What is a surgical suture
Sutures are little stitches that hold the edges of a wound together while the skin heals. Sutures could be made of natural materials such as silk, or synthetic materials such as nylon. Stitching, or suturing, is the most common form of repairing a wound. Other methods include surgical staples, skin closure tapes, and adhesives.
Sutures hold a wound or cut closed so that it can heal. When the cut is healed, the sutures have done their job and are removed (some types of suture will automatically dissolve). Taking good care of the sutures will help the wound heal cleanly and minimize scarring.
Sutures can be used in nearly every part of the body, internally and externally. Doctors literally “sew” the skin together with individual sutures and tie a secure knot. Sutures then allow the skin to heal naturally when it otherwise may not come together. Sutures are used to close a variety of wound types. Accidental cuts or lacerations are often closed with stitches. Also, surgeons use sutures during operations to tie ends of bleeding blood vessels and to close surgical incisions.
Effective suturing technique depends on appropriate selection of sutures, surgical gloves, needles, and needle holders.
Sutures vs Stitches
Stitches are also called sutures and are used to close cuts and wounds in skin. A suture is a stitch or a row of stitches holding together the edges of a wound or surgical incision. Sutures can sometimes be called stitches.
How do doctors decide whether to use stitches?
How and when the wound occurred gives the doctor some idea as to what to expect for potential complications and plan what to do. Animal bites have a high risk of infection, and human bite wounds almost always get infected. The infection rate is so high, that unless the cosmetic benefit overrides that infection risk, most animal bites are anesthetized, explored, washed out, and not sutured. The closed skin would act like a potential abscess: dark, warm, and inviting bacteria to thrive in that situation. The balancing act between good scar and good outcome is one that the doctor decides before a laceration is repaired. Usually, it’s only on the face where cosmetic concerns win out and shift the balance.
Whether Dermabond (the skin glue) or sutures are used for skin closure, the wound still needs to be explored and cleaned. This usually requires anesthetic to accomplish regardless of the method of skin closure. The local anesthetic used (usually lidocaine) can be warmed and buffered so that its injection causes minimal discomfort, and with skill, suturing a wound should not be painful. The expectation of pain and the fear of stitches is no longer reality. Wound repair should not be the painful experience it may have been a generation ago.
Types of sutures
Sutures are divided into two general categories, namely, absorbable and nonabsorbable:
- Regular (non-absorbable) sutures – a non-absorbable suture resists the body’s attempt to dissolve it. Nonabsorbable sutures, on the other hand, maintain their strength for longer than 60 days. Non-absorbable sutures are used to close skin, external wounds, or to repair blood vessels, for example. Non-absorbable sutures may be removed by a surgeon after a surface incision has healed.
- Dissolvable sutures (absorbable sutures) – these are absorbed by the body naturally and don’t need to be removed; they are very useful when stitches are needed under the skin’s surface. Absorbable sutures rapidly break down in the tissues and lose their strength within 60 days.
Table 1. Absorbable Suture Materials
| Material | Structure | Strength | T ½ | Uses |
| Gut | Natural | ++ | 5-7 days | Mucosal closure, rare |
| Chromic Gut | Natural | ++ | 10-14 days | Mucosa, perineal |
| Dexon | Braided | +++ | 25 days | Subcuticular closures |
| Vicryl | Braided | ++++ | 28 days | Mucosal closures |
| Maxon | Monofilament | +++++ | 28-36 days | Subcuticular closures |
Table 2. Non-absorbable Suture Materials
| Material | Structure | Strength | Knot security | Uses |
| Silk | Braided | ++ | ++++ | Easy to handle |
| Nylon | Monofilament | +++ | ++ | Common for skin closure |
| Prolene | Monofilament | ++++ | + | High memory, subcuticular pull |
| Dacron | Braided | ++ | ++++ | Good knot security |
Sutures are made from both man-made and natural materials. Natural suture materials include silk, linen, and catgut, which is actually the dried and treated intestine of a cow or sheep. Synthetic sutures are made from a variety of textiles such as nylon or polyester, formulated specifically for surgical use. Absorbable synthetic sutures are made from polyglycolic acid or other glycolide polymers. Most of the synthetic suture materials have proprietary names, such as Dexon and Vicryl. The water-resistant material Goretex has been used for surgical sutures, and other sutures are made from thin metal wire.
Sutures are also classified according to their form. Some are monofilaments, that is, consisting of only one thread-like structure. Others consist of several filaments braided or twisted together. Surgeons choose which type of suture to use depending on the operation. A monofilament has what is called low tissue drag, meaning it passes smoothly through tissue. Braided or twisted sutures may have higher tissue drag, but are easier to knot and have greater knot strength. Braided sutures are usually coated to improve tissue drag. Other sutures may have a braided or twisted core within a smooth sleeve of extruded material. These are known as pseudo-monofilaments. A suture can also be classified according to its diameter.
Wounds or cuts can also be held together in other ways such as:
- A special glue for skin, which falls off of its own accord in a few weeks. This material is applied to the edges of the wound somewhat like glue and should keep the edges of the wound together until healing occurs. Adhesive glue is the newest method of wound repair and is becoming a popular alternative to stitches, especially for children. The adhesive simply falls off or wears away after about 5-7 days.
- Adhesive tape (such as steri-strips), which also falls off naturally. Skin closure tapes, also known as adhesive strips, have recently gained popularity. The advantages of skin closure tapes are plenty. The rate of wound infection is less with adhesive strips than with stitches. Also, it takes less time to apply skin closure tape. For many people, there is no need for a painful injection of anesthetic when using skin closure tapes. Disadvantages of using skin closure tapes include less precision in bringing wound edges together than suturing. Not all areas of the body can be taped. For example, body areas with secretions such as the armpits, palms, or soles are difficult areas to place adhesive strips. Areas with hair also would not be suitable for taping.
- Metal staples, which must be removed by a doctor or nurse. Surgical staples are useful for closing many types of wounds. Staples have the advantage of being quicker and may cause fewer infections than stitches. Disadvantages of staples are permanent scars if used inappropriately and imperfect aligning of the wound edges, which can lead to improper healing. Staples are used on scalp lacerations and commonly used to close surgical wounds.
Suture sizes
In the United States, suture diameter is represented on a scale descending from 10 to 1, and then descending again from 1-0 to 12-0. A number 9 suture is 0.0012 in (0.03 mm) in diameter, while the smallest, number 12-0, is smaller in diameter than a human hair.
Suture selection
Much of the process surrounding suture selection depends on surgeon training and preference. A wide variety of suture materials are available for each surgical location and surgical requirement. Generally, the surgeon selects the smallest suture that adequately holds the healing wound edges. The tensile strength of the suture should never exceed the tensile strength of the tissue. As the wound heals, the relative loss of suture strength over time should be slower than the gain of tissue tensile strength.
Certain general principles can be applied to suture selection. Sutures are no longer needed when a wound has reached maximum strength. Therefore, nonabsorbable suture should be considered in skin, fascia, and tendons (slowly healing tissues), whereas mucosal wounds (rapidly healing tissues) may be closed with absorbable sutures.
Aesthetic concerns are at a premium in regions of the head and neck such as the eyelid, periorbital area, nose, pinna, lip, and vermillion. In these areas, tensile strength requirements tend to be less, and smaller suture sizes are preferred. However, the mobility of the lip and vermillion requires a relatively higher suture tensile strength.
