
What are uterine polyps
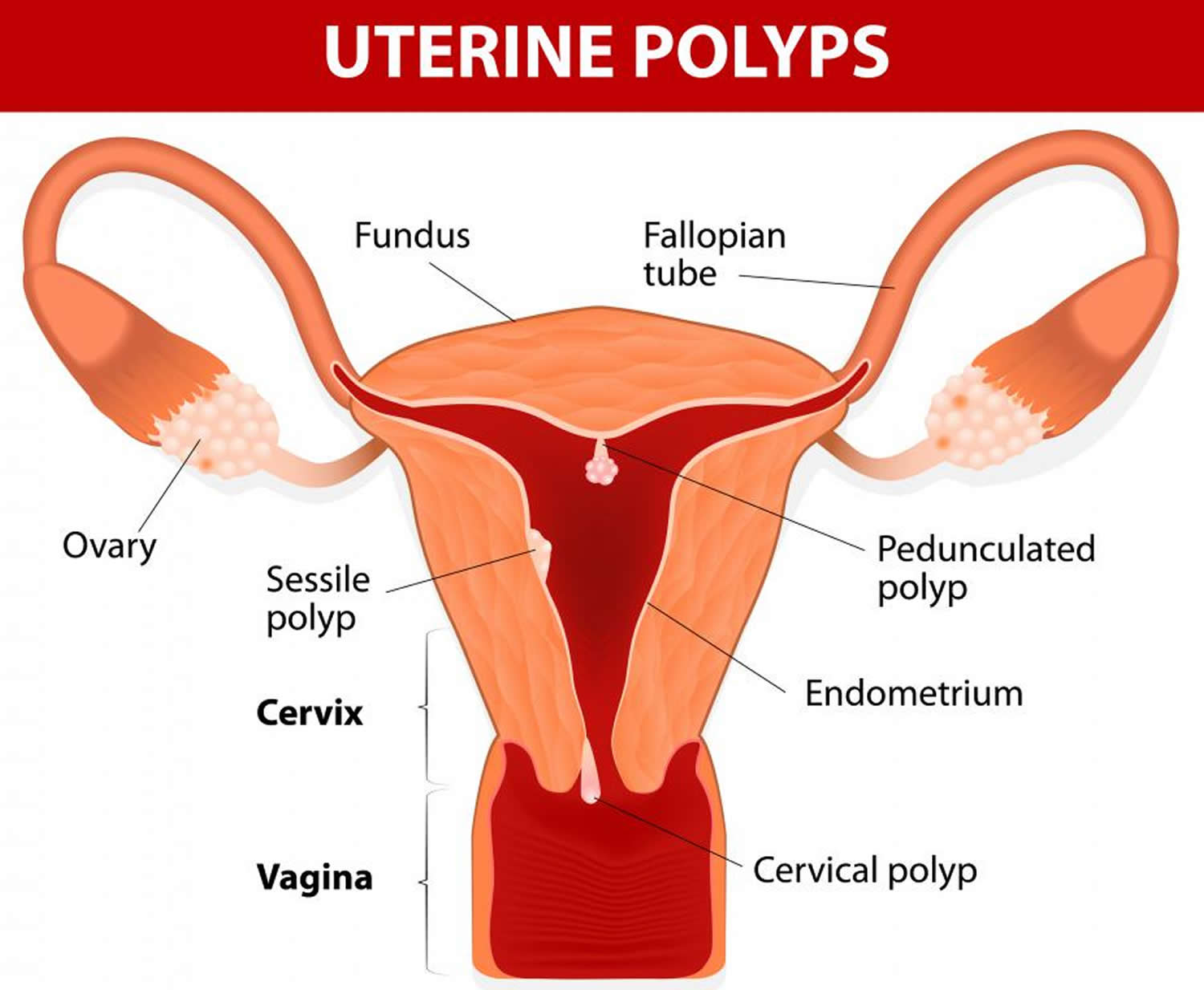
Uterine polyps also known as endometrial polyps, are localized hyperplastic overgrowths of endometrium (inner wall of the uterus) that contain both dilated endometrial glands and fibrous stroma that contains thick-walled blood vessels that extend into the uterine cavity 1. Uterine polyps are formed when there’s an overgrowth of tissue in the lining of the uterus (the endometrium). Uterine polyps are round or oval in shape and usually vary in size from a few millimeters (the size of a grain of rice) to a few centimeters (the size of a ping pong ball or larger). While uterine polyps are usually attached to the uterine wall by a large base or a thin stalk contained within the uterus, some may slip through the opening of the uterus into the vagina.
