
Trichilemmoma
Trichilemmoma also called tricholemmoma, is a benign (non-cancerous) tumor originating from the outer root sheath of the hair follicle. When it is characterized by a central zone of desmoplasia, it is called desmoplastic trichilemmoma 1. Desmoplastic trichilemmomas is a rare histological variant of trichilemmoma predominantly occur in white men over a wide age range, and the highest frequency is in the fifth decade.
Trichilemmomas are relatively common benign neoplasms of the follicular epithelium. Trichilemmoma diagnosis depends on careful histopathological examination of a skin biopsy.
Trichilemmomas predominantly occur in adult patients aged 20-80 years. However, onset may occur as early as age 4 years, with a median age of onset at 30 years 2.
Trichilemmoma often occurs alongside other skin lesions such as trichoblastoma, sebaceous adenoma and sebaceous nevus. Occasionally trichilemmoma may appear as a new growth within a sebaceous nevus lesion.
Multiple trichilemmoma on the face is often associated with Cowden disease, a rare inherited condition characterized by multiple types of skin tumours which can be found throughout different body systems. Although multiple trichilemmoma associated with Cowden disease is very rare, it is important to re-evaluate patients for this disease if a diagnosis of trichilemmoma is confirmed.
Trichilemmoma true incidence is hard to determine and is probably underestimated. Approximately 40 cases per 100,000 consecutive skin biopsies may be found every year in any given dermatopathologic laboratory. Unlike isolated trichilemmomas, multiple trichilemmomas associated with Cowden disease are very rare.
The underlying cause of trichilemmoma is unknown but because of its similarity to a viral wart/verruca, it has been postulated that it may come from a viral infection such as the human papillomavirus (HPV). To date there is no evidence for this.
Desmoplastic trichoepithelioma
Desmoplastic trichoepithelioma is a harmless facial skin lesion. It is an uncommon form of trichoepithelioma, with a reported incidence of 1 in 5000 skin biopsies in a cohort of British adults. It has also been called ‘sclerosing epithelial hamartoma’.
Desmoplastic trichoepithelioma grows from cells lining the hair follicle. It is classified as a benign adnexal or hair follicle tumor.
Desmoplastic trichoepithelioma is most often identified in middle-aged females, although it may also occur at other ages and in males. A lesion may have been present for many years before being brought to medical attention.
Desmoplastic trichoepithelioma typically present as a firm skin-colored to red, annular (ring-shaped) plaque with a central dimple. It is usually found on the upper cheek. Desmoplastic trichoepithelioma is stable or may slowly grow up to 1 cm in diameter. Multiple lesions are quite rare.
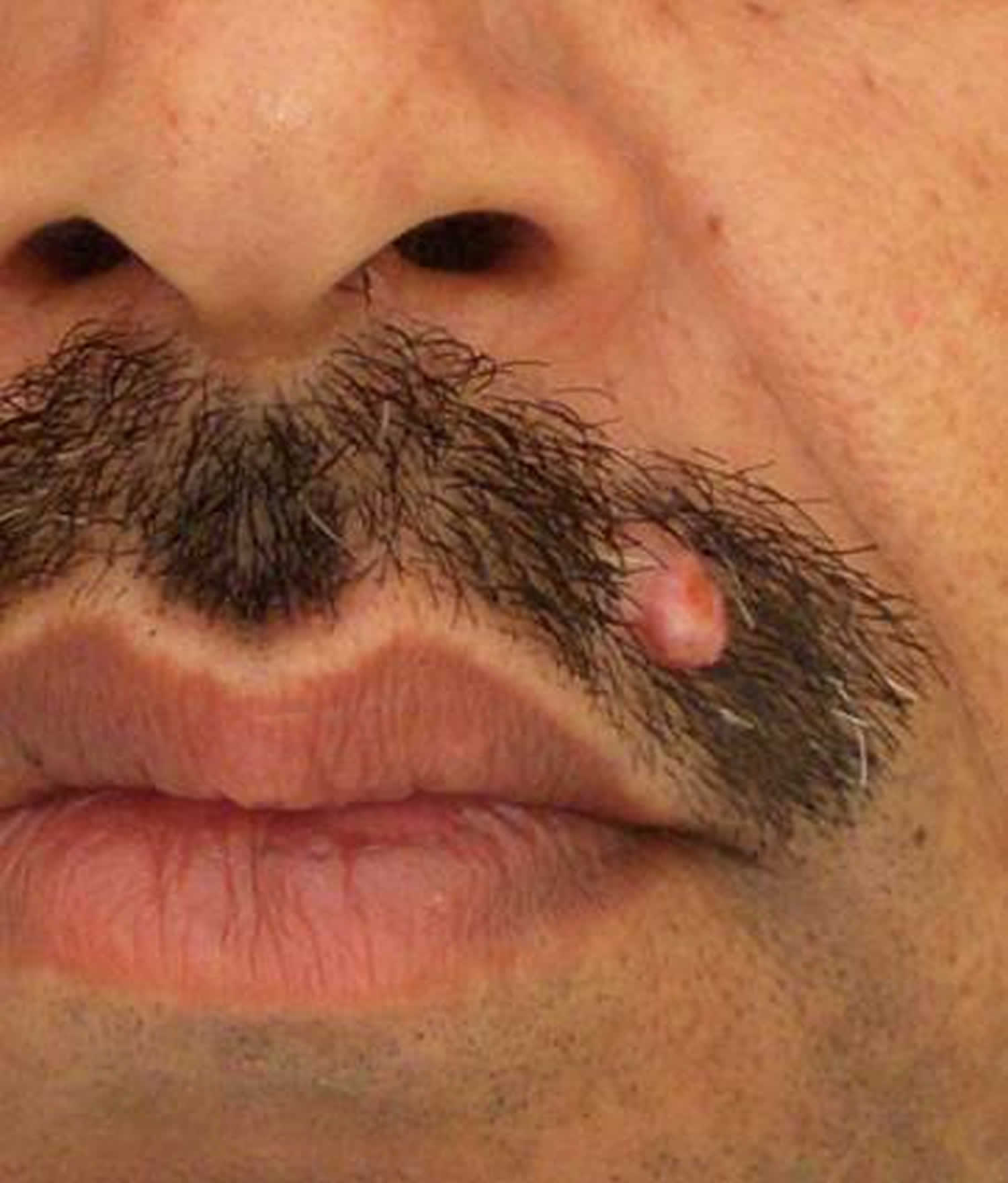
Figure 1. Desmoplastic trichilemmoma
Desmoplastic trichoepithelioma diagnosis
Desmoplastic trichoepithelioma is diagnosed on full-thickness skin biopsy. Small incomplete biopsies may cause uncertainty, as sclerosing basal cell carcinoma and microcystic adnexal carcinoma may appear similar. Resampling or re-excision may be necessary for the definitive diagnosis or complete eradication in uncertain cases.
Desmoplastic trichoepithelioma treatment
True desmoplastic trichoepithelioma is a benign tumor with no malignant potential, so there is no need to remove them. However, it is best to keep the lesion under observation in case the diagnosis is incorrect, as basal cell carcinoma may look very similar.