The activity and mobility of the face, anterior and posterior neck, scalp, superior trunk, and nasal and oral mucosa demand higher tensile strength requirements in suture selection. Additionally, major musculocutaneous flaps tend to be closed under significant tension, requiring maximal long-term tensile strength.
Because the presence of foreign bodies in contaminated tissues may facilitate infection, special consideration of suture selection in these locations (eg, a contaminated posttraumatic wound) is imperative. Multifilament sutures are more likely to harbor contaminants than monofilament sutures are; accordingly, monofilament sutures are generally preferable in potentially contaminated tissues. The smallest inert monofilament suture materials (e.g., nylon or polypropylene) should be sued in this setting.
The optimal suture size is generally the smallest size that can still effectively achieve the desired tension-free closure. If wound tension is high, smaller-diameter sutures may actually injure tissues by cutting through them. Therefore, the tensile strength of the suture and that of the tissue should be closely matched.
Table 3. Suture sizing by indication
| Location | Superficial non-absorbable suture | Deep absorbable suture |
| Scalp, torso (chest, back, abdomen), extremities | 3-0 to 5-0 | 3-0 or 4-0 |
| Face, eyebrow, nose, lip | 6-0 | 5-0 |
| Ear, eyelid | 6-0 | n/a |
| Hand* | 4-0 or 5-0 | 5-0 |
| Foot or sole* | 3-0 or 4-0 | 4-0 |
| Penis | 5-0 or 6-0 | n/a |
Footnote: * deep sutures are to be avoided in the hands and feet unless being used to repair a tendon – they may increase the risk of wound infection.
[Source 1 ]Needle selection
No standardized sizing system or nomenclature is available for needles. The main consideration in needle selection is to minimize trauma. A taper-point needle is sufficient for tissues that are easy to penetrate. Cutting needles are typically reserved for tough tissues. As a general rule, taper-point needles may be used for all closures except skin sutures. The length, diameter, and curvature of the needle influence the surgeon’s ability to place a suture. Ideally, the needle-body diameter matches the suture size.
How to suture
Wound Cleaning and Irrigation
