What is a vasectomy
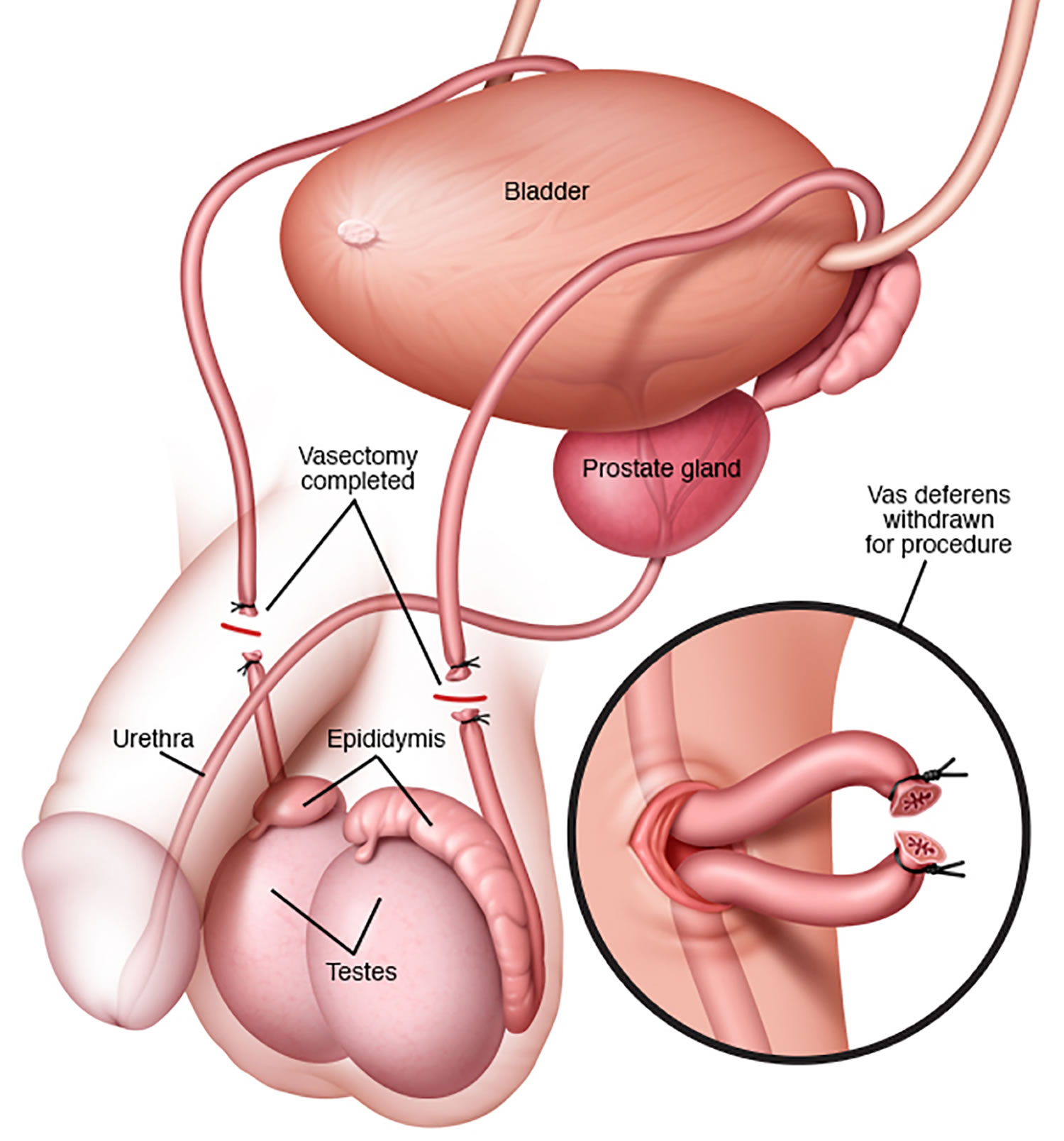
Vasectomy or ‘male sterilization’ is a minor surgical procedure to cut or seal the tubes (vas deferens) that carry a man’s sperm to permanently prevent pregnancy. Vasectomy procedure is done to keep a man’s sperm from going to his penis, so his ejaculate never has any sperm in it that can fertilize an egg. Although sperm continue to be produced, they can no longer exit the body and are phagocytized in the epididymis. Vasectomy is a simple procedure that is done at an outpatient surgical center and reliable method of contraception. Vasectomy is usually considered permanent and is therefore a big decision that should be fully discussed with your doctor beforehand. Although most men who undergo contraceptive sterilization do not regret having had the procedure, the permanence of the vasectomy method is an important consideration, as regret has been documented in studies. Men who have vasectomy before age 30 are the group most likely to want a vasectomy reversal in the future 1.
A vasectomy is a quick and relatively painless surgical procedure. Vasectomy is usually done under local anesthetic, where you’re awake but don’t feel any pain, and takes about 15 to 30 minutes. You can go home the same day. In rare cases, you may have a general anesthetic, where you’re asleep during the operation. Recovery time is less than one week. Patients should refrain from ejaculation for approximately one week after vasectomy. After the operation, you need to visit your doctor for tests to count your sperm and to make sure the sperm count has dropped to zero; this takes about 12 to 16 weeks. Another form of birth control should be used until the your sperm count has dropped to zero.
Vasectomy is the most common non-diagnostic operation performed by urologists in the United States. Data from the National Study of Family Growth in which only married couples were polled indicate a range from 175,000 to 354,000 2. In a physician survey, an estimated 526,501 vasectomies were performed in the US in 2002 3. This number seems to have been approximately stable for the previous decade. More than 75% of vasectomies in the US are done by urologists, family physicians perform approximately 13% 4 and about 90% of urology practices in the US perform vasectomy 5.
Although vasectomy is the safest and most inexpensive option for permanent sterilization 6, female sterilization is used about three times as often (27 versus 9.2 percent of couples who use contraception) see Tables 1 and 2 below 7. In addition, there was a 3 percent overall decrease in the use of sterilization (male and female) and an increase in the use of less-reliable forms of contraception from 1995 to 2002 7. In 2002, data collected in the US show that vasectomy was used by 5.7% of men ages 15-44 and that this represents the fourth most commonly-used contraceptive method. The first three were condoms, used by 29.5% of men, oral contraceptives for women used by 25.6% of couples and tubal ligation used by 8.1% of couples 8. Compared to tubal ligation , which is also a method of permanent contraception, vasectomy is equally effective in preventing pregnancy; however, vasectomy is simpler, faster, safer and less expensive. Vasectomy is one of the most cost-effective of all methods of contraception; its cost is about one-fourth of the cost of tuba lligation 9. Vasectomy requires less time off work, requires only local rather than general anesthesia and is usually performed in a doctor’s office or clinic. The potential complications of vasectomy are less serious than those of tubal ligation.
Despite the clear advantages of vasectomy, prevalence data for 1998-2002 show that tubal ligation (female sterilization) was performed about two to three times more often than vasectomy 2. Among all women in 2002, married and unmarried, ages 15 to 44 years in the United States, only 5.7% relied on vasectomy for contraception compared to 16.7% who relied on tubal ligation 10. Even among married women and married men who desire permanent contraception, in the US the prevalence of tubal ligation has exceeded the prevalence of vasectomy 11.
Worldwide, the discrepancy between vasectomy and tubal ligation is even more marked than in the US. Data compiled in 2008 by the Population Division of the Department of Economic and Social Affairs of the United Nations show that 33 million married women ages 15-49 relied on vasectomy for contraception compared to 225 million who relied on tubal ligation 12. There are only eight nations in which vasectomy use is equal to or more frequent than tubal ligation for contraception – Korea, Canada, the United Kingdom, New Zealand, Bhutan, the Netherlands, Denmark and Austria ()World Contraceptive Use 2011. http://www.un.org/esa/population/publications/contraceptive2011/wallchart_front.pdf)).
Given that vasectomy and tubal ligation have equivalent contraceptive effectiveness and that vasectomy enjoys advantages compared to tubal sterilization of lower cost, less pain, greater safety and faster recovery, vasectomy should be considered for permanent contraception much more frequently than is the current practice in the United States and most nations of the world.
When considering a vasectomy, it’s important to understand that failures can occur. The U.S. Centers for Disease Control and Prevention research has estimated there is a probability of 11 failures per 1,000 procedures over 2 years; half of the failures occurred in the first three months after the vasectomy, and no failures occurred after 72 weeks 13. The U.S. Centers for Disease Control and Prevention research also examined regret among women whose partner underwent a vasectomy 14. In interviews with female partners of men who received vasectomies, the U.S. Centers for Disease Control and Prevention found that while most women did not regret their husband’s vasectomies, the probability of regret over 5 years was about 6%. This is why it is important to know facts about vasectomy and other permanent forms of birth control before making a decision.
Some men may be concerned that vasectomy is linked to prostate cancer. However, a population-based, case-control study including men with newly diagnosed prostate cancer showed no association between prostate cancer and vasectomy 15 and a meta-analysis provided no evidence of an association 16. Studies also have shown that there is no measurable association between vasectomy and testicular cancer 17, 18.
Vasectomy key facts
- A vasectomy is more than 99% effective.
- Vasectomy does not produce immediate sterility. Following vasectomy, another form of contraception is required until vas occlusion is confirmed by post- vasectomy semen analysis. You’ll need to use contraception for at least 8 to 16 weeks after the vasectomy operation, because sperm will still be in the tubes leading to the penis.
- Eight to sixteen weeks after vasectomy is the appropriate time range for the first post- vasectomy semen analysis. The choice of time to do the first post- vasectomy semen analysis should be left to the judgment of the surgeon.
- Up to 2 semen tests are done after the vasectomy operation to make sure that all the sperm have gone.
- Vasectomy should be considered a failure if any motile sperm are seen on post- vasectomy semen analysis at six months after vasectomy, in which case repeat vasectomy should be considered.
- If > 100,000 non-motile sperm/mL persist beyond six months after vasectomy, then trends of serial post- vasectomy semen analyses and clinical judgment should be used to decide whether the vasectomy is a failure and whether repeat vasectomy should be considered 19.
- Even after vas deferens occlusion is confirmed, vasectomy is not 100% reliable in preventing pregnancy. The risk of failure depends on a number of factors. For example, some surgical techniques are more likely to fail than others 1. Additionally, there is a very small risk that the two ends of the vas deferens will grow back together. If this happens, sperm may be able to enter the semen and make pregnancy possible 20.
