What is thoracic outlet syndrome
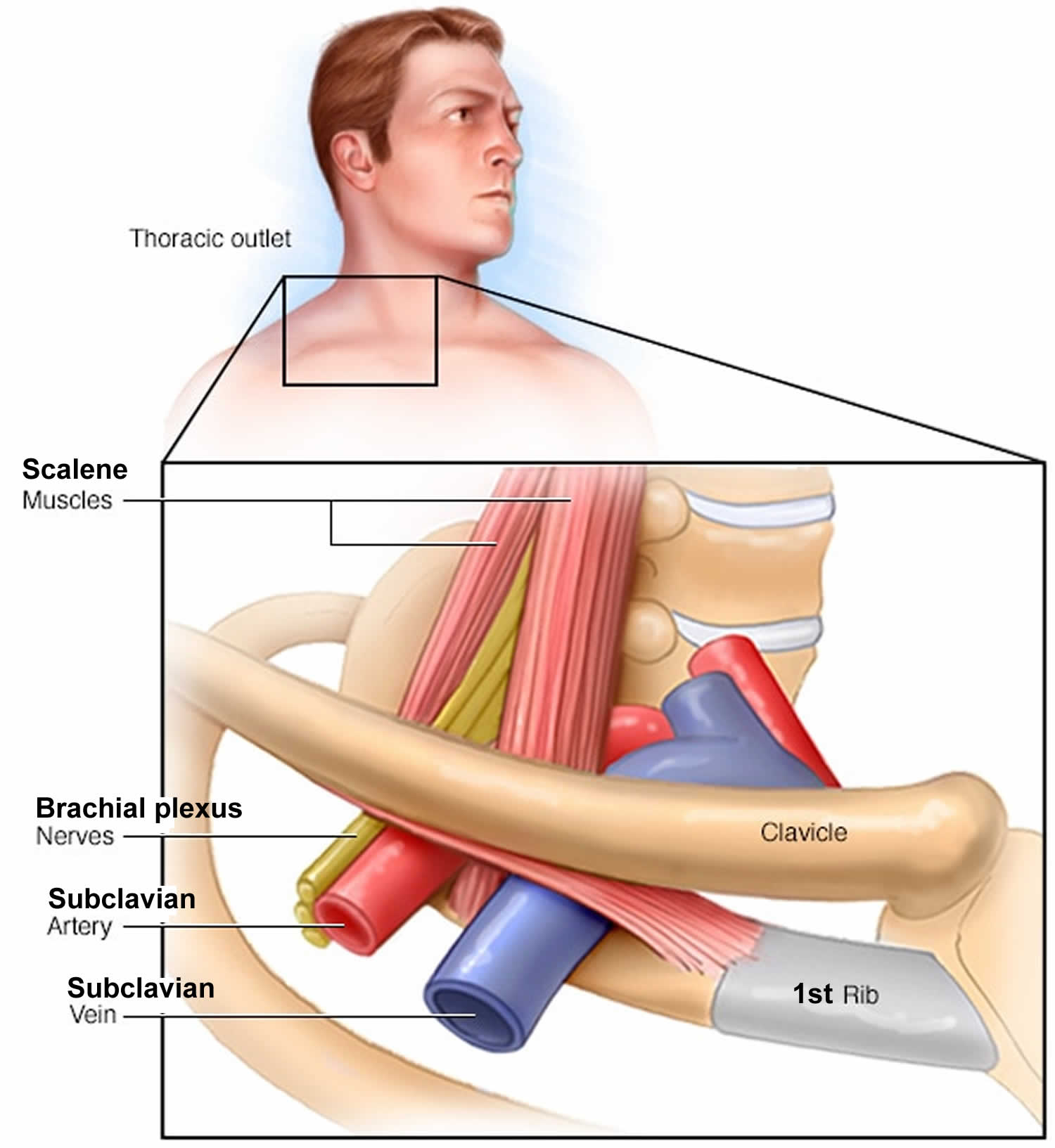
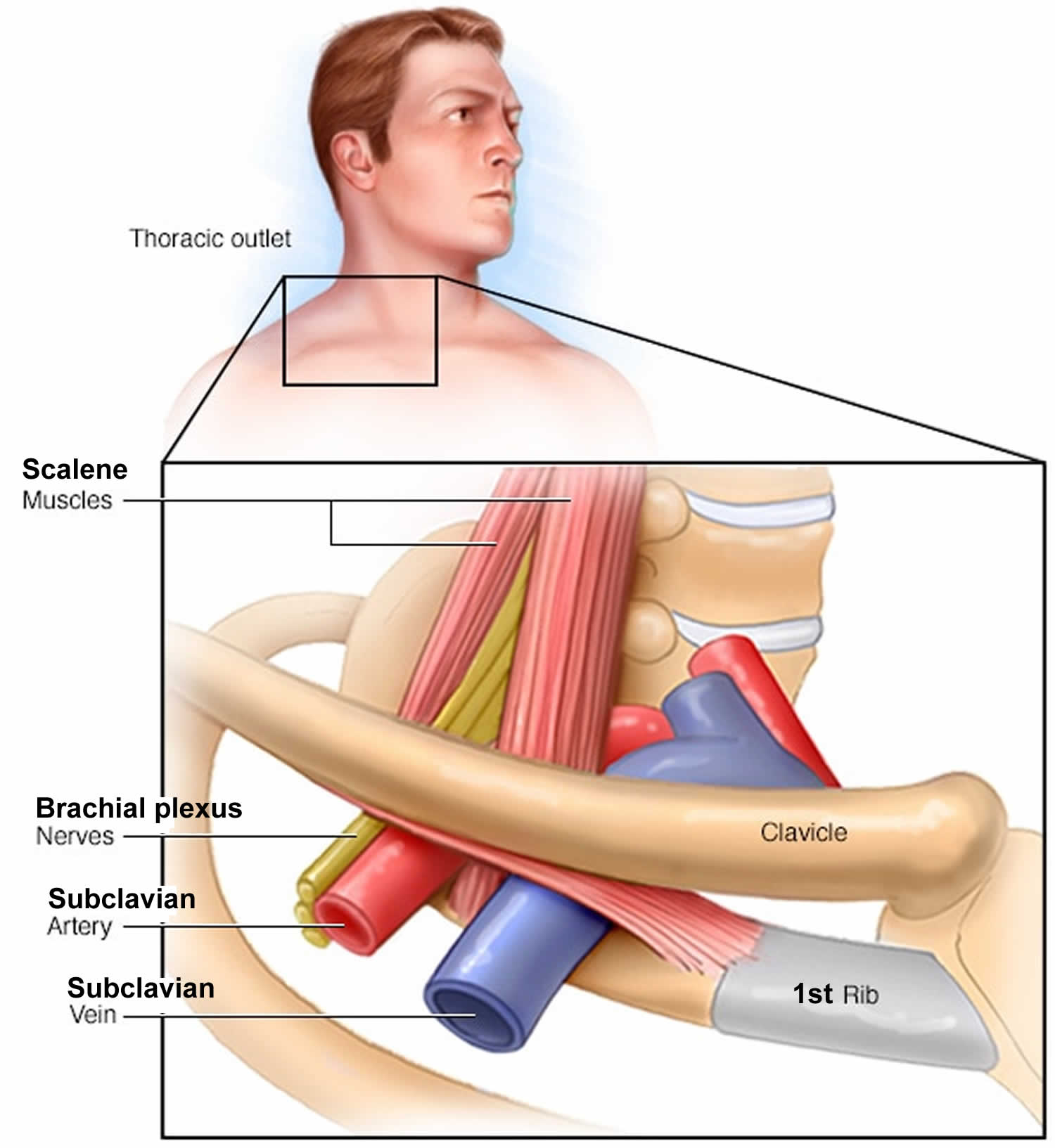
Thoracic outlet syndrome is an umbrella term that encompasses three related syndromes that involve compression of the nerves, arteries, and veins in the lower neck and upper chest area and causing pain, weakness, numbness, or tingling in the arm, shoulder, and neck. Most doctors agree that thoracic outlet syndrome is caused by compression of the brachial plexus or subclavian vessels (subclavian artery and subclavian vein) as they pass through narrow passageways (between the first rib or an abnormal rib, the clavicle and the scalene muscles) leading from the base of the neck to the armpit and arm, but there is considerable disagreement about its diagnosis and treatment.
