
What is tympanometry
Tympanometry also called tympanometry impedance testing, is a clinical test measuring tympanic membrane mobility to detect problems in the middle ear and is graphically displayed as a tympanogram. Tympanometry provides information on acoustic admittance, which is a measure of the ease with which energy flows through the middle ear system, and impedance, which is the opposition to this flow 1. The tympanogram is a measure of middle ear function and can help differentiate many pathologic conditions. The measurements of acoustic admittance at various pressure points are graphed to form a tympanogram 2. Combined with otoscopy, tympanometry is an objective, fast, and highly accurate way to rule out outer and middle ear pathology.
Tympanometry provides information about the stiffness, mass and resistance of the middle ear (often described as mobility of the tympanic membrane) 3. Tympanometry procedure can be used to describe normal or abnormal middle ear function in response to sound and air pressure 4. Tympanometry is used in conjunction with otoscopy and audiometry, to identify deviations from normal such as the presence of middle ear fluid, tympanic membrane perforation and eustachian tube dysfunction, which have the potential to impact on hearing.
Tympanometry is part of a complete test battery and outcomes from other audiological tests should be considered in conjunction with tympanometry results.
Tympanometry test usually commences from when the infant is eight (8) months of age.
Before the test, your health care provider will look inside your ear to make sure nothing is blocking the eardrum (otoscopy examination).
Next, a device is placed into your ear. This device changes the air pressure in your ear and makes the eardrum move back and forth. A machine records the results on graphs called tympanograms.
If any of the following deviations are identified, tympanometry will not be undertaken:
- Within six (6) weeks of ear surgery, or in accordance with medical professional direction.
- Ear pain.
- Tympanic membrane is inflamed, bulging or perforated.
- Evidence of discharge or foreign objects in the auditory canal.
A tympanometry and tympanogram (chart) provide information about:
- Middle ear pressure – the air pressure of the air contained within the middle ear, displayed as the “peak” of the tympanometric trace along the pressure axis. Normal middle ear pressure value for children are +50 daPa to -200 daPa
- Compliance – refers to how well the middle ear system responds to sound, displayed by the height of the “peak”. Normal middle ear compliance values range from 0.3 to 1.5 mL
- Equivalent volume of the ear canal – this value is reported by the tympanometer (not shown on the tympanogram). In children a volume range of 0.5 to 1.5 mL is considered normal.
- An otoscopy examination is always performed prior to tympanometry. If any of the following deviations are identified, tympanometry will not be undertaken:
- Within six (6) weeks of ear surgery, or in accordance with medical professional direction.
- Ear pain.
Figure 1. Ear anatomy
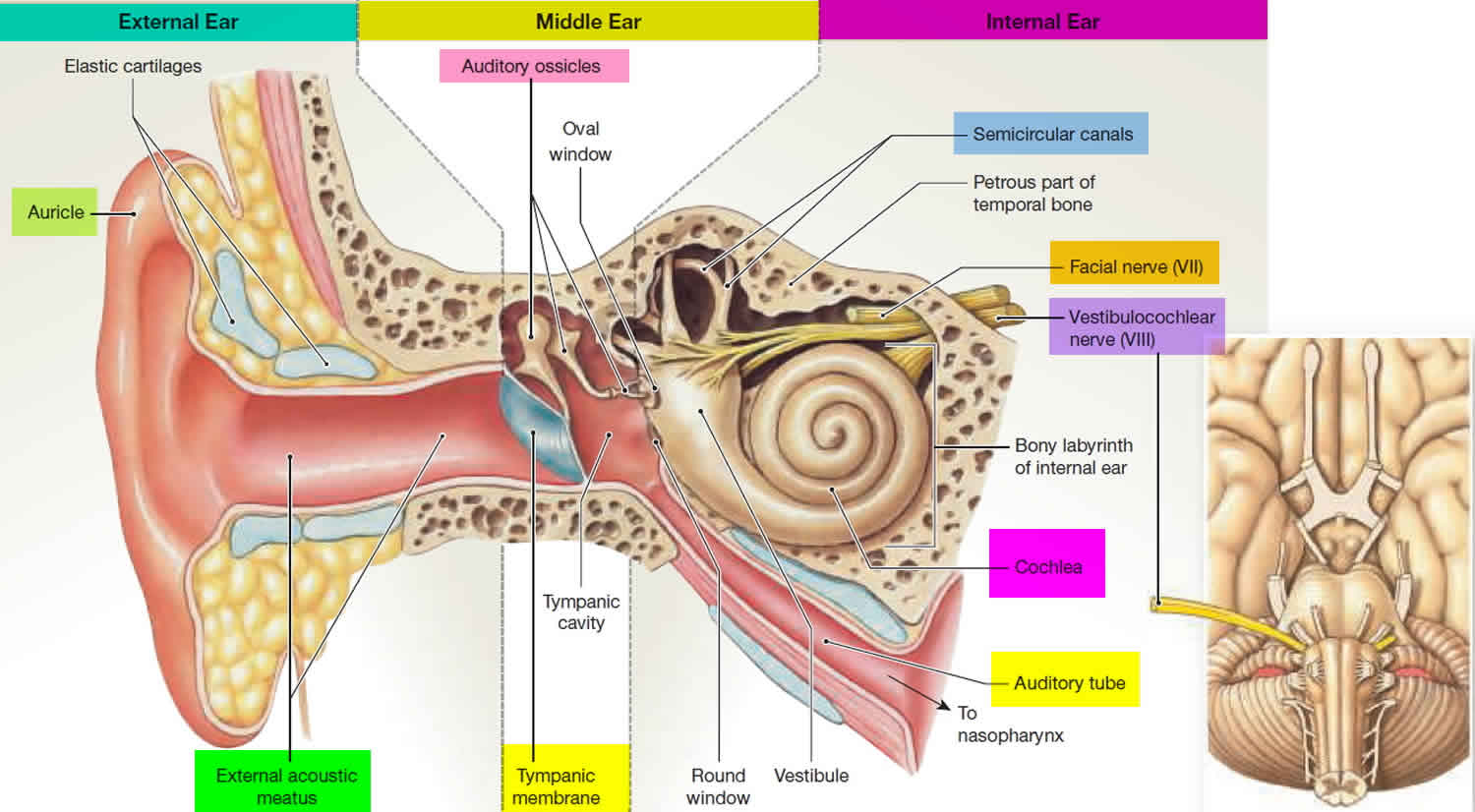
Figure 2. Middle ear anatomy
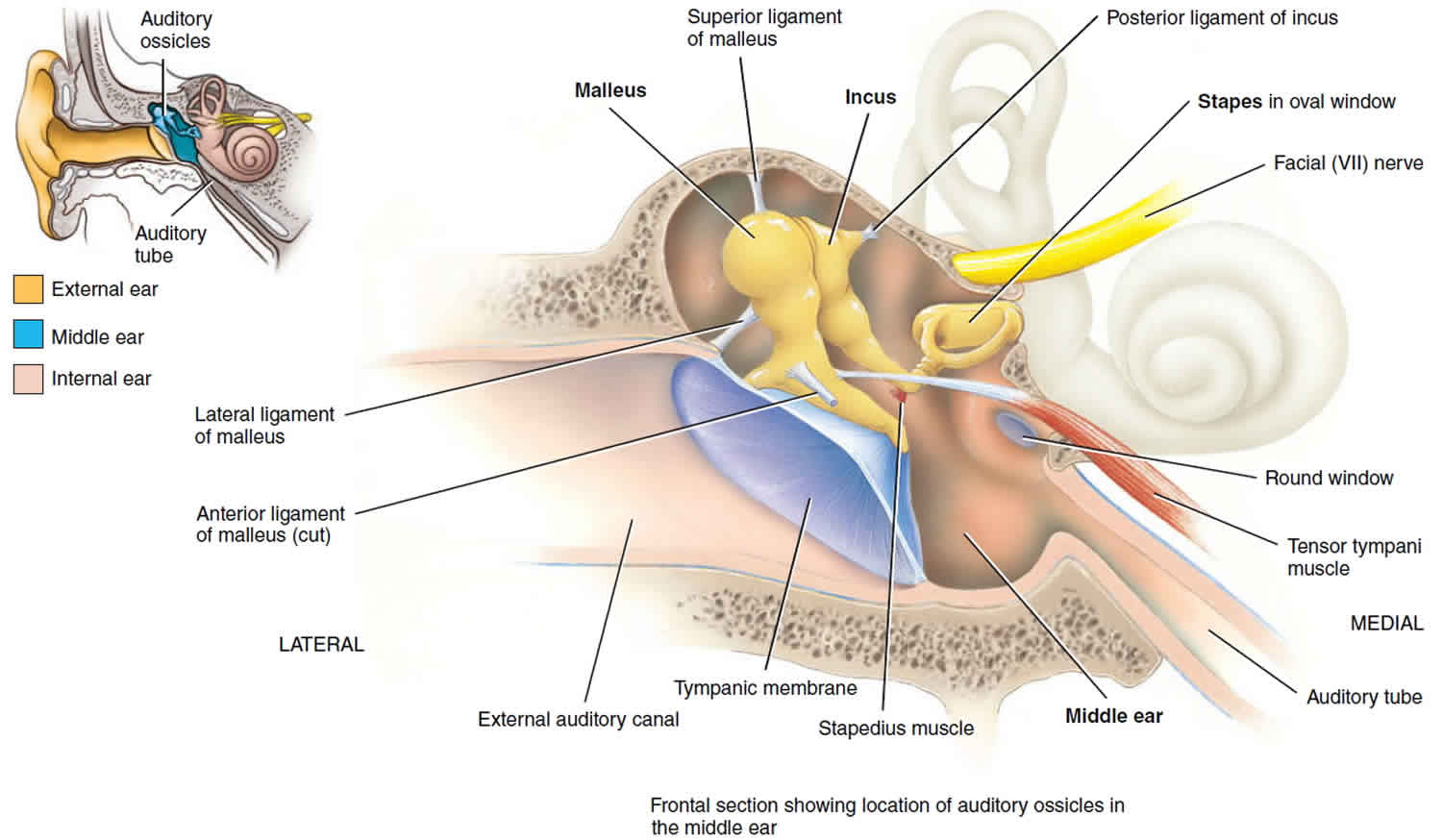
Figure 3. Tympanometry test
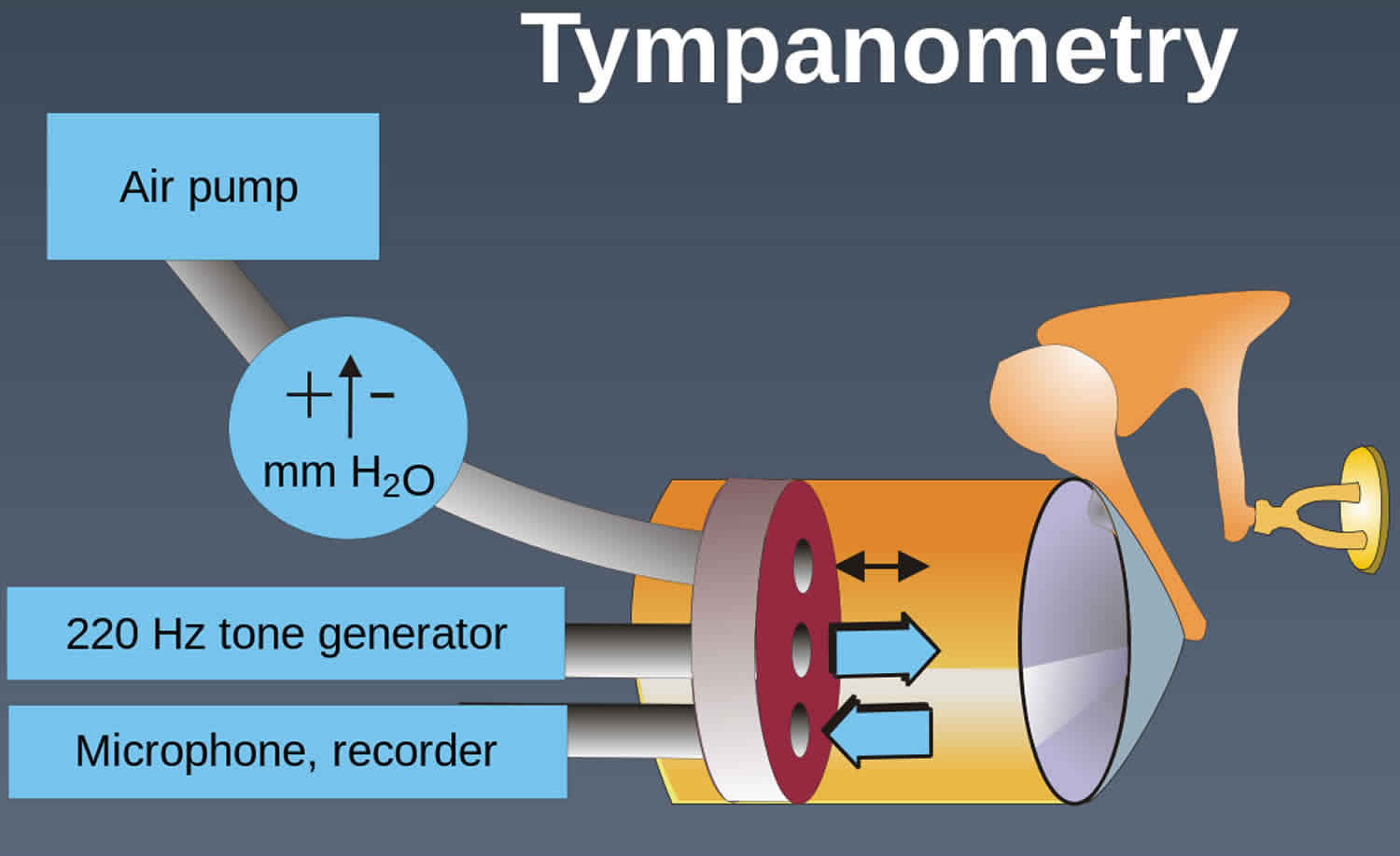
Tympanometry test
Before examination, the subject (or the person responsible for the subject) should be asked if he/she currently has any ear-related symptoms (including discomfort, pain and discharge), is currently being treated for any ear-related problems or has previously had surgery involving the ears. Any symptoms, or other relevant issues, should be explored through questioning as appropriate.
Tympanometry shall be preceded by otoscopic examination to ensure that there are no contraindications to continue.
You should not move, speak, or swallow during the test. Such movements can change the pressure in the middle ear and give incorrect test results.