Uterine polyps prevalence range is between 16% to 34% depending on characteristics of the population studied and detecting methods 2. Uterine polyps are common in women between 20 to 40 years of age.
The large majority (over 95 percent) of these uterine polyps are benign. Uterine polyps have a variable presentation; they can occur as individual or multiple lesions, range in size from millimeters to centimeters and can be sessile or pedunculated. Although uterine polyps may be identified during evaluation of abnormal bleeding, many polyps are asymptomatic and only discovered during the infertility evaluation 1. Up to 25% of women with unexplained infertility have uterine polyps on hysteroscopy 3. However, uterine polyps effect on endometrial receptivity and fertility is unclear.
Overall the prevalence of malignant and premalignant lesions found in the uterine polyps ranges from 0.8% to 4.8% 4. There are numerous studies, which confirm association of uterine serous papillary carcinoma with uterine polyps especially the larger and symptomatic ones 5. The frequency of malignant uterine polyps increased with age and reached statistical significance in the age group > 65 6. A systematic review of the association of menopausal status, uterine bleeding, and uterine polyp size and risk of malignancy among women undergoing polyp resection 7 found that among symptomatic postmenopausal women with endometrial polyps, 4.47% (88 of 1,968) had a malignant polyp in comparison to 1.51% (25 of 1,654) asymptomatic postmenopausal women 7. Subsequently published studies 8, 9 report similar rates:
- Golan et al 8 in a retrospective registration of 1,124 patients who underwent hysteroscopic resection of endometrial polyps. “Pathologic evaluation disclosed 7 cases of malignancy and 4 cases of atypical hyperplasia among bleeding postmenopausal women (11/263, 4%) and 2 malignancies and 3 cases of hyperplasia with atypia among asymptomatic postmenopausal women (5/378, 1.3%).”
- Wethington et al 10 a review of 1011 women with endometrial polyps: “Among symptomatic postmenopausal women with endometrial polyps, 4.47% (88 of 1,968) had a malignant polyp in comparison to 1.51% (25 of 1,654) asymptomatic postmenopausal women.”
You can have one or many uterine polyps. They usually stay contained within your uterus, but occasionally, they slip down through the opening of the uterus (cervix) into your vagina. Uterine polyps most commonly occur in women who are going through or have completed menopause, although younger women can get them, too.
The symptoms commonly associated with uterine polyps include irregular menstrual bleeding, unusually heavy flow during menstruation, bleeding between periods and spotting or bleeding after menopause and infertility. However, many women with uterine polyps have no signs or symptoms of the condition. It’s not uncommon for polyps to be discovered during incidental testing for other issues.
While the exact cause of uterine polyps is unknown, hormones may be a factor. Researchers believe that uterine polyps are estrogen-sensitive and may be an abnormal growth response to estrogen circulating in the blood. Uterine polyps are more likely to appear in women between the ages of 40 and 50 and in women who are obese or have high blood pressure.
Seek medical care if you have:
- Vaginal bleeding after menopause
- Bleeding between menstrual periods
- Irregular menstrual bleeding
Figure 1. Uterine polyps
 Uterine polyps complications
Uterine polyps complications
Uterine polyps might be associated with infertility. If you have uterine polyps and you’re unable to have children, removal of the polyps might allow you to become pregnant, but the data are inconclusive.
What causes uterine polyps
Hormonal factors appear to play a role. Uterine polyps are estrogen-sensitive, meaning they grow in response to circulating estrogen.
Risk factors for uterine polyps
Risk factors for developing uterine polyps include:
- Being perimenopausal or postmenopausal
- Having high blood pressure (hypertension)
- Being obese
- Taking tamoxifen, a drug therapy for breast cancer
- Family history of Lynch syndrome or Cowden syndrome (genetic conditions that run in families).
Uterine polyps signs and symptoms
Signs and symptoms of uterine polyps include:
- Irregular menstrual bleeding — for example, having frequent, unpredictable periods of variable length and heaviness
- Bleeding between menstrual periods
- Excessively heavy menstrual periods
- Vaginal bleeding after menopause
- Infertility
Some women have only light bleeding or spotting; others are symptom-free.