Making the diagnosis of thoracic outlet syndrome even more difficult is that a number of disorders feature symptoms similar to those of thoracic outlet syndrome, including rotator cuff injuries, cervical disc disorders, fibromyalgia, multiple sclerosis, complex regional pain syndrome, and tumors of the syrinx or spinal cord.
Thoracic outlet syndrome disorder can sometimes be diagnosed in a physical exam by tenderness in the supraclavicular area, weakness and/or a “pins and needles” feeling when elevating the hands, weakness in the fifth (“little”) finger, and paleness in the palm of one or both hands when the individual raises them above the shoulders, with the fingers pointing to the ceiling. Symptoms of thoracic outlet syndrome vary depending on the type.
- Neurogenic thoracic outlet syndrome is the most common type and occurs when the nerves in the brachial plexus are compressed, usually between the first rib and the scalene muscles. Most patients have a characteristic sign, called the Gilliatt-Sumner hand, in which there is severe wasting in the fleshy base of the thumb. Other symptoms include paresthesias (pins and needles sensation or numbness) in the fingers and hand, change in hand color, hand coldness, or dull aching pain in the neck, shoulder, and armpit. These symptoms usually worsen when the thoracic outlet is narrowed in certain body positions, such as when the arm is raised overhead. Many patients with neurogenic thoracic outlet syndrome have abnormal anatomy in the thoracic outlet (for example, an extra rib called a cervical rib) and a history of neck trauma (for example, a car accident or repetitive movements while playing sports or working). Other patients have no clear cause, but their symptoms are concerning for thoracic outlet syndrome.
- Venous thoracic outlet syndrome is rare and occurs when the subclavian vein is compressed, usually between the first rib and clavicle (or collarbone), causing a blood clot. It is also called “effort thrombosis” and Paget-Schroetter disease. Symptoms may include numbness, tingling, aching, swelling of the extremity and fingers, and weakness of the neck or arm. Many patients suddenly develop a swollen and discolored arm with pallor, a weak or absent pulse in the affected arm, which also may be cool to the touch and appear paler than the unaffected arm. Immediate treatment is critical. Patients usually require catheter-directed thrombolysis, anticoagulation, and then surgery to decompress the thoracic outlet.
- Arterial thoracic outlet syndrome is extremely rare and occurs when the subclavian artery is compressed, usually near a cervical rib or anomalous first rib. This compression may lead to an aneurysm (widening) of the artery and formation of blood clots that can prevent blood flow to the arm and hand. Patients may have sudden pain, weakness, numbness, and/or tingling in their hands, and they almost always require surgery. Arterial thoracic outlet syndrome most prominently features change in color and cold sensitivity in the hands and fingers, swelling, heaviness, paresthesias (pins and needles sensation or numbness) and poor blood circulation in the arms, hands, and fingers.
- Nonspecific-type thoracic outlet syndrome. This type is also called disputed thoracic outlet syndrome. Some doctors don’t believe it exists, while others say it’s a common disorder. People with nonspecific-type thoracic outlet syndrome have chronic pain in the area of the thoracic outlet that worsens with activity, but a specific cause of the pain can’t be determined.
There are many causes of thoracic outlet syndrome, including physical trauma, anatomical defects, tumors that press on nerves, poor posture that causes nerve compression, pregnancy, and repetitive arm and shoulder movements and activity, such as from playing certain sports.
Thoracic outlet syndrome is more common in women. The onset of symptoms usually occurs between 20 and 50 years of age. Doctors usually recommend nerve conduction studies, electromyography, or imaging studies to confirm or rule out a diagnosis of thoracic outlet syndrome.
The outcome for individuals with thoracic outlet syndrome varies according to type. The majority of individuals with thoracic outlet syndrome will improve with exercise and physical therapy. Vascular thoracic outlet syndrome, and true neurogenic thoracic outlet syndrome often require surgery to relieve pressure on the affected vessel or nerve.
Thoracic outlet syndrome treatment begins with exercise programs and physical therapy to strengthen chest muscles, restore normal posture, and relieve compression by increasing the space of the area the nerve passes through. Doctors will often prescribe non-steroidal anti-inflammatory drugs (such as naproxen or ibuprofen) for pain. Other medicines include thromobolytics to break up blood clots and anticoagulants to prevent clots. If this doesn’t relieve pain, a doctor may recommend thoracic outlet decompression surgery to release or remove the structures causing compression of the nerve or artery. Surgical decompression of the thoracic outlet – removal of the first rib or an anomalous rib, partial removal of the anterior and middle scalene muscles, and decompression of the brachial plexus.
Figure 1. Thoracic outlet syndrome
Thoracic outlet syndrome causes
In general, the cause of thoracic outlet syndrome is compression of the nerves or blood vessels in the thoracic outlet, just under your collarbone (clavicle). The cause of the compression varies and can include:
- Anatomical defects. Inherited defects that are present at birth (congenital) may include an extra rib located above the first rib (cervical rib) or an abnormally tight fibrous band connecting your spine to your rib.
- Cervical rib: A cervical rib is an extra rib that grows from the cervical spine — the neck part of the spine. Between 1 and 3 percent of the population has a cervical rib, which may grow on one side or both, and may reach down to attach to the first rib or may not be fully formed. Having a cervical rib increases the chance of nerve or blood vessel compression between the rib or its muscles and ligamentous connections sharing this small space. A small percentage of people with a cervical rib develop thoracic outlet syndrome. Many people with a cervical rib never know it, because the bone is often tiny and isn’t noticed, even in X-rays.
- Abnormal muscle or first rib formation: Some people may have an extra or aberrant scalene muscle (an inner muscle of the neck) or an abnormal first rib or clavicle (collarbone). Any of these abnormal formations can compress blood vessels or nerves.