- The risk of pregnancy after vasectomy is approximately 1 or 2 out of 1,000 couples get pregnant the first year after a vasectomy even after post-vasectomy azoospermia (absence of sperm during microscopic exam of at least 50 Hpfs in a single well mixed, uncentrifuged semen specimen) or post- vasectomy semen analysis showing rare non-motile sperm.
- Vasectomy is considered permanent, so once it’s done you don’t have to think about contraception again.
- Vasectomy doesn’t affect your sex drive or ability to enjoy sex. You’ll still have erections and ejaculate, but your semen won’t contain sperm.
- Your ball sack (scrotum) may become bruised, swollen or painful – some men have ongoing pain in their testicles. Chronic scrotal pain associated with negative impact on quality of life occurs after vasectomy in about 1-2% of men. Few of these men require additional surgery.
- As with any surgery, there’s a small risk of infection.
- Vasectomy is very difficult to reverse, so be sure it’s right for you.
- A vasectomy doesn’t protect against sexually transmitted infections (STIs), so you will need to use condoms as well.
- Vasectomy is intended to be a permanent form of contraception.
- Repeat vasectomy is necessary in ≤1% of vasectomies, provided that a technique for vas occlusion known to have a low occlusive failure rate has been used.
- Options for fertility after vasectomy include vasectomy reversal and sperm retrieval with in vitro fertilization (IVF). These options are not always successful, and they may be expensive.
- The rates of surgical complications such as symptomatic hematoma and infection are 1-2%. These rates vary with the surgeon’s experience and the criteria used to diagnose these conditions.
- Other permanent and non-permanent alternatives to vasectomy are available.
Before you decide to have a vasectomy
Your doctor will ask about your circumstances, provide information, and may recommend counseling before agreeing to the procedure.
You should only have a vasectomy if you’re certain you don’t want any more children or don’t want children at all.
If you have a partner, discuss it with them before you decide. If possible, you should both agree to the procedure, but it’s not a legal requirement to get your partner’s permission.
Once you have had a vasectomy, it’s very difficult to reverse it, so consider all options and use another method of contraception until you’re completely sure.
You may be more likely to be accepted for a vasectomy if you’re over 30 and have had children.
But your doctor can refuse to carry out the procedure, or refuse to refer you, if they don’t believe it’s in your best interests.
Which patients are good candidates for vasectomy?
Men older than 30 years in a stable, committed relationship appear to be the best candidates for vasectomy.
In a retrospective study involving 365 men who underwent vasectomy, patients in their 20s were 12.5 times more likely to request vasectomy reversal compared with men older than 30 years. In the same study, men whose wives worked outside the home were twice as likely to request vasectomy reversal compared with men whose wives stayed at home. Interestingly, men with children appear to request vasectomy reversal more than men without children. Religious affiliation, occupation, or number of marriages had no impact on request for reversal 21. Finally, change in marital status was strongly associated with request for reversal 22.
Is vasectomy linked to cancer?
Research shows that vasectomy does not increase a man’s risk of cancer. Some studies in the 1990s found that men who had undergone vasectomy had higher rates of prostate cancer. But findings from more recent studies have conclusively shown no link between vasectomy and prostate cancer. Indeed, men who have vasectomy are no more likely to get prostate cancer than men who do not have vasectomy 23. Vasectomy also does not increase a man’s risk of testicular cancer 1.
Post-Vasectomy Semen Analysis
Azoospermia: Absence of sperm during microscopic exam of at least 50 Hpfs in a single well mixed, uncentrifuged semen specimen.
Rare non-motile sperm: Presence of ≤100,000 non-motile sperm/mL based on microscopic exam of at least 50 Hpfs in a single well mixed, uncentrifuged post-vasectomy semen specimen assuming no motile sperm are observed
Recanalization: A histologic diagnosis that shows reconnection of the vas ends, either directly or by microcanaliculi, after vasectomy. Recanalization can be suspected clinically based on post-vasectomy semen analysis results or after an unexpected post-vasectomy pregnancy if a previous post-vasectomy semen analysis showed azoospermia or rare non-motile sperm.
Sterility: The inability to cause pregnancy
Can you reverse a vasectomy?
It’s possible to have a vasectomy reversed. But the procedure isn’t always successful. You have a better chance if it’s done soon after the vasectomy.
If a reversal is carried out within 10 years of your vasectomy, the success rate is about 55%. This falls to 25% if your reversal is carried out more than 10 years after.
Even if a surgeon manages to join up the vas deferens tubes again, pregnancy may still not be possible, so you should be certain before going ahead with the vasectomy.
How does a vasectomy work?
A vasectomy works by stopping sperm getting into a man’s semen, the fluid that he ejaculates.
The tubes (vas deferens) that carry sperm from a man’s testicles to the penis are cut, blocked or sealed with heat.
This means that when a man ejaculates, the semen has no sperm in it and a woman’s egg can’t be fertilized.
How will I know if my vasectomy has worked?
About 12 weeks after the procedure, you’ll need to produce a sample of semen, which will be tested for sperm.
Once tests have confirmed that your semen is sperm-free, the vasectomy is considered successful and you can stop using additional contraception.
Some men may need 2 tests. But until it’s been confirmed that your semen is free of sperm, continue to use another form of contraception.
A few men will continue to have small numbers of sperm in their system, but these sperm don’t move and are less likely to make your partner pregnant.
If you’re one of these men, your doctor will discuss your options with you.
The test also helps to identify the rare cases in which the tubes naturally rejoin themselves.
Can my partner tell if I have had a vasectomy?
Sperm adds very little to the semen volume, so you shouldn’t notice any change in your ejaculate after vasectomy. Your partner may sometimes be able to feel the vasectomy site. This is particularly true if you have developed a granuloma.
Will my sense of orgasm be changed by having a vasectomy?
Ejaculation and orgasm are usually not affected by vasectomy. The special case is the rare man who has developed post-vasectomy pain syndrome.
Can I become impotent after a vasectomy?
An uncomplicated vasectomy can’t cause impotence.
Can a vasectomy fail?
There is a small chance that a vasectomy may fail. This occurs when sperm leaking from one end of the cut vas deferens find a channel to the other cut end.
Can something happen to my testicles?
In rare cases, the testicular artery may be hurt during vasectomy. Other problems, such as a mass of blood (hematoma) or infection, may also affect the testicles.
Can I have children after my vasectomy?
Yes, but if you haven’t stored frozen sperm you’ll need an additional procedure. The vas deferens can be microsurgically reconnected in a procedure called vasectomy reversal. If you don’t want to have vasectomy reversal, sperm can be taken from the testicle or the epididymis and used for in vitro fertilization. These procedures are costly and may not be covered by your health plan. Also, they don’t always work. If you think you may want to have children one day, you should look into nonsurgical forms of birth control before deciding to have a vasectomy.
When and how should semen analysis be performed to check sterility?
One postvasectomy semen analysis demonstrating azoospermia performed after three months and 20 ejaculations is sufficient to establish sterility 24. The entire ejaculate should be obtained after a period of abstinence of two days (but no more than seven days), kept at body temperature, transported within 60 minutes of collection, and analyzed in the laboratory within four hours of ejaculation.
The lack of standardized postvasectomy semen analysis protocols in vasectomy studies has made it difficult to accurately measure failure rates. A systematic review of 56 studies suggested that about 80% of patients achieve azoospermia three months after vasectomy and after 11 to 20 ejaculations 24. A small number of patients (1.4%) had persistent nonmotile sperm after vasectomy; some eventually achieved azoospermia 24. The British Andrology Society recommends that patients with persistent nonmotile sperm undergo monthly postvasectomy semen analysis until one test demonstrates azoospermia or two consecutive tests demonstrate low numbers of nonmotile sperm (< 100,000 per mL) and seven months have elapsed since vasectomy. The latter group may also stop using contraception because the probability of pregnancy is extremely low 25.
Assuming vas deferens disruption and occlusion have been adequately achieved during surgery, and assuming the patient adheres to using another contraceptive method while awaiting confirmation of sterility, true causes of vasectomy failure include recanalization (early and late) and, more rarely, aberrant anatomy (e.g., the presence of a third vas deferens). The presence of motile spermatozoa during the three-month postvasectomy semen analysis likely represents vasectomy failure and should be confirmed with another semen analysis one month later. Once motile spermatozoa are reconfirmed, patients should be notified and repeat vasectomy recommended. Recanalization following vasectomy is rare (0.4%) and pregnancy is even rarer (0.07%) 24.
According to World Health Organization protocols, the entire ejaculate should be obtained by masturbation after a period of abstinence of two days (but no more than seven days), collected in a nontoxic container, kept at body temperature at all times, transported within 60 minutes of collection, and analyzed in the laboratory within four hours of ejaculation. Exceptions to this rigorous protocol can be made if there are extenuating circumstances. However, if sperm motility needs to be verified, this protocol must be followed exactly 26.
A common issue with postvasectomy semen analysis is compliance. In a review of 29 studies, a median of 19% of patients (range: 0% to 63%) failed to provide any semen sample. Of those who sent a semen sample, a median of 5% (range: 0% to 41%) only partially complied with the instructions 24. In response to this compliance issue, a novel, qualitative home test has been developed that can accurately detect sperm counts < 250,000 per mL (positive predictive value = 93%; negative predictive value = 97%). Although approved by the U.S. Food and Drug Administration, this test cannot assess sperm motility and is not yet supported by robust patient-oriented data in larger clinical trials 27.
Who can have a vasectomy?
You should only have a vasectomy if you’re sure that you don’t want more, or any, children. Vasectomy should always be seen as permanent.
This is because although vasectomy reversal is sometimes possible, it may not be successful. Even with a successful operation, it may still not be possible to father a child.
Can I have the vasectomy operation if I’m single?
Yes. But if you’re under 30, you’ll find many surgeons are reluctant to do it in case your circumstances change and you regret it later.
Will vasectomy affect my sex drive?
No. After a successful vasectomy, your testicles will continue to produce the male hormone (testosterone) just as they did before the procedure.
Your sex drive, sensation and ability to have an erection won’t be affected. The only difference is that there’ll be no sperm in your semen. Your body still produces sperm, but they’re absorbed back into your body without harm.
Could being sterile affect me emotionally?
It’s a big decision to have a vasectomy, so you should think it over carefully. If you’re sure about your decision, you may feel relieved that you don’t need to think about contraception and the possibility of pregnancy again.
