
Ulnar deviation
Ulnar deviation is a hand deformity in which the swelling of the metacarpophalangeal (MCP) joints (the big knuckles at the base of your fingers) causes your fingers to become displaced, tending towards the little finger. Ulnar deviation comes from the displacement toward the ulna (as opposed to radial deviation, in which fingers are displaced toward the radius). While the most common cause of ulnar deviation of the fingers is rheumatoid arthritis, it can also be caused by other conditions such as windblown hand or Jaccoud’s arthropathy 1, systemic lupus erythematosus (SLE) 2 or very rarely pigmented villonodular synovitis 3. Ulnar deviation is also a physiological movement of the wrist, where the hand including the fingers move towards the ulna.
To measure radial and ulnar deviation, a goniometer is needed. Place the patient’s forearm in pronation and the carpus aligned with the plane of the forearm. Align the goniometer with the third metacarpal and the axis of the forearm. In radial and ulnar deviation, the carpal rows move as linked segments. The buttress of the radial styloid limits radial deviation so that its arc of motion is significantly less. Normal radial deviation is 20° to 25°, and normal ulnar deviation is 30° to 40° 4.
Table 1. Wrist ulnar deviation goniometry
| Test Position | Normal Range |
|---|---|
|
|
| Goniometer Alignment | Normal End Feel |
|
|
Figure 1. Wrist movements
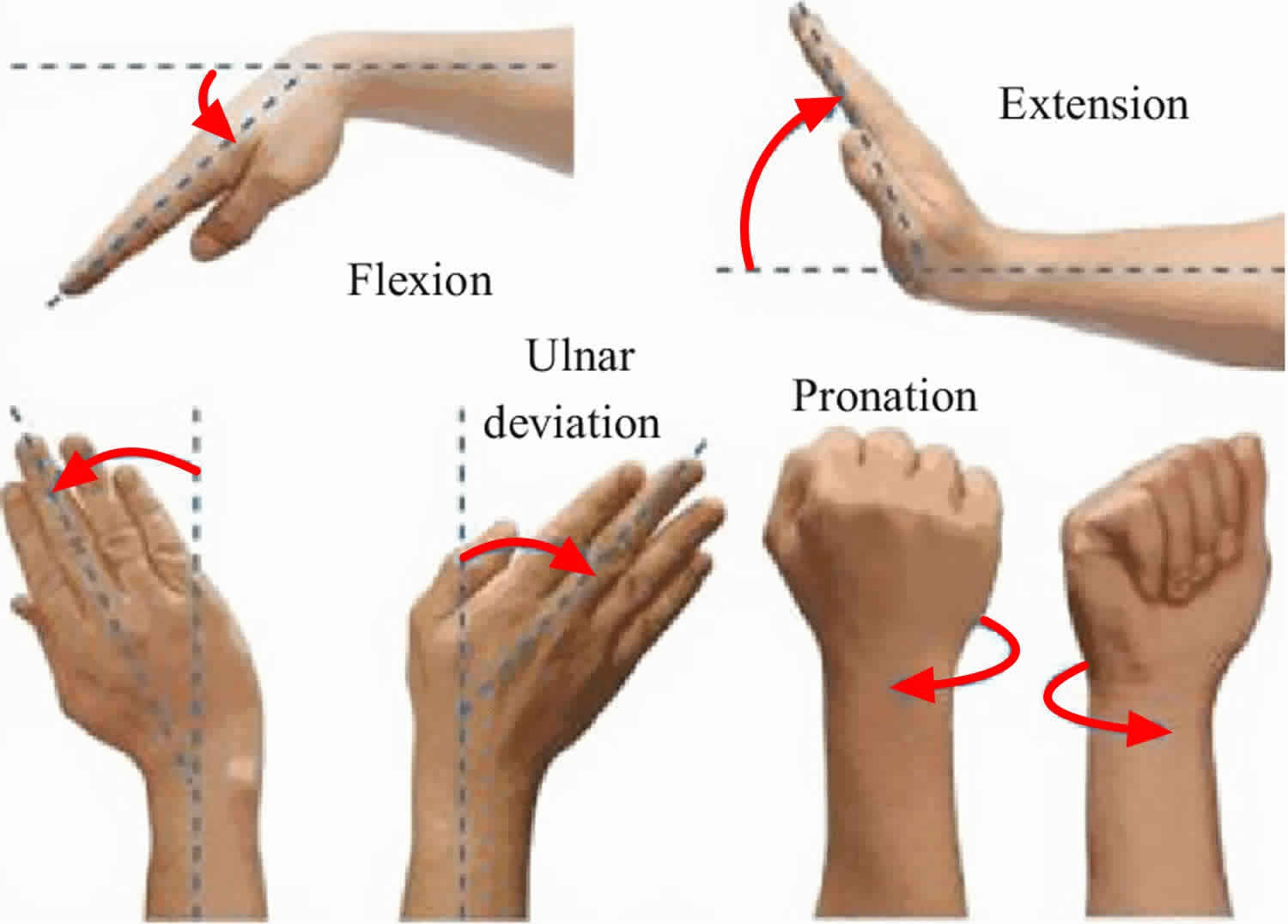
Figure 2. Ulnar deviation of wrist
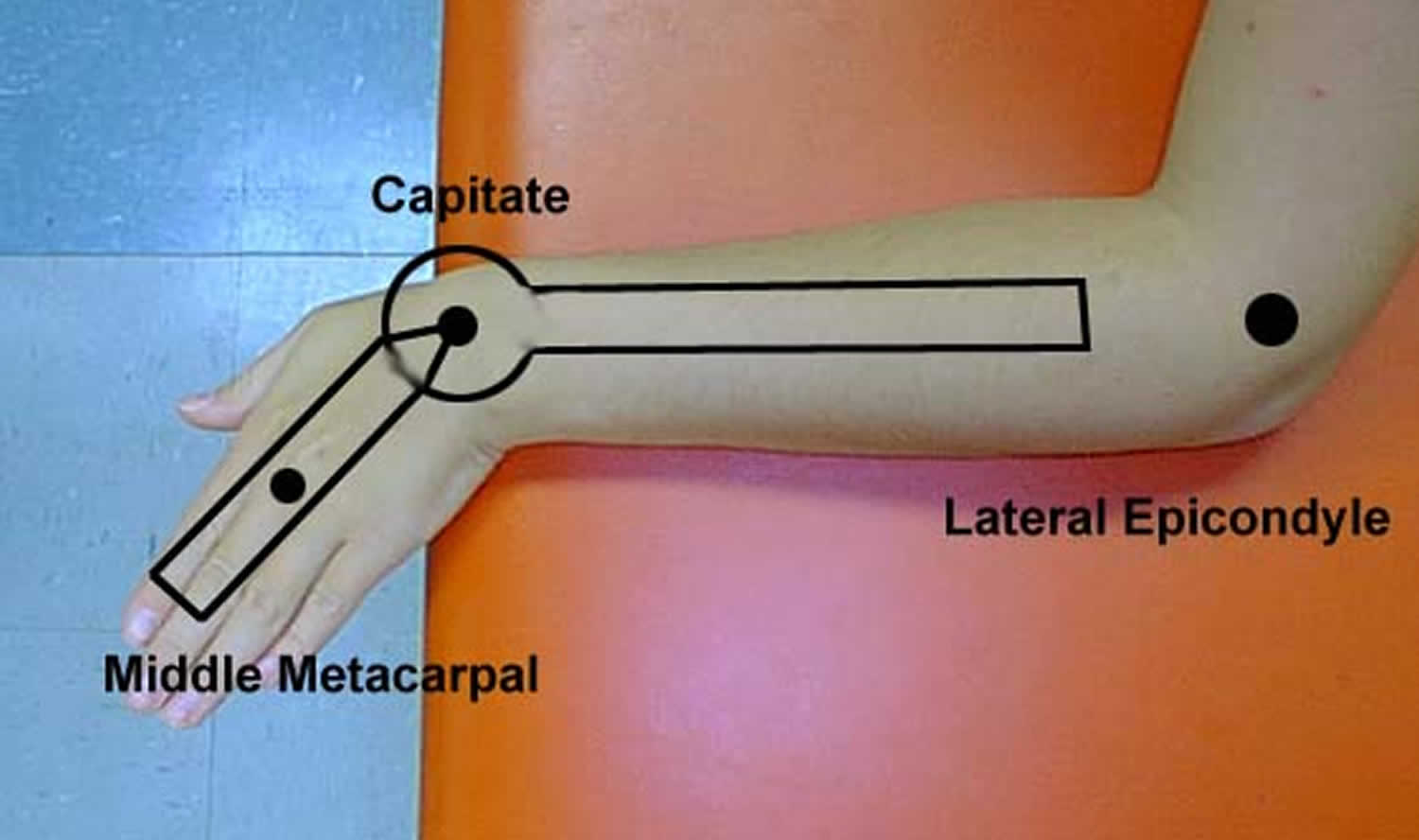
Figure 3. Ulnar drift fingers
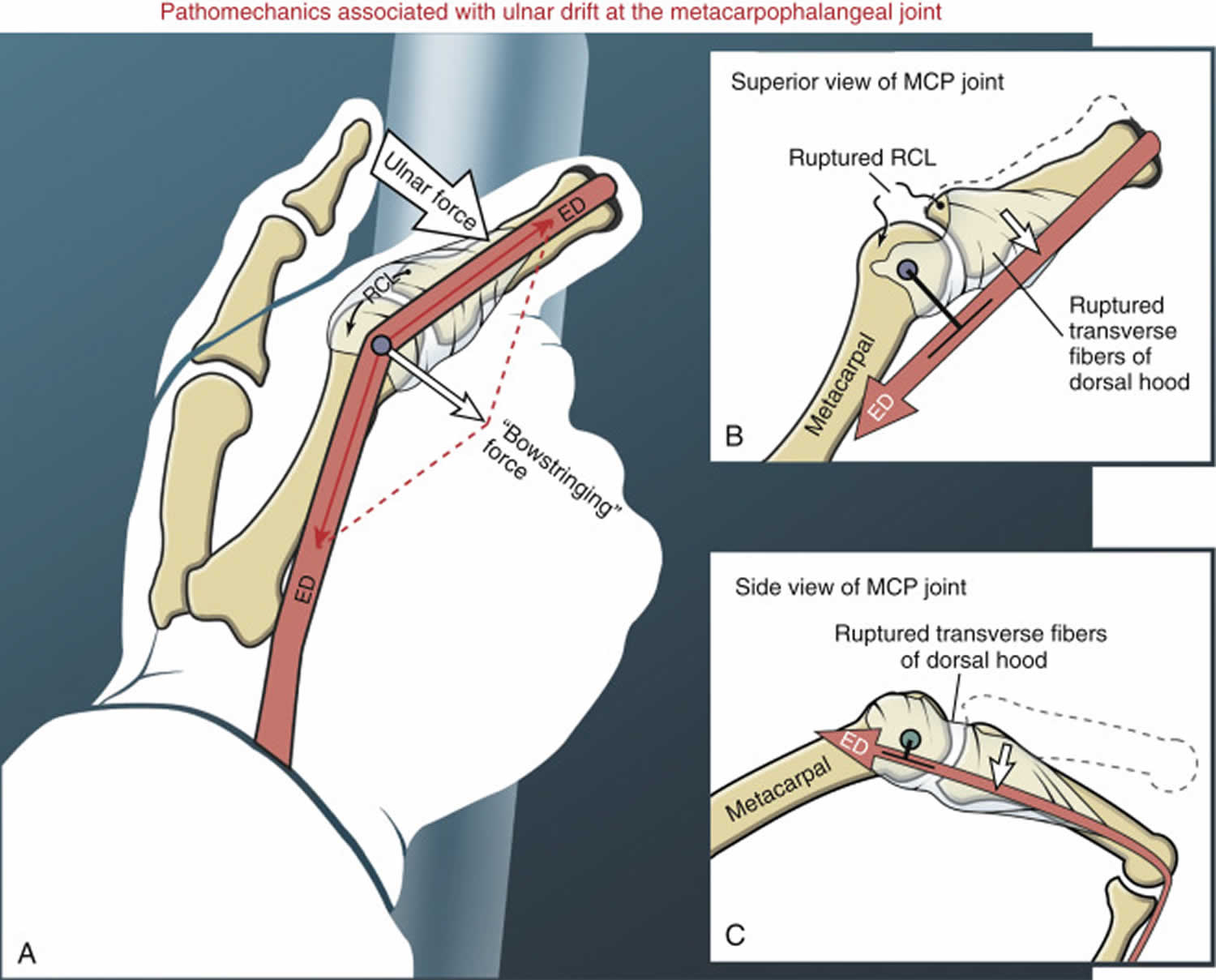
Ulnar drift
Ulnar drift occurs when there is a biomechanical imbalance of forces at the metacarpophalangeal (MCP) joint (Figure 3). An ulnar drift deformity at the metacarpophalangeal joint consists of an excessive ulnar deviation and ulnar translation (slide) of the proximal phalanx relative to the head of the metacarpal. Persons with severe ulnar drift are typically concerned about appearance and reduced function, especially in relation to pinching and gripping. To fully understand the pathomechanics of ulnar drift, it is important to realize that all hands—healthy or otherwise—are constantly subjected to factors that favor an ulnar-deviated posture of the fingers. Perhaps the most important factor stems from the almost constant ulnar-directed forces applied against the fingers by hand-held objects, often combined with pinching forces from the thumb. Figure 3A shows an example of these ulnar-directed forces pushing the index finger in an ulnar direction. Subsequent ulnar deviation of the MCP joint increases ulnar deflection, or bend, in the extensor digitorum tendon as it crosses the dorsal side of the joint. The deflection creates a potentially destabilizing “bowstringing” force on the tendon. In the healthy hand, however, the extensor mechanism and the radial collateral ligament maintain the extensor tendon close to the axis of rotation, thereby minimizing ulnar deviation torque.