- Poor posture. Drooping your shoulders or holding your head in a forward position can cause compression in the thoracic outlet area.
- Trauma. A traumatic event, such as a car accident, can cause internal changes that then compress the nerves in the thoracic outlet. The onset of symptoms related to a traumatic accident often is delayed.
- Repetitive activity. Doing the same thing repeatedly can, over time, wear on your body’s tissue. You may notice symptoms of thoracic outlet syndrome if your job requires you to repeat a movement continuously, such as typing on a computer, working on an assembly line or lifting things above your head, as you would if you were stocking shelves. Athletes, such as baseball pitchers and swimmers, also can develop thoracic outlet syndrome from years of repetitive movements.
- Pressure on your joints. Obesity can put an undue amount of stress on your joints, as can carrying around an oversized bag or backpack.
- Pregnancy. Because joints loosen during pregnancy, signs of thoracic outlet syndrome may first appear while you’re pregnant.
The following events may cause thoracic outlet syndrome, especially in people with the above bone or muscle abnormalities in the neck:
- Whiplash: Arm and hand symptoms that persist long after a whiplash injury may be a sign of thoracic outlet syndrome.
- Bodybuilding: Built-up muscles in the neck may grow too large and compress nerves or the subclavian vessels.
- Repeated overhead motions: People who take up swimming, baseball or painting, or who work as hairstylists, auto mechanics or other jobs that require raised arms may develop thoracic outlet syndrome.
- Weight gain: As with extra muscle mass, extra fat in the neck may compress nerves or subclavian vessels.
- Tumor in the neck: On rare occasions, a tumor may be the cause of the compression.
Risk factors for thoracic outlet syndrome
There are several risk factors that seem to increase the risk of thoracic outlet syndrome, including:
- Sex. Females are far more likely to be diagnosed with thoracic outlet syndrome than are males.
- Age. Thoracic outlet syndrome is more common in young adults, between 20 and 40 years old.
Thoracic outlet syndrome symptoms
The symptoms of thoracic outlet syndrome depend on the type of thoracic outlet syndrome.
Symptoms of neurogenic thoracic outlet syndrome
This form of thoracic outlet syndrome is characterized by compression of the brachial plexus. The brachial plexus is a network of nerves that come from your spinal cord and control muscle movements and sensation in your shoulder, arm and hand. In the majority of thoracic outlet syndrome cases, the symptoms are neurogenic.
- Pain or weakness in the shoulder, arm or hand
- Tingling or discomfort in the fingers
- Arm that tires quickly
- Weakening grip
- Atrophy — shrinking and weakness — of the pad of the thumb, the muscle of the palm that leads to the thumb (Gilliatt-Sumner hand); this is quite rare
Symptoms may come and go, but they are often made worse when arms are held up. The longer the arms stay up, the worse the symptoms can get.
Symptoms of venous thoracic outlet syndrome
This type of thoracic outlet syndrome occurs when one or more of the veins (venous thoracic outlet syndrome) under the collarbone (clavicle) are compressed.
- Edema (swelling) of the arm, hand or fingers
- Blueness of the hand and arm
- Painful tingling in the hand and arm
- Very prominent veins in the shoulder, neck and hand
These symptoms occur because compression of the vein may cause blood clots. This is known as effort thrombosis, or Paget-Schroetter syndrome. Effort thrombosis is a type of deep vein thrombosis. In this case, the clots are formed as the result of overhead motions (efforts) that compress the vein.
Deep vein thrombosis is more common in the legs. When it occurs in the shoulders or arms, the cause is either recent surgery, a foreign object inserted into the upper body — such as a central line, pacemaker or implantable cardioverter defibrillator — or thoracic outlet syndrome.
Symptoms of arterial thoracic outlet syndrome
This type of thoracic outlet syndrome occurs when one or more of the arteries (arterial thoracic outlet syndrome) under the collarbone (clavicle) are compressed.
- Cold and pale hand
- Pain in the hand and arm, especially during overhead motions of the arm
- Embolism (blockage) of an artery in the hand or arm
- Aneurysm of the subclavian artery
Thoracic outlet syndrome complications
If your symptoms haven’t been treated early, you may experience progressive nerve damage, and you may need surgery. Doctors recommend surgery to treat thoracic outlet syndrome only when other treatments haven’t been effective. Surgery has higher risks than do other treatments and may not always treat your symptoms.
Thoracic outlet syndrome that goes untreated for years can cause permanent neurological damage, so it’s important to have your symptoms evaluated and treated early, or take steps to prevent the disorder.
If you’re susceptible to thoracic outlet compression, avoid repetitive movements and lifting heavy objects. If you’re overweight, you can prevent or relieve symptoms associated with thoracic outlet syndrome by losing weight.
Even if you don’t have symptoms of thoracic outlet syndrome, avoid carrying heavy bags over your shoulder, because this can increase pressure on the thoracic outlet. Stretch daily, and perform exercises that keep your shoulder muscles strong.
Thoracic outlet syndrome diagnosis
Thoracic outlet syndrome is sometimes considered controversial, as symptoms can be vague and similar to other conditions. Furthermore, diagnosing thoracic outlet syndrome can be difficult because the symptoms and their severity can vary greatly among people with the disorder.
It’s important that you are evaluated by a doctor who can distinguish between the various types of thoracic outlet syndrome and rule out other conditions.
To diagnose thoracic outlet syndrome, your doctor may review your symptoms and medical history and conduct a physical examination.
Physical examination
Your doctor will perform a physical examination to look for external signs of thoracic outlet syndrome, such as a depression in your shoulder, swelling or pale discoloration in your arm, abnormal pulses, or limited range of motion.
Medical history
Your doctor will likely ask about your medical history and symptoms, as well as your occupation and physical activities.
Thoracic outlet syndrome tests
Provocation tests
Provocation tests are designed to try to reproduce your symptoms. The tests may help your doctor determine the cause of your condition and help rule out other causes that may have similar symptoms.
In these tests, your doctor may ask you to move your arms, neck or shoulders in various positions. Your doctor will check your symptoms and examine you in different positions.
Imaging and nerve study tests
To confirm the diagnosis of thoracic outlet syndrome, your doctor may order one or more of the following tests:
- X-ray. Your doctor may order an X-ray of the affected area, which may reveal an extra rib (cervical rib). X-rays also may rule out other conditions that may be causing your symptoms.
- Ultrasound. An ultrasound uses sound waves to create images of your body. Doctors may use this test to see if you have vascular thoracic outlet syndrome or other vascular problems.
- Computerized tomography (CT) scan. A CT scan uses X-rays to obtain cross-sectional images of your body. A dye may be injected into a vein to view the blood vessels in greater detail (CT angiography). A CT scan may identify the location and cause of blood vessel (vascular) compression.
- Magnetic resonance imaging (MRI). An MRI uses powerful radio waves and magnets to create a detailed view of your body. Your doctor may use an MRI to determine the location and cause of blood vessel (vascular) compression. An MRI may reveal congenital anomalies, such as a fibrous band connecting your spine to your rib or a cervical rib, which may be the cause of your symptoms.