Young children may need to be held by an appropriate adult, which should be the person responsible for the child. For example, the child could be seated sideways on the adult’s lap, with the child’s hands secured by one hand and the child’s head held against the chest with the other hand. In older children and adults, an instruction to remain still will usually suffice. Any objects that may interfere with insertion of the probe (e.g. a hearing aid) should be removed.
The sounds heard during the test may be loud. This may be startling. You will need to try very hard to stay calm and not get startled during the test. If your child is to have this test done, it may be helpful to show how the test is done using a doll. The more your child knows what to expect and why the test is done, the less nervous your child will be.
How the tympanometry test will feel
There may be some discomfort while the probe is in the ear, but no harm will result. You will hear a loud tone and feel pressure in your ear as the measurements are taken.
Eustachian tube function testing
Eustachian tube function testing can be implied by tympanograms. Type A tympanograms reflect normal middle ear pressure with an intact tympanic membrane. This situation only occurs if the eustachian tube is ventilating the middle ear. Similarly, type C tympanograms show significant negative middle ear pressure, implying eustachian tube dysfunction.
In patients with perforated tympanic membranes, type B tympanograms disclose high-volume readings and no information on eustachian tube dysfunction. However, in these patients pressure in the ear canal can be increased via the probe in the ear canal. Instruct the patient to swallow several times or yawn to determine if the eustachian tube can clear the pressure.
Several types of eustachian tube function testing exist and can be useful in evaluating function for divers or in evaluating the efficacy of treatments to improve eustachian tube dysfunction 5.
Perilymphatic fistula testing
Assessment involves the outer, middle, and inner ear. Testing implies presence or absence of a fistula (ie, an abnormal opening in the inner ear labyrinthine system).
Variation of ear canal pressure by the immittance probe (from +200 to -400 daPa) elicits a response. If vertigo or nystagmus occurs (Hennebert sign), the test result is positive.
The accuracy of this test in distinguishing symptomatic patients with patent fistulas from those without is questionable.
Acoustic reflex decay test
The acoustic reflex decay test is used to assess the integrity of cranial nerve 8 (CN VIII or vestibulocochlear nerve). In acoustic reflex testing, the probe tip produces a sudden loud tone and simultaneously records any drop in compliance. If the compliance drops, the tympanometer records the acoustic reflex as present. Interpret as no conductive component, and not more than moderately severe hearing loss If compliance is not affected, the tympanometer records the reflex as absent. Subject to wide range of interpretation.
Using a stimulus of either 500 or 1000 Hz, a contralateral continuous tone is presented for 10 seconds at a stimulus level 10 dB above the acoustic reflex threshold for that stimulus frequency in that ear.
This suprathreshold acoustic reflex then is recorded over the 10-second stimulation period.
If the amplitude of the recorded deflection on the screen decreases by 50% or more within 10 seconds, the test is considered positive. Positive findings on this test may suggest a retrocochlear lesion (eg, vestibular schwannoma, acoustic neuroma) 6.
In some cases of muscular or neuromuscular disorder, tone decay results also may be positive secondary to muscle fatigue.
Tympanometry results
Tympanometric results do not identify pathology uniquely and should be interpreted in the context of other information from the complete test battery being conducted and with particular regard to the otoscopic findings and history 7.
Where spurious results or artefacts are suspected, the test should be repeated and the probe tip should be inspected to ensure it is not blocked, for example by wax. These include flat traces, traces with more than one peak, changes in ear-canal volume during testing, noisy traces and ear-canal volumes that are significantly higher or lower than expected.
Tympanometry normal values
The pressure inside the middle ear can vary by a very small amount. The eardrum should look smooth.
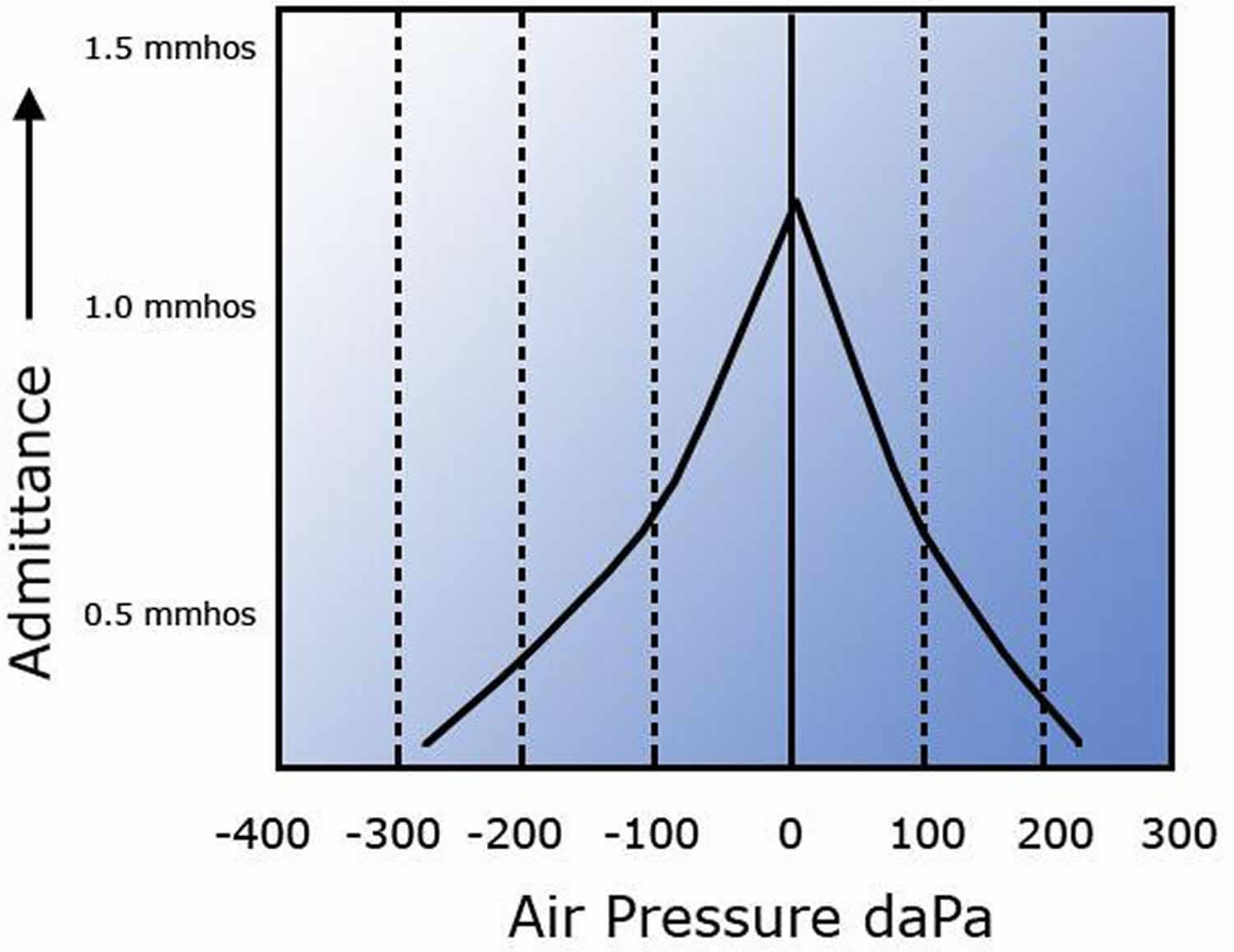
- See Figure 4 below for an illustration of a normal adult tympanogram.