Uterine polyps diagnosis
If your doctor suspects you have uterine polyps, he or she might perform one of the following:
Transvaginal ultrasound. During a transvaginal ultrasound, your doctor or a medical technician inserts a wand-like device (transducer) into your vagina while you are positioned on an exam table. The transducer emits sound waves that generate images of your uterus, ovaries and fallopian tubes. Your doctor may see a polyp that’s clearly present or may identify a uterine polyp as an area of thickened endometrial tissue.
A related procedure, known as hysterosonography — also called sonohysterography. During sonohysterography, your doctor uses a thin, flexible tube (catheter) to inject salt water (saline) into the hollow part of your uterus. The saline expands your uterine cavity, which gives the doctor a clearer view of the inside of your uterus during the ultrasound. With an ultrasound probe, your doctor obtains images of the inside of your uterus and checks for irregularities.
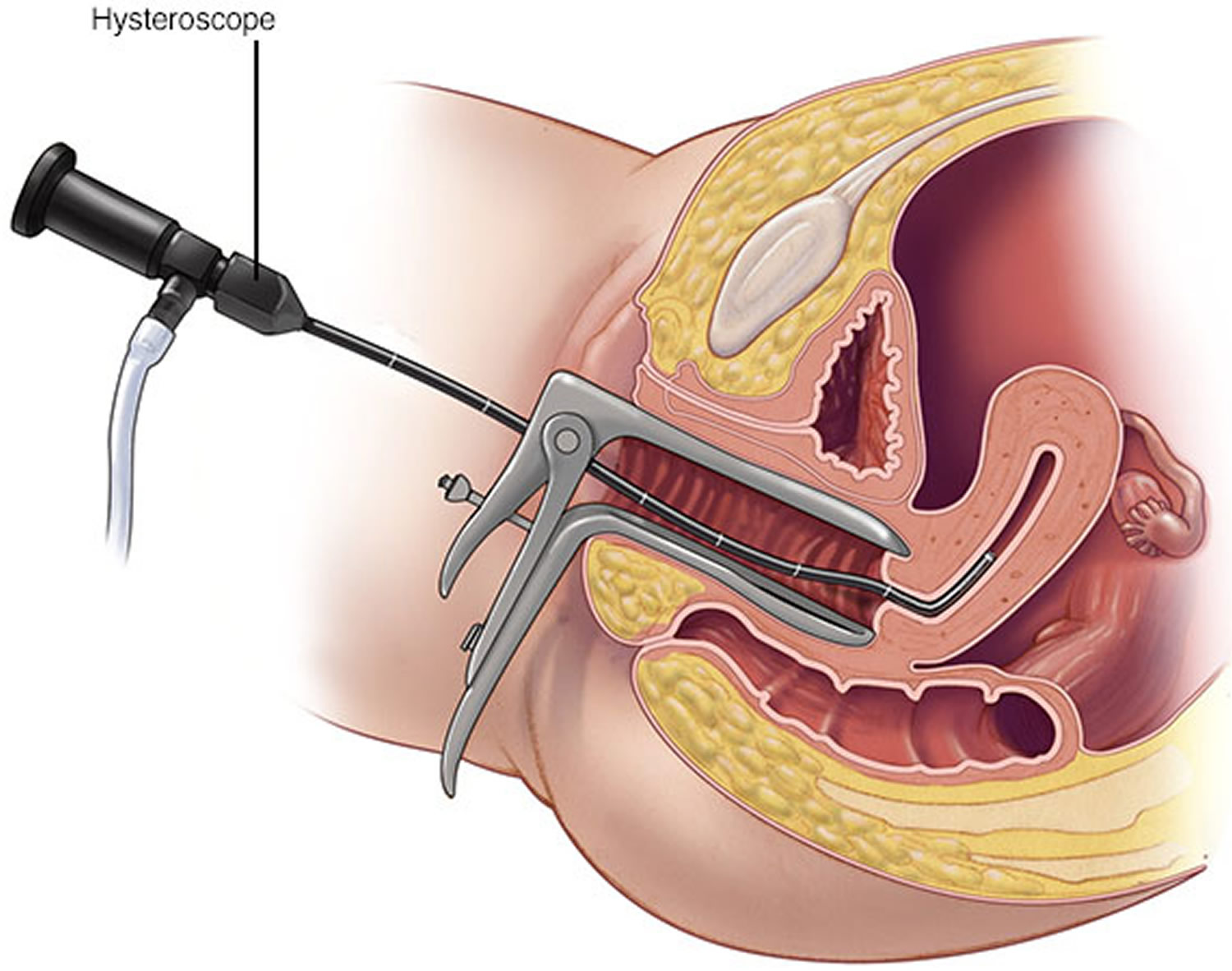
Hysteroscopy. Your doctor inserts a thin, flexible, lighted telescope (hysteroscope) through your vagina and cervix into your uterus. Hysteroscopy allows your doctor to examine the inside of your uterus.