- Angiography. In some cases, you may be given an intravenous dye before a CT or MRI scan. The dye helps to make blood vessels more visible on the images.
- Arteriography and venography. In these tests, your doctor inserts a thin, flexible tube (catheter) through a small incision, usually in your groin. The catheter is moved through your major arteries in arteriography, or through your veins in venography, to the affected blood vessels. Then your doctor injects a dye through the catheter to show X-ray images of your arteries or veins. Doctors can check to see if you have a compressed vein or artery. If a vein or artery has a clot, doctors can deliver medications through the catheter to dissolve the clot.
- Electromyography (EMG). During an EMG, your doctor inserts a needle electrode through your skin into various muscles. The test evaluates the electrical activity of your muscles when they contract and when they’re at rest.
- Nerve conduction study. These tests use a low amount of electrical current to test and measure your nerves’ ability to send impulses to muscles in different areas of your body. This test can determine if you have nerve damage.
- Brachial plexus block: Local anesthetic is injected into the scalene muscles of the neck. The chance of having neurogenic thoracic outlet syndrome is stronger if other symptoms disappear while this area is numb.
- Scalene muscle botulinum toxin injection may be performed for diagnostic and therapeutic purposes. Botulinum toxin causes temporary paralysis of the scalene muscles, which then relax around the nerves in the thoracic outlet. If patients have significant improvement in their symptoms, they are more likely to improve after treatment for thoracic outlet syndrome.
Electromyography and nerve conduction studies may be performed to evaluate for other diseases that may cause similar symptoms. Cervical spine disorders, musculoskeletal disorders, carpal tunnel syndrome, fibromyalgia, and other conditions can all be mistaken for neurogenic thoracic outlet syndrome if a careful work-up is not performed.
Thoracic outlet syndrome treatment
In most cases, a conservative approach to treatment is effective, especially if your condition is diagnosed early. The first step in the treatment of thoracic outlet syndrome is physical and occupational therapy, which includes exercises that widen the thoracic outlet, correct posture, and improve ergonomics.
Scalene muscle botulinum toxin injection, as described above, can be used for both diagnosis and as a temporizing therapy.
Medications
Your doctor may prescribe anti-inflammatory medications, pain medications or muscle relaxants to decrease inflammation, reduce pain and encourage muscle relaxation.
Clot-dissolving medications
If you have venous or arterial thoracic outlet syndrome and have blood clots, your doctor may administer clot-dissolving medications (thrombolytics) into your veins or arteries to dissolve blood clots. After you’re given thrombolytics, your doctor may prescribe medications to prevent blood clots (anticoagulants).
Surgery is performed in patients who have a clear diagnosis of thoracic outlet syndrome and have debilitating symptoms despite physical and occupational therapy. Patients whose symptoms improved after scalene muscle botulinum toxin injection are more likely to have a good outcome after surgery.
Thoracic outlet syndrome physical therapy
Exercise has shown to be a useful approach in 50 to 90% of all thoracic outlet syndrome cases 1. Although there is much variation within and between individuals, symptoms of thoracic outlet syndrome generally improve with exercise and other physical therapy techniques (e.g., manual therapy or manual adjustments) 2, 3. In a general exercise session, emphasis on proper scapular function during upper-body movements, breathing techniques, and head and pelvis alignment during various tasks is essential for treating thoracic outlet syndrome 4. Resistance exercises can be performed with either resistance bands or dumbbells, and with a goal of achieving muscular endurance (i.e., low weight and high number of repetitions). Shortly after diagnosis, women and men should use 2 kg and 3 kg, respectively, if using weights 4. However, strengthening exercises alone will not alter the pathophysiology of thoracic outlet syndrome; a combination of strengthening, stretching, and postural adjustments must all be incorporated for improvements to be observed 4.
Experts recommendation is that exercises should initially incorporate shoulder movements ranging from 0 to 30° flexion, while maintain approximately 40° horizontal abduction 5. Individuals should eventually progress to shoulder movements that incorporate 45° to 90° flexion and functional overhead tasks 5. It is important to initially target scapular muscles (e.g., middle and lower trapezius and rhomboids) in an effort to stabilize the shoulder 4. As patients progress, the strengthening of the serratus anterior musculature is important, but horizontal adduction should be minimized to prevent further injury 4. Proper technique needs to be maintained throughout the rehabilitation process, as improper or inappropriate movements of other joints (e.g., excessive elbow flexion) may alter the recruitment patterns of the shoulder muscles 6. The stretching of the scalenes and pectoralis muscles, while strengthening the muscles of cervical spine (i.e., cervical erectors, rhomboid major and minor, and lower trapezius), should be an area of focus for practitioners 7.
Thoracic outlet syndrome exercises
A summary of exercises targeting the shoulder muscles are displayed in Table 1, while a visual guide for these exercises are given in Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8 and Figure 9. These exercises may have a variety of different modifications and progressions, and it is up to the practitioner’s discretion to provide the correct exercise prescription. For example, a six-month long physical therapy program consisting of at-home exercises, stretching, postural corrections, and muscle recruitment patterns, primarily focusing on the neck and shoulder, can alleviate symptoms associated with thoracic outlet syndrome 8.
Table 1. Summary of suggested exercises to target shoulder and scapular musculature
| Exercise | Muscles Targeted | Exercise | Muscles Targeted |
|---|---|---|---|
| Scapular retraction | – Rhomboids – Trapezius | Prone shoulder extension, abduction, horizontal abduction “I’s, Y’s and T’s” | – Rhomboids – Trapezius – Supraspinatus – Infraspinatus – Deltoid – Latissimus dorsi – Teres major |
| Scapular depression | – Trapezius (lower) – Latissimus dorsi – Rhomboids | Frontal raise | Deltoid |
| Standing external rotation “No Money” | – Trapezius (lower) – Infraspinatus – Teres minor – Subscapularis | Lateral raise | – Deltoid – Supraspinatus – Trapezius |
| Straight arm extension | – Latissimus dorsi – Teres major – Triceps brachii | Serratus push | Serratus anterior |
| Banded high rows | – Latissimus dorsi – Trapezius – Rhomboids – Teres major/minor | Chin tuck | Trapezius |
Figure 2. Thoracic outlet syndrome exercise – scapular retraction and depression
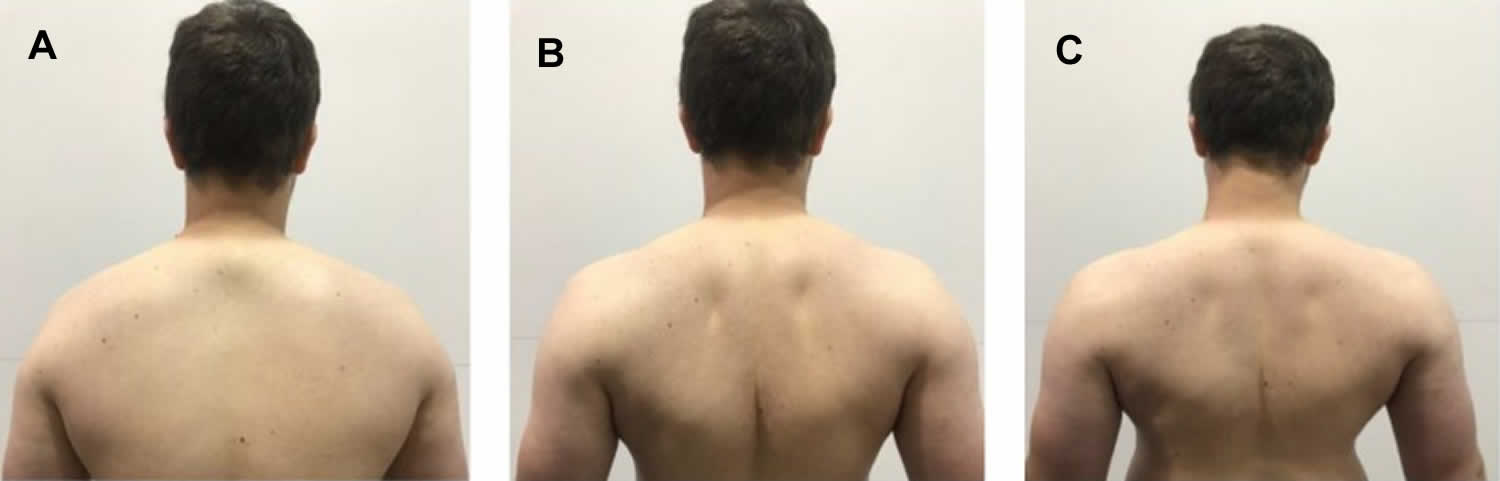
Footnote: Demonstration of scapular retraction and depression in the (A) start position; (B) end position of scapular retraction; (C) end position of scapular depression. For scapular retraction, emphasis is placed on “pulling” the shoulder blades backwards. For scapular depression, emphasis is placed on “pulling” the shoulders back and down.