Wearing eye protection, inspect wound for foreign bodies. Place chucks under the wound to collect drainage. Flush wound with copious amounts of normal saline. This can be done with a 30-60cc syringe with an 18g needle, IV bag with adapter, or special irrigation apparatus. Use a high pressure, direct stream in all areas of the wound. Avoid high pressure, however, on delicate tissues, such as the eye lids. A good rule of thumb is 100cc per 1cm of wound length. Once irrigated, switch to sterile gloves and cover the area with a sterile fenestrated drape. Explore the wound to assess the depth and presence of foreign bodies.
Anesthetization
Clean the area to be anesthetized with chlorhexidine or 1% betadine solution. Choose the appropriate anesthetic (for most cases this will be 1% lidocaine with or without epi). To buffer lidocaine, add bicarbonate to the solution in a 10:1 ratio. To buffer bupivacaine, add bicarbonate to the solution in a 30:1 ratio. Use bupivacaine for longer procedures, and mix with lidocaine for both rapid onset and longer duration. Draw up anesthetic in a 10cc syringe with an 18g needle. Change to 25g or 30g needle and remove all the air. Insert needle into subcutaneous tissue from within the wound margins and make a wheel under the skin. Continue along the entire wound margin to be repaired. Use plenty of anesthetic!
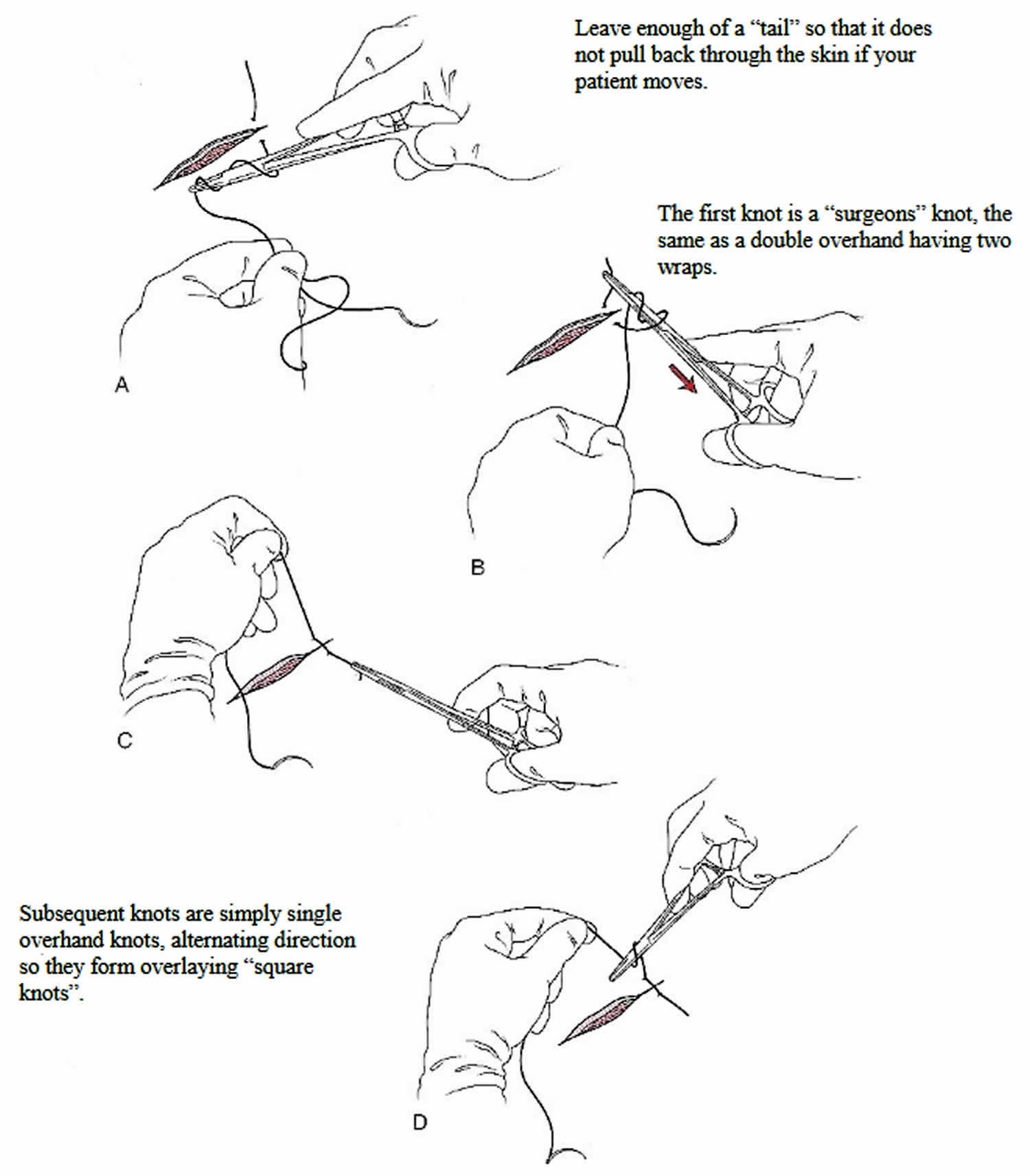
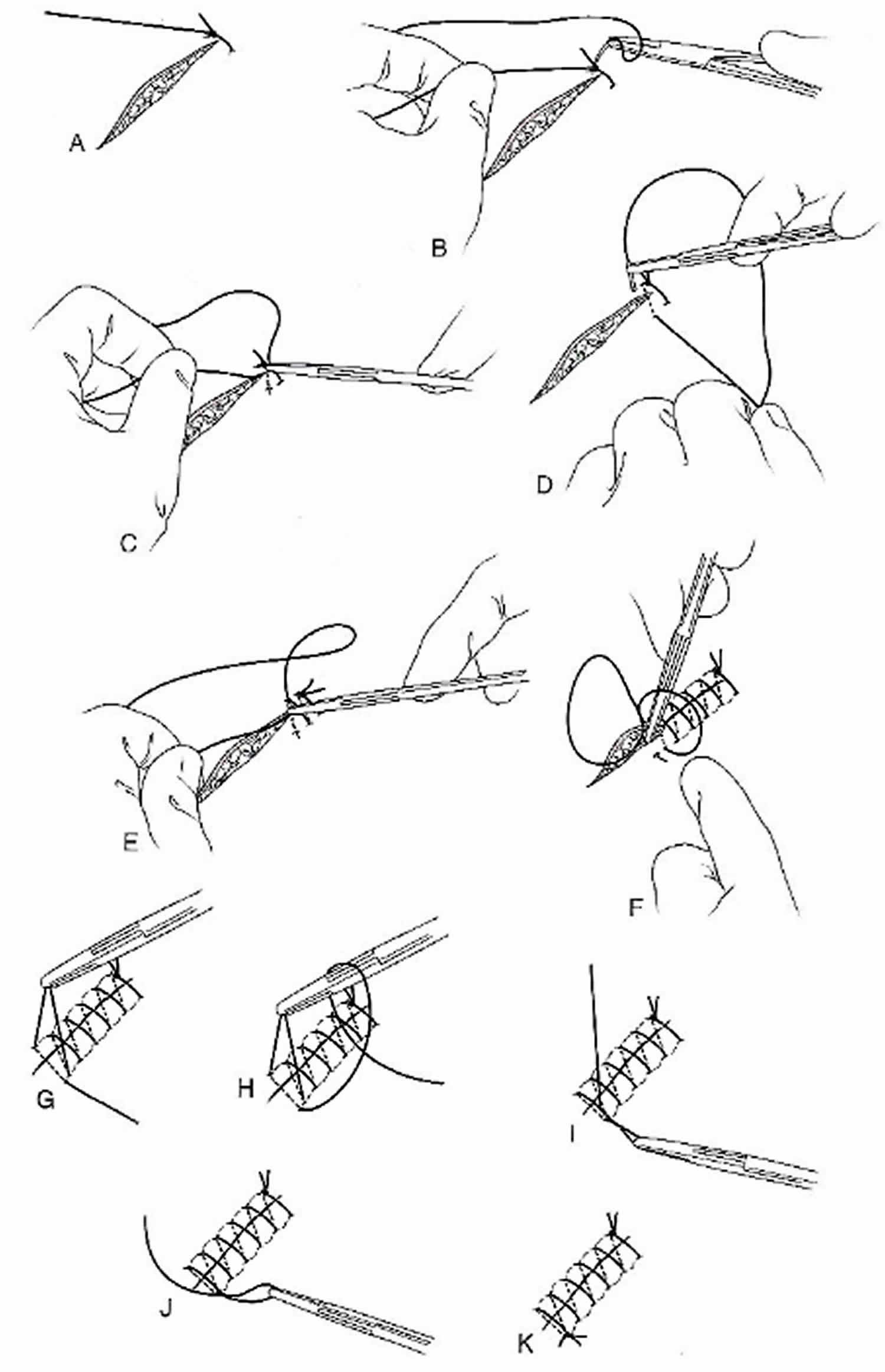
The general technique of placing stitches is simple. The “thread” or suture that is used is attached to a needle.
Then the needle with the thread attached is used to “sew” the edges of the wound together, in an effort to recreate the original appearance. Several stitches may be needed to accomplish this. Once the wound is closed a topical antibiotic gel is often spread over the stitches and a bandage is initially applied to the wound. All sutured wounds that require stitches will have scar formation, but the scarring is usually minimal.
Basic Suturing Techniques
Be sure to place the needle to 90 degrees at the skin margin and rotate the needle through its arc while in the skin. On the opposite wound edge, be sure to run the needle though a symmetrical tract. This will insure level wound edge approximation. Failure to do so can result in worse approximation leading to poor wound healing and scarring. To facilitate this, keep the fingers free of the islet holes in the needle drivers.
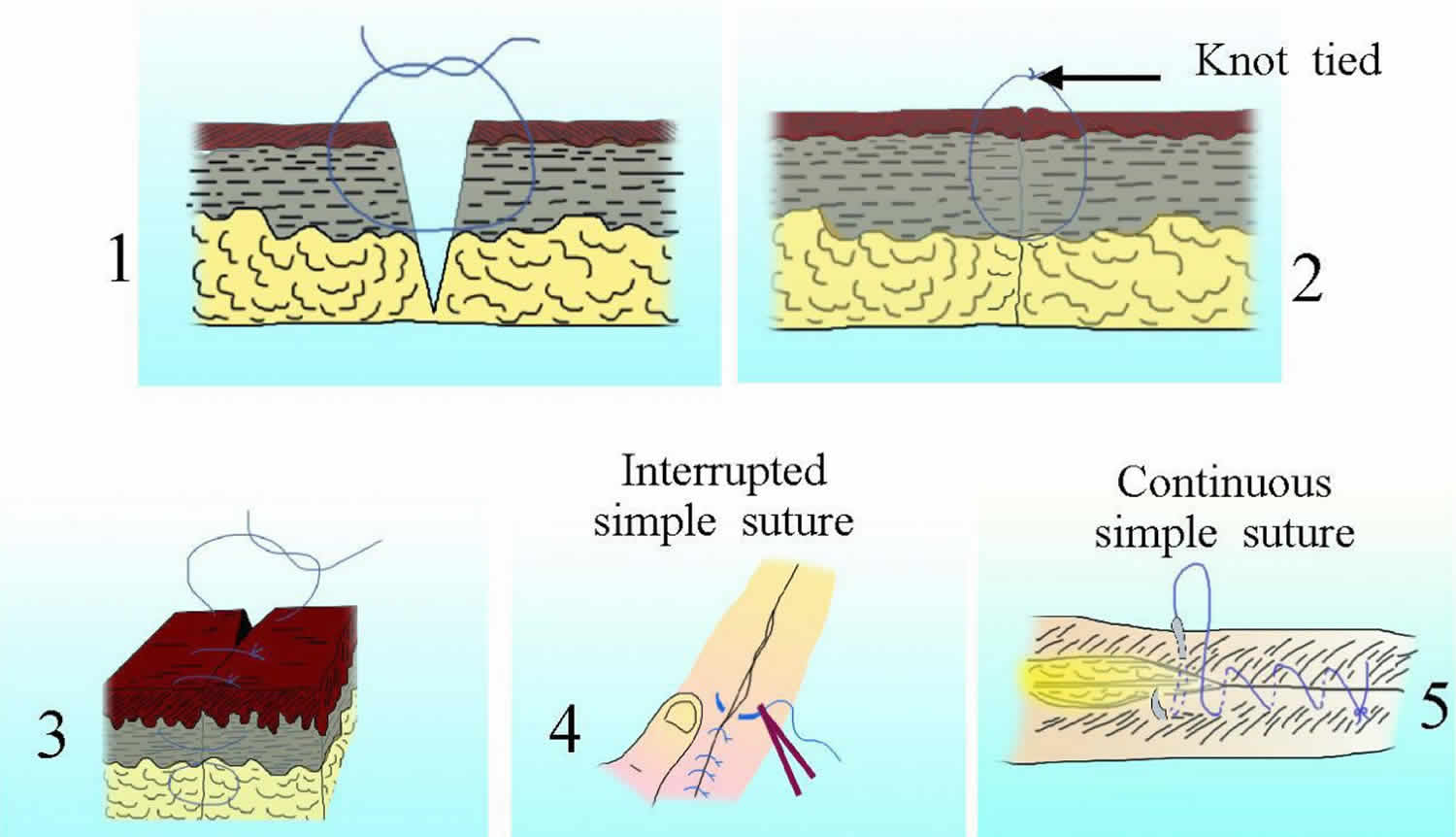
Figure 1. How to suture a wound
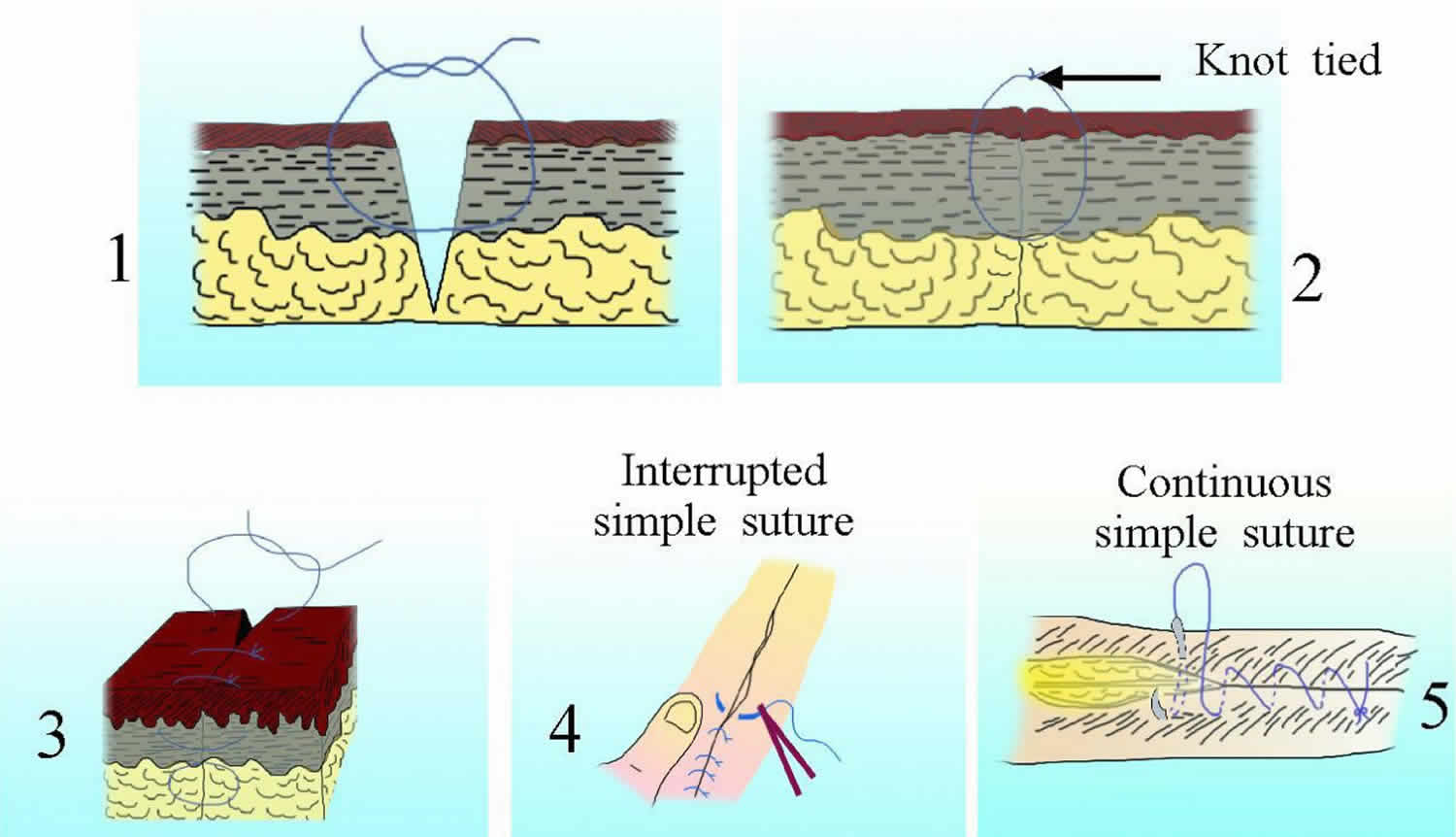
Simple interrupted suture
The simple interrupted suture is the predominant form of basic wound closure and the essential skill of the basic suturing workshop.