Endometrial biopsy. Your doctor might use a suction catheter inside the uterus to collect a specimen for lab testing. Uterine polyps may be confirmed by an endometrial biopsy, but the biopsy could also miss the polyp.
Most uterine polyps are noncancerous (benign). However, some precancerous changes of the uterus (endometrial hyperplasia) or uterine cancers (endometrial carcinomas) appear as uterine polyps. Your doctor will likely recommend removal of the polyp and will send a tissue sample for lab analysis to be certain you don’t have uterine cancer.
Figure 2. Transvaginal ultrasound
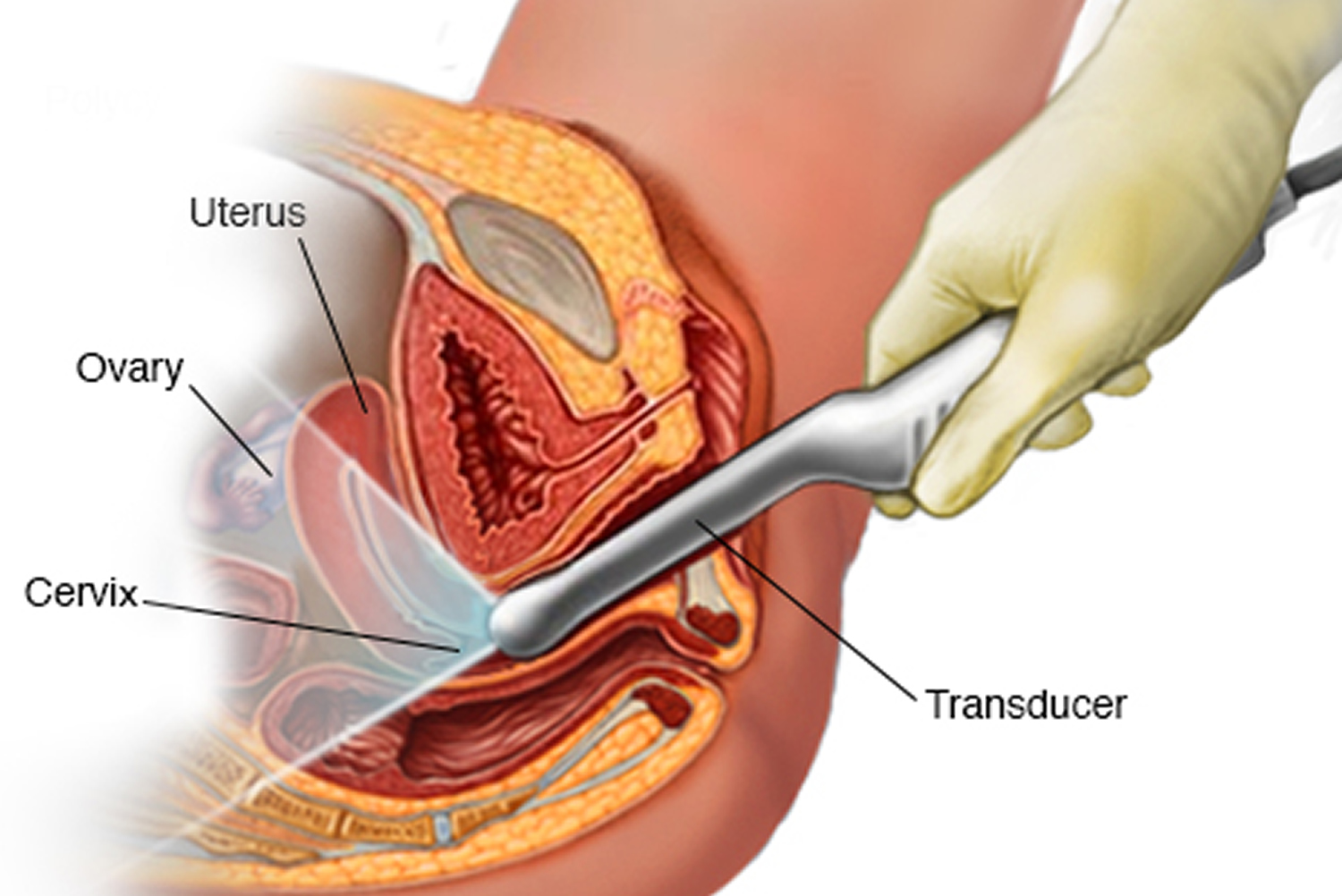
Figure 3. Sonohysterography
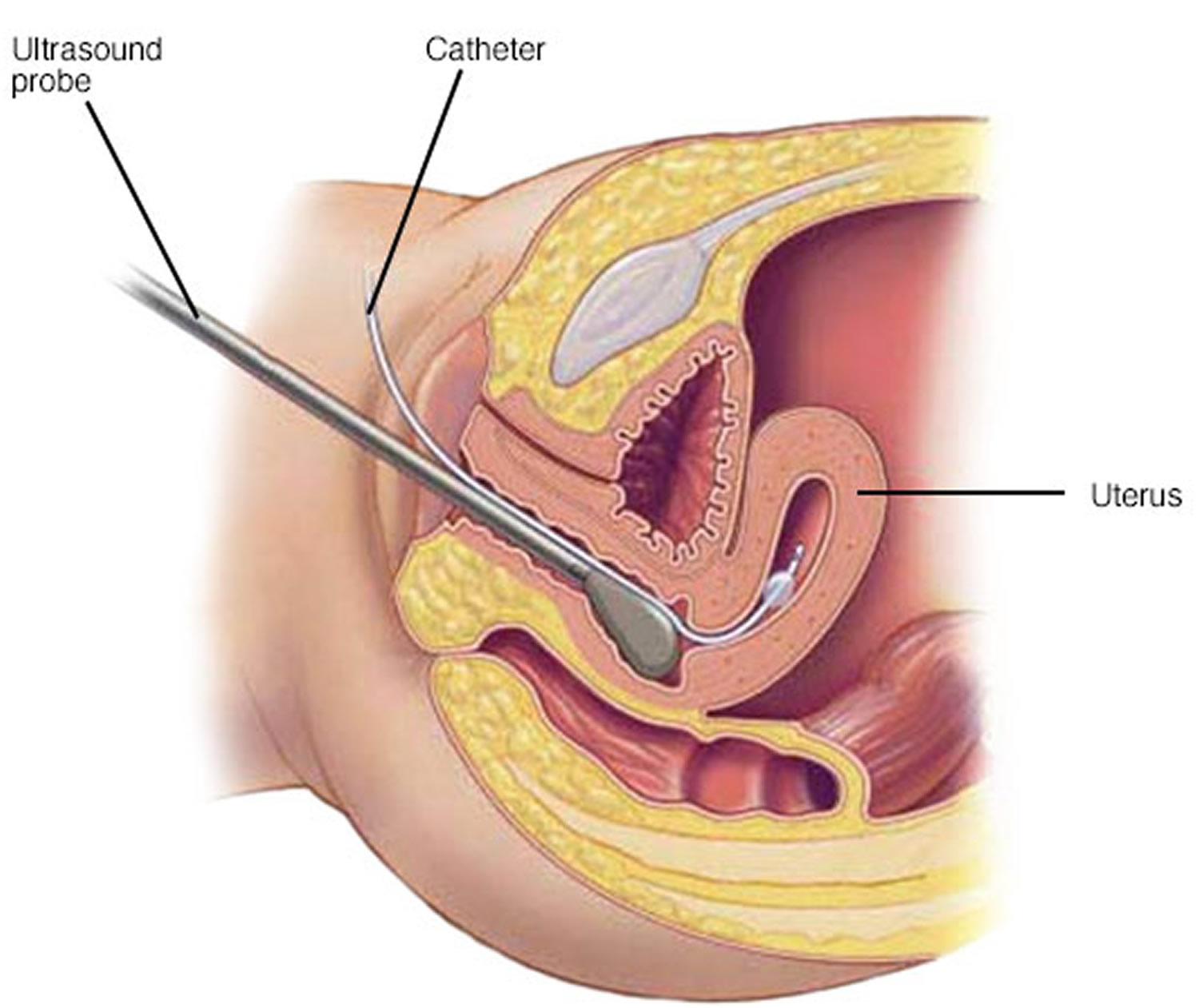 Figure 4. Hysteroscopy
Figure 4. Hysteroscopy
 Uterine polyps treatment
Uterine polyps treatment
Depending on the size of your polyps and symptoms your doctor may recommend:
Monitoring and waiting. Small uterine polyps without symptoms (asymptomatic polyps) might resolve on their own. Treatment of small uterine polyps is unnecessary unless you’re at risk of uterine cancer.