- See Figure 5 below for an illustration of a normal children below 6 months of age tympanogram.
Typical Normative Data for an Adult (British Society of Audiology Guidelines 2013 corrected 2014) 8
- Admittance / Compliance between 0.3 to 1.6 cm³ (‘Y’ Axis)
- Middle Ear Pressure +50 to -50 daPa (Deca Pascal) (‘X’ Axis)
- Ear Canal Volume (ECV) 0.6 to 2.5 cm³
The tympanogram report should include the measurements obtained for middle-ear pressure, admittance or compliance, and ear-canal volume (ECV). Ear-canal volume (ECV) is particularly important where a flat trace is seen in order to identify a possible open perforation and exclude blockage or incorrect placement of the probe (i.e. against the wall of the ear canal). The shape of the tympanogram should also be described and simple descriptions such as ‘normal’, ‘rounded’, ‘flat’, ‘wide’ or ‘W-shaped’ are acceptable 9. In the case of rounded or wide traces, a tympanometric width measurement may also be included for subjects aged between 1 and 7 years. If the tympanogram is flat, or nearly flat, middle-ear pressure may be reported as ‘indeterminate’.
The use of classification systems 10 of tympanograms according to their shape is not recommended since this can lead to confusion or mistakes, and it is also possible that not all parties receiving a copy of the report will be familiar with the classification system used. However, the Jerger system is the most commonly used classification system for tympanograms. While other systems have been proposed, none are in as widespread of clinical use.
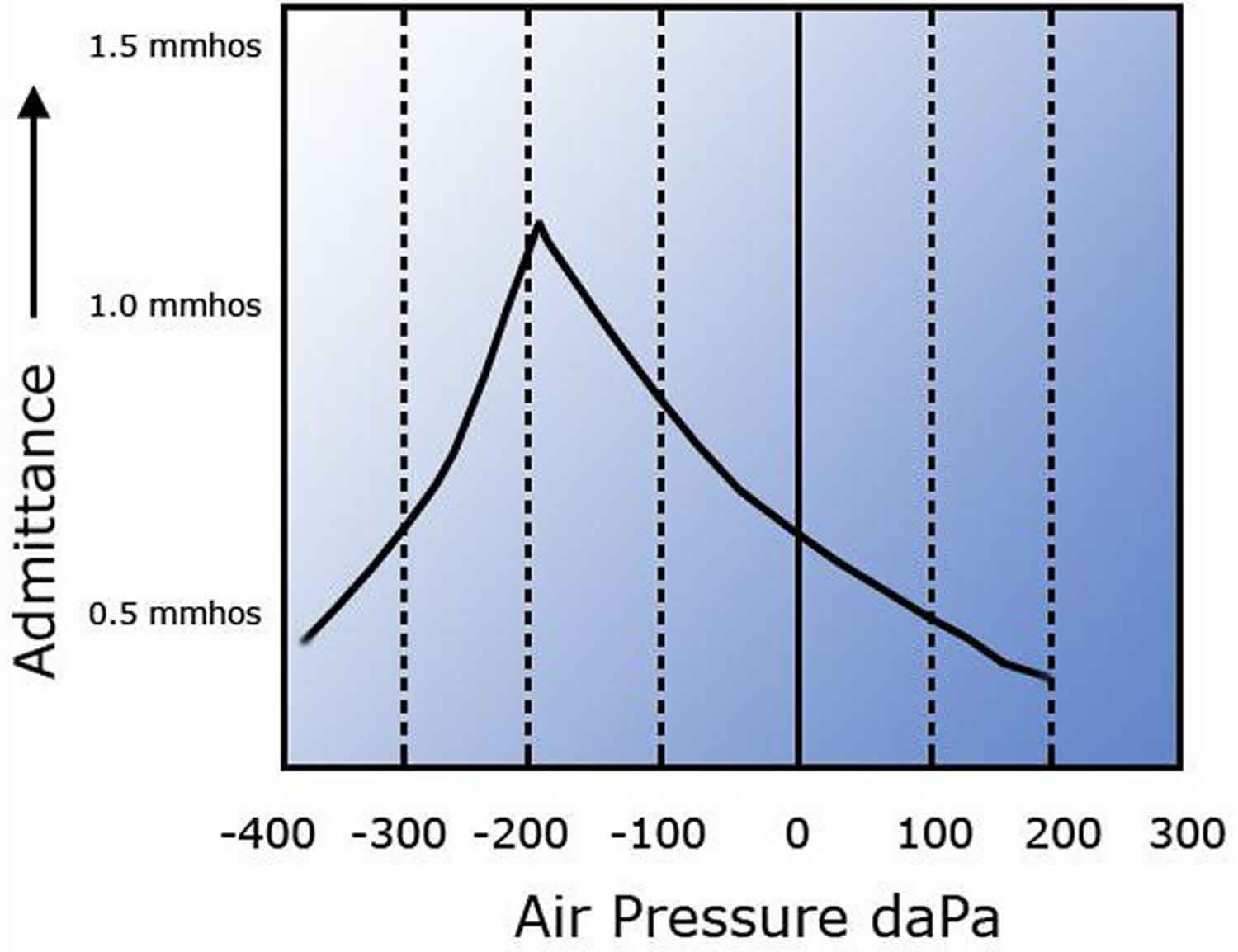
A type A response suggests normal middle ear function, but it occurs in some otosclerotic ears, particularly in early stages. Compliance peak is -150 to +100 daPa, and immittance is 0.2-2.5 millimhos (mmhos) (see Figure 5 below).
Tympanometric shape
The trace should have a single sharp peak, as in Figure 4. Double peaks may be seen when there is scarring on the eardrum, but should be repeated to exclude artefacts. Rounded or wide peaks should also be repeated. The tympanometric width (width at 50 % height) may be used as a descriptor, in which case a value of less than 200 daPa may be considered normal for children between 1 and 7 years of age 11.
Tympanic peak pressure and middle ear pressure
Tympanic peak pressure is the value on the horizontal axis of the tympanogram at which the peak occurs. This is used to estimate the middle-ear pressure. Tympanometry overestimates ear canal volume by as much as 24–39 % 12. Using descending sweeps and slower sweep speeds minimizes this effect. Tympanogram peak pressure can overestimate middle ear pressure by 30–70 daPa, particularly with small middle ear volumes or hypermobile tympanic membranes 13, and when higher sweep speeds are used. Hysteresis is the term for the displacement of the pressure peak in the direction of the sweep, and is greater at higher sweep speeds. Normal middle-ear pressure has a mean value of zero. Under carefully controlled conditions the 95% range in normal subjects is –20 to +20 daPa, though pressures from –50 to +50 daPa can be considered normal in adults; pressures down to –100 daPa may be of little clinical significance in isolation. Children often have slightly low middle-ear pressures; pressures down to –200 daPa may have little clinical significance (normal middle ear pressure peaks (+50 daPa to -200 daPa) for children).
Admittance or compliance
Admittance or compliance is the quantity on the vertical axis. Middle-ear admittance or compliance is the peak value of admittance or compliance, assuming that the contribution of the ear canal has been removed (sometimes referred to as ‘corrected’ or ‘compensated’) as is usually the case by default. Middle-ear admittance or compliance is normally in the range 0.3 to 1.6 cm³ in adults; 0.2 cm³ is acceptable as the lower limit in children aged under 6 years but over 6 months. Note that the units ml, cm³ and mmho are interchangeable when using a 226-Hz probe tone.