Compared with running (continuous) sutures, interrupted sutures are easy to place, have greater tensile strength, and have less potential for causing wound edema and impaired cutaneous circulation. Interrupted sutures also allow the surgeon to make adjustments as needed to properly align wound edges as the wound is sutured.
Disadvantages of interrupted sutures include the length of time required for their placement and the greater risk of crosshatched marks (i.e., train tracks) across the suture line. The risk of crosshatching can be minimized by removing sutures early to prevent the development of suture tracks.
Figure 2. Simple interrupted suture
Simple running suture
Larger wounds can be closed with a continuous simple running suture technique. Running sutures are useful for long wounds in which wound tension has been minimized with properly placed deep sutures and in which approximation of the wound edges is good. This type of suture may also be used to secure a split- or full-thickness skin graft.
The first suture is made in the same manner as the simple interrupted, but subsequent sutures are placed without cutting the suture material. The final knot is made by taking a “bite” of the second to last pass though the tissue and tied in the usual fashion.
Figure 3. Simple running suture
Theoretically, less scarring occurs with running sutures than with interrupted sutures because fewer knots are made with simple running sutures; however, the number of needle insertions remains the same. Both basting sutures and tie-over bolsters have been used to help secure skin grafts 2.
Advantages of the simple running suture over simple interrupted sutures include quicker placement and more rapid reapproximation of wound edges. Disadvantages include possible crosshatching, the risk of dehiscence if the suture material ruptures, difficulty in making fine adjustments along the suture line, and puckering of the suture line when the stitches are placed in thin skin.
Running locked suture
Locked sutures have increased tensile strength; therefore, they are useful in wounds under moderate tension or in those requiring additional hemostasis because of oozing from the skin edges.
Running locked sutures have an increased risk of impairing the microcirculation surrounding the wound, and they can cause tissue strangulation if placed too tightly. Therefore, this type of suture should be used only in areas with good vascularization. In particular, the running locked suture may be useful on the scalp or in the postauricular sulcus, especially when additional hemostasis is needed.