Medication. Certain hormonal medications, including progestins and gonadotropin-releasing hormone agonists, may lessen symptoms of the polyp. But taking such medications is usually a short-term solution at best — symptoms typically recur once you stop taking the medicine.
Surgical removal. When larger polyps are present and are problematic, uterine polyp removal is necessary. Your doctor may perform a hysteroscopy to remove the polyps. During this outpatient procedure, your doctor will insert a thin and flexible, lighted scope (hysteroscope) into your uterus. This allows your doctor to see into your uterus and locate the polyps. The polyps are then removed using surgical instruments inserted through the hysteroscope. The removed polyps are usually sent to a lab for examination to rule out cancerous cells.
If a uterine polyp contains cancerous cells, your doctor will talk with you about the next steps in evaluation and treatment.
Rarely, uterine polyps can recur. If they do, you might need more treatment.
References- Rackow BW, Jorgensen E, Taylor HS. ENDOMETRIAL POLYPS AFFECT UTERINE RECEPTIVITY. Fertility and sterility. 2011;95(8):2690-2692. doi:10.1016/j.fertnstert.2010.12.034. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3096716/
- Rahimi S, Marani C, Renzi C, Natale ME, Giovannini P, Zeloni R. Endometrial polyps and the risk of atypical hyperplasia on biopsies of unremarkable endometrium: a study on 694 patients with benign endometrial polyps. Int J Gynecol Pathol. 2009;28(6):522–8. https://www.ncbi.nlm.nih.gov/pubmed/19851198
- de Sa Rosa e de Silva AC, Rosa e Silva JC, Candido dos Reis FJ, Nogueira AA, Ferriani RA. Routine office hysteroscopy in the investigation of infertile couples before assisted reproduction. J Reprod Med. 2005;50:501–6. https://www.ncbi.nlm.nih.gov/pubmed/16130847
- Savelli L, De Iaco P, Santini D, Rosati F, Ghi T, Pignotti E, et al. Histopathologic features and risk factors for benignity, hyperplasia, and cancer in endometrial polyps. Am J Obstet Gynecol. 2003;188(4):927–31. https://www.ncbi.nlm.nih.gov/pubmed/12712087
- Ferrazzi E, Zupi E, Leone FP, Savelli L, Omodei U, Moscarini M, et al. How often are endometrial polyps malignant in asymptomatic postmenopausal women. A multicenter study? (e1-6).Am J Obstet Gynecol. 2009;200(3):235. https://www.ncbi.nlm.nih.gov/pubmed/19027096
- Hileeto D, Fadare O, Martel M, Zheng W. Age dependent association of endometrial polyps with increased risk of cancer involvement. World J Surg Oncol. 2005;3:8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC549519/
- Lee SC. Kaunitz AM. Sanchez-Ramos L. Rhatigan RM. The oncogenic potential of endometrial polyps: a systematic review and meta-analysis. Obstetrics & Gynecology. 116(5):1197-205, 2010 Nov. https://www.ncbi.nlm.nih.gov/pubmed/20966706
- Golan A. Cohen-Sahar B. Keidar R. Condrea A. Ginath S. Sagiv R. Endometrial polyps: symptomatology, menopausal status and malignancy. Gynecologic & Obstetric Investigation. 70(2):107-12, 2010. https://www.karger.com/Article/Abstract/298767
- Wethington SL. Herzog TJ. Burke WM. Sun X. Lerner JP. Lewin SN. Wright JD. Risk and predictors of malignancy in women with endometrial polyps. Annals of Surgical Oncology. 18(13):3819-23, 2011 Dec. https://www.ncbi.nlm.nih.gov/pubmed/21701931
- Wethington SL. Herzog TJ. Burke WM. Sun X. Lerner JP. Lewin SN. Wright JD. Risk and predictors of malignancy in women with endometrial polyps. Annals of Surgical Oncology. 18(13):3819-23, 2011 Dec. https://link.springer.com/article/10.1245%2Fs10434-011-1815-z





{kind=link}