But if you feel anxious or uncomfortable about the procedure, or you think you would find it hard to accept being infertile, it may not be suitable for you.
See a doctor or a professional at a contraception or sexual health clinic to talk about all of your options.
Can I use IVF to father a child?
If you have a vasectomy and later decide that you want a child, you may be able to use IVF. To do this, a surgeon would retrieve sperm from your testicles and use this to fertilize your partner’s egg.
But IVF:
- isn’t always successful
- can be expensive if done privately
Can I store sperm in a sperm bank, just in case?
You could, but as with IVF, sperm stored in a sperm bank can’t be relied on to bring about a pregnancy. It can also be expensive.
Advantages and disadvantages of a vasectomy
Vasectomy advantages
- a vasectomy is more than 99% effective at preventing pregnancy
- long-term effects on your health are rare
- it doesn’t affect your hormone levels, sex drive or interfere with sex
- it may be chosen as a simpler and safer alternative to female tubal ligation
Vasectomy disadvantages
- vasectomy doesn’t protect against STIs, so you may need to use condoms as well
- a vasectomy can’t be easily reversed
- you need to keep using contraception after the operation until tests show your semen is free of sperm
- possible complications include a collection of blood inside the scrotum (hematoma), hard lumps called sperm granulomas (caused by sperm leaking from the tubes), an infection, or long-term testicle pain (you may need further surgery)
- the vas deferens tubes can reconnect, but this is very rare
What is vas deferens
The vas deferens or the ductus deferens is a continuation of the duct of the epididymis (the spermatic cord). The term vasectomy, the surgical method of male contraception, consists of cutting out a short portion of the ductus deferens to interrupt the passage of sperm out of the testicles. Vas deferens is a muscular tube about 45 cm long and 2.5 mm in diameter. From the tail of the epididymis, it passes upward within the spermatic cord and inguinal canal and enters the pelvic cavity. There, it turns medially and approaches the urinary bladder. After passing between the bladder and ureter, the duct turns downward behind the bladder and widens into a terminal ampulla.
The vas deferens ends by uniting with the duct of the seminal vesicle. The duct has a very narrow lumen and a thick wall of smooth muscle well innervated by sympathetic nerve fibers.
The wall of the vas deferens consists of:
- An inner mucosa with the same pseudostratified epithelium as that of the epididymis, plus a lamina propria.
- An extremely thick muscularis. During ejaculation, the smooth muscle in the muscularis creates strong peristaltic waves that rapidly propel sperm through the ductus deferens to the urethra.
- An outer adventitia of connective tissue.
The ejaculatory duct is about 2 cm (1 in.) long and is formed by the union of the duct from the seminal vesicle and the ampulla of the vas deferens (see Figure 2). The short ejaculatory ducts form just superior to the base (superior portion) of the prostate and pass inferiorly and anteriorly through the prostate. They terminate in the prostatic urethra, where they eject sperm and seminal vesicle secretions just before the release of semen from the urethra to the exterior.
Figure 1. Vas deferens location
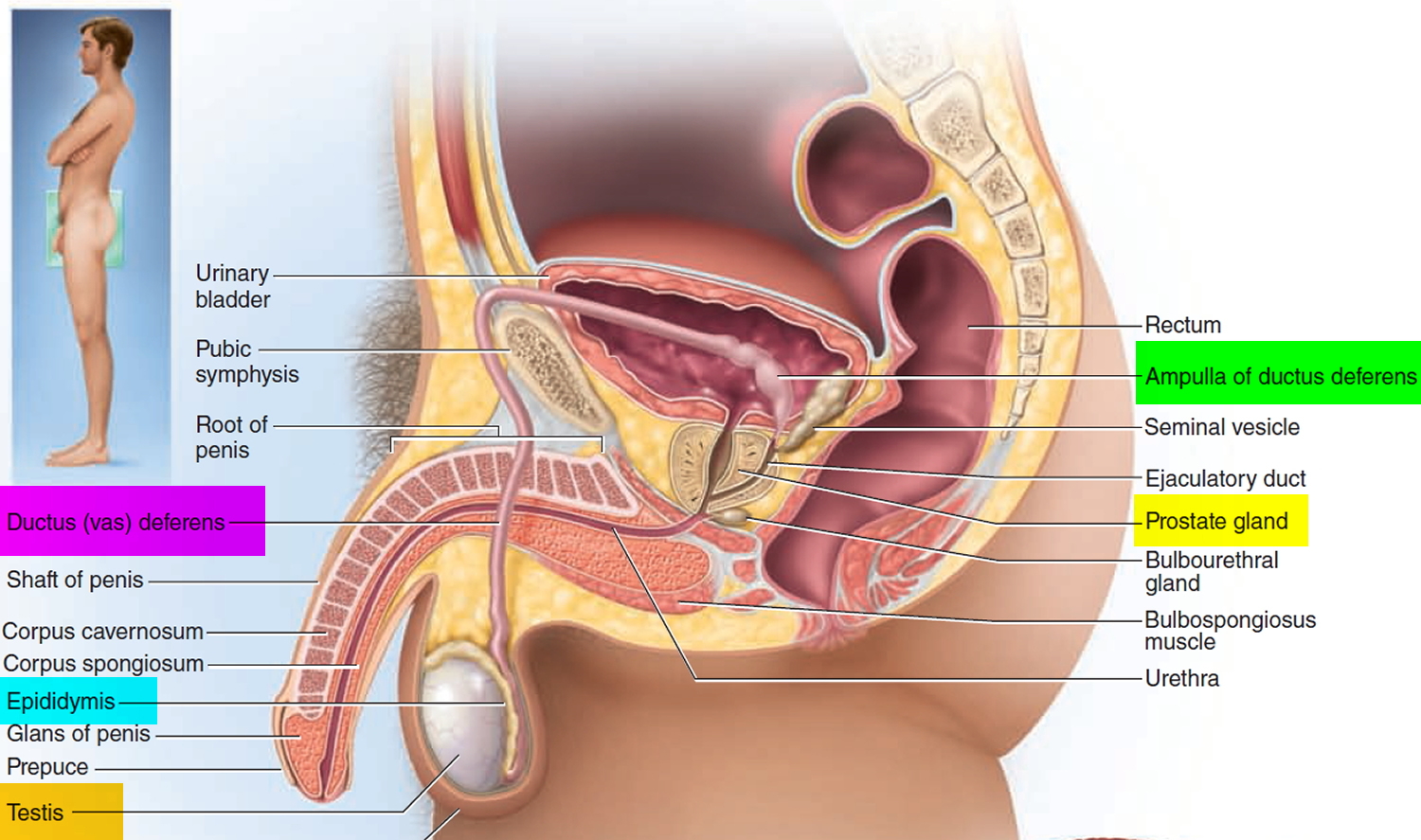
Figure 2. Vas deferens

Vas deferens function
The ductus deferens or vas deferens, stores and transports sperm during ejaculation from the epididymis to the urethra. During ejaculation, vas deferens coordinated muscular contractions propel the spermatozoa toward the urethra. However, the vas deferens does not serve only as a conduit, but also contributes to secretion of fluid for sperm transport and possibly to resorption of spermatozoan remnants from the duct lumen 28.
Vasectomy procedure
A vasectomy is a quick and relatively painless surgical procedure. In most cases, you’ll be able to return home the same day.
Accessing the vas deferens
Accessing the vas deferens can be achieved with a single or double incision to the scrotum using a scalpel, or with the no-scalpel technique using special instruments. No-scalpel vasectomy, in contrast to the traditional incisional technique, is a minimally traumatic approach to accessing the vas deferens that reduces operative complications, shortens operative time, and hastens resumption of sexual activity. No-scalpel vasectomy has been shown to reduce the risk of complications (i.e., bleeding and infection) compared with the incision technique 29. Two randomized controlled trials showed a 1.7- to 6.8-fold reduction in bleeding and hematomas and a 1.6- to 7.5-fold reduction in infections with the no-scalpel technique compared with the incision technique 29, 30. No-scalpel vasectomy is therefore the preferred technique 31.
There are 2 types of vasectomy:
- a conventional vasectomy using a scalpel (surgical knife)
- a no-scalpel vasectomy
The doctor doing your vasectomy will discuss which option is best for you.
Conventional vasectomy
The doctor first numbs your scrotum with a local anesthetic. They then make 2 small cuts in the skin on each side of your scrotum to reach the tubes (vas deferens) that carry sperm out of your testicles.
Each tube (vas deferens) is cut and a small section removed. The ends of the vas deferens tubes are then closed, either by tying them or sealing them using heat.
The cuts are stitched, usually using dissolvable stitches that go away on their own within about a week.
No-scalpel vasectomy
The doctor first numbs your scrotum with local anesthetic. They then make a tiny puncture hole in the skin of your scrotum to reach the tubes. This means they don’t need to cut the skin with a scalpel.
The vas deferens tubes are then closed in the same way as a conventional vasectomy, either by being tied or sealed.
There’s little bleeding and no stitches with this procedure. It’s thought to be less painful and less likely to cause complications than a conventional vasectomy.
What is No-Needle Vasectomy?
No-needle vasectomy involves an alternative technique of administering local anesthesia using a high-pressure jet injector. It may reduce pain associated with local anesthetic infiltration.
No-needle vasectomy is an increasingly popular alternative to the standard local infiltration technique that uses a hypodermic needle. This technique uses a jet injection device (Figure 3) to deliver high-pressure anesthetic spray through intact skin and into the vas and surrounding tissues. A small single-blind randomized controlled trial involving 50 patients demonstrated a statistically significant improvement in pain from anesthetic administration with no-needle vasectomy compared with needle injection. However, there was no difference in intraoperative pain between the two techniques 32. Although the jet injector can prevent injury from needlestick and eliminate the burden of syringe and needle disposal, its disadvantages include the initial cost of the device and the potential for inadvertent self-injection of the physician’s middle finger through a scrotal exit wound created by the high-pressure spray when using the three-finger technique for vas deferens isolation.
Figure 3. No-needle vasectomy procedure – high-pressure jet injector for delivering anesthetic spray

Disrupting the vas deferens
Disruption of the vas deferens can be performed numerous ways (Figure 4). Simple suture ligation with excision likely is the most common method worldwide 33, although this method has been shown to be less effective than previously reported 34. In addition, there is increasing concern that ligating the vas deferens, regardless of technique, often causes tip necrosis and sloughing; this can lead to recanalization of a vasal segment 35. A large randomized trial that included patients in seven countries noted vasectomy failure (i.e., live sperm present 24 weeks after the procedure) in 12.7 percent of men who received suture ligation and excision alone from an experienced physician 36.
