What is vesicoureteral reflux
Vesicoureteral reflux is a condition in which urine abnormally flows backward from the bladder to one or both ureters, thin tubes that connect the kidneys to the bladder and sometimes to the kidneys. Vesicoureteral reflux is most common in infants and young children. Most children don’t have long-term problems from vesicoureteral reflux.
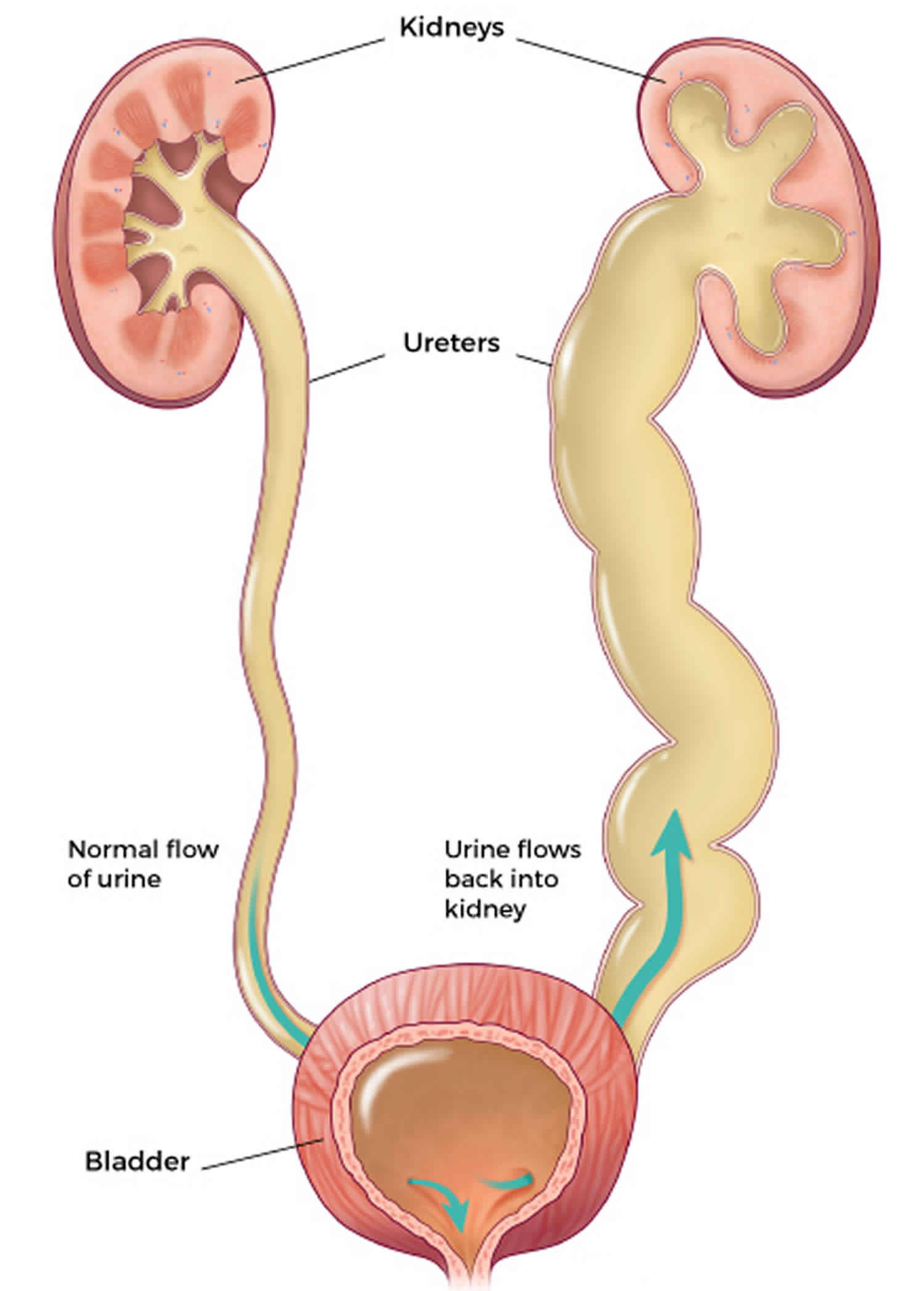
Normally, urine flows down the urinary tract, from the kidneys, through the ureters, into the bladder, where it is stored until urination occurs. The ureters normally have a one-way flap valve to prevent urine from traveling in both directions. During normal urination, the bladder muscle contracts and the sphincter muscle relaxes (this is the control mechanism), allowing the urine to leave the bladder through the urethra. With vesicoureteral reflux, some urine will flow back up—or reflux—through one or both ureters and may reach the kidneys.