Ear-canal volume
The acoustic properties of the ear canal (from probe tip to tympanic membrane) are necessarily involved in tympanometric measurements. Equivalent volume is the volume of an air-filled cavity having the same acoustic admittance (or impedance, compliance etc) as that of the component or system which it represents. One implication of this is that ear canal volume is not measured directly butinferred from the measurement of admittance.
At 226 Hz, the ear canal contributes an admittance (or compliance), which for practical purposes may be added arithmetically to the admittance presented by the middle ear as seen from the tympanic membrane. The canal and middle-ear components are distinguished by applying air pressure in tympanometry. Should the tip of the probe be occluded, for example by the wall of the canal, a seemingly small canal volume will be indicated, whereas an open perforation will add the middle-ear volume to that of the canal so giving an abnormally large result. Probe occlusion and an open perforation will both be accompanied by a flat tympanogram. Typical values for ear-canal volume (ECV) are between 0.6–2.5 cm³ for adults and 0.4-1.0 cm³ for children.
Figure 4. Normal adult tympanogram left ear (at least 6 months of age and above)
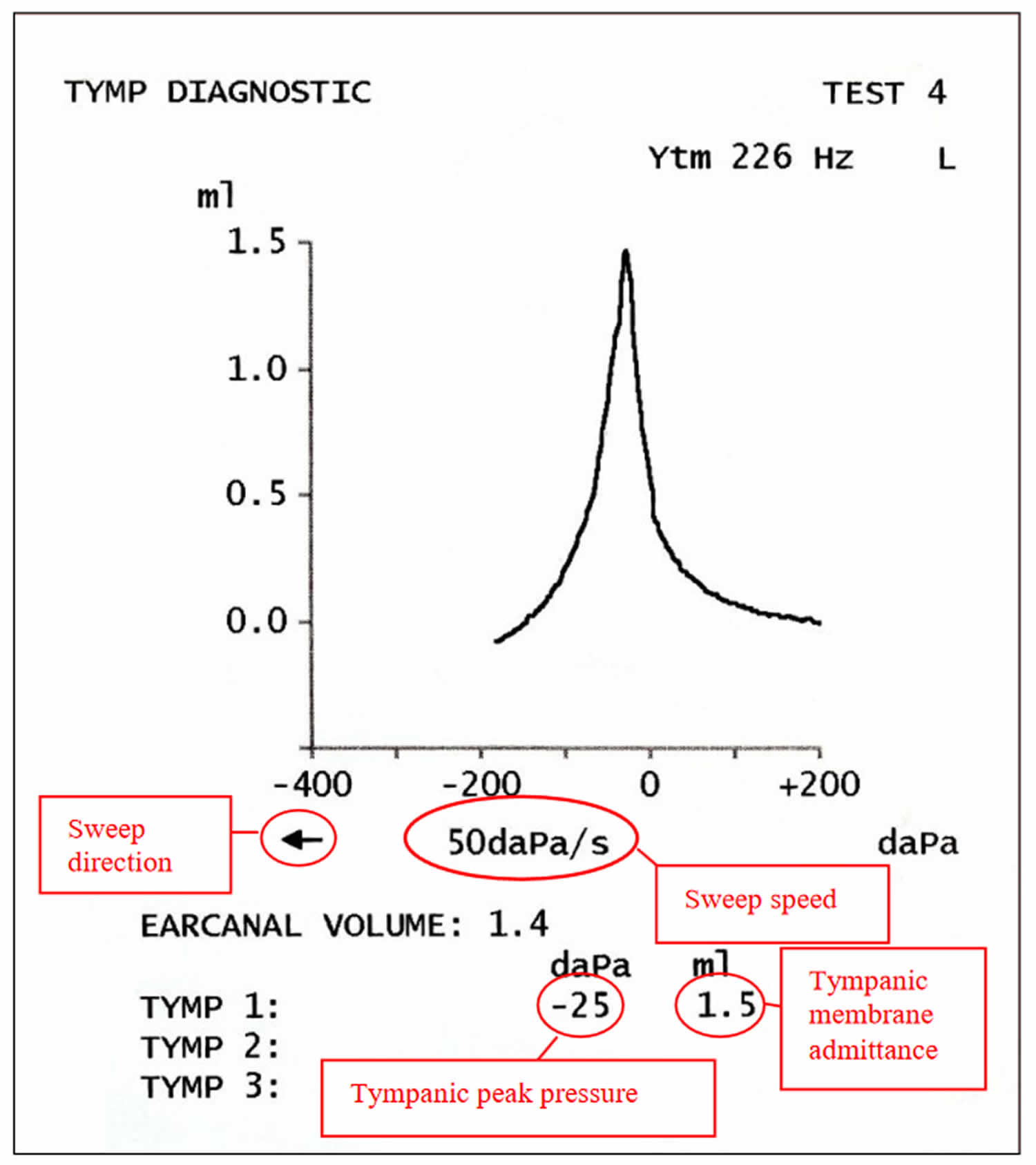
Figure 5. Type A tympanogram suggesting normal function
Subjects with a corrected age under 6 months using a 1000-Hz probe tone
The value of ear canal volume (ECV) should be disregarded when high-frequency probe tones are used because it will not be precise (at higher frequencies where it is not possible to accurately calculate cavity volumes. Without an accurate measure of volume it is not possible to calculate pressure, since pressure = density/volume). The exception is for use as an indicator of a possible blockage (i.e. very small volume given), although this should be verified (e.g. otoscopy or checking the probe).
