. Atherosclerosis plaque
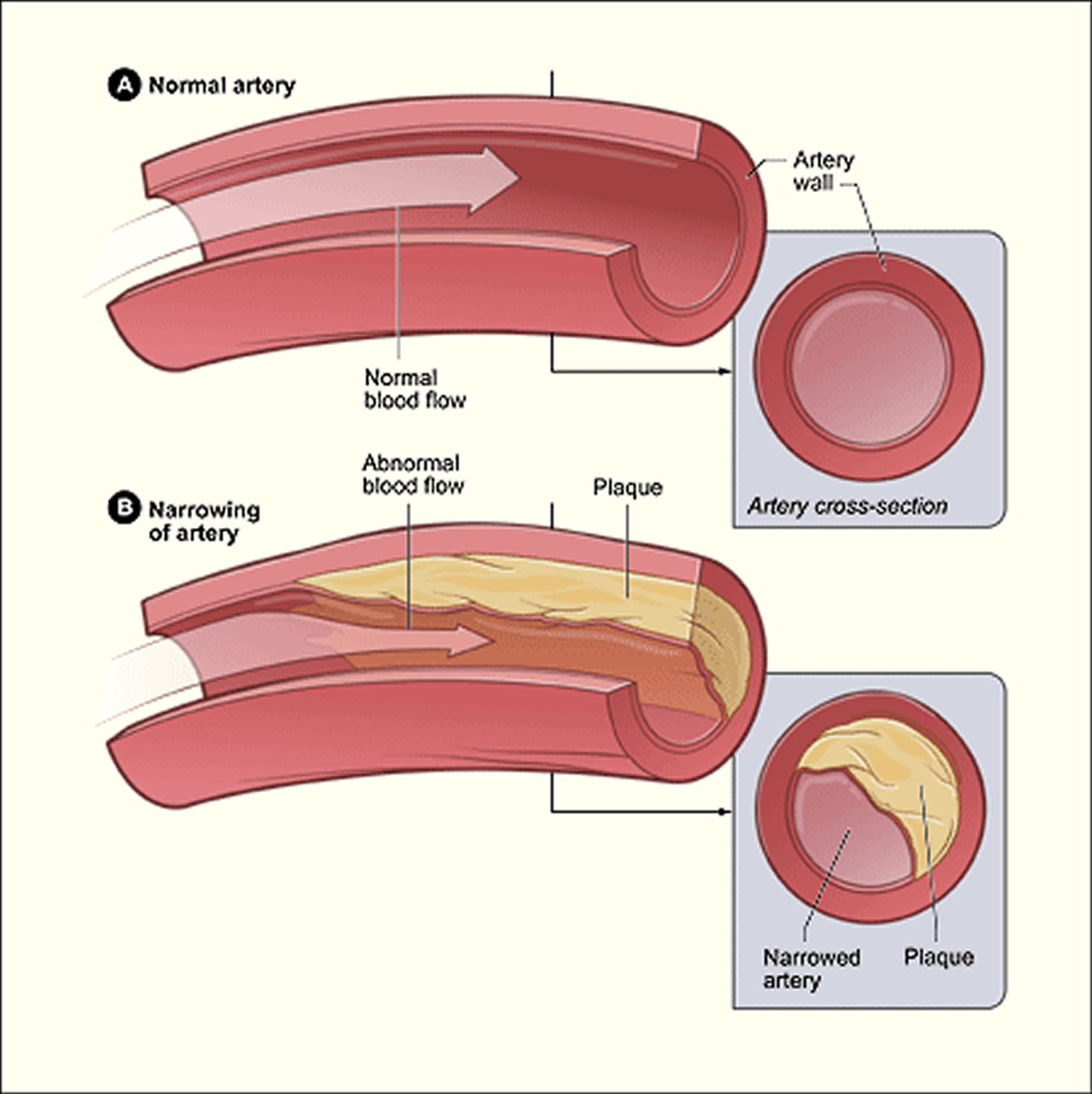
Figure 3. Atherosclerosis blocking the artery supply in your heart
What is Angina?
Angina is chest pain or discomfort that occurs if an area of your heart muscle doesn’t get enough oxygen-rich blood. Angina isn’t a disease; it’s a symptom of an underlying heart problem 41. Angina usually is a symptom of coronary heart disease (CHD).
Other names for Angina
- Acute coronary syndrome
- Angina pectoris
- Chest pain
- Coronary artery spasms
- Microvascular angina
- Prinzmetal’s angina
- Stable or common angina
- Unstable angina
- Variant angina.
Angina may feel like pressure or squeezing in your chest. The pain also can occur in your shoulders, arms, neck, jaw, or back. Angina pain may even feel like indigestion.
Coronary heart disease is the most common type of heart disease in adults. It occurs if a waxy substance called plaque builds up on the inner walls of your coronary arteries. These arteries carry oxygen-rich blood to your heart.
Angina also can be a symptom of coronary microvascular disease (MVD). This is heart disease that affects the heart’s smallest coronary arteries. In coronary microvascular disease, plaque doesn’t create blockages in the arteries like it does in coronary heart disease.
Studies have shown that coronary microvascular disease is more likely to affect women than men. Coronary microvascular disease also is called cardiac syndrome X and nonobstructive coronary heart disease.
Experts believe that nearly 7 million people in the United States suffer from angina 41. The condition occurs equally among men and women.
Angina can be a sign of coronary heart disease, even if initial tests don’t point to the disease. However, not all chest pain or discomfort is a sign of coronary heart disease.
Other conditions also can cause chest pain, such as:
- Pulmonary embolism (a blockage in a lung artery)
- A lung infection
- Aortic dissection (tearing of a major artery)
- Aortic stenosis (narrowing of the heart’s aortic valve)
- Hypertrophic cardiomyopathy (heart muscle disease)
- Pericarditis (inflammation in the tissues that surround the heart)
- A panic attack
All chest pain should be checked by a doctor.
Types of Angina
The major types of angina are stable, unstable, variant (Prinzmetal’s), and microvascular 41. Knowing how the types differ is important. This is because they have different symptoms and require different treatments.
Stable Angina
Stable angina is the most common type of angina. It occurs when the heart is working harder than usual. Stable angina has a regular pattern. (“Pattern” refers to how often the angina occurs, how severe it is, and what factors trigger it.)
If you have stable angina, you can learn its pattern and predict when the pain will occur. The pain usually goes away a few minutes after you rest or take your angina medicine.
Stable angina isn’t a heart attack, but it suggests that a heart attack is more likely to happen in the future.
Unstable Angina
Unstable angina doesn’t follow a pattern. It may occur more often and be more severe than stable angina. Unstable angina also can occur with or without physical exertion, and rest or medicine may not relieve the pain.
Unstable angina is very dangerous and requires emergency treatment. This type of angina is a sign that a heart attack may happen soon.
Variant (Prinzmetal’s) Angina
Variant angina is rare. A spasm in a coronary artery causes this type of angina 41. Variant angina usually occurs while you’re at rest, and the pain can be severe. It usually happens between midnight and early morning. Medicine can relieve this type of angina.
Microvascular Angina
Microvascular angina can be more severe and last longer than other types of angina 41. Medicine may not relieve this type of angina.
Who is at Risk for Angina?
Angina is a symptom of an underlying heart problem. It’s usually a symptom of coronary heart disease, but it also can be a symptom of coronary microvascular disease. So, if you’re at risk for coronary heart disease or coronary microvascular disease, you’re also at risk for angina 42.
The major risk factors for coronary heart disease and coronary microvascular disease include:
- Unhealthy cholesterol levels.
- High blood pressure.
- Smoking.
- Insulin resistance or diabetes.
- Overweight or obesity.
- Metabolic syndrome.
- Lack of physical activity.
- Unhealthy diet.
- Older age. (The risk increases for men after 45 years of age and for women after 55 years of age.)
- Family history of early heart disease.
People sometimes think that because men have more heart attacks than women, men also suffer from angina more often. In fact, overall, angina occurs equally among men and women 42.
Microvascular angina, however, occurs more often in women. About 70 percent of the cases of microvascular angina occur in women around the time of menopause 42.
Unstable angina occurs more often in older adults 42. Variant angina is rare; it accounts for only about 2 out of 100 cases of angina. People who have variant angina often are younger than those who have other forms of angina 42.
What are the Signs and Symptoms of Angina?
Pain and discomfort are the main symptoms of angina. Angina often is described as pressure, squeezing, burning, or tightness in the chest. The pain or discomfort usually starts behind the breastbone 43.
Pain from angina also can occur in the arms, shoulders, neck, jaw, throat, or back. The pain may feel like indigestion. Some people say that angina pain is hard to describe or that they can’t tell exactly where the pain is coming from.