Figure 3. Thoracic outlet syndrome exercise – standing external rotation
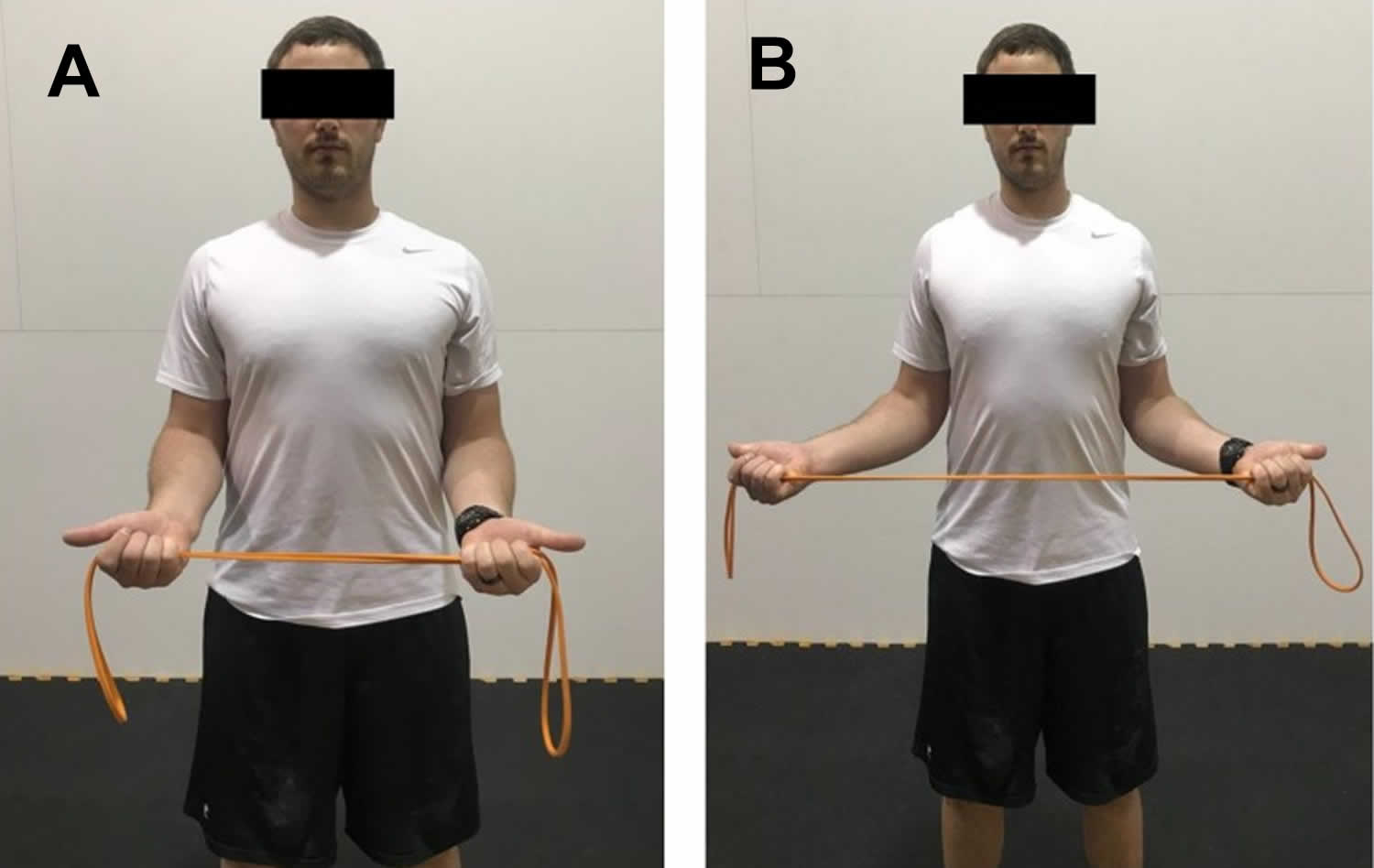
Footnote: Demonstration of standing external rotation in the (A) start position; (B) end position. Hands are pronated and elbows are flexed to approximately 90°. Pull the band apart, while focusing on retracting the scapula.