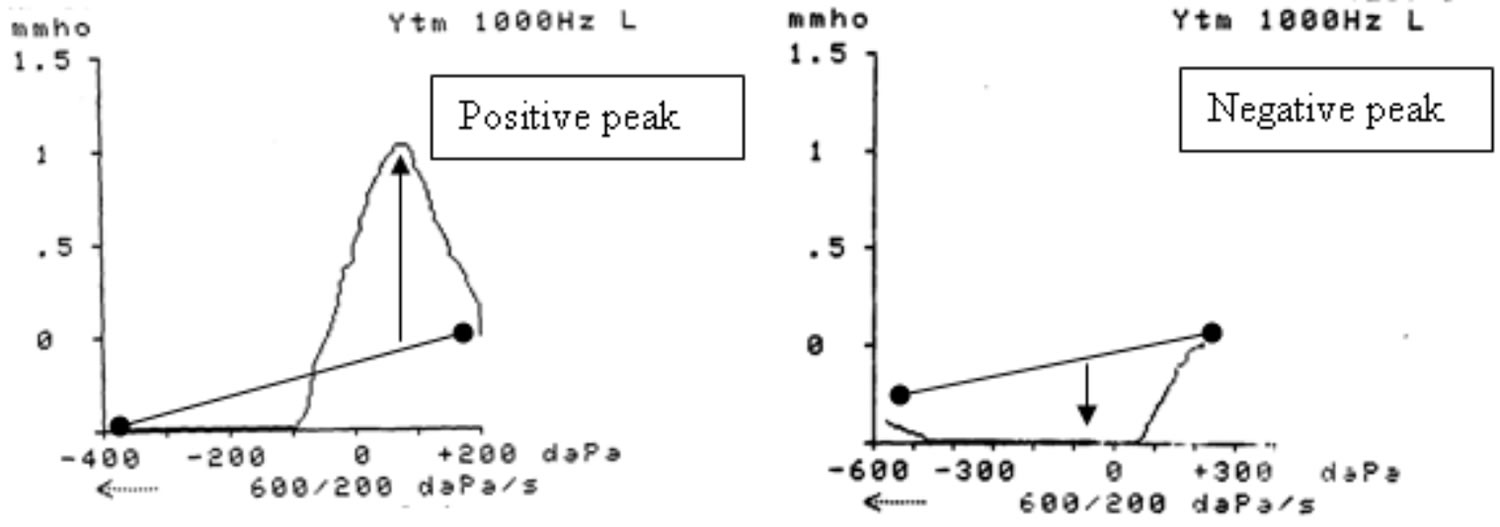
It is recommended that the traces recorded are classified as normal or abnormal using a classification system reported by Baldwin 14, see Figure 7:
- Draw a baseline on the trace at pressure extremes (–400/–600 to +200 daPa); if the trace disappears below the x axis, the baseline should be drawn to the x axis, as shown in Figure 7
- Identify the main peak which can occur at any middle-ear pressure
- Draw a vertical line from the baseline to the peak of the trace
- If the peak is above the baseline it is a positive peak and normal
- If the peak is below the baseline it is a negative peak and abnormal
- If there is a positive and negative peak the trace should be classified as positive (i.e. normal)
- A positive peak at a positive or negative middle-ear pressure is classified as normal, whereas a flat or “trough-shaped” i.e. negative peak is abnormal
If the conditions are good and the outcome is clear, repetition is not always necessary to draw a conclusion. However traces should usually be repeated if possible to check for reliability. Repeated traces should be classified in the same category of positive or negative. If the outcome is not clear the trace should always be repeated.
Figure 6. Normal children below 6 months of age tympanogram
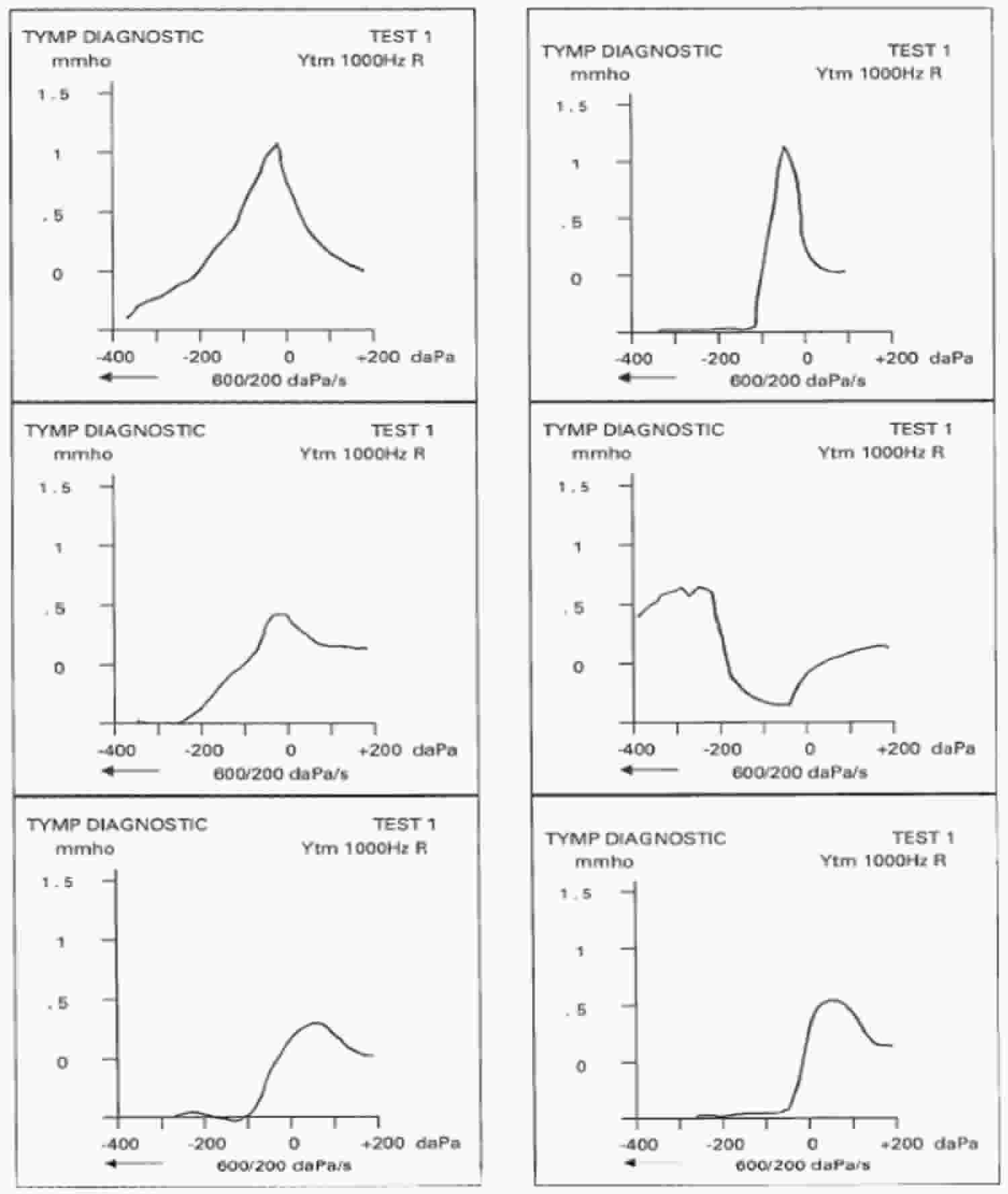
Figure 7. Examples of positive and negative peak tympanogram
Abnormal tympanometry results
Tympanometry may reveal any of the following:
- A tumor in the middle ear
- Fluid in the middle ear
- Impacted ear wax
- Lack of contact between the conduction bones of the middle ear
- Perforated eardrum
- Scarring of the eardrum
Tympanometry types
The following provides a broad interpretation of typical tympanograms by type and possible related pathologies and are based on Adult Probe Frequency 226Hz (i.e. at least 6 months from the child’s due date) and 1000 Hz for subjects below 6 months corrected age 8.
Type As tympanogram
Type As (A shallow) suggests a stiffened middle ear system. Compliance peak is -150 to +100 daPa, and immittance is less than 0.2 mmhos. This type may suggest a glue ear, a thickened or scarred eardrum, or otosclerosis (see Figure 8 below).
Figure 8. Type As (A shallow) tympanogram
Type Ad tympanogram
Type Ad (A deep) suggests a flaccid tympanic membrane, a middle ear system, or a disarticulation of middle ear ossicles. Usually a disarticulation of ossicles results in a compliance peak higher than the recording parameters (ie, off the chart). Compliance peak is -150 to +100 daPa, and immittance is more than 2.5 mmhos (see Figure 9 below).