Approximately 1% of healthy children have vesicoureteral reflux. About 75% of children with vesicoureteral reflux are girls. It is usually diagnosed around 2 to 3 years of age, but it can be discovered at any time.
Doctors usually rank vesicoureteral reflux as grade 1 through 5. Grade 1 is the mildest form of the condition, and grade 5 is the most serious. If backed-up urine reaches the kidneys, it can lead to infection, scarring, and even long-term kidney damage if left untreated. Fortunately, most kids with vesicoureteral reflux don’t have a severe case of it and outgrow it with no long-term complications.
Treatment depends on the severity of the vesicoureteral reflux. In mild cases, no treatment is necessary. Moderate to severe cases may be treated with antibiotic medicines to prevent infection. In cases where kids have infections and fevers along with the vesicoureteral reflux, surgery may be needed.
Moderate to severe vesicoureteral reflux, if not treated, can lead to serious health problems down the road. But with prompt treatment, long-term complications and damage to the kidneys can be prevented.
Figure 1. Vesicoureteral reflux
Vesicoureteral reflux grading
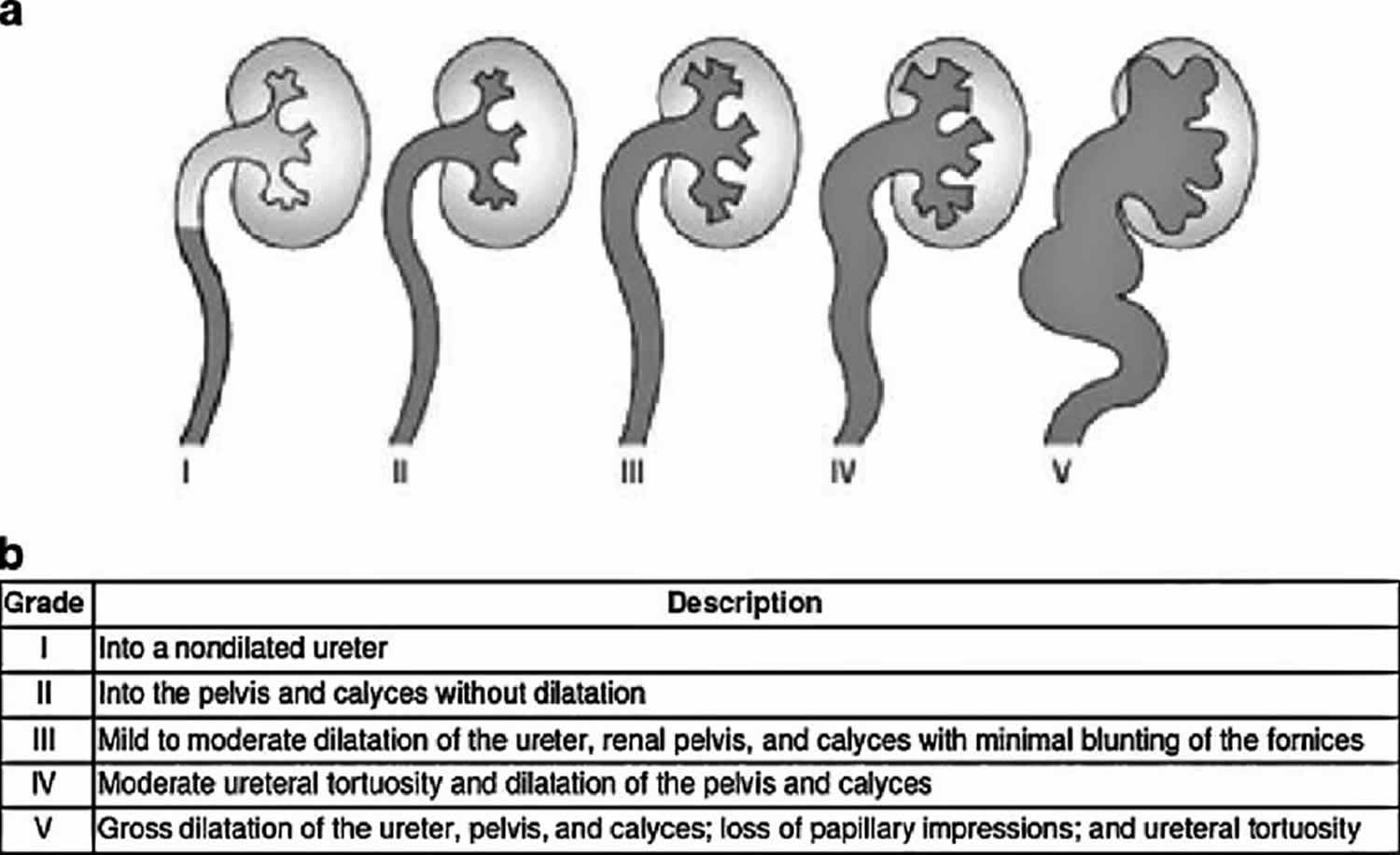
Doctors grade vesicoureteral reflux according to the degree of reflux. A grading system for reflux was established by the International Reflux Study Committee established in 1981 to aid with clinical management and prognostication 1. Five grades are defined based on the extent of reflux and degree of dilation of the upper tract on imaging (Figure 2). In the mildest cases, urine backs up only to the ureter (grade I). The most severe cases involve severe kidney swelling (hydronephrosis) and twisting of the ureter (grade V).