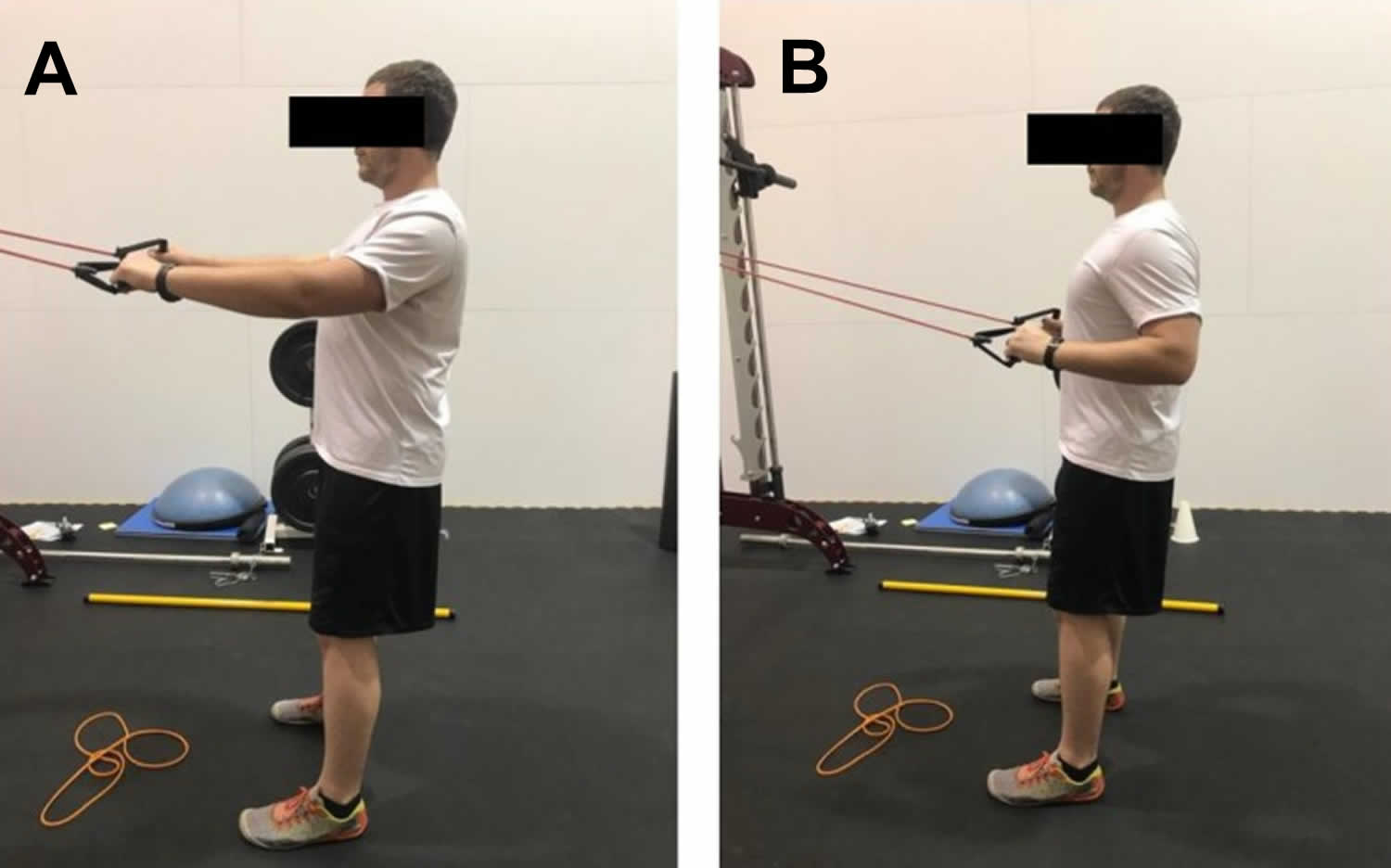
Figure 4. Thoracic outlet syndrome exercise – banded straight arm extension
Footnote: Demonstration of banded straight arm extension in the (A) start position; (B) end position. Arms start either elevated or parallel with the ground. The elbows stay slightly flexed, and the hands are brought down to the thigh while keeping the arms straight.
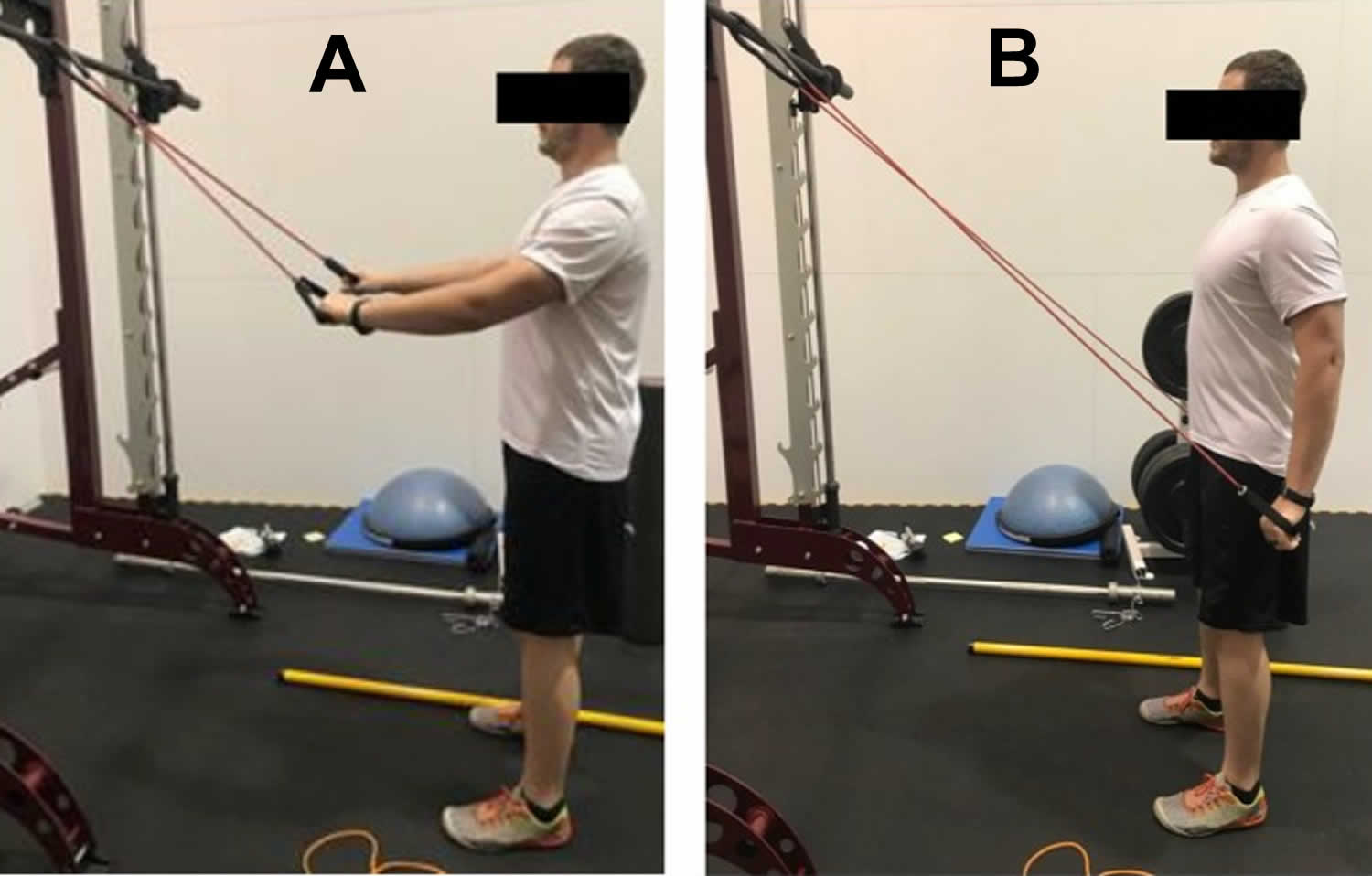
Figure 5. Thoracic outlet syndrome exercise – banded high pull
Footnote: Demonstration of banded high pull in the (A) start position; (B) end position. The scapula is required first to be retracted and depressed. The band is then pulled to the chest.