Signs and symptoms such as nausea (feeling sick to your stomach), fatigue (tiredness), shortness of breath, sweating, light-headedness, and weakness also may occur.
Women are more likely to feel discomfort in the neck, jaw, throat, abdomen, or back. Shortness of breath is more common in older people and those who have diabetes. Weakness, dizziness, and confusion can mask the signs and symptoms of angina in elderly people.
Symptoms also vary based on the type of angina you have.
Because angina has so many possible symptoms and causes, all chest pain should be checked by a doctor. Chest pain that lasts longer than a few minutes and isn’t relieved by rest or angina medicine may be a sign of a heart attack. Call your local emergency number right away.
Stable Angina
The pain or discomfort:
- Occurs when the heart must work harder, usually during physical exertion
- Doesn’t come as a surprise, and episodes of pain tend to be alike
- Usually lasts a short time (5 minutes or less)
- Is relieved by rest or medicine
- May feel like gas or indigestion
- May feel like chest pain that spreads to the arms, back, or other areas.
Unstable Angina
The pain or discomfort:
- Often occurs at rest, while sleeping at night, or with little physical exertion
- Comes as a surprise
- Is more severe and lasts longer than stable angina (as long as 30 minutes)
- Usually isn’t relieved by rest or medicine
- May get worse over time
- May mean that a heart attack will happen soon.
Variant Angina
The pain or discomfort:
- Usually occurs at rest and during the night or early morning hours
- Tends to be severe
- Is relieved by medicine.
Microvascular Angina
The pain or discomfort:
- May be more severe and last longer than other types of angina pain
- May occur with shortness of breath, sleep problems, fatigue, and lack of energy
- Often is first noticed during routine daily activities and times of mental stress.
What Causes Angina?
Angina usually is a symptom of coronary heart disease 44. This means that the underlying causes of angina generally are the same as the underlying causes of coronary heart disease.
Research suggests that coronary heart disease starts when certain factors damage the inner layers of the coronary arteries. These factors include:
- Smoking
- High amounts of certain fats and cholesterol in the blood
- High blood pressure
- High amounts of sugar in the blood due to insulin resistance or diabetes
Plaque may begin to build up where the arteries are damaged. When plaque builds up in the arteries, the condition is called atherosclerosis.
Plaque narrows or blocks the arteries, reducing blood flow to the heart muscle. Some plaque is hard and stable and causes the arteries to become narrow and stiff. This can greatly reduce blood flow to the heart and cause angina.
Other plaque is soft and more likely to rupture (break open) and cause blood clots. Blood clots can partially or totally block the coronary arteries and cause angina or a heart attack.
Immediate Causes
Many factors can trigger angina pain, depending on the type of angina you have.
Stable Angina
Physical exertion is the most common trigger of stable angina. Severely narrowed arteries may allow enough blood to reach the heart when the demand for oxygen is low, such as when you’re sitting.
However, with physical exertion—like walking up a hill or climbing stairs—the heart works harder and needs more oxygen.
Other triggers of stable angina include:
- Emotional stress
- Exposure to very hot or cold temperatures
- Heavy meals
- Smoking
Unstable Angina
Blood clots that partially or totally block an artery cause unstable angina.
If plaque in an artery ruptures, blood clots may form. This creates a blockage. A clot may grow large enough to completely block the artery and cause a heart attack.
Blood clots may form, partially dissolve, and later form again. Angina can occur each time a clot blocks an artery.
Variant Angina
A spasm in a coronary artery causes variant angina. The spasm causes the walls of the artery to tighten and narrow. Blood flow to the heart slows or stops. Variant angina can occur in people who have coronary heart disease and in those who don’t.
The coronary arteries can spasm as a result of:
- Exposure to cold
- Emotional stress
- Medicines that tighten or narrow blood vessels
- Smoking
- Cocaine use
Microvascular Angina
This type of angina may be a symptom of coronary microvascular disease. Coronary microvascular disease is heart disease that affects the heart’s smallest coronary arteries.
Reduced blood flow in the small coronary arteries may cause microvascular angina. Plaque in the arteries, artery spasms, or damaged or diseased artery walls can reduce blood flow through the small coronary arteries.
How can Angina Be Prevented?
You can prevent or lower your risk for angina and heart disease by making lifestyle changes and treating related conditions 45.
Making Lifestyle Changes
Healthy lifestyle choices can help prevent or delay angina and heart disease. To adopt a healthy lifestyle, you can:
- Quit smoking and avoid secondhand smoke
- Avoid angina triggers
- Follow a healthy diet
- Be physically active
- Maintain a healthy weight
- Learn ways to handle stress and relax
- Take your medicines as your doctor prescribes
Treating Related Conditions
You also can help prevent or delay angina and heart disease by treating related conditions, such as high blood cholesterol, high blood pressure, diabetes, and overweight or obesity.
If you have one or more of these conditions, talk with your doctor about how to control them. Follow your treatment plan and take all of your medicines as your doctor prescribes.
How is Angina Diagnosed?
The most important issues to address when you go to the doctor with chest pain are:
- What’s causing the chest pain
- Whether you’re having or are about to have a heart attack.
Angina is a symptom of an underlying heart problem, usually coronary heart disease 46. The type of angina pain you have can be a sign of how severe the coronary heart disease is and whether it’s likely to cause a heart attack.
If you have chest pain, your doctor will want to find out whether it’s angina. He or she also will want to know whether the angina is stable or unstable. If it’s unstable, you may need emergency medical treatment to try to prevent a heart attack.
To diagnose chest pain as stable or unstable angina, your doctor will do a physical exam, ask about your symptoms, and ask about your risk factors for and your family history of coronary heart disease or other heart diseases.
Your doctor also may ask questions about your symptoms, such as:
- What brings on the pain or discomfort and what relieves it?
- What does the pain or discomfort feel like (for example, heaviness or tightness)?
- How often does the pain occur?
- Where do you feel the pain or discomfort?
- How severe is the pain or discomfort?
- How long does the pain or discomfort last?
Diagnostic Tests and Procedures
If your doctor thinks that you have unstable angina or that your angina is related to a serious heart condition, he or she may recommend one or more tests.
- EKG (Electrocardiogram)
An EKG is a simple, painless test that detects and records the heart’s electrical activity. The test shows how fast the heart is beating and its rhythm (steady or irregular). An EKG also records the strength and timing of electrical signals as they pass through the heart.
An EKG can show signs of heart damage due to coronary heart disease and signs of a previous or current heart attack. However, some people who have angina have normal EKGs.
- Stress Testing
During stress testing, you exercise to make your heart work hard and beat fast while heart tests are done. If you can’t exercise, you may be given medicine to make your heart work hard and beat fast.
When your heart is working hard and beating fast, it needs more blood and oxygen. Plaque-narrowed arteries can’t supply enough oxygen-rich blood to meet your heart’s needs.
A stress test can show possible signs and symptoms of coronary heart disease, such as:
- Abnormal changes in your heart rate or blood pressure
- Shortness of breath or chest pain
- Abnormal changes in your heart rhythm or your heart’s electrical activity
As part of some stress tests, pictures are taken of your heart while you exercise and while you rest. These imaging stress tests can show how well blood is flowing in various parts of your heart. They also can show how well your heart pumps blood when it beats.
- Chest X Ray
A chest x ray takes pictures of the organs and structures inside your chest, such as your heart, lungs, and blood vessels.
A chest x ray can reveal signs of heart failure. It also can show signs of lung disorders and other causes of symptoms not related to coronary heart disease. However, a chest x ray alone is not enough to diagnose angina or coronary heart disease.
- Coronary Angiography and Cardiac Catheterization
Your doctor may recommend coronary angiography if he or she suspects you have coronary heart disease. This test uses dye and special x rays to show the inside of your coronary arteries.
To get the dye into your coronary arteries, your doctor will use a procedure called cardiac catheterization.
A thin, flexible tube called a catheter is put into a blood vessel in your arm, groin (upper thigh), or neck. The tube is threaded into your coronary arteries, and the dye is released into your bloodstream.
Special x rays are taken while the dye is flowing through your coronary arteries. The dye lets your doctor study the flow of blood through your heart and blood vessels.
Cardiac catheterization usually is done in a hospital. You’re awake during the procedure. It usually causes little or no pain, although you may feel some soreness in the blood vessel where your doctor inserts the catheter.
- Computed Tomography Angiography
Computed tomography angiography uses dye and special x rays to show blood flow through the coronary arteries. This test is less invasive than coronary angiography with cardiac catheterization.
For computed tomography angiography, a needle connected to an intravenous (IV) line is put into a vein in your hand or arm. Dye is injected through the IV line during the scan. You may have a warm feeling when this happens. The dye highlights your blood vessels on the CT scan pictures.