Spontaneous resolution of primary reflux is common. This is thought to be multi-factorial, due in part to remodeling of the ureterovesical junction, elongation of the intravesical ureter, and stabilization of bladder voiding dynamics over time. At birth, the likelihood of spontaneous resolution is inversely proportional to the initial grade of reflux; approximately 80% of low-grade (I and II) reflux will resolve spontaneously vs. about 50% of grade III reflux. Few or approximately 20% of high-grade (IV and V) reflux will resolve 2. For older children, resolution depends on both initial grade of reflux, gender, and age at initial diagnosis 3. Other factors that affect reflux resolution include voiding dysfunction, presence of renal scarring, and occurrence of reflux during bladder filling or emptying. In general, reflux is more likely to resolve in younger patients with low-grade reflux and normal renal ultrasound.
Figure 2. Vesicoureteral reflux grading
Contact your doctor right away if your child develops any of the signs or symptoms of a urinary tract infection (UTI), such as:
- A strong, persistent urge to urinate
- A burning sensation when urinating
- Abdominal or flank pain
- A hesitancy to urinate
Call your doctor about fever if your child:
- Is younger than 3 months old and has a rectal temperature of 100.4 °F (38 °C) or higher
- Is 3 months or older and has a fever of 102 °F (38.9 °C) or higher without any other explainable factors, such as a recent vaccination
In addition, call your doctor immediately if your infant has the following signs or symptoms:
- Changes in appetite. If your baby refuses several feedings in a row or eats poorly, contact the doctor.
- Changes in mood. If your baby is lethargic or unusually difficult to rouse, tell the doctor right away. Also let the doctor know if your baby is persistently irritable or has periods of inconsolable crying.
- Diarrhea. Contact the doctor if several of your baby’s stools are especially loose or watery.
- Vomiting. Occasional spitting up is normal. Contact the doctor if your baby spits up large portions of multiple feedings or vomits forcefully after feedings.
Vesicoureteral reflux causes
In many children, vesicoureteral reflux seems to be inherited (primary vesicoureteral reflux). If a mother has been treated for vesicoureteral reflux, as many as 50% of her children may also have it. Vesicoureteral reflux cannot be prevented, but most infections that result from vesicoureteral reflux can be.
Normally, urine flows from the kidneys to the bladder, but defects in one or both ureters can allow it to flow the other way. So can a blockage in the ureters or in the bladder.
Children with primary vesicoureteral reflux are born with a defect in the valve that normally prevents urine from flowing backward from the bladder into the ureters. Primary vesicoureteral reflux is the most common type of vesicoureteral reflux affecting kids. If a child is born with primary vesicoureteral reflux, it means that a ureter didn’t grow long enough while the baby was in the womb. This can affect the valve where the ureter enters the bladder. If the valve doesn’t shut properly, urine can flow back up the ureters to reach the kidney. As your child grows, the ureters lengthen and straighten, which may improve the valve function and eventually resolve the vesicoureteral reflux. Primary vesicoureteral reflux tends to run in families, which indicates that it may be genetic, but the exact cause of the defect is unknown.