Ulnar drift deformity is distinct from ulnar deviation, the normal rotation of the proximal phalanx on the metacarpal that facilitates hand grip 5. Classically seen in rheumatoid arthritis, the pathophysiology of ulnar drift is commonly attributed to metacarpophalangeal joint synovitis causing dorsoradial ligament damage and resultant extensor tendon ulnar subluxation 6. More accurately, ulnar drift is a result of multiple factors including innate metacarpophalangeal anatomy, normal hand use, ulnar translation of the flexor tendons, and proximal joint disease (e.g., radial deviation of the wrist). Disruption of stabilizing ligaments at the metacarpophalangeal joint also leads to palmar subluxation of the proximal phalanx and permanent flexion deformities 7.
Ulnar drift can profoundly affect a patient’s quality of life by impairing power grip and precision hand functions 8. Furthermore, pain and esthetic discomfort are common complaints by patients 9. When conservative management is exhausted, surgical interventions may be considered. Silicone metacarpophalangeal arthroplasty is the most proven intervention to correct ulnar drift deformity, relieve pain, and improve hand function 8. Commonly, soft tissue reconstructive procedures are performed concomitantly to reestablish normal anatomical alignment at the metacarpophalangeal joint 10. Long-term follow-up of a multicenter prospective outcomes study of silicone metacarpophalangeal arthroplasty in rheumatoid arthritis patients showed improvement in hand function and appearance when compared to nonsurgical controls 11.
References- Congenital Ulnar Drift in a Surgeon. Case Reports in Orthopedics Volume 2015, Article ID 135350 https://doi.org/10.1155/2015/135350
- ARTICULAR MANIFESTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS. Systemic Lupus Erythematosus 4th Edition, 2004. ISBN 978-0-12-433901-9 https://doi.org/10.1016/B978-0-12-433901-9.X5000-5
- Ulnar deviation is not always rheumatoid. Annals of the Rheumatic Diseases 1996;55:786-788 https://ard.bmj.com/content/annrheumdis/55/11/786.full.pdf
- Norkin CC, White DJ. Measurement of joint motion: a guide to goniometry. FA Davis; 2016 Nov 18.
- Flatt AE. Ulnar drift. J Hand Ther. 1996;9:282–92.
- Ono S, Entezami P, Chung KC. Reconstruction of the rheumatoid hand. Clin Plast Surg. 2011;38:713–27.
- Backhouse KM. The mechanics of normal digital control in the hand an analysis of the ulnar drift of rheumatoid arthritis. Ann R Coll Surg Engl. 1968;43:154–73.
- Chung KC, Burns PB, Wilgis S, Burke FD, et al. A multicenter clinical trial in rheumatoid arthritis comparing silicone metacarpophalangeal joint arthroplasty with medical treatment. J Hand Surg. 2009;34(A):815–23.
- Anderson RJ. Controversy in the surgical treatment of the rheumatoid hand. Hand Clin. 2011;27:21–5.
- Chung KC. Operative techniques: hand and wrist surgery. 2nd ed. Philadelphia, PA: Saunders; 2012.
- Chung KC, Burns PB, Kim MH, et al. Long-term followup for rheumatoid arthritis patients in a multicenter outcomes study of silicone metacarpophalangeal joint arthroplasty. Arthritis Care Res. 2012;64(9):1292–300.





{kind=link}