Sticky patches called electrodes are put on your chest. The patches are attached to an EKG machine to record your heart’s electrical activity during the scan.
The CT scanner is a large machine that has a hollow, circular tube in the middle. You lie on your back on a sliding table. The table slowly slides into the opening of the machine.
Inside the scanner, an x-ray tube moves around your body to take pictures of different parts of your heart. A computer puts the pictures together to make a three-dimensional (3D) picture of the whole heart.
- Blood Tests
Blood tests check the levels of certain fats, cholesterol, sugar, and proteins in your blood. Abnormal levels may show that you have risk factors for coronary heart disease.
Your doctor may recommend a blood test to check the level of a protein called C-reactive protein (CRP) in your blood. Some studies suggest that high levels of CRP in the blood may increase the risk for coronary heart disease and heart attack.
Your doctor also may recommend a blood test to check for low levels of hemoglobin your blood. Hemoglobin is an iron-rich protein in red blood cells. It helps the blood cells carry oxygen from the lungs to all parts of your body. If your hemoglobin level is low, you may have a condition called anemia.
How is Angina Treated?
Treatments for angina include lifestyle changes, medicines, medical procedures, cardiac rehabilitation (rehab), and other therapies 47. The main goals of treatment are to:
- Reduce pain and discomfort and how often it occurs
- Prevent or lower your risk for heart attack and death by treating your underlying heart condition.
Lifestyle changes and medicines may be the only treatments needed if your symptoms are mild and aren’t getting worse. If lifestyle changes and medicines don’t control angina, you may need medical procedures or cardiac rehab.
Unstable angina is an emergency condition that requires treatment in a hospital.
Lifestyle Changes
Making lifestyle changes can help prevent episodes of angina. You can:
- Slow down or take rest breaks if physical exertion triggers angina.
- Avoid large meals and rich foods that leave you feeling stuffed if heavy meals trigger angina.
- Try to avoid situations that make you upset or stressed if emotional stress triggers angina. Learn ways to handle stress that can’t be avoided.
You also can make lifestyle changes that help lower your risk for coronary heart disease. One of the most important changes is to quit smoking. Smoking can damage and tighten blood vessels and raise your risk for coronary heart disease. Talk with your doctor about programs and products that can help you quit. Also, try to avoid secondhand smoke.
If you have trouble quitting smoking on your own, consider joining a support group. Many hospitals, workplaces, and community groups offer classes to help people quit smoking.
Following a healthy diet is another important lifestyle change. A healthy diet can prevent or reduce high blood pressure and high blood cholesterol and help you maintain a healthy weight.
A healthy diet includes a variety of fruits and vegetables (including beans and peas). It also includes whole grains, lean meats, poultry without skin, seafood, and fat-free or low-fat milk and dairy products. A healthy diet also is low in sodium (salt), added sugars, solid fats, and refined grains.
For more information about following a healthy diet, go to:
Other important lifestyle changes include:
- Being physically active. Check with your doctor to find out how much and what kinds of activity are safe for you. For more information, go to the Healthy Exercise article.
- Maintaining a healthy weight. If you’re overweight or obese, work with your doctor to create a reasonable weight-loss plan. Controlling your weight helps you control coronary heart disease risk factors.
- Taking all medicines as your doctor prescribes, especially if you have diabetes.
Medicines
Nitrates are the medicines most commonly used to treat angina. They relax and widen blood vessels. This allows more blood to flow to the heart, while reducing the heart’s workload.
Nitroglycerin is the most commonly used nitrate for angina. Nitroglycerin that dissolves under your tongue or between your cheek and gum is used to relieve angina episodes.
Nitroglycerin pills and skin patches are used to prevent angina episodes. However, pills and skin patches act too slowly to relieve pain during an angina attack.
Other medicines also are used to treat angina, such as beta blockers, calcium channel blockers, ACE inhibitors, oral antiplatelet medicines, or anticoagulants (blood thinners). These medicines can help:
- Lower blood pressure and cholesterol levels
- Slow the heart rate
- Relax blood vessels
- Reduce strain on the heart
- Prevent blood clots from forming
People who have stable angina may be advised to get annual flu shots.
Medical Procedures
If lifestyle changes and medicines don’t control angina, you may need a medical procedure to treat the underlying heart disease. Both angioplasty and coronary artery bypass grafting (CABG) are commonly used to treat heart disease.
Angioplasty opens blocked or narrowed coronary arteries. During angioplasty, a thin tube with a balloon or other device on the end is threaded through a blood vessel to the narrowed or blocked coronary artery.
Once in place, the balloon is inflated to push the plaque outward against the wall of the artery. This widens the artery and restores blood flow.
Angioplasty can improve blood flow to your heart and relieve chest pain. A small mesh tube called a stent usually is placed in the artery to help keep it open after the procedure.
During CABG, healthy arteries or veins taken from other areas in your body are used to bypass (that is, go around) your narrowed coronary arteries. Bypass surgery can improve blood flow to your heart, relieve chest pain, and possibly prevent a heart attack.
You will work with your doctor to decide which treatment is better for you.
Cardiac Rehabilitation
Your doctor may recommend cardiac rehab for angina or after angioplasty, CABG, or a heart attack. Cardiac rehab is a medically supervised program that can help improve the health and well-being of people who have heart problems.
The cardiac rehab team may include doctors, nurses, exercise specialists, physical and occupational therapists, dietitians or nutritionists, and psychologists or other mental health specialists.
Rehab has two parts:
- Exercise training. This part helps you learn how to exercise safely, strengthen your muscles, and improve your stamina. Your exercise plan will be based on your personal abilities, needs, and interests.
- Education, counseling, and training. This part of rehab helps you understand your heart condition and find ways to reduce your risk for future heart problems. The rehab team will help you learn how to adjust to a new lifestyle and deal with your fears about the future.
Enhanced External Counterpulsation Therapy
Enhanced external counterpulsation therapy is helpful for some people who have angina. Large cuffs, similar to blood pressure cuffs, are put on your legs. The cuffs are inflated and deflated in sync with your heartbeat 47.
Enhanced external counterpulsation therapy improves the flow of oxygen-rich blood to your heart muscle and helps relieve angina. You typically get 35 1-hour treatments over 7 weeks 47.
Living With Angina
Angina isn’t a heart attack, but it does increase your risk of having a heart attack 48. The risk is even higher if you have unstable angina. For these reasons, it’s important that you know:
- The usual pattern of your angina, if you have it regularly.
- What medicines you take (keep a list) and how to take them. Make sure your medicines are readily available.
- How to control your angina.
- The limits of your physical activity.
- How and when to seek medical attention.
Know the Pattern of Your Angina
Stable angina usually occurs in a pattern. You should know:
- What causes the pain to occur
- What the pain feels like
- How long the pain usually lasts
- Whether rest or medicine relieves the pain
After several episodes, you’ll learn the pattern of your angina. You’ll want to pay attention to whether the pattern changes. Pattern changes may include angina that occurs more often, lasts longer, is more severe, occurs without physical exertion, or doesn’t go away with rest or medicines.
These changes may be a sign that your symptoms are getting worse or becoming unstable. You should seek medical help. Unstable angina suggests that you’re at high risk for a heart attack very soon.
Know Your Medicines
You should know what medicines you’re taking, the purpose of each, how and when to take them, and possible side effects. Know exactly when and how to take fast-acting nitroglycerin or other nitrates to relieve chest pain.
Correctly storing your angina medicines and knowing when to replace them also is important. Your doctor can advise you about this.
If you have side effects from your medicines, let your doctor know. You should never stop taking your medicines without your doctor’s approval.
Talk with your doctor if you have any questions or concerns about taking your angina medicines. Tell him or her about any other medicines you’re taking. Some medicines can cause serious problems if they’re taken with nitrates or other angina medicines.
Know How To Control Your Angina
After several angina episodes, you’ll know the level of activity, stress, and other factors that trigger your angina. By knowing this, you can take steps to prevent or lessen the severity of episodes.
Physical Exertion
Know what level of physical exertion triggers your angina and try to stop and rest before chest pain starts. For example, if walking up a flight of stairs leads to chest pain, stop halfway and rest before continuing.
If chest pain occurs during physical exertion, stop and rest or take your angina medicine. The pain should go away in a few minutes. If the pain doesn’t go away or lasts longer than usual, call your local emergency number for emergency care.
Emotional Stress
Anger, arguing, and worrying are examples of emotional stress that can trigger angina. Try to avoid or limit situations that cause these emotions.
Exercise and relaxation can help relieve stress. Alcohol and drug use play a part in causing stress and don’t relieve it. If stress is a problem for you, talk with your doctor about getting help for it.