A retrospective Canadian study comparing cautery and fascial interposition with clip ligation and excision reported an 8.7 percent failure rate in patients who received clip ligation and excision 37. The seven-country study showed that adding fascial interposition to suture ligation and excision decreased the failure rate to 5.9 percent 36. These data confirm added protection from fascial interposition. The use of cautery, alone or with fascial interposition, appears to significantly decrease failure rates. The Canadian study showed that cautery with fascial interposition had a 0.3 percent failure rate 37. An observational study reported an early failure rate (i.e., live sperm 12 weeks after vasectomy) of 1 percent with cautery alone 38.
Management of the vas deferens ends, which determines the procedure’s effectiveness, can be accomplished in various ways but fascial interposition should be used routinely because it decreases vasectomy failure rates significantly. A systematic review of six randomized controlled trials demonstrated no difference in failure rate between the ligation and excision technique compared with vas occlusion with surgical clips (without transection of the vas) 39. The same study evaluated the effects of fascial interposition, a method of burying one vasal end within the vasal sheath or surrounding connective tissue to separate the anatomic plane between the two vasal ends, hence minimizing the risk of recanalization. Fascial interposition was found to significantly reduce vasectomy failure at 34 weeks compared with no fascial interposition; however, it lengthened the operative time by two to three minutes 39. Vas irrigation with water (vs. no water) or with spermicidal agent (vs. water) has not been shown to decrease vasectomy failure rates. No randomized controlled trial has evaluated the effectiveness of fulguration or electrocautery to occlude the vasal ends, or examined leaving the vasal ends open (without the use of sutures, clips, or fulguration) 39.
Intraluminal cautery without separation of the vas deferens currently is the preferred method practiced at Marie Stopes International health centers (multinational family planning clinics where 100,000 vasectomies have been performed worldwide) 40. These clinics report a less than 1 percent failure rate with this technique 40. Two studies have compared thermal and electric cautery 41, 42. One study showed a nonsignificant increase in failure rates with electric cautery,18 and the other study showed histologic evidence of more reliable occlusion with thermal cautery 42. Although these studies provide some evidence that thermal cautery is more effective than electric, no firm conclusions about optimal route or type of cautery can be made.
Leaving the testicular end open after the vas deferens disruption phase of vasectomy has the theoretical advantage of decreasing post-vasectomy vasal pressure; however, it also causes a sperm granuloma at the open end 43. Early studies reported a significant decrease in chronic pain with this technique, implying that most chronic pain resulted from congestive epididymitis rather than a granuloma 43, 44. A large retrospective study of 3,761 men who received vasectomies showed no difference in postoperative scrotal pain between open- and closed-ended techniques 37.
Figure 4. Vasectomy
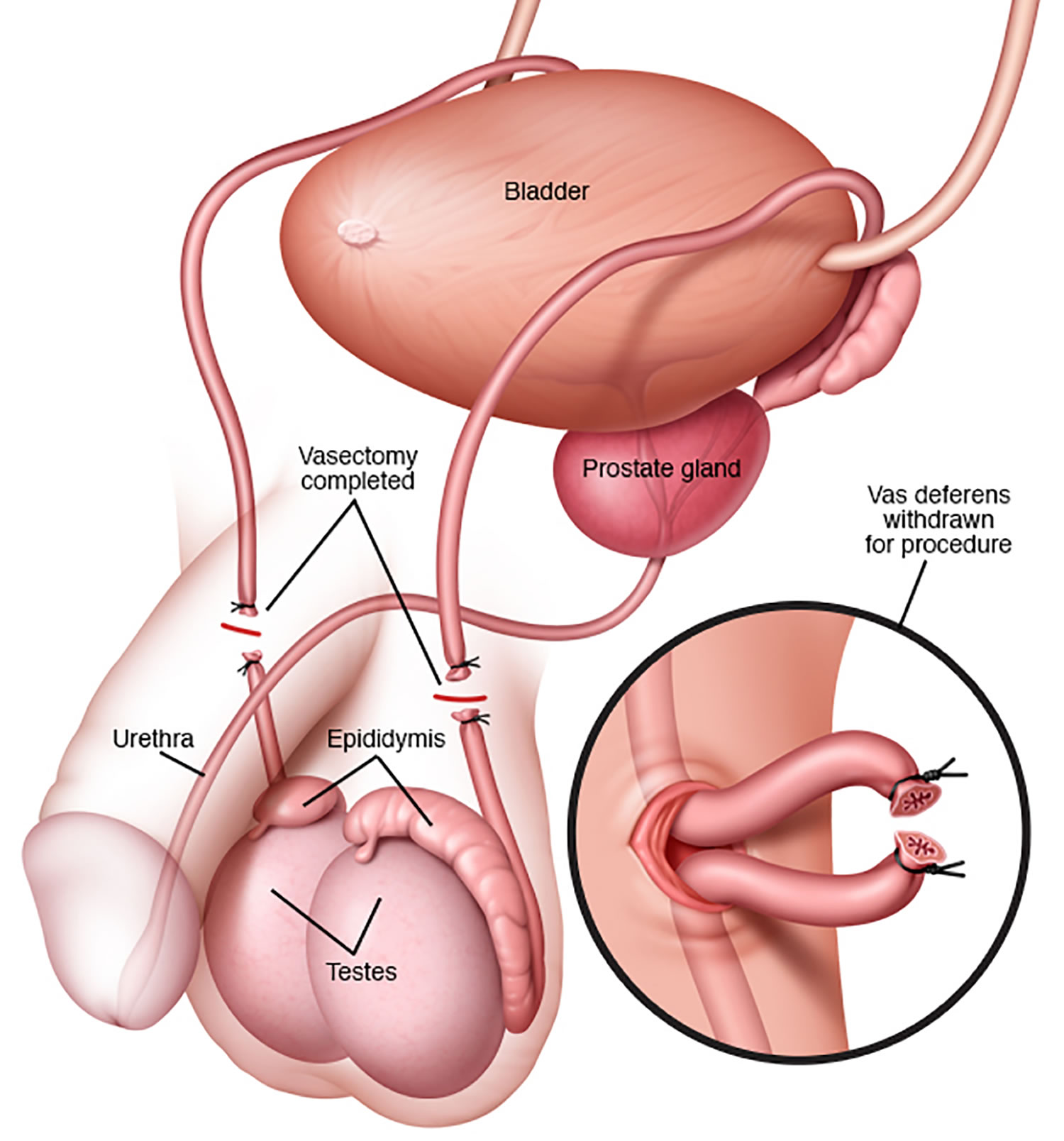 Figure 5. Vas deferens disruption methods for vasectomy
Figure 5. Vas deferens disruption methods for vasectomy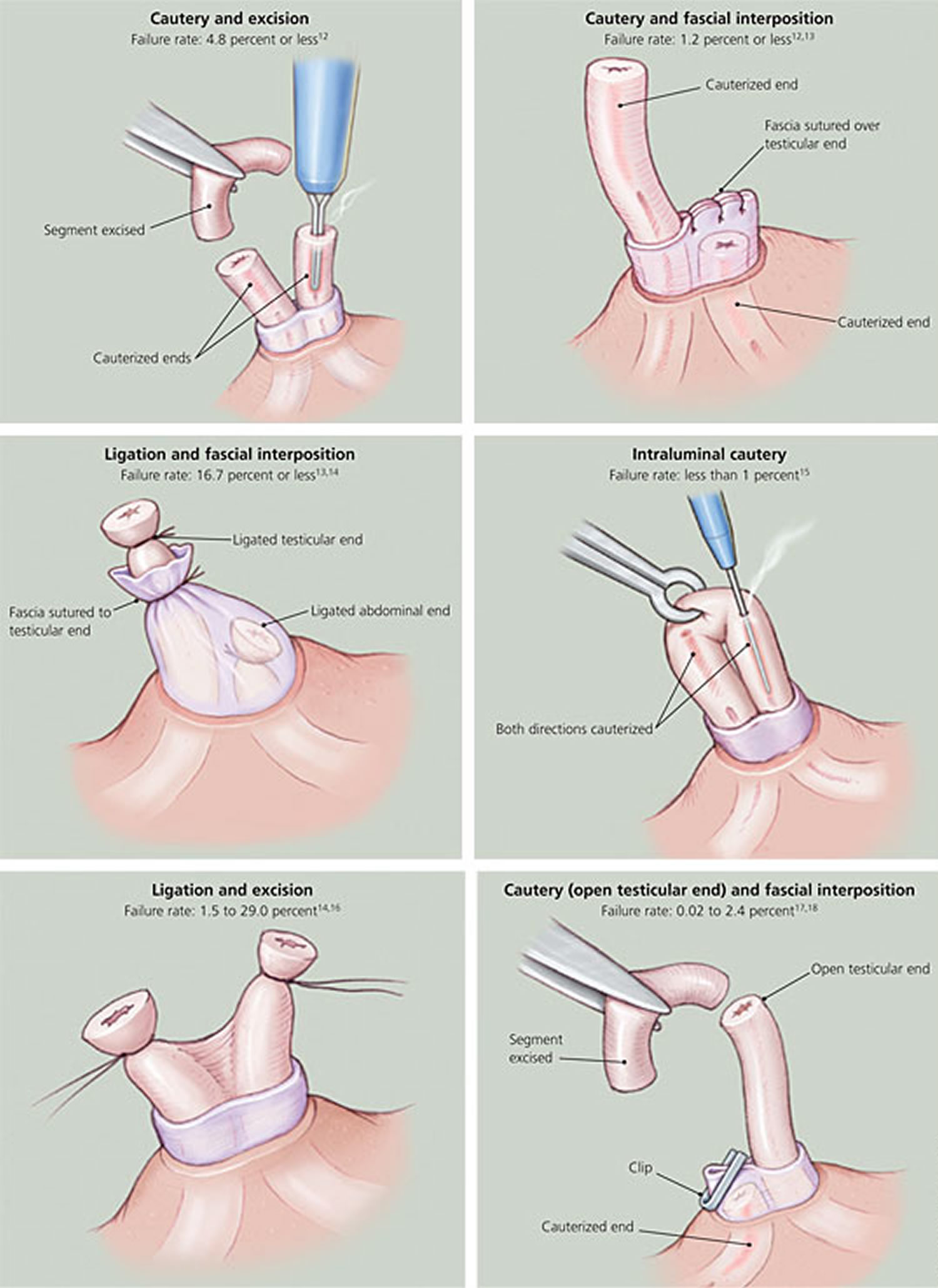
Scrotal closure
Scrotal closure can be accomplished with clips, clamps, sutures, or cyanoacrylate tissue adhesive. The incision also may be left open to heal by secondary intention. Data comparing these methods are limited; therefore, further data are needed before recommendations regarding closure technique can be made.