Vertical mattress suture
The vertical mattress suture is ideal for equalizing high-tension forces across a wound edge. A vertical mattress suture is especially useful in maximizing wound eversion, reducing dead space, and minimizing tension across the wound. The vertical mattress sutures are also helpful in areas where wound edge approximation and proper “tenting” is difficult. These can be intermixed with simple interrupted sutures and removed earlier to prevent scarring. A helpful mnemonic is “far-far … near-near” meaning that you begin your first suture further away from the wound margin, and aim further away on your follow-through. The second pass through the tissue follows a similar tract, but closer (near-near) to the wound margin.
One of the disadvantages of the vertical mattress suture is crosshatching. The risk of crosshatching is greater because of increased tension across the wound and the four entry and exit points of the stitch in the skin.
Figure 4. Vertical mattress suture
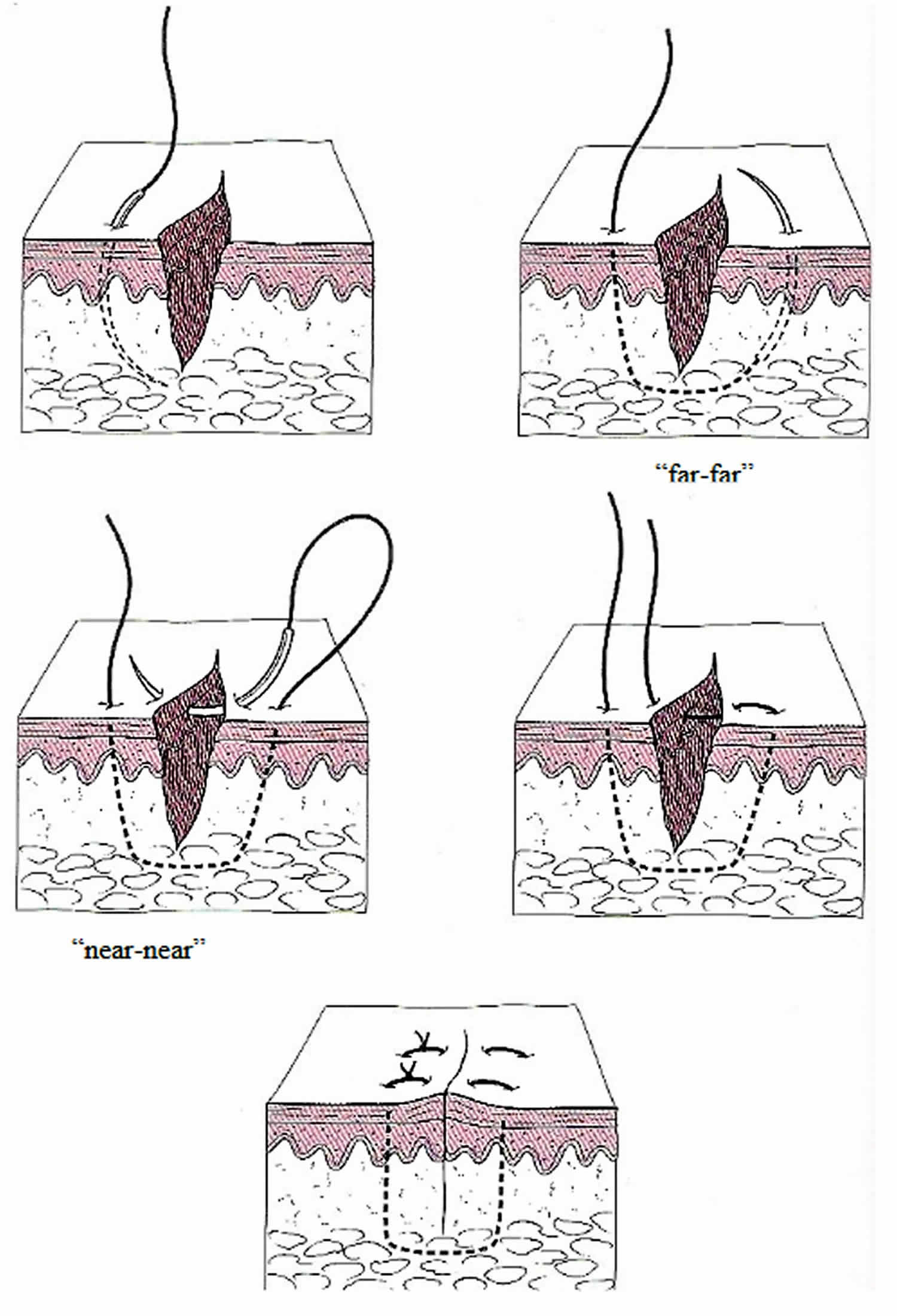
The recommended time for removal of this suture is 5-7 days (before formation of epithelial suture tracks is complete) to reduce the risk of scarring. If the suture must be left in place longer, bolsters may be placed between the suture and the skin to minimize contact. The use of bolsters minimizes strangulation of the tissues when the wound swells in response to postoperative edema. Placing each stitch precisely and taking symmetric bites is especially important with this suture.
Half-buried vertical mattress suture
The half-buried vertical mattress suture is used in cosmetically important areas such as the face.
Pulley suture
The pulley suture facilitates greater stretching of the wound edges and is used when additional wound closure strength is desired.
Far-near near-far modified vertical mattress suture
The far-near near-far modification of the vertical mattress suture, which basically functions as a pulley suture, is useful when tissue expansion is desired, and it may be used intraoperatively for this purpose. This suture is also useful when one is beginning the closure of a wound that is under significant tension. Placing pulley stitches first allows the wound edges to be approximated, thereby facilitating the placement of buried sutures.
When wound closure is complete, the pulley stitches may be either left in place or removed if wound tension has been adequately distributed after placement of the buried and surface sutures.
Horizontal mattress suture
The horizontal mattress suture is useful for wounds under high tension because it provides strength and wound eversion. This suture may also be used as a stay stitch for temporary approximation of wound edges, allowing placement of simple interrupted or subcuticular stitches. The temporary stitches are removed after the tension is evenly distributed across the wound.
Horizontal mattress sutures may be left in place for a few days if wound tension persists after placement of the remaining stitches. In areas of extremely high tension at risk for dehiscence, horizontal mattress sutures may be left in place even after removal of the superficial skin sutures. However, they have a high risk of producing suture marks if left in place for longer than 7 days.
Horizontal mattress sutures may be placed before a proposed excision as a skin expansion technique to reduce tension. Improved eversion may be achieved with this stitch in wounds without significant tension by using small bites and a fine suture.
In addition to the risk of suture marks, horizontal sutures have a high risk of tissue strangulation and wound edge necrosis if tied too tightly. Taking generous bites, using bolsters, and cinching the suture only as tightly as necessary to approximate the wound edges may decrease the risk, as does removing the sutures as early as possible. Placing sutures at a greater distance from the wound edge facilitates their removal.
Half-buried horizontal suture
The half-buried horizontal suture (also referred as the tip stitch or three-point corner stitch) is used primarily to position the corners and tips of flaps and to perform M-plasties and V-Y closures. The corner stitch may provide increased blood flow to flap tips, lowering the risk of necrosis and improving aesthetic outcomes 3. However, in larger flaps with greater tension, this technique has been reported to position the flap tip deeper than the surrounding tissue, often resulting in a depressed scar 4.