Eating Large Meals
If large meals lead to chest pain, eat smaller meals. Also, avoid eating rich foods.
Know the Limits of Your Physical Activity
Most people who have stable angina can continue their normal activities. This includes work, hobbies, and sexual relations. However, if you do very strenuous activities or have a stressful job, talk with your doctor.
Know How and When To Seek Medical Attention
Angina increases your risk for a heart attack. It’s important that you and your family know how and when to seek medical attention.
Talk with your doctor about making an emergency action plan. The plan should include making sure you and your family members know:
- The signs and symptoms of a heart attack
- How to use aspirin and nitroglycerin when needed
- How to access emergency medical services in your community
- The location of the nearest hospital that offers 24-hour emergency heart care
Discuss your emergency plan with your family members. Take action quickly if your chest pain becomes severe, lasts longer than a few minutes, or isn’t relieved by rest or medicine.
Sometimes it’s hard to tell the difference between unstable angina and a heart attack. Both are emergencies, so you should call local emergency number right away.
What is Coronary Microvascular Disease?
Coronary microvascular disease (MVD) is also called nonobstructive coronary heart disease or cardiac syndrome X. Coronary microvascular disease (MVD) is a heart disease that affects the tiny coronary (heart) arteries. In coronary microvascular disease, the walls of the heart’s tiny arteries are damaged or diseased 49.
Coronary microvascular disease is different from traditional coronary heart disease, also called coronary artery disease. In coronary heart disease, a waxy substance called plaque builds up in the large coronary arteries. The plaque narrows the heart’s large arteries and reduces the flow of oxygen-rich blood to your heart muscle. The buildup of plaque also makes it more likely that blood clots will form in your arteries. Blood clots can mostly or completely block blood flow through a coronary artery.
In coronary microvascular disease, however, the heart’s tiny arteries are affected. Plaque doesn’t create blockages in these vessels as it does in the heart’s large arteries 49.
Coronary microvascular disease can affect both men and women. Both men and women who have coronary microvascular disease often have diabetes or high blood pressure (hypertension). Some people who have coronary microvascular disease may have inherited heart muscle diseases 49.
However, women may be at risk for coronary microvascular disease if they have lower than normal levels of estrogen at any point in their adult lives. This refers to the estrogen that the ovaries produce, not the estrogen used in hormone therapy 50. Low estrogen levels before menopause can raise younger women’s risk for the disease. Causes of low estrogen levels in younger women can be mental stress or a problem with the function of the ovaries.
Diagnosing coronary microvascular disease has been a challenge for doctors. Standard tests used to diagnose coronary heart disease aren’t designed to detect coronary microvascular disease. More research is needed to find the best diagnostic tests and treatments for the disease 49.
If you have coronary microvascular disease, you can take action to control it. Follow the steps described in “How can Coronary Microvascular Disease Be Prevented ?”
Coronary microvascular disease, like traditional coronary heart disease, increases your risk for a heart attack. If you have signs or symptoms of a heart attack, call local emergency number at once.
These signs and symptoms may include chest pain, upper body discomfort, shortness of breath, and nausea (feeling sick to your stomach). For more detailed information about the warning signs of a heart attack, go to the section on warning signs of a heart attack.
Ongoing Care
If you have coronary microvascular disease, see your doctor regularly to make sure the disease isn’t getting worse. Work with your doctor to keep track of your cholesterol, blood pressure, and blood sugar levels. This will help your doctor adjust your treatment as needed.
You may need to see a cardiologist (heart specialist) in addition to your primary care doctor. Talk with your doctor about how often you should schedule office visits or blood tests. Between those visits, call your doctor if you have any new symptoms or your symptoms worsen.
You should:
- Know your symptoms and how and when to seek medical help.
- Be able to describe the usual pattern of your symptoms.
- Know which medicines you take and when and how to take them.
- Know how to control your symptoms, including angina.
- Know the limits of your physical activity.
- Learn ways to avoid or cope with stress.
Warning Signs of a Heart Attack
If you have coronary microvascular disease, learn the warning signs of a heart attack 51. The signs and symptoms of a heart attack include:
- Chest pain or discomfort. This involves uncomfortable pressure, squeezing, fullness, or pain in the center or left side of the chest that can be mild or strong. This pain or discomfort often lasts more than a few minutes or goes away and comes back.
- Upper body discomfort in one or both arms, the back, neck, jaw, or upper part of the stomach.
- Shortness of breath, which may occur with or before chest discomfort.
- Nausea (feeling sick to your stomach), vomiting, light-headedness or fainting, or breaking out in a cold sweat.
- Sleep problems, fatigue (tiredness), and lack of energy.
If you think you’re having a heart attack, call local emergency number at once. Early treatment can prevent or limit damage to your heart muscle. Do not drive to the hospital or let someone else drive you. Instead, call an ambulance so that medical personnel can begin life-saving treatment on the way to the emergency room.
- Let the people you see regularly know you’re at risk for a heart attack. They can seek emergency care if you suddenly faint, collapse, or have other severe symptoms.
What Causes Coronary Microvascular Disease?
The same risk factors that cause atherosclerosis may cause coronary microvascular disease. Atherosclerosis is a disease in which plaque builds up inside the arteries.
Risk factors for atherosclerosis include:
- Diabetes. It is a disease in which the body’s blood sugar level is too high because the body doesn’t make enough insulin or doesn’t use its insulin properly.
- Family history of early heart disease. Your risk of atherosclerosis increases if your father or a brother was diagnosed with heart disease before age 55, or if your mother or a sister was diagnosed with heart disease before age 65.
- High blood pressure. Blood pressure is considered high if it stays at or above 140/90 mmHg over time. If you have diabetes or chronic kidney disease, high blood pressure is defined as 130/80 mmHg or higher. (The mmHg is millimeters of mercury—the units used to measure blood pressure.)
- Insulin resistance. This condition occurs if the body can’t use its insulin properly. Insulin is a hormone that helps move blood sugar into cells where it’s used for energy. Overtime, insulin resistance can lead to diabetes.
- Lack of physical activity. Physical inactivity can worsen some other risk factors for atherosclerosis, such as unhealthy blood cholesterol levels, high blood pressure, diabetes, and overweight or obesity.
- Older age. As you age, your risk for atherosclerosis increases. The process of atherosclerosis begins in youth and typically progresses over many decades before disease develops.
- Overweight and obesity. The terms “overweight” and “obesity” refer to body weight that’s greater than what is considered healthy for a certain height.
- Smoking. Smoking can damage and tighten blood vessels, lead to unhealthy cholesterol levels, and raise blood pressure. Smoking also doesn’t allow enough oxygen to reach the body’s tissues.
- Unhealthy blood cholesterol levels. This includes high LDL (“bad”) cholesterol and low HDL (“good”) cholesterol.
- Unhealthy diet. An unhealthy diet can raise your risk for atherosclerosis. Foods that are high in saturated and trans fats, cholesterol, sodium (salt), and sugar can worsen other risk factors for atherosclerosis.
In women, coronary microvascular disease also may be linked to low estrogen levels occurring before or after menopause 52. Also, the disease may be linked to anemia or conditions that affect blood clotting 52. Anemia is thought to slow the growth of cells needed to repair damaged blood vessels.
Researchers continue to explore other possible causes of coronary microvascular disease.