Vasectomy recovery
Recovering after the vasectomy operation
It’s common to have some mild discomfort, swelling and bruising of your scrotum for a few days after the vasectomy.
Appropriate recommendations include intermittent ice applications to the scrotum for eight hours, bed rest and scrotal support for 48 hours, and avoidance of heavy exertion for one week.
You can take painkillers, such as acetaminophen (paracetamol), usually provides sufficient analgesia. See a doctor if it’s still painful after taking painkillers, occasionally narcotic analgesics are necessary.
It’s common to have blood in your semen in the first few ejaculations after a vasectomy. This isn’t harmful.
You can have sex again as soon as it’s comfortable to do so. Another method of contraception should be used until semen analysis has confirmed azoospermia.
Underwear
Wear tight-fitting underwear or athletic support day and night for the first few days to help support your scrotum and ease any discomfort or swelling. Make sure you change your underwear every day.
Hygiene
It’s usually safe for you to have a bath or shower after your operation – check with your doctor what’s suitable for you. Make sure you dry your genital area gently and thoroughly.
Vasectomy recovery time
You can usually return to work 1 or 2 days after a vasectomy, but should avoid sport and heavy lifting for at least a week after the procedure to prevent complications. See a doctor if you still have symptoms after a few days.
Having sex
You can have sex again as soon as it’s comfortable to do so. You’ll need to use another method of contraception for at least the first 8 to 16 weeks, as it can take this long to clear the remaining sperm in your tubes.
How long this takes varies from man to man. There’s still a risk of pregnancy during this time.
Follow-up care
Follow-up after a vasectomy should include one or more semen samples to ensure that recanalization has not occurred 45. Unfortunately, many men do not comply with this recommendation. A case series reported that less than one half (42 percent) of men who received a vasectomy provided a postvasectomy semen sample. Of those who provided an initial sample, only 25 percent provided a subsequent sample 46.
Two studies showed that the median time to loss of sperm motility was three weeks after vasectomy and the median time to azoospermia was 10 weeks 47. A finding of rare, nonmotile sperm after 12 weeks reliably predicts long-term sterility 48; therefore, subsequent monthly samples after 12 weeks is recommended only for those with motile sperm 49. Patients who want earlier confirmation of sterility should be counseled that a second sample is more likely to be needed if the first sample is given before 12 weeks.
Vasectomy effectiveness
Vasectomy is the most effective and the only permanent method of male contraception, with a failure rate of less than 1% in pooled studies 50. Only about 1 or 2 out of 1,000 couples get pregnant the first year after a vasectomy 51. Among 1,000 vasectomies, 11 will likely fail over 2 years; and half of these failures will occur within the first 3 months after surgery 13. The risk of failure depends on a number of factors. For example, some surgical techniques are more likely to fail than others 1. Additionally, there is a very small risk that the two ends of the vas deferens will grow back together. If this happens, sperm may be able to enter the semen and make pregnancy possible 20.
Men or their partners should use other contraceptive methods until vasectomy success is confirmed by post- vasectomy semen analysis. To evaluate sperm motility, a fresh, uncentrifuged semen sample should be examined within two hours after ejaculation. Patients may stop using other methods of contraception when examination of one well-mixed, uncentrifuged, fresh post-vasectomy semen specimen shows azoospermia or only rare non-motile sperm (≤ 100,000 non-motile sperm/mL).
Vasectomy effectiveness can also be defined as either contraceptive effectiveness or occlusive effectiveness. The standard definition of contraceptive effectiveness is the absence of pregnancy (see above). The standard definition of occlusive effectiveness is post-vasectomy azoospermia. However, some men fail to achieve azoospermia after vasectomy yet never father a pregnancy. For example, one study found sperm in the semen of 18 of 186 (9.7%) men prior to vasectomy reversal 52. The average time since vasectomy was 10.7 years and no pregnancies occurred in the partners of these 18 men. Thus the definition of occlusive effectiveness should not be restricted to azoospermia but should include those men whose post- vasectomy semen analyses show rare non-motile sperm or ≤100,000 non-motile sperm/mL and no sperm motility.
Table 1. Birth control methods effectiveness and their risks and side effects
| Method | How it is Used | Failure Rate (average use) | Risks & Side Effects |
| Abstinence | No sexual intercourse and no type of contact between the male and female sexual organs where bodily fluids could be exchanged | 0% | No Side Effects |
| Cervical Cap | A soft rubber barrier that covers the cervix in order to prevent sperm from entering the uterus | 12% (higher after childbirth) | No Side Effects (unless allergic) |
| Condom – Female | A sheath, often made of latex rubber, inserted into the vaginal canal to block the passage of sperm | 21% | No Side Effects (unless allergic) |
| Condom – Male | A sheath, often made of latex rubber, covering the erect penis to block the passage of sperm | 18% | No Side Effects (unless allergic) |
| Depo-Provera Injection | Injection of Progestin that is given every 3 months to prevent ovulation, change cervical mucus to block sperm, and change the lining of the uterus to prevent implantation of a fertilized egg | 6% | Irregular, missed, or heavier than normal menstrual cycle, weight gain, breast tenderness, depression, bloating, abdominal pain, headaches, allergic reaction |
| Diaphragm | A soft rubber dome that covers the cervix to block the passage of sperm. | 12% | No Side Effects (unless allergic) |
| Fertility Awareness | Using the menstrual cycle and other tools to predict ovulation and abstaining from intercourse during these expected fertile times | 25% | No Side Effects |
| Implant – Hormonal | A small, matchstick-sized implant inserted in the upper arm and lasts for 3 years, releasing a hormone supply. Works in a similar way to Depo-Provera. | 0.05% | No period, spotting, light or heavy and prolonged bleeding; painful menstruation, acne, weight gain, depressed mood; blood clots, movement of implant, ectopic pregnancy, ovarian cysts |
| Intrauterine Device (IUD) – Copper | A device is inserted into a woman’s uterus (by a doctor) to block sperm and change the uterus lining to prevent implantation of a fertilized egg | 0.8% | Ectopic pregnancies, increased bleeding during menstrual cycle, severe menstruation cramps, perforation of the uterus, Pelvic Inflammatory Disease (PID) |
| Intrauterine Device (IUD) – Progestin | 0.2% | ||
| Nothing/Chance | No birth control method | 85% | No Side Effects; highest chance of unintended pregnancy |
| Oral Contraceptive (estrogen/progestin) | Taken daily by women to suppress ovulation, change cervical mucus, and change the lining of the uterus to prevent implantation of a fertilized egg | 9% | Nausea, headaches, weight gain, depression, irregular bleeding, acne, blood clots *Women who smoke are advised not to take oral contraceptives |
| Oral Contraceptive (progestin only) | Taken daily by women to change cervical mucus to block sperm and also changes the uterus lining to prevent implantation of a fertilized egg | 9% | Breast tenderness, weight gain, menstrual cycle changes *Women who smoke are advised not to take oral contraceptives |
| Ortho-Evra Patch | A patch containing synthetic hormones placed on your skin; works the same as oral contraceptives | 9% (greater if over 198 lbs) | Similar to oral contraceptives |
| Spermicide (only) | A jelly, foam, or cream containing chemicals that kill sperm | 28% | No Side Effects (unless allergic) |
| Sponge | A soft saucer-shaped polyurethane sponge that blocks the cervix and absorbs semen | 20% (40% after childbirth) | No Side Effects (unless allergic) |
| Sterilization – Female | Permanent surgical procedure to prevent pregnancy: fallopian tube is damaged (cut, tied, burnt) to prevent passage of eggs and sperm | 0.5% | If a woman conceives after a sterilization procedure there is a risk of ectopic pregnancies. The earlier the age of the woman at the time of the procedure, the greater risk of pregnancy after 10 years (up to ~5%). |
| Sterilization – Male | Permanent surgical procedure to prevent pregnancy: vas deferens tube is damaged (cut, tied, burnt) to prevent passage of sperm into ejaculate fluid | 0.15% | No Side Effects |
| Vaginal Ring – Hormonal | A flexible ring placed inside the vagina near the cervix. Active for 3 weeks. Has actions similar to oral contraceptives. | 9% | Blood clots, liver or gallbladder problems, TSS, depressed mood, acne, headache, weight gain, nausea/vomiting, movement of the ring |
| Withdrawal | Withdrawal of the penis before ejaculation | 22% | No Side Effects |
Table 2. Prevalence of Contraceptive Methods
| Method | Prevalence (%)* |
|---|---|
Oral contraceptive | 30.6 |
Female sterilization | 27.0 |
Male condom | 18.0 |
Vasectomy | 9.2 |
Three-month injectable | 5.3 |
Withdrawal | 4.0 |
Other† | 4.0 |
Intrauterine device | 2.0 |
Vasectomy failure
Vasectomy failure is the occurrence of pregnancy or failure to achieve azoospermia or rare non-motile sperm after a reasonable period of time following vasectomy. Vasectomy failure may be a technical failure resulting from a surgical error such as occluding one vas deferens twice without occluding the other vas or failure to identify the very rare situation of vas duplication on one side. Technical failure is characterized by persistently normal or nearly normal motile sperm counts and sperm motility after vasectomy. Vasectomy failure also may result from recanalization at the vasectomy site.
Recanalization following vasectomy should be suspected if motile sperm or rising sperm concentrations are seen after a routine post- vasectomy semen analysis has shown azoospermia or rare non-motile sperm. Recanalization can be either transient or persistent based on the results of serial post- vasectomy semen analyses. It is impossible to know the true incidence of late recanalization because post- vasectomy semen analysis is rarely repeated after a post- vasectomy semen analysis shows azoospermia or rare non-motile sperm. Pregnancy due to recanalization is estimated to occur after approximately 1 in 2000 vasectomies or less often 55. The incidence of recanalization is very likely greater than the reported rate of pregnancy after post-vasectomy azoospermia because not all recanalizations result in pregnancy.