If a blockage in the urinary tract obstructs the flow of urine and causes it to go back into the kidneys, it’s called secondary vesicoureteral reflux. Kids with this type of vesicoureteral reflux often have reflux in both ureters. Secondary vesicoureteral reflux can be caused by nerve damage, infection, or pressure on the ureter from another organ, such as an enlarged prostate often causing abnormally high pressure inside the bladder.
Primary vesicoureteral reflux
Primary vesicoureteral reflux will often get better and will go away as a child gets older.
Until vesicoureteral reflux goes away on its own, doctors treat any UTIs that develop with antibiotics, a type of medicine that fights bacteria. Treating UTIs quickly and preventing UTIs from developing will make it less likely your child will have a kidney infection.
Your child’s doctor also may consider the use of a long-term, low-dose antibiotic to prevent UTIs. Researchers have found that daily use of a low-dose antibiotic may help many children with vesicoureteral reflux. Talk with your child’s doctor about using antibiotics. The bacteria that cause these infections can become harder to fight when antibiotics are used long term.
Sometimes doctors will consider surgery for a child who has vesicoureteral reflux with repeat UTIs, particularly if the child has renal scarring or severe reflux that is not improving. Doctors can use surgery to correct your child’s reflux and prevent urine from flowing back to the kidney.
In certain cases, treatment may include the use of bulking injections. Doctors inject a small amount of gel-like liquid into the bladder wall near the opening of the ureter. The gel makes a bulge in the bladder wall, which acts like a valve to the ureter if a child’s valve doesn’t work properly. The doctor provides the treatment using general anesthesia and a child can usually go home the same day.
Secondary vesicoureteral reflux
Doctors treat secondary vesicoureteral reflux after finding the exact cause of the condition. Treatment may include
- surgery to remove a blockage
- antibiotics to prevent or treat UTIs
- surgery to correct an abnormal bladder or ureter
- intermittent urinary catheterization—draining the bladder by inserting a catheter through the urethra to the bladder. You can do this at home if your child’s bladder does not empty properly.
Risk factors for vesicoureteral reflux
Risk factors for vesicoureteral reflux include:
- Bladder and bowel dysfunction. Children with bladder and bowel dysfunction hold their urine and stool and experience recurrent urinary tract infections, which can contribute to vesicoureteral reflux.
- Race. White children appear to have a higher risk of vesicoureteral reflux.
- Sex. Generally, girls have about double the risk of having this condition as boys do. The exception is for vesicoureteral reflux that’s present at birth, which is more common in boys.
- Age. Infants and children up to age 2 are more likely to have vesicoureteral reflux than older children are.
- Family history. Primary vesicoureteral reflux tends to run in families. Children whose parents had the condition are at higher risk of developing it. Siblings of children who have the condition also are at higher risk, so your doctor may recommend screening for siblings of a child with primary vesicoureteral reflux.
Can I prevent vesicoureteral reflux?
You can’t prevent vesicoureteral reflux, but good habits may help keep your child’s urinary tract as healthy as possible. To prevent some bladder infections and bladder control problems, have your child:
- drink enough liquids based on the doctor’s advice.
- follow good bathroom habits, such as urinating regularly and wiping front to back.
- changed as soon as possible after his or her diaper becomes dirty, if he or she is not potty trained.
- get treated for constipation if necessary. Try to prevent your child’s constipation if possible.
- treated for related health problems such as urinary incontinence or fecal incontinence.
Vesicoureteral reflux symptoms
There are no specific signs and symptoms of vesicoureteral reflux, however children who have had a urinary tract infection (UTI) with a fever are more likely to have vesicoureteral reflux. Urinary tract infections (UTIs) and vesicoureteral reflux can lead to kidney damage, so occasionally patients have symptoms of renal problems.
Urinary tract infections commonly occur in people with vesicoureteral reflux. A urinary tract infection (UTI) doesn’t always cause noticeable signs and symptoms, though most people have some.
Urinary tract infection (UTI) signs and symptoms can include:
- A strong, persistent urge to urinate
- A burning sensation when urinating
- Passing frequent, small amounts of urine
- Blood in the urine (hematuria) or cloudy, strong-smelling urine
- Fever
- Pain in your side (flank) or abdomen
- Hesitancy to urinate or holding urine to avoid the burning sensation
Lower tract infection (in the bladder):
- frequent or urgent need to urinate
- a burning sensation while urinating
- blood in the urine, or urine that is cloudy or foul smelling
Upper tract infection (in the ureters or kidneys):
- pain in the side or abdomen
- fever and chills
A UTI may be difficult to diagnose in children, who may have only nonspecific signs and symptoms. Signs and symptoms in infants with a UTI may also include:
- An unexplained fever
- Diarrhea
- Lack of appetite
- Irritability
As your child gets older, untreated vesicoureteral reflux can lead to:
- Bed-wetting
- Constipation or loss of control over bowel movements
- High blood pressure
- Protein in urine
- Kidney failure
Another indication of vesicoureteral reflux, which may be detected before birth by sonogram, is swelling of the kidneys or the urine-collecting structures of one or both kidneys (hydronephrosis) in the fetus, caused by the backup of urine into the kidneys.