Figure 9. Type Ad (A deep) tympanogram
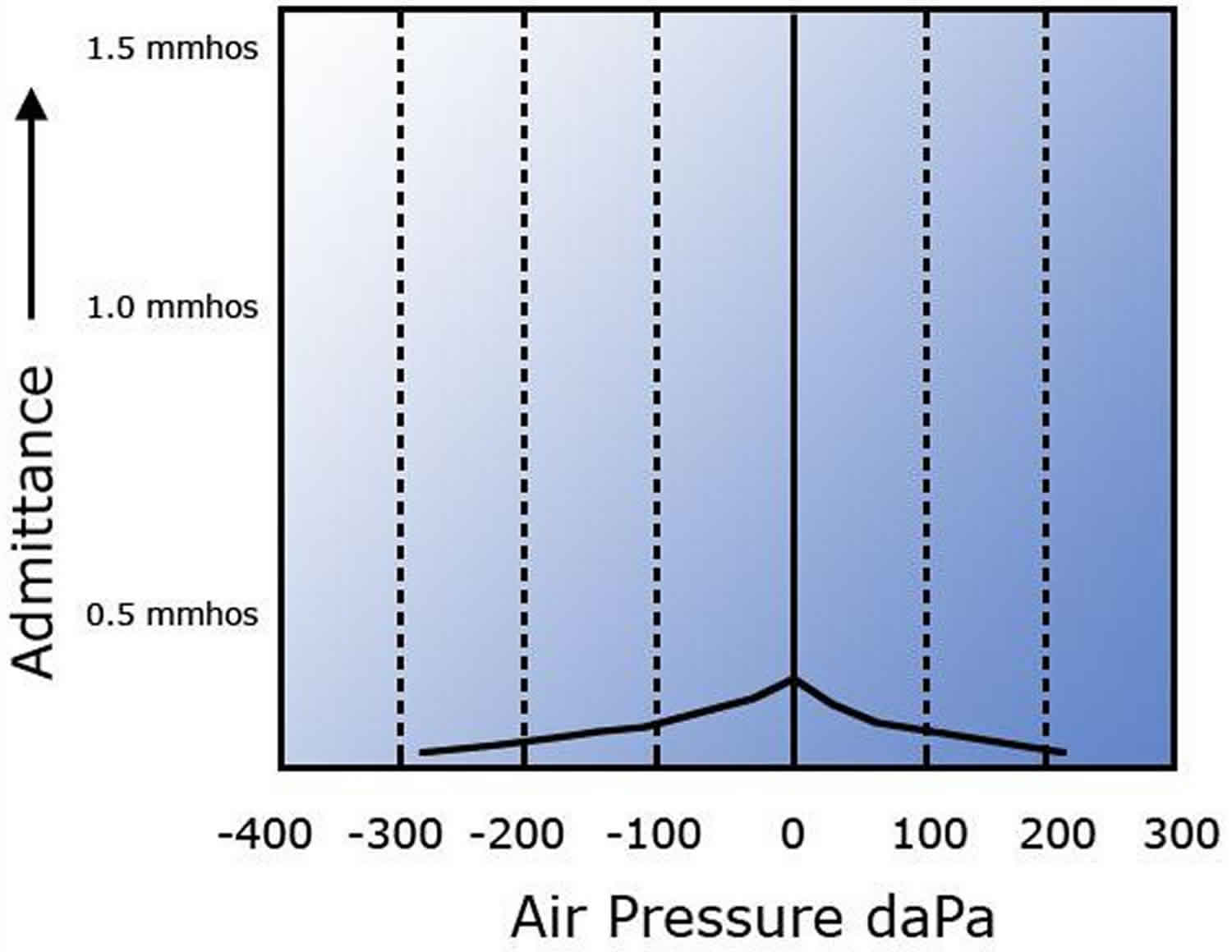
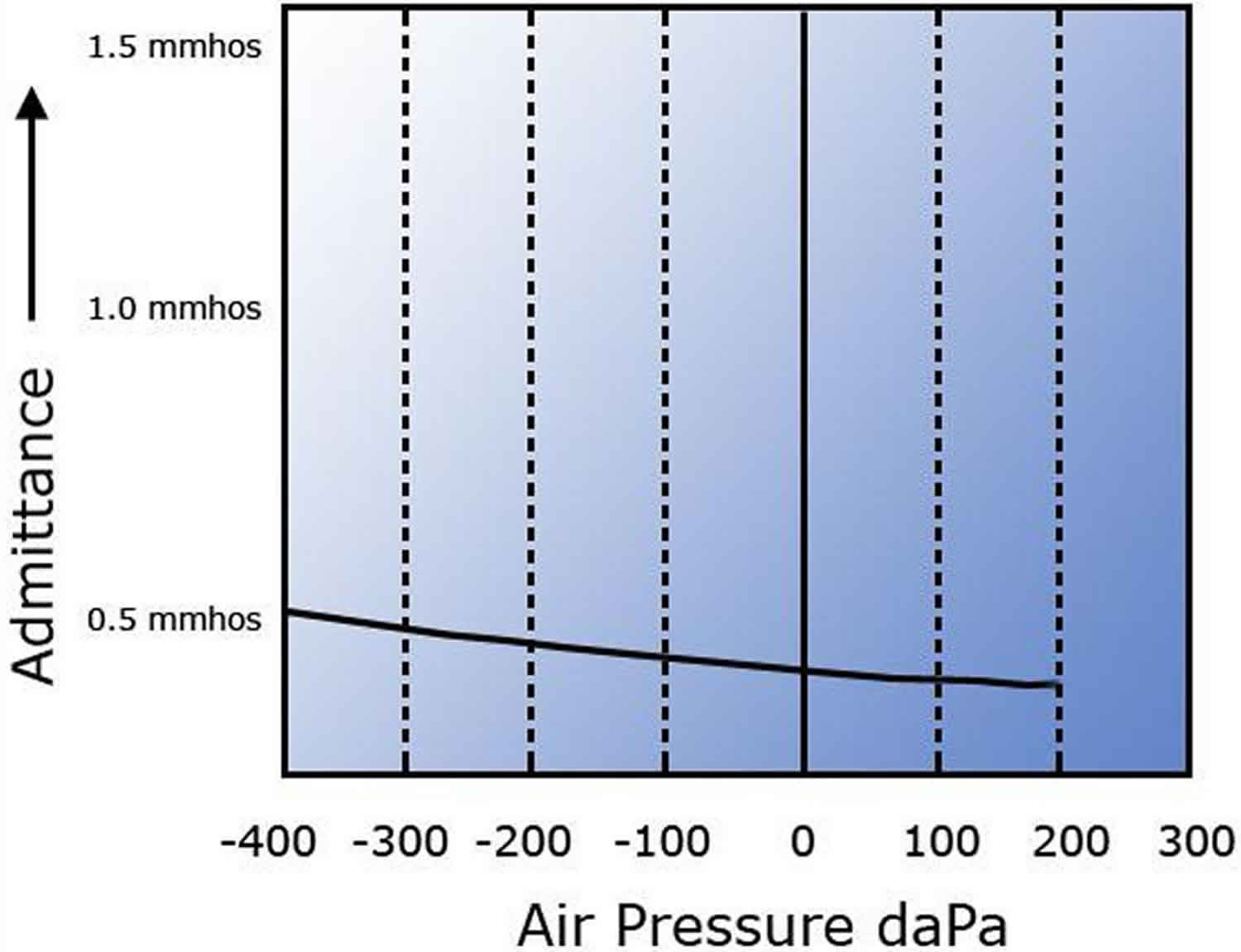
Type B tympanogram
Type B is a flat trace with no observed compliance or immittance peak. Type B tympanograms exhibit no air pressure peaks and are generally described as “flat tympanograms”. This can indicate middle ear conditions, cerumen occlusion, probe tip that is against the side of the external auditory canal, or patent grommets. Type B tympanograms must be interpreted in conjunction with ear canal volume readings (see image below). Average ear canal volumes for children are 0.42-0.97 mL. Average adult volumes are 0.63-1.46 mL.