Figure 4. Coronary Microvascular Disease
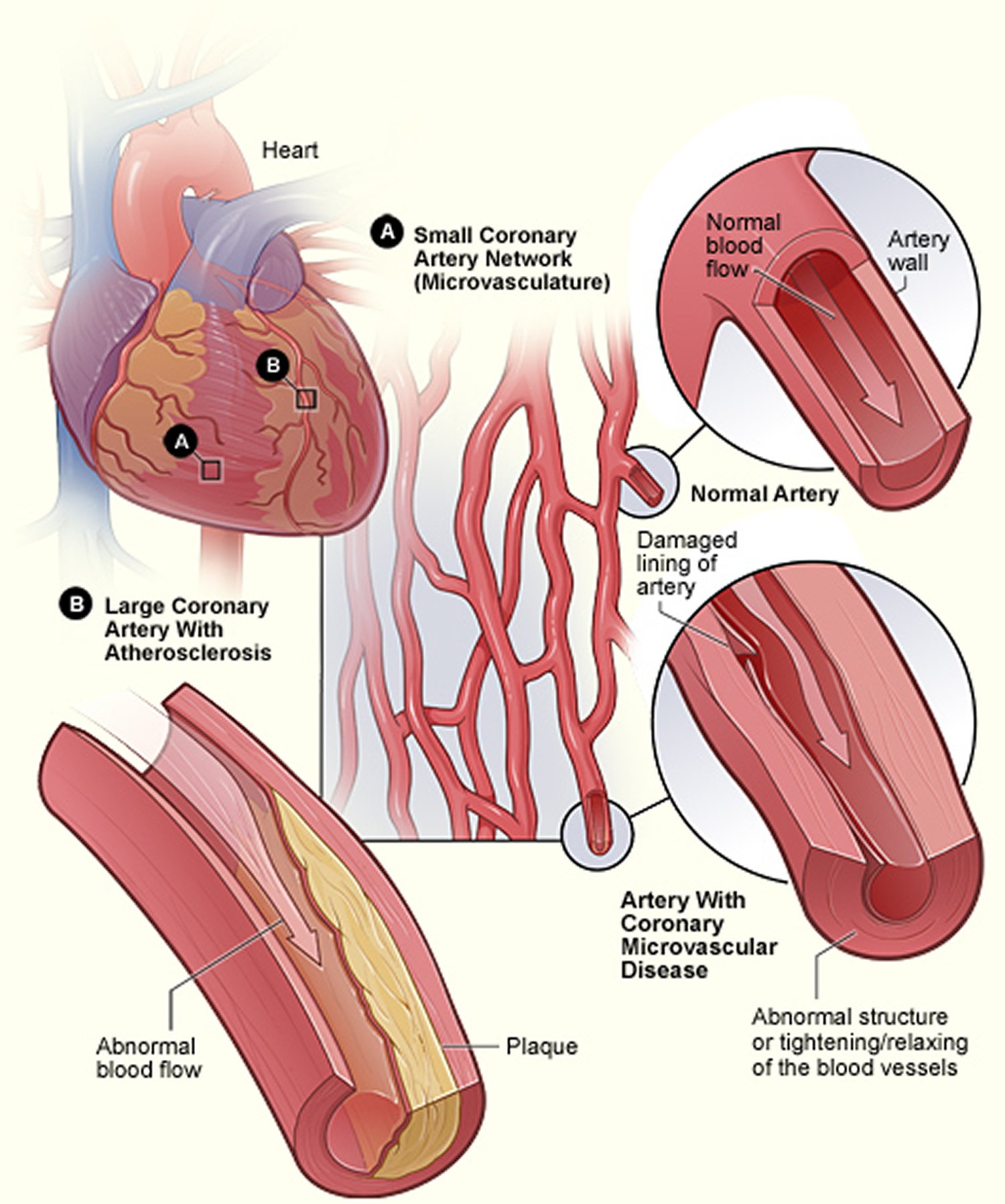
Footnote: A shows the small coronary artery network (microvasculature), containing a normal artery and an artery with coronary microvascular disease. B shows a large coronary artery with plaque buildup.
[Source 49 ]How can Coronary Microvascular Disease Be Prevented?
No specific studies have been done on how to prevent coronary microvascular disease 53.
Researchers don’t yet know how or in what way preventing coronary microvascular disease differs from preventing coronary heart disease. Coronary microvascular disease affects the tiny coronary arteries; coronary heart disease affects the large coronary arteries.
Taking action to control risk factors for heart disease can help prevent or delay coronary heart disease. You can’t control some risk factors, such as older age and family history of heart disease. However, you can take steps to prevent or control other risk factors, such as high blood pressure, overweight and obesity, high blood cholesterol, diabetes, and smoking.
Heart-healthy lifestyle changes and ongoing medical care can help you lower your risk for heart disease.
Heart-Healthy Lifestyle Changes
Your doctor may recommend heart-healthy lifestyle changes if you have coronary microvascular disease. Heart-healthy lifestyle changes include:
- Heart-healthy eating
- Maintaining a healthy weight
- Managing stress
- Physical activity
- Quit smoking
Heart-Healthy Eating
Your doctor may recommend a heart-healthy eating plan, which should include:
- Fat-free or low-fat dairy products, such as skim milk
- Fish high in omega-3 fatty acids, such as salmon, tuna, and trout, about twice a week
- Fruits, such as apples, bananas, oranges, pears, and prunes
- Legumes, such as kidney beans, lentils, chickpeas, black-eyed peas, and lima beans
- Vegetables, such as broccoli, cabbage, and carrots
- Whole grains, such as oatmeal, brown rice, and corn tortillas.
When following a heart-healthy diet, you should avoid eating:
- A lot of red meat
- Palm and coconut oils
- Sugary foods and beverages
Two nutrients in your diet make blood cholesterol levels rise:
- Saturated fat—found mostly in foods that come from animals
- Trans fat (trans fatty acids)—found in foods made with hydrogenated oils and fats, such as stick margarine; baked goods, such as cookies, cakes, and pies; crackers; frostings; and coffee creamers. Some trans fats also occur naturally in animal fats and meats.
Saturated fat raises your blood cholesterol more than anything else in your diet. When you follow a heart-healthy eating plan, only 5 percent to 6 percent of your daily calories should come from saturated fat. Food labels list the amounts of saturated fat.
Not all fats are bad. Monounsaturated and polyunsaturated fats actually help lower blood cholesterol levels.
Some sources of monounsaturated and polyunsaturated fats are:
- Avocados
- Corn, sunflower, and soybean oils
- Nuts and seeds, such as walnuts
- Olive, canola, peanut, safflower, and sesame oils
- Peanut butter
- Salmon and trout
- Tofu
Sodium (salt)
You should try to limit the amount of sodium that you eat. This means choosing and preparing foods that are lower in salt and sodium. Try to use low-sodium and “no added salt” foods and seasonings at the table or while cooking. Food labels tell you what you need to know about choosing foods that are lower in sodium. Try to eat no more than 2,300 milligrams of sodium a day. If you have high blood pressure, you may need to restrict your sodium intake even more.
Dietary Approaches to Stop Hypertension
Your doctor may recommend the Dietary Approaches to Stop Hypertension (DASH) eating plan if you have high blood pressure. The Dietary Approaches to Stop Hypertension (DASH) eating plan focuses on fruits, vegetables, whole grains, and other foods that are heart healthy and low in fat, cholesterol, and sodium and salt.
The Dietary Approaches to Stop Hypertension (DASH) eating plan is a good heart-healthy eating plan, even for those who don’t have high blood pressure. Read more about Dietary Approaches to Stop Hypertension (DASH) by going to What is the DASH Diet ?.
Alcohol
Try to limit alcohol intake. Too much alcohol can raise your blood pressure and triglyceride levels, a type of fat found in the blood. Alcohol also adds extra calories, which may cause weight gain.
Men should have no more than two drinks containing alcohol a day. Women should have no more than one drink containing alcohol a day. One drink is:
- 12 ounces of beer
- 5 ounces of wine
- 1½ ounces of liquor
Maintaining a Healthy Weight
Maintaining a healthy weight is important for overall health and can lower your risk for coronary heart disease. Aim for a Healthy Weight by following a heart-healthy eating plan and keeping physically active.
Knowing your body mass index (BMI) helps you find out if you’re a healthy weight in relation to your height and gives an estimate of your total body fat. To figure out your body mass index (BMI), you can use a FREE online BMI calculators from the Centers for Disease Control and Prevention (CDC) :
- Adults (https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html)
For children and adolescents (younger than 20 years of age), overweight and obesity are based on the Centers for Disease Control and Prevention’s (CDC’s) BMI-for-age growth charts, which are available at 16.
The CDC has a BMI percentile calculator for children and teens at 54.
Body Mass Index for Men and Women Adults
The body mass index is an attempt to quantify the amount of tissue mass (muscle, fat, and bone) in an individual, and then categorize that person as underweight, normal weight, overweight, or obese based on that value. Commonly accepted body mass index ranges are:
- A) Underweight: under 18.5 kg/m2,
- B) Normal weight: 18.5 to 25 kg/m2,
- C) Overweight: 25 to 30 kg/m2,
- D) Obese: over 30 to 39.9 kg/m2.
- E) Severely Obese: over 40 kg/m2.
A general goal to aim for is a BMI below 25 kg/m2. Your doctor or health care provider can help you set an appropriate BMI goal.
Measuring waist circumference helps screen for possible health risks. If most of your fat is around your waist rather than at your hips, you’re at a higher risk for heart disease and type 2 diabetes. This risk may be high with a waist size that is greater than 35 inches for women or greater than 40 inches for men. To learn how to measure your waist, visit Waist Hip Ratio.
If you’re overweight or obese, try to lose weight. A loss of just 3 percent to 5 percent of your current weight can lower your triglycerides, blood glucose, and the risk of developing type 2 diabetes. Greater amounts of weight loss can improve blood pressure readings, lower LDL cholesterol, and increase HDL cholesterol.