Vesicoureteral reflux complications
Kidney damage is the primary concern with vesicoureteral reflux. The more severe the reflux, the more serious the complications are likely to be.
Complications may include:
- Kidney (renal) scarring. Untreated UTIs can lead to scarring, also known as reflux nephropathy, which is permanent damage to kidney tissue. Extensive scarring may lead to high blood pressure and kidney failure.
- High blood pressure (hypertension). Because the kidneys remove waste from the bloodstream, damage to your kidneys and the resultant buildup of wastes can raise your blood pressure.
- Kidney failure. Scarring can cause a loss of function in the filtering part of the kidney. This may lead to kidney failure, which can occur quickly (acute kidney failure) or may develop over time (chronic kidney disease).
Vesicoureteral reflux diagnosis
Vesicoureteral reflux is usually diagnosed after a child has a urinary tract infection (UTI) with a fever, but can be identified before the child is born on prenatal ultrasound. Urinalysis — lab analysis of a urine sample — can reveal whether your child has a urinary tract infection (UTI).
Kidney and bladder ultrasound. Also called sonography, this imaging method uses high-frequency sound waves to produce images of the kidney and bladder. Ultrasound can detect structural abnormalities. This same technology, often used during pregnancy to monitor fetal development, may also reveal swollen kidneys in the baby, an indication of primary vesicoureteral reflux.
Nuclear scan. This test, known as radionuclide cystogram, uses a procedure similar to that used for voiding cystourethrogram (VCUG), except that instead of dye being injected into your child’s bladder through the catheter, this test uses a radioactive tracer (radioisotope). The scanner detects the tracer and shows whether the urinary tract is functioning correctly.
Voiding cystourethrography (VCUG) is the gold standard for diagnosis of vesicoureteral reflux. A voiding cystourethrogram (VCUG) x-ray of the kidneys, ureters, bladder and urethra is necessary to evaluate and diagnose vesicoureteral reflux. A voiding cystourethrogram (VCUG), is a minimally invasive test that uses a special x-ray technology called fluoroscopy to visualize your child’s urinary tract and bladder.
Voiding cystourethrogram (VCUG) test uses X-rays of the bladder when it’s full and when it’s emptying to detect abnormalities. A thin, flexible tube (catheter) is inserted through the urethra and into the bladder while your child lies on his or her back on an X-ray table.
After contrast dye is injected into the bladder through the catheter, your child’s bladder is X-rayed in various positions. Then the catheter is removed so that your child can urinate, and more X-rays are taken of the bladder and urethra during urination to see whether the urinary tract is functioning correctly.
Risks associated with this test include discomfort from the catheter or from having a full bladder and the possibility of a new urinary tract infection.
A voiding cystourethrogram (VCUG) can help:
- diagnose vesicoureteral reflux.
- determine why your child has recurring urinary tract infections
- discover if antibiotic treatment or anti-reflux surgery was effective
- check if there are any abnormalities or blockages of the urethra
Once diagnosed, the vesicoureteral reflux is graded. The grade of vesicoureteral reflux indicates how much urine is flowing backward into the ureters and kidneys and helps the provider to determine which type of care is most appropriate. Vesicoureteral reflux is graded on a scale of 1 to 5, with 5 being the most serious.
Vesicoureteral reflux treatment
Treatment options for vesicoureteral reflux depend on the severity of the condition. Children with mild cases of primary vesicoureteral reflux may eventually outgrow the disorder. In this case, your doctor may recommend a wait-and-see approach. As a child gets older, the ureter gets longer and straighter, and the valve where the ureter enters the bladder is able to shut correctly.
Vesicoureteral reflux that occurs with a UTI needs prompt antibiotic treatment to keep the infection from spreading to the kidneys. Kids who are put on antibiotics should take them for as long as prescribed, even if they start to feel better early on.