Treatment options include:
- Curettage and electrodesiccation
- Surgical excision
- Mohs micrographic surgery, which ensures clear margins.
What causes trichilemmoma?
The cause of a trichilemmoma is unknown. Because trichilemmoma shares some morphologic and histologic features with a verruca, some researchers have postulated that a virus may induce these lesions. Increased risk has also been found when subjects have a history of long exposure to sunlight 3.
Trichilemmoma symptoms
Trichilemmoma typically presents as a solitary papule or mass of small skin-colored papules that are 1-5 cm in diameter. These lesions slowly grow over time and tend to form small plaques that may resemble a wart/verruca or a cutaneous horn. They most commonly occur around the central part of the face, ears and neck, but also occur on the forearms and hands.
Solitary trichilemmomas are relatively common benign follicular tumours and occur in both male and females usually between 20-80 years of age. Desmoplastic trichilemmomas, a subtype of trichilemmoma, mainly occurs in white males around 50 years old. Lesions of this subtype are usually less than 1 cm in diameter and occur mainly on the face, neck and scalp, and sometimes on the chest and vulva.
Trichilemmoma diagnosis
A small biopsy (when a tiny piece of skin is removed under local anaesthetic) is the only definitive diagnosis for trichilemmoma. The histology of trichilemmoma will differentiate it from other skin tumours that have similar clinical presentations, such as trichoepithelioma, trichofolliculoma and basal cell carcinoma.
Where there are multiple lesions on the face, once a diagnosis of trichilemmoma is confirmed, patients should be completely examined for evidence of Cowden disease.
Trichilemmoma treatment
Trichilemmoma is a benign follicular tumour that requires no treatment. Occasionally lesion(s) may be removed for cosmetic reasons or if they occur in functionally sensitive areas. The main reason for surgery is to establish the correct diagnosis and to ensure that a potential malignancy, such as trichilemmal carcinoma, is not left untreated.
Treatment options include.
- curettage and electrodesiccation
- surgical excision
- Mohs micrographic surgery .
- carbon dioxide laser therapy.
Trichilemmoma prognosis
Trichilemmomas are benign follicular epithelial neoplasms. Of themselves, trichilemmomas are associated with minimal morbidity and no mortality. These tumors usually need to be differentiated clinically from a verruca or a basal cell carcinoma. The only morbidity associated with these tumors occurs if they are treated as a basal cell carcinoma before histologic confirmation is obtained.
References- Jardim MML, Souza BCE, Fraga RC, Fraga RC. Rare desmoplastic trichilemmoma associated with sebaceous nevus. An Bras Dermatol. 2017;92(6):836–837. doi:10.1590/abd1806-4841.20176540 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5786400
- Umemura K, Takagi S, Ishigaki Y, Iwabuchi M, Kuroki S, Kinouchi Y. Gastrointestinal polyposis with esophageal polyposis is useful for early diagnosis of Cowden’s disease. World J Gastroenterol. 2008 Oct 7. 14(37):5755-9.
- Lee CA, Kang SJ, Jeon SP, Sun H, Kang MS. Simultaneous Development of Three Different Neoplasms of Trichilemmoma, Desmoplastic Trichilemmoma and Basal Cell Carcinoma Arising from Nevus Sebaceus. Arch Craniofac Surg. 2017 Mar. 18 (1):46-49.





{kind=link}