Absorbable buried suture
Absorbable buried sutures are used as part of a layered closure in wounds under moderate-to-high tension. Buried sutures provide support to the wound and reduce tension on the wound edges, allowing better epidermal approximation of the wound. They are also used to eliminate dead space, or they are used as anchor sutures to fix the overlying tissue to the underlying structures. Wounds under significant tension may benefit from the use of a subcutaneous inverted cross-mattress stitch (SICM stitch), which can approximate such wounds relatively easily via a lateral pulley effect 5.
Dermal-subdermal suture
A buried dermal-subdermal suture maximizes wound eversion. It is placed so that the suture is more superficial away from the wound edge.
Buried horizontal mattress suture
The buried horizontal mattress suture is used to eliminate dead space, reduce the size of a defect, or reduce tension across wounds 6.
Running horizontal mattress suture
The running horizontal mattress suture is used for skin eversion. It is useful in areas with a high tendency for inversion, such as the neck. It can also be useful for reducing the spread of facial scars. If the sutures are tied too tightly, tissue strangulation is a risk. Although it is slightly more time-consuming to place, this suture appears to result in smoother and flatter scars than a simple running suture 7. A modification of the horizontal running suture with intermittent single loops was recently reported to avoid the characteristic track marks resulting from suture tension while increasing wound eversion 8. Other modifications include the V-shaped Victory stitch 9.
Running subcuticular suture
The running subcuticular suture is valuable in areas where tension is minimal, dead space has been eliminated, and the best possible cosmetic result is desired 10. Because the epidermis is penetrated only at the beginning and end of the suture line, the subcuticular suture effectively eliminates the risk of crosshatching.
The suture does not provide significant wound strength, though it does precisely approximate the wound edges. Therefore, the running subcuticular suture is best reserved for wounds in which the tension has been eliminated with deep sutures, and the wound edges are of approximately equal thicknesses.
Running subcutaneous suture
The running subcutaneous suture is used to close the deep portion of surgical defects under moderate tension. It is used in place of buried dermal sutures in large wounds when a quick closure is desired. Disadvantages of running subcutaneous sutures include the risk of suture breakage and the formation of dead space beneath the skin surface. Modifications of this suture have been recently described, which reportedly allows for consistent eversion and excellent cosmetic results in challenging high-tension areas 11.
Running subcutaneous corset plication stitch
The corset plication technique is used in wounds wider than 4 cm that are under excess tension. It creates natural eversion and better wound edge approximation. This technique eases subsequent placement of intradermal sutures, in that wound diameter and tension are significantly reduced.
The strength of the suture relies on inclusion of the septations from the fascial layer beneath the subcutaneous tissue. If tissue ruptured postoperatively, tension would be distributed more broadly. Potential problems include suture breakage and wound distortion 12.
Modified half-buried horizontal mattress suture
The modified corner stitch allows equal eversion of the flap tip edges and improved aesthetic outcomes. Although it may increase risk of necrosis if tied too tightly, a study by Bechara et al 13 suggested that the incidence of flap tip necrosis was comparable with that of the traditional corner stitch. Modified subcutaneous buried horizontal mattress sutures relieve more wound tension and have a lower risk of dehiscence compared with vertical buried mattress sutures 14.
Deep tip stitch
The deep tip stitch is used for M-plasty, W-plasty flaps, and V-Y closures to increase wound eversion. It provides longer-term support to the flap than the traditional corner stitch does and improves alignment of the tip with the sides of closure. This technique also avoids surface sutures, decreasing the risk of track marks. Flap tip necrosis and complications were comparable to that of standard sutures 4.
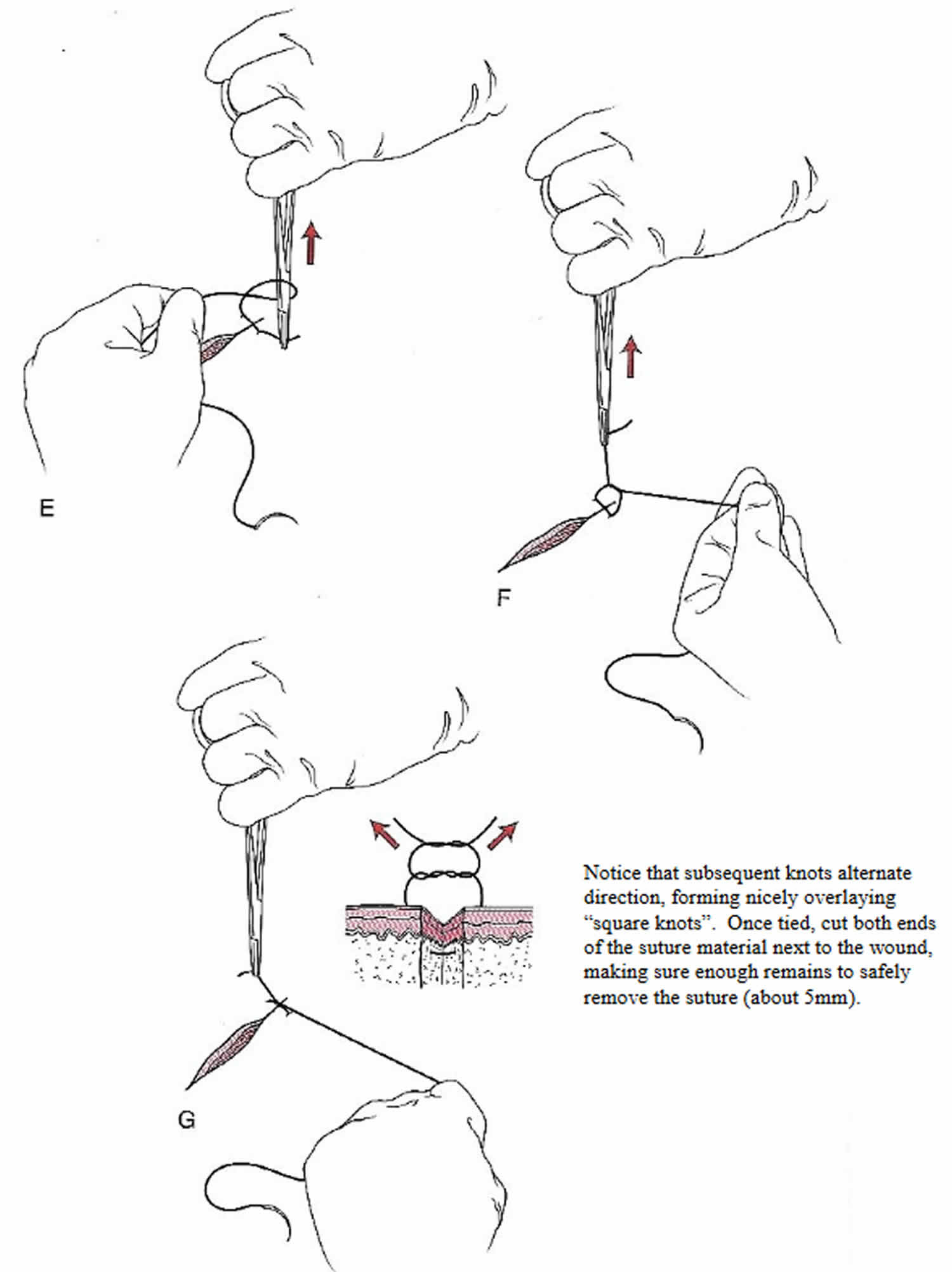
Suture spacing
Suture should be carefully placed to avoid shearing through the tissue wall. One should also avoid strangulating the tissue by tying the knot too tight. This can cause unnecessary scarring and tissue necrosis. The distance between sutures should be roughly ½ the length of the individual sutures. Place the first suture in the center of the wound if approximation will be difficult, continuing by closing the distance to the wound edges by ½ to minimize tension forces on the tissue wall. Notice that the knots are all on the same side. This aids with suture removal.