Managing Stress
Research shows that the most commonly reported “trigger” for a heart attack is an emotionally upsetting event—particularly one involving anger. Also, some of the ways people cope with stress—such as drinking, smoking, or overeating—aren’t healthy.
Learning how to manage stress, relax, and cope with problems can improve your emotional and physical health. Consider healthy stress-reducing activities, such as:
- A stress management program
- Meditation
- Physical activity
- Relaxation therapy
- Talking things out with friends or family
Physical Activity
Routine physical activity can lower many coronary heart disease risk factors, including LDL (“bad”) cholesterol, high blood pressure, and excess weight. Physical activity also can lower your risk for diabetes and raise your HDL cholesterol level. HDL is the “good” cholesterol that helps prevent coronary heart disease.
Everyone should try to participate in moderate-intensity aerobic exercise at least 2 hours and 30 minutes per week, or vigorous aerobic exercise for 1 hour and 15 minutes per week. Aerobic exercise, such as brisk walking, is any exercise in which your heart beats faster and you use more oxygen than usual. The more active you are, the more you will benefit. Participate in aerobic exercise for at least 10 minutes at a time spread throughout the week.
Read more about physical activity at:
Talk with your doctor before you start a new exercise plan. Ask your doctor how much and what kinds of physical activity are safe for you.
Quitting Smoking
If you smoke, quit. Smoking can raise your risk for coronary heart disease and heart attack and worsen other coronary heart disease risk factors. Talk with your doctor about programs and products that can help you quit smoking. Also, try to avoid secondhand smoke.
If you have trouble quitting smoking on your own, consider joining a support group. Many hospitals, workplaces, and community groups offer classes to help people quit smoking.
Read more about quitting smoking at Smoking and Your Heart 55.
Ongoing Medical Care
Learn more about heart disease and the traits, conditions, and habits that can raise your risk for developing it. Talk with your doctor about your risk factors for heart disease and how to control them.
If lifestyle changes aren’t enough, your doctor may prescribe medicines to control your risk factors. Take all of your medicines as your doctor advises. Visit your doctor regularly and have recommended testing.
Know your numbers. Ask your doctor for these three tests and have the results explained to you:
- Blood pressure measurement.
- Fasting blood glucose. This test is for diabetes.
- Lipoprotein panel. This test measures total cholesterol, LDL (“bad”) cholesterol, HDL (“good”) cholesterol, and triglycerides (a type of fat in the blood).
Finally, know your family history of heart disease. If you or someone in your family has heart disease, tell your doctor.
Outlook for coronary microvascular disease
Most of what is known about coronary microvascular disease comes from the National Heart, Lung, and Blood Institute’s Women’s Ischemia Syndrome Evaluation.
Currently, research is ongoing to learn more about the role of hormones in heart disease and to find better ways to diagnose coronary coronary microvascular disease.
Studies also are under way to learn more about the causes of coronary microvascular disease, how to treat the disease, and the expected health outcomes for people with coronary microvascular disease.
What are the Signs and Symptoms of Coronary Microvascular Disease?
The signs and symptoms of coronary microvascular disease often differ from the signs and symptoms of traditional coronary heart disease (CHD). Many women with coronary microvascular disease have angina. Angina is chest pain or discomfort that occurs when your heart muscle doesn’t get enough oxygen-rich blood. Angina may feel like pressure or squeezing in your chest. You also may feel it in your shoulders, arms, neck, jaw, or back. Angina pain may even feel like indigestion.
Angina also is a common symptom of coronary heart disease. However, the angina that occurs in coronary microvascular disease may differ from the typical angina that occurs in coronary heart disease 56. In coronary microvascular disease, the chest pain usually lasts longer than 10 minutes, and it can last longer than 30 minutes. Typical angina is more common in women older than 65 56.
Other signs and symptoms of coronary microvascular disease are shortness of breath, sleep problems, fatigue (tiredness), and lack of energy 56.
Coronary microvascular disease symptoms often are first noticed during routine daily activities (such as shopping, cooking, cleaning, and going to work) and times of mental stress. It’s less likely that women will notice these symptoms during physical activity (such as jogging or walking fast) 56.
This differs from coronary heart disease, in which symptoms often first appear while a person is being physically active—such as while jogging, walking on a treadmill, or going up stairs.
How is Coronary Microvascular Disease Diagnosed?
Your doctor will diagnose coronary microvascular disease based on your medical history, a physical exam, and test results. He or she will check to see whether you have any risk factors for heart disease.
For example, your doctor may measure your weight and height to check for overweight or obesity. He or she also may recommend tests for high blood cholesterol, metabolic syndrome, and diabetes.
Your doctor may ask you to describe any chest pain, including when it started and how it changed during physical activity or periods of stress. He or she also may ask about other symptoms, such as fatigue (tiredness), lack of energy, and shortness of breath. Women may be asked about their menopausal status.
Specialists Involved
Cardiologists and doctors who specialize in family and internal medicine might help diagnose and treat coronary microvascular disease. Cardiologists are doctors who specialize in diagnosing and treating heart diseases and conditions.
Diagnostic Tests
The risk factors for coronary microvascular disease and traditional coronary heart disease often are the same 57. Thus, your doctor may recommend tests for coronary heart disease, such as:
- Coronary angiography. This test uses dye and special x-rays to show the insides of your coronary arteries. Coronary angiography can show plaque buildup in the large coronary arteries. This test often is done during a heart attack to help find blockages in the coronary arteries.
- Stress testing. This test shows how blood flows through your heart during physical stress, such as exercise. Even if coronary angiography doesn’t show plaque buildup in the large coronary arteries, a stress test may still show abnormal blood flow. This may be a sign of coronary microvascular disease.
- Cardiac MRI (magnetic resonance imaging) stress test. Doctors may use this test to evaluate people who have chest pain.
Unfortunately, standard tests for coronary heart disease aren’t designed to detect coronary microvascular disease. These tests look for blockages in the large coronary arteries. Coronary microvascular disease affects the tiny coronary arteries.
If test results show that you don’t have coronary heart disease, your doctor might still diagnose you with coronary microvascular disease. This could happen if signs are present that not enough oxygen is reaching your heart’s tiny arteries.
Coronary microvascular disease symptoms often first occur during routine daily tasks. Thus, your doctor may ask you to fill out a questionnaire called the Duke Activity Status Index. The questionnaire will ask you how well you’re able to do daily activities, such as shopping, cooking, and going to work.
The Duke Activity Status Index results will help your doctor decide which kind of stress test you should have. The results also give your doctor information about how well blood is flowing through your coronary arteries.
Your doctor also may recommend blood tests, including a test for anemia. Anemia is thought to slow the growth of cells needed to repair damaged blood vessels.
Research is ongoing for better ways to detect and diagnose coronary microvascular disease. Currently, researchers have not agreed on the best way to diagnose the disease.
How is Coronary Microvascular Disease Treated?
Relieving pain is one of the main goals of treating coronary microvascular disease. Treatments also are used to control risk factors and other symptoms.
Treatments may include medicines 58, such as:
- ACE inhibitors and beta blockers to lower blood pressure and decrease the heart’s workload
- Aspirin to help prevent blood clots or control inflammation
- Nitroglycerin to relax blood vessels, improve blood flow to the heart muscle, and treat chest pain
- Statin medicines to control or lower your blood cholesterol.
Take all medicines regularly, as your doctor prescribes. Don’t change the amount of your medicine or skip a dose unless your doctor tells you to.
If you’re diagnosed with coronary microvascular disease and also have anemia, you may benefit from treatment for that condition. Anemia is thought to slow the growth of cells needed to repair damaged blood vessels.
If you’re diagnosed with and treated for coronary microvascular disease, you should get ongoing care from your doctor. Research is under way to find the best treatments for coronary microvascular disease.
What is an arrhythmia?
An arrhythmia is a problem with the rate or rhythm of the heartbeat. During an arrhythmia, the heart can beat too fast, too slow, or with an irregular rhythm 59. When the heart doesn’t beat properly, it can’t pump blood effectively. When the heart doesn’t pump blood effectively, the lungs, brain and all other organs can’t work properly and may shut down or be damaged 60.
A heartbeat that is too fast is called tachycardia. A heartbeat that is too slow is called bradycardia.
Most arrhythmias are harmless, but some can be serious or even life threatening. During an arrhythmia, the heart may not be able to pump enough blood to the body. Lack of blood flow can damage the brain, heart, and other organs.
Understanding the Heart’s Electrical System
To understand arrhythmias, it helps to understand the heart’s internal electrical system. The heart’s electrical system controls the rate and rhythm of the heartbeat.
With each heartbeat, an electrical signal spreads from the top of the heart to the bottom. As the signal travels, it causes the heart to contract and pump blood.