Sperm clearance after vasectomy is time dependent with both large inter-individual variations as well as variability across published reports, including those that used the same vas occlusion technique. Inter-individual variation may result from differences in reproductive anatomy and possibly patient age. Sperm may persist in the ejaculate for many months after vasectomy. Such persistence may be due to residual sperm in the seminal vesicles or ampullae of the vasa 56, recanalization, or, very rarely, a failure to have performed the vasectomy on one vas. The main reason for the presence of non-motile sperm is probably that residual sperm in the seminal vesicles or ampullae of the vasa are slowly released from the reproductive tract 56. There are wide variations in the clearance of residual sperm in the seminal vesicles or ampullae of the vasa among men due to inter-individual differences in the anatomy of these structures 56. However, in most men, either no sperm or only small numbers of non-motile residual sperm in the post- vasectomy semen analysis are seen at three months or later after vasectomy. Nevertheless, some men have continued to have sperm or sperm parts in the semen which have been found for as long as 31 years post-vasectomy 52.
With regard to age, several studies have suggested that sperm clearance may take longer in older men compared to younger men 11. For example, Marshall and Lyon 57 reported that younger patients may achieve azoospermia with fewer ejaculations than older patients. Marwood 58 reported that the frequency of ejaculation affected time to azoospermia more in older than in younger men, with a frequency of three times a week associated with rapid clearance regardless of age.
The published literature also contains mixed results regarding the relationship between sperm clearance and number of ejaculations. After 10 ejaculations, rates of azoospermia ranged from 43% to 50% 59. After 12 ejaculations, rates of azoospermia have been reported as 66% 57 and 88% 60. However, one study with relatively complete follow up showed that only 44% of patients were azoospermic after 20 ejaculations 61. Many practitioners recommend that the first post- vasectomy semen analysis should be done after 20 ejaculations.
Variability across published reports in sperm clearance rates may result from surgical technique used to occlude the vas deferens; differences in criteria for vasectomy success (e.g., one, two or three azoospermic specimens); variations in post- vasectomy semen analysis laboratory techniques and reporting; small sample sizes in some studies and varying time points at which post- vasectomy semen analysis was performed. In addition, in many studies, although patients were instructed to report at specific intervals post-vasectomy, some report at later intervals. This inconsistency between requested post- vasectomy semen analysis timing and actual post- vasectomy semen analysis timing creates uncertainty regarding true sperm clearance rates because not all articles clearly indicate when patients actually returned for post- vasectomy semen analyses. In addition, in most studies about a third of patients do not return for the requested post- vasectomy semen analyses 62. The lack of complete follow-up data also creates uncertainty regarding true sperm clearance rates.
Another source of variation in the proportion of men achieving azoospermia is variation in the laboratory techniques used for post- vasectomy semen analysis and for reporting of post- vasectomy semen analysis results. Rigorous semen examination including centrifugation and examination of hundreds of microscopic fields is likely to find more sperm than less rigorous laboratory techniques. If the physician sends post- vasectomy semen analysis specimens to a commercial laboratory, the physician should request that the laboratory perform the post- vasectomy semen analysis without centrifugation because centrifugation may reduce or eliminate sperm motility. The physician should also request the laboratory to report both the presence or absence of sperm and the presence or absence of sperm motility. If only non-motile sperm are present, the physician should request the laboratory to report the number of non-motile sperm per mL. If no sperm are found in the uncentrifuged specimen, then ideally the laboratory should report that the presence of sperm is “below the limit of detection,” although most laboratories report “azoospermia” in this situation.
Clearance of motile sperm. Clearance of motile sperm is much more rapid than clearance of non-motile sperm. Older studies suggest all motile sperm disappear within three weeks after vasectomy 63. More recent studies confirm that when mucosal cautery and fascial interposition are combined to occlude the vas deferens, essentially all motile sperm have disappeared by five to six weeks 64 with only 1% of men continuing to show motile sperm 65. At 7 to 14 weeks, this proportion drops to 0.4% and by more than 14 weeks post-vasectomy, no motile sperm were observed 65.
Numerous studies have reported the reappearance of nonmotile sperm 66 and even motile sperm 67 after azoospermia was confirmed, with most studies reporting this phenomenon in small numbers of patients (i.e., < 1%). However, it should be noted that many patients in these studies did not return for post- vasectomy semen analyses or did not return for a second post- vasectomy semen analysis when requested, making the true rates of sperm reappearance (both motile and non-motile) unclear.
Vasectomy side effects
Although vasectomy is safe and highly effective, men should be aware of problems that could occur after surgery and over time 68.
Bleeding and hematoma formation, the most common complications of vasectomy, often result from injury to the pampiniform venous plexus. Perioperative bleeding occurs in 2.4% of no-scalpel vasectomies and 4.0% of incisional vasectomies, whereas hematoma occurs in 2.4% of no-scalpel vasectomies and 12.5% of incisional vasectomies 31. In extreme cases, these complications can lead to significant morbidity necessitating surgical interventions such as hemostasis, scrotal exploration, and hematoma evacuation. Postoperative infection occurs in 0.7% of no-scalpel vasectomies and 2.2% of incisional vasectomies 31.
Surgical Risks
After surgery, most men have discomfort, bruising, and some swelling, all of which usually go away within 2 weeks. Problems that can occur after surgery and need to be checked by a health care provider include:
- Hematoma. Bleeding under the skin that can lead to painful swelling.
- Infection. Fever and scrotal redness and tenderness are signs of infection 69.
Other Risks
The risk of other problems is small, but they do occur. These include:
- A lump in the scrotum, called a granuloma. This is formed from sperm that leak out of the vas deferens into the tissue 70. A sperm granuloma forms as an immunologic reaction to the extravasation of sperm from the testicular vasal end. This process is hypothesized to be protective because it prevents epididymal and testicular obstruction. Although most sperm granulomas are not painful and often disappear over time, they are believed to play a role in postvasectomy pain syndrome and recanalization during vasectomy failure 71.
- Postvasectomy pain syndrome is persistent or recurrent scrotal pain that occurs months or years after vasectomy. It is thought to be caused by underlying chronic epididymal congestion. Recent studies estimate the incidence of severe postvasectomy pain syndrome to be between 1% and 6% 72. Mild postvasectomy pain syndrome is treated symptomatically, whereas severe cases may require vasectomy reversal.
- Vasectomy failure. There is a small risk that the vasectomy will fail. This can lead to unintended pregnancy.
- Risk of regret. Vasectomy may be a good choice for men and/or couples who are certain that they do not want more or any children. Most men who have vasectomy, as well as spouses of men who have vasectomy, do not regret the decision 73. Men who have vasectomy before age 30 are the group most likely to want a vasectomy reversal in the future 1.
Vasectomy reversal
Vasectomy reversal reconnects the pathway for the sperm to get into the semen. Most often, the cut ends of the vas are reattached. In some cases, the ends of the vas are joined to the epididymis. These surgeries can be done under a special microscope (“microsurgery”). When the tubes are joined, sperm can again flow through the urethra. Vasectomy reversal is relatively expensive and its success rate is highly variable 74. There are many reasons to undo a vasectomy. Two studies showed that change in marital status was the most common reason for wanting a reversal 75. A case-control study showed that age younger than 30 years at the time of the vasectomy and having a spouse who worked outside of the home were associated with later requests for reversal 76. The authors conceded that the latter association likely was multifactorial and culturally based. There was no association between requests for reversal and the patient’s religion, occupation, or number of marriages. Having no children at the time of the vasectomy was associated with a lower risk of a reversal request 76.
Vasectomy reversal techniques involve reanastomosis of the testicular and prostatic vasal ends (vasovasostomy) or connecting the vas to the epididymis (vasoepididymostomy). To reverse a vasectomy, the surgeon makes a small cut in the side of the scrotum and finds the closed ends of the vas deferens. Then a fluid sample is taken from the end closest to the testicle to test for the presence of sperm. If sperm is found in the fluid, the two closed ends of the vas deferens can be reattached 77. Many doctors perform the reversal using a microsurgical approach. Here, a high-powered microscope is used to magnify the ends of the vas deferens. It allows the surgeon to use smaller stitches—as small as an eyelash—which reduces scarring. Microsurgery returns sperm to the semen in the majority of reversals 77.
Vasovasostomy patency rates have been reported between 75% and 86%; pregnancy rates range from 45% to 70% 78. Vasoepididymostomy, a technique used in the presence of epididymal obstruction, has patency rates between 31% and 92%, and pregnancy rates between 10% and 50% 78. Repeat attempts at microsurgical vasectomy reversal appear less successful than first attempts with patency rates between 75% and 79%, and pregnancy rates between 31% and 43% 79.
What happens during vasectomy reversal?
Reversals are most often done on a come-and-go basis by a urologist. Reversals can be done in an outpatient part of a hospital or at a surgery center. If a surgical microscope is used, the surgery is done while you’re asleep under anesthesia. Your urologist and anesthesiologist will talk with you about your choices.
Using microsurgery is the best way to do this surgery. A high-powered microscope used during your surgery magnifies the small tubes 5 to 40 times their size. Your urologist can use stitches much thinner than an eyelash or even a hair to join the ends of the vas.
After you’re asleep, your urologist will make a small cut on each side of the scrotum. Your urologist will trim the scarred ends of the vas where they were closed by the vasectomy. Your urologist will take fluid, (“vasal fluid”) from the vasal end closest to the testis. Your doctor will check to see if it has sperm in it. At this point, there are 2 types of reversal procedures you can have:
Vasovasostomy
If there is sperm in the vasal fluid it shows that the path is clear between the testis and where the vas was cut. This means the ends of the vas can then be joined. The term for reconnecting the ends of the vas is “vasovasostomy.” When microsurgery is used, vasovasostomy works in about 85 out of 100 men. Pregnancy occurs in about 55 out of 100 partners.
Vasoepididymostomy
If there is no sperm in the vasal fluid, it may mean back pressure from the vasectomy caused a form of “blowout” in the epididymal tube. This “blowout” can lead to a block. Your urologist will need to go around the block and join the upper end of the vas to the epididymis instead. This is called a “vasoepididymostomy” and it serves the same purpose as the vasovasostomy.
Vasoepididymostomy is more complex than vasovasostomy, but the results are nearly as good. Sometimes vasovasostomy is done on one side and vasoepididymostomy on the other.