Urinary tract infections, which are so common to vesicoureteral reflux, can be painful. But you can take steps to ease your child’s discomfort until antibiotics clear the infection. They include:
- Encourage your child to drink fluids, particularly water. Drinking water dilutes urine and may help flush out bacteria. Avoid juices and soft drinks containing citrus and caffeine until your child’s infection has cleared. They can irritate the bladder and tend to aggravate the frequent or urgent need to urinate.
- Provide a warm blanket or towel. Place a towel or blanket in the dryer for a few minutes to warm it up. Be sure the towel or blanket is just warm, not hot, and then place it over your child’s abdomen. The warmth can help minimize feelings of bladder pressure or pain.
If bladder and bowel dysfunction contributes to your child’s vesicoureteral reflux, encourage healthy toileting habits. Avoiding constipation and emptying the bladder every two hours while awake may help.
For more severe vesicoureteral reflux, treatment options include:
Medications
Urinary tract infections (UTIs) require prompt treatment with antibiotics to keep the infection from moving to the kidneys. To prevent urinary tract infections (UTIs), doctors may also prescribe antibiotics at a lower dose than for treating an infection.
A child being treated with medication needs to be monitored for as long as he or she is taking antibiotics. This includes periodic physical exams and urine tests to detect breakthrough infections — urinary tract infections (UTIs) that occur despite the antibiotic treatment — and occasional radiographic scans of the bladder and kidneys to determine if your child has outgrown vesicoureteral reflux.
Vesicoureteral reflux surgery
Surgery for vesicoureteral reflux repairs the defect in the valve between the bladder and each affected ureter. A defect in the valve keeps it from closing and preventing urine from flowing backward. The most common type of surgery is ureteral reimplantation, in which one or both ureters are extended further into the bladder to correct the backflow of urine from the bladder to the ureters and kidneys. This type of surgery usually requires kids to spend a few days in the hospital while they recover.
Methods of surgical repair include:
- Open surgery. Performed using general anesthesia, this surgery requires an incision in the lower abdomen through which the surgeon repairs the malformation that’s causing the problem. This type of surgery usually requires a few days’ stay in the hospital, during which a catheter is kept in place to drain your child’s bladder. Vesicoureteral reflux may persist in a small number of children, but it generally resolves on its own without need for further intervention.
- Robotic-assisted laparoscopic surgery. Similar to open surgery, this procedure involves repairing the valve between the ureter and the bladder, but it’s performed using small incisions. Advantages include smaller incisions and possibly less bladder spasms than open surgery. But, preliminary findings suggest that robotic-assisted laparoscopic surgery may not have as high of a success rate as open surgery. The procedure was also associated with a longer operating time, but a shorter hospital stay.
- Endoscopic surgery also known as the deflux procedure. In this procedure, the doctor inserts a lighted tube (cystoscope) through the urethra to see inside your child’s bladder, then injects a bulking agent around the opening of the affected ureter to try to strengthen the valve’s ability to close properly. This method is minimally invasive compared with open surgery and presents fewer risks, though it may not be as effective as open reimplantation. Endoscopic surgery also requires general anesthesia, but generally can be performed as outpatient surgery. Most kids can leave the hospital on the same day that they have this procedure.
Estimated success rates of open and endoscopic reflux correction are 98.1% and 83.0%, respectively 4. Factors that affect the success of endoscopic injection include pre-operative reflux grade and presence of functional or anatomic bladder abnormalities including voiding dysfunction and duplicated collecting systems. Few studies have evaluated the long-term outcomes of endoscopic injection, and with variable results. In patients treated endoscopically, recurrent febrile UTI occurred in 0–21%, new renal damage in 9–12%, and recurrent reflux in 17–47.6% of treated ureters with at least 1 year follow-up 4.
References- International Reflux Study Committee (1981) Medical versus surgical treatment of primary vesicoureteral reflux: report of the International Reflux Study Committee. Pediatrics 67:392–400
- Knudson MJ, Austin JC, McMillan ZM, Hawtrey CE, Cooper CS (2007) Predictive factors of early spontaneous resolution in children with primary vesicoureteral reflux. J Urol 178:1684–1688
- Skoog SJ, Belman AB, Majd M (1987) A nonsurgical approach to the management of primary vesicoureteral reflux. J Urol 138:941–946
- Sung, Jennifer & Skoog, Steven. (2011). Surgical management of vesicoureteral reflux in children. Pediatric nephrology (Berlin, Germany). 27. 551-61. 10.1007/s00467-011-1933-7.





{kind=link}