How to care for sutures
It’s important to keep sutures clean and dry. You should only use creams and lotions if recommended by your doctor.
If you have any bandages or dressings, talk to the doctor or nurse about how to care for them. You’ll need to keep them dry, too; if they get wet, change them. If you can’t do that, see the doctor or nurse.
Risks associated with anesthesia and laceration repair
Complications of laceration repair include infection and wound dehiscence. A wound re-check should be scheduled for 24 to 48 hours after the wound closure if complications are likely. Other complications include scar formation, unrecognized deep-structure injury, and retained foreign body.
Tetanus shot
Any open wound is potentially susceptible to tetanus infection. A booster should be administered if the last tetanus is >10 years old (assuming the patient has received the 3 shot primary series in the past). If the wound is contaminated with debris, a tetanus booster should be considered if the previous tetanus shot is >5 years old. In the event a patient has sustained a tetanus prone wound and has not received the primary 3 shot series, they will require tetanus immune globulin and must be initiated on the primary immunization series.
First 2 days
It’s a good idea to avoid physical activities that might re-open the wound. Children should avoid activities such as playing in sandpits or mud, riding bikes or swimming.
After the first 24-48 hours, patients should gently wash the wound with soap and water, dry it carefully, apply topical antibiotic ointment, and replace the dressing/bandages. Carefully pat the stitches dry. Facial wounds generally only need topical antibiotic ointment without bandaging. Sunscreen SPF 30+ should be applied to the wound to prevent subsequent hyperpigmentation.
It’s best not to soak the wound in a bath, go swimming or wash dishes without gloves until it has healed and the stitches have been taken out or have dissolved.
Pain from the wound and sutures can usually be managed with simple pain relief medicine such as acetaminophen or paracetamol.
As the wound heals, don’t pick at the stitches or scab. Picking at it might increase scarring.
Long-term care
At first, your scar will be red and raised, but over time it will become paler and more flexible
For the first year, protect the scar from sun damage which can make it darker.
Suture removal times
Stitches are often removed after 5 to 10 days, but this depends on where they are. Different parts of the body require suture removal at varying times. Check with the doctor or nurse to find out. Removal time considers both the potential for scarring and the required tensile strength of the wound to withstand stressors.
Removing sutures is generally a quick and painless procedure.
Common periods of time for removal are as follows, but times vary according to the health care professionals that perform the procedure:
- Face: 3-5 days
- Neck: 4-6 days
- Scalp: 7-12 days
- Trunk: 6-10 days
- Upper extremity: 8-14 days
- Extensor surface of hands: 10 days
- Lower extremity: 14-28 days
- Joints: 14 days
Dissolvable sutures may disappear in a week or two, but some take several months.
When should I get my sutures checked?
You should get your sutures checked if:
- the wound re-opens
- the wound looks the same after 5 days as when it was stitched
- the sutures come out before they should
- the wound becomes more red, swollen or painful
- the amount of ooze or pus increases
- you develop a fever
Signs of infection are:
- fever within 48 hours of suturing
- redness
- swelling
- increased pain
- excessive or persistent ooze
- pus or smelly discharge.
If you are concerned about possible signs of infection or have any other concerns visit your doctor or the emergency room.
Removing sutures
If your sutures are not the dissolvable type, see a doctor or nurse when it is time for them to be removed. Do it at the right time – if you have the stitches taken out too soon, the wound might not be healed properly. If you leave them in too long, you can get scarring.
Removing sutures
The wound is cleaned with an antiseptic to remove encrusted blood and loosened scar tissue. Sterile forceps (tongs or pincers) are used to pick up the knot of each suture, and then surgical scissors or a small knife blade is used to cut the suture. Forceps are used to remove the loosened suture and pull the thread from the skin. These relatively painless steps are continued until the sutures have all been removed. You may feel a tug or slight pull as a stitch is removed. The wound is cleansed again. Adhesive strips are often placed over the wound to allow the wound to continue strengthening.
Removing staples
Staple removal is a simple procedure and is similar to suture removal. Doctors use a special instrument called a staple remover. After cleansing the wound, the doctor will gently back out each staple with the remover. The doctor applies pressure to the handle, which bends the staple, causing it to straighten the ends of the staple so that it can easily be removed from the skin. The staple backs out of the skin the very same direction in which it was placed. People may feel a pinch or slight pull. The process is repeated until all staples are removed. The wound is cleansed a second time, and adhesive strips are applied. This is also a relatively painless procedure.
Wound healing and scarring
Scars form as a normal part of healing whenever the skin is damaged. All cuts will heal with a scar, however, the scar will be less noticeable if good care is given to the wound when it is healing.
During the first 6 to 8 weeks after the injury, the scar will change from a thick, red raised scar to a thinner, paler, more flexible one. Scars can take up to 2 years to fully mature.
The final appearance of the scar depends on several factors including the extent of the original wound, inherited skin qualities and how well the scar was looked after.
Looking after your scar
Scar massage
After the sutures have been removed from a wound, or around 2 to 4 weeks after the injury, scar massage can be performed. This should be done for 5 to 10 minutes, twice a day. Do not massage any scar that is open or looks infected.
For the first 2 to 4 weeks, massage should be done along the same direction as the incision. The pressure applied should be enough to change the colour of the scar from pink to pale, but should not be so firm that it is painful.
After about 4 weeks, the scar can be massaged in all directions. Continue to massage daily until the scar is pale and thin.
Moisturizing
Moisturizing lotions such as aloe vera, sorbolene or other un-fragranced products can be used to soften the scar and make massage easier. Many patients use topical vitamin E (alpha-tocopherol) hoping its antioxidant properties will prevent scars. However, there is little evidence that it is helpful, and some patients develop a contact dermatitis that may delay healing 15. Used early on, vitamin E may also reduce the tensile strength of the scar, and its use should be discouraged 16.
Sun protection
It is very important to protect the scar from sun damage, which can permanently discolour the scar. You should always cover the scar with at least SPF 30 sunblock or zinc cream, wear clothing that covers the scar and stay in the shade.
Daily activity
It is important to avoid activities and areas that will get the wound dirty. This includes bike riding, skateboarding and swimming and play areas like sandpits.
Problem scars
A scar is a problem if it is painful or itchy, hard or raised, restricts movement or remains purple or red.
Risk factors for problem scars include certain skin types (especially dark, Mediterranean or Asian skin), previous problem scars, or post-operative wound complications such as poor healing (greater than three weeks) or infection.
Contact your doctor if you are concerned that your scar is not healing as expected.