Should I have a vasovasostomy or a vasoepididymostomy?
You can’t tell before the vasectomy reversal which method is best for you. Your urologist can only find this out during the surgery. If sperm are found in the vasal fluid, then a vasovasostomy is done. If there are no sperm in the fluid, your urologist will decide what to do based on other factors. If there’s a block in the epididymal tube, then a vasoepididymostomy will be needed.
If no block is found, then the way the vasal fluid looks may help your urologist decide which method is best. For the most part, if the fluid looks watery, he/she will tend to do a vasovasostomy even if no sperm are found in the fluid. Fluid that looks creamy without sperm suggests that vasoepididymostomy is needed. Some patients may need a vasovasostomy on one side and a vasoepididymostomy on the other.
What can I expect after a vasectomy reversal?
Healing should be rather quick and fairly easy. Pain after surgery is most often controlled with pills. About 50 out of 100 men say the pain after the reversal is like after their vasectomy. Another 25 out of 100 say the pain is less than after the vasectomy, and 25 out of 100 say it’s greater. Pain bad enough to need medications rarely lasts longer than a few days to a week.
Most men can return to their normal routine and light work within a week. You’ll likely be told to take it easy and not have sex for 2 to 3 weeks. If your job is strenuous, ask your urologist when you can return to work. You’ll most likely wear a jockstrap for support for a few weeks.
It may take 4 months to a year for your partner to get pregnant after vasectomy reversal. Some women get pregnant in the first few months, while others may take years. Pregnancy rates can depend on the amount of time between the vasectomy and reversal. Sperm return to the semen faster and pregnancy rates are highest when the reversal is done sooner after the vasectomy.
Next to pregnancy, testing the sperm count is the only way to tell if the surgery worked. Your urologist will test your semen every 2 to 3 months until your sperm count holds steady or your partner gets pregnant. Sperm often appear in the semen within a few months after a vasovasostomy. It may take from 3 to 15 months after a vasoepididymostomy.
In either case, if the reversal works, you should stay fertile for many years. Only about 5 out of 100 men later get scars in the reconnected part. The scars could block the outflow of sperm all over again.
How successful is vasectomy reversal?
Microsurgical reconstructive techniques for vasectomy reversal have varying success rates. Two important predictors of success are time since vasectomy and age of female partner; reversals performed less than 15 years after vasectomy and having a female partner younger than 40 years are favorable predictors 80.
A large retrospective multi-institutional study involving 1,469 men who underwent microsurgical reconstructive techniques showed a linear decline in patency and pregnancy rates as the time since vasectomy increased 81. Intervals of less than three years showed patency and pregnancy rates of 97% and 76%, respectively; intervals between three and eight years, 88% and 53%; intervals between nine and 14 years, 79% and 44%; and intervals of 15 years or longer, 71% and 30% 81. A smaller retrospective series of 213 microsurgical vasectomy reversal procedures (performed by one surgeon) showed similar patency rates regardless of interval; pregnancy rates were statistically lower (44%) for intervals greater than 15 years compared with less than 15 years (82% to 89%) 82.
A more recent retrospective study of 334 patients undergoing vasectomy reversal (performed by one surgeon) showed similar patency and pregnancy rates regardless of interval. In this study, the only independent predictor of postreversal pregnancy was age of the female partner 80. This finding is identical to that of a retrospective series of 294 vasectomy reversals (performed by three surgeons) that demonstrated lower pregnancy rates if the female partner was 40 years or older than if the female partner was younger than 40 years (14% vs. 56%) 83. Presence of sperm granuloma, one-layer vs. two-layer microsurgical vasovasostomy, and type of anesthesia used appear to have no effect on success rates 82.
Aside from the variability in success rates, microsurgical vasectomy reversal procedures have significant economic implications. The cost of a successful vasectomy reversal, that is, one that leads to a successful pregnancy carried to delivery, ranges from $16,000 to $30,000. This is mostly an out-of-pocket expense for the individual or couple 84.
Who does vasectomy reversals?
Vasectomy reversals are most often done by urologists, but not all urologists do this type of surgery often. You should ask your urologist how many he/she has done, and to what level of success. If your urologist thinks you should have microsurgery, you should ask about his/her track record. This technique calls for extra training and expertise.
Can all vasectomies be reversed?
Almost all vasectomies can be reversed. But if the vasectomy was done while fixing a hernia in the groin it may not be as easy to join the ends of the vas. The ends also may not be able to be joined if a very long piece was removed during the vasectomy, but this is rare.
Is age a factor in conceiving after a vasectomy reversal?
Your age shouldn’t affect the results of your vasectomy reversal. Most men keep making sperm for many years after their partners stop making eggs. Women become less fertile starting in their mid-30s, with a major drop around age 37. Your partner should check with her gynecologist to see if she is still ovulating before you agree to a reversal.
Are there alternatives to vasectomy reversal?
There are other ways to get your partner pregnant without a reversal. Your urologist can take sperm from your testis or epididymis using a needle or by surgery (“sperm retrieval”). But sperm taken this way can’t be used in basic, low-cost office artificial inseminations. Instead, these sperm need more complex, costly ($12,000 to $17,000) in vitro fertilization (IVF) techniques using intracytoplasmic sperm injection (ICSI).
Most centers have about 4 out of 10 pregnancy rate with IVF/ICSI if the female partner is younger than 37. The pregnancy rates are much lower if she is older. Studies show that reversals are more cost-effective in reaching pregnancy than sperm retrieval and IVF/ICSI. Another plus of reversal over sperm retrieval/IVF is the chance for future pregnancies.
Your choice may be influenced by which methods your health plan covers. You might also weigh cost, years since vasectomy (and the chance of needing an epididymovasostomy), and your partner’s age.
If a vasectomy reversal fails, should I try it again?
When done by skilled microsurgeons, success rates for repeat reversals are often the same as for first reversals. Your urologist will review the record of your prior surgery to help you decide. If sperm were found in the vasal fluid then, he/she will likely do a repeat vasovasostomy, which is more likely to succeed.
How much does a vasectomy reversal cost?
The cost of a a successful vasectomy reversal, that is, one that leads to a successful pregnancy carried to delivery, ranges between about $16,000 to $30,000. Most health plans don’t pay for vasectomy reversals. You should talk with your health plan early in the planning to find out what they will cover.
Will a vasectomy reversal cure testis pain from my vasectomy?
Very few men get pain in the testis after a vasectomy that’s bad enough for them to ask about reversal. Because these cases are rare, there aren’t many studies of groups of these men. These studies suggest that it works for most men. Still, your urologist can’t tell beforehand if a reversal will cure your pain.
References- Dassow, P., & Bennett, J. M. (2006). Vasectomy: An update. American Family Physician, 74, 2069-2074.
- Eisenberg ML and Lipshultz LI: Estimating the Number of Vasectomies Performed Annually in the United States: Data From the National Survey of Family Growth. The Journal of urology 2010; 184: 2068.
- Barone MA, Hutchinson PL, Johnson CH et al: Vasectomy in the United States, 2002. J Urol 2006; 176: 232.
- Barone MA, Hutchinson PL, Johnson CH, Hsia J, Wheeler J. Vasectomy in the United States, 2002. J Urol. 2006;176(1):232–236.
- Haws JM, Morgan GT, Pollack AE et al: Clinical aspects of vasectomies performed in the United States in 1995. Urology 1998; 52: 685.
- Hendrix NW, Chauhan SP, Morrison JC. Sterilization and its consequences. Obstet Gynecol Surv. 1999;54:766–77.
- Mosher WD, Martinez GM, Chandra A, Abma JC, Willson SJ. Use of contraception and use of family planning services in the United States: 1982–2002. Adv Data. 2004;350:1–36.
- Martinez GM, Chandra A, Amba JC et al: Fertility, contraception, and fatherhood: data on men and women from cycle 6 (2002) of the 2002 National Survey of Family Growth. Vital and Health Statistics 2006; 23: 1.
- Trussell J, Lalla AM, Doan QV et al: Cost effectiveness of contraceptives in the United States. Contraception 2009; 79: 5.
- Chandra A, Martinez GM, Mosher WD et al: Fertility, family planning, and reproduction health of U.S. women: data from the 2002 National Survey of Family Growth. Vital and Health Statistics 2005; 23: 1.
- Anderson JE, Warner L, Jamieson DJ et al: Contraceptive sterilization use among married men in the United States: results from the male sample of the National Survey of Family Growth. Contraception 2010; 82: 230.
- Department of Economic and Social Affairs Population Division: World Contraceptive Use 2009. United Nations 2009.
- The risk of pregnancy after vasectomy. Obstetrics and Gynecology. 2004;103:848–850. https://www.ncbi.nlm.nih.gov/pubmed/15121555
- A comparison of women’s regret following vasectomy versus tubal sterilization. Obstetrics and Gynecology. 2002;99:1073–1079. https://www.ncbi.nlm.nih.gov/pubmed/12052602
- Cox B, Sneyd MJ, Paul C, Delahunt B, Skegg DC. Vasectomy and risk of prostate cancer. JAMA. 2002;287:3110–5.
- Dennis LK, Dawson DV, Resnick MI. Vasectomy and the risk of prostate cancer: a meta-analysis examining vasectomy status, age at vasectomy, and time since vasectomy. Prostate Cancer Prostatic Dis. 2002;5:193–203.
- Moller H, Knudsen LB, Lynge E. Risk of testicular cancer after vasectomy: cohort study of over 73,000 men. BMJ. 1994;309:295–9.
- Schwingl PJ, Guess HA. Safety and effectiveness of vasectomy. Fertil Steril. 2000;73:923–36.
- Vasectomy. http://www.auanet.org/guidelines/vasectomy-(2012-amended-2015)]
- American Academy of Family Physicians. Vasectomy: What to expect. https://familydoctor.org/vasectomy-what-to-expect/
- Potts JM, Pasqualotto FF, Nelson D, Thomas AJ Jr, Agarwal A. Patient characteristics associated with vasectomy reversal. J Urol. 1999;161(6):1835–1839.
- Hendry WF. Vasectomy and vasectomy reversal. Br J Urol. 1994;73(4):337–344.
- New Study Finds Vasectomy Does Not Increase Prostate Cancer Risk. https://www.nichd.nih.gov/news/releases/vasectomy
- Griffin T, Tooher R, Nowakowski K, Lloyd M, Maddern G. How little is enough? The evidence for post-vasectomy testing. J Urol. 2005;174(1):29–36.