Your heart’s electrical system controls all the events that occur when your heart pumps blood 61. The electrical system also is called the cardiac conduction system. If you’ve ever seen the heart test called an EKG (electrocardiogram), you’ve seen a graphical picture of the heart’s electrical activity.
Your heart’s electrical system is made up of three main parts:
- The Sinoatrial (SA) node, located in the right atrium of your heart
- The Atrioventricular (AV) node, located on the interatrial septum close to the tricuspid valve
- The His-Purkinje system, located along the walls of your heart’s ventricles
A heartbeat is a complex series of events. These events take place inside and around your heart. A heartbeat is a single cycle in which your heart’s chambers relax and contract to pump blood. This cycle includes the opening and closing of the inlet and outlet valves of the right and left ventricles of your heart.
Each heartbeat has two basic parts: diastole and systole. During diastole, the atria and ventricles of your heart relax and begin to fill with blood.
At the end of diastole, your heart’s atria contract (atrial systole) and pump blood into the ventricles. The atria then begin to relax. Your heart’s ventricles then contract (ventricular systole), pumping blood out of your heart.
Each electrical signal begins in a group of cells called the sinus node or sinoatrial (SA) node. The SA node is located in the heart’s upper right chamber, the right atrium. In a healthy adult heart at rest, the SA node fires off an electrical signal to begin a new heartbeat 60 to 100 times a minute. In a normal, healthy heart, each beat begins with a signal from the SA node. This is why the SA node sometimes is called your heart’s natural pacemaker. Your pulse, or heart rate, is the number of signals the SA node produces per minute.
The signal is generated as the vena cavae fill your heart’s right atrium with blood from other parts of your body. The signal spreads across the cells of your heart’s right and left atria.
From the SA node, the electrical signal travels through special pathways in the right and left atria. This causes the atria to contract and pump blood through the open valves from the atria into heart’s two lower chambers, the ventricles.
The electrical signal then moves down to a group of cells called the atrioventricular (AV) node, located between the atria and the ventricles. Here, the signal slows down just a little, allowing your heart’s right and left ventricles time to finish filling with blood.
The electrical signal then leaves the AV node and travels along a pathway called the bundle of His. This pathway divides into a right bundle branch and a left bundle branch. The signal goes down these branches to the ventricles, causing them to contract and pump blood to the lungs and the rest of the body.
From the bundle of His, the signal fibers divide into left and right bundle branches through the Purkinje fibers. These fibers connect directly to the cells in the walls of your heart’s left and right ventricles.
The signal spreads across the cells of your ventricle walls, and both ventricles contract. However, this doesn’t happen at exactly the same moment.
The left ventricle contracts an instant before the right ventricle. This pushes blood through the pulmonary valve (for the right ventricle) to your lungs, and through the aortic valve (for the left ventricle) to the rest of your body.
As the signal passes, the walls of the ventricles relax and await the next signal.
This process continues over and over as the atria refill with blood and more electrical signals come from the SA node.
A problem with any part of this process can cause an arrhythmia. For example, in atrial fibrillation, a common type of arrhythmia, electrical signals travel through the atria in a fast and disorganized way. This causes the atria to quiver instead of contract.
Figure 3. The heart’s electrical system

Outlook for arrhythmia
There are many types of arrhythmia. Most arrhythmias are harmless, but some are not. The outlook for a person who has an arrhythmia depends on the type and severity of the arrhythmia.
Even serious arrhythmias often can be successfully treated. Most people who have arrhythmias are able to live normal, healthy lives.
What is heart failure?
Heart failure is a condition in which the heart can’t pump enough blood to meet the body’s needs 62. In some cases, the heart can’t fill with enough blood. In other cases, the heart can’t pump blood to the rest of the body with enough force. Some people have both problems.
The term “heart failure” doesn’t mean that your heart has stopped or is about to stop working 62. However, heart failure is a serious condition that requires medical care.
Other Names for Heart Failure
- Congestive heart failure.
- Left-side heart failure. This is when the heart can’t pump enough oxygen-rich blood to the body.
- Right-side heart failure. This is when the heart can’t fill with enough blood.
- Cor pulmonale. This term refers to right-side heart failure caused by high blood pressure in the pulmonary arteries and right ventricle (lower right heart chamber).
Overview
Heart failure develops over time as the heart’s pumping action grows weaker. The condition can affect the right side of the heart only, or it can affect both sides of the heart. Most cases involve both sides of the heart.
Right-side heart failure occurs if the heart can’t pump enough blood to the lungs to pick up oxygen. Left-side heart failure occurs if the heart can’t pump enough oxygen-rich blood to the rest of the body.
Right-side heart failure may cause fluid to build up in the feet, ankles, legs, liver, abdomen, and the veins in the neck. Right-side and left-side heart failure also may cause shortness of breath and fatigue (tiredness).
The leading causes of heart failure are diseases that damage the heart. Examples include coronary heart disease, high blood pressure, and diabetes.
Outlook
Heart failure is a very common condition. About 5.7 million people in the United States have heart failure 62. Both children and adults can have the condition, although the symptoms and treatments differ 62.
Currently, heart failure has no cure 62. However, treatments—such as medicines and lifestyle changes—can help people who have the condition live longer and more active lives. Researchers continue to study new ways to treat heart failure and its complications.
References- National Institutes of Health. National Heart, Lung and Blood Institute. Heart Attack. https://www.nhlbi.nih.gov/health/health-topics/topics/heartattack
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, et al. Heart Disease and Stroke Statistics—2017 Update: A Report From the American Heart Association. 2017; 135:e1–e458. DOI: 10.1161/CIR.0000000000000485.
- Zheng ZJ, Croft JB, Giles WH, Ayala CI, Greenlund KJ, Keenan NL, Neff L, Wattigney WA, Mensah GA. State Specific Mortality from Sudden Cardiac Death: United States, 1999. MMWR 2002;51(6):123–126. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5106a3.htm
- National Institutes of Health. National Heart, Lung and Blood Institute. What Causes a Heart Attack ? https://www.nhlbi.nih.gov/health/health-topics/topics/heartattack/causes
- National Institutes of Health. National Heart, Lung and Blood Institute. Who Is at Risk for a Heart Attack ? https://www.nhlbi.nih.gov/health/health-topics/topics/heartattack/risks
- Lloyd-Jones DM, Hong Y, Labarthe D, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation. 2010;121:586-613. http://circ.ahajournals.org/content/121/4/586.long
- Kenfield SA, Stampfer MJ, Rosner BA, Colditz GA. Smoking and smoking cessation in relation to mortality in women. JAMA. 2008;299:2037-47. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2879642/
- Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, Giles WH, Capewell S. Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. N Engl J Med. 2007; 356: 2388–2398. http://www.nejm.org/doi/full/10.1056/NEJMsa053935
- National Center for Chronic Disease Prevention and Health Promotion. Smoking & Tobacco Use – How to Quit. https://www.cdc.gov/tobacco/quit_smoking/how_to_quit/quit_tips/index.htm
- Willett WC, Manson JE, Stampfer MJ, et al. Weight, weight change, and coronary heart disease in women. Risk within the ‘normal’ weight range. JAMA. 1995;273:461-5. https://www.ncbi.nlm.nih.gov/pubmed/7654270
- Bogers RP, Bemelmans WJ, Hoogenveen RT, et al. Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21 cohort studies including more than 300 000 persons. Archives of internal medicine. 2007;167:1720-8. https://www.ncbi.nlm.nih.gov/pubmed/17846390
- Berrington de Gonzalez A, Hartge P, Cerhan JR, et al. Body-mass index and mortality among 1.46 million white adults. N Engl J Med. 2010;363:2211-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3066051/
- Canoy D, Cairns BJ, Balkwill A, et al. Body mass index and incident coronary heart disease in women: a population-based prospective study. BMC Med. 2013;11:87. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3661394/
- Rimm EB, Stampfer MJ, Giovannucci E, et al. Body size and fat distribution as predictors of coronary heart disease among middle-aged and older US men. American journal of epidemiology. 1995;141:1117-27. https://www.ncbi.nlm.nih.gov/pubmed/7771450
- Maclure KM, Hayes KC, Colditz GA, Stampfer MJ, Speizer FE, Willett WC. Weight, diet, and the risk of symptomatic gallstones in middle-aged women. N Engl J Med. 1989;321:563-9. https://www.ncbi.nlm.nih.gov/pubmed/2761600
- Centers for Disease Control and Prevention. CDC Clinical Growth Charts. https://www.cdc.gov/growthcharts/clinical_charts.htm
- Centers for Disease Control and Prevention. BMI Percentile Calculator for Child and Teen. https://www.cdc.gov/healthyweight/bmi/calculator.html
- Zhang C, Rexrode KM, van Dam RM, Li TY, Hu FB. Abdominal obesity and the risk of all-cause, cardiovascular, and cancer mortality: sixteen years of follow-up in US women. Circulation. 2008;117:1658-67. http://circ.ahajournals.org/content/117/13/1658.long
- National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. Bethesda, MD; 1998. https://www.nhlbi.nih.gov/health/health-topics/topics/obe
- Ford ES, Caspersen CJ. Sedentary behaviour and cardiovascular disease: a review of prospective studies. International journal of epidemiology. 2012;41:1338-53. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4582407/
- Matthews CE, George SM, Moore SC, et al. Amount of time spent in sedentary behaviors and cause-specific mortality in US adults. The American journal of clinical nutrition. 2012;95:437-45. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3260070/
- Chomistek AK, Manson JE, Stefanick ML, et al. Relationship of sedentary behavior and physical activity to incident cardiovascular disease: results from the Women’s Health Initiative. Journal of the American College of Cardiology. 2013;61:2346-54. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3676694/
- Dunstan DW, Barr EL, Healy GN, et al. Television viewing time and mortality: the Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Circulation. 2010;121:384-91. http://circ.ahajournals.org/content/121/3/384.long
- Patel AV, Bernstein L, Deka A, et al. Leisure time spent sitting in relation to total mortality in a prospective cohort of US adults. American journal of epidemiology. 2010;172:419-29. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3590043/
- Warren TY, Barry V, Hooker SP, Sui X, Church TS, Blair SN. Sedentary behaviors increase risk of cardiovascular disease mortality in men. Med Sci Sports Exerc. 2010;42:879-85. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2857522/
- Chiuve SE, Fung TT, Rimm EB, et al. Alternative dietary indices both strongly predict risk of chronic disease. The Journal of nutrition. 2012;142:1009-18. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3738221/
- Estruch, R., et al., Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med, 2013. 368(14): p. 1279-90.