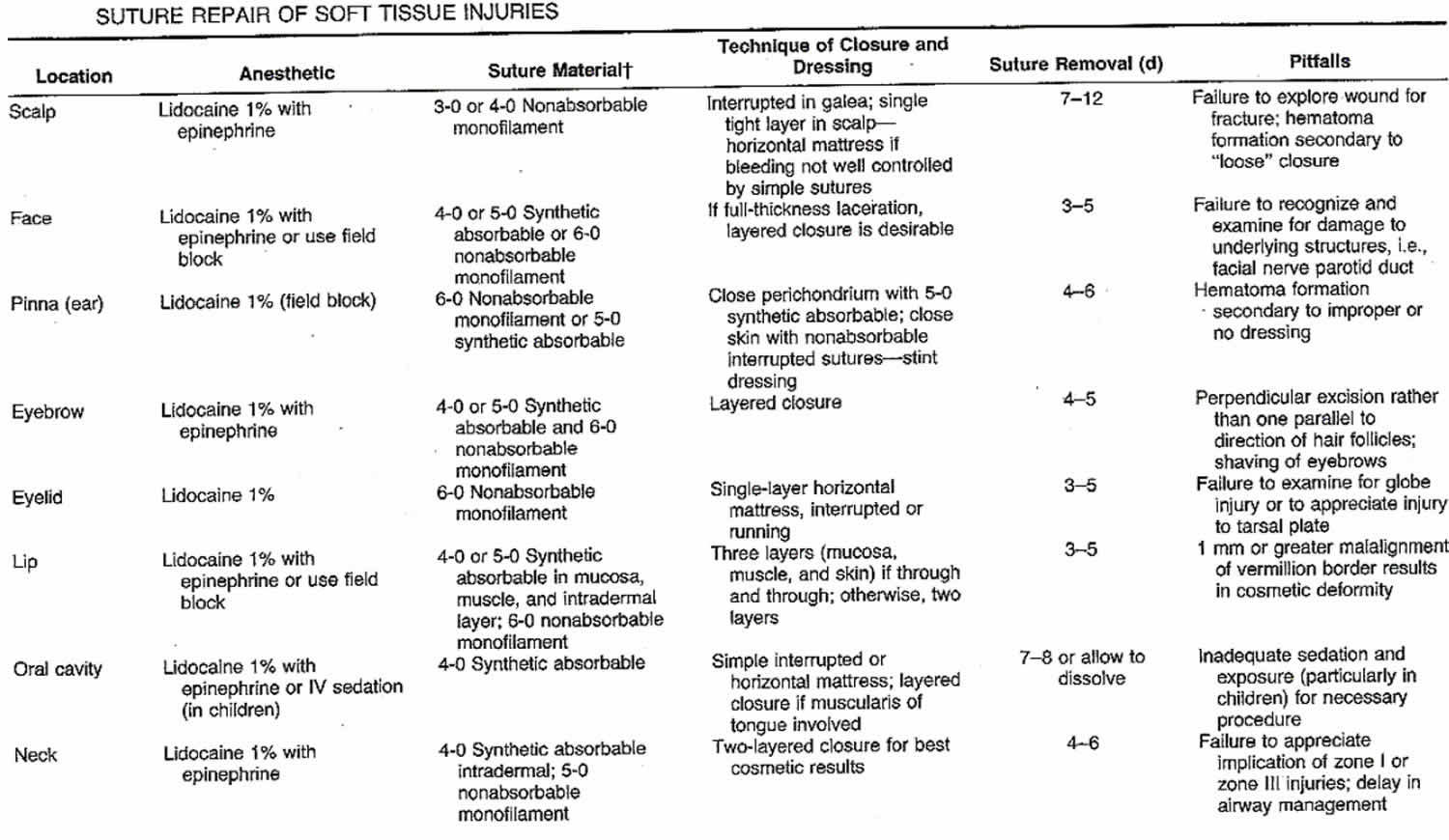
Suture summary
Table 4. Suture repair of soft tissue injuries
- UNIVERSITY OF WASHINGTON EMERGENCY MEDICINE INTEREST GROUP. A GUIDE TO THE BASIC SUTURE WORKSHOP. http://depts.washington.edu/uwemig/media_files/EMIG%20Suture%20Handout.pdf
- Kromka W, Cameron M, Fathi R. Tie-Over Bolster Dressings vs Basting Sutures for the Closure of Full-Thickness Skin Grafts: A Review of the Literature. J Cutan Med Surg. 2018 Jun 1. 1203475418782152
- Kandel EF, Bennett RG. The effect of stitch type on flap tip blood flow. J Am Acad Dermatol. 2001 Feb. 44(2):265-72.
- Chan JL, Miller EK, Jou RM, Posten W. Novel surgical technique: placement of a deep tip stitch. Dermatol Surg. 2009 Dec. 35(12):2001-3.
- Wade RG, Wormald JC, Figus A. Absorbable versus non-absorbable sutures for skin closure after carpal tunnel decompression surgery. Cochrane Database Syst Rev. 2018 Feb 1. 2:CD011757
- Alam M, Goldberg LH. Utility of fully buried horizontal mattress sutures. J Am Acad Dermatol. 2004 Jan. 50(1):73-6.
- Moody BR, McCarthy JE, Linder J, Hruza GJ. Enhanced cosmetic outcome with running horizontal mattress sutures. Dermatol Surg. 2005 Oct. 31(10):1313-6.
- Chacon AH, Shiman MI, Strozier N, Zaiac MN. Horizontal running mattress suture modified with intermittent simple loops. J Cutan Aesthet Surg. 2013 Jan. 6(1):54-6.
- Eleftheriou LI, Weinberger CH, Endrizzi BT, et al. The Victory stitch: a novel running v-shaped horizontal mattress suturing technique. Dermatol Surg. 2011 Nov. 37(11):1663-5.
- Alam M, Posten W, Martini MC, Wrone DA, Rademaker AW. Aesthetic and functional efficacy of subcuticular running epidermal closures of the trunk and extremity: a rater-blinded randomized control trial. Arch Dermatol. 2006 Oct. 142(10):1272-8.
- Yag-Howard C. Zipper stitch: a novel aesthetic subcutaneous closure. Dermatol Surg. 2013 Sep. 39(9):1400-2.
- Tierney E, Kouba DJ. A subcutaneous corset plication rapidly and effectively relieves tension on large linear closures. Dermatol Surg. 2009 Nov. 35(11):1806-8.
- Bechara FG, Al-Muhammadi R, Sand M, Tomi NS, Altmeyer P, Hoffmann K. A modified corner stitch for fixation of flap tips. Dermatol Surg. 2007 Oct. 33(10):1277-9.
- Meng F, Andrea S, Cheng S, Wang Q, Huo R. Modified Subcutaneous Buried Horizontal Mattress Suture Compared With Vertical Buried Mattress Suture. Ann Plast Surg. 2017 Mar 7.
- Khoosal D, Goldman R. Vitamin E for treating children’s scars. Does it help reduce scarring? Can Fam Physician. 2006;52:855–856.
- Management of Keloids and Hypertrophic Scars. Am Fam Physician. 2009 Aug 1;80(3):253-260. https://www.aafp.org/afp/2009/0801/p253.html





{kind=link}