- Hancock P, McLaughlin E; British Andrology Society. British Andrology Society guidelines for the assessment of post vasectomy semen samples (2002). J Clin Pathol. 2002;55(11):812–816.
- World Health Organization. WHO Laboratory Manual for the Examination of Human Semen and Sperm-Cervical Mucus Interaction. 4th ed. Cambridge, United Kingdom: Cambridge University Press. 1999.
- Klotz KL, Coppola MA, Labrecque M, et al. Clinical and consumer trial performance of a sensitive immunodiagnostic home test that qualitatively detects low concentrations of sperm following vasectomy. J Urol. 2008;180(6):2569–2576.
- Koslov DS, Andersson K-E. Physiological and pharmacological aspects of the vas deferens—an update. Frontiers in Pharmacology. 2013;4:101. doi:10.3389/fphar.2013.00101. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3749770/
- Christensen P, al-Aqidi OA, Jensen FS, Dorflinger T. Vasectomy. A prospective, randomized trial of vasectomy with bilateral incision versus the Li vasectomy [in Danish]. Ugeskr Laeger. 2002;164:2390–4.
- Sokal D, McMullen S, Gates D, Dominik R. for the Male Sterilization Investigator Team. A comparative study of the no scalpel and standard incision approaches to vasectomy in 5 countries. J Urol. 1999;162:1621–5.
- Cook LA, Pun A, van Vliet H, Gallo MF, Lopez LM. Scalpel versus no-scalpel incision for vasectomy. Cochrane Database Syst Rev. 2007;(2):CD004112.
- White MA, Maatman TJ. Comparative analysis of effectiveness of two local anesthetic techniques in men undergoing no-scalpel vasectomy. Urology. 2007;70(6):1187–1189.
- Aradhya KW, Best K, Sokal DC. Recent developments in vasectomy. BMJ. 2005;330:296–9.
- Trussell J, Kowal D. The essentials of contraception: efficacy, safety, and personal considerations. In: Hatcher RA, Trussell J, Stewart F, Cates W Jr, Stewart GK, Guest F, eds. Contraceptive Technology. 17th ed. New York, N.Y.: Ardent Media, 1998:211–47.
- Schmidt SS. Technics and complications of elective vasectomy. The role of spermatic granuloma in spontaneous recanalization. Fertil Steril. 1966;17:467–82.
- Chen-Mok M, Bangdiwala SI, Dominik R, Hays M, Irsula B, Sokal DC. Termination of a randomized controlled trial of two vasectomy techniques. Control Clin Trials. 2003;24:78–84.
- Labrecque M, Nazerali H, Mondor M, Fortin V, Nasution M. Effectiveness and complications associated with 2 vasectomy occlusion techniques. J Urol. 2002;168:2495–8.
- Sokal D, Irsula B, Chen-Mok M, Labrecque M, Barone MA. A comparison of vas occlusion techniques: cautery more effective than ligation and excision with fascial interposition. BMC Urol. 2004;4:12.
- Cook LA, Van Vliet H, Lopez LM, Pun A, Gallo MF. Vasectomy occlusion techniques for male sterilization. Cochrane Database Syst Rev. 2007;(2):CD003991.
- Marie Stopes International. Vasectomy—your questions answered. https://www.mariestopes-us.org/
- Li SQ, Xu B, Hou YH, Li CH, Pan QR, Cheng DS. Relationship between vas occlusion techniques and recanalization. Adv Contracept Deliv Syst. 1994;10:153–9.
- Schmidt SS, Minckler TM. The vas after vasectomy: comparison of cauterization methods. Urology. 1992;40:468–70.
- Shapiro EI, Silber SJ. Open-ended vasectomy, sperm granuloma, and postvasectomy orchialgia. Fertil Steril. 1979;32:546–50.
- Errey BB, Edwards IS. Open-ended vasectomy: an assessment. Fertil Steril. 1986;45:843–6.
- Hancock P, McLaughlin E. British Andrology Society guidelines for the assessment of post vasectomy semen samples (2002). J Clin Pathol. 2002;55:812–6.
- Christensen RE, Maples DC Jr. Postvasectomy semen analysis: are men following up?. J Am Board Fam Pract. 2005;18:44–7.
- Cortes M, Flick A, Barone MA, Amatya R, Pollack AE, Otero-Flores J, et al. Results of a pilot study of the time to azoospermia after vasectomy in Mexico City. Contraception. 1997;56:215–22.
- Chawla A, Bowles B, Zini A. Vasectomy follow-up: clinical significance of rare nonmotile sperm in postoperative semen analysis. Urology. 2004;64:1212–5.
- Badrakumar C, Gogoi NK, Sundaram SK. Semen analysis after vasectomy: when and how many?. BJU Int. 2000;86:479–81.
- Sharlip ID, Belker AM, Honig S, et al. Vasectomy: American Urological Association Guideline. American Urological Association Research and Education, Inc. http://www.auanet.org/guidelines/vasectomy-(2012-amended-2015)]
- Vasectomy. American Urological Association. http://www.auanet.org/guidelines/vasectomy-(2012-amended-2015)]
- Lemack GE and Goldstein M: Presence of sperm in the pre-vasectomy reversal semen analysis: incidence and implications. J Urol 1996; 155: 167.
- Birth Control Failure. http://americanpregnancy.org/preventing-pregnancy/birth-control-failure
- Mosher WD, Martinez GM, Chandra A, Abma JC, Willson SJ. Use of contraception and use of family planning services in the United States: 1982–2002. Adv Data 2004;350:18.
- Black T and Francome C: The evolution of the Marie Stopes electrocautery no-scalpel vasectomy procedure. J Fam Plann Reprod Health Care 2002; 28: 137.
- Schiff J, Chan P, Li PS et al: Outcome and late failures compared in 4 techniques of microsurgical vasoepididymostomy in 153 consecutive men. J Urol 2005; 174: 651.
- Marshall S and Lyon RP: Variability of sperm disappearance from the ejaculate after vasectomy. J Urol 1972; 107: 815.
- Marwood RP and Beral V: Disappearance of spermatozoa from ejaculate after vasectomy. Br Med J 1979; 1: 87.
- Edwards IS and Farlow JL: Non-motile sperms persisting after vasectomy: do they matter? Br Med J 1979; 1: 1019.
- Smucker DR, Mayhew HE, Nordlund DJ et al: Postvasectomy semen analysis: why do patients don’t follow-up. JABFP 1991; 4: 5.
- Barone MA, Nazerali H, Cortes M et al: A prospective study of time and number of ejaculations to azoospermia after vasectomy by ligation and excision. J Urol 2003; 170: 892.
- Belker AM, Sexter MS, Sweitzer SJ et al: The high rate of noncompliance for post-vasectomy semen examination: medical and legal considerations. J Urol 1990; 144: 284.
- Bedford JM and Zelikovsky G: Viability of spermatozoa in the human ejaculate after vasectomy. Fertil Steril 1979; 32: 460.
- Labrecque M, Hays M, Chen-Mok M et al: Frequency and patterns of early recanalization after vasectomy. BMC Urol 2006; 6: 25.
- Edwards IS: Earlier testing after vasectomy, based on the absence of motile sperm. Fertil Steril 1993; 59: 431.
- Smith AG, Crooks J, Singh NP et al: Is the timing of post-vasectomy seminal analysis important? Br J Urol 1998; 81: 458.
- Sherlock DJ and Holl-Allen RT: Delayed spontaneous recanalization of the vas deferens. Br J Surg 1984; 71: 532.
- U.S. Centers for Disease Control and Prevention. Reproductive health: Contraception: How effective are birth control methods? https://www.cdc.gov/reproductivehealth/contraception/index.htm
- American Urological Association Foundation. What is a Vasectomy? http://www.urologyhealth.org/urologic-conditions/vasectomy?article=53
- FamilyDoctor.org. Vasectomy: What to expect. https://familydoctor.org/vasectomy-what-to-expect/
- Awsare NS, Krishnan J, Boustead GB, Hanbury DC, McNicholas TA. Complications of vasectomy. Ann R Coll Surg Engl. 2005;87(6):406–410.
- Leslie TA, Illing RO, Cranston DW, Guillebaud J. The incidence of chronic scrotal pain after vasectomy: a prospective audit. BJU Int. 2007;100(6):1330–1333.
- U.S. Centers for Disease Control and Prevention.Reproductive health: Contraception. How effective are birth control methods? https://www.cdc.gov/reproductivehealth/contraception/index.htm
- Practice Committee of the American Society for Reproductive Medicine. Vasectomy reversal. Fertil Steril. 2004;82(suppl 1):S194–8.
- Sharlip ID. What is the best pregnancy rate that may be expected from vasectomy reversal?. J Urol. 1993;149:1469–71
- Potts JM, Pasqualotto FF, Nelson D, Thomas AJ Jr, Agarwal A. Patient characteristics associated with vasectomy reversal. J Urol. 1999;161:1835–9.
- What is Vasectomy Reversal? http://www.urologyhealth.org/urologic-conditions/vasectomy-reversal?article=54
- Nagler HM, Jung H. Factors predicting successful microsurgical vasectomy reversal. Urol Clin North Am. 2009;36(3):383–390.
- Hernandez J, Sabanegh ES. Repeat vasectomy reversal after initial failure: overall results and predictors for success. J Urol. 1999;161(4):1153–1156.
- Magheli A, Rais-Bahrami S, Kempkensteffen C, Weiske WH, Miller K, Hinz S. Impact of obstructive interval and sperm granuloma on patency and pregnancy after vasectomy reversal. Int J Androl. 2010;33(5):730–735.
- Belker AM, Thomas AJ Jr, Fuchs EF, Konnak JW, Sharlip ID. Results of 1,469 microsurgical vasectomy reversals by the Vasovasostomy Study Group. J Urol. 1991;145(3):505–511
- Boorjian S, Lipkin M, Goldstein M. The impact of obstructive interval and sperm granuloma on outcome of vasectomy reversal. J Urol. 2004;171(1):304–306.
- Gerrard ER Jr, Sandlow JI, Oster RA, Burns JR, Box LC, Kolettis PN. Effect of female partner age on pregnancy rates after vasectomy reversal. Fertil Steril. 2007;87(6):1340–1344.
- Garceau L, Henderson J, Davis LJ, et al. Economic implications of assisted reproductive techniques: a systematic review. Hum Reprod. 2002;17(12):3090–3109.

{kind=link}