Figure 6. Thoracic outlet syndrome exercise – prone shoulder extension, abduction and horizontal abduction
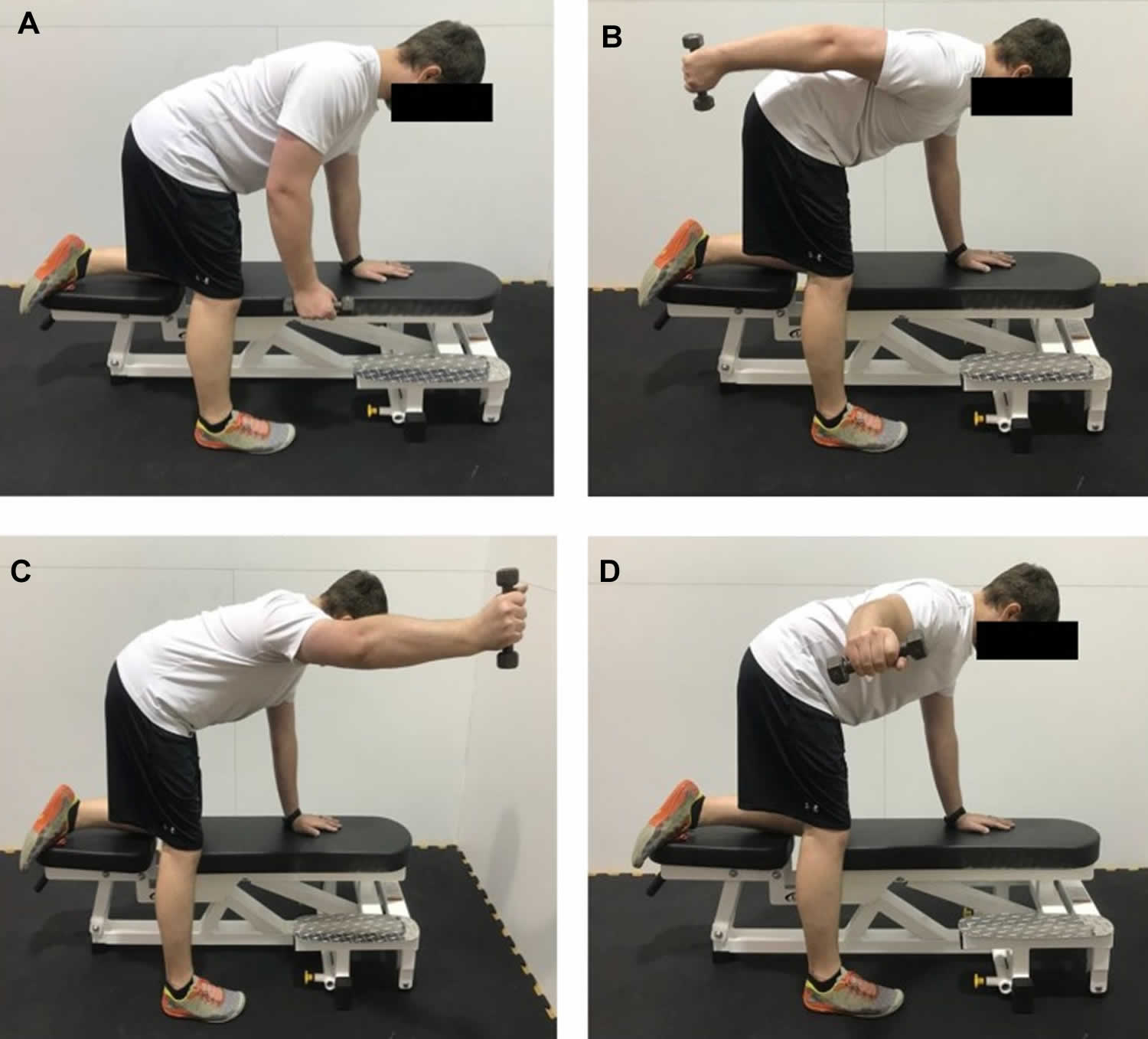
Footnote: Demonstration of prone shoulder extension, abduction, and horizontal abduction in the (A) start position; (B) end position for extension; (C) end position for abduction; (D) end position for horizontal abduction. The goal in performing these exercises is to keep the scapula flush against the rib cage while moving through the various shoulder motions. This shows a modified version, utilizing a bench if a table is not available.
Figure 7. Thoracic outlet syndrome exercise – frontal raise and lateral raise
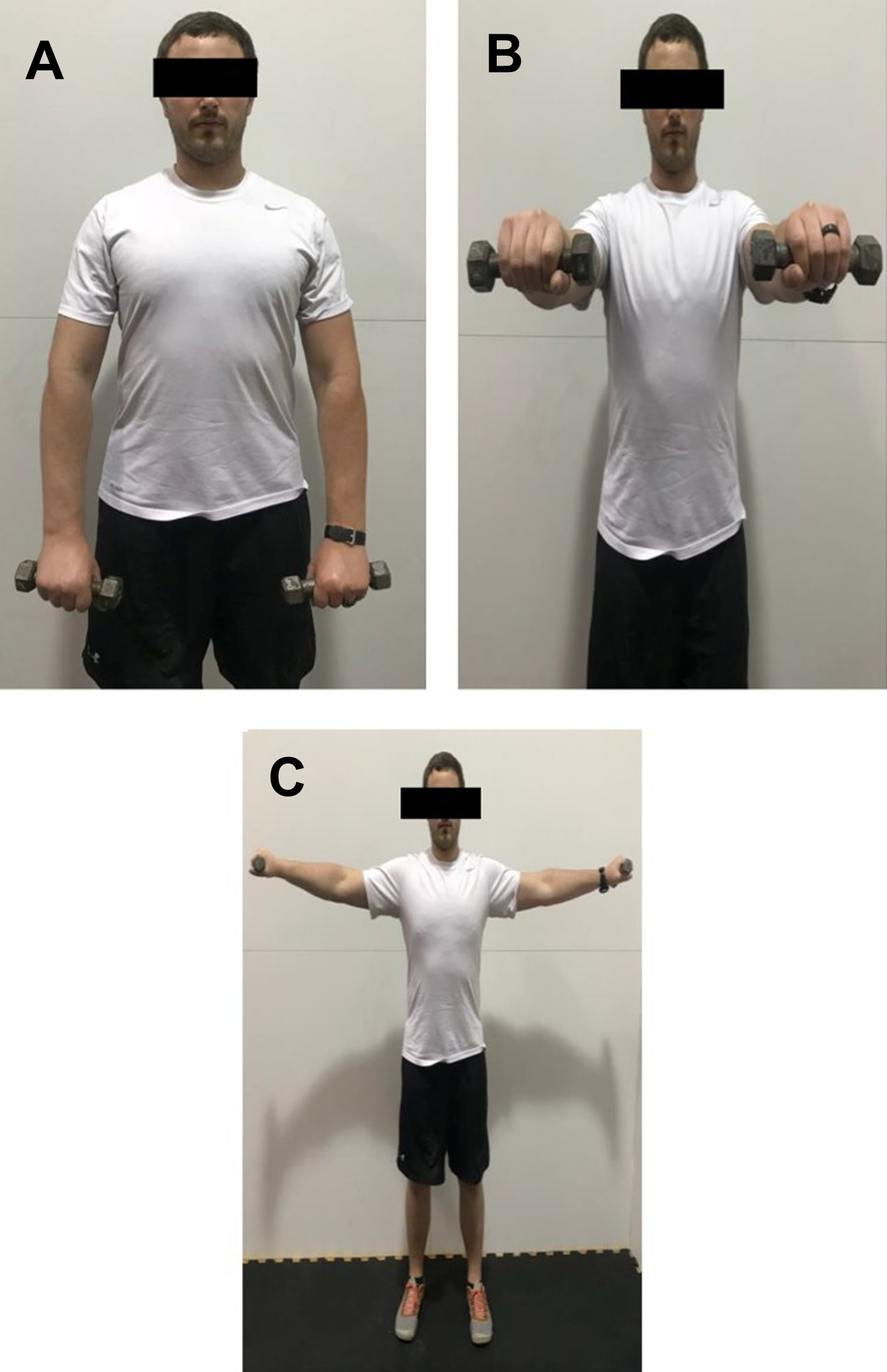
Footnote: Demonstration of frontal raise and lateral raise in the (A) start position; (B) end position for frontal raise; (C) end position for lateral raise. Brace the abdominal muscles and slowly raise and lower the weight.