- Type B (normal ear canal volume) usually suggests otitis media.
- Type B (small ear canal volume) may suggest that the ear canal is occluded with wax/debris or that the immittance probe is pushed against the side of the ear canal.
- Type B (large ear canal volume) suggests a patent pressure equalization tube or perforation of the tympanic membrane.
Figure 10. Type B tympanogram
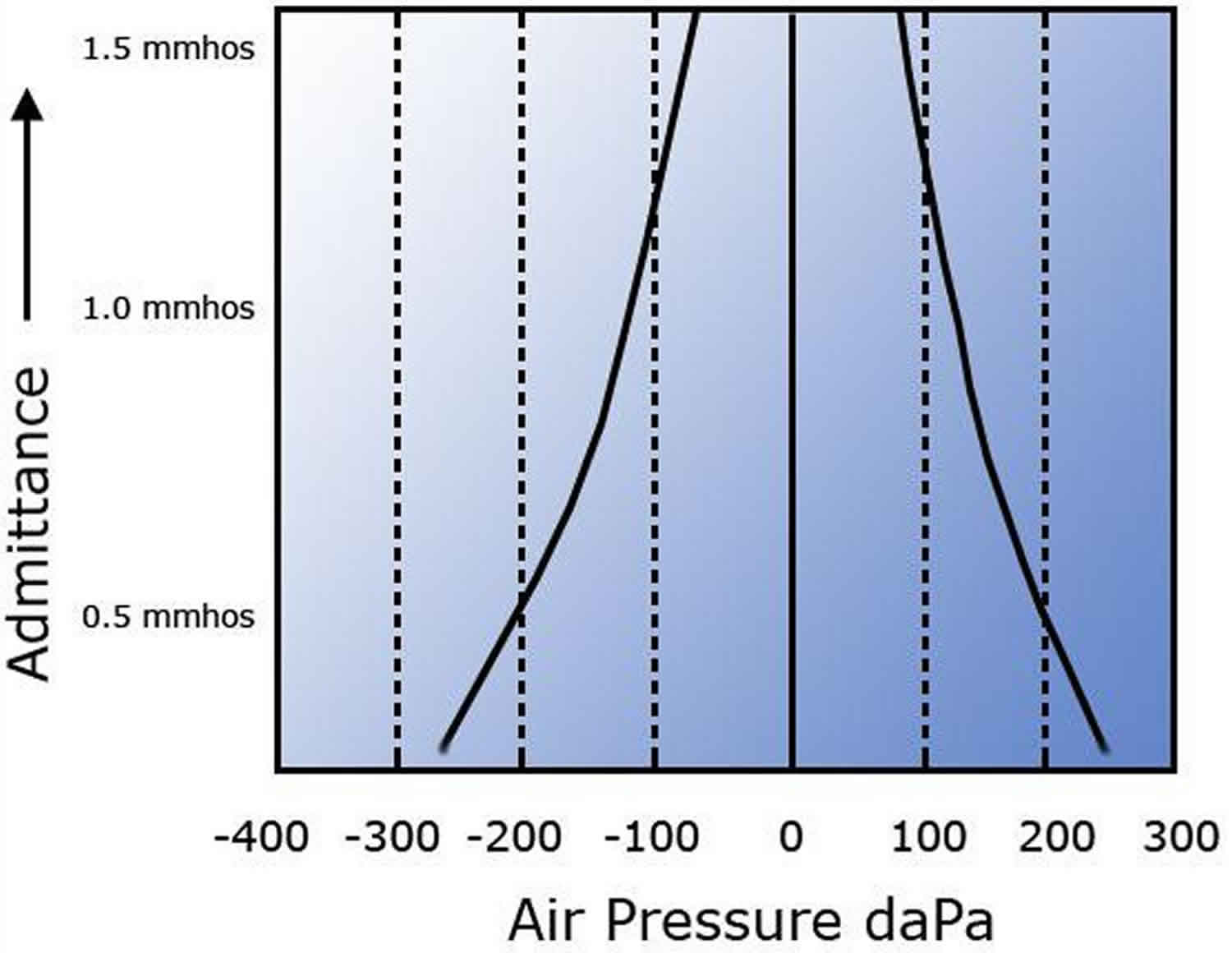
Type C tympanogram
Type C suggests significant negative pressure in the middle ear system and may suggest developing or resolving otitis media. Additionally, this type indicates a malfunctioning eustachian tube. Immittance peak is measurable, but compliance peak is less than -150 daPa (see Figure 11 below)
Figure 11. Type C tympanogram
- Hall JW, Mueller HG (1997) Audiologists’ desk reference, vol I, Diagnostic audiology principles, procedures, and practices. Singular Publishing Group, San Diego, pp 175–204
- Katz J (2002) Handbook of clinical audiology, 5th edn. Lippincott Williams & Wilkins, Baltimore, pp 159–204
- Australian Government Department of Health and Ageing. Recommendations for Clinical Care Guidelines on the management of Otitis Media in Aboriginal and Torres Strait Islander Populations. ACT: 2010.
- Coates H, Kong K, Mackendrick A, Lannigan F, Vijayasekaran S, Bumbak P. Aboriginal and Torres Strait Islander Ear Health Manual. n.d.
- Duplessis C, Fothergill D, Gertner J, Hughes L, Schwaller D. A pilot study evaluating surfactant on eustachian tube function in divers. Mil Med. 2008 Dec. 173(12):1225-32.
- Hullar TE. Vascular pulsations on impedance audiometry as a sign of a third-mobile window lesion. Otol Neurotol. 2010 Jun. 31(4):565-6.
- British Society of Audiology (2010) Recommended Procedure for Ear Examination. Reading: British Society of Audiology.
- https://www.thebsa.org.uk/wp-content/uploads/2013/04/Tympanometry-1.pdf
- Feldman AS (1975) Tympanometry: procedures, interpretation and variables.In: Feldman AS, Wilbur LA (eds), Acoustic Impedance and Admittance: The Measurement of Middle Ear Function, pp. 103–155. Baltimore: Williams and Williams.
- Jerger J, Jerger SJ, Maudlin L (1972) Studies in impedance audiometry: I. normal and sensorineural ears. Arch Otolaryngol 96: 513–523
- Nozza RJ, Bluestone CD, Kardatze D, Bachman R (1994) Identification of middle ear effusion by aural acoustic immittance measurements for diagnosis of middle ear effusion in children. Ear Hear 15: 310–323.
- Shanks JE, Lilly DJ, Margolis RH, Wiley TL, Wilson RH (1988) Tutorial: tympanometry. J Speech Hear Dis 53: 354–377.
- Renvall U, Holmquist J (1976) Tympanometryrevealing middle ear pathology. Ann Otol Rhinol Laryngol 85: 209–215.
- Baldwin M (2006) Choice of probe tone and classification oftrace patterns in tympanometry undertaken in early infancy. Int J Audiol 45: 417–427.





{kind=link}