- Stamler R. Implications of the INTERSALT study. Hypertension. 1991; 17 (suppl): I16–I20. https://www.ncbi.nlm.nih.gov/pubmed/1986996
- US Department of Health and Human Services and US Department of Agriculture. Dietary Guidelines for Americans, 2005. 6th ed. Washington, DC: US Government Printing Office; 2005.
- Johnson RK, Appel LJ, Brands M, Howard BV, Lefevre M, Lustig RH, Sacks F, Steffen LM, Wylie-Rosett J; on behalf of the American Heart Association Nutrition Committee of the Council on Nutrition, Physical Activity, and Metabolism and the Council on Epidemiology and Prevention. Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation. 2009; 120: 1011–1020. http://circ.ahajournals.org/content/120/11/1011
- Dowse GK, Gareebo H, Alberti KG, Zimmet P, Tuomilehto J, Purran A, Fareed D, Chitson P, Collins VR. Changes in population cholesterol concentrations and other cardiovascular risk factor levels after five years of the Non-communicable Disease Intervention Programme in Mauritius. BMJ. 1995; 311: 1255–1259. http://www.bmj.com/content/311/7015/1255
- http://www.bmj.com/content/313/7064/1044
- Chiuve SE, Rexrode KM, D. S, Logroscino G, Manson JE, Rimm EB. Primary prevention of stroke by healthy lifestyle. Circulation. 2008;118:947-54. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2730914/
- Chiuve SE, Fung TT, Rexrode KM, et al. Adherence to a low-risk, healthy lifestyle and risk of sudden cardiac death among women. JAMA. 2011;306:62-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3210472/
- van Dam RM, Li T, Spiegelman D, Franco OH, Hu FB. Combined impact of lifestyle factors on mortality: prospective cohort study in US women. BMJ. 2008;337:a1440. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2658866/
- National Institutes of Health. National Heart, Lung and Blood Institute. What Are the Symptoms of a Heart Attack ? https://www.nhlbi.nih.gov/health/health-topics/topics/heartattack/signs
- National Institutes of Health. National Heart, Lung and Blood Institute. How Is a Heart Attack Diagnosed ? https://www.nhlbi.nih.gov/health/health-topics/topics/heartattack/diagnosis
- National Institutes of Health. National Heart, Lung and Blood Institute. How Is a Heart Attack Treated ? https://www.nhlbi.nih.gov/health/health-topics/topics/heartattack/treatment
- National Institutes of Health. National Heart, Lung and Blood Institute. Life After a Heart Attack. https://www.nhlbi.nih.gov/health/health-topics/topics/heartattack/lifeafter
- National Institutes of Health. National Heart, Lung and Blood Institute. Coronary Heart Disease. https://www.nhlbi.nih.gov/health/health-topics/topics/cad
- National Institutes of Health. National Heart, Lung and Blood Institute. Angina. https://www.nhlbi.nih.gov/health/health-topics/topics/angina
- National Institutes of Health. National Heart, Lung and Blood Institute. Who Is at Risk for Angina ? https://www.nhlbi.nih.gov/health/health-topics/topics/angina/atrisk
- National Institutes of Health. National Heart, Lung and Blood Institute. What Are the Signs and Symptoms of Angina ? https://www.nhlbi.nih.gov/health/health-topics/topics/angina/signs
- National Institutes of Health. National Heart, Lung and Blood Institute. What Causes Angina ? https://www.nhlbi.nih.gov/health/health-topics/topics/angina/causes
- National Institutes of Health. National Heart, Lung and Blood Institute. How Can Angina Be Prevented ? https://www.nhlbi.nih.gov/health/health-topics/topics/angina/prevention
- National Institutes of Health. National Heart, Lung and Blood Institute. How Is Angina Diagnosed ? https://www.nhlbi.nih.gov/health/health-topics/topics/angina/diagnosis
- National Institutes of Health. National Heart, Lung and Blood Institute. How Is Angina Treated ? https://www.nhlbi.nih.gov/health/health-topics/topics/angina/treatment
- National Institutes of Health. National Heart, Lung and Blood Institute. Living With Angina. https://www.nhlbi.nih.gov/health/health-topics/topics/angina/livingwith
- National Institutes of Health. National Heart, Lung and Blood Institute. Coronary Microvascular Disease. https://www.nhlbi.nih.gov/health/health-topics/topics/cmd
- National Institutes of Health. National Heart, Lung and Blood Institute. Who Is at Risk for Coronary Microvascular Disease ? https://www.nhlbi.nih.gov/health/health-topics/topics/cmd/risk
- National Institutes of Health. National Heart, Lung and Blood Institute. Living With Coronary Microvascular Disease. https://www.nhlbi.nih.gov/health/health-topics/topics/cmd/livingwith
- National Institutes of Health. National Heart, Lung and Blood Institute. What Causes Coronary Microvascular Disease ? https://www.nhlbi.nih.gov/health/health-topics/topics/cmd/causes
- National Institutes of Health. National Heart, Lung and Blood Institute. How Can Coronary Microvascular Disease Be Prevented ? https://www.nhlbi.nih.gov/health/health-topics/topics/cmd/prevention
- Centers for Disease Control and Prevention. BMI Percentile Calculator for Child and Teen. https://nccd.cdc.gov/dnpabmi/Calculator.aspx
- National Institutes of Health. National Heart, Lung and Blood Institute. Smoking and Your Heart. https://www.nhlbi.nih.gov/health/health-topics/topics/smo/
- National Institutes of Health. National Heart, Lung and Blood Institute. What Are the Signs and Symptoms of Coronary Microvascular Disease ? https://www.nhlbi.nih.gov/health/health-topics/topics/cmd/signs
- National Institutes of Health. National Heart, Lung and Blood Institute. How Is Coronary Microvascular Disease Diagnosed ? https://www.nhlbi.nih.gov/health/health-topics/topics/cmd/diagnosis
- National Institutes of Health. National Heart, Lung and Blood Institute. How Is Coronary Microvascular Disease Treated ? https://www.nhlbi.nih.gov/health/health-topics/topics/cmd/treatment
- National Institutes of Health. National Heart, Lung and Blood Institute. Arrhythmia. https://www.nhlbi.nih.gov/health/health-topics/topics/arr
- American Heart Association. About Arrhythmia. http://www.heart.org/HEARTORG/Conditions/Arrhythmia/AboutArrhythmia/About-Arrhythmia_UCM_002010_Article.jsp
- National Institutes of Health. National Heart, Lung and Blood Institute. Your Heart’s Electrical System. https://www.nhlbi.nih.gov/health/health-topics/topics/hhw/electrical
- National Institutes of Health. National Heart, Lung and Blood Institute. Heart Failure. https://www.nhlbi.nih.gov/health/health-topics/topics/hf





{kind=link}