Figure 8. Thoracic outlet syndrome exercise – serratus push

Footnote: Demonstration of serratus push in the (A) start position; (B) end position. Hold the bar further than shoulder width. The goal is to avoid excessive horizontal adduction, while keeping the arms straight and pushing the bar upwards.
Figure 9. Thoracic outlet syndrome exercise – chin tuck

Footnote: Demonstration of chin tuck in the (A) start position; (B) end position. The goal is to tuck the chin and “push” the chin into the body.
Thoracic outlet syndrome surgery
Your doctor may recommend surgery if other treatment hasn’t been effective, if you’re experiencing ongoing symptoms or if you have progressive neurological problems.
A surgeon trained in chest (thoracic) surgery or blood vessel (vascular) surgery will perform the procedure.
Thoracic outlet syndrome surgery has risks of complications, such as injury to the brachial plexus. Also, surgery may not relieve your symptoms, and symptoms may recur.
Surgery to treat thoracic outlet syndrome, called thoracic outlet decompression, may be performed using several different approaches, including:
- Transaxillary approach. In this surgery, your surgeon makes an incision in your chest to access the first rib, divide the muscles in front of the rib and remove a portion of the first rib to relieve compression. This approach gives your surgeon easy access to the first rib without disturbing the nerves or blood vessels. But, that only gives your surgeon limited access and makes it harder to see muscles and cervical ribs that may be contributing to compression behind the nerves and blood vessels.
- Supraclavicular approach. This operation, is performed through a three-inch incision above the clavicle (or collarbone) and this approach repairs compressed blood vessels. Your surgeon makes an incision just under your neck to expose your brachial plexus region. Your surgeon then looks for signs of trauma or muscles contributing to compression near your first (uppermost) rib. Your surgeon may remove the muscles causing the compression and repair compressed blood vessels. Your first rib may be removed if necessary to relieve compression. Patients stay in the hospital for about two to three days after the operation and resume physical and occupational therapy afterwards.
- Infraclavicular approach. In this approach, your surgeon makes an incision under your collarbone and across your chest. This procedure may be used to treat compressed veins that require extensive repair.
Some patients have symptoms primarily at the pectoralis minor area below the clavicle (or collarbone). These individuals may benefit from division of the pectoralis minor muscle, either in addition to, or instead of, thoracic outlet decompression. This operation is performed through a two-inch incision in the armpit (axilla). Patients are usually discharged home the same day as the procedure.
In venous or arterial thoracic outlet syndrome, your surgeon may deliver medications to dissolve blood clots prior to thoracic outlet compression. Also, in some cases, your surgeon may conduct a procedure to remove a clot from the vein or artery or repair the vein or artery prior to thoracic outlet decompression.
If you have arterial thoracic outlet syndrome, your surgeon may need to replace the damaged artery with a section of an artery from another part of your body (graft) or an artificial graft. This procedure may be done at the same time as your procedure to have the first rib removed.
Home remedies
If you’re diagnosed with thoracic outlet syndrome, your doctor or physical therapist will instruct you to do exercises at home to strengthen and support the muscles surrounding your thoracic outlet.
In general, to avoid unnecessary stress on your shoulders and muscles surrounding the thoracic outlet:
- Maintain good posture
- Take frequent breaks at work to move and stretch
- Maintain a healthy weight
- Avoid carrying heavy bags over your shoulder
- Avoid activities that worsen symptoms, or find ways to adapt activities so that they don’t cause symptoms
- Create a work area that allows you to keep good posture and doesn’t make symptoms worse.
- Huang J.H., Zager E.L. Thoracic Outlet Syndrome. Neurosurgery. 2004;55:897–903. doi: 10.1227/01.NEU.0000137333.04342.4D
- Heneghan N., Smith R., Tyros I., Falla D., Rushton A. Thoracic Dysfunction in Whiplash Associated Disorders: A Systematic Review. PLoS ONE. 2018;13:e0194235 doi: 10.1371/journal.pone.0194235
- Wiangkham T., Duda J., Haque S., Madi M., Rushton A. The Effectiveness of Conservative Management for Acute Whiplash Associated Disorder (WAD) II: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. PLoS ONE. 2015;10:1–22. doi: 10.1371/journal.pone.0133415
- Watson L.A., Pizzari T., Balster S. Thoracic Outlet Syndrome Part 2: Conservative Management of Thoracic Outlet. Man. Ther. 2010;15:305–314. doi: 10.1016/j.math.2010.03.002
- Levine NA, Rigby BR. Thoracic Outlet Syndrome: Biomechanical and Exercise Considerations. Healthcare (Basel). 2018;6(2):68. Published 2018 Jun 19. doi:10.3390/healthcare6020068 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6023437/
- Yu J., Ackland D.C., Pandy M.G. Shoulder Muscle Function Depends on Elbow Joint Position: An Illustration of Dynamic Coupling in the Upper Limb. J. Biomech. 2011;44:1859–1868. doi: 10.1016/j.jbiomech.2011.04.017
- Vanti C., Natalini L., Romeo A., Tosarelli D., Pillastrini P. Conservative Treatment of Thoracic Outlet Syndrome: A Review of Literature. Eura Medicophys. 2007;43:55–70
- Hanif S., Tassadaq N., Rathore M.F.A., Rashid P., Ahmed N., Niazi F. Role of Therapeutic Exercises in Neurogenic Thoracic Outlet Syndrome. J. Ayub Med. Coll. Abbottabad. 2007;19:85–88





{kind=link}